
Effects of Bifidobacterium longum BB536 and Bifidobacterium breve MCC1274 on Body Composition in Normal and Overweight Adults in Randomized Placebo-Controlled Study

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Ethics
2.2. Participants
2.3. Intervention
2.4. Primary Outcomes
2.5. Secondary Outcomes
2.6. Diary Survey
2.7. Safety Assessment
2.8. Sample Size
2.9. Randomization
2.10. Statistical Analysis
3. Results
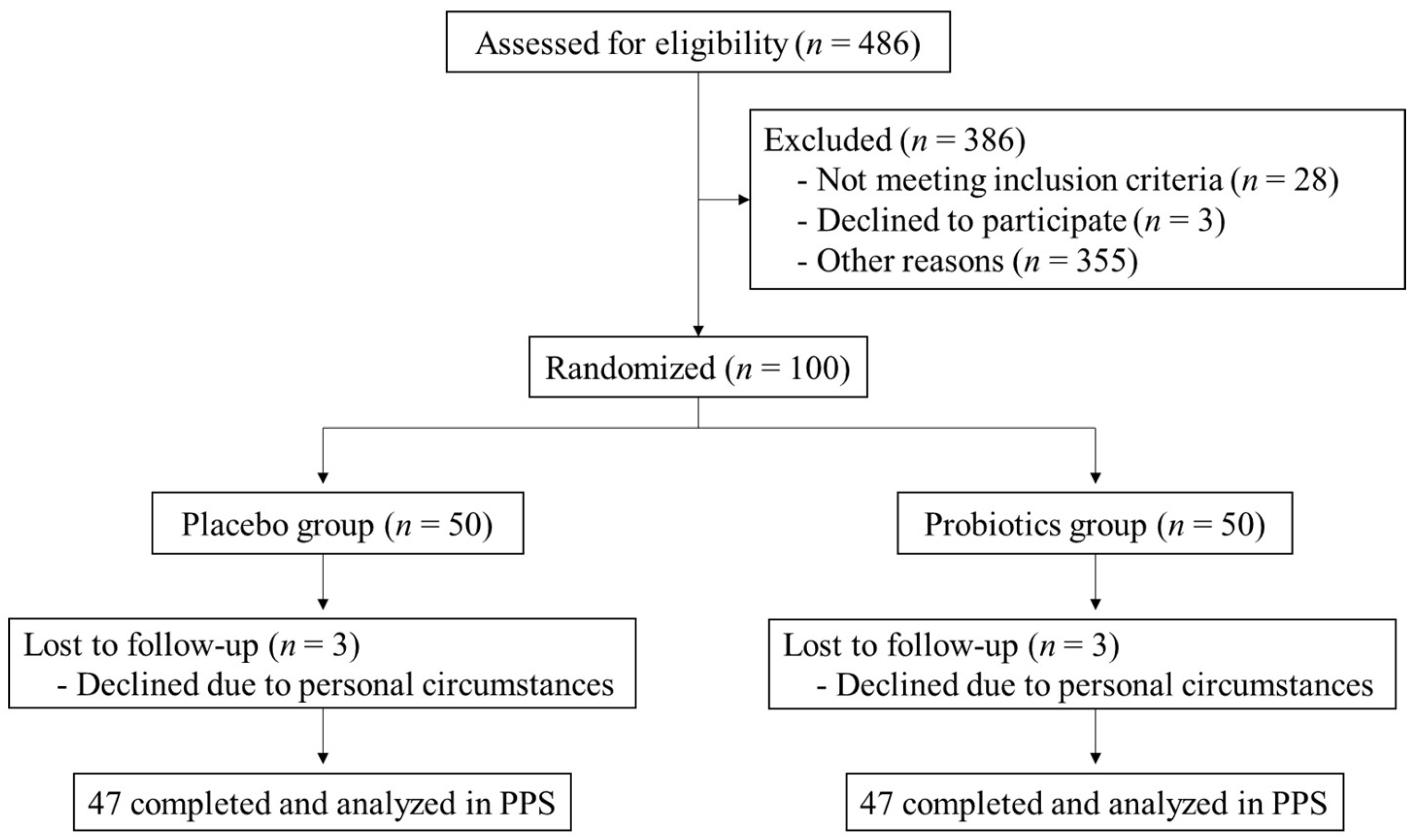
3.1. Participants
3.2. Participant Characteristics
3.3. Effects on Body Composition and Blood Parameters
3.4. Safety Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chooi, Y.C.; Ding, C.; Magkos, F. The epidemiology of obesity. Metabolism 2019, 92, 6–10. [Google Scholar] [CrossRef]
- Apovian, C.M. Obesity: Definition, comorbidities, causes, and burden. Am. J. Manag. Care 2016, 22, s176–s185. [Google Scholar] [PubMed]
- Mittal, B. Subcutaneous adipose tissue & visceral adipose tissue. Indian. J. Med. Res. 2019, 149, 571–573. [Google Scholar] [CrossRef] [PubMed]
- Safaei, M.; Sundararajan, E.A.; Driss, M.; Boulila, W.; Shapi′i, A. A systematic literature review on obesity: Understanding the causes & consequences of obesity and reviewing various machine learning approaches used to predict obesity. Comput. Biol. Med. 2021, 136, 104754. [Google Scholar] [CrossRef]
- Wadden, T.A.; Tronieri, J.S.; Butryn, M.L. Lifestyle modification approaches for the treatment of obesity in adults. Am. Psychol. 2020, 75, 235–251. [Google Scholar] [CrossRef] [PubMed]
- Wicinski, M.; Gebalski, J.; Golebiewski, J.; Malinowski, B. Probiotics for the Treatment of Overweight and Obesity in Humans—A Review of Clinical Trials. Microorganisms 2020, 8, 1148. [Google Scholar] [CrossRef]
- Angelakis, E.; Armougom, F.; Million, M.; Raoult, D. The relationship between gut microbiota and weight gain in humans. Future Microbiol. 2012, 7, 91–109. [Google Scholar] [CrossRef]
- El-Zahar, K.M.; Hassan, M.F.Y.; Al-Qaba, S.F. Protective Effect of Fermented Camel Milk Containing Bifidobacterium longum BB536 on Blood Lipid Profile in Hypercholesterolemic Rats. J. Nutr. Metab. 2021, 2021, 1557945. [Google Scholar] [CrossRef]
- Kurose, Y.; Minami, J.; Sen, A.; Iwabuchi, N.; Abe, F.; Xiao, J.; Suzuki, T. Bioactive factors secreted by Bifidobacterium breve B-3 enhance barrier function in human intestinal Caco-2 cells. Benef. Microbes 2019, 10, 89–100. [Google Scholar] [CrossRef]
- Kondo, S.; Kamei, A.; Xiao, J.Z.; Iwatsuki, K.; Abe, K. Bifidobacterium breve B-3 exerts metabolic syndrome-suppressing effects in the liver of diet-induced obese mice: A DNA microarray analysis. Benef. Microbes 2013, 4, 247–251. [Google Scholar] [CrossRef]
- Minami, J.; Kondo, S.; Yanagisawa, N.; Odamaki, T.; Xiao, J.Z.; Abe, F.; Nakajima, S.; Hamamoto, Y.; Saitoh, S.; Shimoda, T. Oral administration of Bifidobacterium breve B-3 modifies metabolic functions in adults with obese tendencies in a randomised controlled trial. J. Nutr. Sci. 2015, 4, e17. [Google Scholar] [CrossRef] [PubMed]
- Minami, J.; Iwabuchi, N.; Tanaka, M.; Yamauchi, K.; Xiao, J.Z.; Abe, F.; Sakane, N. Effects of Bifidobacterium breve B-3 on body fat reductions in pre-obese adults: A randomized, double-blind, placebo-controlled trial. Biosci. Microbiota Food Health 2018, 37, 67–75. [Google Scholar] [CrossRef]
- Sung, H.K.; Youn, S.J.; Choi, Y.; Eun, S.W.; Shin, S.M. Body Fat Reduction Effect of Bifidobacterium breve B-3: A Randomized, Double-Blind, Placebo Comparative Clinical Trial. Nutrients 2022, 15, 28. [Google Scholar] [CrossRef] [PubMed]
- Ishii, Y.; Matsuoka, S.; Kitano, R.; Yui, K.; Hosoi, T.; Orimo, H. Effects of Bifidobacterium bifidum B-3 and BB536 and N-acetylglucosamine-containing supplements on body composition and intestinal flora in mildly obese individuals: A randomized, double-blind, parallel-group comparative study. J. Jpn. Soc. Study Obes. 2016, 22, 133–144. [Google Scholar]
- Kadooka, Y.; Sato, M.; Imaizumi, K.; Ogawa, A.; Ikuyama, K.; Akai, Y.; Okano, M.; Kagoshima, M.; Tsuchida, T. Regulation of abdominal adiposity by probiotics (Lactobacillus gasseri SBT2055) in adults with obese tendencies in a randomized controlled trial. Eur. J. Clin. Nutr. 2010, 64, 636–643. [Google Scholar] [CrossRef] [PubMed]
- Shah, R.V.; Murthy, V.L.; Abbasi, S.A.; Blankstein, R.; Kwong, R.Y.; Goldfine, A.B.; Jerosch-Herold, M.; Lima, J.A.; Ding, J.; Allison, M.A. Visceral adiposity and the risk of metabolic syndrome across body mass index: The MESA Study. JACC Cardiovasc. Imaging 2014, 7, 1221–1235. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, N.; Okuda, T.; Shinohara, H.; Yamasaki, R.S.; Hirano, N.; Kang, J.; Ogawa, M.; Nishi, N.N. Relationship between Seasonal Changes in Food Intake and Energy Metabolism, Physical Activity, and Body Composition in Young Japanese Women. Nutrients 2022, 14, 506. [Google Scholar] [CrossRef]
- Cani, P.D.; Amar, J.; Iglesias, M.A.; Poggi, M.; Knauf, C.; Bastelica, D.; Neyrinck, A.M.; Fava, F.; Tuohy, K.M.; Chabo, C.; et al. Metabolic endotoxemia initiates obesity and insulin resistance. Diabetes 2007, 56, 1761–1772. [Google Scholar] [CrossRef]
- Monteiro, R.; Azevedo, I. Chronic inflammation in obesity and the metabolic syndrome. Mediat. Inflamm. 2010, 2010, 289645. [Google Scholar] [CrossRef]
- Liu, L.; Mei, M.; Yang, S.; Li, Q. Roles of chronic low-grade inflammation in the development of ectopic fat deposition. Mediat. Inflamm. 2014, 2014, 418185. [Google Scholar] [CrossRef]
- Xiao, L.; Harrison, D.G. Inflammation in Hypertension. Can. J. Cardiol. 2020, 36, 635–647. [Google Scholar] [CrossRef] [PubMed]
- Esteve, E.; Ricart, W.; Fernandez-Real, J.M. Dyslipidemia and inflammation: An evolutionary conserved mechanism. Clin. Nutr. 2005, 24, 16–31. [Google Scholar] [CrossRef] [PubMed]
- Berbudi, A.; Rahmadika, N.; Tjahjadi, A.I.; Ruslami, R. Type 2 Diabetes and its Impact on the Immune System. Curr. Diabetes Rev. 2020, 16, 442–449. [Google Scholar] [CrossRef] [PubMed]
- Park, S.J.; Sharma, A.; Lee, H.J. Postbiotics against Obesity: Perception and Overview Based on Pre-Clinical and Clinical Studies. Int. J. Mol. Sci. 2023, 24, 6414. [Google Scholar] [CrossRef] [PubMed]
- Van der Meulen, R.; Makras, L.; Verbrugghe, K.; Adriany, T.; De Vuyst, L. In vitro kinetic analysis of oligofructose consumption by Bacteroides and Bifidobacterium spp. indicates different degradation mechanisms. Appl. Environ. Microbiol. 2006, 72, 1006–1012. [Google Scholar] [CrossRef] [PubMed]
- Kimura, I.; Inoue, D.; Maeda, T.; Hara, T.; Ichimura, A.; Miyauchi, S.; Kobayashi, M.; Hirasawa, A.; Tsujimoto, G. Short-chain fatty acids and ketones directly regulate sympathetic nervous system via G protein-coupled receptor 41 (GPR41). Proc. Natl. Acad. Sci. USA 2011, 108, 8030–8035. [Google Scholar] [CrossRef] [PubMed]
- Kimura, I.; Ozawa, K.; Inoue, D.; Imamura, T.; Kimura, K.; Maeda, T.; Terasawa, K.; Kashihara, D.; Hirano, K.; Tani, T.; et al. The gut microbiota suppresses insulin-mediated fat accumulation via the short-chain fatty acid receptor GPR43. Nat. Commun. 2013, 4, 1829. [Google Scholar] [CrossRef]
- Sakurai, T.; Odamaki, T.; Xiao, J.Z. Production of Indole-3-Lactic Acid by Bifidobacterium Strains Isolated fromHuman Infants. Microorganisms 2019, 7, 340. [Google Scholar] [CrossRef]
- Roager, H.M.; Licht, T.R. Microbial tryptophan catabolites in health and disease. Nat. Commun. 2018, 9, 3294. [Google Scholar] [CrossRef]
- Lanis, J.M.; Alexeev, E.E.; Curtis, V.F.; Kitzenberg, D.A.; Kao, D.J.; Battista, K.D.; Gerich, M.E.; Glover, L.E.; Kominsky, D.J.; Colgan, S.P. Tryptophan metabolite activation of the aryl hydrocarbon receptor regulates IL-10 receptor expression on intestinal epithelia. Mucosal Immunol. 2017, 10, 1133–1144. [Google Scholar] [CrossRef]
- Postal, B.G.; Ghezzal, S.; Aguanno, D.; André, S.; Garbin, K.; Genser, L.; Brot-Laroche, E.; Poitou, C.; Soula, H.; Leturque, A.; et al. AhR activation defends gut barrier integrity against damage occurring in obesity. Mol. Metab. 2020, 39, 101007. [Google Scholar] [CrossRef]
- Koba, K.; Yanagita, T. Health benefits of conjugated linoleic acid (CLA). Obes. Res. Clin. Pract. 2014, 8, e525–e532. [Google Scholar] [CrossRef]
- Gao, S.; He, Y.; Zhang, L.; Liu, L.; Qu, C.; Zheng, Z.; Miao, J. Conjugated linoleic acid ameliorates hepatic steatosis by modulating intestinal permeability and gut microbiota in ob/ob mice. Food Nutr. Res. 2022, 66, 8226. [Google Scholar] [CrossRef]
- Schellekens, H.; Torres-Fuentes, C.; van de Wouw, M.; Long-Smith, C.M.; Mitchell, A.; Strain, C.; Berding, K.; Bastiaanssen, T.F.S.; Rea, K.; Golubeva, A.V.; et al. Bifidobacterium longum counters the effects of obesity: Partial successful translation from rodent to human. eBioMedicine 2021, 63, 103176. [Google Scholar] [CrossRef]
- Purnell, J.Q.; Kahn, S.E.; Samuels, M.H.; Brandon, D.; Loriaux, D.L.; Brunzell, J.D. Enhanced cortisol production rates, free cortisol, and 11beta-HSD-1 expression correlate with visceral fat and insulin resistance in men: Effect of weight loss. Am. J. Physiol. Endocrinol. Metab. 2009, 296, E351–E357. [Google Scholar] [CrossRef]
- Huang, C.Y.; Huang, H.L.; Yang, K.C.; Lee, L.T.; Yang, W.S.; Huang, K.C.; Tseng, F.Y. Serum Triglyceride Levels Independently Contribute to the Estimation of Visceral Fat Amount Among Nondiabetic Obese Adults. Medicine 2015, 94, e965. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Placebo (n = 47) | Probiotics (n = 47) | p Value | |
|---|---|---|---|
| Mean ± SD | Mean ± SD | ||
| Age | 50.11 ± 7.21 | 50.43 ± 7.59 | 0.835 b |
| Sex (Male/Female) | 33/14 | 33/14 | 1.000 c |
| Total fat area (cm2) a | 315.68 ± 68.52 | 316.61 ± 58.16 | 0.953 b |
| Visceral fat area (cm2) a | 112.77 ± 36.61 | 115.32 ± 35.91 | 0.741 b |
| Subcutaneous fat area (cm2) a | 202.91 ± 37.80 | 201.28 ± 35.65 | 0.904 b |
| Body fat mass (kg) | 22.45 ± 4.68 | 22.55 ± 5.07 | 0.928 b |
| Body fat percentage (%) | 30.65 ± 6.83 | 30.83 ± 7.22 | 0.903 b |
| Body weight (kg) | 73.74 ± 7.69 | 73.55 ± 7.51 | 0.900 b |
| BMI (kg/m2) | 26.02 ± 1.87 | 26.20 ± 1.77 | 0.643 b |
| Group | Week 0 | Week 16 | p Value (vs. Week 0) b | |
|---|---|---|---|---|
| Mean ± SD | Mean ± SD | |||
| Energy (kcal/day) | Placebo (n = 47) | 1761.1 ± 385.6 | 1799.7 ± 456.4 | 0.527 |
| Probiotics (n = 47) | 1851.9 ± 516.7 | 1871.6 ± 362.9 | 0.767 | |
| p value a | 0.337 | 0.400 | ||
| Protein (g/day) | Placebo (n = 47) | 64.0 ± 16.0 | 66.4 ± 18.7 | 0.344 |
| Probiotics (n = 47) | 67.0 ± 18.6 | 70.2 ± 14.2 | 0.154 | |
| p value a | 0.399 | 0.269 | ||
| Fat (g/day) | Placebo (n = 47) | 57.4 ± 17.7 | 60.0 ± 21.8 | 0.367 |
| Probiotics (n = 47) | 67.5 ± 23.0 | 67.5 ± 20.1 | 0.987 | |
| p value a | 0.018 | 0.088 | ||
| Carbohydrates (g/day) | Placebo (n = 47) | 222.0 ± 56.9 | 236.2 ± 57.3 | 0.064 |
| Probiotics (n = 47) | 226.0 ± 69.0 | 232.6 ± 48.4 | 0.467 | |
| p value a | 0.758 | 0.741 | ||
| Fiber (g/day) | Placebo (n = 47) | 10.6 ± 3.5 | 11.4 ± 3.7 | 0.173 |
| Probiotics (n = 47) | 10.7 ± 4.5 | 11.3 ± 3.0 | 0.410 | |
| p value a | 0.869 | 0.907 |
| Group | Baseline | Week 16 | p Value (vs. Baseline) c | |
|---|---|---|---|---|
| Mean ± SEM | Mean ± SEM | |||
| CT measurement | ||||
| Total fat area (cm2) a | Placebo (n = 44) | 315.68 ± 11.71 | 320.95 ± 11.04 | 0.115 |
| Probiotics (n = 45) | 316.61 ± 10.43 | 312.42 ± 10.87 | 0.233 | |
| p value b | 0.049 | |||
| Visceral fat area (cm2) a | Placebo (n = 44) | 112.77 ± 5.52 | 115.69 ± 5.70 | 0.199 |
| Probiotics (n = 45) | 115.32 ± 5.35 | 111.50 ± 5.31 | 0.068 | |
| p value b | 0.031 | |||
| Subcutaneous fat area (cm2) a | Placebo (n = 44) | 202.91 ± 10.33 | 205.26 ± 10.09 | 0.280 |
| Probiotics (n = 45) | 201.28 ± 8.67 | 200.91 ± 9.17 | 0.864 | |
| p value b | 0.373 | |||
| Bioelectrical impedance analysis | ||||
| Body fat mass (kg) | Placebo (n = 47) | 22.45 ± 0.68 | 23.32 ± 0.64 | <0.001 |
| Probiotics (n = 47) | 22.54 ± 0.74 | 22.86 ± 0.79 | 0.272 | |
| p value b | 0.107 | |||
| Body fat percentage (%) | Placebo (n = 47) | 30.64 ± 1.00 | 31.45 ± 0.92 | <0.001 |
| Probiotics (n = 47) | 30.83 ± 1.05 | 31.10 ± 1.08 | 0.401 | |
| p value b | 0.158 | |||
| Other parameters | ||||
| Body weight (kg) | Placebo (n = 47) | 73.74 ± 1.12 | 74.64 ± 1.14 | <0.001 |
| Probiotics (n = 47) | 73.55 ± 1.10 | 73.82 ± 1.13 | 0.244 | |
| p value b | 0.056 | |||
| BMI (kg/m2) | Placebo (n = 47) | 26.02 ± 0.27 | 26.35 ± 0.27 | <0.001 |
| Probiotics (n = 47) | 26.20 ± 0.26 | 26.28 ± 0.27 | 0.319 | |
| p value b | 0.046 | |||
| Triglycerides (mg/dL) | Placebo (n = 47) | 120.49 ± 7.84 | 127.57 ± 10.44 | 0.342 |
| Probiotics (n = 47) | 130.87 ± 11.78 | 108.98 ± 7.29 | 0.028 | |
| p value b | 0.021 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sato, S.; Arai, S.; Kato, K.; Yoshida, K.; Iwabuchi, N.; Sagami, T.; Tanaka, M. Effects of Bifidobacterium longum BB536 and Bifidobacterium breve MCC1274 on Body Composition in Normal and Overweight Adults in Randomized Placebo-Controlled Study. Nutrients 2024, 16, 815. https://doi.org/10.3390/nu16060815
Sato S, Arai S, Kato K, Yoshida K, Iwabuchi N, Sagami T, Tanaka M. Effects of Bifidobacterium longum BB536 and Bifidobacterium breve MCC1274 on Body Composition in Normal and Overweight Adults in Randomized Placebo-Controlled Study. Nutrients. 2024; 16(6):815. https://doi.org/10.3390/nu16060815
Chicago/Turabian StyleSato, Soichiro, Satoshi Arai, Kumiko Kato, Keisuke Yoshida, Noriyuki Iwabuchi, Toru Sagami, and Miyuki Tanaka. 2024. "Effects of Bifidobacterium longum BB536 and Bifidobacterium breve MCC1274 on Body Composition in Normal and Overweight Adults in Randomized Placebo-Controlled Study" Nutrients 16, no. 6: 815. https://doi.org/10.3390/nu16060815
APA StyleSato, S., Arai, S., Kato, K., Yoshida, K., Iwabuchi, N., Sagami, T., & Tanaka, M. (2024). Effects of Bifidobacterium longum BB536 and Bifidobacterium breve MCC1274 on Body Composition in Normal and Overweight Adults in Randomized Placebo-Controlled Study. Nutrients, 16(6), 815. https://doi.org/10.3390/nu16060815