

Understanding the Interplay of Dietary Intake and Eating Behavior in Type 2 Diabetes

 , , ,
, , ,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data Collection
2.2.1. Measurement of Demographic and Anthropometric Data
2.2.2. Measurement of Dietary Intake
2.2.3. Measurement of Eating Behavior
2.3. Ethical Consideration
2.4. Statistical Analysis
3. Results
3.1. General and Anthropometric Characteristics of the Studied Population
3.2. Dietary Intake in the Studied Population
3.3. Eating Behavior in the Studied Population
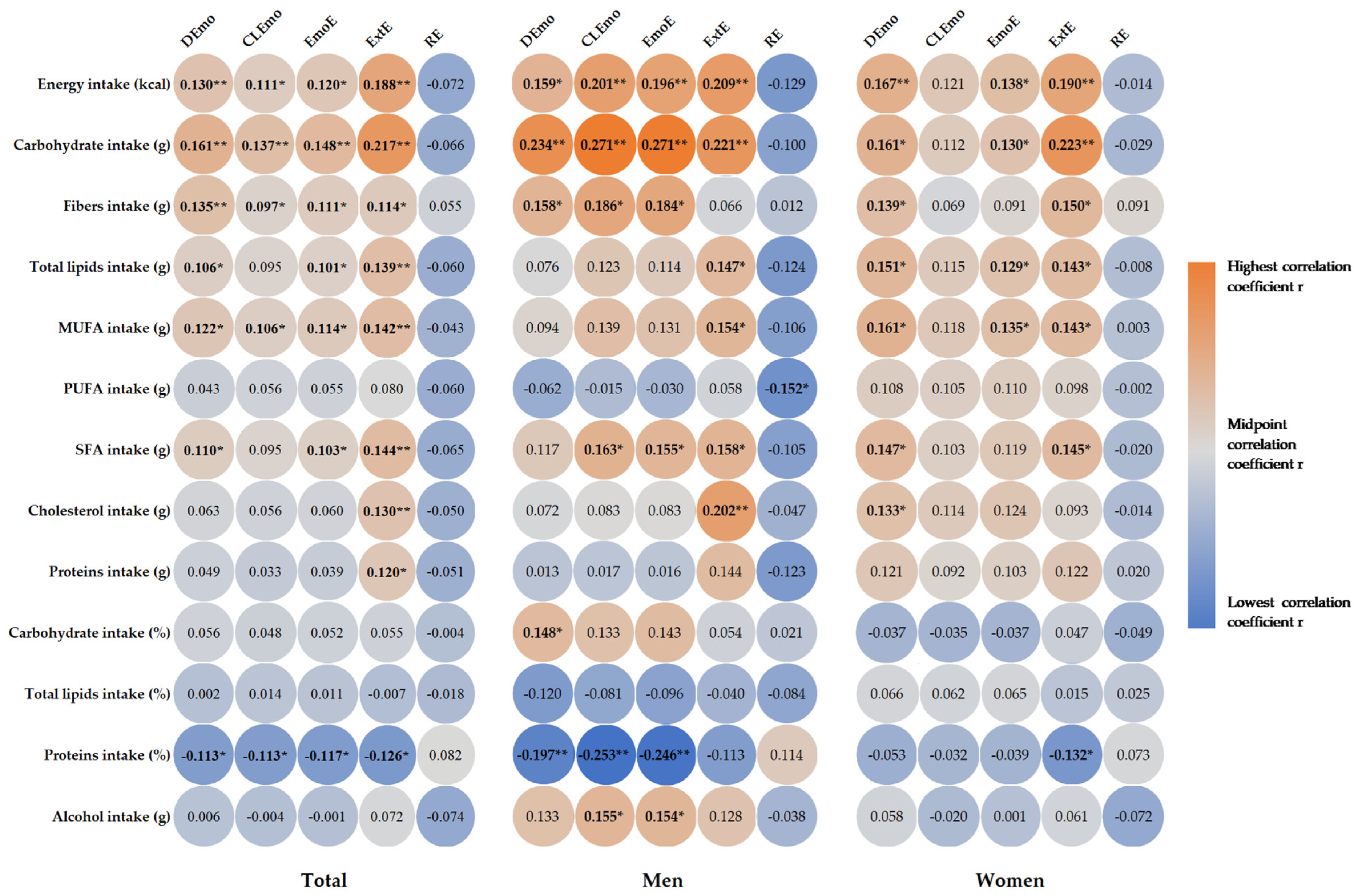
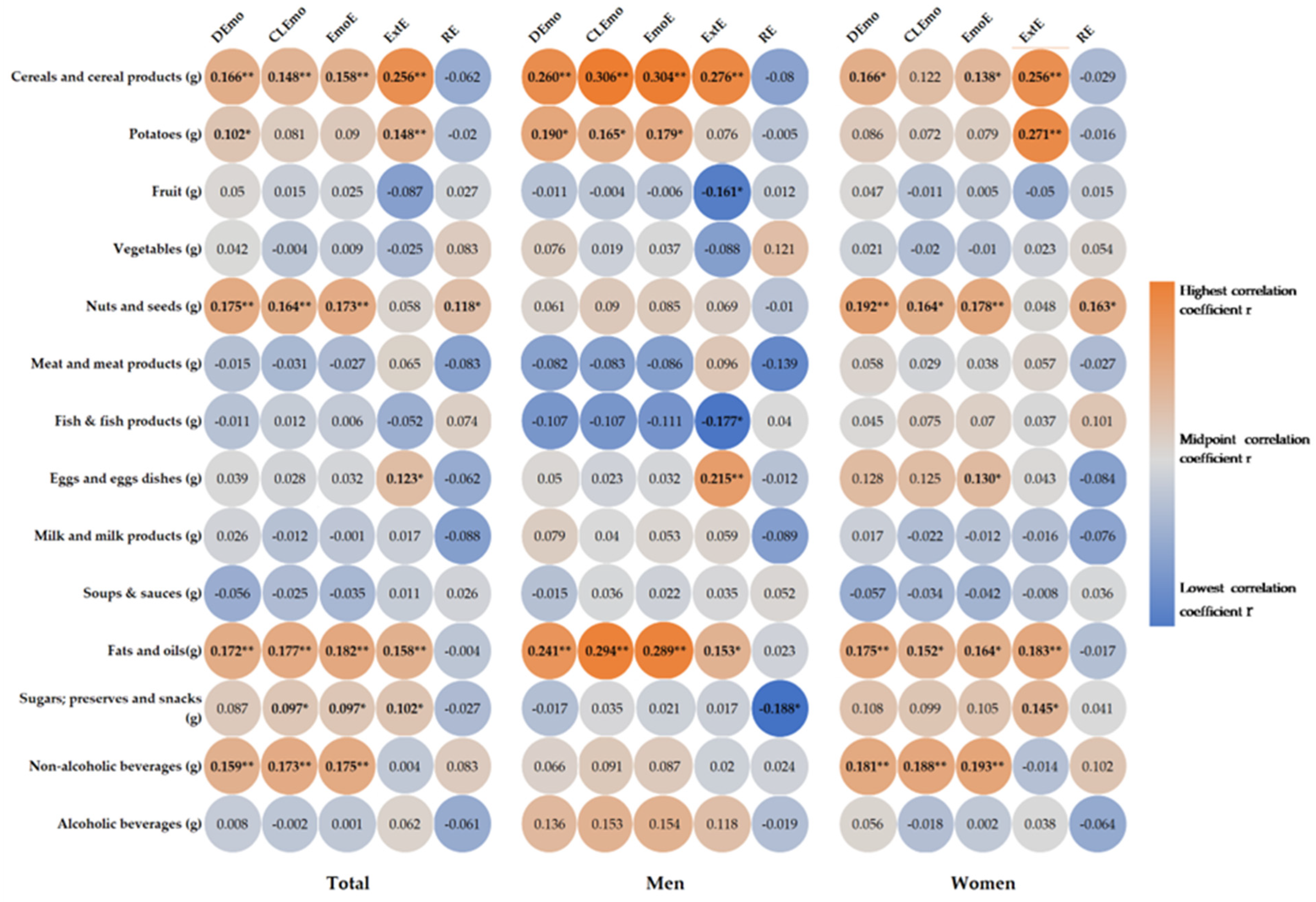
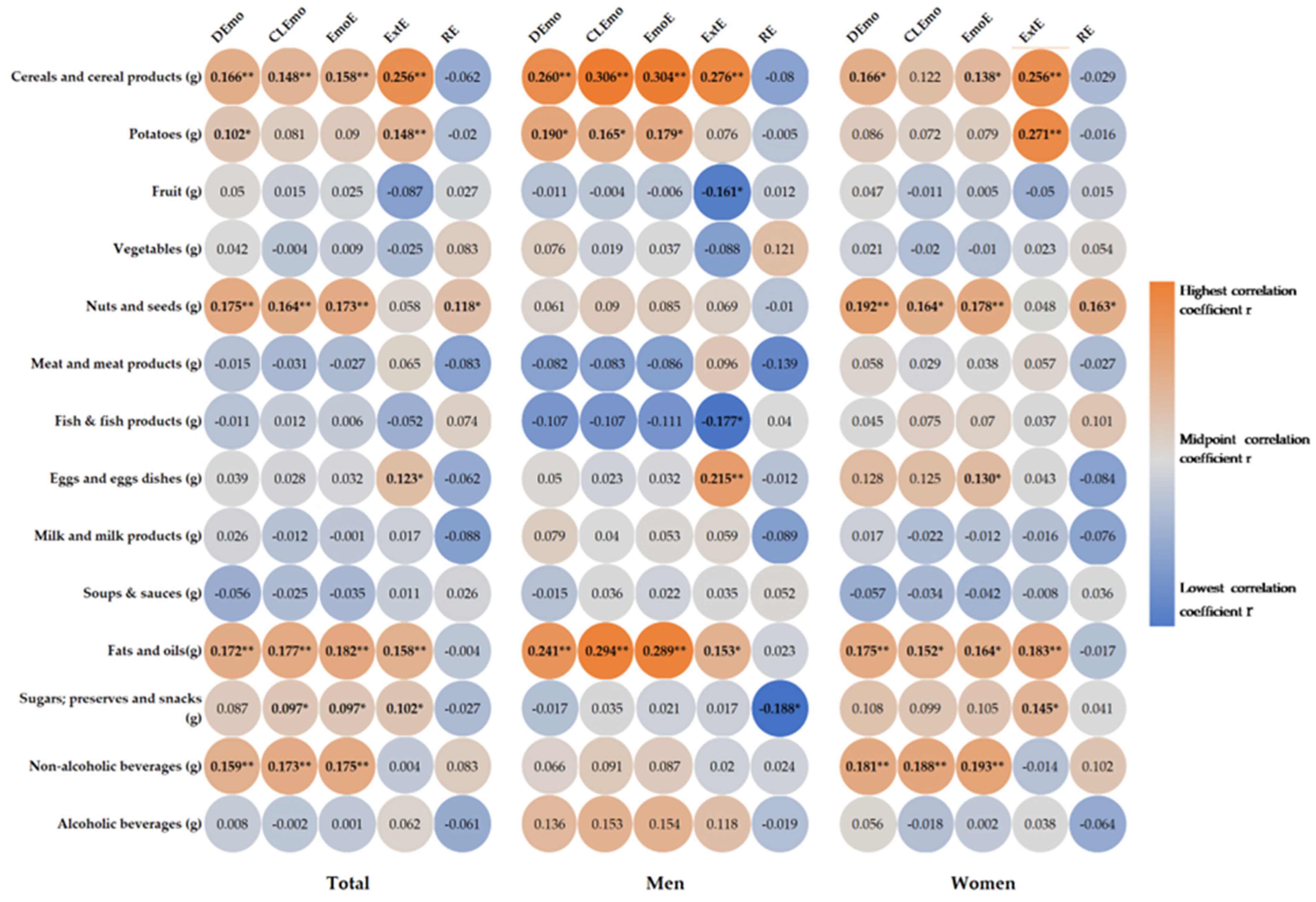
3.4. Correlations between Food Intake and Eating Behavior in the Studied Group
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ortiz-Martínez, M.; González-González, M.; Martagón, A.J.; Hlavinka, V.; Willson, R.C.; Rito-Palomares, M. Recent Developments in Biomarkers for Diagnosis and Screening of Type 2 Diabetes Mellitus. Curr. Diabetes Rep. 2022, 22, 95–115. [Google Scholar] [CrossRef]
- Yun, J.-S.; Ko, S.-H. Current Trends in Epidemiology of Cardiovascular Disease and Cardiovascular Risk Management in Type 2 Diabetes. Metabolism 2021, 123, 154838. [Google Scholar] [CrossRef]
- Hallberg, S.J.; Gershuni, V.M.; Hazbun, T.L.; Athinarayanan, S.J. Reversing Type 2 Diabetes: A Narrative Review of the Evidence. Nutrients 2019, 11, 766. [Google Scholar] [CrossRef]
- Magliano, D.; Boyko, E.J. IDF Diabetes Atlas, 10th ed.; International Diabetes Federation: Brussels, Belgium, 2021; ISBN 978-2-930229-98-0. [Google Scholar]
- Sun, H.; Saeedi, P.; Karuranga, S.; Pinkepank, M.; Ogurtsova, K.; Duncan, B.B.; Stein, C.; Basit, A.; Chan, J.C.N.; Mbanya, J.C.; et al. IDF Diabetes Atlas: Global, Regional and Country-Level Diabetes Prevalence Estimates for 2021 and Projections for 2045. Diabetes Res. Clin. Pract. 2022, 183, 109119. [Google Scholar] [CrossRef]
- American Diabetes Association. Standards of Medical Care in Diabetes—2019 Abridged for Primary Care Providers. Clin. Diabetes 2019, 37, 11–34. [Google Scholar] [CrossRef]
- Salvia, M.G.; Quatromoni, P.A. Behavioral Approaches to Nutrition and Eating Patterns for Managing Type 2 Diabetes: A Review. Am. J. Med. Open 2023, 9, 100034. [Google Scholar] [CrossRef]
- Stover, P.J.; Field, M.S.; Andermann, M.L.; Bailey, R.L.; Batterham, R.L.; Cauffman, E.; Frühbeck, G.; Iversen, P.O.; Starke-Reed, P.; Sternson, S.M.; et al. Neurobiology of Eating Behavior, Nutrition and Health. J. Intern. Med. 2023, 294, 582–604. [Google Scholar] [CrossRef]
- Yannakoulia, M. Eating Behavior among Type 2 Diabetic Patients: A Poorly Recognized Aspect in a Poorly Controlled Disease. Rev. Diabet. Stud. RDS 2006, 3, 11–16. [Google Scholar] [CrossRef]
- Dakin, C.; Beaulieu, K.; Hopkins, M.; Gibbons, C.; Finlayson, G.; Stubbs, R.J. Do Eating Behavior Traits Predict Energy Intake and Body Mass Index? A Systematic Review and Meta-Analysis. Obes. Rev. 2023, 24, e13515. [Google Scholar] [CrossRef]
- Cradock, K.A.; ÓLaighin, G.; Finucane, F.M.; McKay, R.; Quinlan, L.R.; Martin Ginis, K.A.; Gainforth, H.L. Diet Behavior Change Techniques in Type 2 Diabetes: A Systematic Review and Meta-Analysis. Diabetes Care 2017, 40, 1800–1810. [Google Scholar] [CrossRef]
- Tak, S.R.; Hendrieckx, C.; Nefs, G.; Nyklíček, I.; Speight, J.; Pouwer, F. The Association between Types of Eating Behaviour and Dispositional Mindfulness in Adults with Diabetes. Results from Diabetes MILES. The Netherlands. Appetite 2015, 87, 288–295. [Google Scholar] [CrossRef]
- Park, M.; Quinn, L.; Park, C.; Martyn-Nemeth, P. Pathways of the Relationships among Eating Behavior, Stress, and Coping in Adults with Type 2 Diabetes: A Cross-Sectional Study. Appetite 2018, 131, 84–93. [Google Scholar] [CrossRef]
- Koopman, A.D.M.; Vd Ven, M.; Beulens, J.W.; Welschen, L.M.; Elders, P.J.; Nijpels, G.; Rutters, F. The Association between Eating Traits and Weight Change after a Lifestyle Intervention in People with Type 2 Diabetes Mellitus. J. Diabetes Res. 2018, 2018, 9264204. [Google Scholar] [CrossRef]
- Betancourt-Núñez, A.; Torres-Castillo, N.; Martínez-López, E.; De Loera-Rodríguez, C.O.; Durán-Barajas, E.; Márquez-Sandoval, F.; Bernal-Orozco, M.F.; Garaulet, M.; Vizmanos, B. Emotional Eating and Dietary Patterns: Reflecting Food Choices in People with and without Abdominal Obesity. Nutrients 2022, 14, 1371. [Google Scholar] [CrossRef]
- Van Strien, T.; Van De Laar, F.A. Intake of Energy Is Best Predicted by Overeating Tendency and Consumption of Fat Is Best Predicted by Dietary Restraint: A 4-Year Follow-up of Patients with Newly Diagnosed Type 2 Diabetes. Appetite 2008, 50, 544–547. [Google Scholar] [CrossRef]
- Huisman, S.D.; Hendrieckx, C.; Bot, M.; Pouwer, F.; Nefs, G. Prevalence, Associations and Health Outcomes of Binge Eating in Adults with Type 1 or Type 2 Diabetes: Results from Diabetes MILES–The Netherlands. Diabet. Med. 2023, 40, e14953. [Google Scholar] [CrossRef]
- Forouhi, N.G.; Misra, A.; Mohan, V.; Taylor, R.; Yancy, W. Dietary and Nutritional Approaches for Prevention and Management of Type 2 Diabetes. Br. Med. J. 2018, 361. [Google Scholar] [CrossRef]
- Al-Salmi, N.; Cook, P.; D’Souza, M.S. Diet Adherence among Adults with Type 2 Diabetes Mellitus: A Concept Analysis. Oman Med. J. 2022, 37, e361. [Google Scholar] [CrossRef]
- American Diabetes Association. Prevention or Delay of Type 2 Diabetes: Standards of Medical Care in Diabetes—2021. Diabetes Care 2021, 44, S34–S39. [Google Scholar] [CrossRef]
- Ajala, O.; English, P.; Pinkney, J. Systematic Review and Meta-Analysis of Different Dietary Approaches to the Management of Type 2 Diabetes. Am. J. Clin. Nutr. 2013, 97, 505–516. [Google Scholar] [CrossRef]
- Esposito, K.; Maiorino, M.I.; Bellastella, G.; Chiodini, P.; Panagiotakos, D.; Giugliano, D. A Journey into a Mediterranean Diet and Type 2 Diabetes: A Systematic Review with Meta-Analyses. BMJ Open 2015, 5, e008222. [Google Scholar] [CrossRef]
- Schwingshackl, L.; Hoffmann, G. Mediterranean Dietary Pattern, Inflammation and Endothelial Function: A Systematic Review and Meta-Analysis of Intervention Trials. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 929–939. [Google Scholar] [CrossRef]
- Inagaki, S.; Matsuda, T.; Muramae, N.; Abe, K.; Kato, K. Diabetes-Related Shame among People with Type 2 Diabetes: An Internet-Based Cross-Sectional Study. BMJ Open Diabetes Res. Care 2022, 10, e003001. [Google Scholar] [CrossRef]
- de Queiroz, F.L.N.; Raposo, A.; Han, H.; Nader, M.; Ariza-Montes, A.; Zandonadi, R.P. Eating Competence, Food Consumption and Health Outcomes: An Overview. Int. J. Environ. Res. Public Health 2022, 19, 4484. [Google Scholar] [CrossRef]
- Przybyłowicz, K.E.; Danielewicz, A. Eating Habits and Disease Risk Factors. Nutrients 2022, 14, 3143. [Google Scholar] [CrossRef]
- World Health Organization. Physical Status: The Use and Interpretation of Anthropometry: Report of a WHO Expert Committee; WHO Expert Committee on Physical Status, Ed.; WHO Technical Report Series; World Health Organization: Geneva, Switzerland, 1995; ISBN 978-92-4-120854-3. [Google Scholar]
- Mulligan, A.A.; Luben, R.N.; Bhaniani, A.; Parry-Smith, D.J.; O’Connor, L.; Khawaja, A.P.; Forouhi, N.G.; Khaw, K.-T. A New Tool for Converting Food Frequency Questionnaire Data into Nutrient and Food Group Values: FETA Research Methods and Availability. BMJ Open 2014, 4, e004503. [Google Scholar] [CrossRef]
- Gherasim, A.; Arhire, L.I.; Niță, O.; Strateanu, R.; Oprescu, A.C.; Graur, M.; Mihalache, L. Can the Epic Food Frequency Questionnaire Be Applied to the Population in Romania. Rev. Med. Chir. Soc. Med. Nat. Iasi 2015, 119, 856–863. [Google Scholar]
- van Strien, T.; Frijters, J.E.; Bergers, G.P.; Defares, P.B. The Dutch Eating Behavior Questionnaire (DEBQ) for Assessment of Restrained, Emotional, and External Eating Behavior. Int. J. Eat. Disord. 1986, 5, 295–315. [Google Scholar] [CrossRef]
- Arhire, L.I.; Niță, O.; Popa, A.D.; Gal, A.-M.; Dumitrașcu, O.; Gherasim, A.; Mihalache, L.; Graur, M. Validation of the Dutch Eating Behavior Questionnaire in a Romanian Adult Population. Nutrients 2021, 13, 3890. [Google Scholar] [CrossRef]
- Mihalache, L.; Graur, L.I.; Popescu, D.S.; Niţă, O.; Graur, M. Anthropometric Parameters—Predictive Factors for Cardio-Metabolic Diseases. Rev. Med. Chir. Soc. Med. Nat. Iasi 2012, 116, 794–798. [Google Scholar]
- World Health Organization. Fact Sheet about Diabetes; World Health Organization: Geneva, Switzerland, 2022. [Google Scholar]
- Mihalache, L. The Prevalence of the Metabolic Syndrome and Its Components in a Rural Community. Acta Endocrinol. Buchar. 2012, 8, 595–606. [Google Scholar] [CrossRef]
- Daousi, C.; Casson, I.F.; Gill, G.V.; MacFarlane, I.A.; Wilding, J.P.H.; Pinkney, J.H. Prevalence of Obesity in Type 2 Diabetes in Secondary Care: Association with Cardiovascular Risk Factors. Postgrad. Med. J. 2006, 82, 280–284. [Google Scholar] [CrossRef]
- Nascimento, A.G.; Grassi, T.; Reischak de Oliveira, A.; Steemburgo, T. Under-reporting of the Energy Intake in Patients with Type 2 Diabetes. J. Hum. Nutr. Diet. 2021, 34, 73–80. [Google Scholar] [CrossRef]
- Thewjitcharoen, Y.; Chotwanvirat, P.; Jantawan, A.; Siwasaranond, N.; Saetung, S.; Nimitphong, H.; Himathongkam, T.; Reutrakul, S. Evaluation of Dietary Intakes and Nutritional Knowledge in Thai Patients with Type 2 Diabetes Mellitus. J. Diabetes Res. 2018, 2018, 9152910. [Google Scholar] [CrossRef]
- Katsukawa, F. Energy Requirements for Older Patients with Type 2 Diabetes: A Narrative Review of the Current Findings and Future Tasks. Nutrients 2021, 13, 753. [Google Scholar] [CrossRef]
- McKenzie, B.L.; Coyle, D.H.; Burrows, T.; Rosewarne, E.; Peters, S.A.E.; Carcel, C.; Collins, C.E.; Norton, R.; Woodward, M.; Jaacks, L.M.; et al. Gender Differences in the Accuracy of Dietary Assessment Methods to Measure Energy Intake in Adults: Protocol for a Systematic Review and Meta-Analysis. BMJ Open 2020, 10, e035611. [Google Scholar] [CrossRef]
- Goode, J.P.; Smith, K.J.; Kilpatrick, M.; Breslin, M.; Oddy, W.H.; Dwyer, T.; Venn, A.J.; Magnussen, C.G. Retrospectively Estimating Energy Intake and Misreporting from a Qualitative Food Frequency Questionnaire: An Example Using Australian Cohort and National Survey Data. Front. Nutr. 2021, 8, 624305. [Google Scholar] [CrossRef]
- Miyazawa, I.; Morino, K.; Fuse, K.; Kondo, K.; Ohi, A.; Nishida, K.; Kurihara, M.; Yasuhara, S.; Nakanishi, N.; Nishida, Y.; et al. Impact of Obesity on Underreporting of Energy Intake in Type 2 Diabetic Patients: Clinical Evaluation of Energy Requirements in Patients with Diabetes Mellitus (CLEVER-DM) Study. Clin. Nutr. ESPEN 2020, 39, 251–254. [Google Scholar] [CrossRef]
- Davies, M.J.; D’Alessio, D.A.; Fradkin, J.; Kernan, W.N.; Mathieu, C.; Mingrone, G.; Rossing, P.; Tsapas, A.; Wexler, D.J.; Buse, J.B. Management of Hyperglycemia in Type 2 Diabetes, 2018. A Consensus Report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care 2018, 41, 2669–2701. [Google Scholar] [CrossRef]
- Evert, A.B.; Dennison, M.; Gardner, C.D.; Garvey, W.T.; Lau, K.H.K.; MacLeod, J.; Mitri, J.; Pereira, R.F.; Rawlings, K.; Robinson, S.; et al. Nutrition Therapy for Adults with Diabetes or Prediabetes: A Consensus Report. Diabetes Care 2019, 42, 731–754. [Google Scholar] [CrossRef]
- American Diabetes Association. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes—2021. Diabetes Care 2021, 44, S15–S33. [Google Scholar] [CrossRef]
- Gray, A.; Threlkeld, R.J. Nutritional Recommendations for Individuals with Diabetes. In Endotext; Feingold, K.R., Anawalt, B., Blackman, M.R., Boyce, A., Chrousos, G., Corpas, E., de Herder, W.W., Dhatariya, K., Dungan, K., Hofland, J., et al., Eds.; MDText.com, Inc.: South Dartmouth, MA, USA, 2000. [Google Scholar]
- Abassi, M.M.; Sassi, S.; El Ati, J.; Ben Gharbia, H.; Delpeuch, F.; Traissac, P. Gender Inequalities in Diet Quality and Their Socioeconomic Patterning in a Nutrition Transition Context in the Middle East and North Africa: A Cross-Sectional Study in Tunisia. Nutr. J. 2019, 18, 18. [Google Scholar] [CrossRef]
- Leblanc, V.; Bégin, C.; Corneau, L.; Dodin, S.; Lemieux, S. Gender Differences in Dietary Intakes: What Is the Contribution of Motivational Variables? J. Hum. Nutr. Diet. 2015, 28, 37–46. [Google Scholar] [CrossRef]
- Nishida, C.; Uauy, R.; Kumanyika, S.; Shetty, P. The Joint WHO/FAO Expert Consultation on Diet, Nutrition and the Prevention of Chronic Diseases: Process, Product and Policy Implications. Public Health Nutr. 2004, 7, 245–250. [Google Scholar] [CrossRef]
- Vitale, M.; Masulli, M.; Cocozza, S.; Anichini, R.; Babini, A.C.; Boemi, M.; Bonora, E.; Buzzetti, R.; Carpinteri, R.; Caselli, C.; et al. Sex Differences in Food Choices, Adherence to Dietary Recommendations and Plasma Lipid Profile in Type 2 Diabetes—The TOSCA.IT Study. Nutr. Metab. Cardiovasc. Dis. 2016, 26, 879–885. [Google Scholar] [CrossRef]
- Herman, C.P.; Polivy, J. External Cues in the Control of Food Intake in Humans: The Sensory-Normative Distinction. Physiol. Behav. 2008, 94, 722–728. [Google Scholar] [CrossRef]
- Andrés, A.; Oda-Montecinos, C.; Saldaña, C. Eating Behaviors in a Male and Female Community Sample: Psychometric Properties of the DEBQ. Ter. Psicológica 2017, 35, 141–152. [Google Scholar] [CrossRef]
- Daly, A.; O’Sullivan, E.; McNulty, B.; Walton, J.; Kearney, J. Age, Sex & BMI Are Associated with Different Eating Behaviour Styles in Irish Teens. Proc. Nutr. Soc. 2020, 79, E351. [Google Scholar] [CrossRef]
- Mason, T.B.; Lewis, R.J. Profiles of Binge Eating: The Interaction of Depressive Symptoms, Eating Styles, and Body Mass Index. Eat. Disord. 2014, 22, 450–460. [Google Scholar] [CrossRef] [PubMed]
- Guerrero-Hreins, E.; Stammers, L.; Wong, L.; Brown, R.M.; Sumithran, P. A Comparison of Emotional Triggers for Eating in Men and Women with Obesity. Nutrients 2022, 14, 4144. [Google Scholar] [CrossRef]
- Gorrell, S.; Trainor, C.; Le Grange, D. The Impact of Urbanization on Risk for Eating Disorders. Curr. Opin. Psychiatry 2019, 32, 242–247. [Google Scholar] [CrossRef] [PubMed]
- Aguiar-Bloemer, A.C.; Diez-Garcia, R.W. Influence of Emotions Evoked by Life Events on Food Choice. Eat. Weight Disord. Stud. Anorex. Bulim. Obes. 2018, 23, 45–53. [Google Scholar] [CrossRef]
- Torres, S.J.; Nowson, C.A. Relationship between Stress, Eating Behavior, and Obesity. Nutrition 2007, 23, 887–894. [Google Scholar] [CrossRef] [PubMed]
- Standen, E.C.; Finch, L.E.; Tiongco-Hofschneider, L.; Schopp, E.; Lee, K.M.; Parker, J.E.; Bamishigbin, O.N.; Tomiyama, A.J. Healthy versus Unhealthy Comfort Eating for Psychophysiological Stress Recovery in Low-Income Black and Latinx Adults. Appetite 2022, 176, 106140. [Google Scholar] [CrossRef]
- Laitinen, J.; Ek, E.; Sovio, U. Stress-Related Eating and Drinking Behavior and Body Mass Index and Predictors of This Behavior. Prev. Med. 2002, 34, 29–39. [Google Scholar] [CrossRef]
- Piano, M.R. Alcohol’s Effects on the Cardiovascular System. Alcohol Res. Curr. Rev. 2017, 38, 219–241. [Google Scholar]
- Anschutz, D.J.; Van Strien, T.; Van De Ven, M.O.M.; Engels, R.C.M.E. Eating Styles and Energy Intake in Young Women. Appetite 2009, 53, 119–122. [Google Scholar] [CrossRef]
- Paans, N.P.G.; Gibson-Smith, D.; Bot, M.; van Strien, T.; Brouwer, I.A.; Visser, M.; Penninx, B.W.J.H. Depression and Eating Styles Are Independently Associated with Dietary Intake. Appetite 2019, 134, 103–110. [Google Scholar] [CrossRef]
- Shukri, M.; Jones, F.; Conner, M. Relationship between Work-Family Conflict and Unhealthy Eating: Does Eating Style Matter? Appetite 2018, 123, 225–232. [Google Scholar] [CrossRef]
- Burton, P.; Smit, H.J.; Lightowler, H.J. The Influence of Restrained and External Eating Patterns on Overeating. Appetite 2007, 49, 191–197. [Google Scholar] [CrossRef]
- Małachowska, A.; Jeżewska-Zychowicz, M.; Gębski, J. Polish Adaptation of the Dutch Eating Behaviour Questionnaire (DEBQ): The Role of Eating Style in Explaining Food Intake—A Cross-Sectional Study. Nutrients 2021, 13, 4486. [Google Scholar] [CrossRef]
- Narain, A.; Kwok, C.S.; Mamas, M.A. Soft Drinks and Sweetened Beverages and the Risk of Cardiovascular Disease and Mortality: A Systematic Review and Meta-Analysis. Int. J. Clin. Pract. 2016, 70, 791–805. [Google Scholar] [CrossRef]
- Gherasim, A.; Arhire, L.I.; Nita, O.; Oprescu, A.C.; Gavril, R.S.; Mitu, O.; Graur, M.; Mihalache, L. Dietary Patterns in Romanian Patients with Type 2 Diabetes Mellitus. Med.-Surg. J. 2022, 126, 181–194. [Google Scholar] [CrossRef]
- Liem, D.G.; Russell, C.G. The Influence of Taste Liking on the Consumption of Nutrient Rich and Nutrient Poor Foods. Front. Nutr. 2019, 6, 174. [Google Scholar] [CrossRef] [PubMed]
- Kabir, A.; Miah, S.; Islam, A. Factors Influencing Eating Behavior and Dietary Intake among Resident Students in a Public University in Bangladesh: A Qualitative Study. PLoS ONE 2018, 13, e0198801. [Google Scholar] [CrossRef]
- Lowe, M.R.; Doshi, S.D.; Katterman, S.N.; Feig, E.H. Dieting and Restrained Eating as Prospective Predictors of Weight Gain. Front. Psychol. 2013, 4, 577. [Google Scholar] [CrossRef]
- Arhire, L.I. Orthorexia Nervosa: The Unhealthy Obsession for Healthy Food. Med.-Surg. J. 2015, 119, 632–638. [Google Scholar]
- Quattlebaum, M.; Wilson, D.K.; Sweeney, A.M.; Zarrett, N. Moderating Effects of Parental Feeding Practices and Emotional Eating on Dietary Intake among Overweight African American Adolescents. Nutrients 2021, 13, 1920. [Google Scholar] [CrossRef]
- Bell, B.M.; Spruijt-Metz, D.; Naya, C.H.; Lane, C.J.; Wen, C.K.F.; Davis, J.N.; Weigensberg, M.J. The Mediating Role of Emotional Eating in the Relationship between Perceived Stress and Dietary Intake Quality in Hispanic/Latino Adolescents. Eat. Behav. 2021, 42, 101537. [Google Scholar] [CrossRef]
- Plaza-Diaz, J.; Flores-Rojas, K.; de la Torre-Aguilar, M.J.; Gomez-Fernández, A.R.; Martín-Borreguero, P.; Perez-Navero, J.L.; Gil, A.; Gil-Campos, M. Dietary Patterns, Eating Behavior, and Nutrient Intakes of Spanish Preschool Children with Autism Spectrum Disorders. Nutrients 2021, 13, 3551. [Google Scholar] [CrossRef]
- Schneider-Worthington, C.R.; Smith, K.E.; Roemmich, J.N.; Salvy, S.-J. External Food Cue Responsiveness and Emotional Eating in Adolescents: A Multimethod Study. Appetite 2022, 168, 105789. [Google Scholar] [CrossRef]
- Dubois, L.; Bédard, B.; Goulet, D.; Prud’homme, D.; Tremblay, R.E.; Boivin, M. Eating Behaviors, Dietary Patterns and Weight Status in Emerging Adulthood and Longitudinal Associations with Eating Behaviors in Early Childhood. Int. J. Behav. Nutr. Phys. Act. 2022, 19, 139. [Google Scholar] [CrossRef]
- Maneschy, I.; Moreno, L.A.; Ruperez, A.I.; Jimeno, A.; Miguel-Berges, M.L.; Widhalm, K.; Kafatos, A.; Molina-Hidalgo, C.; Molnar, D.; Gottrand, F.; et al. Eating Behavior Associated with Food Intake in European Adolescents Participating in the HELENA Study. Nutrients 2022, 14, 3033. [Google Scholar] [CrossRef]
- Al-Najim, W.; Docherty, N.G.; le Roux, C.W. Food Intake and Eating Behavior After Bariatric Surgery. Physiol. Rev. 2018, 98, 1113–1141. [Google Scholar] [CrossRef]
- Sarwer, D.B.; Dilks, R.J.; West-Smith, L. Dietary Intake and Eating Behavior after Bariatric Surgery: Threats to Weight Loss Maintenance and Strategies for Success. Surg. Obes. Relat. Dis. 2011, 7, 644–651. [Google Scholar] [CrossRef]
- Morita, A.; Aiba, N.; Miyachi, M.; Watanabe, S.; Saku Cohort Study Group. The Associations of Eating Behavior and Dietary Intake with Metabolic Syndrome in Japanese: Saku Cohort Baseline Study. J. Physiol. Anthropol. 2020, 39, 40. [Google Scholar] [CrossRef]
- Van De Laar, F.A.; Van De Lisdonk, E.H.; Lucassen, P.L.B.J.; Stafleu, A.; Mulder, J.; Van Den Hoogen, H.J.M.; Rutten, G.E.H.M.; Van Weel, C. Eating Behaviour and Adherence to Diet in Patients with Type 2 Diabetes Mellitus. Diabet. Med. 2006, 23, 788–794. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Total (n = 416) | Women (n = 236) | Men (n = 180) | |
|---|---|---|---|
| Age (years) | 62.64 ± 9.91 | 63.30 ± 9.31 | 62.11 ± 9.81 |
| Weight (kg) | 87.18 ± 17.59 | 81.12 ± 14.98 a | 95.08 ± 17.64 b |
| BMI (kg/m2) | 31.85 ± 5.33 | 31.98 ± 5.39 | 31.65 ± 5.25 |
| Place of living | |||
| Urban (%) | 59.6 (n = 248) | 58.1 (n = 137) | 61.7 (n = 111) |
| Rural (%) | 40.4 (n = 168) | 41.9 (n = 99) | 38.3 (n = 69) |
| Smoking status | |||
| Non-smoking (%) | 89.9 (n = 374) | 95.3 (n = 225) | 82.8 (n = 149) |
| Undeclared (%) | 1.7 (n = 7) | 1.7 (n = 4) | 1.7 (n = 3) |
| BMI-status | |||
| Normal weight (%) | 7.5 (n = 31) | 7.2 (n = 17) | 7.8 (n = 14) |
| Overfweight (%) | 33.3 (n = 138) | 33.1 (n = 78) | 33.9 (n = 61) |
| Obesity (%) | 59.3 (n = 246) | 59.7 (n = 141) | 58.3 (n = 105) |
| Daily Intake (Mean ± SD) | Total (n = 416) | Women (n = 236) | Men (n = 180) |
|---|---|---|---|
| Energy (kcal) | 1584.78 ± 605.57 | 1509.01 ± 645.15 a | 1684.13 ± 535.05 b |
| Carbohydrate (g) | 195.08 ± 71.87 | 189.18 ± 75.43 | 202.80 ± 66.33 |
| Carbohydrate (%) | 50.05 ± 8.33 | 51.09 ± 8.23 a | 48.70 ± 8.28 b |
| Fiber (g) | 18.67 ± 6.1 | 18.52 ± 6.17 | 18.88 ± 6.01 |
| Total lipids (g) | 56.95 ± 31.36 | 54.25 ± 34.17 a | 60.50 ± 26.93 b |
| Total lipids (%) | 31.74 ± 6.81 | 31.23 ± 7.20 | 31.61 ± 6.06 |
| MUFA (g) | 20.38 ± 12.78 | 19.51 ± 14.21 | 21.53 ± 10.54 |
| PUFA (g) | 12.27 ± 6.81 | 11.81 ± 7.65 | 12.88 ± 5.48 |
| SFA (g) | 18.87 ± 10.82 | 17.79 ± 11.10 a | 20.28 ± 10.29 b |
| Cholesterol (g) | 322.47 ± 149.57 | 295.80 ± 140.30 a | 357.43 ± 154.45 b |
| Proteins (g) | 81.13 ± 28.44 | 76.73 ± 30.35 a | 86.90 ± 24.62 b |
| Proteins (%) | 20.77 ± 3.55 | 20.59 ± 3.54 | 21.03 ± 3.56 |
| Cereals and cereal products | 210.34 ± 111.04 | 198.50 ± 115.83 a | 225.86 ± 102.69 b |
| Potatoes | 63.18 ± 53.65 | 58.58 ± 38.26 a | 69.22 ± 68.46 b |
| Fruit | 336.51 ± 214.27 | 358.52 ± 224.76 a | 307.65 ± 196.60 b |
| Vegetables | 314.57 ± 135.92 | 316.08 ± 132.80 | 312.60 ± 140.25 |
| Nuts and seeds | 4.17 ± 9.10 | 5.04 ± 10.42 a | 3.03 ± 6.86 b |
| Meat and meat products | 123.42 ± 79.19 | 113.74 ± 84.00 a | 136.11 ± 70.62 b |
| Fish & fish products | 38.03 ± 35.87 | 37.48 ± 36.30 a | 38.74 ± 35.38 b |
| Eggs and eggs dishes | 21.16 ± 15.70 | 18.51 ± 11.02 a | 24.63 ± 19.77 b |
| Milk and milk products | 221.30 ± 180.55 | 210.69 ± 161.44 | 235.20 ± 202.53 |
| Soups & sauces | 224.16 ± 142.23 | 207.46 ± 91.05 a | 246.06 ± 187.53 b |
| Fats and oils | 7.76 ± 10.36 | 7.14 ± 7.92 | 8.58 ± 12.85 |
| Sugars; preserves and snacks | 16.98 ± 22.99 | 18.74 ± 25.53 | 14.69 ± 18.97 |
| Non-alcoholic beverages | 339.75 ± 237.76 | 362.71 ± 243.22 a | 309.65 ± 227.59 b |
| Alcoholic beverages | 32.08 ± 77.35 | 9.31 ± 25.22 a | 61.92 ± 107.04 b |
| Score for DEmo | Score for CLEmo | Score for EmoE | Score for ExtE | Score for RE | |
|---|---|---|---|---|---|
| Women | 1.97 ± 1.07 ** | 1.93 ± 1.28 ** | 1.94 ± 1.17 ** | 2.44 ± 1.02 | 2.31 ± 0.97 ** |
| Men | 1.58 ± 0.77 ** | 1.49 ± 0.83 ** | 1.52 ± 0.78 ** | 2.36 ± 0.97 | 2.09 ± 0.90 ** |
| BMI-status | |||||
| Normal weight | 1.71 ± 0.94 | 1.42 ± 0.70 | 1.51 ± 0.71 | 2.40 ± 1.13 | 1.68 ± 0.62 ** |
| Overweight | 1.81 ± 0.96 | 1.75 ± 1.13 | 1.76 ± 1.04 | 2.43 ± 1.00 | 2.10 ± 0.85 ** |
| Obesity | 1.81 ± 0.98 | 1.78 ± 1.17 | 1.79 ± 1.08 | 2.39 ± 0.99 | 2.34 ± 1.00 ** |
| Place of living | |||||
| Urban | 1.90 ± 0.97 * | 1.85 ± 1.12 * | 1.87 ± 1.04 * | 2.43 ± 0.98 | 2.29 ± 0.92 * |
| Rural | 1.66 ± 0.95 * | 1.57 ± 1.11 * | 1.60 ± 1.03 * | 2.36 ± 1.02 | 2.10 ± 0.97 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gal, A.M.; Iatcu, C.O.; Popa, A.D.; Arhire, L.I.; Mihalache, L.; Gherasim, A.; Nita, O.; Soimaru, R.M.; Gheorghita, R.; Graur, M.; et al. Understanding the Interplay of Dietary Intake and Eating Behavior in Type 2 Diabetes. Nutrients 2024, 16, 771. https://doi.org/10.3390/nu16060771
Gal AM, Iatcu CO, Popa AD, Arhire LI, Mihalache L, Gherasim A, Nita O, Soimaru RM, Gheorghita R, Graur M, et al. Understanding the Interplay of Dietary Intake and Eating Behavior in Type 2 Diabetes. Nutrients. 2024; 16(6):771. https://doi.org/10.3390/nu16060771
Chicago/Turabian StyleGal, Ana Maria, Camelia Oana Iatcu, Alina Delia Popa, Lidia Iuliana Arhire, Laura Mihalache, Andreea Gherasim, Otilia Nita, Raluca Meda Soimaru, Roxana Gheorghita, Mariana Graur, and et al. 2024. "Understanding the Interplay of Dietary Intake and Eating Behavior in Type 2 Diabetes" Nutrients 16, no. 6: 771. https://doi.org/10.3390/nu16060771
APA StyleGal, A. M., Iatcu, C. O., Popa, A. D., Arhire, L. I., Mihalache, L., Gherasim, A., Nita, O., Soimaru, R. M., Gheorghita, R., Graur, M., & Covasa, M. (2024). Understanding the Interplay of Dietary Intake and Eating Behavior in Type 2 Diabetes. Nutrients, 16(6), 771. https://doi.org/10.3390/nu16060771