
Combined Effect of Early Nutrition Therapy and Rehabilitation for Patients with Chronic Obstructive Pulmonary Disease Exacerbation: A Prospective Randomized Controlled Trial
 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Statement of Ethics
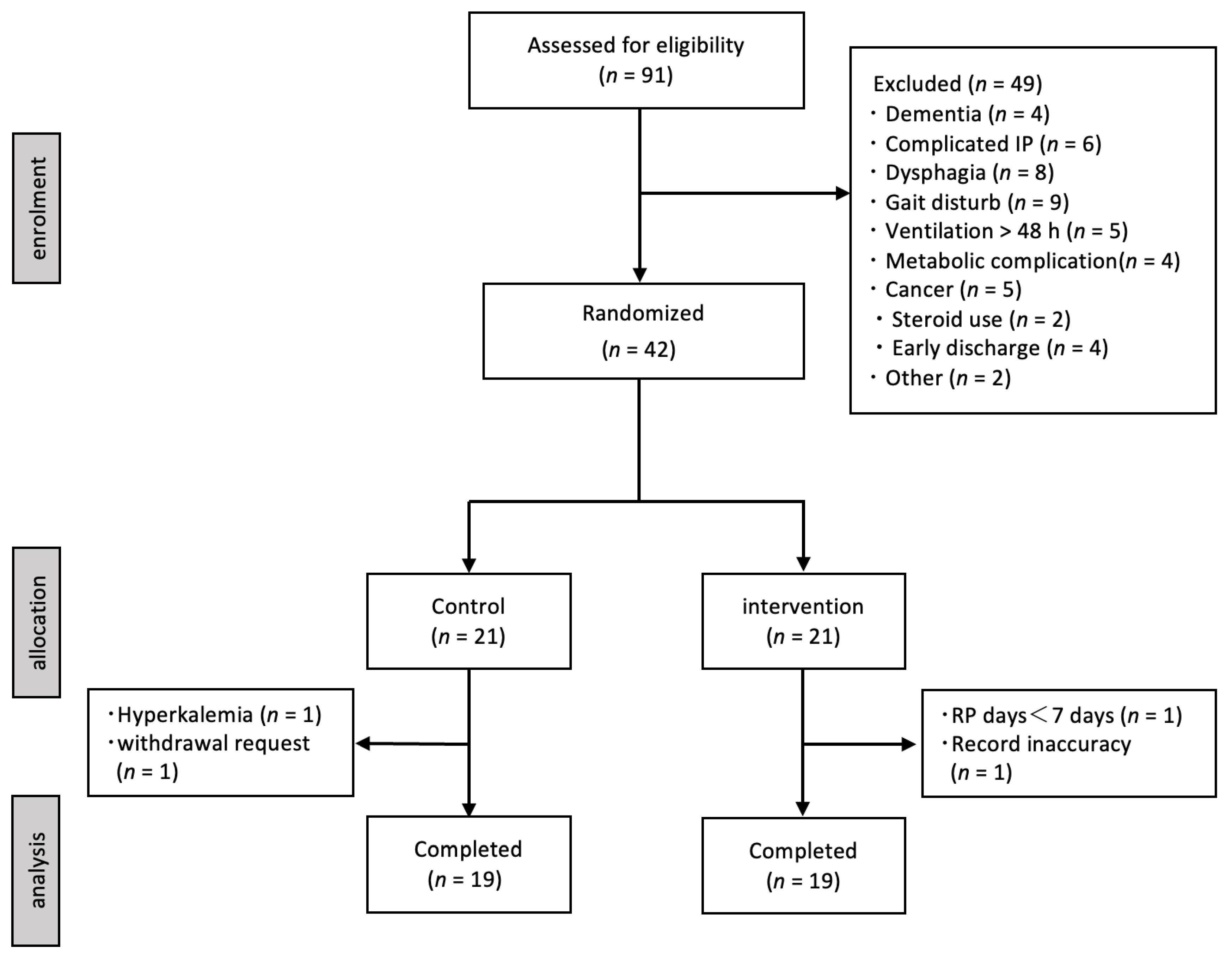
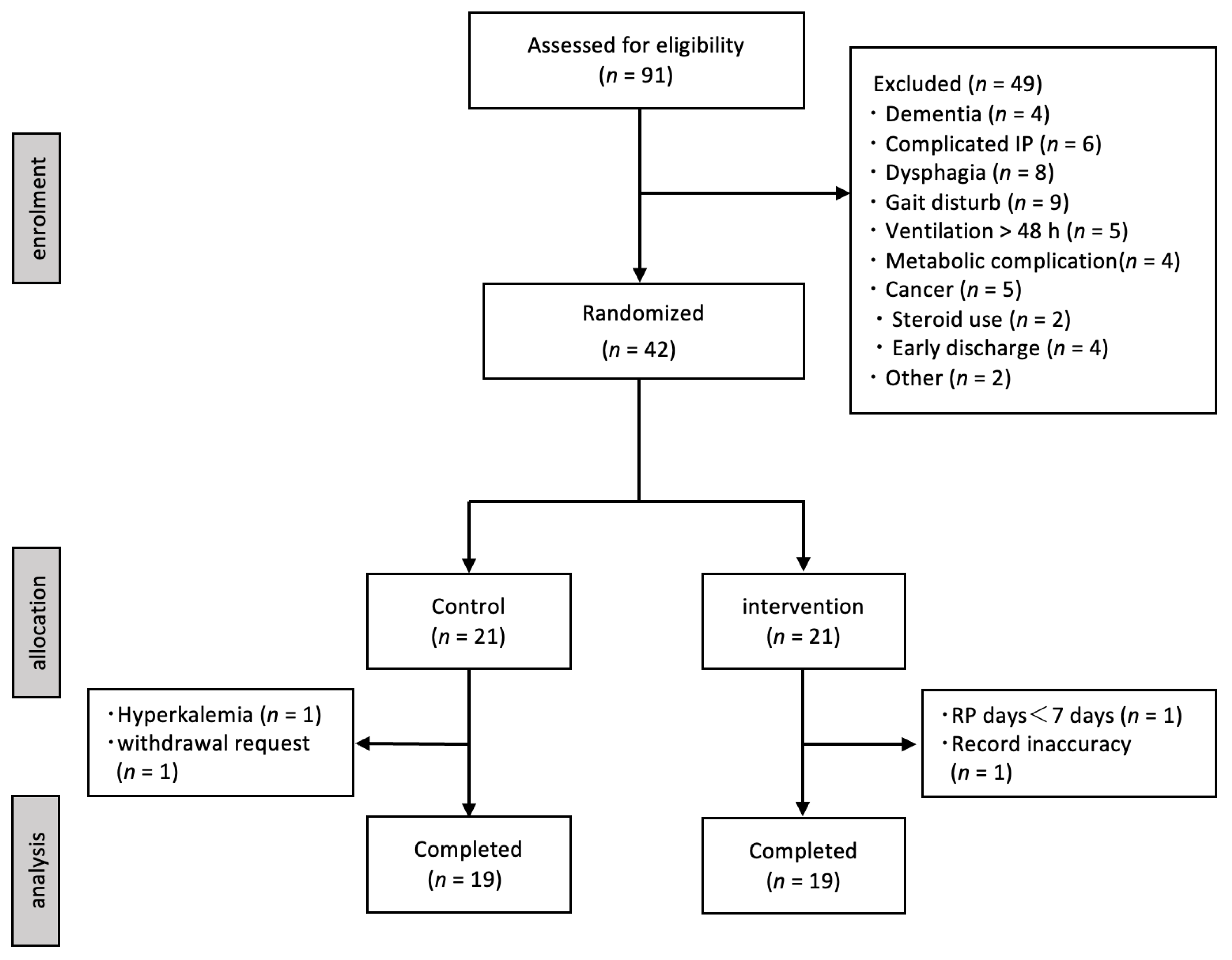
2.2. Study Participants
2.3. Study Design
2.4. Nutrition Therapy
2.5. Rehabilitation Programs
2.6. Primary and Secondary Outcomes
2.7. Data Collection
2.7.1. Basic Characteristics
2.7.2. Physical Function
2.7.3. Nutrition Status
2.8. Measurement
2.8.1. Measurement of Physical Function
2.8.2. Measurement of Nutritional Status
2.9. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Comparison between the Two Groups
3.3. Comparison within Each Group
3.4. Univariate and Multivariate Logistic Regression Analyses
3.5. Adverse Event
4. Discussion
4.1. Nutrition Status
4.2. Physical Function
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Celli, B.; Fabbri, L.; Criner, G.; Martinez, F.J.; Mannino, D.; Vogelmeier, C.; de Oca, M.M.; Papi, A.; Sin, D.D.; Han, M.K.; et al. Definition and nomenclature of chronic obstructive pulmonary disease: Time for its revision. Am. J. Respir. Crit. Care Med. 2022, 206, 1317–1325. [Google Scholar] [CrossRef]
- World Health Organization. The Top 10 Causes of Death. 2020. Available online: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death (accessed on 6 April 2021).
- Lacasse, Y.; Brosseau, L.; Milne, S.; Wong, E.; Guyatt, G.H.; Goldstein, R.S. Pulmonary rehabilitation for chronic obstructive pulmonary disease. Cochrane Database Syst. Rev. 2002, 2, CD003793. [Google Scholar] [CrossRef]
- Ries, A.L.; Bauldoff, G.S.; Carlin, B.W.; Casaburi, R.; Emery, C.F.; Mahler, D.A.; Make, B.; Rochester, C.L.; Zuwallack, R.; Herrerias, C. Pulmonary rehabilitation: Joint ACCP/AACVPR Evidence-Based Clinical Practice Guidelines. Chest 2007, 131, 4S–42S. [Google Scholar] [CrossRef]
- Casaburi, R.; Patessio, A.; Ioli, F.; Zanaboni, S.; Donner, C.F.; Wasserman, K. Reductions in exercise lactic acidosis and ventilation as a result of exercise training in patients with obstructive lung disease. Am. Rev. Respir. Dis. 1991, 143, 9–18. [Google Scholar] [CrossRef]
- Foglio, K.; Bianchi, L.; Bruletti, G.; Porta, R.; Vitacca, M.; Balbi, B.; Ambrosino, N. Seven-year time course of lung function, symptoms, health-related quality of life, and exercise tolerance in COPD patients undergoing pulmonary rehabilitation programs. Respir. Med. 2007, 101, 1961–1970. [Google Scholar] [CrossRef] [PubMed]
- Kurosaki, H.; Ishii, T.; Motohashi, N.; Motegi, T.; Yamada, K.; Kudoh, S.; Jones, R.C.M.; Kida, K. Extent of emphysema on HRCT affects loss of fat-free mass and fat mass in COPD. Intern. Med. 2009, 48, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, E.; Nakano, Y.; Ohara, T.; Muro, S.; Hirai, T.; Sato, S.; Sakai, H.; Tsukino, M.; Kinose, D.; Nishioka, M.; et al. Body mass index in male patients with COPD: Correlation with low attenuation areas on CT. Thorax 2009, 64, 20–25. [Google Scholar] [CrossRef]
- Sahebjami, H.; Doers, J.T.; Render, M.L.; Bond, T.L. Anthropometric and pulmonary function test profiles of outpatients with stable chronic obstructive pulmonary disease. Am. J. Med. 1993, 94, 469–474. [Google Scholar] [CrossRef] [PubMed]
- Yoshikawa, M.; Fujita, Y.; Yamamoto, Y.; Yamauchi, M.; Tomoda, K.; Koyama, N.; Kimura, H. Mini Nutritional Assessment Short-Form predicts exacerbation frequency in patients with chronic obstructive pulmonary disease. Respirology 2014, 19, 1198–1203. [Google Scholar] [CrossRef] [PubMed]
- Yuceege, M.; Salman, S.O.; Duru, S.; Saygıdeğer, Y.M.D.; Sonmez, Z.M.D.; Ardıç, S. The evaluation of nutrition in male COPD patients using subjective global assessment and mini nutritional assessment. Int. J. Intern. Med. 2013, 2, 1–5. [Google Scholar] [CrossRef]
- Rutten, E.P.A.; Calverley, P.M.A.; Casaburi, R.; Agusti, A.; Bakke, P.; Celli, B.; Coxson, H.O.; Crim, C.; Lomas, D.A.; Macnee, W.; et al. Changes in body composition in patients with chronic obstructive pulmonary disease: Do they influence patient-related outcomes? Ann. Nutr. Metab. 2013, 63, 239–247. [Google Scholar] [CrossRef]
- Schols, A.M.W.J.; Broekhuizen, R.; Weling-Scheepers, C.A.; Wouters, E.F. Body composition and mortality in chronic obstructive pulmonary disease. Am. J. Clin. Nutr. 2005, 82, 53–59. [Google Scholar] [CrossRef] [PubMed]
- Troosters, T.; Probst, V.S.; Crul, T.; Pitta, F.; Gayan-Ramirez, G.; Decramer, M.; Gosselink, R. Resistance training prevents deterioration in quadriceps muscle function during acute exacerbations of chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2010, 181, 1072–1077. [Google Scholar] [CrossRef] [PubMed]
- Borges, R.C.; Carvalho, C.R. Impact of resistance training in chronic obstructive pulmonary disease patients during periods of acute exacerbation. Arch. Phys. Med. Rehabil. 2014, 95, 1638–1645. [Google Scholar] [CrossRef]
- Torres-Sánchez, I.; Valenza, M.C.; Cabrera-Martos, I.; López-Torres, I.; Benítez-Feliponi, Á.; Conde-Valero, A. Effects of an Exercise Intervention in Frail Older Patients with Chronic Obstructive Pulmonary Disease Hospitalized due to an Exacerbation: A Randomized Controlled Trial. COPD 2017, 14, 37–42. [Google Scholar] [CrossRef] [PubMed]
- Matsui, H.; Jo, T.; Fushimi, K.; Yasunaga, H. Outcomes after early and delayed rehabilitation for exacerbation of chronic obstructive pulmonary disease: A nationwide retrospective cohort study in Japan. Respir. Res. 2017, 18, 68. [Google Scholar] [CrossRef]
- Oliveira, A.; Rebelo, P.; Paixão, C.; Jácome, C.; Cruz, J.; Martins, V.; Simão, P.; Brooks, D.; Marques, A. Minimal Clinically Important Difference for quadriceps muscle Strength in People with COPD following Pulmonary Rehabilitation. COPD 2021, 18, 35–44. [Google Scholar] [CrossRef]
- Zhang, D.; Zhang, H.; Li, X.; Lei, S.; Wang, L.; Guo, W.; Li, J. Pulmonary rehabilitation programmes within three days of hospitalization for acute exacerbation of chronic obstructive pulmonary disease: A systematic review and meta-analysis. Int. J. Chronic Obstr. Pulm. Dis. 2021, 16, 3525–3538. [Google Scholar] [CrossRef]
- Landbo, C.; Prescott, E.; Lange, P.; Almdal, T.P. Prognostic value of nutritional status in chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 1999, 160, 1856–1861. [Google Scholar] [CrossRef]
- Slinde, F.; Grönberg, A.M.; Engström, C.P.; Rossander-Hulthén, L.; Larsson, S. Body composition by bioelectrical impedance predicts mortality in chronic obstructive pulmonary disease patients. Respir. Med. 2005, 99, 1004–1009. [Google Scholar] [CrossRef]
- Alqahtani, J.S.; Oyelade, T.; Aldhahir, A.M.; Mendes, R.G.; Alghamdi, S.M.; Miravitlles, M.; Mandal, S.; Hurst, J.R. Reduction in hospitalised COPD exacerbations during COVID-19: A systematic review and meta-analysis. PLoS ONE 2021, 16, e0255659. [Google Scholar] [CrossRef]
- Joppa, P.; Tkacova, R.; Franssen, F.M.E.; Hanson, C.; Rennard, S.I.; Silverman, E.K.; McDonald, M.L.N.; Calverley, P.M.A.; Tal-Singer, R.; Spruit, M.A.; et al. Sarcopenic Obesity, Functional Outcomes, and Systemic Inflammation in Patients with Chronic Obstructive Pulmonary Disease. J. Am. Med. Dir. Assoc. 2016, 17, 712–718. [Google Scholar] [CrossRef]
- Kawayama, T.; Takahashi, K.; Ikeda, T.; Fukui, K.; Makita, N.; Tashiro, N.; Saito, J.; Shirai, T.; Inoue, H. Exacerbation rates in Japanese patients with obstructive lung disease: A subanalysis of the prospective, observational NOVELTY study. Allergol. Int. 2024, 73, 71–80. [Google Scholar] [CrossRef]
- Vermeeren, M.A.P.; Wouters, E.F.M.; Geraerts-Keeris, A.J.W.; Schols, A.M.W.J. Nutritional support in patients with chronic obstructive pulmonary disease during hospitalization for an acute exacerbation; a randomized controlled feasibility trial. Clin. Nutr. 2004, 23, 1184–1192. [Google Scholar] [CrossRef]
- Bernardes, S.; Eckert, I.D.C.; Burgel, C.F.; Teixeira, P.J.Z.; Silva, F.M. Increased energy and/or protein intake improves anthropometry and muscle strength in chronic obstructive pulmonary disease patients: A systematic review with meta-analysis on randomised controlled clinical trials. Br. J. Nutr. 2022, 129, 1332–1349. [Google Scholar] [CrossRef] [PubMed]
- Ogasawara, T.; Marui, S.; Miura, E.; Sugiura, M.; Matsuyama, W.; Aoshima, Y.; Kasamatsu, N.; Ogiku, M.; Ikematsu, Y. Effect of eicosapentaenoic acid on prevention of lean body mass depletion in patients with exacerbation of chronic obstructive pulmonary disease: A prospective randomized controlled trial. Clin. Nutr. ESPEN 2018, 28, 67–73. [Google Scholar] [CrossRef] [PubMed]
- Vermeeren, M.A.P.; Schols, A.M.W.J.; Wouters, E.F.M. Effects of an acute exacerbation on nutritional and metabolic profile of patients with COPD. Eur. Respir. J. 1997, 10, 2264–2269. [Google Scholar] [CrossRef]
- van de Bool, C.; Rutten, E.P.A.; van Helvoort, A.; Franssen, F.M.E.; Wouters, E.F.M.; Schols, A.M.W.J. A randomized clinical trial investigating the efficacy of targeted nutrition as adjunct to exercise training in COPD. J. Cachexia Sarcopenia Muscle 2017, 8, 748–758. [Google Scholar] [CrossRef] [PubMed]
- Shirai, Y.; Momosaki, R.; Kokura, Y.; Kato, Y.; Okugawa, Y.; Shimizu, A. Validation of Asian body mass index cutoff values for the classification of malnutrition severity according to the global leadership initiative on malnutrition criteria in patients with chronic obstructive pulmonary disease exacerbations. Nutrients 2022, 14, 4746. [Google Scholar] [CrossRef]
- He, M.; Yu, S.; Wang, L.; Lv, H.; Qiu, Z. Efficiency and safety of pulmonary rehabilitation in acute exacerbation of chronic obstructive pulmonary disease. Med. Sci. Monit. 2015, 21, 806–812. [Google Scholar] [CrossRef]
- Torres-Sánchez, I.; Cruz-Ramírez, R.; Cabrera-Martos, I.; Díaz-Pelegrina, A.; Valenza, M.C. Results of physiotherapy treatments in exacerbations of chronic obstructive pulmonary disease: A systematic review. Physiother. Can. 2017, 69, 122–132. [Google Scholar] [CrossRef] [PubMed]
- Mohan, D.; Benson, V.S.; Allinder, M.; Galwey, N.; Bolton, C.E.; Cockcroft, J.R.; MacNee, W.; Wilkinson, I.B.; Tal-Singer, R.; Polkey, M.I.; et al. Short physical performance battery: What does each sub-test measure in patients with chronic obstructive pulmonary disease? Chronic Obstr. Pulm. Dis. 2020, 7, 13–25. [Google Scholar] [CrossRef] [PubMed]
- Bernabeu-Mora, R.; Giménez-Giménez, L.M.; Montilla-Herrador, J.; García-Guillamón, G.; García-Vidal, J.A.; Medina-Mirapeix, F. Determinants of each domain of the Short Physical Performance Battery in COPD. Int. J. Chronic Obstr. Pulm. Dis. 2017, 12, 2539–2544. [Google Scholar] [CrossRef] [PubMed]
- Bernabeu-Mora, R.; Medina-Mirapeix, F.; Llamazares-Herrán, E.; García-Guillamón, G.; Giménez-Giménez, L.M.; Sánchez-Nieto, J.M. The short physical performance battery is a discriminative tool for identifying patients with COPD at risk of disability. Int. J. Chronic Obstr. Pulm. Dis. 2015, 10, 2619–2626. [Google Scholar] [CrossRef]
- Walsh, J.A.; Barker, R.E.; Kon, S.S.C.; Jones, S.E.; Banya, W.; Nolan, C.M.; Patel, S.; Polgar, O.; Haselden, B.M.; Polkey, M.I.; et al. Gait speed and adverse outcomes following hospitalised exacerbation of COPD. Eur. Respir. J. 2021, 58, 2004047. [Google Scholar] [CrossRef]

{kind=link}
| Control Group (n = 19) | Intervention Group (n = 19) | p-Value | |
|---|---|---|---|
| Age, years (IQR) | 74 (70–81) | 72 (67–80) | 0.518 |
| Sex (male), n (%) | 14 (73.7) | 16 (84.2) | 0.693 |
| GOLD category, n (A/B/E) | 2/12/5 | 4/9/6 | 0.677 |
| mMRC score | 2 (2–3) | 2 (2–3) | 0.529 |
| SpO2/FIO2 ratio | 382.7 ± 68.3 | 395 ± 56.0 | 0.539 |
| LTOT use, n (%) | 7 (36.8) | 6 (31.6) | 1.000 |
| Infection, n (%) | 11 (57.9) | 11 (57.9) | 1.000 |
| Charlson index | 1.4 ± 0.8 | 1.4 ± 0.8 | 1.000 |
| Corticosteroid use, n (%) | 11 (57.9) | 10 (52.6) | 1.000 |
| Length of stay, days | 17.5 ± 4.9 | 23.3 ± 20.5 | 0.236 |
| TP, g/dL | 6.3 ± 0.4 | 6.5 ± 0.5 | 0.117 |
| Alb, g/dL | 3.5 ± 0.8 | 3.3 ± 0.5 | 0.434 |
| CRP, mg/dL | 3.9 ± 4.3 | 3.2 ± 4.0 | 0.603 |
| BW, kg | 53.3 ± 14.1 | 51.8 ± 12.1 | 0.722 |
| BMI, kg/m2 * | 20.3 ± 4.0 | 19.9 ± 4.2 | 0.754 |
| %QS, kgf/kg | 48.0 ± 14.6 | 48.7 ± 16.0 | 0.898 |
| 6MWD, m | 225.1 ± 154.3 | 255.0 ± 157.9 | 0.563 |
| 10 m timed gait test, sec | 9.8 ± 3.6 | 12.1 ± 4.4 | 0.095 |
| SPPB, point | 9.3 ± 3.2 | 9.3 ± 3.3 | 1.000 |
| LMBI, kg/m2 | 14.6 ± 2.0 | 14.8 ± 2.1 | 0.745 |
| SMI, kg/m2 | 5.9 ± 2.0 | 5.8 ± 2.1 | 0.851 |
| Control Group (n = 19) | Intervention Group (n = 19) | p-Value | |
|---|---|---|---|
| Average nutritional intake | |||
| Energy intake, kcal/kg | 28.3 ± 8.4 | 37.0 ± 11.1 | 0.015 |
| Protein intake, g/kg | 1.2 ± 0.4 | 1.6 ± 0.4 | 0.011 |
| Changes in physical function and body compositions | |||
| %QS, kgf/kg | 1.4 ± 7.5 | 6.9 ± 7.7 | 0.031 |
| 6MWD, m | 65.8 ± 70.5 | 57.7 ± 61.0 | 0.711 |
| 10 m timed gait test, sec | −0.5 ± 1.5 | −2.5 ± 2.3 | 0.025 |
| SPPB, point | 0.4 ± 1.5 | 1.4 ± 1.6 | 0.010 |
| LMBI, kg/m2 | −0.5 ± 0.5 | 0.1 ± 0.3 | <0.001 |
| SMI, kg/m2 | −0.3 ± 0.2 | 0.1 ± 0.2 | <0.001 |
| BW, kg | −1.5 ± 1.3 | 0.3 ± 0.3 | <0.001 |
| Control Group (n = 19) | Intervention Group (n = 19) | |||||
|---|---|---|---|---|---|---|
| Pre | Post | p-Value | Pre | Post | p-Value | |
| TP, g/dL | 6.3 ± 0.4 | 6.4 ± 0.4 | 0.183 | 6.5 ± 0.5 | 6.6 ± 0.6 | 0.697 |
| Alb, g/dL | 3.5 ± 0.8 | 3.4 ± 0.5 | 0.522 | 3.3 ± 0.5 | 3.4 ± 0.5 | 0.576 |
| CRP, mg/dL | 3.9 ± 4.3 | 1.5 ± 2.9 | 0.025 | 3.2 ± 4.3 | 1.3 ± 2.9 | 0.133 |
| BW, kg | 53.3 ± 14.8 | 51.9 ± 13.6 | 0.001 | 51.8 ± 12.1 | 51.7 ± 11.6 | 0.915 |
| BMI, kg/m2 | 20.3 ± 4.0 | 19.7 ± 3.7 | <0.001 | 19.9 ± 4.2 | 19.8 ± 4.0 | 0.762 |
| Energy intake, kcal/kg | 28.3 ± 8.4 | 30.5 ± 9.9 | 0.079 | 37.0 ± 11.1 | 38.7 ± 10.1 | 0.013 |
| Protein intake, g/kg | 1.2 ± 0.4 | 1.3 ± 0.4 | 0.166 | 1.6 ± 0.4 | 1.6 ± 0.4 | 0.065 |
| LMBI, kg/m2 | 14.6 ± 2.0 | 14.1 ± 1.9 | 0.001 | 14.8 ± 2.1 | 14.9 ± 2.2 | 0.252 |
| SMI, kg/m2 | 5.9 ± 1.3 | 5.6 ± 1.2 | <0.001 | 5.8 ± 1.1 | 5.9 ± 1.1 | 0.243 |
| %QS, kgf/kg | 48.0 ± 14.6 | 49.4 ± 16.1 | 0.438 | 48.7 ± 16.0 | 55.6 ± 18.4 | 0.001 |
| 6MWD, m | 225 ± 154 | 291 ± 184 | <0.001 | 241 ± 164 | 313 ± 176 | <0.001 |
| 10 m timed gait test, sec | 9.8 ± 3.6 | 9.3 ± 3.8 | 0.178 | 12.1 ± 4.4 | 9.5 ± 2.5 | <0.001 |
| SPPB, point | 9.3 ± 3.2 | 9.8 ± 3.3 | 0.037 | 9.3 ± 3.3 | 10.7 ± 3.2 | 0.001 |
| Univariate Regression Analysis | Multivariate Regression Analysis | |||||
|---|---|---|---|---|---|---|
| Odds Ratio | 95% CI | p-Value | Odds Ratio | 95% CI | p-Value | |
| Age, years | 1.025 | 0.937–1.122 | 0.584 | − | − | − |
| GOLD category (A,B = 0, E = 1) | 1.143 | 0.264–4.951 | 0.853 | − | − | − |
| LTOT use, n (yes = 1, no = 0) | 0.638 | 0.137–2.973 | 0.561 | − | − | − |
| Total steroid use, mg | 0.998 | 0.993–1.002 | 0.208 | − | − | − |
| CRP, mg/dL | 0.859 | 0.681–1.165 | 0.145 | − | − | − |
| Number of RP sessions | 1.014 | 0.926–1.110 | 0.766 | 1.040 | 0.135–96.371 | 0.444 |
| Nutrition therapy (yes = 1, no = 0) | 7.65 | 1.370–−42.713 | 0.010 | 7.494 | 1.336–42.039 | 0.022 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oyama, Y.; Tatsumi, H.; Takikawa, H.; Taniguchi, N.; Masuda, Y. Combined Effect of Early Nutrition Therapy and Rehabilitation for Patients with Chronic Obstructive Pulmonary Disease Exacerbation: A Prospective Randomized Controlled Trial. Nutrients 2024, 16, 739. https://doi.org/10.3390/nu16050739
Oyama Y, Tatsumi H, Takikawa H, Taniguchi N, Masuda Y. Combined Effect of Early Nutrition Therapy and Rehabilitation for Patients with Chronic Obstructive Pulmonary Disease Exacerbation: A Prospective Randomized Controlled Trial. Nutrients. 2024; 16(5):739. https://doi.org/10.3390/nu16050739
Chicago/Turabian StyleOyama, Yohei, Hiroomi Tatsumi, Hiroko Takikawa, Natsuko Taniguchi, and Yoshiki Masuda. 2024. "Combined Effect of Early Nutrition Therapy and Rehabilitation for Patients with Chronic Obstructive Pulmonary Disease Exacerbation: A Prospective Randomized Controlled Trial" Nutrients 16, no. 5: 739. https://doi.org/10.3390/nu16050739
APA StyleOyama, Y., Tatsumi, H., Takikawa, H., Taniguchi, N., & Masuda, Y. (2024). Combined Effect of Early Nutrition Therapy and Rehabilitation for Patients with Chronic Obstructive Pulmonary Disease Exacerbation: A Prospective Randomized Controlled Trial. Nutrients, 16(5), 739. https://doi.org/10.3390/nu16050739