
A Herbal Prescription of Insamyangyeongtang as a Therapeutic Agent for Frailty in Elderly: A Narrative Review

Abstract
1. Introduction
2. Scientific Studies on the Herbal Medicine Prescription of IYT
2.1. The Origin of the Tonification Effect of IYT
2.2. Effect of IYT on Frailty Associated with Chronic Respiratory Diseases
2.3. Effect of IYT on Frailty Associated with Cognitive Impairments
2.4. Effect of IYT on Frailty Associated with Aging
2.5. Effect of IYT on Frailty Associated with Other Conditions
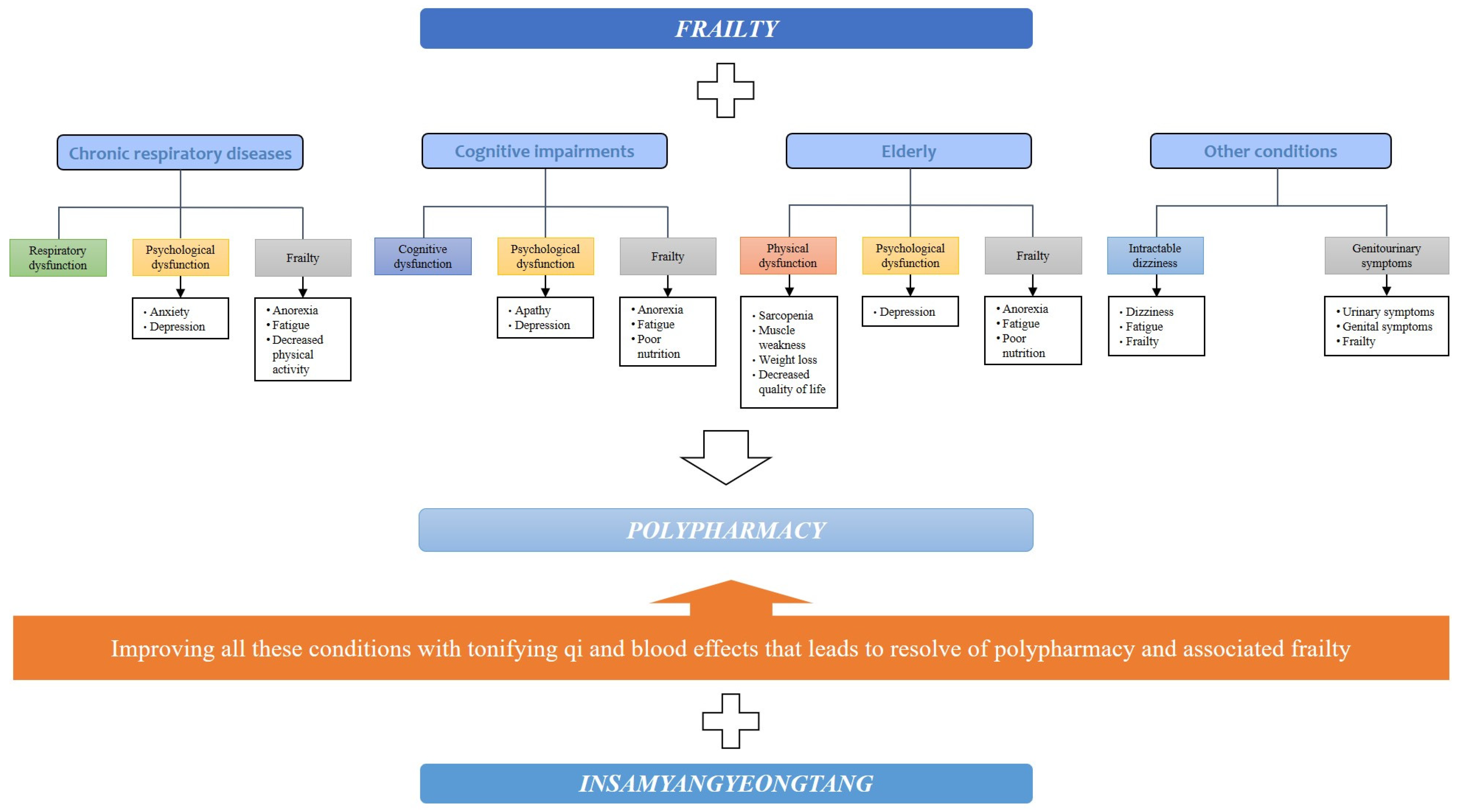
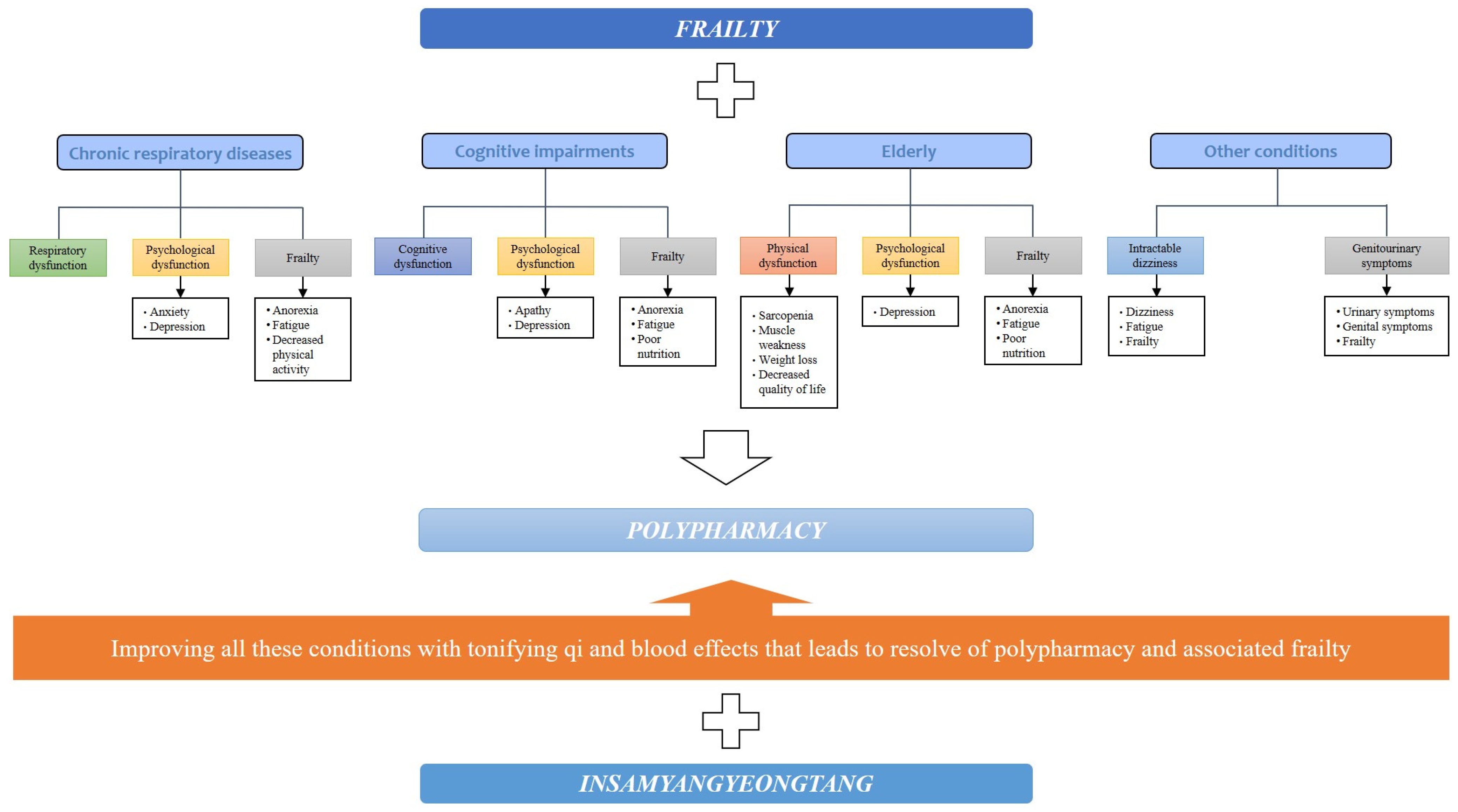
2.6. Possible Effect of IYT on Polypharmacy Associated with Frailty
3. Conclusions and Clinical Recommendation
Author Contributions
Funding
Conflicts of Interest
References
- Chen, X.; Mao, G.; Leng, S.X. Frailty syndrome: An overview. Clin. Interv. Aging 2014, 9, 433–441. [Google Scholar] [CrossRef]
- Cesari, M.; Prince, M.; Thiyagarajan, J.A.; De Carvalho, I.A.; Bernabei, R.; Chan, P.; Gutierrez-Robledo, L.M.; Michel, J.-P.; Morley, J.E.; Ong, P.; et al. Frailty: An Emerging Public Health Priority. J. Am. Med. Dir. Assoc. 2016, 17, 188–192. [Google Scholar] [CrossRef]
- Clegg, A.; Young, J.; Iliffe, S.; Rikkert, M.O.; Rockwood, K. Frailty in elderly people. Lancet 2013, 381, 752–762. [Google Scholar] [CrossRef]
- Rau, R.; Soroko, E.; Jasilionis, D.; Vaupel, J.W. Continued Reductions in Mortality at Advanced Ages. Popul. Dev. Rev. 2008, 34, 747–768. [Google Scholar] [CrossRef]
- Puts, M.T.E.; Toubasi, S.; Andrew, M.K.; Ashe, M.C.; Ploeg, J.; Atkinson, E.; Ayala, A.P.; Roy, A.; Monforte, M.R.; Bergman, H.; et al. Interventions to prevent or reduce the level of frailty in community-dwelling older adults: A scoping review of the literature and international policies. J. Am. Geriatr. Soc. 2017, 46, 383–392. [Google Scholar] [CrossRef]
- Basaria, S.; Coviello, A.D.; Travison, T.G.; Storer, T.W.; Farwell, W.R.; Jette, A.M.; Eder, R.; Tennstedt, S.; Ulloor, J.; Zhang, A.; et al. Adverse Events Associated with Testosterone Administration. N. Engl. J. Med. 2010, 363, 109–122. [Google Scholar] [CrossRef] [PubMed]
- Rossouw, J.E.; Anderson, G.L.; Prentice, R.L.; LaCroix, A.Z.; Kooperberg, C.; Stefanick, M.L.; Jackson, R.D.; Beresford, S.A.A.; Howard, B.V.; Johnson, K.C.; et al. Risks and Benefits of Estrogen Plus Progestin in Healthy Postmenopausal Women: Principal Results from the Women’s Health Initiative Randomized Controlled Trial. JAMA 2002, 288, 321–333. [Google Scholar] [CrossRef]
- Campbell, S.; Szoeke, C. Pharmacological treatment of frailty in the elderly. J. Pharm. Pract. Res. 2009, 39, 147–151. [Google Scholar] [CrossRef]
- Tsang, I.; Huang, S.; Koehler, B. Integration of Chinese medicine and Western medicine in clinical practice (Patient Care): Past, present, and a proposed model for the future. Chin. J. Integr. Med. 2013, 19, 83–85. [Google Scholar] [CrossRef]
- Keji, C.; Hao, X. The integration of traditional Chinese medicine and Western medicine. Eur. Rev. 2003, 11, 225–235. [Google Scholar] [CrossRef]
- Zhao, X.; Tan, X.; Shi, H.; Xia, D. Nutrition and traditional Chinese medicine (TCM): A system’s theoretical perspective. Eur. J. Clin. Nutr. 2020, 75, 267–273. [Google Scholar] [CrossRef]
- Zhang, Y.; Zhang, L.; Zhao, X.; Liu, Y.; Du, S.; Li, J.; Liu, T.; Liu, F.; Su, Z.; Jiang, Y.; et al. Symptom characteristics and prevalence of qi deficiency syndrome in people of varied health status and ages: A multicenter cross-sectional study. J. Tradit. Chin. Med. Sci. 2015, 2, 173–182. [Google Scholar] [CrossRef]
- He, Y.; Gao, T.; Li, J.; Chen, Z.; Wang, L.; Zhang, J.; Gao, F.; Fu, C. Metabonomics study on the effect of Siwu Decoction for blood deficiency syndrome in rats using UPLC–Q/TOF–MS analysis. Biomed. Chromatogr. 2019, 33, e4617. [Google Scholar] [CrossRef]
- Chiang, H.-C.; Chang, H.-H.; Huang, P.-Y.; Hsu, M. On the qi deficiency in traditional Chinese medicine. Taiwan. J. Obstet. Gynecol. 2014, 53, 317–323. [Google Scholar] [CrossRef]
- Nakae, H.; Hiroshima, Y.; Hebiguchi, M. Kampo Medicines for Frailty in Locomotor Disease. Front. Nutr. 2018, 5, 31. [Google Scholar] [CrossRef]
- Amitani, M.; Amitani, H.; Sloan, R.A.; Suzuki, H.; Sameshima, N.; Asakawa, A.; Nerome, Y.; Owaki, T.; Inui, A.; Hoshino, E. The translational aspect of complementary and alternative medicine for cancer with particular emphasis on Kampo. Front. Pharmacol. 2015, 6, 00150. [Google Scholar] [CrossRef] [PubMed]
- Miyano, K.; Nonaka, M.; Uzu, M.; Ohshima, K.; Uezono, Y. Multifunctional Actions of Ninjinyoeito, a Japanese Kampo Medicine: Accumulated Scientific Evidence Based on Experiments with Cells and Animal Models, and Clinical Studies. Front. Nutr. 2018, 5, 93. [Google Scholar] [CrossRef] [PubMed]
- Takayama, S.; Arita, R.; Ohsawa, M.; Kikuchi, A.; Yasui, H.; Makino, T.; Motoo, Y.; Ishii, T. Perspectives on the Use of Ninjin’yoeito in Modern Medicine: A Review of Randomized Controlled Trials. Evid.-Based Complement. Altern. Med. 2019, 2019, 9590260. [Google Scholar] [CrossRef] [PubMed]
- Japan Kampo Medicines Manufacturers Association. Kampo Formulations for Prescription 2022—Information in Package Inserts of 148 Formulation. Available online: https://www.nikkankyo.org/seihin/info_pi_english/introduction.pdf (accessed on 1 November 2023).
- Symvoulakis, E.K.; Kamekis, A.; Drakonaki, E.; Mastrodemou, S.; Ryerson, C.J.; Antoniou, K. Frailty and chronic respiratory disease: The need for a multidisciplinary care model. Sarcoidosis Vasc. Diffuse Lung Dis. 2021, 38, e2021031. [Google Scholar] [CrossRef] [PubMed]
- Bousquet, J.; Farrell, J.; Crooks, G.; Hellings, P.; Bel, E.H.; Bewick, M.; Chavannes, N.H.; de Sousa, J.C.; Cruz, A.A.; Haahtela, T.; et al. Scaling up strategies of the chronic respiratory disease programme of the European Innovation Partnership on Active and Healthy Ageing (Action Plan B3: Area 5). Clin. Transl. Allergy 2016, 6, 29. [Google Scholar] [CrossRef] [PubMed]
- Marengoni, A.; Vetrano, D.L.; Manes-Gravina, E.; Bernabei, R.; Onder, G.; Palmer, K. The Relationship Between COPD and Frailty. Chest 2018, 154, 21–40. [Google Scholar] [CrossRef] [PubMed]
- Sheth, J.S.; Xia, M.; Murray, S.; Martinez, C.H.; Meldrum, C.A.; Belloli, E.A.; Salisbury, M.L.; White, E.S.; Holtze, C.H.; Flaherty, K.R. Frailty and geriatric conditions in older patients with idiopathic pulmonary fibrosis. Respir. Med. 2019, 148, 6–12. [Google Scholar] [CrossRef] [PubMed]
- Raghu, G.; Collard, H.R.; Egan, J.J.; Martinez, F.J.; Behr, J.; Brown, K.K.; Colby, T.V.; Cordier, J.-F.; Flaherty, K.R.; Lasky, J.A.; et al. An Official ATS/ERS/JRS/ALAT Statement: Idiopathic Pulmonary Fibrosis: Evidence-based Guidelines for Diagnosis and Management. Am. J. Respir. Crit. Care Med. 2011, 183, 788–824. [Google Scholar] [CrossRef] [PubMed]
- Panossian, A.; Wikman, G. Pharmacology of Schisandra chinensis Bail.: An overview of Russian research and uses in medicine. J. Ethnopharmacol. 2008, 118, 183–212. [Google Scholar] [CrossRef] [PubMed]
- Hirai, K.; Homma, T.; Matsunaga, T.; Akimoto, K.; Yamamoto, S.; Suganuma, H.; Kashima, A.; Sato, H.; Ebato, T.; Miyata, Y.; et al. Usefulness of Ninjin’yoeito for Chronic Obstructive Pulmonary Disease Patients with Frailty. J. Altern. Complement. Med. 2020, 26, 750–757. [Google Scholar] [CrossRef] [PubMed]
- Kushima, H.; Kinoshita, Y.; Fujita, M.; Ishii, H. A retrospective study on the efficacy of Ninjin’yoeito on fatigue in patients with interstitial pneumonia. Neuropeptides 2021, 89, 102178. [Google Scholar] [CrossRef]
- Hirai, K.; Tanaka, A.; Homma, T.; Mikuni, H.; Kawahara, T.; Ohta, S.; Kusumoto, S.; Yamamoto, M.; Yamaguchi, F.; Suzuki, S.; et al. Improvement in Frailty in a Patient with Severe Chronic Obstructive Pulmonary Disease after Ninjin’yoeito Therapy: A Case Report. Front. Nutr. 2018, 5, 71. [Google Scholar] [CrossRef]
- Kashima, M. Case Report: Ninjin’yoeito May Improve Quality of Life After Hospitalization for Acute Illness in Patients with Frailty. Front. Nutr. 2021, 8, 547512. [Google Scholar] [CrossRef]
- Kushima, H.; Ishii, H.; Fujita, M. Case Report: Efficacy of Ninjin’yoeito Treatment for Idiopathic Pulmonary Fibrosis. Front. Nutr. 2021, 8, 548076. [Google Scholar] [CrossRef]
- Panza, F.; Seripa, D.; Solfrizzi, V.; Tortelli, R.; Greco, A.; Pilotto, A.; Logroscino, G. Targeting Cognitive Frailty: Clinical and Neurobiological Roadmap for a Single Complex Phenotype. J. Alzheimer’s Dis. 2015, 47, 793–813. [Google Scholar] [CrossRef]
- Panza, F.; Solfrizzi, V.; Barulli, M.R.; Santamato, A.; Seripa, D.; Pilotto, A.; Logroscino, G. Cognitive Frailty: A Systematic Review of Epidemiological and Neurobiological Evidence of an Age-Related Clinical Condition. Rejuvenation Res. 2015, 18, 389–412. [Google Scholar] [CrossRef]
- Robertson, D.A.; Savva, G.M.; Kenny, R.A. Frailty and cognitive impairment—A review of the evidence and causal mechanisms. Ageing Res. Rev. 2013, 12, 840–851. [Google Scholar] [CrossRef]
- Northey, J.M.; Cherbuin, N.; Pumpa, K.L.; Smee, D.J.; Rattray, B. Exercise interventions for cognitive function in adults older than 50: A systematic review with meta-analysis. Br. J. Sports Med. 2018, 52, 154–160. [Google Scholar] [CrossRef]
- Liu, Z.; Hsu, F.-C.; Trombetti, A.; King, A.C.; Liu, C.K.; Manini, T.M.; Fielding, R.A.; Pahor, M.; Newman, A.B.; Kritchevsky, S.; et al. Effect of 24-month physical activity on cognitive frailty and the role of inflammation: The LIFE randomized clinical trial. BMC Med. 2018, 16, 185. [Google Scholar] [CrossRef] [PubMed]
- Sugimoto, T.; Arai, H.; Sakurai, T. An update on cognitive frailty: Its definition, impact, associated factors and underlying mechanisms, and interventions. Geriatr. Gerontol. Int. 2021, 22, 99–109. [Google Scholar] [CrossRef] [PubMed]
- Seiwa, C.; Yamamoto, M.; Tanaka, K.; Fukutake, M.; Ueki, T.; Takeda, S.; Sakai, R.; Ishige, A.; Watanabe, K.; Akita, M.; et al. Restoration of FcRγ/Fyn signaling repairs central nervous system demyelination. J. Neurosci. Res. 2007, 85, 954–966. [Google Scholar] [CrossRef]
- Kudoh, C.; Arita, R.; Honda, M.; Kishi, T.; Komatsu, Y.; Asou, H.; Mimura, M. Effect of ninjin’yoeito, a Kampo (traditional Japanese) medicine, on cognitive impairment and depression in patients with Alzheimer’s disease: 2 years of observation. Psychogeriatrics 2015, 16, 85–92. [Google Scholar] [CrossRef]
- Deng, X.; Zhao, S.; Liu, X.; Han, L.; Wang, R.; Hao, H.; Jiao, Y.; Han, S.; Bai, C. Polygala tenuifolia: A source for anti-Alzheimer’s disease drugs. Pharm. Biol. 2020, 58, 410–416. [Google Scholar] [CrossRef] [PubMed]
- Shin, K.Y.; Lee, J.-Y.; Won, B.Y.; Jung, H.Y.; Chang, K.-A.; Koppula, S.; Suh, Y.-H. BT-11 is effective for enhancing cognitive functions in the elderly humans. Neurosci. Lett. 2009, 465, 157–159. [Google Scholar] [CrossRef]
- Lee, J.-Y.; Kim, K.Y.; Shin, K.Y.; Won, B.Y.; Jung, H.Y.; Suh, Y.-H. Effects of BT-11 on memory in healthy humans. Neurosci. Lett. 2009, 454, 111–114. [Google Scholar] [CrossRef]
- Yabe, T.; Iizuka, S.; Komatsu, Y.; Yamada, H. Enhancements of choline acetyltransferase activity and nerve growth factor secretion by Polygalae radix-extract containing active ingredients in Kami-untan-to. Phytomedicine 1997, 4, 199–205. [Google Scholar] [CrossRef]
- Ohsawa, M.; Tanaka, Y.; Ehara, Y.; Makita, S.; Onaka, K. A Possibility of Simultaneous Treatment with the Multicomponent Drug, Ninjin’yoeito, for Anorexia, Apathy, and Cognitive Dysfunction in Frail Alzheimer’s Disease Patients: An Open-Label Pilot Study. J. Alzheimer’s Dis. Rep. 2017, 1, 229–235. [Google Scholar] [CrossRef]
- Okahara, K.; Ohsawa, M.; Haruta-Tsukamoto, A.; Miyoshi, R.; Funahashi, H.; Fukutani, Y.; Makita, S.; Matsuo, H.; Ishida, Y. Frailty Improvement by Multicomponent Drug, Ninjin’Yoeito, in Mild Cognitive Impairment and Mild Alzheimer’s Disease Patients: An Open-Label Exploratory Study (FRAMINGO). J. Alzheimer’s Dis. Rep. 2023, 7, 107–117. [Google Scholar] [CrossRef] [PubMed]
- Matsui, Y.; Matsui, I. Case Report: Nutritional Examination of Weight Loss Treatment Using Kampo. Front. Nutr. 2021, 8, 551373. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, S.; Aihara, F.; Shibahara, M.; Sakai, K. Safety and Effectiveness of Ninjin’yoeito: A Utilization Study in Elderly Patients. Front. Nutr. 2019, 6, 14. [Google Scholar] [CrossRef] [PubMed]
- Xue, Q.-L.; Bandeen-Roche, K.; Varadhan, R.; Zhou, J.; Fried, L.P. Initial Manifestations of Frailty Criteria and the Development of Frailty Phenotype in the Women’s Health and Aging Study II. J. Gerontol. Ser. A 2008, 63, 984–990. [Google Scholar] [CrossRef] [PubMed]
- Bartali, B.; Frongillo, E.A.; Bandinelli, S.; Lauretani, F.; Semba, R.D.; Fried, L.P.; Ferrucci, L. Low Nutrient Intake Is an Essential Component of Frailty in Older Persons. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2006, 61, 589–593. [Google Scholar] [CrossRef] [PubMed]
- Bonnefoy, M.; Cornu, C.; Normand, S.; Boutitie, F.; Bugnard, F.; Rahmani, A.; Lacour, J.R.; Laville, M. The effects of exercise and protein–energy supplements on body composition and muscle function in frail elderly individuals: A long-term controlled randomised study. Br. J. Nutr. 2003, 89, 731–738. [Google Scholar] [CrossRef]
- Sakisaka, N. Frailty and ninjin’yoeito. Phil Kampo 2017, 64, 17–19. [Google Scholar]
- Sakisaka, N.; Mitani, K.; Sempuku, S.; Imai, T.; Takemoto, Y.; Shimomura, H.; Ushiroyama, T. A Clinical Study of Ninjin’yoeito with Regard to Frailty. Front. Nutr. 2018, 5, 73. [Google Scholar] [CrossRef]
- Arai, H. Implication of frailty in elderly care. Nihon Ronen Igakkai Zasshi 2014, 51, 497–501. [Google Scholar]
- Kamegaya, T.; Yamaguchi, H.; Hayashi, K. Evaluation by the Basic Checklist and the risk of 3 years incident long-term care insurance certification. J. Gen. Fam. Med. 2017, 18, 230–236. [Google Scholar] [CrossRef]
- Nakagawa, Y.; Kagohashi, K.; Shioya, A.; Kinoshita, K.; Tsuji, H.; Satoh, H. Maintaining Weight and Nutritional Status with Ninjinyoueito in Elderly Patients with Chronic Wasting Diseases. Sultan Qaboos Univ. Med. J. 2021, 22, 280–282. [Google Scholar] [CrossRef]
- Morinaga, A.; Nakamura, H.; Hattanmaru, K.; Rokot, N.T.; Kimura, Y.; Ito, T. Good Rehabilitation Outcomes and Improved Nutritional Status After Treatment with the Japanese Herbal Medicine Ninjin’yoeito in an Elderly Patient with Hip Fracture and Sarcopenia: A Case Report. Front. Nutr. 2020, 7, 85. [Google Scholar] [CrossRef]
- Sakisaka, N. Long-term administration of ninjin’yoeito to treat frailty in older adults: A case series. Neuropeptides 2022, 93, 102244. [Google Scholar] [CrossRef]
- Arai, M. Evaluating the usefulness of Ninjin’yoeito Kampo medicine in combination with rehabilitation therapy in patients with frailty complicated by intractable dizziness. Neuropeptides 2021, 90, 102189. [Google Scholar] [CrossRef]
- Taguchi, C.K.; Menezes, P.d.L.; Melo, A.C.S.; de Santana, L.S.; Conceição, W.R.S.; de Souza, G.F.; Araújo, B.C.L.; da Silva, A.R. Frailty syndrome and risks for falling in the elderly community. CoDAS 2022, 34, e20210025. [Google Scholar] [CrossRef]
- Sun, Y.; Harlow, B.L. The association of vulvar pain and urological urgency and frequency: Findings from a community-based case–control study. Int. Urogynecol. J. 2019, 30, 1871–1878. [Google Scholar] [CrossRef] [PubMed]
- Mercier, J.; Dumoulin, C.; Carrier-Noreau, G. Pelvic floor muscle rehabilitation for genitourinary syndrome of menopause: Why, how and when? Climacteric 2023, 26, 302–308. [Google Scholar] [CrossRef] [PubMed]
- Okui, N.; Okui, M. Ninjin’yoeito Improves Genitourinary Symptoms in Patients with Frailty. Cureus 2023, 15, e40767. [Google Scholar] [CrossRef] [PubMed]
- Jokanovic, N.; Tan, E.C.K.; Dooley, M.J.; Kirkpatrick, C.M.; Bell, J.S. Prevalence and factors associated with polypharmacy in long-term care facilities: A systematic review. J. Am. Med. Dir. Assoc. 2015, 16, 535.e1–535.e12. [Google Scholar] [CrossRef] [PubMed]
- Field, T.S.; Gurwitz, J.H.; Harrold, L.R.; Rothschild, J.; DeBellis, K.R.; Seger, A.C.; Auger, J.C.; Garber, L.A.; Cadoret, C.; Fish, L.S.; et al. Risk Factors for Adverse Drug Events Among Older Adults in the Ambulatory Setting. J. Am. Geriatr. Soc. 2004, 52, 1349–1354. [Google Scholar] [CrossRef] [PubMed]
- Gómez, C.; Vega-Quiroga, S.; Bermejo-Pareja, F.; Medrano, M.J.; Louis, E.D.; Benito-León, J. Polypharmacy in the Elderly: A Marker of Increased Risk of Mortality in a Population-Based Prospective Study (NEDICES). Gerontology 2014, 61, 301–309. [Google Scholar] [CrossRef] [PubMed]
- Maher, R.L.; Hanlon, J.; Hajjar, E.R. Clinical consequences of polypharmacy in elderly. Expert Opin. Drug Saf. 2013, 13, 57–65. [Google Scholar] [CrossRef]
- Palmer, K.; Marengoni, A.; Russo, P.; Mammarella, F.; Onder, G. Frailty and drug use. Frailty 2016, 38, 102. [Google Scholar] [CrossRef]
- Derhem, B.; Özsari, S. Frailty and Polypharmacy in Primary Care. Biol. Res. Nurs. 2023, 25, 658–663. [Google Scholar] [CrossRef]
- Gutiérrez-Valencia, M.; Izquierdo, M.; Cesari, M.; Casas-Herrero, Á.; Inzitari, M.; Martínez-Velilla, N. The relationship between frailty and polypharmacy in older people: A systematic review. Br. J. Clin. Pharmacol. 2018, 84, 1432–1444. [Google Scholar] [CrossRef]
- Barnett, K.; Mercer, S.W.; Norbury, M.; Watt, G.; Wyke, S.; Guthrie, B. Epidemiology of multimorbidity and implications for health care, research, and medical education: A cross-sectional study. Lancet 2012, 380, 37–43. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| First Author (Year) | Subjects, Design and Intervention | Results |
|---|---|---|
| Hirai (2020) [26] | 62 patients with COPD with frailty Randomized controlled trial IYT group: IYT (dried extract 6.7 g/day) for 24 weeks (n = 31) Control group: Conventional treatment for 24 weeks (n = 31) Primary outcome: Changes of KCL score (frailty basic checklist score) Secondary outcomes: Changes of SNAQ, CAT, HADS | Primary outcome: IYT [−1 (−3 to 0)] vs. control [0 (−2 to 0)], p = 0.09 SNAQ: IYT [1 (0 to 2)] vs. control [0 (0 to 1)], p = 0.03 CAT: IYT [−1 (−4 to 1)] vs. control [1 (−1 to 3)], p = 0.03 HADS-Anxeity: IYT [−2 (−3 to 0)] vs. control [1 (−1 to 1)], p < 0.01 HADS-Depression: IYT [0 (−3 to 0)] vs. control [0 (−2 to 2)], p = 0.02 |
| Kushima (2021) [27] | 16 patients with interstitial pneumonia with fatigue Retrospective study IYT (dried extract 6.7 g/day) + conventional treatment for 12 weeks Primary outcome: CFS Secondary outcomes: SNAQ, mMRC | CFS significantly decrease (17.1 ± 6.8 to 13.4 ± 5.7, p = 0.0389) SNAQ increased without significance (14.3 ± 1.6 to 14.4 ± 1.9, p = 0.8145) mMRC median decreased without significance [3 (2–3) to 2 (1–3), p = 0.0956] |
| Kuniaki (2018) [28] | A 76-year-old patient with severe COPD with frailty Case report IYT (dried extract 6.7 g/day) for 1 month | Body composition (kg): Body weight (46.5 to 54.5), Muscle mass (32.1 to 38.3). Factors: CAT (26 to 12), KCL (15 to 6), HADS-Anxiety (13 to 5), HADS-Depression (15 to 5) |
| Kashima (2021) [29] | 3 frail patients who started taking IYT from the time of discharge after being hospitalized for COPD and pneumonia Case report IYT (dried extract 6.7 g/day) for 12 weeks SF-36 component: Physical function, PF; role physical, RP; body pain, BP; general health, GH; vitality, VT; social function, SF; role emotional, RE; mental health, MH | Case 1 (87-year-old male with COPD): SF-36 score 0, 4, 12 weeks after taking IYT [(BP; 41, 51, 100), (SF; 50, 100, 100), (MH; 75, 75, 90) Case 2 (65-year-old male with COPD): SF-36 score 0, 12 weeks after taking IYT [(PF; 70, 95), (RP; 75, 100), (BP; 72, 84), (GH; 45, 52), (VT; 37.5, 75), (RE; 75, 100), (MH; 70, 90) Case 3 (80-year-old with Pneumonia): SF-36 score 0, 4 weeks after taking IYT [(RP; 68.8, 100), (BP; 52, 61), (GH; 52, 72), (VT; 43.8, 62.5), (SF; 37.5, 100), (RE; 58.3, 91.7) |
| Kushima (2021) [30] | 2 patients with idiopathic pulmonary fibrosis Case report IYT (dried extract 6.7 g/day) for 12 weeks | Case 1 (59-year-old male): SNAQ (15 to 16), CFS (6 to 4), Body weight (51.8 kg to 55.2 kg) Case 2 (59-year-old male): SNAQ (14 to 14), CFS (27 to 24), Body weight (50.2 kg to 51.9 kg) |
| First Author (Year) | Subjects, Design and Intervention | Results |
|---|---|---|
| Ohsawa (2017) [43] | 20 frail AD patients with anorexia and apathy Single-arm, nonrandomized, historical-controlled study IYT (dried extract 4 or 6 g/day) for 12 weeks Primary outcome: NPI-anorexia score Secondary outcomes: NPI-apathy score, vitality index, MMSE score, physical and blood nutrition indices | NPI-anorexia score significantly decreased by week 4 (baseline: 4.85 ± 0.58; 4 w: 3.06 ± 0.60, p < 0.05; 8 w: 1.50 ± 0.43, p < 0.001; 12 w: 1.00 ± 0.44, p < 0.001). NPI-apathy score significantly decreased by week 4 (baseline 5.85 ± 0.65; 4 w: 4.00 ± 0.57, p < 0.001; 8 w: 3.38 ± 0.54, p < 0.001; 12 w: 3.31 ± 0.51, p < 0.001) Meal ingestion amount improved by week 4 (4 w: 0.61 ± 0.14, p < 0.01; 8 w: 0.94 ± 0.17, p < 0.001; 12 w: 0.94 ± 0.19, p < 0.001) Vitality index improved in 12 weeks (baseline: 7.05 ± 0.43; 12 w: 7.94 ± 0.39, p < 0.05) MMSE improved in 12 weeks (baseline: 17.32 ± 1.29, 12 w: 19.44 ± 1.30, p < 0.001) |
| Okahara (2023) [44] | 14 frail or prefrail patients with MCI (n = 9) or mild AD (n = 5) A open label exploratory study IYT (dried extract 4 or 6 g/day) for 24 weeks Primary outcomes: NPI-anorexia score Secondary outcomes: J-CHS score, body composition, fatigue VAS, blood nutrition index, CONUT score, total lymphocyte count, total cholesterol level, NPI-depression and apathy, global CDR and CDR-SB, MoCA-J | NPI-anorexia score significantly decreased in 4, 8, 16 and 24 week [Baseline: 8.0 (4.0–8.0); 4 w: 0.0 (0.0–2.8), p < 0.01; 8 w: 0.0 (0.0–1.8), p < 0.01; 16 w: 0.0 (0.0–0.8), p < 0.001; 24 w: 0.0 (0.0–1.0), p < 0.01] J-CHS score significantly decreased in 24 weeks [baseline: 3.0 (3.0–3.0); 24 weeks: 2.0 (1.0–2.0), p < 0.01] Fatigue VAS score decreased significantly in 16 weeks [baseline: 40.5 (30.0–51.5); 16 weeks: 25.0 (20.3–29.5), p < 0.05] NPI-depression score significantly decreased in 8 and 16 weeks [baseline: 1.0 (0.0–1.0); 8 w: 0.0 (0.0–0.8), p < 0.05; 16 w: 0.0 (0.0–0.0), p < 0.05] No significant change in body composition and CONUT score Global CDR, CDR-SB and MoCA-J scores remained at the baseline level for 24 weeks |
| Matsui (2021) [45] | 3 AD patients with loss of appetite and weight loss Case report Case 1: 84-year-old female, IYT (dried extract 3.35 g/day) for 9 months Case 2: 74-year-old female, IYT (dried extract 3.35 g/day) for 14 months Case 3: 81-year-old male, IYT (dried extract 3.35 g/day) for 14 months | Case 1: Body weight, muscle mass and weight after removing the body fluid weight increased [1.0 kg (50.4 kg to 51.4 kg), 0.6 kg (30.2 kg to 30.8kg), 0.6 kg (31.3 kg to 31.9 kg), respectively] Case 2: Body weight, muscle mass and weight after removing the body fluid weight increased [3.4 kg (53.3 kg to 56.7 kg), 0.4 kg (32.6 kg to 33.0 kg), 3.9 kg (28.8 kg to 32.7 kg), respectively] Case 3: Body weight, muscle mass and weight after removing the body fluid weight increased [2.5 kg (46.8 kg to 49.3 kg), 2.4 kg (34.3 kg to 36.7 kg), 1.0 kg (25.1 kg to 26.1 kg), respectively] |
| First Author (Year) | Subjects, Design and Intervention | Results |
|---|---|---|
| Sakisaka (2018) [51] | 113 elderly frail patients Comparative study using envelop method IYT group: IYT (dried extract 6.7 g/day) + conventional treatment for 24 weeks (n = 64) Control group: Conventional treatment for 24 w (n = 49) Outcomes: Grip strength, muscle quality score | Grip strength: Significantly improved in IYT group [Right hand: baseline (18.2 ± 5.7) vs. 24 w (19.0 ± 5.8), p < 0.01; Left hand: baseline (17.9 ± 5.8) vs. 24 w (19.0 ± 5.8), p < 0.01] and vs. control group by amount of changes in 24w [Right hand: IYT group (0.80 ± 2.67) vs. control group (−0.43 ± 2.16), p < 0.01; Left hand: IYT group (1.10 ± 3.15) vs. control group (−1.03 ± 2.82), p < 0.001] Mucle quality score: No change in IYT group, significantly deteriorated in control group [baseline (42.6 ± 16.0) vs. 24 w (40.6 ± 16.5), p < 0.05], compared by amount of change in 24 w, significantly improved in IYT group [IYT group (0.80 ± 2.67) vs. control croup (−0.43 ± 2.16), p < 0.01] |
| Suzuki (2019) [46] | 808 elderly patients prescribed IYT in 383 centers Open-label, non-comparative, prospective, multicenter, post-marketing survey Outcomes: Safety (Adverse reaction), Efficacy (VAS scores in fatigue/malaise and anorexia at 8, 16, 24 weeks, Basic Checklist by the Ministry of Health, Labor and Welfare of Japan at 8, 16 and 24 weeks) | ① Safety (n = 808) Adverse reactions: 31 occurred in 25 patients (Incidence of 3.1%) ② Efficacy (n = 537) VAS score: Significantly decreased in fatigue/malaise (8, 16 and 24 weeks, p < 0.01) and anorexia (8 weeks, p < 0.05; 24 weeks, p < 0.01) Basic checklist: The proportion of patients expected to requre nursin care significantly decreased in four domains (activities of daily living, motor function, oral function, and depression) Physician assessment: Related as “effective” or “moderately effective” in 486/537 cases (90.5%) |
| Nakagawa (2022) [54] | 11 elderly patients with chronic wasting disease A retrospective study IYT (dried extract 4 or 6 g/day) for 6 or more months Outcomes: Body weight, serum levels of total protein and albumin before and after IYT administration | Body weight: No significant difference (median: 47.9 kg, range: 43.5–70.0 kg, vs. median: 48 kg, range: 42.7–70.0 kg; p = 0.176) Serum total protein level: No significant differnce (median: 7.0 g/dL, range: 5.7–8.2 g/dL vs. median: 6.9 g/dL, range: 5.8–7.9 g/dL; p = 0.766) Serum albumin level: No significant differnce (median: 3.9 g/dL, range: 2.8–4.6 g/dL vs. median: 3.9 g/dL, range: 2.4–4.6 g/dL; p = 0.550) |
| Morinaga (2020) [55] | A 92-year-old male patient with hip fracture and sarcopenia Case report IYT (dried extract 6.7 g/day) for 2 months Outcomes: Body weight, body fat percentage, muscle mass, serum level of proteins, total FIM score, average daily calorie intake | Body weight: 61 kg to 56.5 kg Body fat percentage: 34.1% to 21.1% Muscle mass: 38.2 kg to 38.9 kg Serum level of proteins: Total protein (6.8 g/dL to 7.1 g/dL), transferrin (227 mg/dL to 238 mg/dL), prealbumin (24.7 mg/dL to 27.9 mg/dL), retinol-binding protein (2.9 mg/dL to 3.6 mg/dL) Total FIM score: 49 to 105 Average daily calorie intake: 992 kcal to 1159 kcal |
| Sakisaka (2022) [56] | 3 elderly with frailty Case report IYT (dried extract 6.7 g/day) for 24 months Outcomes: Both grip strength, muscle quality score | Case 1 (82-year-old man with prior surgery for lung cancer): Grip strength increased [Right 1.4% (22.0 kg to 22.6 kg), Left 16.9% (16.0 kg to 21.4 kg)], muscle quality score improved 17.1% (35 to 47) Case 2 (68-year-old woman with history of pancreatic cancer): Grip strength increased [Right 3.0% (24.09 kg to 25.55 kg), Left 1.7% (22.30 kg to 23.05 kg)], muscle quality score improved 1.2% (42 to 43) Case 3 (73-year-old woman with sequelae of a cerebral hemorrhage): Grip strength increased [Right 24.5% (9.10 kg to 13.55 kg), Left 0.1% (21.20 kg to 21.25 kg)], muscle quality score improved 0.4% (40 to 40) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, H.-G.; Arai, I.; Kwon, S. A Herbal Prescription of Insamyangyeongtang as a Therapeutic Agent for Frailty in Elderly: A Narrative Review. Nutrients 2024, 16, 721. https://doi.org/10.3390/nu16050721
Lee H-G, Arai I, Kwon S. A Herbal Prescription of Insamyangyeongtang as a Therapeutic Agent for Frailty in Elderly: A Narrative Review. Nutrients. 2024; 16(5):721. https://doi.org/10.3390/nu16050721
Chicago/Turabian StyleLee, Han-Gyul, Ichiro Arai, and Seungwon Kwon. 2024. "A Herbal Prescription of Insamyangyeongtang as a Therapeutic Agent for Frailty in Elderly: A Narrative Review" Nutrients 16, no. 5: 721. https://doi.org/10.3390/nu16050721
APA StyleLee, H.-G., Arai, I., & Kwon, S. (2024). A Herbal Prescription of Insamyangyeongtang as a Therapeutic Agent for Frailty in Elderly: A Narrative Review. Nutrients, 16(5), 721. https://doi.org/10.3390/nu16050721