

Beneficial Effects of Spirulina Supplementation in the Management of Cardiovascular Diseases
 , , ,
, , ,
Abstract
1. Introduction
Chemical Composition of Spirulina
2. Hypertension and Stroke
2.1. Clinical Studies
2.2. Animal Studies
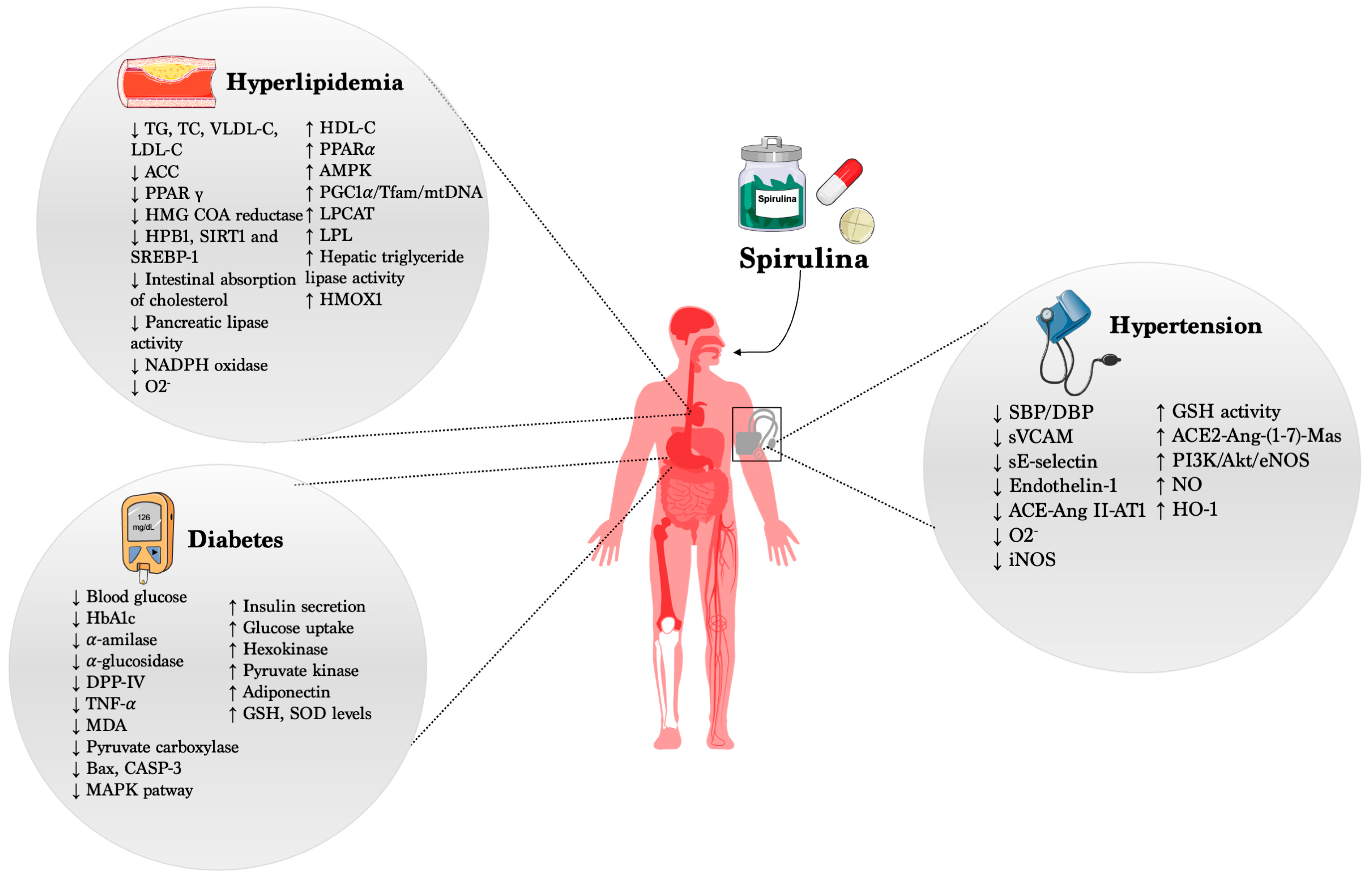
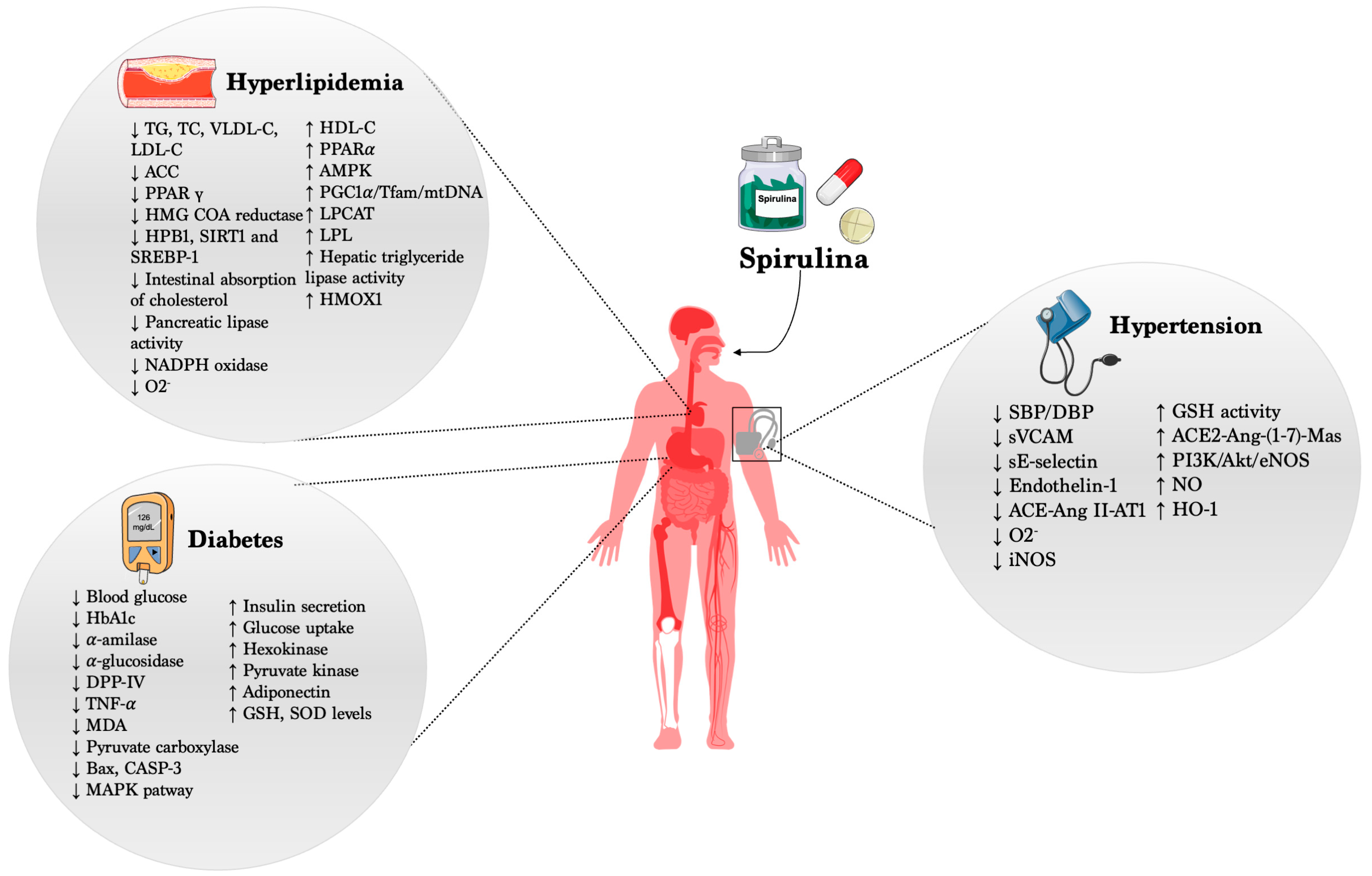
2.3. Mechanisms of Action
3. Diabetes
3.1. Clinical Studies
3.2. Animal Studies
3.3. Mechanism of Action
4. Hyperlipidemia
4.1. Clinical Studies
4.2. Animal Studies
4.3. Mechanism of Action
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Komárek, J.; Kaštovský, J.; Mareš, J.; Johansen, J.R. Taxonomic classification of cyanoprokaryotes (cyanobacterial genera) 2014, using a polyphasic approach. Preslia 2014, 86, 295–335. [Google Scholar]
- Volkmann, H.; Imianovsky, U.; Oliveira, J.L.; Sant’Anna, E.S. Cultivation of Arthrospira (Spirulina) platensis in desalinator wastewater and salinated synthetic medium: Protein content and amino-acid profile. Braz. J. Microbiol. 2008, 39, 98–101. [Google Scholar] [CrossRef] [PubMed]
- Tamagnini, P.; Axelsson, R.; Lindberg, P.; Oxelfelt, F.; Wünschiers, R.B.; Lindblad, P. Hydrogenases and hydrogen metabolism of cyanobacteria. Microbiol. Mol. Biol. Rev. 2002, 66, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Vonshak, A. Spirulina Platensis Arthrospira: Physiology, Cell-Biology and Biotechnology; CRC Press: Boca Raton, FL, USA, 1997. [Google Scholar]
- Kulshreshtha, A.; Jarouliya, U.; Bhadauriya, P.; Prasad, G.; Bisen, P. Spirulina in health care management. Curr. Pharm. Biotechnol. 2008, 9, 400–405. [Google Scholar] [CrossRef]
- Ahmad, A.M.R.; Intikhab, A.; Zafar, S.; Farooq, U.; Shah, H.B.U.; Akram, S.; Abid, J.; Parveen, Z.; Iqbal, S. Spirulina, an FDA-approved functional food: Worth the hype? Cell. Mol. Biol. 2023, 69, 137–144. [Google Scholar] [CrossRef]
- Lafarga, T. Effect of microalgal biomass incorporation into foods: Nutritional and sensorial attributes of the end products. Algal Res. 2019, 41, 101566. [Google Scholar] [CrossRef]
- Morais, M.G.D.; Vaz, B.D.S.; Morais, E.G.D.; Costa, J.A.V. Biological effects of Spirulina (Arthrospira) biopolymers and biomass in the development of nanostructured scaffolds. BioMed Res. Int. 2014, 2014, 762705. [Google Scholar] [CrossRef]
- Karkos, P.; Leong, S.; Karkos, C.; Sivaji, N.; Assimakopoulos, D. Spirulina in clinical practice: Evidence-based human applications. Evid.-Based Complement. Altern. Med. 2011, 2011, 531053. [Google Scholar] [CrossRef]
- Chei, S.; Oh, H.; Song, J. Spirulina maxima extract prevents activation of the NLRP3 in ammasome by inhibiting ERK signaling. Sci. Rep. 2020, 10, 2075. [Google Scholar] [CrossRef]
- Deng, R.; Chow, T.J. Hypolipidemic, antioxidant, and antiinflammatory activities of microalgae Spirulina. Cardiovasc. Ther. 2010, 28, e33–e45. [Google Scholar] [CrossRef]
- Rao, A.V.; Rao, L.G. Carotenoids and human health. Pharmacol. Res. 2007, 55, 207–216. [Google Scholar] [CrossRef]
- Grover, P.; Bhatnagar, A.; Kumari, N.; Bhatt, A.N.; Nishad, D.K.; Purkayastha, J. C-Phycocyanin-a novel protein from Spirulina platensis-In vivo toxicity, antioxidant and immunomodulatory studies. Saudi J. Biol. Sci. 2021, 28, 1853–1859. [Google Scholar] [CrossRef] [PubMed]
- Sommella, E.; Conte, G.M.; Salviati, E.; Pepe, G.; Bertamino, A.; Ostacolo, C.; Sansone, F.; Prete, F.D.; Aquino, R.P.; Campiglia, P. Fast profiling of natural pigments in different spirulina (Arthrospira platensis) dietary supplements by DI-FT-ICR and evaluation of their antioxidant potential by pre-column DPPH-UHPLC assay. Molecules 2018, 23, 1152. [Google Scholar] [CrossRef] [PubMed]
- Bhat, V.B.; Madyastha, K. C-phycocyanin: A potent peroxyl radical scavenger in vivo and in vitro. Biochem. Biophys. Res. Commun. 2000, 275, 20–25. [Google Scholar] [CrossRef] [PubMed]
- Gaidai, O.; Cao, Y.; Loginov, S. Global cardiovascular diseases death rate prediction. Curr. Probl. Cardiol. 2023, 48, 101622. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J. Nutraceuticals, nutritional therapy, phytonutrients, and phytotherapy for improvement of human health: A perspective on plant biotechnology application. Recent Pat. Biotechnol. 2007, 1, 75–97. [Google Scholar] [CrossRef] [PubMed]
- ElFar, O.A.; Billa, N.; Lim, H.R.; Chew, K.W.; Cheah, W.Y.; Munawaroh, H.S.H.; Balakrishnan, D.; Show, P.L. Advances in delivery methods of Arthrospira platensis (spirulina) for enhanced therapeutic outcomes. Bioengineered 2022, 13, 14681–14718. [Google Scholar] [CrossRef] [PubMed]
- Chauhan, B.; Kumar, G.; Kalam, N.; Ansari, S.H. Current concepts and prospects of herbal nutraceutical: A review. J. Adv. Pharm. Technol. Res. 2013, 4, 4. [Google Scholar]
- Garrido-Cardenas, J.A.; Manzano-Agugliaro, F.; Acien-Fernandez, F.G.; Molina-Grima, E. Microalgae research worldwide. Algal Res. 2018, 35, 50–60. [Google Scholar] [CrossRef]
- Lafarga, T.; Fernández-Sevilla, J.M.; González-López, C.; Acién-Fernández, F.G. Spirulina for the food and functional food industries. Food Res. Int. 2020, 137, 109356. [Google Scholar] [CrossRef]
- da Rosa, G.M.; Moraes, L.; Cardias, B.B.; Costa, J.A.V. Chemical absorption and CO2 biofixation via the cultivation of Spirulina in semicontinuous mode with nutrient recycle. Bioresour. Technol. 2015, 192, 321–327. [Google Scholar] [CrossRef]
- Matos, Â.P.; Feller, R.; Moecke, E.H.S.; de Oliveira, J.V.; Junior, A.F.; Derner, R.B.; Sant’Anna, E.S. Chemical characterization of six microalgae with potential utility for food application. J. Am. Oil Chem. Soc. 2016, 93, 963–972. [Google Scholar] [CrossRef]
- Ljubic, A.; Safafar, H.; Holdt, S.L.; Jacobsen, C. Biomass composition of Arthrospira platensis during cultivation on industrial process water and harvesting. J. Appl. Phycol. 2018, 30, 943–954. [Google Scholar] [CrossRef]
- Carcea, M.; Sorto, M.; Batello, C.; Narducci, V.; Aguzzi, A.; Azzini, E.; Fantauzzi, P.; Finotti, E.; Gabrielli, P.; Galli, V. Nutritional characterization of traditional and improved dihé, alimentary blue-green algae from the lake Chad region in Africa. LWT-Food Sci. Technol. 2015, 62, 753–763. [Google Scholar] [CrossRef]
- Watanabe, F.; Katsura, H.; Takenaka, S.; Fujita, T.; Abe, K.; Tamura, Y.; Nakatsuka, T.; Nakano, Y. Pseudovitamin B12 is the predominant cobamide of an algal health food, spirulina tablets. J. Agric. Food Chem. 1999, 47, 4736–4741. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira Rangel-Yagui, C.; Danesi, E.D.G.; De Carvalho, J.C.M.; Sato, S. Chlorophyll production from Spirulina platensis: Cultivation with urea addition by fed-batch process. Bioresour. Technol. 2004, 92, 133–141. [Google Scholar] [CrossRef]
- Lafarga, T. Cultured microalgae and compounds derived thereof for food applications: Strain selection and cultivation, drying, and processing strategies. Food Rev. Int. 2020, 36, 559–583. [Google Scholar] [CrossRef]
- Markou, G.; Chatzipavlidis, I.; Georgakakis, D. Carbohydrates production and bio-flocculation characteristics in cultures of Arthrospira (Spirulina) platensis: Improvements through phosphorus limitation process. BioEnergy Res. 2012, 5, 915–925. [Google Scholar] [CrossRef]
- Oparil, S.; Acelajado, M.; Bakris, G.; Berlowitz, D.; Cifkova, R.; Dominiczak, A. Hypertension. Nat. Rev. Dis. Primers 2018, 4, 18014. [Google Scholar] [CrossRef]
- World Health Organization. Diet, Nutrition, and the Prevention of Chronic Diseases: Report of a Joint WHO/FAO Expert Consultation; World Health Organization: Geneva, Switzerland, 2003; Volume 916. [Google Scholar]
- Goodfriend, T.L.; Lyerly, K.M. Essential Hypertension. In Pathophysiology of Kidney Disease and Hypertension; Elsevier: Amsterdam, The Netherlands, 2009; pp. 179–195. [Google Scholar]
- Cifu, A.S.; Davis, A.M. Prevention, detection, evaluation, and management of high blood pressure in adults. JAMA 2017, 318, 2132–2134. [Google Scholar] [CrossRef]
- Iadecola, C.; Davisson, R.L. Hypertension and cerebrovascular dysfunction. Cell Metab. 2008, 7, 476–484. [Google Scholar] [CrossRef]
- Unger, T.; Borghi, C.; Charchar, F.; Khan, N.A.; Poulter, N.R.; Prabhakaran, D.; Ramirez, A.; Schlaich, M.; Stergiou, G.S.; Tomaszewski, M. 2020 International Society of Hypertension global hypertension practice guidelines. Hypertension 2020, 75, 1334–1357. [Google Scholar] [CrossRef] [PubMed]
- Wermelt, J.; Schunkert, H. Management of arterial hypertension. Herz 2017, 42, 515–526. [Google Scholar] [CrossRef] [PubMed]
- Niranjan, P.K.; Bahadur, S. Recent Developments in Drug Targets and Combination Therapy for the Clinical Management of Hypertension. Cardiovasc. Haematol. Disord.-Drug Targets (Former. Curr. Drug Targets-Cardiovasc. Hematol. Disord.) 2023, 23, 226–245. [Google Scholar] [CrossRef] [PubMed]
- Egan, B.M.; Bandyopadhyay, D.; Shaftman, S.R.; Wagner, C.S.; Zhao, Y.; Yu-Isenberg, K.S. Initial monotherapy and combination therapy and hypertension control the first year. Hypertension 2012, 59, 1124–1131. [Google Scholar] [CrossRef] [PubMed]
- Ghaem Far, Z.; Babajafari, S.; Kojuri, J.; Mohammadi, S.; Nouri, M.; Rostamizadeh, P.; Rahmani, M.H.; Azadian, M.; Ashrafi-Dehkordi, E.; Zareifard, A. Antihypertensive and antihyperlipemic of spirulina (Arthrospira platensis) sauce on patients with hypertension: A randomized triple-blind placebo-controlled clinical trial. Phytother. Res. 2021, 35, 6181–6190. [Google Scholar] [CrossRef]
- Miczke, A.; Szulińska, M.; Hansdorfer-Korzon, R.; Kręgielska-Narożna, M.; Suliburska, J.; Walkowiak, J.; Bogdański, P. Effects of spirulina consumption on body weight, blood pressure, and endothelial function in overweight hypertensive Caucasians: A doubleblind, placebo-controlled, randomized trial. Eur. Rev. Med. Pharmacol. Sci. 2016, 20, 150–156. [Google Scholar] [PubMed]
- Martínez-Sámano, J.; Torres-Montes de Oca, A.; Luqueño-Bocardo, O.I.; Torres-Durán, P.V.; Juárez-Oropeza, M.A. Spirulina maxima Decreases Endothelial Damage and Oxidative Stress Indicators in Patients with Systemic Arterial Hypertension: Results from Exploratory Controlled Clinical Trial. Mar. Drugs 2018, 16, 496. [Google Scholar] [CrossRef]
- Torres-Duran, P.V.; Ferreira-Hermosillo, A.; Juarez-Oropeza, M.A. Antihyperlipemic and antihypertensive effects of Spirulina maxima in an open sample of Mexican population: A preliminary report. Lipids Health Dis. 2007, 6, 33. [Google Scholar] [CrossRef]
- van den Driessche, J.J.; Plat, J.; Konings, M.C.; Mensink, R.P. Effects of spirulina and wakame consumption on intestinal cholesterol absorption and serum lipid concentrations in non-hypercholesterolemic adult men and women. Eur. J. Nutr. 2020, 59, 2229–2236. [Google Scholar] [CrossRef]
- Pan, H.; She, X.; Wu, H.; Ma, J.; Ren, D.; Lu, J. Long-term regulation of the local renin–angiotensin system in the myocardium of spontaneously hypertensive rats by feeding bioactive peptides derived from Spirulina platensis. J. Agric. Food Chem. 2015, 63, 7765–7774. [Google Scholar] [CrossRef]
- Suo, Q.; Yue, Y.; Wang, J.; Wu, N.; Geng, L.; Zhang, Q. Isolation, identification and in vivo antihypertensive effect of novel angiotensin I-converting enzyme (ACE) inhibitory peptides from Spirulina protein hydrolysate. Food Funct. 2022, 13, 9108–9118. [Google Scholar] [CrossRef]
- Arthur-Ataam, J.; Bideaux, P.; Charrabi, A.; Sicard, P.; Fromy, B.; Liu, K.; Eddahibi, S.; Pasqualin, C.; Jouy, N.; Richard, S. Dietary supplementation with silicon-enriched spirulina improves arterial remodeling and function in hypertensive rats. Nutrients 2019, 11, 2574. [Google Scholar] [CrossRef]
- Wang, Y.; Chang, C.-F.; Chou, J.; Chen, H.-L.; Deng, X.; Harvey, B.K.; Cadet, J.L.; Bickford, P.C. Dietary supplementation with blueberries, spinach, or spirulina reduces ischemic brain damage. Exp. Neurol. 2005, 193, 75–84. [Google Scholar] [CrossRef]
- Almeida, T.; Manfroi, G.; Silva, S.; Beggiora, P.; Schwingel, D.; Bertolin, T.E. Exploring the Neuroprotective Effects of Spirulina platensis: Insights Into Hemorrhagic Volume and Histological Outcomes. Cureus 2023, 15, e42078. [Google Scholar] [CrossRef]
- Lafarga, T.; Álvarez, C.; Hayes, M. Bioactive peptides derived from bovine and porcine co-products: A review. J. Food Biochem. 2017, 41, e12418. [Google Scholar] [CrossRef]
- Cao, S.; Wang, Y.; Hao, Y.; Zhang, W.; Zhou, G. Antihypertensive Effects in Vitro and in Vivo of Novel Angiotensin-Converting Enzyme Inhibitory Peptides from Bovine Bone Gelatin Hydrolysate. J. Agric. Food Chem. 2020, 68, 759–768. [Google Scholar] [CrossRef]
- Giani, J.F.; Veiras, L.C.; Shen, J.Z.Y.; Bernstein, E.A.; Cao, D.; Okwan-Duodu, D.; Khan, Z.; Gonzalez-Villalobos, R.A.; Bernstein, K.E. Novel roles of the renal angiotensin-converting enzyme. Mol. Cell. Endocrinol. 2021, 529, 111257. [Google Scholar] [CrossRef] [PubMed]
- He, Y.Y.; Li, T.T.; Chen, J.X.; She, X.X.; Ren, D.F.; Lu, J. Transport of ACE Inhibitory Peptides Ile-Gln-Pro and Val-Glu-Pro Derived from Spirulina platensis Across Caco-2 Monolayers. J. Food Sci. 2018, 83, 2586–2592. [Google Scholar] [CrossRef] [PubMed]
- Carrizzo, A.; Conte, G.M.; Sommella, E.; Damato, A.; Ambrosio, M.; Sala, M.; Scala, M.C.; Aquino, R.P.; De Lucia, M.; Madonna, M.; et al. Novel Potent Decameric Peptide of Spirulina platensis Reduces Blood Pressure Levels Through a PI3K/AKT/eNOS-Dependent Mechanism. Hypertension 2019, 73, 449–457. [Google Scholar] [CrossRef] [PubMed]
- Majewski, M.; Klett-Mingo, M.; Verdasco-Martin, C.M.; Otero, C.; Ferrer, M. Spirulina extract improves age-induced vascular dysfunction. Pharm. Biol. 2022, 60, 627–637. [Google Scholar] [CrossRef]
- Heo, S.Y.; Ko, S.C.; Kim, C.S.; Oh, G.W.; Ryu, B.; Qian, Z.J.; Kim, G.; Park, W.S.; Choi, I.W.; Phan, T.T.; et al. A heptameric peptide purified from Spirulina sp. gastrointestinal hydrolysate inhibits angiotensin I-converting enzyme- and angiotensin II-induced vascular dysfunction in human endothelial cells. Int. J. Mol. Med. 2017, 39, 1072–1082. [Google Scholar] [CrossRef]
- Haddad, J.A.; Haddad, A.N. The past decade in type 2 diabetes and future challenges. Hormones 2018, 17, 451–459. [Google Scholar] [CrossRef]
- Ha, H.; Kim, K.H. Pathogenesis of diabetic nephropathy: The role of oxidative stress and protein kinase C. Diabetes Res. Clin. Pract. 1999, 45, 147–151. [Google Scholar] [CrossRef]
- Hu, F.B. Globalization of diabetes: The role of diet, lifestyle, and genes. Diabetes Care 2011, 34, 1249–1257. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes, A. Standards of Medical Care in Diabetes-2019 Abridged for Primary Care Providers. Clin. Diabetes 2019, 37, 11–34. [Google Scholar] [CrossRef] [PubMed]
- Wulffele, M.G.; Kooy, A.; de Zeeuw, D.; Stehouwer, C.D.; Gansevoort, R.T. The effect of metformin on blood pressure, plasma cholesterol and triglycerides in type 2 diabetes mellitus: A systematic review. J. Intern. Med. 2004, 256, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Saluja, M.; Pareek, K.K.; Swami, Y.K. Study of Diversity of Metformin Related Gastrointestinal Side Effects. J. Assoc. Physicians India 2020, 68, 36–38. [Google Scholar] [PubMed]
- Sivaraman, S.; Weickert, M.O. Nutrition and exercise in the treatment of type 2 diabetes mellitus. Hamdan Med. J. 2012, 5, 131–144. [Google Scholar] [CrossRef]
- Meng, X.; Li, Q.; Shi, R.; Chang, J.; Chang, H.; Li, M. Food supplements could be an effective improvement of diabetes mellitus: A review. J. Future Foods 2021, 1, 67–81. [Google Scholar] [CrossRef]
- Ray, K.K.; Seshasai, S.R.; Wijesuriya, S.; Sivakumaran, R.; Nethercott, S.; Preiss, D.; Erqou, S.; Sattar, N. Effect of intensive control of glucose on cardiovascular outcomes and death in patients with diabetes mellitus: A meta-analysis of randomised controlled trials. Lancet 2009, 373, 1765–1772. [Google Scholar] [CrossRef] [PubMed]
- Karizi, S.R.; Armanmehr, F.; Azadi, H.G.; Zahroodi, H.S.; Ghalibaf, A.M.; Bazzaz, B.S.F.; Abbaspour, M.; Boskabadi, J.; Eslami, S.; Taherzadeh, Z. A randomized, double-blind placebo-controlled add-on trial to assess the efficacy, safety, and anti-atherogenic effect of spirulina platensis in patients with inadequately controlled type 2 diabetes mellitus. Phytother. Res. 2023, 37, 1435–1448. [Google Scholar] [CrossRef]
- Alam, A.; Ma, S.; Quamri, A.; Fatima, S.; Roqaiya, M.; Ahmad, Z. Efficacy of Spirulina (Tahlab) in Patients of Type 2 Diabetes Mellitus (Ziabetus Shakri)—A Randomized Controlled Trial. J. Diabetes Metab. 2016, 7, 1–5. [Google Scholar] [CrossRef]
- Sowjanya, M.; Manjula, K. Effect of Food-based Approach with Spirulina on Blood Glucose Profile of Non-insulin Dependent Diabetics. Asian Pac. J. Health Sci. 2022. [Google Scholar] [CrossRef]
- Parikh, P.; Mani, U.V.; Iyer, U.M. Role of Spirulina in the Control of Glycemia and Lipidemia in Type 2 Diabetes Mellitus. J. Med. Food 2001, 4, 193–199. [Google Scholar] [CrossRef]
- Beihaghi, M.; Ghodrati Azadi, H.; Taherzadeh, Z.; Bahrami, H.R. The effects of oral administration of spirulina platensis (cultured iranian) on blood glucose and glycosylated hemoglobin blood in type ii diabetes mellitus patients. Iran. J. Diabetes Lipid Disord. 2017, 16, 183–190. [Google Scholar]
- Mazokopakis, E.E.; Papadomanolaki, M.G.; Fousteris, A.A.; Kotsiris, D.A.; Lampadakis, I.M.; Ganotakis, E.S. The hepatoprotective and hypolipidemic effects of Spirulina (Arthrospira platensis) supplementation in a Cretan population with non-alcoholic fatty liver disease: A prospective pilot study. Ann. Gastroenterol. Q. Publ. Hell. Soc. Gastroenterol. 2014, 27, 387–394. [Google Scholar]
- Layam, A.; Reddy, C.K. Antidiabetic property of spirulina. Diabetol. Croat. 2006, 35, 29–33. [Google Scholar]
- El-Moataaz, S.; Ismael, H.; Abo-Rhyem, S.M. Assessment of Chemical Composition of Spirulina Platensis and its Effect on Fasting Blood Glucose and Lipid Profile in Diabetic Rats. J. High Inst. Public Health 2019, 49, 199–211. [Google Scholar] [CrossRef]
- El-Sayed, E.-S.M.; Hikal, M.S.; Khair, B.E.A.E.; El-Ghobashy, R.E.; El-Assar, A.M. Hypoglycemic and hypolipidemic effects of spirulina platensis, phycocyanin, phycocyanopeptide and phycocyanobilin on male diabetic rats. Arab Univ. J. Agric. Sci. 2018, 26, 1121–1134. [Google Scholar] [CrossRef]
- Hannan, J.M.A.; Ansari, P.; Azam, S.; Flatt, P.R.; Abdel Wahab, Y.H.A. Effects of Spirulina platensis on insulin secretion, dipeptidyl peptidase IV activity and both carbohydrate digestion and absorption indicate potential as an adjunctive therapy for diabetes. Br. J. Nutr. 2020, 124, 1021–1034. [Google Scholar] [CrossRef]
- Hu, S.; Fan, X.; Qi, P.; Zhang, X. Identification of anti-diabetes peptides from Spirulina platensis. J. Funct. Foods 2019, 56, 333–341. [Google Scholar] [CrossRef]
- Yamina, M.; Oumelkheir, S.; Ismail, M. Effect of Adding the Spirulina (Arthrospira platensis), to Date Syrup on Glycemic Response and its Effectiveness to Reduce Post Prandial Blood Glucose. Int. J. Sci. Res. 2015, 4, 837–840. [Google Scholar]
- Hozayen, W.G.; Mahmoud, A.M.; Soliman, H.A.; Mostafa, S.R. Spirulina versicolor improves insulin sensitivity and attenuates hyperglycemia-mediated oxidative stress in fructose-fed rats. J. Intercult. Ethnopharmacol. 2016, 5, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Brito, A.D.F.; Silva, A.S.; de Oliveira, C.V.C.; de Souza, A.A.; Ferreira, P.B.; de Souza, I.L.L.; da Cunha Araujo, L.C.; da Silva Félix, G.; de Souza Sampaio, R.; Tavares, R.L.; et al. Spirulina platensis prevents oxidative stress and inflammation promoted by strength training in rats: Dose-response relation study. Sci. Rep. 2020, 10, 6382. [Google Scholar] [CrossRef] [PubMed]
- Sadek, K.M.; Lebda, M.A.; Nasr, S.M.; Shoukry, M. Spirulina platensis prevents hyperglycemia in rats by modulating gluconeogenesis and apoptosis via modification of oxidative stress and MAPK-pathways. Biomed. Pharmacother. 2017, 92, 1085–1094. [Google Scholar] [CrossRef] [PubMed]
- Grundy, S.M.; Stone, N.J.; Bailey, A.L.; Beam, C.T.; Birtcher, K.; Blumenthal, R.S.; Braun, L.; de Ferranti, S.D.; Faiella-Tommasino, J.; Forman, D.E.; et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2019, 73, 3168–3209. [Google Scholar] [CrossRef] [PubMed]
- Ference, B.A.; Ginsberg, H.N.; Graham, I.M.; Ray, K.K.; Packard, C.J.; Bruckert, E.; Hegele, R.A.; Krauss, R.M.; Raal, F.J.; Schunkert, H.; et al. Low-density lipoproteins cause atherosclerotic cardiovascular disease. 1. Evidence from genetic, epidemiologic, and clinical studies. A consensus statement from the European Atherosclerosis Society Consensus Panel. Eur. Heart J. 2017, 38, 2459–2472. [Google Scholar] [CrossRef] [PubMed]
- Thompson, P.D.; Clarkson, P.; Karas, R.H. Statin-associated myopathy. JAMA 2003, 289, 1681–1690. [Google Scholar] [CrossRef] [PubMed]
- Serban, M.-C.; Sahebkar, A.; Dragan, S.R.; Stoichescu-Hogea, G.; Ursoniu, S.; Andrica, F.; Banach, M. A systematic review and meta-analysis of the impact of Spirulina supplementation on plasma lipid concentrations. Clin. Nutr. 2016, 35, 842–851. [Google Scholar] [CrossRef]
- Zeinalian, R.; Farhangi, M.A.; Shariat, A.; Saghafi-Asl, M. The effects of Spirulina Platensis on anthropometric indices, appetite, lipid profile and serum vascular endothelial growth factor (VEGF) in obese individuals: A randomized double blinded placebo controlled trial. BMC Complement. Altern. Med. 2017, 17, 225. [Google Scholar] [CrossRef]
- Szulińska, M.; Gibas-Dorna, M.; Miller-Kasprzak, E.; Suliburska, J.; Miczke, A.; Walczak-Gałęzewska, M.; Stelmach-Mardas, M.; Walkowiak, J.; Bogdański, P. Spirulina maxima improves insulin sensitivity, lipid profile, and total antioxidant status in obese patients with well-treated hypertension: A randomized double-blind placebo-controlled study. Eur. Rev. Med. Pharmacol. Sci. 2017, 21, 2473–2481. [Google Scholar]
- Hernández-Lepe, M.A.; Wall-Medrano, A.; López-Díaz, J.A.; Juárez-Oropeza, M.A.; Hernández-Torres, R.P.; Ramos-Jiménez, A. Hypolipidemic Effect of Arthrospira (Spirulina) maxima Supplementation and a Systematic Physical Exercise Program in Overweight and Obese Men: A Double-Blind, Randomized, and Crossover Controlled Trial. Mar. Drugs 2019, 17, 270. [Google Scholar] [CrossRef]
- Golestani, F.; Mogharnasi, M.; Erfani-Far, M.; Abtahi-Eivari, S.H. The effects of spirulina under high-intensity interval training on levels of nesfatin-1, omentin-1, and lipid profiles in overweight and obese females: A randomized, controlled, single-blind trial. J. Res. Med. Sci. Off. J. Isfahan Univ. Med. Sci. 2021, 26, 10. [Google Scholar]
- Mazokopakis, E.E.; Starakis, I.K.; Papadomanolaki, M.G.; Mavroeidi, N.G.; Ganotakis, E.S. The hypolipidaemic effects of Spirulina (Arthrospira platensis) supplementation in a Cretan population: A prospective study. J. Sci. Food Agric. 2014, 94, 432–437. [Google Scholar] [CrossRef] [PubMed]
- Mazloomi, S.M.; Samadi, M.T.; Davarpanah, H.; Babajafari, S.; Clark, C.C.T.; Ghaemfar, Z.; Rezaiyan, M.; Mosallanezhad, A.; Shafiee, M.; Rostami, H. The effect of Spirulina sauce, as a functional food, on cardiometabolic risk factors, oxidative stress biomarkers, glycemic profile, and liver enzymes in nonalcoholic fatty liver disease patients: A randomized double-blinded clinical trial. Food Sci. Nutr. 2021, 10, 317–328. [Google Scholar] [CrossRef]
- Koite, N.; Sanogo, N.G.I.; Lépine, O.; Bard, J.M.; Ouguerram, K. Antioxidant Efficacy of a Spirulina Liquid Extract on Oxidative Stress Status and Metabolic Disturbances in Subjects with Metabolic Syndrome. Mar. Drugs 2022, 20, 441. [Google Scholar] [CrossRef]
- Nasirian, F.; Dadkhah, M.; Moradi-kor, N.; Obeidavi, Z. Effects of Spirulina platensis microalgae on antioxidant and anti-inflammatory factors in diabetic rats. Diabetes Metab. Syndr. Obes. Targets Ther. 2018, 11, 375–380. [Google Scholar] [CrossRef]
- Nagaoka, S.; Shimizu, K.; Kaneko, H.; Shibayama, F.; Morikawa, K.; Kanamaru, Y.; Otsuka, A.; Hirahashi, T.; Kato, T. A novel protein C-phycocyanin plays a crucial role in the hypocholesterolemic action of Spirulina platensis concentrate in rats. J. Nutr. 2005, 135, 2425–2430. [Google Scholar] [CrossRef] [PubMed]
- Kata, F.S.; Athbi, A.M.; Manwar, E.Q.; Al-Ashoor, A.; Abdel-Daim, M.M.; Aleya, L. Therapeutic effect of the alkaloid extract of the cyanobacterium Spirulina platensis on the lipid profile of hypercholesterolemic male rabbits. Environ. Sci. Pollut. Res. 2018, 25, 19635–19642. [Google Scholar] [CrossRef]
- Sengupta, S.; Koley, H.; Dutta, S.; Bhowal, J. Hypocholesterolemic effect of Spirulina platensis (SP) fortified functional soy yogurts on diet-induced hypercholesterolemia. J. Funct. Foods 2018, 48, 54–64. [Google Scholar] [CrossRef]
- Li, T.-T.; Huang, Z.-R.; Jia, R.-B.; Lv, X.-C.; Zhao, C.; Liu, B. Spirulina platensis polysaccharides attenuate lipid and carbohydrate metabolism disorder in high-sucrose and high-fat diet-fed rats in association with intestinal microbiota. Food Res. Int. 2021, 147, 110530. [Google Scholar] [CrossRef]
- Hua, P.; Yu, Z.; Xiong, Y.; Liu, B.; Zhao, L.-N. Regulatory Efficacy of Spirulina platensis Protease Hydrolyzate on Lipid Metabolism and Gut Microbiota in High-Fat Diet-Fed Rats. Int. J. Mol. Sci. 2018, 19, 4023. [Google Scholar] [CrossRef]
- Oriquat, G.A.; Ali, M.A.; Mahmoud, S.A.; Eid, R.S.M.; Hassan, R.; Kamel, M.A. Improving hepatic mitochondrial biogenesis as a postulated mechanism for the antidiabetic effect of Spirulina platensis in comparison with metformin. Appl. Physiol. Nutr. Metab. 2019, 44, 357–364. [Google Scholar] [CrossRef]
- Ama Moor, V.J.; Nya Biapa, P.C.; Nono Njinkio, B.L.; Moukette Moukette, B.; Sando, Z.; Kenfack, C.A.; Ateba, B.A.; Ngo Matip, M.E.; Pieme, C.A.; Ngogang, J.Y. Hypolipidemic effect and activation of Lecithin Cholesterol Acyl Transferase (LCAT) by aqueous extract of Spirulina platensis during toxicological investigation. BMC Nutr. 2017, 3, 25. [Google Scholar] [CrossRef]
- Iwata, K.; Inayama, T.; Kato, T. Effects of Spirulina platensis on plasma lipoprotein lipase activity in fructose-induced hyperlipidemic rats. J. Nutr. Sci. Vitaminol. 1990, 36, 165–171. [Google Scholar] [CrossRef]
- Oriquat, G.A. Therapeutic effects of Spirulina against experimentally-induced non-alcoholic fatty liver in rats may involve miR-21, -34a and -122. Meta Gene 2018, 18, 115–121. [Google Scholar] [CrossRef]
- Han, L.-K.; Li, D.-X.; Xiang, L.; Gong, X.J.; Kondo, Y.; Suzuki, I.; Okuda, H. Isolation of pancreatic lipase activity-inhibitory component of spirulina platensis and it reduce postprandial triacylglycerolemia. Yakugaku Zasshi J. Pharm. Soc. Jpn. 2006, 126, 43–49. [Google Scholar] [CrossRef] [PubMed]
- Ma, P.; Huang, R.; Jiang, J.; Ding, Y.; Li, T.; Ou, Y. Potential use of C-phycocyanin in non-alcoholic fatty liver disease. Biochem. Biophys. Res. Commun. 2020, 526, 906–912. [Google Scholar] [CrossRef] [PubMed]
- Riss, J.; Décordé, K.; Sutra, T.; Delage, M.; Baccou, J.C.; Jouy, N.; Brune, J.-P.; Oréal, H.; Cristol, J.-P.; Rouanet, J.M. Phycobiliprotein C-phycocyanin from Spirulina platensis is powerfully responsible for reducing oxidative stress and NADPH oxidase expression induced by an atherogenic diet in hamsters. J. Agric. Food Chem. 2007, 55, 7962–7967. [Google Scholar] [CrossRef] [PubMed]
- Strasky, Z.; Zemánková, L.; Němečková, I.; Rathouská, J.; Wong, R.J.; Muchová, L.; Subhanová, I.; Vaníková, J.; Vanova, K.H.; Vítek, L.; et al. Spirulina platensis and phycocyanobilin activate atheroprotective heme oxygenase-1: A possible implication for atherogenesis. Food Funct. 2013, 4, 1586–1594. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| References | Patients’ Cohort | Dose of Spirulina | Duration Treatment (Weeks/Months) | Outcomes in Spirulina Group; (p-Value) | Outcomes in Control Group; (p-Value) | p-Value |
|---|---|---|---|---|---|---|
| SBP (mmHg) | SBP (mmHg) | |||||
| Baseline 144.72 ± 2.98 | Baseline 140.59 ± 3.81 | 0.39 | ||||
| End 138.46 ± 2.98 | End 141.07 ± 3.22 | 0.55 | ||||
| Ghaem Far et al., 2021 [39] | Spirulina group; | 2 g/day | 8 weeks | p = 0.02 | p = 0.89 | |
| Placebo group | DBP (mmHg) | DBP (mmHg) | ||||
| Baseline 96.60 ± 1.76 | Baseline 90.94 ± 3.6 | 0.17 | ||||
| End 92.58 ± 2.21 | End 89.70 ± 2.98 | 0.43 | ||||
| p = 0.03 | p = 0.61 | |||||
| SBP (mmHg) | SBP (mmHg) | |||||
| Baseline 149 ± 7 | Baseline 150 ± 7 | 0.36 | ||||
| End 143 ± 9 | End 151 ± 9 | <0.001 | ||||
| Miczke et al., 2016 [40] | Spirulina group; | 2 g/day | 3 months | p = 0.0023 | p = 0.38 | |
| Placebo group | DBP (mmHg) | DBP (mmHg) | ||||
| Baseline 84 ± 9 | Baseline 85 ± 9 | 0.81 | ||||
| End 79 ± 9 | End 86 ± 7 | <0.001 | ||||
| p = 0.057 | p = 0.19 | |||||
| SBP (mmHg) | SBP (mmHg) | |||||
| Baseline 140.38 ± 9.04 | Baseline 140.75 ± 7.03 | n.s | ||||
| End 126.50 ± 5.53 | End 140± 6.05 | p < 0.05 | ||||
| Martínez-Sámano et al., 2018 [41] | Spirulina group; | 4.5 g/day | 12 weeks | p < 0.05 | n.s | |
| Placebo group | DBP (mmHg) | DBP (mmHg) | ||||
| Baseline 83.75 ± 5.31 | Baseline 84.25 ± 5.28 | n.s | ||||
| End NA | End NA | n.s | ||||
| n.s | n.s | |||||
| SBP (mmHg) | ||||||
| Baseline 120 ± 9 | ||||||
| End 109 ± 9 | ||||||
| Torres-Duran et al., 2007 [42] | Spirulina group | 4.5 g/day | 6 weeks | p < 0.001 | NA | |
| DBP (mmHg) | ||||||
| Baseline 85 ± 9 | ||||||
| End 79 ± 8 | ||||||
| p < 0.05 | ||||||
| SBP (mmHg) | SBP (mmHg) | |||||
| Baseline − | Baseline − | n.s | ||||
| End 113.9 ± 13.7 | End 114.4 ± 14.5 | n.s | ||||
| van den Driessche et al., 2020 [43] | Spirulina group; | 4.8 g/day | 17 days | n.s | n.s | |
| Placebo group | DBP (mmHg) | DBP (mmHg) | ||||
| Baseline − | Baseline − | n.s | ||||
| End 75.4 ± 9.4 | End 74.9 ± 9.5 | n.s | ||||
| n.s | n.s |
| References | Patients’ Cohort | Dose of Spirulina | Duration Treatment (Weeks/Months) | Outcomes in Spirulina Group; (p-Value) | Outcomes in Control Group; (p-Value) | p-Value |
|---|---|---|---|---|---|---|
| HbA1c (mg/dL) | HbA1c (mg/dL) | |||||
| Baseline 8.87 ± 0.29 | Baseline 8.47 ± 0.21 | 0.65 | ||||
| End 7.44 ± 0.20 | End 8.15 ± 0.17 | NA | ||||
| Karizi et al., 2022 [65] | Spirulina + Metformin group; | 2 g/day | 3 months | p = 0.001 | p = 0.016 | |
| Placebo + Metformin group | FBS (mg/dL) | FBS (mg/dL) | ||||
| Baseline 167.30 ± 4.34 | Baseline 227.60 ± 67.85 | 0.47 | ||||
| End 136.33 ± 4.42 | End 165.47 ± 3.37 | NA | ||||
| p = 0.001 | p = 0.99 | |||||
| HbA1c (mg/dL) | HbA1c (mg/dL) | |||||
| Baseline 9.73 ± 1.92 | Baseline 9.61 ± 1.49 | 0.862 | ||||
| End 9.95 ± 2.11 | End 9.15 ± 2.03 | 0.303 | ||||
| p = 0.525 | p = 0.459 | |||||
| FBS (mg/dL) | FBS (mg/dL) | |||||
| Alam et al., 2016 [66] | Spirulina group; | 7 g/day | 45 days | Baseline 245.53 ± 78.95 | Baseline 227.60 ± 67.85 | 0.525 |
| Placebo + Metformin group | End 204.87 ± 78.15 | End 191.80 ± 78.91 | 0.65 | |||
| p = 0.003 | p = 0.212 | |||||
| PPBS (mg/dL) | PPBS (mg/dL) | |||||
| Baseline 345.73 ± 98.33 | Baseline 329.60 ± 72.92 | NA | ||||
| End 303.67 ± 96.16 | End 282.80 ± 99.90 | NA | ||||
| NA | NA | |||||
| HbA1c (mg/dL) | HbA1c (mg/dL) | |||||
| Baseline EG-I M 9.19 ± 0.88; W 8.88 ± 0.70 EG-II M 7.33 ± 0.54; W 7.20 ± 0.33 | Baseline M 8.00 ± 1.05; W 8.64 ± 0.79 | NA | ||||
| End EG-I M 7.11 ± 0.64; W 7.64 ± 0.48 EG-II M 6.48 ± 0.36; W 6.58 ± 0.35 | End M 7.98 ± 1.03; W 8.62 ± 0.74 | NA | ||||
| EG-I M p < 0.01; W p < 0.01 EG-II M p < 0.01 W p < 0.01 | M n.s; W n.s | |||||
| EG1 group; | FBS (mg/dL) | FBS (mg/dL) | ||||
| Sowjanya et al., 2022 [67] | EG2 group | 2 g/day | 3 months | Baseline EG-I M 138.00 ± 18.39; W 128.08 ± 11.76 EG-II M 135.02 ± 18.22; W 132.33 ± 10.89 | Baseline M 146.10 ± 25.29; W 135.12 ± 10.27 | NA |
| Control group | End EG-I M 122.21 ± 14.48; W 111.00 ± 14.48 EG-II M 119.31 ± 14.33; W 123.12 ± 9.81 | End M 141.43 ± 20.84; W 130.12 ± 9.76 | ||||
| EG-I M p < 0.01; W p < 0.01 EG-II M p < 0.01; W p < 0.05 | M n.s; W n.s | NA | ||||
| PPBS (mg/dL) | PPBS (mg/dL) | |||||
| Baseline EG-I M 210.33 ± 28.99; W 212.12 ± 39.45 EG-II M 197.45 ± 23.31 W 190.03 ± 14.86 | Baseline M 206.17 ± 22.83; W 179.24 ± 17.82 | NA | ||||
| End EG-I M 165.56 ± 25.35; W 175.58 ± 32.11 EG-II M 171.28 ± 24.77 W 175.50 ± 18.38 | End M 202.37 ± 22.76; W 172.09 ± 15.49 | NA | ||||
| EG-I M p < 0.01; W p < 0.01 EG-II M p < 0.01; W p < 0.05 | M n.s; W n.s | |||||
| HbA1c (mg/dL) | HbA1c (mg/dL) | |||||
| Baseline 9.0 ± 2.3 | Baseline 8.7 ± 1.5 | NA | ||||
| End 8.0 ± 1.3 | End 8.7 ± 1.3 | NA | ||||
| p < 0.05 | n.s | |||||
| FBS (mg/dL) | FBS (mg/dL) | |||||
| Baseline 161.7 ± 48.6 | Baseline 164.3 ± 59.4 | NA | ||||
| Parikh et al., 2001 [68] | Spirulina group; | 2 g/day | 2 months | End 142.4 ± 27.4 | End 165.1 ± 44.3 | NA |
| Control group | NA | NA | ||||
| PPBS (mg/dL) | PPBS (mg/dL) | |||||
| Baseline 264.9 6 65.2 | Baseline 215.2 6 67.3 | NA | ||||
| End 248.8 6 68.9 | End 212.3 6 57.6 | NA | ||||
| NA | NA | |||||
| FBS (mg/dL) | ||||||
| Beihaghi et al., 2017 [69] | Spirulina group; | 8 g/day | 3 months | Baseline 158.1 ± 44.2 | NA | |
| Control group | End 127.8 ± 36.7 | |||||
| NA |
| References | Patients’ Cohort | Dose of Spirulina | Duration Treatment (Weeks/Months) | Outcomes in Spirulina Group; (p-Value) | Outcomes in Control Group; (p-Value) | p-Value |
|---|---|---|---|---|---|---|
| TG (mg/dL) | TG (mg/dL) | |||||
| Baseline 144.13 ± 57.57 | Baseline 156.14 ± 79.01 | 0.486 | ||||
| End 136.65 ± 60.80 | End 140.88 ± 72.73 | NA | ||||
| p = 0.365 | p = 0.052 | |||||
| LDL-C (mg/dL) | LDL-C (mg/dL) | |||||
| Baseline 116.27 ± 34.79 | Baseline 119.90 ± 21.69 | 0.725 | ||||
| End 115.42 ± 28.61 | End 116.68 ± 21.31 | NA | ||||
| Zeinalian et al., 2017 [84] | Spirulina group; | 1 g/day | 12 weeks | p = 0.886 | p = 0.196 | |
| Control group | HDL-C (mg/dL) | HDL-C (mg/dL) | ||||
| Baseline 36.55 ± 10.21 | Baseline 34.88 ± 11.56 | 0.385 | ||||
| End 38.75 ± 8.84 | End 38.37 ± 9.44 | NA | ||||
| p = 0.05 | p = 0.001 | |||||
| TC (mg/dL) | TC (mg/dL) | |||||
| Baseline 190.48 ± 35.25 | Baseline 187.25 ± 27.10 | 0.123 | ||||
| End 180.10 ± 31.13 | End 183.03 ± 28.07 | NA | ||||
| p = 0.002 | p = 0.09 | |||||
| TG (mmol/L) | TG (mmol/L) | |||||
| Baseline 1.9 ± 1.0 | Baseline 2.0 ± 1.2 | 0.334 | ||||
| End 1.8 ± 0.9 | End 2.1 ± 1.1 | 0.224 | ||||
| p = 0.633 | p = 0.981 | |||||
| LDL-C(mmol/L) | LDL-C (mmol/L) | 0.412 | ||||
| Baseline 3.5 ± 0.9 | Baseline 3.6 ±0.9 | <0.001 | ||||
| End 3.0 ± 0.6 | End 3.6 ± 0.9 | |||||
| Szulinska et al., 2017 [85] | Spirulina group; | 2 g/day | 3 months | p < 0.001 | p = 0.223 | |
| Placebo group | HDL-C (mmol/L) | HDL-C (mmol/L) | ||||
| Baseline 1.4 ± 0.3 | Baseline 1.3 ± 0.4 | 0.357 | ||||
| End 1.4 ± 0.3 | End 1.2 ± 0.3 | 0.002 | ||||
| p = 0.227 | p = 0.204 | |||||
| TC (mmol/L) | TC (mmol/L) | |||||
| Baseline 5.5 ± 1.1 | Baseline 5.2± 0.9 | 0.191 | ||||
| End 5.2± 0.9 | End 5.4± 0.8 | 0.150 | ||||
| p < 0.001 | p = 0.306 | |||||
| TG (mg/dL) | TG (mg/dL) | |||||
| Baseline Sp 167 ± 11 Sp + exercise 184 ± 40 | Baseline Placebo 160 ± 6. Placebo + exercise 180 ± 25 | NA | ||||
| End Sp 148 ± 19 Sp + exercise 156 ± 29 | End Placebo 153 ± 12 Placebo + exercise 164 ± 21 | NA | ||||
| Spirulina group; | Sp p < 0.05 Sp + exercise p < 0.05 | Placebo p = 0.156 Placebo + exercise p = 0.096 | ||||
| Spirulina + exercise group; | LDL-C (mg/dL) | LDL-C (mg/dL) | ||||
| Hernández-Lepe et al., 2019 [86] | Control group; | 4.5 g/day | 6 weeks | Baseline Sp 148 ± 33 Sp + exercise 141 ± 29 | Baseline Placebo 140 ± 29 Placebo + exercise 148 ± 33 | NA |
| Control + exercise group | End Sp 128 ± 32 Sp + exercise 101 ± 34 | End Placebo 135 ± 27 Placebo + exercise 124 ± 33 | NA | |||
| Sp p = 0.060 Sp + exercise p < 0.05 | Placebo p = 0.650 Placebo + exercise p < 0.05 | |||||
| HDL-C (mg/dL) | HDL-C (mg/dL) | |||||
| Baseline Sp 29 ± 6 Sp + exercise 30 ± 6 | Baseline Placebo 28 ± 8 Placebo + exercise 28 ± 6 | NA | ||||
| End Sp 35 ± 10 Sp + exercise 40 ± 10 | End Placebo 31 ± 5 Placebo + exercise 33 ± 6 | NA | ||||
| Sp p < 0.05 Sp + exercise p < 0.05 | Placebo p = 0.172 Placebo + exercise p < 0.05 | |||||
| TC (mg/dL) | TC (mg/dL) | |||||
| Baseline Sp 233 ± 21 Sp + exercise 226 ± 22 | Baseline Placebo 219 ± 16 Placebo + exercise 232 ± 23 | NA | ||||
| End Sp 212 ± 23 Sp + exercise 189 ± 20 | End Placebo 213 ± 18 Placebo + exercise 208 ± 28 | NA | ||||
| Sp p < 0.05 Sp + exercise p < 0.05 | Placebo p = 0.412 Placebo + exercise p < 0.05 | |||||
| TG (mg/dL) | TG (mg/dL) | |||||
| Baseline 94.09 ± 61.44 | Baseline 86.57 ± 33.26 | NA | ||||
| End 93.82 ± 55.29 | End 74.76 ± 18.41 | NA | ||||
| HIIT+ Spirulina group; | p = 0.97 | p = 0.22 | ||||
| Golestani et al., 2021 [87] | HIIT+ Placebo group | 1 g/day | 4 weeks | LDL-C (mg/dL) | LDL-C (mg/dL) | |
| Baseline 132.43 ± 19.80 | Baseline 130.93 ± 17.23 | NA | ||||
| End 125.32 ± 30.59 | End 123.04 ± 10.90 | NA | ||||
| p = 0.37 | p = 0.21 | |||||
| HDL-C (mg/dL) | HDL-C (mg/dL) | |||||
| Baseline 54.23 ± 6.97 | Baseline 59.49 ± 3.85 | |||||
| End 57.62 ± 5.18 | End 60.37 ± 5.39 | |||||
| p = 0.15 | p = 0.65 | |||||
| TC (mg/dL) | TC (mg/dL) | |||||
| Baseline 167.35 ± 39.48 | Baseline 170.81 ± 26.62 | NA | ||||
| End 163.24 ± 38.85 | End 159.13 ± 23.85 | NA | ||||
| p = 0.69 | p = 0.14 | |||||
| TG (mg/dL) | TG (mg/dL) | |||||
| Baseline 184 ± 12.9 | Baseline 181 ± 11.7 | 0.96 | ||||
| End 113.63 ± 40.56 | End 180.37 ± 63.76 | NA | ||||
| p = 0.001 | p = 0.001 | |||||
| LDL-C (mg/dL) | LDL-C (mg/dL) | |||||
| Baseline 112 ± 9.12 | Baseline 110 ± 8.6 | 0.87 | ||||
| End 73.47 ± 37.4 | End 110.97 ± 47.54 | NA | ||||
| Karizi et al., 2022 [65] | Spirulina + Metformin group; | 2 g/day | 3 months | p = 0.001 | p = 0.001 | |
| Placebo + Metformin group | HDL-C (mg/dL) | HDL-C (mg/dL) | ||||
| Baseline 42 ± 1.3 | Baseline 42 ± 1.3 | 0.78 | ||||
| End 45.1 ± 6.83 | End 40.5 ± 6.25 | NA | ||||
| p = 0.001 | p = 0.001 | |||||
| TC (mg/dL) | TC (mg/dl) | |||||
| Baseline 190 ± 8.8 | Baseline 186 ± 8.0 | 0.78 | ||||
| End 149.07 ± 40.02 | End 187.63 ± 43.39 | NA | ||||
| p = 0.001 | p = 0.001 | |||||
| TG (mg/dL) | ||||||
| Baseline 184.8 ± 16.8 | ||||||
| End 138.9 ± 23.8 | ||||||
| p < 0.0001 | ||||||
| LDL-C (mg/dL) | ||||||
| Baseline 200.6 ± 27.6 | ||||||
| Mazokopakis et al., 2014 [88] | Spirulina group | 1 g/day | 3 months | End 183 ± 23.6 | NA | |
| p < 0.0001 | ||||||
| HDL-C (mg/dL) | ||||||
| Baseline 38 ± 6.9 | ||||||
| End 39.6 ± 6.3 | ||||||
| p = 0.0002 | ||||||
| TC (mg/dL) | ||||||
| Baseline 275.5 ± 29.9 | ||||||
| End 250.3 ± 26.7 | ||||||
| p < 0.0001 | ||||||
| TG (mg/dL) | TG (mg/dL) | |||||
| Baseline 195.77 ± 16.74 | Baseline 161.21 ± 15.26 | 0.07 | ||||
| End 175.13 ± 16.46 | End 155.42 ± 16.51 | 0.29 | ||||
| p = 0.01 | p = 0.44 | |||||
| LDL-C (mg/dL) | LDL-C (mg/dL) | |||||
| Baseline 108.22 ± 5.62 | Baseline 108.57 ± 5.61 | 0.96 | ||||
| End 106.13 ± 5.66 | End 113.63 ± 5.46 | 0.35 | ||||
| Ghaem Far et al., 2021 [39] | Spirulina group; | 2 g/day | 8 weeks | p = 0.55 | p = 0.28 | |
| Placebo group | HDL-C (mg/dL) | HDL-C (mg/dL) | ||||
| Baseline 38.59 ± 1.68 | Baseline 42.31 ± 2.22 | 0.18 | ||||
| End 39.81 ± 1.89 | End 41.57 ± 2.09 | 0.33 | ||||
| p = 0.17 | p = 0.38 | |||||
| TC (mg/dL) | TC (mg/dL) | |||||
| Baseline 187.00 ± 7.48 | Baseline 186.26 ± 7.8 | 0.94 | ||||
| End 183.68 ± 7.06 | End 190.57 ± 6.95 | 0.49 | ||||
| p = 0.47 | p = 0.51 | |||||
| TG (mg/dL) | TG (mg/dL) | |||||
| Baseline 165.30 ± 41.20 | Baseline 152.83 ± 21.12 | 0.20 | ||||
| End 138.65 ± 41.70 | End 164.89 ± 38.82 | |||||
| p = 0.03 | p = 0.05 | |||||
| LDL-C (mg/dL) | LDL-C (mg/dL) | |||||
| Baseline 126.96 ± 45.18 | Baseline 117.70 ± 40.62 | 0.46 | ||||
| End 116.60 ± 41.76 | End 123.53 ± 23.76 | |||||
| Mazloomi et al., 2021 [89] | Spirulina sauce group; | 2 g/day | 8 weeks | p = 0.11 | p = 0.71 | |
| Placebo group | HDL-C (mg/dL) | HDL-C (mg/dL) | ||||
| Baseline 42.43 ± 8.29 | Baseline 37.61 ± 11.27 | 0.10 | ||||
| End 46.40 ± 11.64 | End 38.58 ± 10.65 | |||||
| p = 0.02 | p = 0.86 | |||||
| TC (mg/dL) | TC (mg/dL) | |||||
| Baseline 202.48 ± 45 | Baseline 185.96 ± 39.90 | 0.19 | ||||
| End 186.75 ± 49.86 | End 195.11 ± 24.86 | |||||
| p = 0.14 | p = 0.42 | |||||
| TG (g/L) | TG (g/L) | |||||
| Baseline 1.35 ± 0.4 | Baseline 1.83 ± 0.82 | 0.11 | ||||
| End 1.23 ± 0.57 | End 1.97 ± 0.80 | 0.003 | ||||
| NA | NA | |||||
| LDL-C (g/L) | LDL-C (g/L) | |||||
| Baseline 1.52 ± 0.33 | Baseline 1.53 ± 0.36 | 0.88 | ||||
| End 1.49 ± 0.33 | End 1.43 ± 0.38 | 0.22 | ||||
| Koite et al., 2022 [90] | Spirulysat® group; | Arthrospira Liquid Extract | 12 weeks | NA | NA | |
| Placebo group | (Spirulysat®) | HDL-C (g/L) | HDL-C (g/L) | |||
| Baseline 0.54 ± 0.09 | Baseline 0.47 ± 0.13 | 0.004 | ||||
| End 0.55 ± 0.14 | End 0.48 ± 0.18 | 0.031 | ||||
| NA | NA | |||||
| TC (g/L) | TC (g/L) | |||||
| Baseline 2.33 ± 0.36 | Baseline 2.36 ± 0.46 | 0.96 | ||||
| End 2.30 ± 0.34 | End 2.31 ± 0.43 | 0.57 | ||||
| NA | NA | |||||
| TG (mmol/L) | TG (mmol/L) | |||||
| Baseline NA | Baseline NA | NA | ||||
| End 1.09 ± 0.63 | End 1.06 ± 0.61 | 0.684 | ||||
| NA | NA | |||||
| LDL-C (mmol/L) | LDL-C (mmol/L) | |||||
| Baseline NA | Baseline NA | NA | ||||
| End 2.75 ± 0.97 | End 2.77 ± 1.07 | 0.677 | ||||
| van den Driessche et al., 2020 [43] | Spirulina group; | 4.5 g/day | 17 days | NA | NA | |
| Placebo group | HDL-C (mmol/L) | HDL-C (mmol/L) | ||||
| Baseline NA | Baseline NA | NA | ||||
| End 1.52 ± 0.43 | End 1.56 ± 0.49 | 0.273 | ||||
| NA | NA | |||||
| TC (mmol/L) | TC (mmol/L) | |||||
| Baseline NA | Baseline NA | NA | ||||
| End 4.75 ± 1.00 | End 4.81 ± 1.09 | 0.443 | ||||
| NA | NA |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Prete, V.; Abate, A.C.; Di Pietro, P.; De Lucia, M.; Vecchione, C.; Carrizzo, A. Beneficial Effects of Spirulina Supplementation in the Management of Cardiovascular Diseases. Nutrients 2024, 16, 642. https://doi.org/10.3390/nu16050642
Prete V, Abate AC, Di Pietro P, De Lucia M, Vecchione C, Carrizzo A. Beneficial Effects of Spirulina Supplementation in the Management of Cardiovascular Diseases. Nutrients. 2024; 16(5):642. https://doi.org/10.3390/nu16050642
Chicago/Turabian StylePrete, Valeria, Angela Carmelita Abate, Paola Di Pietro, Massimiliano De Lucia, Carmine Vecchione, and Albino Carrizzo. 2024. "Beneficial Effects of Spirulina Supplementation in the Management of Cardiovascular Diseases" Nutrients 16, no. 5: 642. https://doi.org/10.3390/nu16050642
APA StylePrete, V., Abate, A. C., Di Pietro, P., De Lucia, M., Vecchione, C., & Carrizzo, A. (2024). Beneficial Effects of Spirulina Supplementation in the Management of Cardiovascular Diseases. Nutrients, 16(5), 642. https://doi.org/10.3390/nu16050642