
Dietary Patterns Associated with Breast Cancer in the Middle East: A Scoping Review

 and
and
Abstract
1. Introduction
2. Method
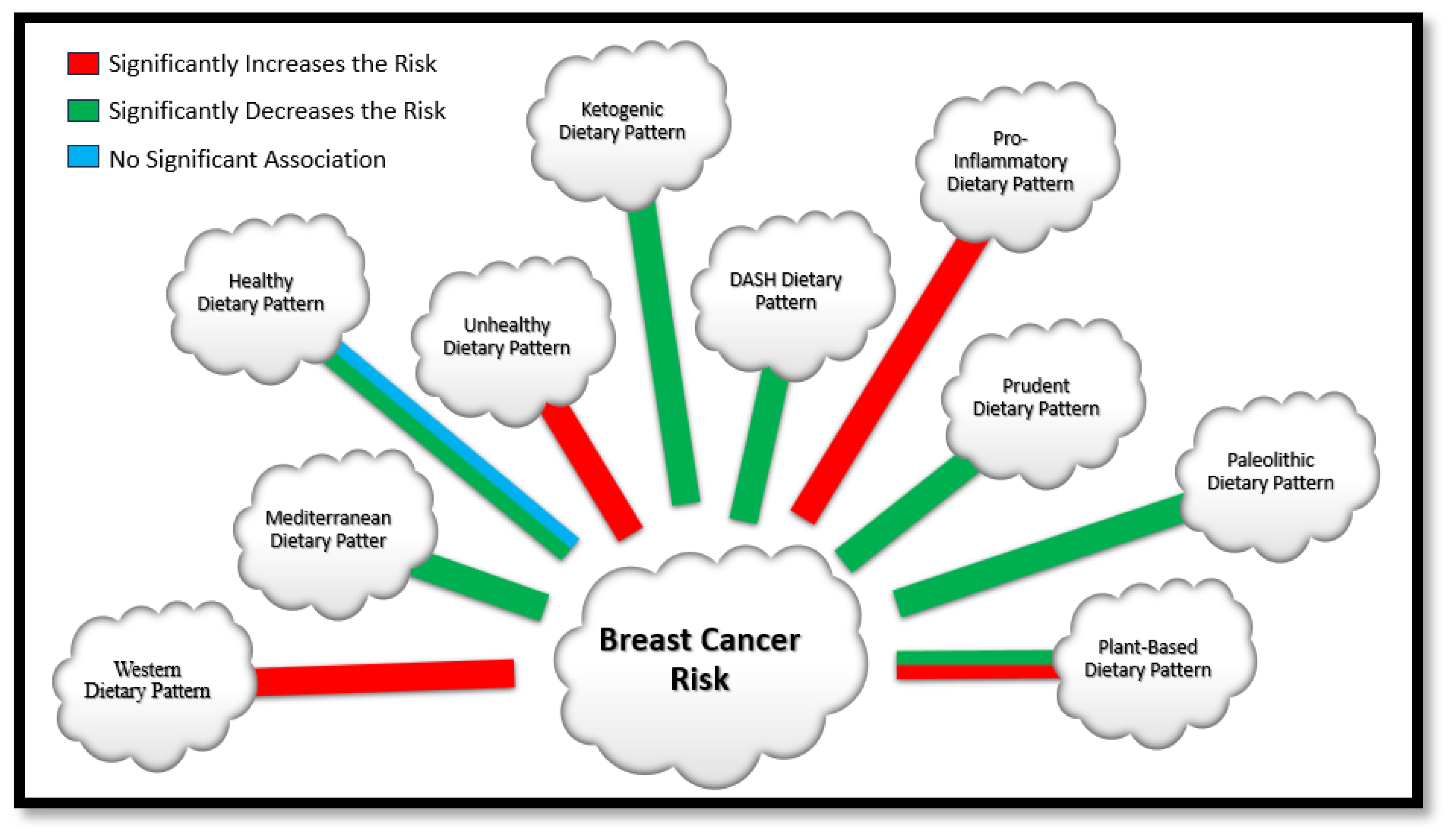
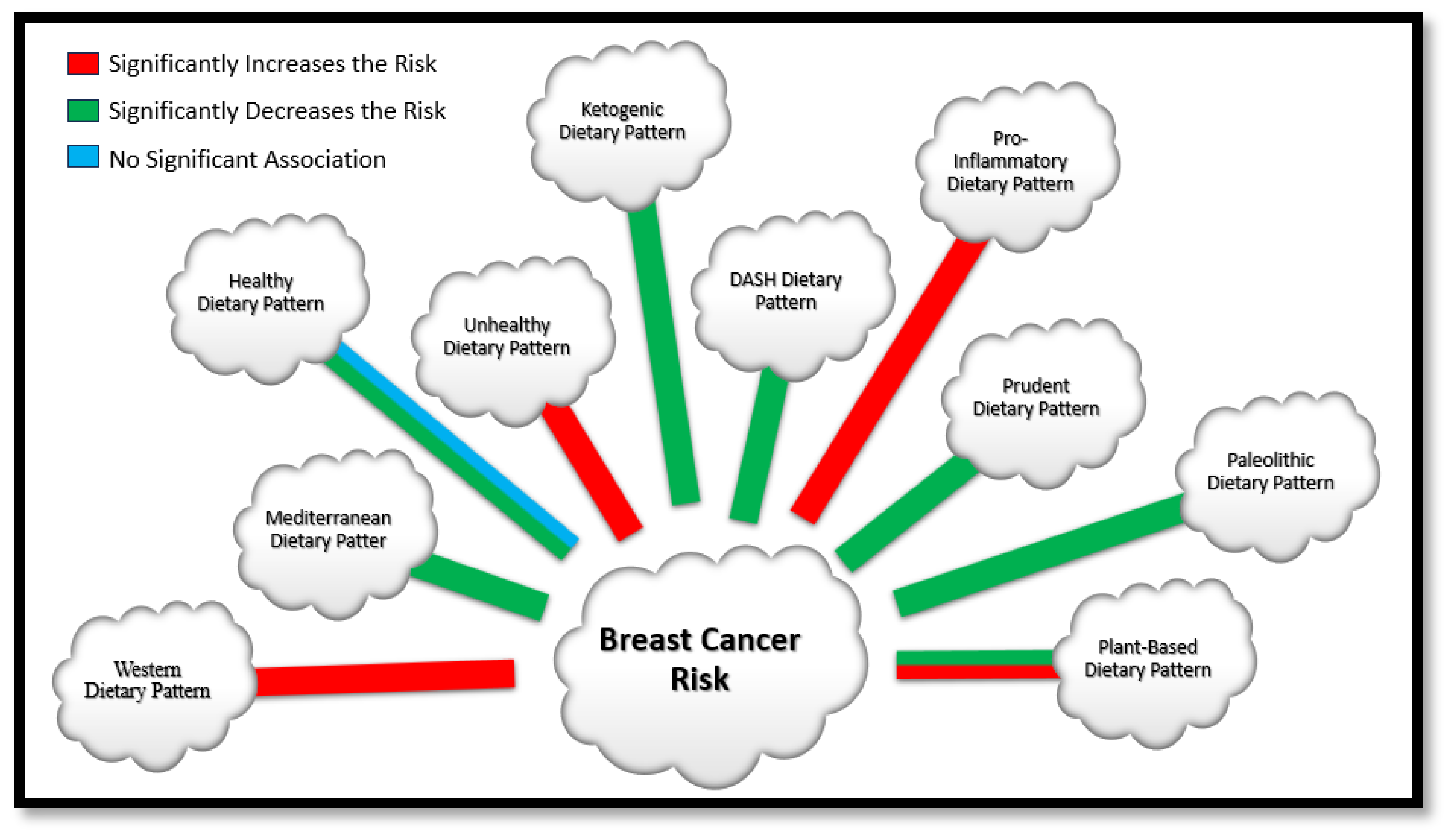
3. Dietary Patterns
3.1. Mediterranean Dietary Pattern
3.2. Plant-Based Dietary Pattern
3.3. Prudent Dietary Pattern
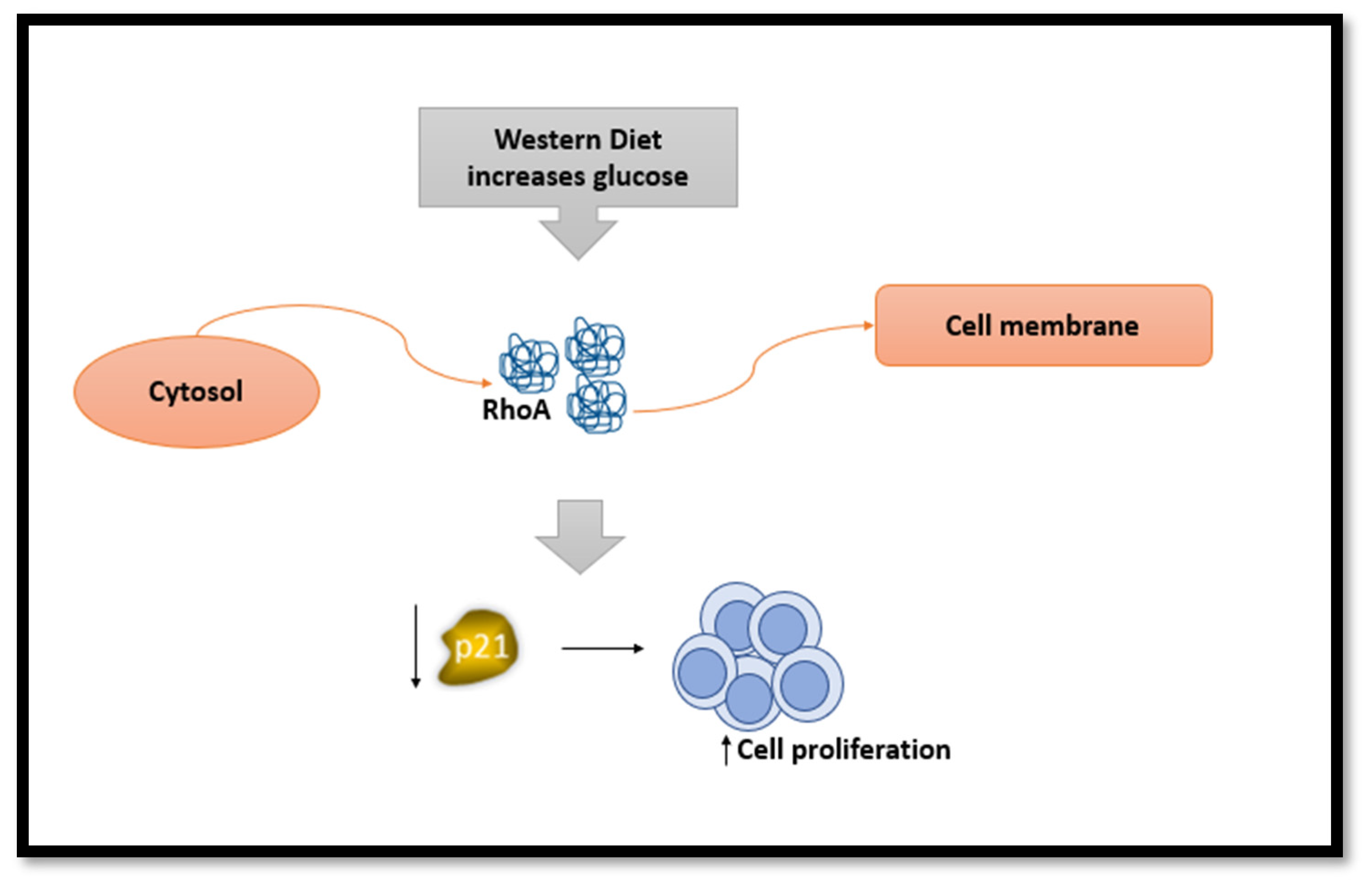
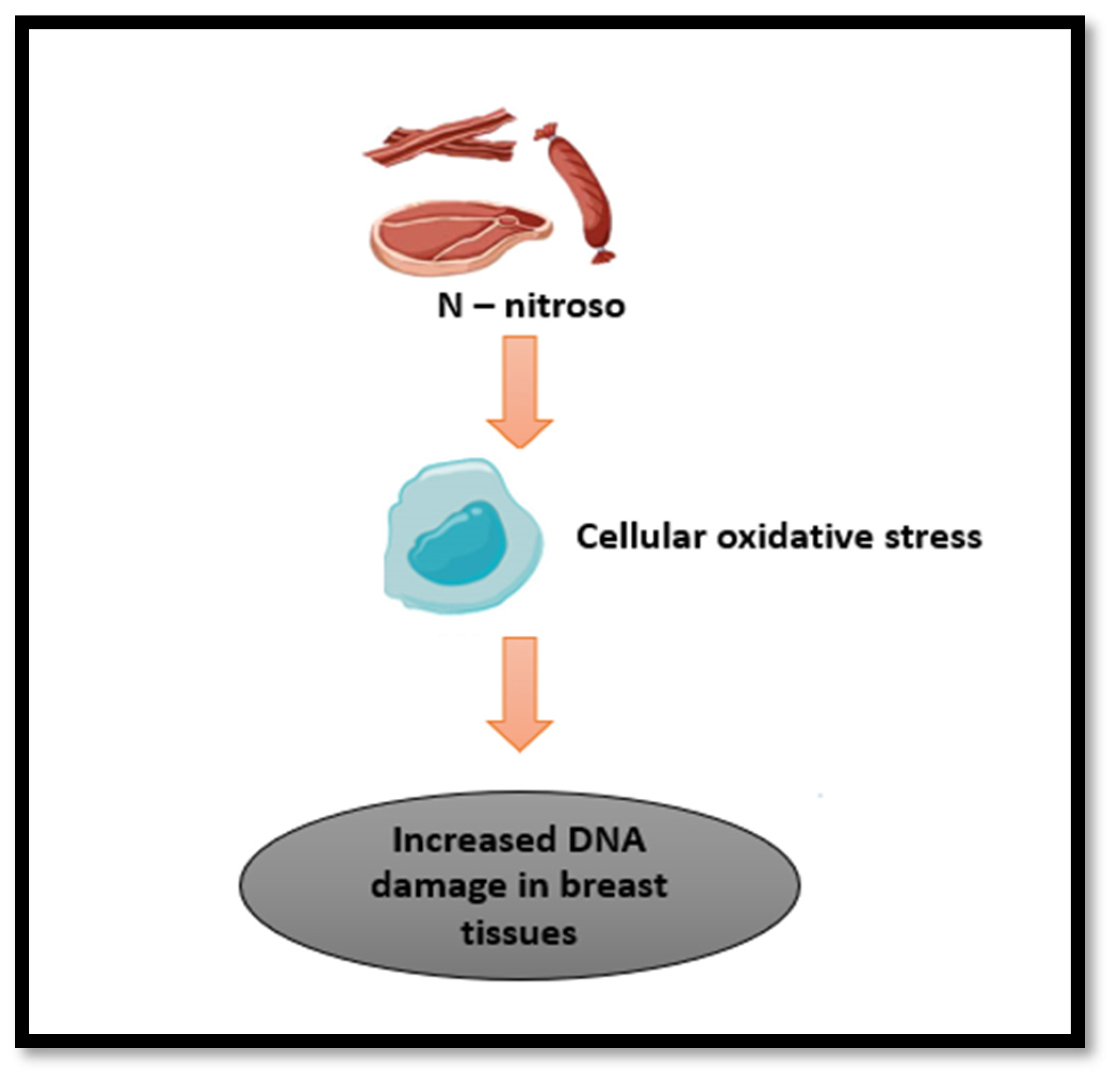
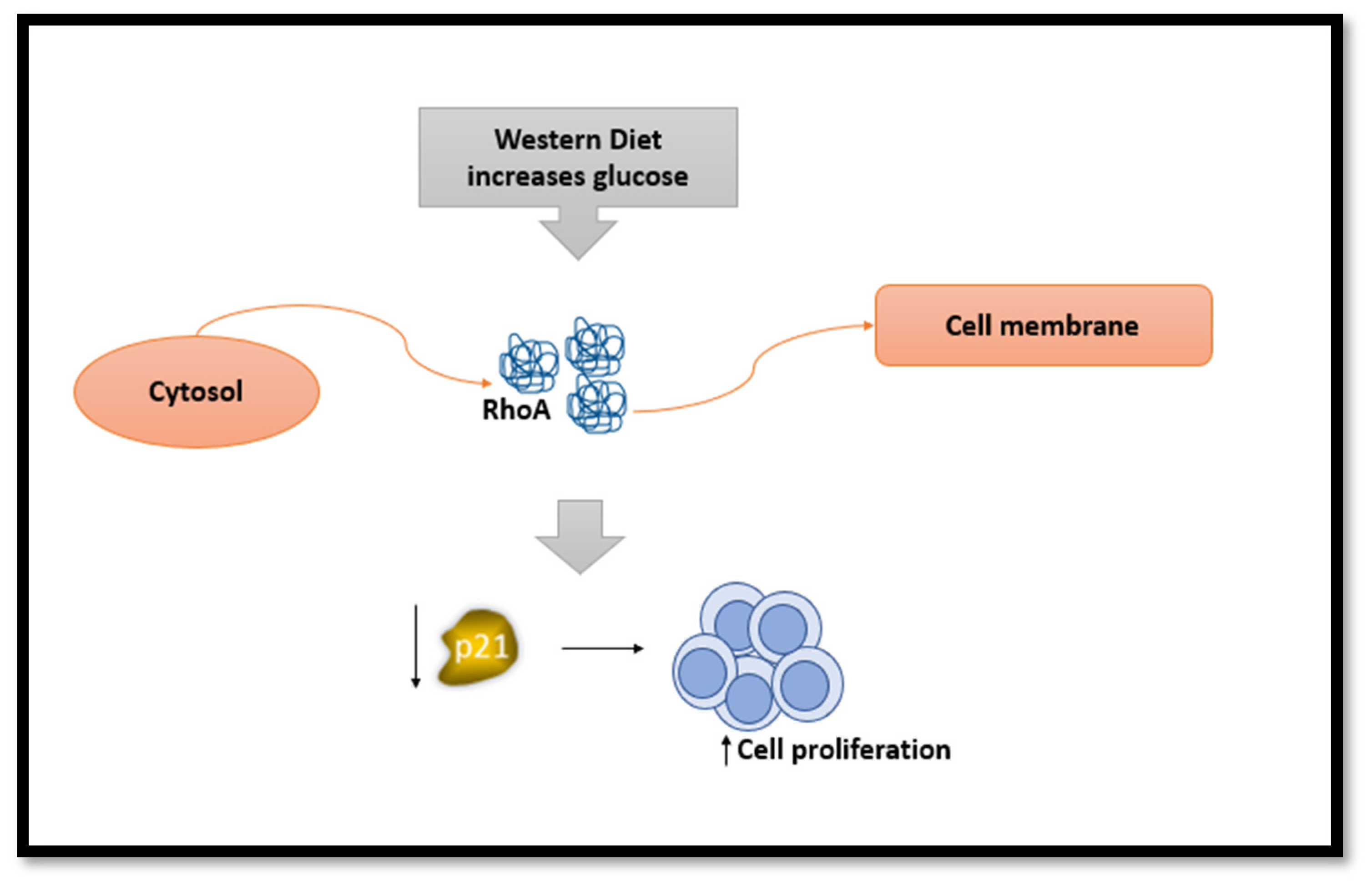
3.4. Western Dietary Pattern
3.5. Unhealthy Dietary Pattern
3.6. Healthy Dietary Pattern
3.7. Ketogenic Dietary Pattern
3.8. Pro-Inflammatory Dietary Pattern
3.9. Paleolithic Dietary Pattern
3.10. Dietary Approaches to Stop Hypertension (DASH) Dietary Pattern
4. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Global Cancer Observatory: Breast Cancer Fact Sheet; World Health Organization, International Agency for Research on Cancer: Lyon, France, 2020.
- Breast Cancer. Available online: https://www.who.int/news-room/fact-sheets/detail/breast-cancer (accessed on 18 November 2023).
- Global Cancer Observatory—Syrian Arab Republic Fact Sheet; World Health Organization, International Agency for Research on Cancer: Lyon, France, 2020.
- Global Cancer Observatory: Bahrain Fact Sheet; World Health Organization, International Agency for Research on Cancer: Lyon, France, 2020.
- Global Cancer Observatory: Egypt Fact Sheet; World Health Organization, International Agency for Research on Cancer: Lyon, France, 2020.
- Global Cancer Observatory: Gaza Strip and West Bank Fact Sheet; World Health Organization, International Agency for Research on Cancer: Lyon, France, 2020.
- Global Cancer Observatory: Iraq Fact Sheet; World Health Organization, International Agency for Research on Cancer: Lyon, France, 2020.
- Global Cancer Observatory: Islamic Republic of Iran Fact Sheet; World Health Organization, International Agency for Research on Cancer: Lyon, France, 2020.
- Global Cancer Observatory: Jordan Fact Sheet; World Health Organization, International Agency for Research on Cancer: Lyon, France, 2020.
- Global Cancer Observatory: Kuwait Fact Sheet; World Health Organization, International Agency for Research on Cancer: Lyon, France, 2020.
- Global Cancer Observatory: Lebanon Fact Sheet; World Health Organization, International Agency for Research on Cancer: Lyon, France, 2020.
- Global Cancer Observatory: Oman Fact Sheet; World Health Organization, International Agency for Research on Cancer: Lyon, France, 2020.
- Global Cancer Observatory: Qatar Fact Sheet; World Health Organization, International Agency for Research on Cancer: Lyon, France, 2020.
- Global Cancer Observatory: Saudi Arabia Fact Sheet; World Health Organization, International Agency for Research on Cancer: Lyon, France, 2020.
- Global Cancer Observatory: Turkey Fact Sheet; World Health Organisation, International Agency for Research on Cancer: Lyon, France, 2020.
- Global Cancer Observatory: United Arab Emirates Fact Sheet; World Health Organization, International Agency for Research on Cancer: Lyon, France, 2020.
- Global Cancer Observatory: Yemen Fact Sheet; World Health Organization, International Agency for Research on Cancer: Lyon, France, 2020.
- Saadeh, S.; Abdel-Razeq, H. Breast Cancer in the Arab World. In Cancer in the Arab World; Al-Shamsi, H.O., Abu-Gheida, I.H., Iqbal, F., Al-Awadhi, A., Eds.; Springer: Singapore, 2022; pp. 353–362. [Google Scholar] [CrossRef]
- Shin, S.; Fu, J.; Shin, W.K.; Huang, D.; Min, S.; Kang, D. Association of food groups and dietary pattern with breast cancer risk: A systematic review and meta-analysis. Clin. Nutr. 2023, 42, 282–297. [Google Scholar] [CrossRef] [PubMed]
- De Cicco, P.; Catani, M.V.; Gasperi, V.; Sibilano, M.; Quaglietta, M.; Savini, I. Nutrition and Breast Cancer: A Literature Review on Prevention, Treatment and Recurrence. Nutrients 2019, 11, 1514. [Google Scholar] [CrossRef]
- Cespedes, E.M.; Hu, F.B. Dietary patterns: From nutritional epidemiologic analysis to national guidelines. Am. J. Clin. Nutr. 2015, 101, 899–900. [Google Scholar] [CrossRef] [PubMed]
- Gardner, C.D.; Vadiveloo, M.K.; Petersen, K.S.; Anderson, C.A.M.; Springfield, S.; Horn, L.V.; Khera, A.; Lamendola, C.; Mayo, S.M.; Joseph, J.J. Popular Dietary Patterns: Alignment with American Heart Association 2021 Dietary Guidance: A Scientific Statement from the American Heart Association. Circulation 2023, 147, 1715–1730. [Google Scholar] [CrossRef] [PubMed]
- Dandamudi, A.; Tommie, J.; Nommsen-Rivers, L.; Couch, S. Dietary Patterns and Breast Cancer Risk: A Systematic Review. Anticancer Res. 2018, 38, 3209–3222. [Google Scholar] [CrossRef] [PubMed]
- Ghanbari, M.; Shahinfar, H.; Imani, H.; Safabakhsh, M.; Shab-Bidar, S. Association of Empirically Derived Food-Based Inflammatory Potential of the Diet and Breast Cancer: A Hospital-Based Case-Control Study. Clin. Breast Cancer 2022, 22, e567–e575. [Google Scholar] [CrossRef] [PubMed]
- Sohouli, M.H.; Buckland, G.; Clark, C.C.T.; Santos, H.O.; Athayde, F.L.; Sanati, V.; Janani, L.; Akram Sadat, S.; Mitra, Z. The relationship between diet quality indices and odds of breast cancer in women: A case-control study. BMC Women’s Health 2023, 23, 90. [Google Scholar] [CrossRef]
- Sohouli, M.H.; Hadizadeh, M.; Mardali, F.; Sanati, V.; da Silva Magalhães, E.I.; Zarrati, M. Association between novel dietary and lifestyle inflammation indices with risk of breast cancer (BrCa): A case-control study. Nutr. J. 2022, 21, 14. [Google Scholar] [CrossRef]
- Naja, F.; Nasreddine, L.; Awada, S.; El Sayed Ahmad, R.; Hwalla, N. Nutrition in the Prevention of Breast Cancer: A Middle Eastern Perspective. Front. Public Health 2019, 7, 316. [Google Scholar] [CrossRef]
- Golzarand, M.; Mirmiran, P.; Jessri, M.; Toolabi, K.; Mojarrad, M.; Azizi, F. Dietary trends in the Middle East and North Africa: An ecological study (1961 to 2007). Public Health Nutr. 2012, 15, 1835–1844. [Google Scholar] [CrossRef]
- Sikalidis, A.K.; Kelleher, A.H.; Kristo, A.S. Mediterranean Diet. Encyclopedia 2021, 1, 371–387. [Google Scholar] [CrossRef]
- Sadeghi, O.; Eshaghian, N.; Benisi-Kohansal, S.; Azadbakht, L.; Esmaillzadeh, A. A case-control study on the association between adherence to a Mediterranean-style diet and breast cancer. Front. Nutr. 2023, 10, 1140014. [Google Scholar] [CrossRef] [PubMed]
- Djafari, F.; Ghorbaninejad, P.; Firouzabadi, F.D.; Sheikhhossein, F.; Shahinfar, H.; Safabakhsh, M.; Imani, H.; Shab-Bidar, S. Adherence to Mediterranean dietary quality index and risk of breast cancer in adult women: A case-control study. BMC Women’s Health 2023, 23, 107. [Google Scholar] [CrossRef]
- Castro-Espin, C.; Bonet, C.; Crous-Bou, M.; Nadal-Zaragoza, N.; Tjønneland, A.; Mellemkjær, L.; Hajji-Louati, M.; Truong, T.; Katzke, V.; Le Cornet, C.; et al. Association of Mediterranean diet with survival after breast cancer diagnosis in women from nine European countries: Results from the EPIC cohort study. BMC Med. 2023, 21, 225. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Hu, B.-Q.; Wu, X.-J.; Qi, X.-W.; Jiang, J.; Cui, X.; Zhang, F.; Yang, X.-H. Adherence to Mediterranean diet and the risk of breast cancer: A meta-analysis. Transl. Cancer Res. 2018, 7, 1290–1297. [Google Scholar] [CrossRef]
- Turati, F.; Carioli, G.; Bravi, F.; Ferraroni, M.; Serraino, D.; Montella, M.; Giacosa, A.; Toffolutti, F.; Negri, E.; Levi, F.; et al. Mediterranean Diet and Breast Cancer Risk. Nutrients 2018, 10, 326. [Google Scholar] [CrossRef] [PubMed]
- Azzeh, F.S.; Hasanain, D.M.; Qadhi, A.H.; Ghafouri, K.J.; Azhar, W.F.; Ghaith, M.M.; Aldairi, A.F.; Almasmoum, H.A.; Assaggaf, H.M.; Alhussain, M.H.; et al. Consumption of Food Components of the Mediterranean Diet Decreases the Risk of Breast Cancer in the Makkah Region, Saudi Arabia: A Case-Control Study. Front. Nutr. 2022, 9, 863029. [Google Scholar] [CrossRef] [PubMed]
- Rigi, S.; Mousavi, S.M.; Benisi-Kohansal, S.; Azadbakht, L.; Esmaillzadeh, A. The association between plant-based dietary patterns and risk of breast cancer: A case-control study. Sci. Rep. 2021, 11, 3391. [Google Scholar] [CrossRef]
- Sasanfar, B.; Toorang, F.; Booyani, Z.; Vassalami, F.; Mohebbi, E.; Azadbakht, L.; Zendehdel, K. Adherence to plant-based dietary pattern and risk of breast cancer among Iranian women. Eur. J. Clin. Nutr. 2021, 75, 1578–1587. [Google Scholar] [CrossRef]
- Romanos-Nanclares, A.; Willett, W.C.; Rosner, B.A.; Collins, L.C.; Hu, F.B.; Toledo, E.; Eliassen, A.H. Healthful and Unhealthful Plant-Based Diets and Risk of Breast Cancer in U.S. Women: Results from the Nurses’ Health Studies. Cancer Epidemiol. Biomark. Prev. 2021, 30, 1921–1931. [Google Scholar] [CrossRef]
- Shah, S.; Mahamat-Saleh, Y.; Ait-Hadad, W.; Koemel, N.A.; Varraso, R.; Boutron-Ruault, M.C.; Laouali, N. Long-term adherence to healthful and unhealthful plant-based diets and breast cancer risk overall and by hormone receptor and histologic subtypes among postmenopausal females. Am. J. Clin. Nutr. 2023, 117, 467–476. [Google Scholar] [CrossRef] [PubMed]
- DeClercq, V.; Nearing, J.T.; Sweeney, E. Plant-Based Diets and Cancer Risk: What is the Evidence? Curr. Nutr. Rep. 2022, 11, 354–369. [Google Scholar] [CrossRef]
- Payandeh, N.; Shahinfar, H.; Amini, M.R.; Jafari, A.; Safabakhsh, M.; Imani, H.; Shab-Bidar, S. The Lack of Association between Plant-Based Dietary Pattern and Breast Cancer: A Hospital-Based Case-Control Study. Clin. Nutr. Res. 2021, 10, 115. [Google Scholar] [CrossRef]
- Abbas, M.O.; Baig, M. Knowledge and Practice Concerning Breast Cancer Risk Factors and Screening among Females in UAE. Asian Pac. J. Cancer Prev. 2023, 24, 479–487. [Google Scholar] [CrossRef]
- Alfawaz, H.; Khan, N.; Alhuthayli, H.; Wani, K.; Aljumah, M.A.; Khattak, M.N.K.; Alghanim, S.A.; Al-Daghri, N.M. Awareness and Knowledge Regarding the Consumption of Dietary Fiber and Its Relation to Self-Reported Health Status in an Adult Arab Population: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2020, 17, 4226. [Google Scholar] [CrossRef]
- Eliassen, A.H.; Liao, X.; Rosner, B.; Tamimi, R.M.; Tworoger, S.S.; Hankinson, S.E. Plasma carotenoids and risk of breast cancer over 20 y of follow-up. Am. J. Clin. Nutr. 2015, 101, 1197–1205. [Google Scholar] [CrossRef] [PubMed]
- Foroutan-Ghaznavi, M.; Mazloomi, S.M.; Montazeri, V.; Pirouzpanah, S. Dietary patterns in association with the expression of pro-metastatic genes in primary breast cancer. Eur. J. Nutr. 2022, 61, 3267–3284. [Google Scholar] [CrossRef]
- Brennan, S.F.; Cantwell, M.M.; Cardwell, C.R.; Velentzis, L.S.; Woodside, J.V. Dietary patterns and breast cancer risk: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2010, 91, 1294–1302. [Google Scholar] [CrossRef]
- Xiao, Y.; Xia, J.; Li, L.; Ke, Y.; Cheng, J.; Xie, Y.; Chu, W.; Cheung, P.; Kim, J.H.; Colditz, G.A.; et al. Associations between dietary patterns and the risk of breast cancer: A systematic review and meta-analysis of observational studies. Breast Cancer Res. 2019, 21, 16. [Google Scholar] [CrossRef]
- Flores-García, M.K.; Mérida-Ortega, Á.; Denova-Gutiérrez, E.; Rothenberg, S.J.; López-Carrillo, L. “Western” and “prudent” dietary patterns are associated with breast cancer among Mexican pre- and postmenopausal women. Nutr. Res. 2022, 105, 138–146. [Google Scholar] [CrossRef] [PubMed]
- Fu, L.; Xu, B.T.; Xu, X.R.; Gan, R.Y.; Zhang, Y.; Xia, E.Q.; Li, H.B. Antioxidant capacities and total phenolic contents of 62 fruits. Food Chem. 2011, 129, 345–350. [Google Scholar] [CrossRef]
- Andersen, J.L.M.; Hansen, L.; Thomsen, B.L.R.; Christiansen, L.R.; Dragsted, L.O.; Olsen, A. Pre- and post-diagnostic intake of whole grain and dairy products and breast cancer prognosis: The Danish Diet, Cancer and Health cohort. Breast Cancer Res. Treat. 2020, 179, 743–753. [Google Scholar] [CrossRef]
- Roswall, N.; Weiderpass, E. Alcohol as a risk factor for cancer: Existing evidence in a global perspective. J. Prev. Med. Public Health 2015, 48, 1–9. [Google Scholar] [CrossRef]
- Foroozani, E.; Akbari, A.; Amanat, S.; Rashidi, N.; Bastam, D.; Ataee, S.; Sharifnia, G.; Faraouei, M.; Dianatinasab, M.; Safdari, H. Adherence to a western dietary pattern and risk of invasive ductal and lobular breast carcinomas: A case-control study. Sci. Rep. 2022, 12, 5859. [Google Scholar] [CrossRef]
- Tsai, H.H.; Yu, J.C.; Hsu, H.M.; Chu, C.H.; Chang, T.M.; Hong, Z.J.; Feng, A.C.; Fu, C.Y.; Hsu, K.F.; Dai, M.S.; et al. The Risk of Breast Cancer between Western and Mediterranean Dietary Patterns. Nutrients 2023, 15, 2057. [Google Scholar] [CrossRef] [PubMed]
- Heidari, Z.; Jalali, S.; Sedaghat, F.; Ehteshami, M.; Rashidkhani, B. Dietary patterns and breast cancer risk among Iranian women: A case-control study. Eur. J. Obstet. Gynecol. Reprod. Biol. 2018, 230, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Karimi, Z.; Jessri, M.; Houshiar-Rad, A.; Mirzaei, H.R.; Rashidkhani, B. Dietary patterns and breast cancer risk among women. Public Health Nutr. 2014, 17, 1098–1106. [Google Scholar] [CrossRef]
- Khodabakhshi, A.; Seyfried, T.N.; Kalamian, M.; Beheshti, M.; Davoodi, S.H. Does a ketogenic diet have beneficial effects on quality of life, physical activity or biomarkers in patients with breast cancer: A randomized controlled clinical trial. Nutr. J. 2020, 19, 87. [Google Scholar] [CrossRef] [PubMed]
- Sasanfar, B.; Toorang, F.; Esmaillzadeh, A.; Zendehdel, K. Adherence to the low carbohydrate diet and the risk of breast Cancer in Iran. Nutr. J. 2019, 18, 86. [Google Scholar] [CrossRef]
- Khodabakhshi, A.; Akbari, M.E.; Mirzaei, H.R.; Mehrad-Majd, H.; Kalamian, M.; Davoodi, S.H. Feasibility, Safety, and Beneficial Effects of MCT-Based Ketogenic Diet for Breast Cancer Treatment: A Randomized Controlled Trial Study. Nutr. Cancer 2020, 72, 627–634. [Google Scholar] [CrossRef]
- İyikesici, M.S.; Slocum, A.K.; Slocum, A.; Berkarda, F.B.; Kalamian, M.; Seyfried, T.N. Efficacy of Metabolically Supported Chemotherapy Combined with Ketogenic Diet, Hyperthermia, and Hyperbaric Oxygen Therapy for Stage IV Triple-Negative Breast Cancer. Cureus 2017, 9, e1445. [Google Scholar] [CrossRef]
- Gholamalizadeh, M.; Afsharfar, M.; Fathi, S.; Tajadod, S.; Mohseni, G.K.; Shekari, S.; Vahid, F.; Doaei, S.; Shafaei Kachaei, H.; Majidi, N.; et al. Relationship between breast cancer and dietary inflammatory index; a case-control study. Clin. Nutr. ESPEN 2022, 51, 353–358. [Google Scholar] [CrossRef]
- Vahid, F.; Shivappa, N.; Hatami, M.; Sadeghi, M.; Ameri, F.; Jamshidi Naeini, Y.; Hebert, J.R.; Davoodi, S.H. Association between Dietary Inflammatory Index (DII) and Risk of Breast Cancer: A Case-Control Study. Asian Pac. J. Cancer Prev. 2018, 19, 1215–1221. [Google Scholar] [CrossRef]
- Jalali, S.; Shivappa, N.; Hébert, J.R.; Heidari, Z.; Hekmatdoost, A.; Rashidkhani, B. Dietary Inflammatory Index and Odds of Breast Cancer in a Case-Control Study from Iran. Nutr. Cancer 2018, 70, 1034–1042. [Google Scholar] [CrossRef]
- Hayati, Z.; Montazeri, V.; Shivappa, N.; Hebert, J.R.; Pirouzpanah, S. The association between the inflammatory potential of diet and the risk of histopathological and molecular subtypes of breast cancer in northwestern Iran: Results from the Breast Cancer Risk and Lifestyle study. Cancer 2022, 128, 2298–2312. [Google Scholar] [CrossRef]
- Hammad, S.S.; Mahmoud, R.; Shivappa, N.; Hebert, J.R.; Marie, L.; Tayyem, R.F. Dietary inflammatory index and odds of breast cancer: A case-control study. Food Sci. Nutr. 2021, 9, 5211–5219. [Google Scholar] [CrossRef]
- Castro-Espin, C.; Agudo, A.; Bonet, C.; Katzke, V.; Turzanski-Fortner, R.; Aleksandrova, K.; Schulze, M.B.; Tjønneland, A.; Dahm, C.C.; Quirós, J.R.; et al. Inflammatory potential of the diet and risk of breast cancer in the European Investigation into Cancer and Nutrition (EPIC) study. Eur. J. Epidemiol. 2021, 36, 953–964. [Google Scholar] [CrossRef]
- Hajji-Louati, M.; Gelot, A.; Frenoy, P.; Laouali, N.; Guénel, P.; Romana Mancini, F. Dietary Inflammatory Index and risk of breast cancer: Evidence from a prospective cohort of 67,879 women followed for 20 years in France. Eur. J. Nutr. 2023, 62, 1977–1989. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Chen, R.; Wang, H.; Liang, F. Mechanisms Linking Inflammation to Insulin Resistance. Int. J. Endocrinol. 2015, 2015, 508409. [Google Scholar] [CrossRef]
- Sohouli, M.H.; Baniasadi, M.; Hernández-Ruiz, Á.; Magalhães, E.; Santos, H.O.; Akbari, A.; Zarrati, M. Associations of the Paleolithic Diet Pattern Scores and the Risk of Breast Cancer among Adults: A Case-Control Study. Nutr. Cancer 2023, 75, 256–264. [Google Scholar] [CrossRef] [PubMed]
- Dixon, K.A.; Michelsen, M.K.; Carpenter, C.L. Modern Diets and the Health of Our Planet: An Investigation into the Environmental Impacts of Food Choices. Nutrients 2023, 15, 692. [Google Scholar] [CrossRef]
- Xiao, Y.; Wang, Y.; Gu, H.; Xu, Z.; Tang, Y.; He, H.; Peng, L.; Xiang, L. Adherence to the Paleolithic diet and Paleolithic-like lifestyle reduce the risk of colorectal cancer in the United States: A prospective cohort study. J. Transl. Med. 2023, 21, 482. [Google Scholar] [CrossRef]
- Shah, S.; Mahamat-Saleh, Y.; Hajji-Louati, M.; Correia, E.; Oulhote, Y.; Boutron-Ruault, M.-C.; Laouali, N. Palaeolithic diet score and risk of breast cancer among postmenopausal women overall and by hormone receptor and histologic subtypes. Eur. J. Clin. Nutr. 2023, 77, 596–602. [Google Scholar] [CrossRef]
- Heidari, Z.; Mohammadi, E.; Aghamohammadi, V.; Jalali, S.; Rezazadeh, A.; Sedaghat, F.; Assadi, M.; Rashidkhani, B. Dietary Approaches to Stop Hypertension (DASH) diets and breast cancer among women: A case control study. BMC Cancer 2020, 20, 708. [Google Scholar] [CrossRef]
- Toorang, F.; Sasanfar, B.; Esmaillzadeh, A.; Zendehdel, K. Adherence to the DASH Diet and Risk of Breast Cancer. Clin. Breast Cancer 2022, 22, 244–251. [Google Scholar] [CrossRef]
- Soltani, S.; Benisi-Kohansal, S.; Azadbakht, L.; Esmaillzadeh, A. Association between Adherence to “Dietary Approaches to Stop Hypertension” Eating Plan and Breast Cancer. Nutr. Cancer 2021, 73, 433–441. [Google Scholar] [CrossRef]
- Xia, H.; Wang, L.; Wang, H. Current research trends, hotspots, and frontiers of medical nutrition therapy on cancer: A bibliometric analysis. Front. Oncol. 2023, 13, 1170198. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| List | Details |
|---|---|
| Search Date | October–November 2023 |
| Databases | PubMed, ProQuest, and Cochrane |
| Search Terms | “Dietary pattern” “diet” “food pattern” “Mediterranean diet” “plant-based diet” “healthy diet” “unhealthy diet” “prudent diet” “pro-inflammatory diet” “western diet” “Palaeolithic diet” “nutrient” “processed food” “DASH” AND “Breast Cancer” “Breast carcinoma” “mammary cancer” AND “Bahrain” “Egypt” “Iran” “Iraq” “Jordan” “Kuwait” “Lebanon” “Oman” “Palestine” “Qatar” “Saudi Arabia” “Syria” “Turkey” “United Arab Emirates” “Yemen” “Middle East” “Arab countries” |
| Time Frame | 2000–2023 |
| Inclusion/Exclusion Criteria | All study designs except for narrative/literature review. English Studies |
| Collection Procedure | The literature search was conducted independently by all authors |
| Compound/Nutrient | Proposed Mechanism |
|---|---|
| Fibers |
|
Antioxidants
| Protecting cells from mutations that cause breast cancer by reducing DNA damage induced by oxidative stress [37]. |
| They have protective roles by influencing hormonal pathways, via antiproliferative, antioxidant, antiangiogenic and apoptotic properties [36,37]. |
| Folate | Affect gene expression on tumour suppressors by taking a role in DNA methylation [36]. |
| Carotenoids |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zamzam, S.; Said, S.; Yaghi, J.; Faisal, F.S.; Hassan, D.; Abdul Majeed, S.; Al Rajabi, A.; Tayyem, R. Dietary Patterns Associated with Breast Cancer in the Middle East: A Scoping Review. Nutrients 2024, 16, 579. https://doi.org/10.3390/nu16050579
Zamzam S, Said S, Yaghi J, Faisal FS, Hassan D, Abdul Majeed S, Al Rajabi A, Tayyem R. Dietary Patterns Associated with Breast Cancer in the Middle East: A Scoping Review. Nutrients. 2024; 16(5):579. https://doi.org/10.3390/nu16050579
Chicago/Turabian StyleZamzam, Syed, Suad Said, Juman Yaghi, Fathima Sahar Faisal, Dana Hassan, Safa Abdul Majeed, Ala Al Rajabi, and Reema Tayyem. 2024. "Dietary Patterns Associated with Breast Cancer in the Middle East: A Scoping Review" Nutrients 16, no. 5: 579. https://doi.org/10.3390/nu16050579
APA StyleZamzam, S., Said, S., Yaghi, J., Faisal, F. S., Hassan, D., Abdul Majeed, S., Al Rajabi, A., & Tayyem, R. (2024). Dietary Patterns Associated with Breast Cancer in the Middle East: A Scoping Review. Nutrients, 16(5), 579. https://doi.org/10.3390/nu16050579