

Nutrient Intake and Its Association with Appendicular Total Lean Mass and Muscle Function and Strength in Older Adults: A Population-Based Study
 , , ,
, , ,  , ,
, ,  ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Design, Settings, and Participants
2.2. Anthropometry
2.3. Muscle Strength and Performance
2.4. Dietary Examination
2.5. Dietary Components Included
2.6. Statistical Analysis
2.7. Ethical Considerations
3. Results
3.1. Descriptive Results
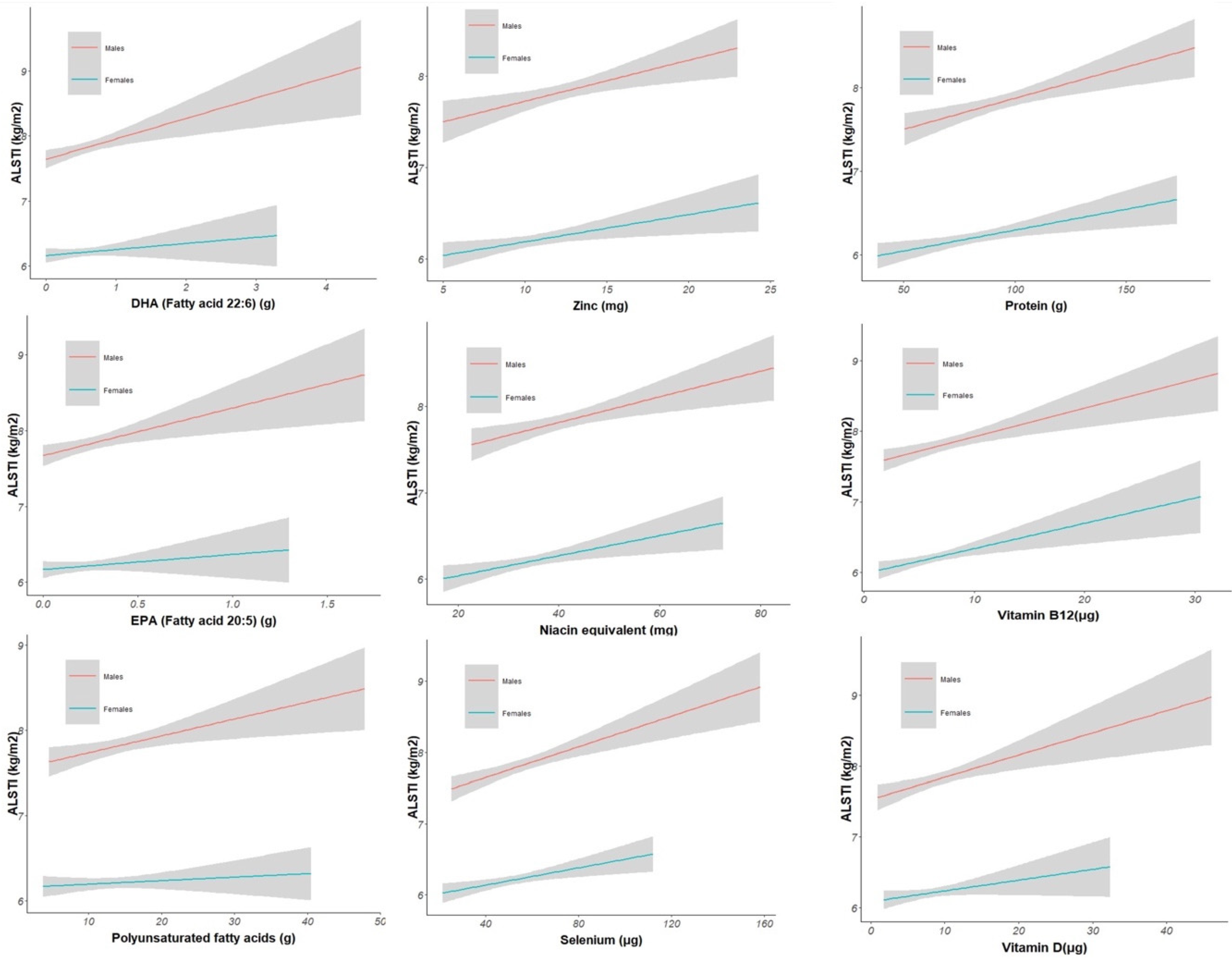
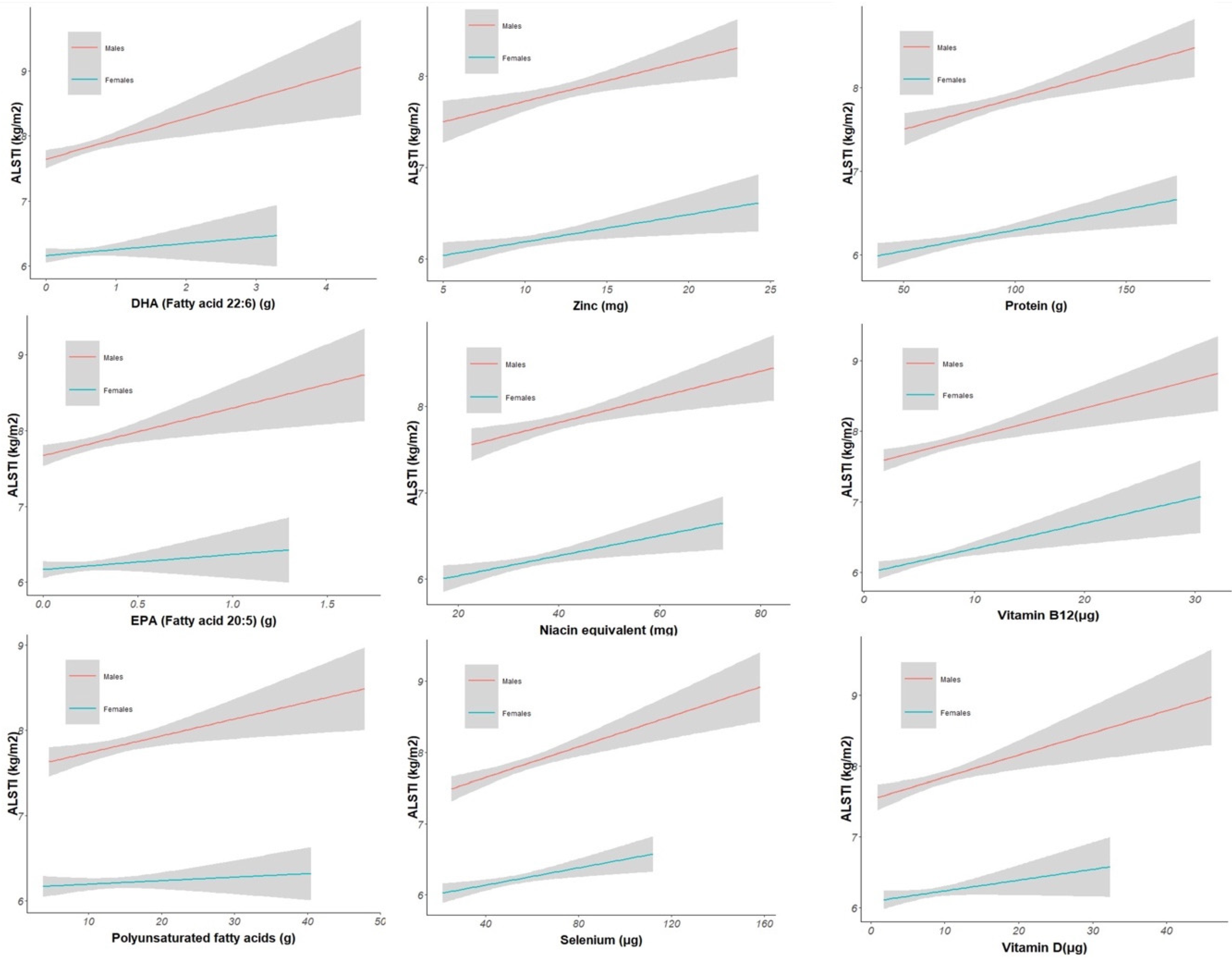
3.2. Association between Nutrients and ALSTI
3.3. Association between Nutrients and Handgrip Strength (kPa)
3.4. Association between Nutrients and Gait Speed 30 m (m/s)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef]
- Yeung, S.S.Y.; Reijnierse, E.M.; Pham, V.K.; Trappenburg, M.C.; Lim, W.K.; Meskers, C.G.M.; Maier, A.B. Sarcopenia and its association with falls and fractures in older adults: A systematic review and meta-analysis. J. Cachexia Sarcopenia Muscle 2019, 10, 485–500. [Google Scholar] [CrossRef]
- Cipolli, G.C.; Aprahamian, I.; Borim, F.S.A.; Falcão, D.V.S.; Cachioni, M.; Melo, R.C.; Batistoni, S.S.T.; Neri, A.L.; Yassuda, M.S. Probable sarcopenia is associated with cognitive impairment among community-dwelling older adults: Results from the FIBRA study. Arq. Neuropsiquiatr. 2021, 79, 376–383. [Google Scholar] [CrossRef]
- Inouye, S.K.; Studenski, S.; Tinetti, M.E.; Kuchel, G.A. Geriatric syndromes: Clinical, research, and policy implications of a core geriatric concept. J. Am. Geriatr. Soc. 2007, 55, 780–791. [Google Scholar] [CrossRef]
- Rosenberg, I.H. Sarcopenia: Origins and clinical relevance. J. Nutr. 1997, 127 (Suppl. S5), 990s–991s. [Google Scholar] [CrossRef]
- Yuan, S.; Larsson, S.C. Epidemiology of sarcopenia: Prevalence, risk factors, and consequences. Metabolism 2023, 144, 155533. [Google Scholar] [CrossRef]
- Herrera-Martínez, A.D.; Muñoz Jiménez, C.; López Aguilera, J.; Crespin04910sal, M.C.; Manzano García, G.; Gálvez Moreno, M.; Calañas Continente, A.; Molina Puerta, M.J. Mediterranean Diet, Vitamin D, and Hypercaloric, Hyperproteic Oral Supplements for Treating Sarcopenia in Patients with Heart Failure-A Randomized Clinical Trial. Nutrients 2024, 16, 110. [Google Scholar] [CrossRef] [PubMed]
- Kakehi, S.; Wakabayashi, H.; Inuma, H.; Inose, T.; Shioya, M.; Aoyama, Y.; Hara, T.; Uchimura, K.; Tomita, K.; Okamoto, M.; et al. Rehabilitation Nutrition and Exercise Therapy for Sarcopenia. World J. Mens Health 2022, 40, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Morley, J.E. Treatment of sarcopenia: The road to the future. J. Cachexia Sarcopenia Muscle 2018, 9, 1196–1199. [Google Scholar] [CrossRef] [PubMed]
- van Dronkelaar, C.; van Velzen, A.; Abdelrazek, M.; van der Steen, A.; Weijs, P.J.M.; Tieland, M. Minerals and Sarcopenia; The Role of Calcium, Iron, Magnesium, Phosphorus, Potassium, Selenium, Sodium, and Zinc on Muscle Mass, Muscle Strength, and Physical Performance in Older Adults: A Systematic Review. J. Am. Med. Dir. Assoc. 2018, 19, 6–11.e13. [Google Scholar] [CrossRef]
- Robinson, S.; Granic, A.; Sayer, A.A. Nutrition and Muscle Strength, As the Key Component of Sarcopenia: An Overview of Current Evidence. Nutrients 2019, 11, 2942. [Google Scholar] [CrossRef]
- Da Boit, M.; Sibson, R.; Sivasubramaniam, S.; Meakin, J.R.; Greig, C.A.; Aspden, R.M.; Thies, F.; Jeromson, S.; Hamilton, D.L.; Speakman, J.R.; et al. Sex differences in the effect of fish-oil supplementation on the adaptive response to resistance exercise training in older people: A randomized controlled trial. Am. J. Clin. Nutr. 2017, 105, 151–158. [Google Scholar] [CrossRef]
- Wetterberg, H.; Rydén, L.; Ahlner, F.; Falk Erhag, H.; Gudmundsson, P.; Guo, X.; Joas, E.; Johansson, L.; Kern, S.; Mellqvist Fässberg, M.; et al. Representativeness in population-based studies of older adults: Five waves of cross-sectional examinations in the Gothenburg H70 Birth Cohort Study. BMJ Open 2022, 12, e068165. [Google Scholar] [CrossRef]
- Rydberg Sterner, T.; Ahlner, F.; Blennow, K.; Dahlin-Ivanoff, S.; Falk, H.; Havstam Johansson, L.; Hoff, M.; Holm, M.; Hörder, H.; Jacobsson, T.; et al. The Gothenburg H70 Birth cohort study 2014–16: Design, methods and study population. Eur. J. Epidemiol. 2019, 34, 191–209. [Google Scholar] [CrossRef]
- Bohannon, R.W. Comfortable and maximum walking speed of adults aged 20–79 years: Reference values and determinants. Age Ageing 1997, 26, 15–19. [Google Scholar] [CrossRef]
- Skillbäck, T.; Blennow, K.; Zetterberg, H.; Skoog, J.; Rydén, L.; Wetterberg, H.; Guo, X.; Sacuiu, S.; Mielke, M.M.; Zettergren, A.; et al. Slowing gait speed precedes cognitive decline by several years. Alzheimers Dement. 2022, 18, 1667–1676. [Google Scholar] [CrossRef]
- Sipers, W.M.; Verdijk, L.B.; Sipers, S.J.; Schols, J.M.; van Loon, L.J. The Martin Vigorimeter Represents a Reliable and More Practical Tool Than the Jamar Dynamometer to Assess Handgrip Strength in the Geriatric Patient. J. Am. Med. Dir. Assoc. 2016, 17, e461–e467. [Google Scholar] [CrossRef] [PubMed]
- Wallengren, O.; Bosaeus, I.; Frändin, K.; Lissner, L.; Falk Erhag, H.; Wetterberg, H.; Rydberg Sterner, T.; Rydén, L.; Rothenberg, E.; Skoog, I. Comparison of the 2010 and 2019 diagnostic criteria for sarcopenia by the European Working Group on Sarcopenia in Older People (EWGSOP) in two cohorts of Swedish older adults. BMC Geriatr. 2021, 21, 600. [Google Scholar] [CrossRef] [PubMed]
- Samuelsson, J.; Rothenberg, E.; Lissner, L.; Eiben, G.; Zettergren, A.; Skoog, I. Time trends in nutrient intake and dietary patterns among five birth cohorts of 70-year-olds examined 1971-2016: Results from the Gothenburg H70 birth cohort studies, Sweden. Nutr. J. 2019, 18, 66. [Google Scholar] [CrossRef] [PubMed]
- Chan, Y.H. Biostatistics 104: Correlational analysis. Singap. Med. J. 2003, 44, 614–619. [Google Scholar]
- Dancey, C.P.; Reidy, J. Statistics without Maths for Psychology; Pearson Education: Upper Saddle River, NJ, USA, 2007. [Google Scholar]
- Haynes, W. Benjamini–Hochberg Method. In Encyclopedia of Systems Biology; Dubitzky, W., Wolkenhauer, O., Cho, K.-H., Yokota, H., Eds.; Springer: New York, NY, USA, 2013; p. 78. [Google Scholar]
- Muscaritoli, M. The Impact of Nutrients on Mental Health and Well-Being: Insights From the Literature. Front. Nutr. 2021, 8, 656290. [Google Scholar] [CrossRef]
- Bagheri, A.; Hashemi, R.; Heshmat, R.; Motlagh, A.D.; Esmaillzadeh, A. Patterns of Nutrient Intake in Relation to Sarcopenia and Its Components. Front. Nutr. 2021, 8, 645072. [Google Scholar] [CrossRef] [PubMed]
- Bauer, J.; Biolo, G.; Cederholm, T.; Cesari, M.; Cruz-Jentoft, A.J.; Morley, J.E.; Phillips, S.; Sieber, C.; Stehle, P.; Teta, D.; et al. Evidence-Based Recommendations for Optimal Dietary Protein Intake in Older People: A Position Paper From the PROT-AGE Study Group. J. Am. Med. Dir. Assoc. 2013, 14, 542–559. [Google Scholar] [CrossRef] [PubMed]
- Yang, A.; Lv, Q.; Chen, F.; Wang, Y.; Liu, Y.; Shi, W.; Wang, D. The effect of vitamin D on sarcopenia depends on the level of physical activity in older adults. J. Cachexia Sarcopenia Muscle 2020, 11, 678–689. [Google Scholar] [CrossRef]
- Uchitomi, R.; Oyabu, M.; Kamei, Y. Vitamin D and Sarcopenia: Potential of Vitamin D Supplementation in Sarcopenia Prevention and Treatment. Nutrients 2020, 12, 3189. [Google Scholar] [CrossRef]
- Dent, E.; Morley, J.E.; Cruz-Jentoft, A.J.; Arai, H.; Kritchevsky, S.B.; Guralnik, J.; Bauer, J.M.; Pahor, M.; Clark, B.C.; Cesari, M.; et al. International Clinical Practice Guidelines for Sarcopenia (ICFSR): Screening, Diagnosis and Management. J. Nutr. Health Aging 2018, 22, 1148–1161. [Google Scholar] [CrossRef]
- Remelli, F.; Vitali, A.; Zurlo, A.; Volpato, S. Vitamin D Deficiency and Sarcopenia in Older Persons. Nutrients 2019, 11, 2861. [Google Scholar] [CrossRef] [PubMed]
- Gkekas, N.K.; Anagnostis, P.; Paraschou, V.; Stamiris, D.; Dellis, S.; Kenanidis, E.; Potoupnis, M.; Tsiridis, E.; Goulis, D.G. The effect of vitamin D plus protein supplementation on sarcopenia: A systematic review and meta-analysis of randomized controlled trials. Maturitas 2021, 145, 56–63. [Google Scholar] [CrossRef]
- Taherkhani, S.; Valaei, K.; Arazi, H.; Suzuki, K. An Overview of Physical Exercise and Antioxidant Supplementation Influences on Skeletal Muscle Oxidative Stress. Antioxidants 2021, 10, 1528. [Google Scholar] [CrossRef]
- Pritam, P.; Deka, R.; Bhardwaj, A.; Srivastava, R.; Kumar, D.; Jha, A.K.; Jha, N.K.; Villa, C.; Jha, S.K. Antioxidants in Alzheimer’s Disease: Current Therapeutic Significance and Future Prospects. Biology 2022, 11, 212. [Google Scholar] [CrossRef]
- Chae, S.A.; Kim, H.S.; Lee, J.H.; Yun, D.H.; Chon, J.; Yoo, M.C.; Yun, Y.; Yoo, S.D.; Kim, D.H.; Lee, S.A.; et al. Impact of Vitamin B12 Insufficiency on Sarcopenia in Community-Dwelling Older Korean Adults. Int. J. Environ. Res. Public Health 2021, 18, 12433. [Google Scholar] [CrossRef]
- Marchi, G.; Busti, F.; Zidanes, A.L.; Vianello, A.; Girelli, D. Cobalamin Deficiency in the Elderly. Mediterr. J. Hematol. Infect. Dis. 2020, 12, e2020043. [Google Scholar] [CrossRef] [PubMed]
- Polidori, M.C.; Mecocci, P. Plasma susceptibility to free radical-induced antioxidant consumption and lipid peroxidation is increased in very old subjects with Alzheimer disease. J. Alzheimers Dis. 2002, 4, 517–522. [Google Scholar] [CrossRef] [PubMed]
- Jeromson, S.; Gallagher, I.J.; Galloway, S.D.; Hamilton, D.L. Omega-3 Fatty Acids and Skeletal Muscle Health. Mar. Drugs 2015, 13, 6977–7004. [Google Scholar] [CrossRef]
- Smith, G.I.; Julliand, S.; Reeds, D.N.; Sinacore, D.R.; Klein, S.; Mittendorfer, B. Fish oil-derived n-3 PUFA therapy increases muscle mass and function in healthy older adults. Am. J. Clin. Nutr. 2015, 102, 115–122. [Google Scholar] [CrossRef] [PubMed]
- Smith, G.I.; Atherton, P.; Reeds, D.N.; Mohammed, B.S.; Rankin, D.; Rennie, M.J.; Mittendorfer, B. Dietary omega-3 fatty acid supplementation increases the rate of muscle protein synthesis in older adults: A randomized controlled trial. Am. J. Clin. Nutr. 2011, 93, 402–412. [Google Scholar] [CrossRef]
- Dupont, J.; Dedeyne, L.; Dalle, S.; Koppo, K.; Gielen, E. The role of omega-3 in the prevention and treatment of sarcopenia. Aging Clin. Exp. Res. 2019, 31, 825–836. [Google Scholar] [CrossRef]
- Soininen, H.; Solomon, A.; Visser, P.J.; Hendrix, S.B.; Blennow, K.; Kivipelto, M.; Hartmann, T. 36-month LipiDiDiet multinutrient clinical trial in prodromal Alzheimer’s disease. Alzheimers Dement. 2021, 17, 29–40. [Google Scholar] [CrossRef]
- Wurtman, R.J. A Nutrient Combination that Can Affect Synapse Formation. Nutrients 2014, 6, 1701–1710. [Google Scholar] [CrossRef]
- Rossato, L.T.; Schoenfeld, B.J.; de Oliveira, E.P. Is there sufficient evidence to supplement omega-3 fatty acids to increase muscle mass and strength in young and older adults? Clin. Nutr. 2020, 39, 23–32. [Google Scholar] [CrossRef]
- Houston, D.K.; Nicklas, B.J.; Ding, J.; Harris, T.B.; Tylavsky, F.A.; Newman, A.B.; Lee, J.S.; Sahyoun, N.R.; Visser, M.; Kritchevsky, S.B. Dietary protein intake is associated with lean mass change in older, community-dwelling adults: The Health, Aging, and Body Composition (Health ABC) Study. Am. J. Clin. Nutr. 2008, 87, 150–155. [Google Scholar] [CrossRef]
- Ni Lochlainn, M.; Bowyer, R.C.E.; Welch, A.A.; Whelan, K.; Steves, C.J. Higher dietary protein intake is associated with sarcopenia in older British twins. Age Ageing 2023, 52, afad018. [Google Scholar] [CrossRef]

{kind=link}
| Characteristic * | Males | Females | Overall | p-Value ** |
|---|---|---|---|---|
| (n = 311) | (n = 408) | (n = 719) | ||
| Age | 70.54 (0.26) | 70.54 (0.25) | 70.54 (0.26) | 0.812 |
| BMI (kg/m2) | 26.3 (3.9) | 25.9 (4.7) | 26.1 (4.4) | 0.257 |
| BMI class | ||||
| Less than 18.5 | 1 (0.3%) | 9 (2.2%) | 10 (1.4%) | 0.001 |
| 18.5–25 | 121 (39%) | 195 (48%) | 316 (44%) | |
| 25–30 | 144 (46%) | 136 (33%) | 280 (39%) | |
| 30 and above | 45 (14%) | 68 (17%) | 113 (16%) | |
| Handgrip strength (kPa) | 87 (15) | 74 (14) | 80 (16) | <0.001 |
| Handgrip strength (kPa) class | ||||
| Low | 281 (90%) | 366 (90%) | 647 (90%) | 0.774 |
| Normal | 30 (9.6%) | 42 (10%) | 72 (10%) | |
| Gait speed 30 m (m/s) | 1.32 (0.17) | 1.30 (0.18) | 1.31 (0.17) | 0.101 |
| Gait speed 30 m (m/s) class | ||||
| Low | 5 (1.6%) | 4 (1.0%) | 9 (1.3%) | 0.511 |
| Normal | 306 (98%) | 404 (99%) | 710 (99%) | |
| Appendicular Lean Soft Tissue (kg/m2) | 7.83 (0.77) | 6.21 (0.64) | 6.91 (1.07) | <0.001 |
| Muscle mass by Appendicular Lean Soft Tissue (kg/m2) | ||||
| Low | 269 (86%) | 362 (89%) | 631 (88%) | 0.366 |
| Normal | 42 (14%) | 46 (11%) | 88 (12%) | |
| Sarcopenia probable | ||||
| No | 281 (90%) | 366 (90%) | 647 (90%) | 0.774 |
| Yes | 30 (9.6%) | 42 (10%) | 72 (10%) | |
| Sarcopenia confirmed | ||||
| No | 300 (96%) | 403 (99%) | 703 (98%) | 0.037 |
| Yes | 11 (3.5%) | 5 (1.2%) | 16 (2.2%) | |
| Sarcopenia severe | ||||
| No | 300 (96%) | 403 (99%) | 703 (98%) | 0.037 |
| Yes | 11 (3.5%) | 5 (1.2%) | 16 (2.2%) |
| Characteristic * | Males | Females | Overall | p-Value ** |
|---|---|---|---|---|
| (n = 311) | (n = 408) | (n = 719) | ||
| Energy kcal | 2367 (510) | 1986 (433) | 2151 (504) | <0.001 |
| Protein (g) | 95 (22) | 82 (20) | 88 (21) | <0.001 |
| Fat (g) | 96 (27) | 83 (26) | 88 (27) | <0.001 |
| Carbohydrates (g) | 239 (66) | 199 (55) | 216 (64) | <0.001 |
| Fibers (g) | 27 (9) | 25 (8) | 26 (8) | <0.001 |
| Vitamin C (mg) | 149 (79) | 151 (73) | 150 (76) | 0.759 |
| Iron (mg) | 13.1 (3.3) | 11.5 (3.4) | 12.2 (3.4) | <0.001 |
| Calcium (mg) | 1069 (417) | 1016 (370) | 1039 (392) | 0.078 |
| Retinol equivalent (µg) | 1263 (787) | 1048 (543) | 1141 (668) | <0.001 |
| Vitamin D (µg) | 9.7 (4.6) | 8.3 (3.6) | 8.9 (4.1) | <0.001 |
| Vitamin E (mg) | 16 (12) | 16 (15) | 16 (14) | 0.782 |
| Thiamine (mg) | 1.49 (0.38) | 1.29 (0.35) | 1.38 (0.38) | <0.001 |
| Riboflavin (mg) | 1.90 (0.57) | 1.67 (0.50) | 1.77 (0.54) | <0.001 |
| Niacin equivalent (mg) | 41 (9) | 35 (8) | 38 (9) | <0.001 |
| Vitamin B6 (mg) | 2.45 (0.82) | 2.26 (0.90) | 2.34 (0.87) | 0.003 |
| Vitamin B12 (µg) | 7.84 (3.92) | 6.45 (2.92) | 7.05 (3.45) | <0.001 |
| Phosphorus (mg) | 1680 (413) | 1482 (387) | 1568 (410) | <0.001 |
| Magnesium (mg) | 419 (103) | 374 (101) | 394 (104) | <0.001 |
| Potassium (mg) | 3880 (962) | 3513 (809) | 3672 (897) | <0.001 |
| Zinc (mg) | 12.41 (2.98) | 10.70 (2.76) | 11.44 (2.98) | <0.001 |
| Alcohol (g) | 16 (16) | 9 (10) | 12 (14) | <0.001 |
| Saturated fatty acids (g) | 38 (13) | 33 (13) | 35 (13) | <0.001 |
| Monounsaturated fatty acids (g) | 35 (10) | 30 (9) | 32 (10) | <0.001 |
| Polyunsaturated fatty acids (g) | 14.9 (5.9) | 13.2 (5.6) | 13.9 (5.8) | <0.001 |
| EPA (Fatty acid 20:5) (g) | 0.26 (0.20) | 0.22 (0.16) | 0.24 (0.18) | 0.014 |
| DHA (Fatty acid 22:6) (g) | 0.61 (0.45) | 0.54 (0.37) | 0.57 (0.41) | 0.028 |
| Folate (µg) | 359 (108) | 345 (107) | 351 (107) | 0.083 |
| Selenium (µg) | 57 (18) | 52 (16) | 54 (17) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Borda, M.G.; Samuelsson, J.; Cederholm, T.; Baldera, J.P.; Pérez-Zepeda, M.U.; Barreto, G.E.; Zettergren, A.; Kern, S.; Rydén, L.; Gonzalez-Lara, M.; et al. Nutrient Intake and Its Association with Appendicular Total Lean Mass and Muscle Function and Strength in Older Adults: A Population-Based Study. Nutrients 2024, 16, 568. https://doi.org/10.3390/nu16040568
Borda MG, Samuelsson J, Cederholm T, Baldera JP, Pérez-Zepeda MU, Barreto GE, Zettergren A, Kern S, Rydén L, Gonzalez-Lara M, et al. Nutrient Intake and Its Association with Appendicular Total Lean Mass and Muscle Function and Strength in Older Adults: A Population-Based Study. Nutrients. 2024; 16(4):568. https://doi.org/10.3390/nu16040568
Chicago/Turabian StyleBorda, Miguel Germán, Jessica Samuelsson, Tommy Cederholm, Jonathan Patricio Baldera, Mario Ulises Pérez-Zepeda, George E. Barreto, Anna Zettergren, Silke Kern, Lina Rydén, Mariana Gonzalez-Lara, and et al. 2024. "Nutrient Intake and Its Association with Appendicular Total Lean Mass and Muscle Function and Strength in Older Adults: A Population-Based Study" Nutrients 16, no. 4: 568. https://doi.org/10.3390/nu16040568
APA StyleBorda, M. G., Samuelsson, J., Cederholm, T., Baldera, J. P., Pérez-Zepeda, M. U., Barreto, G. E., Zettergren, A., Kern, S., Rydén, L., Gonzalez-Lara, M., Salazar-Londoño, S., Duque, G., Skoog, I., & Aarsland, D. (2024). Nutrient Intake and Its Association with Appendicular Total Lean Mass and Muscle Function and Strength in Older Adults: A Population-Based Study. Nutrients, 16(4), 568. https://doi.org/10.3390/nu16040568