

Dietary Provision, GLIM-Defined Malnutrition and Their Association with Clinical Outcome: Results from the First Decade of nutritionDay in China

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
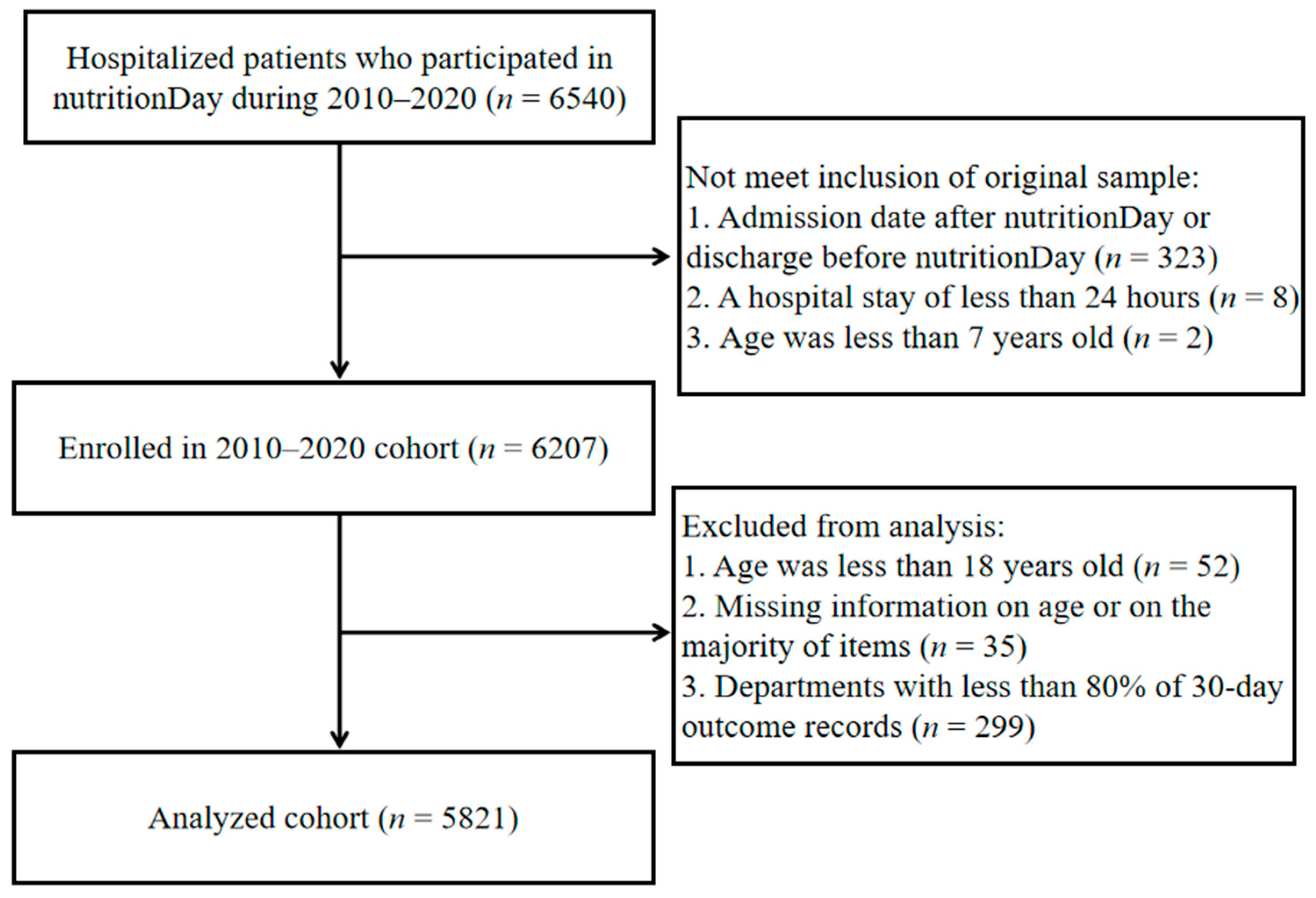
2.1. Study Population
2.2. Data Collection
2.3. Nutritional Status Evaluation
2.4. Outcomes
2.5. Statistical Analysis
3. Results
3.1. Demographic Characteristics of the Hospitalized Patients
3.2. Dietary Provision with Meal Consumption on nutritionDay
3.3. GLIM Diagnostic Flow Chart with Dietary Provision and Good 30-Day Outcome
3.4. Dietary Provision and Malnutrition Diagnosis Associated with Good 30-Day Outcome
3.5. Cumulative Incidence of Good Outcome within 30 Days after nutritionDay
4. Discussion
4.1. Dietary Provision with Meal Consumption on nutritionDay
4.2. GLIM Diagnostic Flow Chart with Dietary Provision and Good 30-Day Outcome
4.3. Dietary Provision and Malnutrition Diagnosis Associated with Good 30-Day Outcome
4.4. Cumulative Incidence of Good Outcome within 30 Days after nutritionDay
4.5. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Schuetz, P.; Seres, D.; Lobo, D.N.; Gomes, F.; Kaegi-Braun, N.; Stanga, Z. Management of disease-related malnutrition for patients being treated in hospital. Lancet 2021, 398, 1927–1938. [Google Scholar] [CrossRef]
- Cass, A.R.; Charlton, K.E. Prevalence of hospital-acquired malnutrition and modifiable determinants of nutritional deterioration during inpatient admissions: A systematic review of the evidence. J. Hum. Nutr. Diet 2022, 35, 1043–1058. [Google Scholar] [CrossRef]
- Steiber, A.; Hegazi, R.; Herrera, M.; Zamor, M.L.; Chimanya, K.; Pekcan, A.G.; Redondo-Samin, D.C.; Correia, M.I.; Ojwang, A.A. Spotlight on Global Malnutrition: A Continuing Challenge in the 21st Century. J. Acad. Nutr. Diet 2015, 115, 1335–1341. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Wang, X.; Huang, Y.; Gao, Y.; Peng, N.; Zhu, W.; Li, N.; Li, J. NutritionDay 2010 audit in Jinling hospital of China. Asia Pac. J. Clin. Nutr. 2013, 22, 206–213. [Google Scholar]
- Hiesmayr, M.; Schindler, K.; Pernicka, E.; Schuh, C.; Schoeniger-Hekele, A.; Bauer, P.; Laviano, A.; Lovell, A.D.; Mouhieddine, M.; Schuetz, T.; et al. Decreased food intake is a risk factor for mortality in hospitalised patients: The NutritionDay survey 2006. Clin. Nutr. 2009, 28, 484–491. [Google Scholar] [CrossRef] [PubMed]
- Frantal, S.; Pernicka, E.; Hiesmayr, M.; Schindler, K.; Bauer, P. Length bias correction in one-day cross-sectional assessments—The NutritionDay study. Clin. Nutr. 2016, 35, 522–527. [Google Scholar] [CrossRef] [PubMed]
- Barker, L.A.; Gout, B.S.; Crow, T.C. Hospital malnutrition: Prevalence, identification and impact on patients and the healthcare system. Int. J. Environ. Res. Public Health 2011, 8, 514–527. [Google Scholar] [CrossRef]
- Jensen, G.L.; Compher, C.; Sullivan, D.H.; Mullin, G.E. Recognizing malnutrition in adults: Definitions and characteristics, screening, assessment, and team approach. J. Parenter. Enter. Nutr. 2013, 37, 802–807. [Google Scholar] [CrossRef] [PubMed]
- Cederholm, T.; Jensen, G.L.; Correia, M.I.T.D.; Gonzalez, M.C.; Fukushima, R.; Higashiguchi, T.; Baptista, G.; Barazzoni, R.; Blaauw, R.; Coats, A.; et al. GLIM criteria for the diagnosis of malnutrition—A consensus report from the global clinical nutrition community. Clin. Nutr. 2019, 38, 1–9. [Google Scholar] [CrossRef]
- Volpp, K.G.; Berkowitz, S.A.; Sharma, S.V.; Anderson, C.A.M.; Brewer, L.C.; Elkind, M.S.V.; Gardner, C.D.; Gervis, J.E.; Harrington, R.A.; Herrero, M.; et al. Food Is Medicine: A Presidential Advisory from the American Heart Association. Circulation 2023, 148, 1417–1439. [Google Scholar] [CrossRef]
- Reznikov, E.A.; Suskind, D.L. Current Nutritional Therapies in Inflammatory Bowel Disease: Improving Clinical Remission Rates and Sustainability of Long-Term Dietary Therapies. Nutrients 2023, 15, 668. [Google Scholar] [CrossRef]
- Castro-Barquero, S.; Ruiz-León, A.M.; Sierra-Pérez, M.; Estruch, R.; Casas, R. Dietary Strategies for Metabolic Syndrome: A Comprehensive Review. Nutrients 2020, 12, 2983. [Google Scholar] [CrossRef]
- Kahleova, H.; Levin, S.; Barnard, N. Cardio-Metabolic Benefits of Plant-Based Diets. Nutrients 2017, 9, 848. [Google Scholar] [CrossRef] [PubMed]
- Che, X.; Gross, S.M.; Wang, G.; Hong, X.; Pearson, C.; Bartell, T.; Wang, X. Impact of consuming a Mediterranean-style diet during pregnancy on neurodevelopmental disabilities in offspring: Results from the Boston Birth Cohort. Precis. Nutr. 2023, 2, e00047. [Google Scholar]
- Lesser, M.N.R.; Lesser, L.I. Nutrition Support Therapy. Am. Fam. Physician 2021, 104, 580–588. [Google Scholar]
- Kaegi-Braun, N.; Mueller, M.; Schuetz, P.; Mueller, B.; Kutz, A. Evaluation of Nutritional Support and In-Hospital Mortality in Patients With Malnutrition. JAMA Netw. Open 2021, 4, e2033433. [Google Scholar] [CrossRef]
- Sun, H.; Zhang, L.; Zhang, P.; Yu, J.; Kang, W.; Guo, S.; Chen, W.; Li, X.; Wang, S.; Chen, L.; et al. A comprehensive nutritional survey of hospitalized patients: Results from nutritionDay 2016 in China. PLoS ONE 2018, 13, e0194312. [Google Scholar] [CrossRef]
- Sauer, A.C.; Goates, S.; Malone, A.; Mogensen, K.M.; Gewirtz, G.; Sulz, I.; Moick, S.; Laviano, A.; Hiesmayr, M. Prevalence of Malnutrition Risk and the Impact of Nutrition Risk on Hospital Outcomes: Results from NutritionDay in the U.S. J. Parenter. Enter. Nutr. 2019, 43, 918–926. [Google Scholar] [CrossRef] [PubMed]
- Stratton, R.J.; Hackston, A.; Longmore, D.; Dixon, R.; Price, S.; Stroud, M.; King, C.; Elia, M. Malnutrition in hospital outpatients and inpatients: Prevalence, concurrent validity and ease of use of the ‘malnutrition universal screening tool’ (‘MUST’) for adults. Br. J. Nutr. 2004, 92, 799–808. [Google Scholar] [CrossRef] [PubMed]
- Rabito, E.I.; Marcadenti, A.; da Silva Fink, J.; Figueira, L.; Silva, F.M. Nutritional Risk Screening 2002, Short Nutritional Assessment Questionnaire, malnutrition screening tool, and malnutrition universal screening tool are good predictors of nutrition risk in an emergency service. Nutr. Clin. Pract. 2017, 32, 526–532. [Google Scholar] [CrossRef]
- Kruizenga, H.; van Keeken, S.; Weijs, P.; Bastiaanse, L.; Beijer, S.; Huisman-de Waal, G.; Jager-Wittenaar, H.; Jonkers-Schuitema, C.; Klos, M.; Remijnse-Meester, W.; et al. Undernutrition screening survey in 564,063 patients: Patients with a positive undernutrition screening score stay in hospital 1.4 d longer. Am. J. Clin. Nutr. 2016, 103, 1026–1032. [Google Scholar] [CrossRef]
- Wang, M.; Guo, Q.; Liu, H.; Liu, M.; Tang, C.; Wu, J.; Feng, G.; Wu, W. GLIM criteria using NRS-2002 and MUST as the first step adequately diagnose the malnutrition in Crohn’s disease inpatients: A retrospective study. Front. Nutr. 2023, 9, 1059191. [Google Scholar] [CrossRef]
- Moick, S.; Hiesmayr, M.; Mouhieddine, M.; Kiss, N.; Bauer, P.; Sulz, I.; Singer, P.; Simon, J. Reducing the knowledge to action gap in hospital nutrition care—Developing and implementing NutritionDay 2.0. Clin. Nutr. 2021, 40, 936–945. [Google Scholar] [CrossRef]
- Ostrowska, J.; Sulz, I.; Tarantino, S.; Hiesmayr, M.; Szostak-Węgierek, D. Hospital Malnutrition, Nutritional Risk Factors, and Elements of Nutritional Care in Europe: Comparison of Polish Results with All European Countries Participating in the nDay Survey. Nutrients 2021, 13, 263. [Google Scholar] [CrossRef]
- Lang, T.; Mason, P. Sustainable diet policy development: Implications of multi-criteria and other approaches, 2008–2017. Proc. Nutr. Soc. 2018, 77, 331–346. [Google Scholar] [CrossRef] [PubMed]
- Garnica Rosas, L.; Mensink, G.B.M.; Finger, J.D.; Schienkiewitz, A.; Do, S.; Wolters, M.; Stanley, I.; Abu Omar, K.; Wieczorowska-Tobis, K.; Woods, C.B.; et al. Selection of key indicators for European policy monitoring and surveillance for dietary behaviour, physical activity and sedentary behaviour. Int. J. Behav. Nutr. Phys. Act. 2021, 18, 48. [Google Scholar] [CrossRef] [PubMed]
- Fismen, A.S.; Mathisen, J.R.; Vlad, I.; Oldridge-Turner, K.; O’Mara, J.; Klepp, K.I.; Brinsden, H.; Rutter, H.; Kokkorou, M.; Helleve, A. Pilot test of the NOURISHING policy index-Assessing governmental nutrition policies in five European countries. Obes. Rev. 2023, 24 (Suppl. S1), e13532. [Google Scholar] [CrossRef]
- Weldon, I.; Parkhurst, J. Governing evidence use in the nutrition policy process: Evidence and lessons from the 2020 Canada food guide. Nutr. Rev. 2022, 80, 467–478. [Google Scholar] [CrossRef]
- Neale, E.P.; Tapsell, L.C. Perspective: The Evidence-Based Framework in Nutrition and Dietetics: Implementation, Challenges, and Future Directions. Adv. Nutr. 2019, 10, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Bannerman, E.; Cantwell, L.; Gaff, L.; Conroy, A.; Davidson, I.; Jones, J. Dietary intakes in geriatric orthopaedic rehabilitation patients: Need to look at food consumption not just provision. Clin. Nutr. 2016, 35, 892–899. [Google Scholar] [CrossRef]
- Lima, J.; Brizola Dias, A.J.; Burgel, C.F.; Bernardes, S.; Gonzalez, M.C.; Silva, F.M. Complementarity of nutritional screening tools to GLIM criteria on malnutrition diagnosis in hospitalised patients: A secondary analysis of a longitudinal study. Clin. Nutr. 2022, 41, 2325–2332. [Google Scholar] [CrossRef] [PubMed]
- Tran, Q.C.; Banks, M.; Hannan-Jones, M.; Do, T.N.D.; Gallegos, D. Validity of four nutritional screening tools against subjective global assessment for inpatient adults in a low-middle income country in Asia. Eur. J. Clin. Nutr. 2018, 72, 979–985. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.Y.; Zhu, M.W.; Zhang, H.; Li, L.; Tang, P.X.; Chen, W.; Wei, J.M. A Cross-Sectional Study of GLIM-Defined Malnutrition Based on New Validated Calf Circumference Cut-off Values and Different Screening Tools in Hospitalised Patients over 70 Years Old. J. Nutr. Health Aging 2020, 24, 832–838. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.Y.; Zhang, X.N.; Jiang, Z.M.; Jie, B.; Wang, Y.; Li, W.; Kondrup, J.; Nolan, M.T.; Andrews, M.; Kang, W.M.; et al. Nutritional support therapy after GLIM criteria may neglect the benefit of reducing infection complications compared with NRS2002: Reanalysis of a cohort study. Nutrition 2020, 79–80, 110802. [Google Scholar] [CrossRef] [PubMed]
- Groothof, D.; Post, A.; Polinder-Bos, H.A.; Hazenberg, B.P.C.; Gans, R.O.B.; Bakker, S.J.L. Muscle mass versus body mass index as predictor of adverse outcome. J. Cachexia Sarcopenia Muscle 2021, 12, 517–518. [Google Scholar] [CrossRef] [PubMed]
- Yugawa, K.; Itoh, S.; Kurihara, T.; Yoshiya, S.; Mano, Y.; Takeishi, K.; Harada, N.; Ikegami, T.; Soejima, Y.; Mori, M.; et al. Skeletal muscle mass predicts the prognosis of patients with intrahepatic cholangiocarcinoma. Am. J. Surg. 2019, 218, 952–958. [Google Scholar] [CrossRef] [PubMed]
- De Giorgi, A.; Marra, A.M.; Iacoviello, M.; Triggiani, V.; Rengo, G.; Cacciatore, F.; Maiello, C.; Limongelli, G.; Masarone, D.; Perticone, F.; et al. Insulin-like growth factor-1 (IGF-1) as predictor of cardiovascular mortality in heart failure patients: Data from the T.O.S.CA. registry. Intern. Emerg. Med. 2022, 17, 1651–1660. [Google Scholar] [CrossRef]
- Thibault, R.; Abbasoglu, O.; Ioannou, E.; Meija, L.; Ottens-Oussoren, K.; Pichard, C.; Rothenberg, E.; Rubin, D.; Siljamäki-Ojansuu, U.; Vaillant, M.F.; et al. ESPEN guideline on hospital nutrition. Clin. Nutr. 2021, 40, 5684–5709. [Google Scholar] [CrossRef]
- Ridley, E.J.; Chapple, L.S.; Chapman, M.J. Nutrition intake in the post-ICU hospitalization period. Curr. Opin. Clin. Nutr. Metab. Care 2020, 23, 111–115. [Google Scholar] [CrossRef]
- Coghlan, B.; Coghlan, S.; Wilson, A. Nutrition education fit for modern health systems. Lancet 2019, 394, 2071. [Google Scholar] [CrossRef]
- van den Berg, G.H.; Huisman-de Waal, G.G.J.; Vermeulen, H.; de van der Schueren, M.A.E. Effects of nursing nutrition interventions on outcomes in malnourished hospital inpatients and nursing home residents: A systematic review. Int. J. Nurs. Stud. 2021, 117, 103888. [Google Scholar] [CrossRef]
- Roberts, H.C.; Pilgrim, A.L.; Jameson, K.A.; Cooper, C.; Sayer, A.A.; Robinson, S. The Impact of Trained Volunteer Mealtime Assistants on the Dietary Intake of Older Female In-Patients: The Southampton Mealtime Assistance Study. J. Nutr. Health Aging 2017, 21, 320–328. [Google Scholar] [CrossRef]
- Downer, S.; Berkowitz, S.A.; Harlan, T.S.; Olstad, D.L.; Mozaffarian, D. Food is medicine: Actions to integrate food and nutrition into healthcare. BMJ 2020, 369, m2482. [Google Scholar] [CrossRef]
- Laur, C.; McCullough, J.; Davidson, B.; Keller, H. Becoming Food Aware in Hospital: A Narrative Review to Advance the Culture of Nutrition Care in Hospitals. Healthcare 2015, 3, 393–407. [Google Scholar] [CrossRef]
- Agarwal, E.; Ferguson, M.; Banks, M.; Vivanti, A.; Batterham, M.; Bauer, J.; Capra, S.; Isenring, E. Malnutrition, poor food intake, and adverse healthcare outcomes in non-critically ill obese acute care hospital patients. Clin. Nutr. 2019, 38, 759–766. [Google Scholar] [CrossRef] [PubMed]
- Khoury, T.; Ilan, Y. Platform introducing individually tailored variability in nerve stimulations and dietary regimen to prevent weight regain following weight loss in patients with obesity. Obes. Res. Clin. Pract. 2021, 15, 114–123. [Google Scholar] [CrossRef] [PubMed]
- Carino, S.; Collins, J.; Malekpour, S.; Porter, J. Harnessing the pillars of institutions to drive environmentally sustainable hospital foodservices. Front. Nutr. 2022, 9, 905932. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Median (IQR) or n (%) | |
|---|---|
| Age, years, median (IQR) | 58.0 (45.0–67.0) |
| Sex [female/male/unknown, n (%)] | 2352 (40.4%)/3461 (59.5%)/8 (0.1%) |
| BMI, kg/m2, median (IQR) | 22.8 (20.2–25.2) |
| BMI < 18.5 kg/m2, n (%) | 710 (12.2%) |
| Surgical patients, n (%) | 1797 (30.9%) |
| Weight loss within the last 3 months, n (%) | 2246 (38.6%) |
| Less than half of normal food intake in the previous week, n (%) | 1152 (19.8%) |
| Dietary provision [hospital food/special diet/both, n (%)] | 3015 (51.8%)/ 2699 (46.4%)/239 (4.1%)/77 (1.3%) |
| Full meal eaten on nutritionDay, n (%) | 2173 (37.3%) |
| Full meal not eaten on nutritionDay, n (%) | 3372 (57.9%) |
| Full meal not eaten due to not being allowed to eat, n (%) | 968 (16.6%) |
| Full meal not eaten due to decreased appetite, n (%) | 930 (16.0%) |
| At risk of malnutrition defined by MUST, MUST ≥ 1, n (%) | 1924 (33.1%) |
| Malnutrition defined by GLIM, n (%) | 1328 (22.8%) |
| LOS after nutritionDay, days, median (IQR) | 6.0 (3.0–12.0) |
| Good 30-day outcome, n (%) | 5093 (87.5%) |
| Eating on nutritionDay | n | Type of Nutritional Provision (Row Percentages) | ||||||
|---|---|---|---|---|---|---|---|---|
| Food/Diet | Multi-form of Food and Artificial Nutrition | No Food/Diet | Unsure/Missing | |||||
| Hospital food (regular and fortified/enriched hospital food) | Special diet | Multi-form of food and diet | Artificial nutrition a | Nothing | ||||
| All | 5821 | 46.4% | 4.1% | 1.3% | 10.5% | 23.2% | 3.3% | 11.2% |
| Eaten all | 2173 | 64.5% | 4.8% | 1.7% | 10.3% | 8.2% | 2.0% | 8.4% |
| Eaten half | 1176 | 56.5% | 5.6% | 1.9% | 12.9% | 12.3% | 2.9% | 7.8% |
| Eaten quarter | 558 | 37.8% | 6.1% | 1.8% | 17.2% | 26.5% | 2.0% | 8.6% |
| Eaten nothing but allowed to eat | 721 | 36.9% | 3.6% | 1.0% | 8.7% | 25.2% | 4.7% | 19.8% |
| Eaten nothing due to not being allowed to eat | 917 | 9.9% | 0.5% | 0% | 5.1% | 63.8% | 6.5% | 14.1% |
| Missing data | 276 | 23.2% | 1.1% | 0% | 11.6% | 40.6% | 2.9% | 20.7% |
| Model Ⅰ | Model II (Including GLIM) | Model III (Including Malnutrition Diagnosis with Dietary Provision) | ||
|---|---|---|---|---|
| Variable | Category | HR [95% CI] | HR [95% CI] | HR [95% CI] |
| Dietary provision | No food/diet | Reference | Reference | |
| Food/diet | 1.47 [1.35–1.60] *** | 1.49 [1.38–1.61] *** | ||
| Multi-form of food and artificial nutrition | 1.26 [1.13–1.41] *** | 1.29 [1.16–1.43] *** | ||
| Unsure or missing | 1.43 [1.28–1.60] *** | 1.44 [1.29–1.61] *** | ||
| Malnutrition defined by GLIM | No | Reference | ||
| Yes | 0.83 [0.77–0.89] *** | |||
| Undefined | 0.97 [0.88–1.08] | |||
| Malnutrition diagnosis with dietary provision | Malnutrition without food/diet | Reference | ||
| Malnutrition with food/diet | 1.58 [1.36–1.83] *** | |||
| Malnutrition with multi-form of food and artificial nutrition | 1.34 [1.11–1.63] ** | |||
| Non-malnutrition without food/diet | 1.29 [1.13–1.46] *** | |||
| Non-malnutrition with food/diet | 1.86 [1.64–2.11] *** | |||
| Non-malnutrition with multi-form of food and artificial nutrition | 1.56 [1.33–1.81] *** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhou, B.; Zhang, Y.; Hiesmayr, M.; Gao, X.; Huang, Y.; Liu, S.; Shen, R.; Zhao, Y.; Cui, Y.; Zhang, L.; et al. Dietary Provision, GLIM-Defined Malnutrition and Their Association with Clinical Outcome: Results from the First Decade of nutritionDay in China. Nutrients 2024, 16, 569. https://doi.org/10.3390/nu16040569
Zhou B, Zhang Y, Hiesmayr M, Gao X, Huang Y, Liu S, Shen R, Zhao Y, Cui Y, Zhang L, et al. Dietary Provision, GLIM-Defined Malnutrition and Their Association with Clinical Outcome: Results from the First Decade of nutritionDay in China. Nutrients. 2024; 16(4):569. https://doi.org/10.3390/nu16040569
Chicago/Turabian StyleZhou, Bei, Yupeng Zhang, Michael Hiesmayr, Xuejin Gao, Yingchun Huang, Sitong Liu, Ruting Shen, Yang Zhao, Yao Cui, Li Zhang, and et al. 2024. "Dietary Provision, GLIM-Defined Malnutrition and Their Association with Clinical Outcome: Results from the First Decade of nutritionDay in China" Nutrients 16, no. 4: 569. https://doi.org/10.3390/nu16040569
APA StyleZhou, B., Zhang, Y., Hiesmayr, M., Gao, X., Huang, Y., Liu, S., Shen, R., Zhao, Y., Cui, Y., Zhang, L., Wang, X., & on behalf of the nutritionDay Chinese Working Group. (2024). Dietary Provision, GLIM-Defined Malnutrition and Their Association with Clinical Outcome: Results from the First Decade of nutritionDay in China. Nutrients, 16(4), 569. https://doi.org/10.3390/nu16040569