

Study Protocol for a Controlled Trial of Nutrition Education Intervention about Celiac Disease in Primary School: ZELIAKIDE Project

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Description
2.2. Participants
2.3. Sample Size Calculation
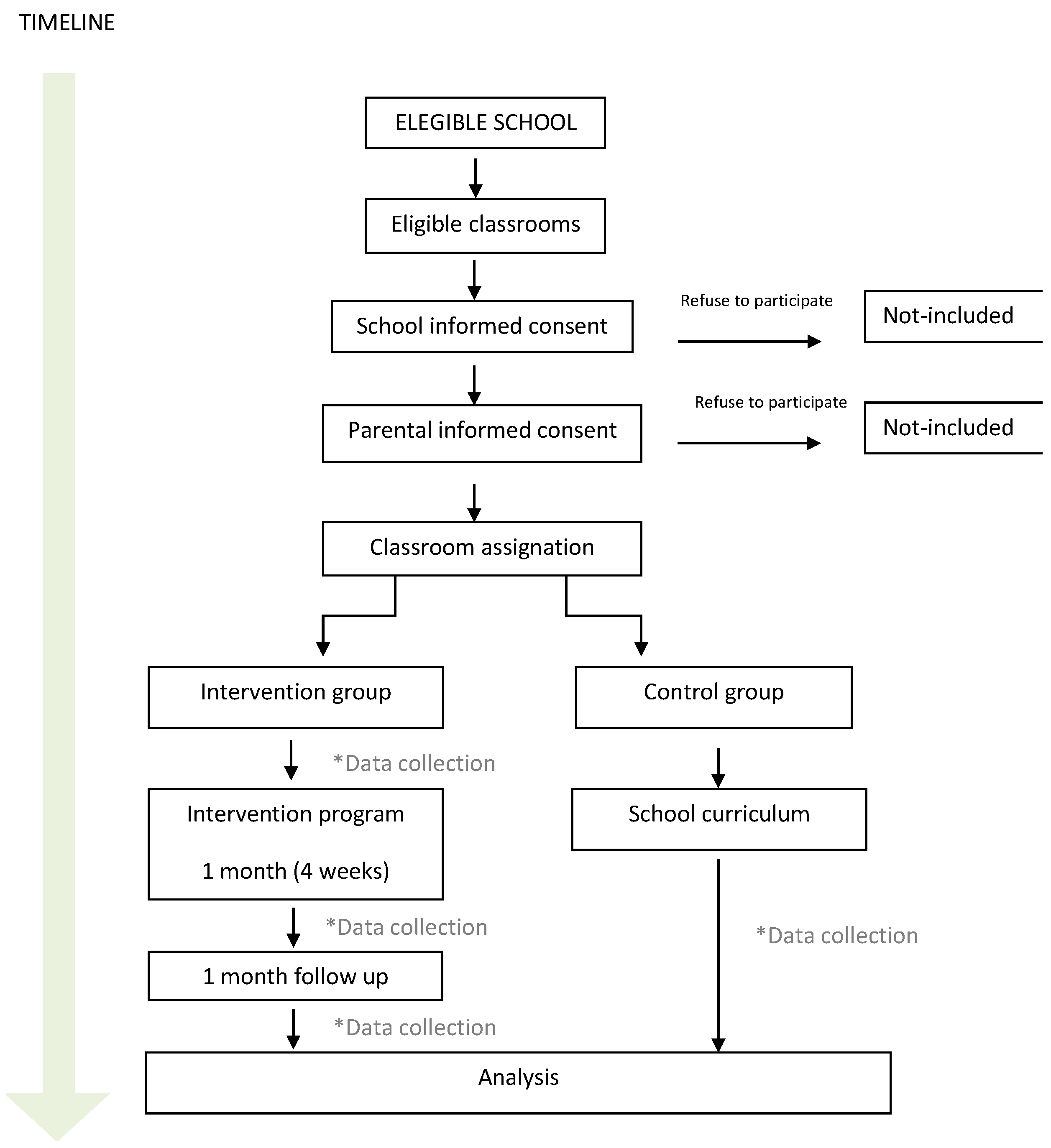
2.4. Allocation to Groups
2.5. Intervention
2.5.1. Intervention Design
2.5.2. Study Procedure
2.6. Outcome Measures
2.6.1. Primary Outcomes
2.6.2. Secondary Outcomes
- Opinion of the parents/guardians of the children in relation to the project: it will be completed by parents/guardians, online and without the presence of any member of the research group.
- Opinion of the children about the project reported by their parents/guardians: it will be completed by parents/guardians, online and without the presence of any member of the research group.
2.7. Data Management and Monitoring
2.8. Statistical Analysis
3. Discussion
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Competence | Question | Response | |
|---|---|---|---|
| 1 | Do you know which foods are found in the different parts of the food pyramid? | Yes/No/No response | |
| Which foods are at the top of the pyramid? | Open question | ||
| Which foods are at the bottom of the pyramid? | Open question | ||
| Of the food pairs below, which do you think is highest in the food pyramid? | Tomato/Sweet, Pizza/Rice, Bread/Juice, Olive oil/Red meat, Potato/Ham | ||
| 2 | Of the foods you eat during the day, do you know which are unhealthy? | Yes/No | |
| Which are the unhealthy foods you eat? | Open question | ||
| Are the foods that are often featured in advertisements usually healthy? | Yes/No/There is a bit of everything | ||
| How much fruit and vegetables should you eat per day? | Open question | ||
| What do you think you should improve your diet, for example, by eating more fruit, less sweets? | Open question | ||
| 3 | How many days a week do you usually take a healthy lunch to school (fruit, dairy products, wholemeal bread…)? | Scale 0 days–5 days | |
| Of the foods at the top of the food pyramid, how many do you eat at the weekend? | I eat them on Fridays, Saturdays and Sundays, more than once a day. I eat them on Fridays, Saturdays and Sundays, once a day. I only eat them one day at the weekend. I don’t eat them every weekend, only once in a while. | ||
| Do you think it is important to eat a healthy diet? | No, if you do sport it is enough Yes, it is important but it is better for everyone to eat what they want Yes, it is very important for me. | ||
| With what you have learned in these sessions, do you think you are able to improve your diet? | Yes, I know what mistakes I make in my diet and I am able to improve it Yes, I have learned a lot but I am not able to improve my diet No, I have not learned enough | ||
| In the last month, have you eaten more, less or the same amount of the following food groups? (dairy products, fruits, vegetables, meat, fish, pulses, cereals, sweets) | Less/Equal/More/I do not know/No response | ||
| 4 | How much do you know about CD? | Scale 0 (nothing)–4 (much) | |
| What symptoms do people with CD have? | Open question | ||
| When do people with CD develop symptoms? | Open question | ||
| What compound in food is harmful to people with CD? | Open question | ||
| 5 | How do you think people with CD feel? | Open question | |
| Does a person with CD enjoy eating? | Scale 0 (nothing)–4 (much) | ||
| What would you do if it was your birthday and a classmate had CD? | Bring the cake that I like the most. Bring the cake that I like the most and another gluten-free cake for the person with CD. Bring a gluten-free cake for everyone. No response. | ||
| 6 | Where is the gluten? | Open question | |
| What makes a dough elastic? | Gluten Water I do not know | ||
| How can we know (without experimenting) whether a food contains gluten or not? | Open question | ||
| Which symbols indicate that a food does not contain gluten? | Open question | ||
| 7 | Which of the following foods a person with CD cannot eat? | Meat and fish Eggs and dairy Fruit and vegetables Wheat-based products: biscuits, bread and pasta Rice and maize Sweets They can eat anything I do not know | |
| From the following list of foods, which ones may contain gluten? | Raw rice, raw beans, fresh fruits, fresh vegetables, natural dairy products, fresh meat or fish, biscuits, some sweets, sweetened cocoa powder, some ice-creams, chocolate | ||
| Can a prepared food (cream of vegetables, prepared beans…) have gluten, even if it is made from gluten-free ingredients? | Yes/No | ||
| 8 | Please rate these sentences according to your level of agreement. | In order to detect gluten, laboratory experiments must be carried out. | Scale 1 (not agree)–5 (very agree) |
| It is important for scientists to do experiments. | Scale 1 (not agree)–5 (very agree) | ||
| In the future I would like to become a scientist. | Scale 1 (not agree)–5 (very agree) | ||
| Researchers are crazy, weird and male. | Scale 1 (not agree)–5 (very agree) | ||
References
- Husby, S.; Koletzko, S.; Korponay-Szabó, I.; Kurppa, K.; Mearin, M.L.; Ribes-Koninckx, C.; Shamir, R.; Troncone, R.; Auricchio, R.; Castillejo, G.; et al. European Society Paediatric Gastroenterology, Hepatology and Nutrition Guidelines for Diagnosing Coeliac Disease 2020. J. Pediatr. Gastroenterol. Nutr. 2020, 70, 141–156. [Google Scholar] [CrossRef] [PubMed]
- King, J.A.; Jeong, J.; Underwood, F.E.; Quan, J.; Panaccione, N.; Windsor, J.W.; Coward, S.; de Bruyn, J.; Ronksley, P.E.; Shaheen, A.A.; et al. Incidence of Celiac Disease Is Increasing Over Time: A Systematic Review and Meta-analysis. Am. J. Gastroenterol. 2020, 115, 507–525. [Google Scholar] [CrossRef] [PubMed]
- Nevoral, J. Celiac Disease in Children: What Has Changed? Int. J. Celiac Dis. 2014, 2, 18–23. [Google Scholar] [CrossRef][Green Version]
- Mustalahti, K.; Catassi, C.; Reunanen, A.; Fabiani, E.; Heier, M.; McMillan, S.; Murray, L.; Metzger, M.H.; Gasparin, M.; Bravi, E.; et al. The prevalence of celiac disease in Europe: Results of a centralized, international mass screening project. Ann. Med. 2010, 42, 587–595. [Google Scholar] [CrossRef] [PubMed]
- Lebwohl, B.; Rubio-Tapia, A. Epidemiology, Presentation, and Diagnosis of Celiac Disease. Gastroenterology 2021, 160, 63–75. [Google Scholar] [CrossRef] [PubMed]
- Stahl, M.; Li, Q.; Lynch, K.; Koletzko, S.; Mehta, P.; Gragert, L.; Norris, J.M.; Andrén Aronsson, C.; Lindfords, K.; Kurppa, K.; et al. Incidence of Pediatric Celiac Disease Varies by Region. Am. J. Gastroenterol. 2023, 118, 539–545. [Google Scholar] [CrossRef]
- Churruca, I.; Miranda, J.; Lasa, A.; Bustamante, M.; Larretxi, I.; Simon, E. Analysis of Body Composition and Food Habits of Spanish Celiac Women. Nutrients 2015, 7, 5515–5531. [Google Scholar] [CrossRef]
- González, T.; Larretxi, I.; Vitoria, J.C.; Castaño, L.; Simón, E.; Churruca, I.; Navarro, V.; Lasa, A. Celiac Male’s Gluten-Free Diet Profile: Comparison to that of the Control Population and Celiac Women. Nutrients 2018, 10, 1713. [Google Scholar] [CrossRef]
- Bascuñán, K.A.; Elli, L.; Pellegrini, N.; Scricciolo, A.; Lombardo, V.; Doneda, L.; Vecchi, M.; Scarpa, C.; Araya, M.; Roncoroni, L. Impact of FODMAP Content Restrictions on the Quality of Diet for Patients with Celiac Disease on a Gluten-Free Diet. Nutrients 2019, 11, 2220. [Google Scholar] [CrossRef]
- Jamieson, J.A.; Neufeld, A. Food sources of energy and nutrients among Canadian adults following a gluten-free diet. PeerJ 2020, 8, e9590. [Google Scholar] [CrossRef]
- Ballestero-Fernández, C.; Varela-Moreiras, G.; Úbeda, N.; Alonso-Aperte, E. Nutritional Status in Spanish Adults with Celiac Disease Following a Long-Term Gluten-Free Diet Is Similar to Non-Celiac. Nutrients 2021, 13, 1626. [Google Scholar] [CrossRef] [PubMed]
- Casellas, F.; Burgos, R.; Marcos, A.; Santos, J.; Ciriza-de-los-Ríos, C.; García-Manzanares, A.; Polanco, I.; Puy-Portillo, M.; Villarino, A.; Lema-Marqués, B.; et al. Documento de Consenso sobre las Dietas de Exclusión en el Síndrome del Intestino Irritable; Sociedad Española de Patología Digestiva (SEPD): Madrid, Spain, 2019. [Google Scholar]
- Sevinç, E.; Çetin, F.H.; Coşkun, B.D. Psychopathology, quality of life, and related factors in children with celiac disease. J. Pediatr. 2017, 93, 267–273. [Google Scholar] [CrossRef] [PubMed]
- Zysk, W.; Głąbska, D.; Guzek, D. Social and Emotional Fears and Worries Influencing the Quality of Life of Female Celiac Disease Patients Following a Gluten-Free Diet. Nutrients 2018, 10, 1414. [Google Scholar] [CrossRef] [PubMed]
- Zarkadas, M.; Cranney, A.; Case, S.; Molloy, M.; Switzer, C.; Graham, I.D.; Butzner, J.D.; Rashid, M.; Warren, R.E.; Burrows, V. The impact of a gluten-free diet on adults with coeliac disease: Results of a national survey. J. Hum. Nutr. Diet. 2006, 19, 41–49. [Google Scholar] [CrossRef] [PubMed]
- Zarkadas, M.; Dubois, S.; MacIsaac, K.; Cantin, I.; Rashid, M.; Roberts, K.C.; La Vieille, S.; Godefroy, S.; Pulido, O.M. Living with coeliac disease and a gluten-free diet: A Canadian perspective. J. Hum. Nutr. Diet. 2013, 26, 10–23. [Google Scholar] [CrossRef] [PubMed]
- Halmos, E.P.; Deng, M.; Knowles, S.R.; Sainsbury, K.; Mullan, B.; Tye-Din, J.A. Food knowledge and psychological state predict adherence to a gluten-free diet in a survey of 5310 Australians and New Zealanders with coeliac disease. Aliment. Pharmacol. Ther. 2018, 48, 78–86. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Martinez, M.I.; Alegre-Martínez, A.; García-Ibánez, J.; Cauli, O. Quality of Life in People with Coeliac Disease: Psychological and Socio-Economic Aspects. Endocr. Metab. Immune Disord. Drug Targets 2019, 19, 116–120. [Google Scholar] [CrossRef]
- Chellan, D.; Muktesh, G.; Vaiphei, K.; Berry, N.; Dhaka, N.; Sinha, S.K.; Thapa, B.R.; Kochhar, R. Effect of gluten-free diet and compliance on quality of life in pediatric celiac disease patients. JGH Open 2019, 3, 388–393. [Google Scholar] [CrossRef]
- Barrio, J.; Cilleruelo, M.L.; Román, E.; Fernández, C. Health-related quality of life in Spanish coeliac children using the generic KIDSCREEN-52 questionnaire. Eur. J. Pediatr. 2018, 177, 1515–1522. [Google Scholar] [CrossRef]
- Germone, M.M.; Ariefdjohan, M.; Stahl, M.; Shull, M.; Mehta, P.; Nagle, S.; Tarbell, S.; Liu, E. Family ties: The impact of celiac disease on children and caregivers. Qual. Life Res. 2022, 31, 2107–2118. [Google Scholar] [CrossRef]
- Satherley, R.M.; Coburn, S.S.; Germone, M. The Impact of Celiac Disease on Caregivers’ Well-being: An Integrative Review. J. Pediatr. Gastroenterol. Nutr. 2020, 70, 295–303. [Google Scholar] [CrossRef] [PubMed]
- Abreu Paiva, L.M.; Gandolfi, L.; Pratesi, R.; Harumi Uenishi, R.; Puppin Zandonadi, R.; Nakano, E.Y.; Pratesi, C.B. Measuring Quality of Life in Parents or Caregivers of Children and Adolescents with Celiac Disease: Development and Content Validation of the Questionnaire. Nutrients 2019, 11, 2302. [Google Scholar] [CrossRef] [PubMed]
- Li, B.; Liu, W.J.; Adab, P.; Pallan, M.; Hemming, K.; Frew, E.; Lin, R.; Martin, J.; Liu, W.; Cheng, K.K. Cluster-randomised controlled trial to assess the effectiveness and cost-effectiveness of an obesity prevention programme for Chinese primary school-aged children: The CHIRPY DRAGON study protocol. BMJ Open 2017, 7, e018415. [Google Scholar] [CrossRef] [PubMed]
- Patriota, P.F.; Filgueiras, A.R.; de Almeida, V.B.P.; Alexmovitz, G.A.C.; da Silva, C.E.; de Carvalho, V.F.F.; Carvalho, N.; de Albuquerque, M.P.; Domene, S.M.A.; do Prado, W.L.; et al. Effectiveness of a 16-month multi-component and environmental school-based intervention for recovery of poor income overweight/obese children and adolescents: Study protocol of the health multipliers program. BMC Public Health 2017, 17, 708. [Google Scholar] [CrossRef]
- Li, B.; Pallan, M.; Liu, W.J.; Hemming, K.; Frew, E.; Lin, R.; Liu, W.; Martin, J.; Zanganeh, M.; Hurley, K.; et al. The CHIRPY DRAGON intervention in preventing obesity in Chinese primary-school-aged children: A cluster-randomised controlled trial. PLoS Med. 2019, 16, e1002971. [Google Scholar] [CrossRef]
- Xu, H.; Li, Y.; Zhang, Q.; Hu, X.L.; Liu, A.; Du, S.; Li, T.; Guo, H.; Li, Y.; Xu, G.; et al. Comprehensive school-based intervention to control overweight and obesity in China: A cluster randomized controlled trial. Asia Pac. J. Clin. Nutr. 2017, 26, 1139–1151. [Google Scholar]
- Minossi, V.; Pellanda, L.C. The “Happy Heart” educational program for changes in health habits in children and their families: Protocol for a randomized clinical trial. BMC Pediatr. 2015, 15, 19. [Google Scholar] [CrossRef][Green Version]
- Gold, A.; Larson, M.; Tucker, J.; Strang, M. Classroom Nutrition Education Combined With Fruit and Vegetable Taste Testing Improves Children’s Dietary Intake. J. Sch. Health 2017, 87, 106–113. [Google Scholar] [CrossRef]
- Bartelink, N.H.M.; van Assema, P.; Kremers, S.P.J.; Savelberg, H.H.C.M.; Oosterhoff, M.; Willeboordse, M.; van Schayck, O.C.P.; Winkens, B.; Jansen, M.W.J. One- and Two-Year Effects of the Healthy Primary School of the Future on Children’s Dietary and Physical Activity Behaviours: A Quasi-Experimental Study. Nutrients 2019, 11, 689. [Google Scholar] [CrossRef]
- Bustos, N.; Olivares, S.; Leyton, B.; Cano, M.; Albala, C. Impact of a school-based intervention on nutritional education and physical activity in primary public schools in Chile (KIND) programme study protocol: Cluster randomised controlled trial. BMC Public Health 2016, 16, 1217. [Google Scholar] [CrossRef]
- García-Fuentes, O.; Raposo-Rivas, M.; Martínez-Figueira, M.-E. El enfoque educativo STEAM: Una revisión de la literatura. Rev. Complut. Educ. 2022, 34(1), 191–202. [Google Scholar] [CrossRef]
- Potvin, J.; Chappell, K.; Balestracci, K.; Greene, G.W.; Sweetman, S.; Amin, S. Formative evaluation of a STEAM and nutrition education summer program for low-income youth. Eval. Program. Plann. 2023, 97, 102255. [Google Scholar] [CrossRef] [PubMed]
- Bayles, J.; Peterson, A.D.; Jilcott Pitts, S.; Bian, H.; Goodell, L.S.; Burkholder, S.; Hedge, A.V.; Stage, V.C. Food-Based Science, Technology, Engineering, Arts, and Mathematics (STEAM) Learning Activities May Reduce Decline in Preschoolers’ Skin Carotenoid Status. J. Nutr. Educ. Behav. 2021, 53, 343–351. [Google Scholar] [CrossRef]
- Bucher Della Torre, S.; Akré, C.; Suris, J.C. Obesity prevention opinions of school stakeholders: A qualitative study. J. Sch. Health 2010, 80, 233–239. [Google Scholar] [CrossRef] [PubMed]
- Pearson, N.; Biddle, S.J.; Gorely, T. Family correlates of fruit and vegetable consumption in children and adolescents: A systematic review. Public Health Nutr. 2009, 12, 267–283. [Google Scholar] [CrossRef] [PubMed]
- Yee, A.Z.; Lwin, M.O.; Ho, S.S. The influence of parental practices on child promotive and preventive food consumption behaviors: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 47. [Google Scholar] [CrossRef]
- Bloom, B.S.; Krathwohl, D.R. Taxonomy of Educational Objetives: The Classification of Educational Goals, by a Committee of College and University Examiners; Handbook I: Cognitive Domain; Longmans, Green and Co.: New York, NY, USA, 1956. [Google Scholar]
- Anderson, L. Taxonomy of Educational Objectives. In Encyclopedia of Educational Theory and Philosophy; Phillips, E., Ed.; SAGE Publications: Washington, DC, USA, 2014; pp. 789–791. [Google Scholar]
- López-Pérez, M.; Piñeiro-Fernández, S.; Lasa, A.; Bustamante, M.A.; Martínez, O.; Miranda, J.; Larretxi, I.; Simón, E.; Txurruka, I.; Navarro, V. Nutritional \Education: A Teaching Learning Sequence about Celiac and Gluten for Primary School Children. In Proceedings of the EDULEARN19 Conference, Palma de Mallorca, Spain, 1–3 July 2019; Available online: https://library.iated.org/view/LOPEZPEREZ2019NUT (accessed on 4 December 2023).
- Arriassecq, I.; Greca, I.; Cayul, E. Secuencias de enseñanza y aprendizaje basadas en resultados de investigación: Propuesta de un marco teórico para el abordaje de la teoría especial de la relatividad. Enseñanza Cienc. 2017, 35, 133–155. [Google Scholar] [CrossRef][Green Version]
- Regulation (EU) 2016/679 of the European Parliament and of the Council of 27 April 2016 on the protection of natural persons with regard to the processing of personal data and on the free movement of such data, and repealing Directive 95/46/EC (General Data Protection Regulation). Off. J. Eur. Union 2016, 119, 1–88.
- Akbari Namvar, Z.; Mahdavi, R.; Shirmohammadi, M.; Nikniaz, Z. The effect of group-based education on gastrointestinal symptoms and quality of life in patients with celiac disease: Randomized controlled clinical trial. BMC Gastroenterol. 2022, 22, 18. [Google Scholar] [CrossRef]
- Suárez-González, M.; Bousoño-García, C.; Jiménez-Treviño, S.; Díaz-Martín, J.J. Gluten-Free Diet: Nutritional Strategies to Improve Eating Habits in Children with Celiac Disease: A Prospective, Single-arm Intervention Study. Nutrients 2021, 13, 1108. [Google Scholar] [CrossRef]
- Suárez-González, M.; Bousoño García, C.; Jiménez Treviño, S.; Iglesias Cabo, T.; Díaz Martín, J.J. Influence of nutrition education in paediatric coeliac disease: Impact of the role of the registered dietitian: A prospective, single-arm intervention study. J. Hum. Nutr. Diet. 2020, 33, 775–785. [Google Scholar] [CrossRef] [PubMed]
- Haas, K.; Martin, A.; Park, K.T. Text Message Intervention (TEACH) Improves Quality of Life and Patient Activation in Celiac Disease: A Randomized Clinical Trial. J. Pediatr. 2017, 185, 62–67.e2. [Google Scholar] [CrossRef]
- Rej, A.; Trott, N.; Kurien, M.; Branchi, F.; Richman, E.; Subramanian, S.; Sanders, D.S. Is Peer Support in Group Clinics as Effective as Traditional Individual Appointments? The First Study in Patients with Celiac Disease. Clin. Transl. Gastroenterol. 2020, 11, e00121. [Google Scholar] [CrossRef] [PubMed]
- Sainsbury, K.; Mullan, B. Measuring beliefs about gluten free diet adherence in adult coeliac disease using the theory of planned behaviour. Appetite 2011, 56, 476–483. [Google Scholar] [CrossRef]
- Verrill, L.; Zhang, Y.; Kane, R. Food label usage and reported difficulty with following a gluten-free diet among individuals in the USA with coeliac disease and those with noncoeliac gluten sensitivity. J. Hum. Nutr. Diet. 2013, 26, 479–487. [Google Scholar] [CrossRef] [PubMed]
- Twist, S.R.; Hackett, A.F. An investigation of some implications of coeliac disease. J. Hum. Nutr. Diet. 1992, 5, 343–350. [Google Scholar] [CrossRef]
- Barratt, S.M.; Leeds, J.S.; Sanders, D.S. Quality of life in Coeliac Disease is determined by perceived degree of difficulty adhering to a gluten-free diet, not the level of dietary adherence ultimately achieved. J. Gastrointestin. Liver Dis. 2011, 20, 241–245. [Google Scholar]
- Lee, A.R.; Ng, D.L.; Diamond, B.; Ciaccio, E.J.; Green, P.H.R. Living with coeliac disease: Survey results from the USA. J. Hum. Nutr. Diet. 2012, 25, 233–238. [Google Scholar] [CrossRef]
- Rose, C.; Howard, R. Living with coeliac disease: A grounded theory study. J. Hum. Nutr. Diet. 2014, 27, 30–40. [Google Scholar] [CrossRef]
- Pinto-Sanchez, M.I.; Silvester, J.A.; Lebwohl, B.; Leffler, D.A.; Anderson, R.P.; Therrien, A.; Kelly, C.P.; Verdu, E.F. Society for the Study of Celiac Disease position statement on gaps and opportunities in coeliac disease. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 875–884. [Google Scholar] [CrossRef]
- Abu-Janb, N.; Jaana, M. Facilitators and barriers to adherence to gluten-free diet among adults with celiac disease: A systematic review. J. Hum. Nutr. Diet. 2020, 33, 786–810. [Google Scholar] [CrossRef] [PubMed]
- Vázquez-Polo, M.; Navarro, V.; Larretxi, I.; Perez-Junkera, G.; Lasa, A.; Matias, S.; Simon, E.; Churruca, I. Uncovering the Concerns and Needs of Individuals with Celiac Disease: A Cross-Sectional Study. Nutrients 2023, 15, 3681. [Google Scholar] [CrossRef] [PubMed]
- Rocha, S.; Gandolfi, L.; Santos, J.E. The psychosocial impacts caused by diagnosis and treatment of Coeliac Disease. Rev. Esc. Enferm. USP 2016, 50, 66–72. [Google Scholar] [CrossRef]
- Olsson, C.; Lyon, P.; Hörnell, A.; Ivarsson, A.; Sydner, Y.M. Food that makes you different: The stigma experienced by adolescents with celiac disease. Qual. Health Res. 2009, 19, 976–984. [Google Scholar] [CrossRef] [PubMed]
- Medeiros, G.C.B.S.; Azevedo, K.P.M.; Garcia, D.; Oliveira Segundo, V.H.; Mata, A.N.S.; Fernandes, A.K.P.; Santos, R.P.D.; Trindade, D.D.B.B.; Moreno, I.M.; Guillén Martínez, D.; et al. Effect of School-Based Food and Nutrition Education Interventions on the Food Consumption of Adolescents: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 10522. [Google Scholar] [CrossRef] [PubMed]
- Pereira, A.R.; Oliveira, A. Dietary Interventions to Prevent Childhood Obesity: A Literature Review. Nutrients 2021, 13, 3447. [Google Scholar] [CrossRef] [PubMed]
- Scherr, R.E.; Linnell, J.D.; Dharmar, M.; Beccarelli, L.M.; Bergman, J.J.; Briggs, M.; Brian, K.M.; Feenstra, G.; Hillhouse, J.C.; Keen, C.L.; et al. A Multicomponent, School-Based Intervention, the Shaping Healthy Choices Program, Improves Nutrition-Related Outcomes. J. Nutr. Educ. Behav. 2017, 49, 368–379.e1. [Google Scholar] [CrossRef]
- Pablos, A.; Nebot, V.; Vañó-Vicent, V.; Ceca, D.; Elvira, L. Effectiveness of a school-based program focusing on diet and health habits taught through physical exercise. Appl. Physiol. Nutr. Metab. 2018, 43, 331–337. [Google Scholar] [CrossRef]
- Schneider, R.M.; Krajcik, J.; Marx, R.W.; Soloway, E. Performance of students in project-based science classrooms on a national measure of science achievement. J. Res. Sci. Teach. 2002, 39, 410–422. [Google Scholar] [CrossRef]
- Spires, H.A.; Himes, M.P.; Krupa, E. Supporting Students’ Science Content Knowledge and Motivation through Project-Based Inquiry (PBI) Global in a Cross-School Collaboration. Educ. Sci. 2022, 12, 412. [Google Scholar] [CrossRef]
- Navarro, V.; Ruiz-González, A.; García, A.; Churruca, I.; Miranda, J.; Bustamante, M.A.; Simón, E.; Lasa, A. Design and implementation of a teaching-learning sequence about celiac disease in primary school classrooms. In Proceedings of the ICERI2017 Conference, Seville, Spain, 16–18 November 2017. [Google Scholar]
- Bagherniya, M.; Sharma, M.; Mostafavi Darani, F.; Maracy, M.R.; Safarian, M.; Allipour Birgani, R.; Bitarafan, V.; Keshavarz, S.A. School-Based Nutrition Education Intervention Using Social Cognitive Theory for Overweight and Obese Iranian Adolescent Girls: A Cluster Randomized Controlled Trial. Int. Q. Community Health Educ. 2017, 38, 37–45. [Google Scholar] [CrossRef] [PubMed]
- Ledoux, T.; Griffith, M.; Thompson, D.; Nguyen, N.; Watson, K.; Baranowski, J.; Buday, R.; Abdelsamad, D.; Baranoswski, T. An educational video game for nutrition of young people: Theory and design. Simul. Gaming 2016, 47, 490–516. [Google Scholar] [CrossRef] [PubMed]
- Najimi, A.; Ghaffari, M. Promoting fruit and vegetable consumption among students: A randomized controlled trial based on social cognitive theory. J. Pak. Med. Assoc. 2013, 63, 1235–1240. [Google Scholar] [PubMed]
- Powers, A.R.; Struempler, B.J.; Guarino, A.; Parmer, S.M. Effects of a nutrition education program on the dietary behavior and nutrition knowledge of second-grade and third-grade students. J. Sch. Health 2005, 75, 129–133. [Google Scholar] [CrossRef] [PubMed]
- UNESCO. Boosting Gender Equality in Science and Technology, a Challenge for TVET Programmes and Cereers; United Nations Educational, Scientific and Cultural Organization (UNESCO): Paris, France, 2020; ISBN 978-92-3-100417-9. [Google Scholar]
- Kim, A.Y.; Sinatra, G.M.; Seyranian, V. Developing a STEM Identity Among Young Women: A Social Identity Perspective. Rev. Educ. Res. 2018, 88, 589–625. [Google Scholar] [CrossRef]
- Duncan, S.; Stewart, T.; McPhee, J.; Borotkanics, R.; Prendergast, K.; Zinn, C.; Meredith-Jones, K.; Taylor, R.; McLachlan, C.; Schofield, G. Efficacy of a compulsory homework programme for increasing physical activity and improving nutrition in children: A cluster randomised controlled trial. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 80. [Google Scholar] [CrossRef] [PubMed]
- Young, K.M.; Northern, J.J.; Lister, K.M.; Drummond, J.A.; O’Brien, W.H. A meta-analysis of family-behavioral weight-loss treatments for children. Clin. Psychol. Rev. 2007, 27, 240–249. [Google Scholar] [CrossRef] [PubMed]
- Silveira, J.A.; Taddei, J.A.; Guerra, P.H.; Nobre, M.R. Effectiveness of school-based nutrition education interventions to prevent and reduce excessive weight gain in children and adolescents: A systematic review. J. Pediatr. 2011, 87, 382–392. [Google Scholar] [CrossRef]
- Gatto, N.M.; Martinez, L.C.; Spruijt-Metz, D.; Davis, J.N. LA sprouts randomized controlled nutrition, cooking and gardening programme reduces obesity and metabolic risk in Hispanic/Latino youth. Pediatr. Obes. 2017, 12, 28–37. [Google Scholar] [CrossRef]
- Keihner, A.; Rosen, N.; Wakimoto, P.; Goldstein, L.; Sugerman, S.; Hudes, M.; Ritchie, L.; McDevitt, K. Impact of California Children’s Power Play! Campaign on Fruit and Vegetable Intake and Physical Activity among Fourth- and Fifth-Grade Students. Am. J. Health Promot. 2017, 31, 189–191. [Google Scholar] [CrossRef]
- Mirmiran, P.; Bahadoran, Z.; Gaeini, Z. Common Limitations and Challenges of Dietary Clinical Trials for Translation into Clinical Practices. Int. J. Endocrinol. Metab. 2021, 19, e108170. [Google Scholar] [CrossRef] [PubMed]
- Coppoolse, H.L.; Seidell, J.C.; Dijkstra, S.C. Impact of nutrition education on nutritional knowledge and intentions towards nutritional counselling in Dutch medical students: An intervention study. BMJ Open 2020, 10, e034377. [Google Scholar] [CrossRef] [PubMed]
- Yao, C.K.; Gibson, P.R.; Shepherd, S.J. Design of clinical trials evaluating dietary interventions in patients with functional gastrointestinal disorders. Am. J. Gastroenterol. 2013, 108, 748–758. [Google Scholar] [CrossRef] [PubMed]
- Byrd-Bredbenner, C.; Wu, F.; Spaccarotella, K.; Quick, V.; Martin-Biggers, J.; Zhang, Y. Systematic review of control groups in nutrition education intervention research. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 91. [Google Scholar] [CrossRef]


| Competence | Learning Outcome | Activity | Topic Day |
|---|---|---|---|
| The student should be able to place the food groups in the food pyramid. | Bloom level 3. Application The student adequately organises different foods in the pyramid. | Game about the food pyramid. | Day 1. Food groups Day 2. Healthy diet |
| The student should be able to identify dietary errors and make recommendations for its modification. | Bloom level 4. Analysis The student identifies foods to be consumed infrequently. Bloom level 6. Evaluation The student offers recommendations to adapt its consumption. | Complete and adapt a 24 h recall. | Day 1. Food groups Day 2. Healthy diet |
| The student should be able to consume less food from the top of the pyramid. | Bloom level 6. Evaluation Students consume less unhealthy food than before the activities. | Game about the food pyramid. Complete and adapt a 24 h recall. Healthy snacks challenge. | Days 2 to 8. Healthy snacks challenge. Day 2. Healthy diet (transversally) |
| The student should be able to explain what celiac disease is. | Bloom level 2. Understanding The student acknowledges that gluten harms people with celiac disease and makes them sick. The student concludes that people with CD should follow a gluten-free diet. | Game to learn the characteristics of the disease. | Day 3. Celiac Disease |
| The student should be able to analyse gluten | Bloom level 3. Application The student manipulates gluten and finds it. The student figures out that gluten gives elasticity to the doughs. Bloom level 4. Analysis Students deduce where gluten is by analysing food labels. | Experiment 1: Learning by doing: pasta made with different types of flour. Experiment 2: Food analysis through the senses. | Day 4. What gluten is Day 5. Where gluten is (transversally) |
| The student should be able to classify food groups according to gluten content. | Bloom level 4. Analysis The student identifies the food groups that contain gluten: placing them in cereals. The student concludes that processed foods may contain gluten. | Experiment 3: Gluten detection experiment, immunochromatography. Experiment 4: Study of food labelling. | Day 6. Food labels Day 7.Where gluten is Day 4. What gluten is (transversally) |
| The student should be able to understand the work of scientists, to know that the gluten content of foods is analysed through experimentation. | Bloom level 6. Evaluation The student is able to perform experimental work, observe, analyse and evaluate the results. | All the experiments. | Day 4. What gluten is Day 5. Differences between gluten and gluten free foods Day 6. Food labels Day 7. Where gluten is |
| The student should be able to assess the impact of own actions on others. | Bloom level 6. Evaluation The student demonstrates empathetic behaviour. The student selects actions and behaviours to overcome differences between people. | Game to learn the characteristics of the disease. Case study to work on inclusion: discussion. | Day 8. Social inclusion of people with celiac disease Day 3. Celiac Disease (transversally) Day 5. Differences between gluten and gluten free foods (transversally) |
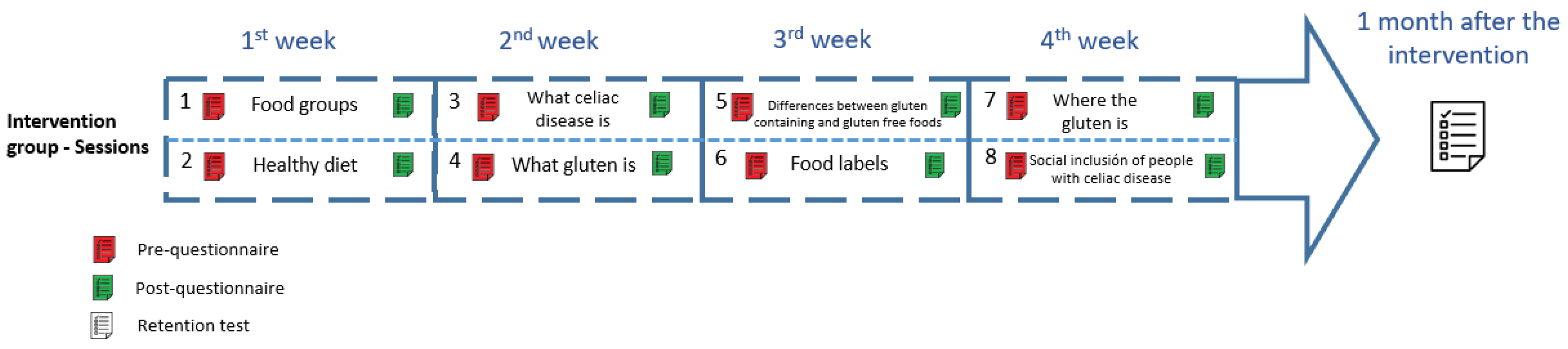
| Intervention Group | Control Group | |||
|---|---|---|---|---|
| Week | Topic Session 1 | Topic Session 2 | Challenge | No intervention |
| 1 | Day 1. Food groups | Day 2. Healthy diet | “Healthy snacks challenge” | |
| 2 | Day 3. Celiac Disease | Day 4. What gluten is | ||
| 3 | Day 5. Differences between gluten containing and gluten free foods | Day 6. Food labels | ||
| 4 | Day 7. Where gluten is | Day 8. Social inclusion of people with celiac disease | ||
| Competence | Outcome Measures |
|---|---|
| The student should be able to place the food groups in the food pyramid. | Change in nutrition knowledge |
| The student should be able to identify dietary errors and make recommendations for modification. | Change in nutrition knowledge |
| The student should be able to consume less food from the top of the pyramid. | Change in behaviour in relation to the consumption of unhealthy foods |
| The student should be able to explain what celiac disease is. | Change in Celiac Disease knowledge |
| The student is able to assess the impact of their own actions on others. | Change in intentional behaviour related to the social inclusion of people with celiac condition: perception of the influence of one’s own actions on others. |
| The student should be able to analyse gluten | Change in knowledge regarding gluten and its presence in foods |
| The student should be able to classify food groups according to gluten content. | Change in knowledge regarding gluten and its presence in foods |
| The student should be able to understand the work of scientists, to know that the gluten content of foods is analysed through experimentation. | Change in attitude in relation to interest in science |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vázquez-Polo, M.; Churruca, I.; Perez-Junkera, G.; Larretxi, I.; Lasa, A.; Esparta, J.; Cantero-Ruiz de Eguino, L.; Navarro, V. Study Protocol for a Controlled Trial of Nutrition Education Intervention about Celiac Disease in Primary School: ZELIAKIDE Project. Nutrients 2024, 16, 338. https://doi.org/10.3390/nu16030338
Vázquez-Polo M, Churruca I, Perez-Junkera G, Larretxi I, Lasa A, Esparta J, Cantero-Ruiz de Eguino L, Navarro V. Study Protocol for a Controlled Trial of Nutrition Education Intervention about Celiac Disease in Primary School: ZELIAKIDE Project. Nutrients. 2024; 16(3):338. https://doi.org/10.3390/nu16030338
Chicago/Turabian StyleVázquez-Polo, Maialen, Itziar Churruca, Gesala Perez-Junkera, Idoia Larretxi, Arrate Lasa, Jon Esparta, Leire Cantero-Ruiz de Eguino, and Virginia Navarro. 2024. "Study Protocol for a Controlled Trial of Nutrition Education Intervention about Celiac Disease in Primary School: ZELIAKIDE Project" Nutrients 16, no. 3: 338. https://doi.org/10.3390/nu16030338
APA StyleVázquez-Polo, M., Churruca, I., Perez-Junkera, G., Larretxi, I., Lasa, A., Esparta, J., Cantero-Ruiz de Eguino, L., & Navarro, V. (2024). Study Protocol for a Controlled Trial of Nutrition Education Intervention about Celiac Disease in Primary School: ZELIAKIDE Project. Nutrients, 16(3), 338. https://doi.org/10.3390/nu16030338