
Differential Effects of Two Isocaloric Healthy Diets on Postprandial Lipid Responses in Individuals with Type 2 Diabetes

 , ,
, ,  , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Study Design
2.3. Laboratory Methods
2.4. Statistical Analysis
3. Results
3.1. Anthropometrics and Fasting Measurements
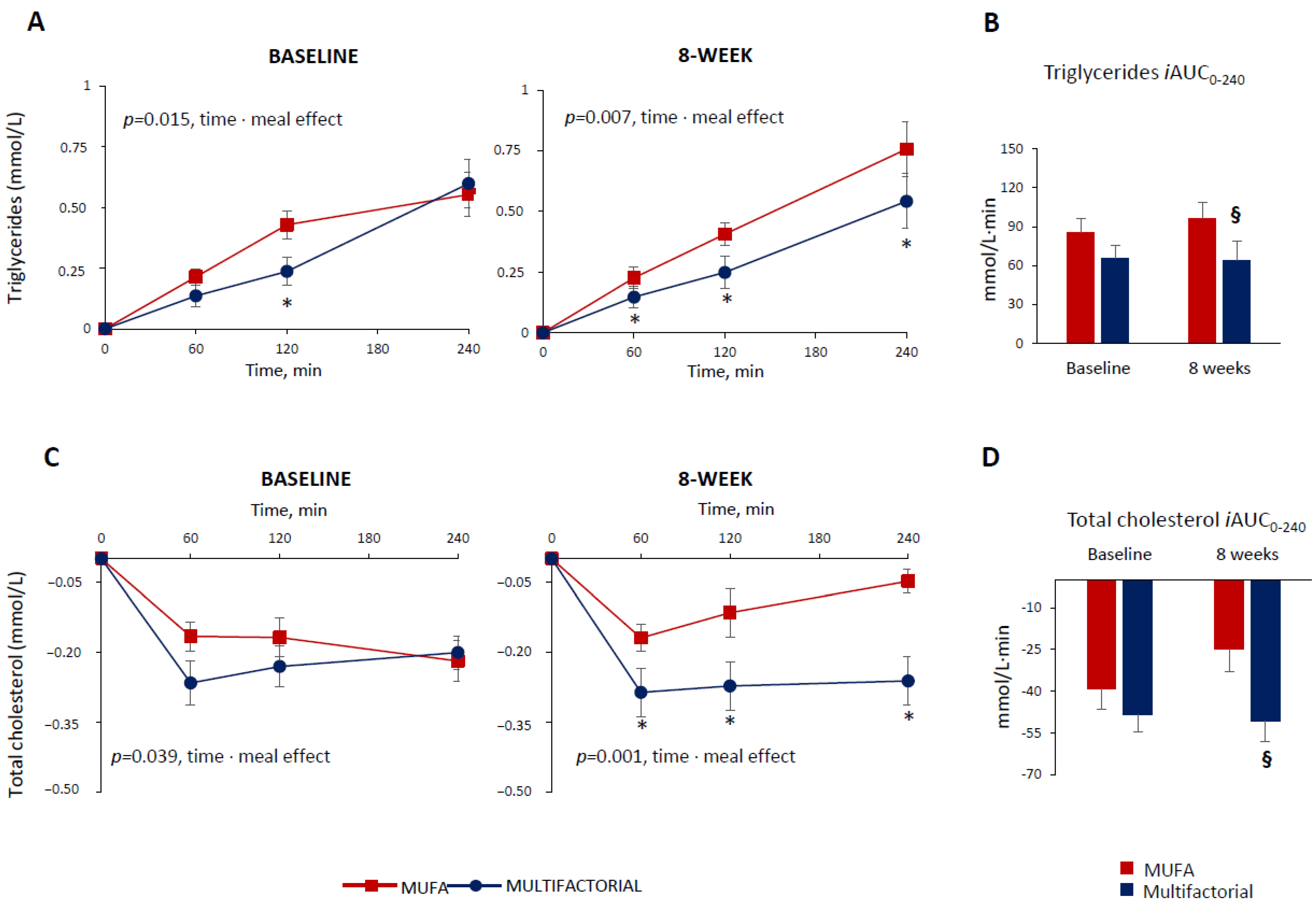
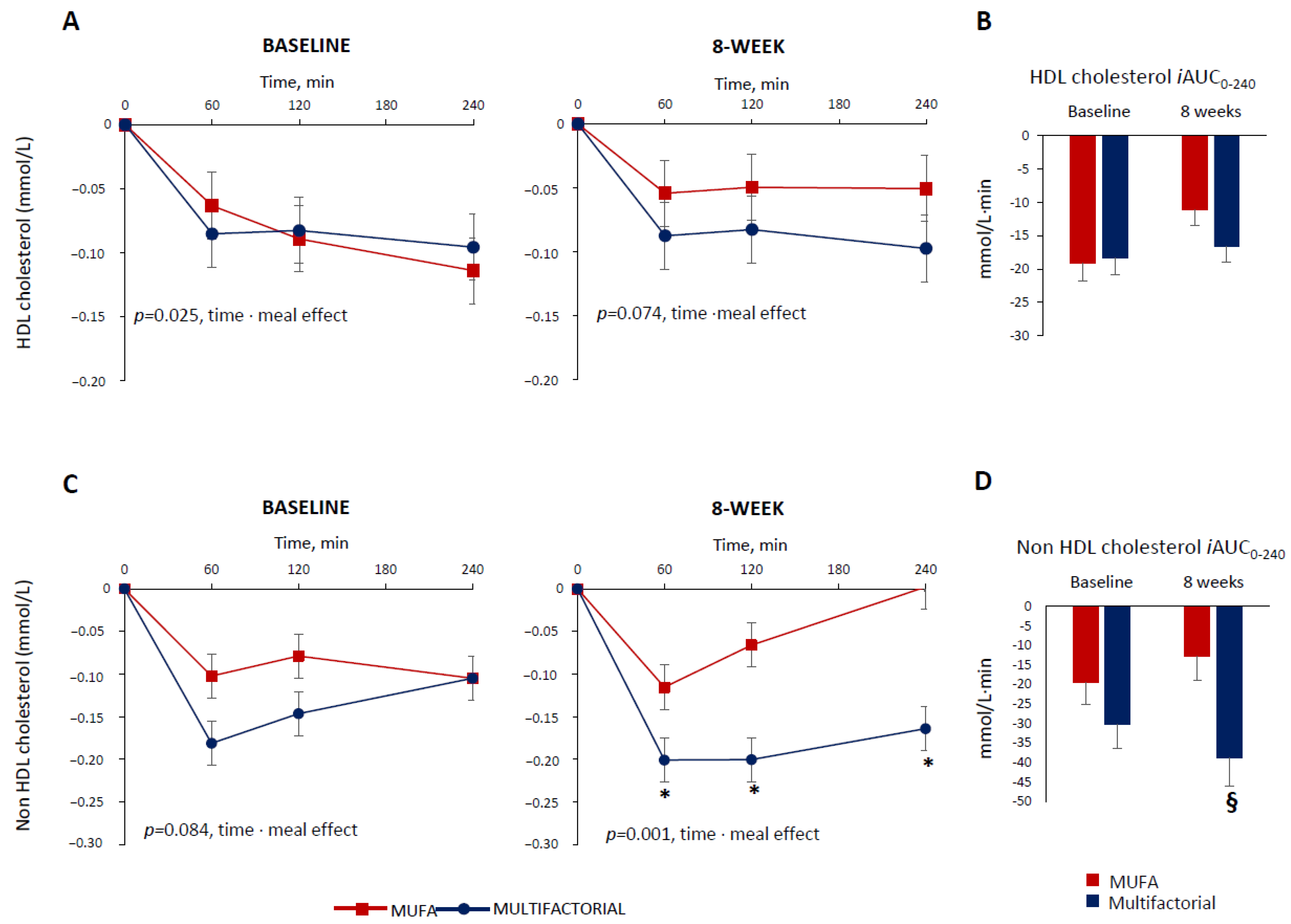
3.2. Postprandial Lipid Response
3.3. Postprandial Glucose and Insulin Response
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nordestgaard, B.G.; Benn, M.; Schnohr, P.; Tybjaerg-Hansen, A. Nonfasting triglycerides and risk of myocardial infarction, ischemic heart disease, and death in men and women. JAMA 2007, 298, 299–308. [Google Scholar] [CrossRef] [PubMed]
- Pirillo, A.; Norata, G.D.; Catapano, A.L. Postprandial lipemia as a cardiometabolic risk factor. Curr. Med. Res. Opin. 2014, 30, 1489–1503. [Google Scholar] [CrossRef] [PubMed]
- Yanai, H.; Adachi, H.; Hakoshima, M.; Katsuyama, H. Postprandial Hyperlipidemia: Its Pathophysiology, Diagnosis, Atherogenesis, and Treatments. Int. J. Mol. Sci. 2023, 24, 13942. [Google Scholar] [CrossRef] [PubMed]
- Enkhmaa, B.; Ozturk, Z.; Anuurad, E.; Berglund, L. Postprandial lipoproteins and cardiovascular disease risk in diabetes mellitus. Curr. Diab Rep. 2010, 10, 61–69. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.; Kim, Y.J.; Khang, A.R.; Eckel, R.H. Postprandial dyslipidemia after a standardized high-fat meal in BMI-matched healthy individuals, and in subjects with prediabetes or type 2 diabetes. Clin. Nutr. 2021, 40, 5538–5546. [Google Scholar] [CrossRef] [PubMed]
- Vergès, B. Intestinal lipid absorption and transport in type 2 diabetes. Diabetologia 2022, 65, 1587–1600. [Google Scholar] [CrossRef] [PubMed]
- Tomlinson, B.; Chan, P.; Lam, C.W.K. Postprandial hyperlipidemia as a risk factor in patients with type 2 diabetes. Expert. Rev. Endocrinol. Metab. 2020, 15, 147–157. [Google Scholar] [CrossRef] [PubMed]
- Desmarchelier, C.; Borel, P.; Lairon, D.; Maraninchi, M.; Valéro, R. Effect of Nutrient and Micronutrient Intake on Chylomicron Production and Postprandial Lipemia. Nutrients 2019, 11, 1299. [Google Scholar] [CrossRef]
- Bozzetto, L.; Della Pepa, G.; Vetrani, C.; Rivellese, A.A. Dietary Impact on Postprandial Lipemia. Front. Endocrinol. 2020, 11, 337. [Google Scholar] [CrossRef]
- Bozzetto, L.; Annuzzi, G.; Costabile, G.; Costagliola, L.; Giorgini, M.; Alderisio, A.; Strazzullo, A.; Patti, L.; Cipriano, P.; Mangione, A.; et al. A CHO/fibre diet reduces and a MUFA diet increases postprandial lipaemia in type 2 diabetes: No supplementary effects of low-volume physical training. Acta Diabetol. 2014, 51, 385–393. [Google Scholar] [CrossRef]
- Giuntini, E.B.; Sardá, F.A.H.; de Menezes, E.W. The Effects of Soluble Dietary Fibers on Glycemic Response: An Overview and Futures Perspectives. Foods 2022, 11, 3934. [Google Scholar] [CrossRef] [PubMed]
- Neumann, H.F.; Egert, S. Impact of Meal Fatty Acid Composition on Postprandial Lipemia in Metabolically Healthy Adults and Individuals with Cardiovascular Disease Risk Factors: A Systematic Review. Adv. Nutr. 2022, 13, 193–207. [Google Scholar] [CrossRef] [PubMed]
- Bergeron, N.; Havel, R.J. Influence of diets rich in saturated and omega-6 polyunsaturated fatty acids on the postprandial responses of apolipoproteins B-48, B-100, E, and lipids in triglyceride-rich lipoproteins. Arterioscler. Thromb. Vasc. Biol. 1995, 15, 2111–2121. [Google Scholar] [CrossRef] [PubMed]
- Lopes, L.L.; Rocha, D.M.U.P.; Silva, A.D.; Peluzio, M.D.C.G.; Bressan, J.; Hermsdorff, H.H.M. Postprandial Lipid Response to High-Saturated and High-Monounsaturated Fat Meals in Normal-Weight or Overweight Women. J. Am. Coll. Nutr. 2018, 37, 308–315. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.; Zhang, X.; Zhou, N.; Shen, Y.; Li, B.; Chen, B.E.; Li, X. Association Between Omega-3 Fatty Acid Intake and Dyslipidemia: A Continuous Dose-Response Meta-Analysis of Randomized Controlled Trials. J. Am. Heart Assoc. 2023, 12, e029512. [Google Scholar] [CrossRef]
- Miyoshi, T.; Noda, Y.; Ohno, Y.; Sugiyama, H.; Oe, H.; Nakamura, K.; Kohno, K.; Ito, H. Omega-3 fatty acids improve postprandial lipemia and associated endothelial dysfunction in healthy individuals—A randomized cross-over trial. Biomed. Pharmacother. Biomedecine Pharmacother. 2014, 68, 1071–1077. [Google Scholar] [CrossRef] [PubMed]
- Finnegan, Y.E.; Minihane, A.M.; Leigh-Firbank, E.C.; Kew, S.; Meijer, G.W.; Muggli, R.; Calder, P.C.; Williams, C.M. Plant- and marine-derived n-3 polyunsaturated fatty acids have differential effects on fasting and postprandial blood lipid concentrations and on the susceptibility of LDL to oxidative modification in moderately hyperlipidemic subjects. Am. J. Clin. Nutr. 2003, 77, 783–795. [Google Scholar] [CrossRef]
- Feldman, F.; Koudoufio, M.; Desjardins, Y.; Spahis, S.; Delvin, E.; Levy, E. Efficacy of Polyphenols in the Management of Dyslipidemia: A Focus on Clinical Studies. Nutrients 2021, 13, 672. [Google Scholar] [CrossRef]
- Annuzzi, G.; Bozzetto, L.; Costabile, G.; Giacco, R.; Mangione, A.; Anniballi, G.; Vitale, M.; Vetrani, C.; Cipriano, P.; Della Corte, G.; et al. Diets naturally rich in polyphenols improve fasting and postprandial dyslipidemia and reduce oxidative stress: A randomized controlled trial. Am. J. Clin. Nutr. 2014, 99, 463–471. [Google Scholar] [CrossRef]
- Della Pepa, G.; Vetrani, C.; Brancato, V.; Vitale, M.; Monti, S.; Annuzzi, G.; Lombardi, G.; Izzo, A.; Tommasone, M.; Cipriano, P.; et al. Effects of a multifactorial ecosustainable isocaloric diet on liver fat in patients with type 2 diabetes: Randomized clinical trial. BMJ Open Diabetes Res. Care 2020, 8, e001342. [Google Scholar] [CrossRef]
- Costabile, G.; Della Pepa, G.; Salamone, D.; Luongo, D.; Naviglio, D.; Brancato, V.; Cavaliere, C.; Salvatore, M.; Cipriano, P.; Vitale, M.; et al. Reduction of De Novo Lipogenesis Mediates Beneficial Effects of Isoenergetic Diets on Fatty Liver: Mechanistic Insights from the MEDEA Randomized Clinical Trial. Nutrients 2022, 14, 2178. [Google Scholar] [CrossRef] [PubMed]
- Della Pepa, G.; Brancato, V.; Costabile, G.; Salamone, D.; Corrado, A.; Vitale, M.; Cavaliere, C.; Mancini, M.; Salvatore, M.; Luongo, D.; et al. An Isoenergetic Multifactorial Diet Reduces Pancreatic Fat and Increases Postprandial Insulin Response in Patients with Type 2 Diabetes: A Randomized Controlled Trial. Diabetes Care 2022, 45, 1935–1942. [Google Scholar] [CrossRef]
- Friedewald, W.T.; Levy, R.I.; Fredrickson, D.S. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin. Chem. 1972, 18, 499–502. [Google Scholar] [CrossRef] [PubMed]
- Lairon, D.; Defoort, C. Effects of nutrients on postprandial lipemia. Curr. Vasc. Pharmacol. 2011, 9, 309–312. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Miranda, J.; Marin, C. Dietary, Physiological, and Genetic Impacts on Postprandial Lipid Metabolism. In Fat Detection: Taste, Texture, and Post Ingestive Effects; Montmayeur, J.P., le Coutre, J., Eds.; CRC Press/Taylor & Francis: Boca Raton, FL, USA, 2010; Chapter 17. [Google Scholar]
- Frayn, K.N. Dietary factors and postprandial lipaemia. Br. J. Nutr. 1998, 80, 409–410. [Google Scholar] [CrossRef] [PubMed]
- Lairon, D.; Play, B.; Jourdheuil-Rahmani, D. Digestible and indigestible carbohydrates: Interactions with postprandial lipid metabolism. J. Nutr. Biochem. 2007, 18, 217–227. [Google Scholar] [CrossRef] [PubMed]
- Bladé, C.; Arola, L.; Salvadó, M.J. Hypolipidemic effects of proanthocyanidins and their underlying biochemical and molecular mechanisms. Mol. Nutr. Food Res. 2010, 54, 37–59. [Google Scholar] [CrossRef]
- Soliman, G.A. Dietary Fiber, Atherosclerosis, and Cardiovascular Disease. Nutrients 2019, 11, 1155. [Google Scholar] [CrossRef]
- Brown, L.; Rosner, B.; Willett, W.W.; Sacks, F.M. Cholesterol-lowering effects of dietary fiber: A meta-analysis. Am. J. Clin. Nutr. 1999, 69, 30–42. [Google Scholar] [CrossRef]
- Othman, R.A.; Moghadasian, M.H.; Jones, P.J. Cholesterol-lowering effects of oat β-glucan. Nutr. Rev. 2011, 69, 299–309. [Google Scholar] [CrossRef]
- Lamarche, B.; Desroches, S.; Jenkins, D.J.; Kendall, C.W.; Marchie, A.; Faulkner, D.; Vidgen, E.; Lapsley, K.G.; Trautwein, E.A.; Parker, T.L.; et al. Combined effects of a dietary portfolio of plant sterols, vegetable protein, viscous fibre and almonds on LDL particle size. Br. J. Nutr. 2004, 92, 657–663. [Google Scholar] [CrossRef] [PubMed]
- Brunner, F.J.; Waldeyer, C.; Ojeda, F.; Salomaa, V.; Kee, F.; Sans, S.; Thorand, B.; Giampaoli, S.; Brambilla, P.; Tunstall-Pedoe, H.; et al. Application of non-HDL cholesterol for population-based cardiovascular risk stratification: Results from the Multinational Cardiovascular Risk Consortium. Lancet 2019, 394, 2173–2183. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, D.J.; Kathariya, M.G.; Verma, D.P.K. LDL-C, NON-HDL-C and APO-B for cardiovascular risk assessment: Looking for the ideal marker. Indian Heart J. 2021, 73, 44–548. [Google Scholar] [CrossRef] [PubMed]
- Huynh, K. Non-HDL cholesterol levels linked with long-term risk of CVD. Nat. Rev. Cardiol. 2020, 17, 132–133. [Google Scholar] [CrossRef] [PubMed]
- Freese, E.C.; Gist, N.H.; Cureton, K.J. Effect of prior exercise on postprandial lipemia: An updated quantitative review. J. Appl. Physiol. 2014, 116, 67–75. [Google Scholar] [CrossRef]
- Pfeuffer, M.; Auinger, A.; Bley, U.; Kraus-Stojanowic, I.; Laue, C.; Winkler, P.; Rüfer, C.E.; Frank, J.; Bösch-Saadatmandi, C.; Rimbach, G.; et al. Effect of quercetin on traits of the metabolic syndrome, endothelial function and inflammation in men with different APOE isoforms. Nutr. Metab. Cardiovasc. Dis. 2013, 23, 403–409. [Google Scholar] [CrossRef]
- Timmers, S.; Konings, E.; Bilet, L.; Houtkooper, R.H.; van de Weijer, T.; Goossens, G.H.; Hoeks, J.; van der Krieken, S.; Ryu, D.; Kersten, S.; et al. Calorie restriction-like effects of 30 days of resveratrol supplementation on energy metabolism and metabolic profile in obese humans. Cell Metab. 2011, 14, 612–622. [Google Scholar] [CrossRef]
- Desroches, S.; Paradis, M.E.; Pérusse, M.; Archer, W.R.; Bergeron, J.; Couture, P.; Bergeron, N.; Lamarche, B. Apolipoprotein A-I, A-II, and VLDL-B-100 metabolism in men: Comparison of a low-fat diet and a high-monounsaturated fatty acid diet. J. Lipid Res. 2004, 45, 2331–2338. [Google Scholar] [CrossRef]
- Hernáez, Á.; Castañer, O.; Elosua, R.; Pintó, X.; Estruch, R.; Salas-Salvadó, J.; Corella, D.; Arós, F.; Serra-Majem, L.; Fiol, M.; et al. Mediterranean Diet Improves High-Density Lipoprotein Function in High-Cardiovascular-Risk Individuals: A Randomized Controlled Trial. Circulation 2017, 135, 633–643. [Google Scholar] [CrossRef]
- Bardagjy, A.S.; Steinberg, F.M. Relationship Between HDL Functional Characteristics and Cardiovascular Health and Potential Impact of Dietary Patterns: A Narrative Review. Nutrients 2019, 11, 1231. [Google Scholar] [CrossRef]
- Node, K.; Inoue, T. Postprandial hyperglycemia as an etiological factor in vascular failure. Cardiovasc. Diabetol. 2009, 8, 23. [Google Scholar] [CrossRef]
- Nakamura, A.; Monma, Y.; Kajitani, S.; Kozu, K.; Ikeda, S.; Noda, K.; Nakajima, S.; Endo, H.; Takahashi, T.; Nozaki, E. Different postprandial lipid metabolism and insulin resistance between non-diabetic patients with and without coronary artery disease. J. Cardiol. 2015, 66, 435–444. [Google Scholar] [CrossRef][Green Version]
- Esser, N.; Utzschneider, K.M.; Kahn, S.E. Early beta cell dysfunction vs insulin hypersecretion as the primary event in the pathogenesis of dysglycaemia. Diabetologia 2020, 63, 2007–2021. [Google Scholar] [CrossRef]
- Kolovou, G.D.; Mikhailidis, D.P.; Kovar, J.; Lairon, D.; Nordestgaard, B.G.; Ooi, T.C.; Perez-Martinez, P.; Bilianou, H.; Anagnostopoulou, K.; Panotopoulos, G. Assessment and clinical relevance of non-fasting and postprandial triglycerides: An expert panel statement. Curr. Vasc. Pharmacol. 2011, 9, 258–270. [Google Scholar] [CrossRef]
- Lairon, D.; Lopez-Miranda, J.; Williams, C. Methodology for studying postprandial lipid metabolism. Eur. J. Clin. Nutr. 2007, 61, 1145–1161. [Google Scholar] [CrossRef]
- Weiss, E.P.; Fields, D.A.; Mittendorfer, B.; Haverkort, M.A.; Klein, S. Reproducibility of postprandial lipemia tests and validity of an abbreviated 4-hour test. Metabolism 2008, 57, 1479–1485. [Google Scholar] [CrossRef]
- Bansal, S.; Buring, J.; Rifai, N.; Mora, S.; Sacks, F.; Ridker, P. Fasting compared with nonfasting triglycerides and risk of cardiovascular events in women. JAMA 2007, 298, 309–316. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| MUFA Diet | Multifactorial Diet | |
|---|---|---|
| Energy (kcal) | 843 | 821 |
| Protein (% TEI) | 18 | 18 |
| Fat (% TEI) | 42 | 42 |
| Saturated (% TEI) | 7 | 7 |
| Monounsaturated (% TEI) | 28 | 28 |
| Polyunsaturated (% TEI) | 3.4 | 4.5 |
| n-3 (g) | 0.36 | 1.20 |
| n-6 (g) | 2.87 | 2.91 |
| Carbohydrates (% TEI) | 40 | 40 |
| Sugars (% TEI) | 7.6 | 7.9 |
| Fiber (g/1000 kcal) | 7.7 | 14.2 |
| Glycemic index (%) | 84 | 39 |
| Glycemic load | 70 | 32 |
| Vitamin E (mg) | 8.3 | 8.5 |
| Vitamin D (μg) | 1.83 | 2.72 |
| Vitamin C (mg) | 33 | 168 |
| Polyphenols (mg) | 16 | 758 |
| Total ORAC (μmolT) | 1584 | 4441 |
| MUFA Diet (n = 22) | Multifactorial Diet (n = 21) | ||||
|---|---|---|---|---|---|
| Baseline | 8 Weeks | Baseline | 8 Weeks | p § | |
| Gender (Male/Female) | 12/10 | - | 13/8 | - | - |
| Age (years) | 63 (5) | - | 63 (7) | - | 0.784 |
| Body weight (kg) | 84 (14) | 83 (14) * | 85 (12) | 84 (12) * | 0.951 |
| BMI (Kg/m2) | 31(3) | 30(3) * | 32(4) | 31(4) | 0.894 |
| Waist circumference (cm) | 104 (11) | 104 (11) | 106 (10) | 106 (10) | 0.495 |
| Hb1Ac (%) | 6.6 (0.6) | 6.4 (0.7) * | 6.6 (0.5) | 6.3 (0.5) | 0.760 |
| Glucose (mmol/L) | 7.2 (0.9) | 7.1 (0.9) | 6.8 (0.8) | 7.0 (1.0) | 0.480 |
| Insulin (pmol/L) | 126 (68) | 133 (79) | 130 (72) | 110 (56) | 0.120 |
| HOMA-IR | 5.8 (3.0) | 6.1 (3.6) | 5.6 (2.7) | 4.9 (2.6) | 0.256 |
| Total cholesterol (mmol/L) | 3.70 (0.7) | 3.57 (0.7) | 3.85 (0.8) | 3.83 (0.9) | 0.372 |
| HDL cholesterol (mmol/L) | 1.01 (0.2) | 0.98 (0.2) | 1.09 (0.3) | 1.01 (0.2) | 0.115 |
| Plasma triglycerides (mmol/L) | 1.21 (0.4) | 1.18 (0.5) | 1.29 (0.3) | 1.58 (0.6) | 0.496 |
| LDL cholesterol (mmol/L) | 2.12 (0.6) | 2.02 (0.5) | 2.18 (0.5) | 2.23 (0.6) | 0.192 |
| Non-HDL cholesterol (mmol/L) | 2.69 (0.1) | 2.56 (0.1) | 2.77 (0.1) | 2.82 (0.2) | 0.146 |
| Lipid-lowering drugs | 14 (58%) | - | 10 (42%) | - | 0.364 |
| Glucose-lowering drugs | 17 (55%) | - | 14 (45%) | - | 0.438 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Costabile, G.; Salamone, D.; Della Pepa, G.; Vitale, M.; Testa, R.; Cipriano, P.; Scidà, G.; Rivellese, A.A.; Annuzzi, G.; Bozzetto, L. Differential Effects of Two Isocaloric Healthy Diets on Postprandial Lipid Responses in Individuals with Type 2 Diabetes. Nutrients 2024, 16, 333. https://doi.org/10.3390/nu16030333
Costabile G, Salamone D, Della Pepa G, Vitale M, Testa R, Cipriano P, Scidà G, Rivellese AA, Annuzzi G, Bozzetto L. Differential Effects of Two Isocaloric Healthy Diets on Postprandial Lipid Responses in Individuals with Type 2 Diabetes. Nutrients. 2024; 16(3):333. https://doi.org/10.3390/nu16030333
Chicago/Turabian StyleCostabile, Giuseppina, Dominic Salamone, Giuseppe Della Pepa, Marilena Vitale, Roberta Testa, Paola Cipriano, Giuseppe Scidà, Angela Albarosa Rivellese, Giovanni Annuzzi, and Lutgarda Bozzetto. 2024. "Differential Effects of Two Isocaloric Healthy Diets on Postprandial Lipid Responses in Individuals with Type 2 Diabetes" Nutrients 16, no. 3: 333. https://doi.org/10.3390/nu16030333
APA StyleCostabile, G., Salamone, D., Della Pepa, G., Vitale, M., Testa, R., Cipriano, P., Scidà, G., Rivellese, A. A., Annuzzi, G., & Bozzetto, L. (2024). Differential Effects of Two Isocaloric Healthy Diets on Postprandial Lipid Responses in Individuals with Type 2 Diabetes. Nutrients, 16(3), 333. https://doi.org/10.3390/nu16030333