

The Relationship Between the Mediterranean Dietary Pattern and Exercise and Sport Performance—A Scoping Review



Highlights
- This is the first scoping review of MedDiet adherence focusing on outcomes relating to sport.
- Almost all the studies were conducted in Mediterranean countries.
- A limited number of studies have looked at the impact of adherence to MedDiet on performance and health in adolescent and adult athletes.
- Only two studies assessed the adequacy of CHO and protein in the MedDiet.
Abstract
1. Introduction
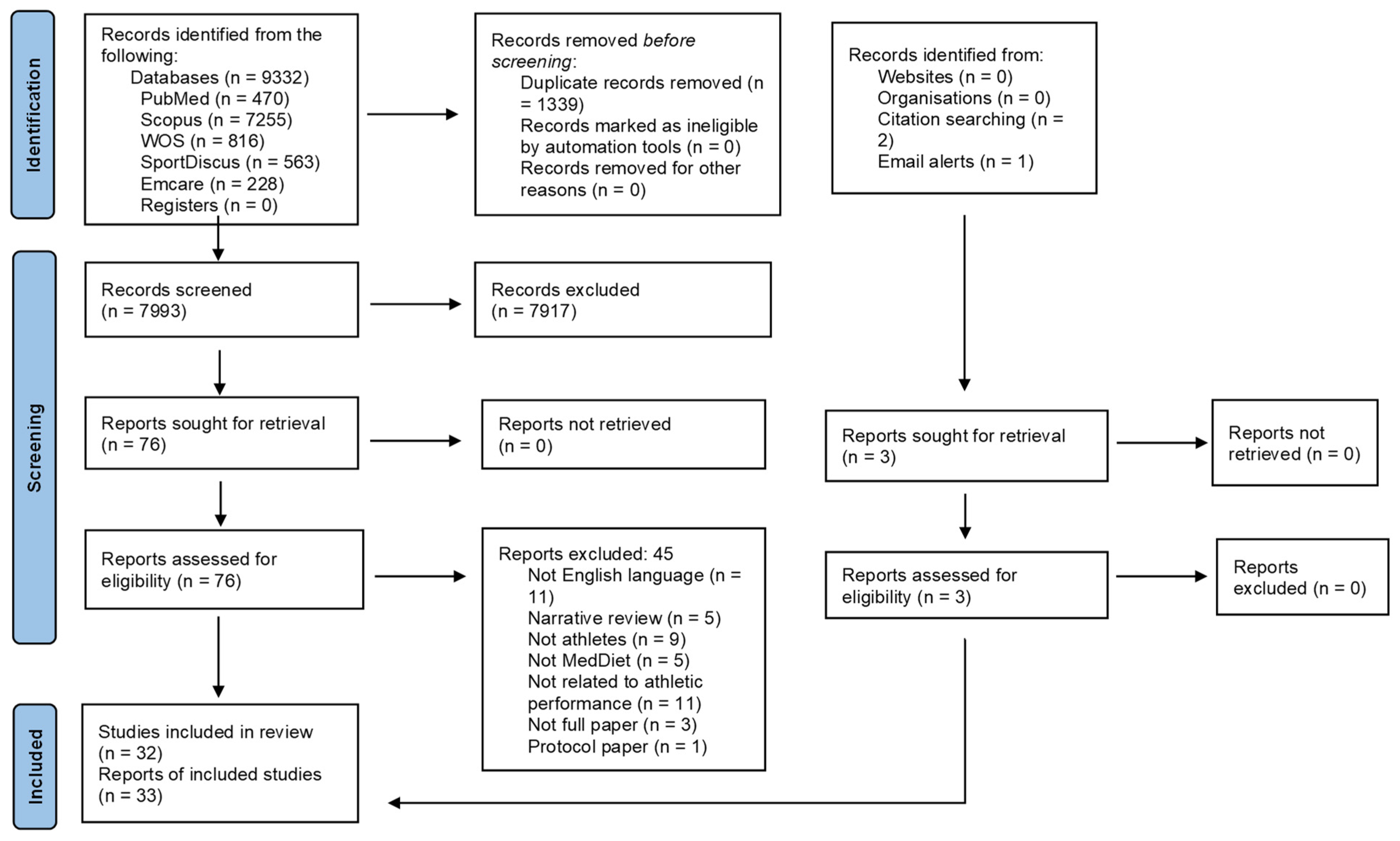
2. Materials and Methods
2.1. Literature Search Strategy
2.2. Eligibility Criteria
2.3. Study Selection, Data Management, and Extraction
2.4. Analysis and Reporting
2.5. Quality Assessment
2.6. Equity, Diversity, and Inclusion Statement
3. Results

{kind=link}
| Observational Studies | |||||
|---|---|---|---|---|---|
| Author Country of Study | Participants | MedDiet Measure and Adherence Level (Mean ± SD or %) | Outcomes | JBI Score for Quality of Cross-Sectional Study | |
| Altavilla et al., 2021 [34] Spain | Semi-professional adolescent swimmers with minimum 3 years of experience and 5–6 swimming sessions (90–120 min, covering minimum 3000 m)/week m—n = 34, age 14.5 ± 1.3 years wt 56.5 ± 9.8 kg, BMI 20.06 ± 2.5 kg/m2 f—n = 40), age 13.6 ± 1.2 years wt 50.2 ± 8.1 kg, BMI 20 ± 2.8 kg/m2 | KidMed m—8.09 ± 1.5 f—7.23 ± 2.2 (medium adherence) | BMI, Waist–Hip Ratio | 6/8 | |
| Citarella et al., 2021 [35] Italy | Elite runners from Italian national ultramarathon team n = 10, age 41.1 ± 7.59 years, BMI 21.66 ± 1.11 kg/m2 m—n = 6, age 40.80 ± 5.4; BMI 21.79 ± 1.06 kg/m2 f—n = 4, age 39.5 ± 10.47, BMI 21.45 ± 1.31 kg/m2 | MDAS Total 46.97 ± 11.96 m—39.94 ± 6.33 f—57.50 ± 10.78 | Weight, Body composition, training volume (km per week), record in the 100 km competition | 4/8 | |
| Kontele et al., 2021 [51] Greece | Adolescent female athletes who participated in all disciplines of gymnastics in Greece n = 269 btw age 11 and 18 years, mean age 13.89 ± 1.75 years, BMI 19.0 ± 2.45 kg/m2 | KidMed 34.9% high adherence 56.1% moderate adherence 8.9% low adherence | Weight, BMI | 6/8 | |
| Leao et al., 2023 [52] Portugal | Male soccer players Three training sessions/week of 90 min duration, and one competitive match/week n = 132, age 7–15 years | KidMed ave 8.36 ± 1.92 68.2% high, 31.1% moderate, 0.8% low adherence | BMI | 7/8 | |
| Lopez-Jimenez et al., 2023 [53] Spain | Elite male rugby union players n = 35, age 24.8 ± 0.8 years, wt 99.2 ± 2.72 kg | KidMed Moderate adherence | Body weight, BMI | 8/8 | |
| Manzano-Carrasco et al., 2020 [36] Spain | Athletes enrolled in different municipal school sports n = 1198; m—n = 875; and f—n = 323 age 6–17 years | KidMed m—35.3% high, 57.6% moderate, 7.1% low adherence f—33.1% high, 59.8% moderate, 7.1% low adherence | Body composition, 20 m shuttle run test, countermovement jump, forced vital capacity, forced expiratory volume, peak expiratory flow, mean forced expiratory flow | 6/8 | |
| Manzano-Carrasco et al., 2020 [37] Spain | Adolescent male football players, enrolled in 3 municipal football sport schools, trained 2 d/w for at least 2 h n = 194, aged 8–16 years; average 12 ± 2 years | KidMed 7.14 ± 1.95 | 20 m shuttle run test, handgrip strength test | 6/8 | |
| Manzano-Carrasco et. al., 2020 [38] Spain | Athletes who practice any sport modality at least 2 days a week for 1 h n = 1676, age 6–17 years; ave 11.11 ± 2.62 years wt 44.48 ± 15.25 kg, 56.6% of sample (n = 947) were classified as normoweight, 26.6% (n = 445) as overweight, and 16.9% (n = 284) as obese | KidMed 35.7% high, 57.6% medium, 6.7% low adherence | Weight, BMI, Body composition, 20mSRT, Abalakov jump, handgrip strength | 6/8 | |
| Marques-Sule et al., 2022 [50] Spain | Professional canoe polo athletes n = 43 (m—36, f—5), n = 23 under 21 years, n = 20 over 21 years, mean age—21.54 ± 6.03 years BMI 23.27 ± 2.61 kg/m2 | MEDAS-14, Healthy-Eating Index-Spanish 0% high, 30.2% moderate, 69.8% low adherence | Body fat; BMI; shoulder rotation range of motion; handgrip strength; push strength—overall; push strength—rowing; countermovement jump; push-up test; sit-to-stand test; motivation to exercise (Exercise Motivation index) | 6/8 | |
| Martinez-Rodriguez et al., 2018 [40] & Martinez-Rodriguez et al., 2017 [41] Spain | Young elite sailors n = 75, m—n = 50, f—n = 25, age 15.7 ± 1.8 years | MEDAS n = 47 low adherence (<6 pts), n = 28 high adherence (>6 pts) | Sex, BMI, competition success, anxiety | 8/8 | |
| Martinez-Rodriguez et al., 2021 [39] Spain | Female beach handball players (n = 33) on Spanish national team n = 18 juniors (Age 16.7 ± 0.50 years) N = 15 seniors (Age 24.8 ± 4.71 years) BMI (juniors): 22.5 ± 2.28 kg/m2 BMI (seniors): 22.8 ± 2.75 kg/m2 | KidMed Junior—7.33 ± 1.61 (moderate adherence) Senior—6.27 ± 2.05 (moderate adherence) | Weight, BMI, handgrip test, Abalakov, yo-yo test, Bone Quality (Broadband ultrasound attenuation, sound of speed, and stiffness) | 5/8 | |
| Martinez-Rodriguez et al., 2021 [42] Spain | Spanish national beach handball players, n = 59 Female n = 21, Junior: 16.1 ± 1.46 years; 14–17 years, wt—56.3 ± 8.7 kg, Senior: 23.2 ± 2.9 years; 18–28 years, wt—63.7 ± 8.9 kg Male n = 38, Junior: 17.0 ± 0.1 years; 15–18 years, wt—70.1 ± 11.2 kg, Senior: 25.5 ± 4.7 years; 18–35 years, wt—81.3 ± 7.6 kg | KidMed f—76% moderate, 9.52% low adherence m—66% moderate, 20% low adherence | BMI, Body composition, height, weight, handgrip strength, countermovement jump | 6/8 | |
| Martinez-Rodriguez et al., 2022 [48] Spain | Professional male beach handball players n = 36, age 16–35 years, mean 20.9 ± 5.55 years Weight range 63.5–115 kg, mean 84.1 ± 14.0 kg BMI range 19.8–30.4 kg/m2, mean 24.6 ± 2.73 kg/m2 | KidMed 6.78 ± 2.38 Junior—6.83 ± 2.26 Senior—6.72 ± 2.56 | Body composition, weight, height, BMI, countermovement jump, Abalakov, handgrip strength, yo-yo test, VO2 max | 6/8 | |
| Martinovic et al., 2022 [57] Croatia | Professional athletes n = 150, m—n= 58, BMI 24.8 ± 3.3 kg/m2, age 24.5 ± 4.0 year Recreational athletes n = 150—m 52 BMI 23.8 ± 3.0 kg/m2, age 24.0 ± 5.5 years | MDSS Professional athletes—24% high adherence Recreational athletes—14% high adherence | MET score, orthorexia nervosa (ORTO-15) | 8/8 | |
| Mayolas-Pi et al., 2017 [43] Spain | Cyclists n = 859, m—751, and f—108, and inactive subjects n = 718, m = 307, and f—411 | MEDAS Overall adherence not reported | Risk of exercise addiction | 5/8 | |
| Morales-Suarez-Varela et al., 2023 [54] Spain | Basketball players, age 8–15 years n = 183, m—n = 107, f—n = 76 | KidMed Mean scores between 8.71 ± 1.98 and 9.07 ± 1.48 across different groups | Athlete burnout questionnaire ABQ | 6/8 | |
| Papdopoulou et al., 2017 [44] Greece | Male cycling athletes, age 15–50 years, with 6 years of sequential training and competed on Greek national team, n = 50, age 32 ± 20 years, BMI 23.65 ± 2.74 kg/m2 | MedDiet Score n = 1 high, n = 43 moderate, n-6 low adherence | Physical performance | 7/8 | |
| Pelaez-Barrios et al., 2022 [49] Spain | Acrobatic gymnasts N = 151 (N = 81 gymnasts and N = 70 non-gymnasts), age 10–19 years (mean 13.85 ± 2.45 years) | KidMed Gymnasts—70.4% high, 26.2% moderate, 2.5% low adherence Non-gymnasts—31.4% high, 62.9% moderate, 5.7% low adherence | Body shape questionnaire, height, weight, waist circumference, BMI, % body fat | 6/8 | |
| Peraita-Costa et al., 2020 [45] Spain | Tennis players—children and adolescents, training minimum 2 h/day n = 94, age 8–15 years, n = 56 boys, and n = 38 girls | KidMed 78.7% moderate, 21.3% high adherence | Burnout syndrome | 6/8 | |
| Romero-Garcia et al., 2022 [55] Spain | Male handball players from 12 to 28 years old n = 136, infant n = 35, 13.41 ± 0.4 year; cadets n = 46 14.83 ± 0.64 years and juniors n = 26 17.2 ± 0.55 years | KidMed Total—42.1% high, 47.4% moderate, 10.5% low adherence | Weight, height, Body composition, BMI, T-Half test, yo-yo test, VO2 max, squat jump, countermovement jump, overhead medicine ball throw test, 30 m sprint | 6/8 | |
| Santana et al., 2019 [46] Spain | Female rhythmic gymnastics from 6 to 17 years old n = 221 (56.11% < 13 years) | KidMed 41.63% high, 52.94% medium, 5.43% low adherence | Waist circumference, BMI, height, weight | 6/8 | |
| Santos-Sanchez et al., 2021 [72] Spain | 71 U12 male soccer players Age 8–12 years (grouped as 8–10 and 10–12) | KidMed 7.83 ± 2.03 | MedDiet adherence, weight, height, BMI, % body fat | 5/8 | |
| Toti et al., 2022 [56] Italy | Wheelchair adult male basketballers, n = 15, age 28.5 ± 1.5 year; gym attendees, n = 15, age 31.5 ± 2.2 years; healthy non-active people, n = 15, age 30.1 ± 2.2 years | MDS 3-day diet record wheelchair basketballers 6.3 ± 0.6, gym attendees 7.5 ± 0.5, healthy non-active people 6.7 ± 0.5 | Orthorexia nervosa, gastro-oesophageal reflux, neurogenic bowel dysfunction | 8/8 | |
| Experimental Studies | |||||
| Author Country of Study | Athlete Characteristics | Intervention and Study Design | Dietary Assessment and Monitoring of Adherence | Outcomes Assessed | JBI Score for Quality of RCT Study or Quasi-Experimental Study |
| Randomised Controlled Trials | |||||
| Baker et al., 2019 [58] United States of America | Recreationally active athletes f—n = 7, m—n = 4 age 28 ± 3 year, BMI 24.6 ± 3.2 kg/m2 | Randomised sequence cross-over trial. A total of 4 days of MedDiet and 4 days of Western diet. A 9–16-day washout period between 2 diets Not indicated if dietitians provided diets No specific sports nutrition recommendations provided | A 3 × 4-day weighed electronic dietary record during each diet period. Research dietitians monitored adherence and assessed food records Significant increase in intake of fruits, vegetables, fish, and olive oil | 5 km treadmill time trial, Wingate cycle test, vertical jump test, handgrip strength, heart rate | 10/13 |
| Chilelli et al., 2016 [59] Italy | Male masters cyclists, n = 47 | 3-month RCT 2 groups: 1. MedDiet—age 46 ± 8 years, wt 71.8 ± 9.6 kg, BMI 23.0 ± 6.4 kg/m2 2. MedDiet + curcumin (10 mg) + Boswellia (140 mg)—age 45 ± 9 years, wt 72.4 ± 8.0 kg, BMI 23.7 ± 2.1 kg/m2 No specific sports nutrition recommendations provided | FFQ—assessed by dietitians, adherence to MedDiet and intake not assessed | Oxidative stress, total advanced glycation endpoints (AGEs), inflammatory mediators | 7/13 |
| Ficarra et al., 2022 [62] Italy | Cross-fit athletes with 1 yr of regular training for a minimum 3 times/week n = 30, f—n = 15, m—n = 15, age 20–50 years | 8-week RCT, MedDiet vs. Habitual Diet Diets planned by dietitian Protein intake based on training sessions and training load per week—range was 1.4–2.0 g/kg/d | Dietary intakes not assessed | Body composition, body circumferences, Wingate 30 s, quat jump, countermovement jump, 30 s jump, push-up test to exhaustion, chin-up test to exhaustion, Fran training | 6/13 |
| Malaguti et al., 2008 [60] Italy | Male, non-professional volleyball athletes who trained at least 3 times/week, and each training session lasted 2 h n = 11 | 2-month RCT MedDiet vs. High-protein low-caloric diet + fish oil diet No specific sports nutrition recommendations provided | Detailed record of weekly food intake (frequency not stated) FFQ—3 times during study Adherence to diet not reported Not stated if dietitians assessed food records | BMI Body composition, total antioxidant activity | 6/13 |
| Miralles-Amoros et al., 2023 [63] Spain | Elite female professional handball players n = 21, age 22 ± 4 years | 12-week RCT with 3 diet arms: 1. Free diet. 2. MedDiet. 3. High-antioxidant diet. | 7-day self-recorded dietary record at 3 timepoints Adherence not reported | Weight, height, BMI, Body composition, Eating behaviour (EAT-26), Body image BSQ, Mood (POMS) | 8/13 |
| Soldati et al., 2019 [61] Italy | Kickboxers Male n = 20 and Half-marathon runners Male n = 20 Athletes from all competition levels | 3-month Nutritional counselling intervention on MedDiet vs. Control diet Sports-specific recommendations—considered primary energy source dependent on sports | 3-day diary at beginning and end of study MedDiet adherence checked by food recall by nutritionists but not reported | Countermovement jump, squat jump, 15″ test, bench test, VO2 max, Body fat mass, RMR | 7/13 |
| Quasi-experimental Studies | |||||
| Caparello et al., 2023 [66] Italy | Male volleyballers from national league n = 11, age 19–37 years | All athletes underwent a nutrition education session and were provided with personalised plan before pre-season on MedDiet +/− ergogenic supplements by nutritionists Protein intake based on training sessions and training load per week—range was 1.0–1.5 g/kg/d | Weekly food diary MEDAS Not stated who checked food diaries Adherence at baseline 9.8 ± 1.1, pre-season 10 ± 0.2, season 10.3 ± 0.1, play-offs 10.2 ± 0.1 (all not significant) | MedDiet adherence, BMI, Body composition, Basal and Resting Metabolic rate | 8/9 |
| Philippou et al., 2017 [64] Cyprus | Adolescent competitive swimmers, f—n = 11, m—n = 23, and 22 parents) Mean age 15.2 ± 1.5 years | Nutrition education session on MedDiet (1/2 day) | KidMed Improvement in adherence with 47% having good adherence post-intervention vs. 21% at baseline (p < 0.01) and an increase in KIDMED Index score (median [interquartile range]: 5.0 [4.0–7.0] vs. 7.0 [7.0–9.0]; p < 0.01) | Nutrition knowledge, MedDiet adherence, changes in intakes of foods in MedDiet | 8/9 |
| Sahnoune et al., 2020 [65] Algeria | Adolescent athletes who train for 6–10 h/week in handball, athletics, basketball, swimming, judo | Nutrition education sessions on MedDiet (6 sessions). Changes assessed after 6 months | KidMed At baseline, 8% good, 31% moderate, 61% poor adherence After intervention, 60% good, 30% moderate, 10% poor adherence. | MedDiet adherence, weight, BMI, International physical activity questionnaire (IPAQ) | 7/9 |
Assessment of Quality of Studies
4. Discussion
Recommendations
- Theoretical and intervention studies should consider the nutritional adequacy of the MedDiet for its potential to meet prescriptive sports nutrition guidelines (e.g., protein and CHO).
- Theoretical and intervention studies need to consider the nutritional adequacy of the MedDiet for injury and rehabilitation—specifically looking at protein and other key micronutrients.
- Future studies need to be conducted with athletes from non-Mediterranean countries to assess the adherence, feasibility, and acceptance of the MedDiet.
- More high-quality intervention studies are needed that assess changes in anthropometric measures, sport-related performance outcomes, and wellbeing in a range of athletes (different ages and genders) to provide high-quality causal evidence.
- A more rigorous reporting (both qualitative and quantitative) of the prescribed components of the MedDiet and adherence to the MedDiet is needed in future intervention studies.
- Future studies should explore the feasibility and acceptability of the MedDiet for athletes while travelling for training and competition.
- The nutritional adequacy, acceptability, and benefits of the MedDiet in masters athletes and para athletes need to be evaluated.
- Future intervention and longitudinal observational studies should consider the impact of the MedDiet on short- and long-term health outcomes for athletes.
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Schenk, M.; Miltenberger, R. A review of behavioral interventions to enhance sports performance. Behav. Interv. 2019, 34, 248–279. [Google Scholar] [CrossRef]
- Bonnar, D.; Bartel, K.; Kakoschke, N.; Lang, C. Sleep Interventions Designed to Improve Athletic Performance and Recovery: A Systematic Review of Current Approaches. Sports Med. 2018, 48, 683–703. [Google Scholar] [CrossRef] [PubMed]
- Ross, M.; Abbiss, C.; Laursen, P.; Martin, D.; Burke, L. Precooling Methods and Their Effects on Athletic Performance. Sports Med. 2013, 43, 207–225. [Google Scholar] [CrossRef] [PubMed]
- Thomas, D.T.; Erdman, K.A.; Burke, L.M. Position of the Academy of Nutrition and Dietetics, Dietitians of Canada, and the American College of Sports Medicine: Nutrition and Athletic Performance. J. Acad. Nutr. Diet. 2016, 116, 501–528. [Google Scholar] [CrossRef]
- Lambert, V.; Carbuhn, A.; Culp, A.; Ketterly, J.; Twombley, B.; White, D. Interassociation Consensus Statement on Sports Nutrition Models for the Provision of Nutrition Services from Registered Dietitian Nutritionists in Collegiate Athletics. J. Athl. Train. 2022, 57, 717–732. [Google Scholar] [CrossRef]
- Heaney, S.; O’Connor, H.; Naughton, G.; Gifford, J. Towards an Understanding of the Barriers to Good Nutrition for Elite Athletes. Int. J. Sports Sci. Coach. 2008, 3, 391–401. [Google Scholar] [CrossRef]
- Trakman, G.L.; Forsyth, A.; Hoye, R.; Belski, R. Australian team sports athletes prefer dietitians, the internet and nutritionists for sports nutrition information. Nutr. Diet. 2019, 76, 428–437. [Google Scholar] [CrossRef]
- Janiczak, A.; Devlin, B.L.; Forsyth, A.; Trakman, G.L. A systematic review update of athletes’ nutrition knowledge and association with dietary intake. Br. J. Nutr. 2022, 128, 1156–1169. [Google Scholar] [CrossRef]
- Boidin, A.; Tam, R.; Mitchell, L.; Cox, G.R.; O’Connor, H. The effectiveness of nutrition education programmes on improving dietary intake in athletes: A systematic review. Br. J. Nutr. 2021, 125, 1359–1373. [Google Scholar] [CrossRef]
- Riviere, A.J.; Leach, R.; Mann, H.; Robinson, S.; Burnett, D.O.; Babu, J.R.; Frugé, A.D. Nutrition Knowledge of Collegiate Athletes in the United States and the Impact of Sports Dietitians on Related Outcomes: A Narrative Review. Nutrients 2021, 13, 1772. [Google Scholar] [CrossRef]
- Tapsell, L.C.; Neale, E.P.; Satija, A.; Hu, F.B. Foods, Nutrients, and Dietary Patterns: Interconnections and Implications for Dietary Guidelines. Adv. Nutr. 2016, 7, 445–454. [Google Scholar] [CrossRef] [PubMed]
- Bach-Faig, A.; Berry, E.M.; Lairon, D.; Reguant, J.; Trichopoulou, A.; Dernini, S.; Medina, F.X.; Battino, M.; Belahsen, R.; Miranda, G.; et al. Mediterranean diet pyramid today. Science and cultural updates. Public Health Nutr. 2011, 14, 2274–2284. [Google Scholar] [CrossRef]
- Dinu, M.; Pagliai, G.; Casini, A.; Sofi, F. Mediterranean diet and multiple health outcomes: An umbrella review of meta-analyses of observational studies and randomised trials. Eur. J. Clin. Nutr. 2018, 72, 30–43. [Google Scholar] [CrossRef] [PubMed]
- Guasch-Ferre, M.; Willett, W.C. The Mediterranean diet and health: A comprehensive overview. J. Intern. Med. 2021, 290, 549–566. [Google Scholar] [CrossRef] [PubMed]
- Willett, W.C.; Sacks, F.; Trichopoulou, A.; Drescher, G.; Ferro-Luzzi, A.; Helsing, E.; Trichopoulos, D. Mediterranean diet pyramid: A cultural model for healthy eating. Am. J. Clin. Nutr. 1995, 61, 1402S–1406S. [Google Scholar] [CrossRef] [PubMed]
- Villani, A.; Sultana, J.; Doecke, J.; Mantzioris, E. Differences in the interpretation of a modernized Mediterranean diet prescribed in intervention studies for the management of type 2 diabetes: How closely does this align with a traditional Mediterranean diet? Eur. J. Nutr. 2019, 58, 1369–1380. [Google Scholar] [CrossRef]
- Vetrani, C.; Piscitelli, P.; Muscogiuri, G.; Barrea, L.; Laudisio, D.; Graziadio, C.; Marino, F.; Colao, A. “Planeterranea”: An attempt to broaden the beneficial effects of the Mediterranean diet worldwide. Front. Nutr. 2022, 9, 973757. [Google Scholar] [CrossRef]
- Burt, K. The whiteness of the Mediterranean Diet: A historical, sociopolitical, and dietary analysis using Critical Race Theory. J. Crit. Diet. 2021, 5, 41–52. [Google Scholar] [CrossRef]
- Martínez-González, M.A.; Salas-Salvadó, J.; Estruch, R.; Corella, D.; Fitó, M.; Ros, E. Benefits of the Mediterranean Diet: Insights from the PREDIMED Study. Prog. Cardiovasc. Dis. 2015, 58, 50–60. [Google Scholar] [CrossRef]
- Schwingshackl, L.; Morze, J.; Hoffmann, G. Mediterranean diet and health status: Active ingredients and pharmacological mechanisms. Br. J. Pharmacol. 2020, 177, 1241–1257. [Google Scholar] [CrossRef]
- Trichopoulou, A.; Martínez-González, M.A.; Tong, T.Y.N.; Forouhi, N.G.; Khandelwal, S.; Prabhakaran, D.; Mozaffarian, D.; de Lorgeril, M. Definitions and potential health benefits of the Mediterranean diet: Views from experts around the world. BMC Med. 2014, 12, 112. [Google Scholar] [CrossRef] [PubMed]
- Alacid, F.; Vaquero-Cristóbal, R.; Sánchez-Pato, A.; Muyor, J.M.; López-Miñarro, P.Á. Habit based consumptions in the mediterranean diet and the relationship with anthropometric parameters in young female kayakers. Nutr. Hosp. 2014, 29, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Mayolas-Pi, C.; Munguia-Iziquierdo, D.; Penaarrubia-Lozano, C.; Reverter-Masia, J.; Bueno-Antequera, J.; Lopez-Lavali, I.; Oviedo-Caro, M.Á.; Murillo-Lorente, V.; Murillo-Fuentes, A.; Paris-Garcia, F.; et al. Adherence to the Mediterranean diet in inactive adults, indoor cycling practitioners and amateur cyclists. Nutr. Hosp. 2018, 35, 131–139. [Google Scholar]
- Muros, J.J.; Zabala, M. Differences in mediterranean diet adherence between cyclists and triathletes in a sample of Spanish athletes. Nutrients 2018, 10, 1480. [Google Scholar] [CrossRef]
- Rubio-Arias, J.Á.; Ramos-Campo, D.J.; Nunez, J.M.R.; Poyatos, M.C.; Ramon, P.E.A. Adherence to a Mediterranean Diet and Sport Performance in a elite female athletes futsal population. Nutr. Hosp. 2015, 31, 2276–2282. [Google Scholar]
- Sanchez-Benito, J.; Sanchez-Soriano, E.; Suarez, J.G. Assessment of the Mediterranean Diet Adequacy Index of a collective of young cyclists. Nutr. Hosp. 2009, 24, 77–86. [Google Scholar]
- Calella, P.; Gallè, F.; Di Onofrio, V.; Cerullo, G.; Liguori, G.; Valerio, G. Adherence to Mediterranean diet in athletes: A narrative review. Sport. Sci. Health 2022, 18, 1141–1148. [Google Scholar] [CrossRef]
- Pelaez Barrios, E.; Sanatana, M. Adherence to the Mediterranean Diet in children and adolescent athletes: A systematic review. Think. Motion J. Exerc. Health Sci. 2021, 19, e42850. [Google Scholar] [CrossRef]
- Griffiths, A.; Matu, J.; Whyte, E.; Akin-Nibosun, P.; Clifford, T.; Stevenson, E.; Shannon, O.M. The Mediterranean dietary pattern for optimising health and performance in competitive athletes: A narrative review. Br. J. Nutr. 2021, 128, 1285–1298. [Google Scholar] [CrossRef]
- d’Unienville, N.M.A.; Blake, H.T.; Coates, A.M.; Hill, A.M.; Nelson, M.J.; Buckley, J.D. Effect of food sources of nitrate, polyphenols, L-arginine and L-citrulline on endurance exercise performance: A systematic review and meta-analysis of randomised controlled trials. J. Int. Soc. Sports Nutr. 2021, 18, 1–28. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Moola, S.; Munn, Z.; Tufanaru, C.; Aromataris, E.; Sears, K.; Srfectu, R.; Currie, M.; Qureshi, R.; Mattis, P.; Lisy, K.; et al. Chapter 7: Systematic reviews of etiology and risk. In JBI Manual for Evidence Synthesis; Aromataris, E., Munn, Z., Eds.; JBI: Adelaide, Australia, 2020; Available online: https://synthesismanual.jbi.global (accessed on 21 June 2021).
- Radd-Vagenas, S.; Singh, M.A.F.; Daniel, K.; Noble, Y.; Jain, N.; O’Leary, F.; Mavros, Y.; Heffernan, M.; Meiklejohn, J.; Guerrero, Y.; et al. Validity of the mediterranean diet and culinary index (Medicul) for online assessment of adherence to the ’traditional’ diet and aspects of cuisine in older adults. Nutrients 2018, 10, 1913. [Google Scholar] [CrossRef] [PubMed]
- Altavilla, C.; Joulianos, A.; Guijarro, J.M.C.; Perez, P.C. Adherence to the Mediterranean diet, is there any relationship with main indices of central fat in adolescent competitive swimmers? Arch. Med. Deporte 2021, 38, 113–118. [Google Scholar] [CrossRef]
- Citarella, R.; Itani, L.; Intini, V.; Zucchinali, G.; Scevaroli, S.; Tannir, H.; El Masri, D.; Kreidieh, D.; El Ghoch, M. Association between dietary practice, body composition, training volume and sport performance in 100-Km elite ultramarathon runners. Clin. Nutr. ESPEN 2021, 42, 239–243. [Google Scholar] [CrossRef]
- Manzano-Carrasco, S.; Felipe, J.L.; Sanchez-Sanchez, J.; Hernandez-Martin, A.; Clavel, I.; Gallardo, L.; Garcia-Unanue, J. Relationship between adherence to the mediterranean diet and body composition with physical fitness parameters in a young active population. Int. J. Environ. Res. Public Health 2020, 17, 3337. [Google Scholar] [CrossRef]
- Manzano-Carrasco, S.; Felipe, J.L.; Sanchez-Sanchez, J.; Hernandez-Martin, A.; Gallardo, L.; Garcia-Unanue, J. Physical fitness, body composition, and adherence to the mediterranean diet in young football players: Influence of the 20 msrt score and maturational stage. Int. J. Environ. Res. Public Health 2020, 17, 3257. [Google Scholar] [CrossRef]
- Manzano-Carrasco, S.; Felipe, J.L.; Sanchez-Sanchez, J.; Hernandez-Martin, A.; Gallardo, L.; Garcia-Unanue, J. Weight status, adherence to the mediterranean diet, and physical fitness in spanish children and adolescents: The active health study. Nutrients 2020, 12, 1680. [Google Scholar] [CrossRef]
- Martínez-Rodríguez, A.; Sánchez-Sánchez, J.; Martínez-Olcina, M.; Vicente-Martínez, M.; Miralles-Amorós, L.; Sánchez-Sáez, J.A. Study of Physical Fitness, Bone Quality, and Mediterranean Diet Adherence in Professional Female Beach Handball Players: Cross-Sectional Study. Nutrients 2021, 13, 1911. [Google Scholar] [CrossRef]
- Martínez-Rodríguez, A.; Chicoy-García, I.; Leyva-Vela, B.; Martínez-Hernández, M.; Serrano, A.M. Influence of low fat Mediterranean diet adherence in young elite sailors’ performance. Rev. Esp. Nutr. Comunitaria 2018, 24. [Google Scholar]
- Martínez-Rodríguez, A.; Chicoy-García, I.; Leyva-Vela, B.; Martínez-Hernández, M.; Serrano, A.M. Could low fat mediterranean diet improves competitive anxiety in young sailors? Cross-sectional study according to the STROBE statement. Cuad. Psicol. Deporte 2017, 17, 95–104. [Google Scholar]
- Martínez-Rodríguez, A.; Martínez-Olcina, M.; Hernández-García, M.; Rubio-Arias, J.Á.; Sánchez-Sánchez, J.; Lara-Cobos, D.; Vicente-Martínez, M.; Carvalho, M.J.; Sánchez-Sáez, J.A. Mediterranean diet adherence, body composition and performance in beach handball players: A cross sectional study. Int. J. Environ. Res. Public Health 2021, 18, 2837. [Google Scholar] [CrossRef] [PubMed]
- Mayolas-Pi, C.; Simón-Grima, J.; Peñarrubia-Lozano, C.; Munguía-Izquierdo, D.; Moliner-Urdiales, D.; Legaz-Arrese, A. Exercise addiction risk and health in male and female amateur endurance cyclists. J. Behav. Addict. 2017, 6, 74–83. [Google Scholar] [CrossRef] [PubMed]
- Papadopoulou, S.; Kroustalloudi, E.; Pagkalos, I.; Kokkinopoulou, A.; Hassapidou, M. The Effect of Ergogenic Supplements and Mediterranean Diet on Cycling Performance. Differences According to Duration and Intensity. Arab. J. Nutr. Exerc. (AJNE) 2017, 2, 23–29. [Google Scholar] [CrossRef]
- Peraita-Costa, I.; Llopis-Morales, A.; Marí-Bauset, S.; Marí-Sanchis, A.; Marí-Sanchis, S.; Morales-Suárez-varela, M. Burnout syndrome risk in child and adolescent tennis players and the role of adherence to the mediterranean diet. Int. J. Environ. Res. Public Health 2020, 17, 929. [Google Scholar] [CrossRef] [PubMed]
- Santana, M.V.; Mirón, I.M.; Vargas, L.A.; Bedoya, J.L. Comparative analysis of adherence to the mediterranean diet among girls and adolescents who perform rhythmic gymnastics. Rev. Bras. Med. Esporte 2019, 25, 280–284. [Google Scholar] [CrossRef]
- Santos-Sánchez, G.; Cruz-Chamorro, I.; Perza-Castillo, J.L.; Vicente-Salar, N. Body Composition Assessment and Mediterranean Diet Adherence in U12 Spanish Male Professional Soccer Players: Cross-Sectional Study. Nutrients 2021, 13, 4045. [Google Scholar] [CrossRef]
- Martínez-Rodríguez, A.; Sánchez-Sánchez, J.; Martínez-Olcina, M.; Vicente-Martínez, M.; Yáñez-Sepúlveda, R.; Cortés-Roco, G.; Vázquez-Diz, J.A.; Sánchez-Sáez, J.A. Professional Male Beach Handball Players Performance Profile. Nutrients 2022, 14, 4839. [Google Scholar] [CrossRef]
- Pelaez-Barrios, E.M.; Vernetta, M. Body Dissatisfaction, Mediterranean Diet Adherence and Anthropometric Data in Female Gymnasts and Adolescents. Apunts. Educ. Fís. Esports 2022, 149, 13–22. [Google Scholar] [CrossRef]
- Marques-Sule, E.; Arnal-Gómez, A.; Monzani, L.; Deka, P.; López-Bueno, J.P.; Saavedra-Hernández, M.; Suso-Martí, L.; Espí-López, G.V. Canoe polo Athletes’ Anthropometric, Physical, Nutritional, and Functional Characteristics and Performance in a Rowing Task: Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 13518. [Google Scholar] [CrossRef]
- Kontele, I.; Grammatikopoulou, M.G.; Vassilakou, T. Level of Adherence to the Mediterranean Diet and Weight Status among Adolescent Female Gymnasts: A Cross-Sectional Study. Children 2021, 8, 1135. [Google Scholar] [CrossRef]
- Leão, C.; Rocha-Rodrigues, S.; Machado, I.; Lemos, J.; Leal, S.; Nobari, H. Adherence to the Mediterranean diet in young male soccer players. BMC Nutr. 2023, 9, 101. [Google Scholar] [CrossRef] [PubMed]
- López-Jiménez, A.; Morán-Fagúndez, L.; Sánchez-Sánchez, A.M.; Fernández-Pachón, M.-S. The associations between anthropometric characteristics and nutritional parameters in male elite rugby union players. Int. J. Food Sci. Nutr. 2023, 74, 707–718. [Google Scholar] [CrossRef] [PubMed]
- Morales-Suárez-Varela, M.; Peraita-Costa, I.; Llopis-Morales, A.; Llopis-González, A. Athletic Burnout and Its Association with Diet in Children and Adolescents. Life 2023, 13, 1381. [Google Scholar] [CrossRef] [PubMed]
- Romero-García, D.; Esparza-Ros, F.; Picó García, M.; Martínez-Sanz, J.M.; Vaquero-Cristóbal, R. Adherence to the Mediterranean diet, kinanthropometric characteristics and physical performance of young male handball players. PeerJ 2022, 10, e14329. [Google Scholar] [CrossRef] [PubMed]
- Toti, E.; Cavedon, V.; Raguzzini, A.; Fedullo, A.L.; Milanese, C.; Bernardi, E.; Bellito, S.; Bernardi, M.; Sciarra, T.; Peluso, I. Dietary Intakes and Food Habits of Wheelchair Basketball Athletes Compared to Gym Attendees and Individuals who do not Practice Sport Activity. Endocr. Metab. Immune Disord. Drug Targets 2022, 22, 38–48. [Google Scholar] [CrossRef]
- Martinovic, D.; Tokic, D.; Martinovic, L.; Vilovic, M.; Vrdoljak, J.; Kumric, M.; Bukic, J.; Kurir, T.T.; Tavra, M.; Bozic, J. Adherence to Mediterranean Diet and Tendency to Orthorexia Nervosa in Professional Athletes. Nutrients 2022, 14, 237. [Google Scholar] [CrossRef]
- Baker, M.E.; DeCesare, K.N.; Johnson, A.; Kress, K.S.; Inman, C.L.; Weiss, E.P. Short-Term Mediterranean Diet Improves Endurance Exercise Performance: A Randomized-Sequence Crossover Trial. J. Am. Coll. Nutr. 2019, 38, 597–605. [Google Scholar] [CrossRef]
- Chilelli, N.C.; Ragazzi, E.; Valentini, R.; Cosma, C.; Ferraresso, S.; Lapolla, A.; Sartore, G. Curcumin and Boswellia serrata modulate the glyco-oxidative status and lipo-oxidation in master athletes. Nutrients 2016, 8, 745. [Google Scholar] [CrossRef]
- Malaguti, M.; Baldini, M.; Angeloni, C.; Biagi, P.; Hrelia, S. High-protein-PUFA supplementation, red blood cell membranes, and plasma antioxidant activity in volleyball athletes. Int. J. Sport Nutr. Exer. Metabol. 2008, 18, 301–312. [Google Scholar] [CrossRef]
- Soldati, L.; Pivari, F.; Parodi, C.; Brasacchio, C.; Dogliotti, E.; de Simone, P.; Rossi, M.; Vezzoli, G.; Paoli, A. The benefits of nutritional counselling for improving sport performance. J. Sports Med. Phys. Fit. 2019, 59, 1878–1884. [Google Scholar] [CrossRef]
- Ficarra, S.; Di Raimondo, D.; Navarra, G.A.; Izadi, M.; Amato, A.; Macaluso, F.P.; Proia, P.; Musiari, G.; Buscemi, C.; Barile, A.M.; et al. Effects of Mediterranean Diet Combined with CrossFit Training on Trained Adults’ Performance and Body Composition. J. Pers. Med. 2022, 12, 1238. [Google Scholar] [CrossRef] [PubMed]
- Miralles-Amorós, L.; Vicente-Martínez, M.; Martínez-Olcina, M.; Asencio-Mas, N.; Gonzálvez-Alvarado, L.; Peñaranda-Moraga, M.; Leyva-Vela, B.; Yáñez-Sepúlveda, R.; Cortés-Roco, G.; Martínez-Rodríguez, A. Study of Different Personalised Dietary Plans on Eating Behaviour, Body Image and Mood in Young Female Professional Handball Players: A Randomised Controlled Trial. Children 2023, 10, 259. [Google Scholar] [CrossRef] [PubMed]
- Philippou, E.; Middleton, N.; Pistos, C.; Andreou, E.; Petrou, M. The impact of nutrition education on nutrition knowledge and adherence to the Mediterranean Diet in adolescent competitive swimmers. J. Sci. Med. Sport 2017, 20, 328–332. [Google Scholar] [CrossRef] [PubMed]
- Sahnoune, R.; Bouchenak, M. Nutritional intervention promoting Mediterranean diet improves dietary intake and enhances score adherence in adolescent athletes. Mediterr. J. Nutr. Metab. 2020, 13, 237–253. [Google Scholar] [CrossRef]
- Caparello, G.; Galluccio, A.; Ceraudo, F.; Pecorella, C.; Buzzanca, F.; Cuccomarino, F.; Bonofiglio, D.; Avolio, E. Evaluation of Body Composition Changes by Bioelectrical Impedance Vector Analysis in Volleyball Athletes Following Mediterranean Diet Recommendations during Italian Championship: A Pilot Study. Appl. Sci. 2023, 13, 2794. [Google Scholar] [CrossRef]
- Calella, P.; Gallè, F.; Cerullo, G.; Postiglione, N.; Ricchiuti, R.; Liguori, G.; D’Angelo, S.; Valerio, G. Adherence to Mediterranean Diet among athletes participating at the XXX summer universiade. Nutr. Health 2022, 29, 645–651. [Google Scholar] [CrossRef]
- Desbrow, B.; McCormack, J.; Burke, L.M.; Cox, G.R.; Fallon, K.; Hislop, M.; Logan, R.; Marino, N.; Sawyer, S.M.; Shaw, G.; et al. Sports Dietitians Australia Position Statement: Sports Nutrition for the Adolescent Athlete. Int. J. Sport. Nutr. Exer. Metabol. 2014, 24, 570–584. [Google Scholar] [CrossRef]
- Mountjoy, M.; Armstrong, N.; Bizzini, L.; Blimkie, C.; Evans, J.; Gerrard, D.; Hangen, J.; Knoll, K.; Micheli, L.; Sangenis, P.; et al. IOC consensus statement on training the elite child athlete. Clin. J. Sport Med. 2008, 18, 122–123. [Google Scholar] [CrossRef]
- Association, A.D.; Canada, D.o.; Medicine, A.C.o.S.; Rodriguez, N.; Demarco, N.; Langley, S. Position Paper: Nutrition and athleteic performance. J. Am. Diet. Assoc. 2009, 109, 509–527. [Google Scholar]
- Jäger, R.; Kerksick, C.M.; Campbell, B.I.; Cribb, P.J.; Wells, S.D.; Skwiat, T.M.; Purpura, M.; Ziegenfuss, T.N.; Ferrando, A.A.; Arent, S.M.; et al. International Society of Sports Nutrition Position Stand: Protein and exercise. J. Int. Soc. Sports Nutr. 2017, 14, 20. [Google Scholar] [CrossRef]
- Barrios, E.M.P.; Santana, M.V. Differences in body image among female adolescent schools practicing and non-practicing acrobatic gymnastics. Psychol. Soc. Educ. 2022, 14, 48–58. [Google Scholar] [CrossRef]
- Burke, L.M.; Hawley, J.A.; Wong, S.H.; Jeukendrup, A.E. Carbohydrates for training and competition. J. Sports Sci. 2011, 29 (Suppl. S1), S17–S27. [Google Scholar] [CrossRef] [PubMed]
- Guo, S.; Shaoni, G.L.L.; Stuart-Smith, W.A.; Davies, A.J.; Gifford, J.A. Dietary Intake of Masters Athletes: A Systematic Review. Nutrients 2023, 15, 4973. [Google Scholar] [CrossRef] [PubMed]
- McClure, R.; Villani, A. Mediterranean Diet attenuates risk of frailty and sarcopenia: New insights and future directions. JCSM Clin. Rep. 2017, 2, 1–17. [Google Scholar] [CrossRef]
- Islamoglu, A.H.; Kenger, E.B. Nutrition Considerations for Athletes with Physical Disabilities. Curr. Sports Med. Rep. 2019, 18, 270–274. [Google Scholar] [CrossRef]
- Figel, K.; Pritchett, K.; Pritchett, R.; Broad, E. Energy and Nutrient Issues in Athletes with Spinal Cord Injury: Are They at Risk for Low Energy Availability? Nutrients 2018, 10, 1078. [Google Scholar] [CrossRef]
- Reilly, T.; Waterhouse, J.; Burke, L.M.; Alonso, J.M. Nutrition for travel. J. Sports Sci. 2007, 25, S125–S134. [Google Scholar] [CrossRef]
- Lopez-Gil, J.F.; Garcia-Hermoso, A.; Sotos-Prieto, M.; Cavero-Redondo, I.; Martinez-Vizcaino, V.; Kales, S.N. Mediterranean Diet-Based Interventions to Improve Anthropometric and Obesity Indicators in Children and Adolescents: A Systematic Review with Meta-Analysis of Randomized Controlled Trials. Adv. Nutr. 2023, 14, 858–869. [Google Scholar] [CrossRef]
- Scannell, N.; Villani, A.; Mantzioris, E.; Swanepoel, L. Understanding the Self-Perceived Barriers and Enablers toward Adopting a Mediterranean Diet in Australia: An Application of the Theory of Planned Behaviour Framework. Int. J. Environ. Res. Public Health 2020, 17, 9321. [Google Scholar] [CrossRef]
- Renard, M.; Kelly, D.T.; Ní Chéilleachair, N.; Lavelle, F.; Ó Catháin, C. Cooking and food skills confidence of team sport athletes in Ireland. Nutr. Bull. 2023, 48, 329–342. [Google Scholar] [CrossRef]
- Pelly, F.E.; Thurecht, R.L.; Slater, G. Determinants of Food Choice in Athletes: A Systematic Scoping Review. Sports Med. Open 2022, 8, 77. [Google Scholar] [CrossRef] [PubMed]
- Lewis, M.D. Chapter 27—Utilization of Fish Oil for the Prevention and Treatment of Traumatic Brain Injury. In Fish and Fish Oil in Health and Disease Prevention; Raatz, S.K., Bibus, D.M., Eds.; Academic Press: San Diego, CA, USA, 2016; pp. 291–304. [Google Scholar] [CrossRef]
- Mullins, V.A.; Graham, S.; Cummings, D.; Wood, A.; Ovando, V.; Skulas-Ray, A.C.; Polian, D.; Wang, Y.; Hernandez, G.D.; Lopez, C.M.; et al. Effects of Fish Oil on Biomarkers of Axonal Injury and Inflammation in American Football Players: A Placebo-Controlled Randomized Controlled Trial. Nutrients 2022, 14, 2139. [Google Scholar] [CrossRef] [PubMed]
- Therdyothin, A.; Prokopidis, K.; Galli, F.; Witard, O.C.; Isanejad, M. The effects of omega-3 polyunsaturated fatty acids on muscle and whole-body protein synthesis: A systematic review and meta-analysis. Nutr. Rev. 2024, nuae055. [Google Scholar] [CrossRef] [PubMed]
- Mantzioris, E.; Muhlhausler, B.S.; Villani, A. Impact of the Mediterranean Dietary pattern on n-3 fatty acid tissue levels—A systematic review. Prostaglandins Leukot. Essent. Fat. Acids 2022, 176, 102387. [Google Scholar] [CrossRef] [PubMed]
- Altun, A.; Brown, H.; Szoeke, C.; Goodwill, A.M. The Mediterranean dietary pattern and depression risk: A systematic review. Neurol. Psychiatry Brain Res. 2019, 33, 1–10. [Google Scholar] [CrossRef]
- Shafiei, F.; Salari-Moghaddam, A.; Larijani, B.; Esmaillzadeh, A. Adherence to the Mediterranean diet and risk of depression: A systematic review and updated meta-analysis of observational studies. Nutr. Rev. 2019, 77, 230–239. [Google Scholar] [CrossRef]
- Aridi, Y.S.; Walker, J.L.; Wright, O.R.L. The Association between the Mediterranean Dietary Pattern and Cognitive Health: A Systematic Review. Nutrients 2017, 9, 674. [Google Scholar] [CrossRef]
- Petersson, S.D.; Philippou, E. Mediterranean Diet, Cognitive Function, and Dementia: A Systematic Review of the Evidence. Adv. Nutr. 2016, 7, 889–904. [Google Scholar] [CrossRef]
- McKay, A.K.A.; Stellingwerff, T.; Smith, E.S.; Martin, D.T.; Mujika, I.; Goosey-Tolfrey, V.L.; Sheppard, J.; Burke, L.M. Defining Training and Performance Caliber: A Participant Classification Framework. Int. J. Sports Physiol. Perform. 2022, 17, 317–331. [Google Scholar] [CrossRef]
- Sanz de la Garza, M.; Adami, P.E. Definition of Athletes and Classification of Sports. In Textbook of Sports and Exercise Cardiology; Pressler, A., Niebauer, J., Eds.; Springer: Cham, Switzerland, 2020; pp. 3–11. [Google Scholar] [CrossRef]
| Inclusion Criterion | Exclusion Criterion | |
|---|---|---|
| Participants | Human studies with any competing, recreational, professional, elite, or occupational athlete (of any age) who plays a physical sport as part of a team or as an individual. | Studies which included participants involved in non-physical sports such as chess or video gaming |
| Intervention/exposure | Intervention studies which included a whole MedDiet intervention. Observational studies assessing adherence to the MedDiet using a Mediterranean dietary adherence tool. Studies assessing the delivery of single meals aligned with the MedDiet (acute feeding studies). | Studies administering only one or two components or constituents of the MedDiet (i.e., olive oil, nuts) |
| Comparisons | Intervention studies using any other type of dietary intervention or usual diet. | |
| Outcomes | Studies reporting on any outcome related to anthropometry, the assessment of body composition, or sporting or exercise performance or health outcome, e.g., cognitive performance, adherence to the MedDiet, sleep, burnout/fatigue. | Studies not reporting these outcomes |
| Study design | Any intervention study (RCT, pre–post-test series, open-label design RCT). Any observational study. | Systematic reviews and meta-analyses of intervention and observational studies. Conference abstracts, case studies |
| Author, Country, Athletes | Age | Sex | Weight | Height | Body Mass Index | Waist–Height Ratio | Waist Circumference | Arm/Leg Circumference | Body Composition | Performance/Success in Competition | Training Volume/MET Score | Range of Motion | 20 m Shuttle Run Test | 30 m Sprint | Countermovement Jump | Abalakov Jump | Squat Jump | Yo-yo Test | Medicine Ball test | T-half Test | Handgrip Strength | Push Strength | VO2 Max | Forced Vital Capacity | Forced Expiratory Flow | Peak Expiratory Flow | Body Dissatisfaction | Bone Quality | Motivation to Exercise | Burnout Syndrome | Anxiety | Obsession with Food | Risk Exercise Anxiety | Orthorexia Nervosa | Gastro-oesophageal Reflux | Neurogenic Bowel Dysfunction |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Altavilla et al., 2021, Spain, Swimmers [34] | o | o | o | x | o | o | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x |
| Citarella et al., 2021, Italy, Runners [35] | x | +ve f | x | x | x | o | x | x | o | o | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x |
| Kontele et al., 2021, Greece, Gymnasts [51] | x | x | −ve | x | −ve | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x |
| Leao et al., 2023, Portugal, Soccer athletes [52] | x | x | x | x | o | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x |
| Lopez-Jimenz et al., 2023, Spain, Rugby union athletes [53] | x | x | x | x | x | x | x | x | +ve p | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x |
| Manzanio-Carrasco et al., 2020, Spain, Athletes [36] all | x | x | x | x | x | x | x | x | x | x | x | x | +ve | x | o | x | x | x | x | x | o | x | x | o | x | x | x | x | x | x | x | x | x | x | x | x |
| boys | x | x | x | x | o | x | x | x | o | x | x | x | o | x | o | x | x | x | x | x | +ve | x | x | +ve | +ve | +ve | x | x | x | x | x | x | x | x | x | x |
| girls | x | x | x | x | o | x | x | x | o | x | x | x | o | x | o | x | x | x | x | x | o | x | x | o | o | o | x | x | x | x | x | x | x | x | x | x |
| Manzano-Carrasco et al., 2020, Spain Footballers [37] | x | x | x | x | x | x | x | x | x | x | x | x | o | x | x | x | x | x | x | x | o | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x |
| Manzano-Carrasco et al., 2020, Spain, Athletes [38] | ||||||||||||||||||||||||||||||||||||
| boys | x | x | +ve g | x | o | x | x | x | +ve g | x | x | x | +ve | x | o | x | x | x | x | x | +ve | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x |
| girls | x | x | o | x | o | x | x | x | o | x | x | x | o | x | +ve g | x | x | x | x | x | o | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x |
| Marques-Sule et al., 2022, Spain Canoe polo athletes [50] | x | x | x | x | o | x | x | x | o | x | o | o | x | x | o | x | x | x | x | x | o | o | x | x | x | x | x | x | o | x | x | x | x | x | x | x |
| Martinez-Rodriguez et al., 2018, Spain, Sailors [40,41] | x | o | x | x | +ve f | x | x | x | x | o | x | x | x | x | x | x | xx | x | x | x | x | x | x | x | x | x | x | x | x | x | o | x | x | x | x | x |
| Martinez-Rodriguez et al., 2021, Spain, Beach handball athletes [39] | x | x | o | x | +ve | x | x | x | x | x | x | x | x | x | x | −ve | x | o | x | x | o | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x |
| Martinez-Rodriguez et al., 2021, Spain, Beach handball athletes [42] | ||||||||||||||||||||||||||||||||||||
| Junior | x | x | −ve f | o | o | x | x | x | o | x | x | x | x | x | o | x | x | x | x | x | −ve f | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x |
| Senior | x | x | o | o | o | x | x | x | o | x | x | x | x | x | o | x | x | x | x | x | o | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x |
| Martinez-Rodriguez et al., 2022, Spain Beach handball athletes [48] | x | x | −ve | o | −ve | x | x | x | o | x | x | x | x | x | o | o | x | +ve | x | x | o | x | +ve | x | x | x | x | x | x | x | x | x | x | x | x | x |
| Martinovic et al., 2022, Croatia, Professional athletes [57] | x | x | x | x | x | x | x | +ve | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | +ve | x | x | x | x |
| Mayolas-Pi et al., 2017, Spain, Endurance cyclists [43] | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | o | x | x | x |
| Morales-Suarez-Varela et al., 2023 Spain, Basketball athletes [54] | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | −ve | x | x | x | x | x | x |
| Papdopolou et al., 2017, Greece, Cyclists [44] | x | x | x | x | x | x | x | x | x | o | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x |
| Pelaez-Barrios et al., 2022, Spain, Gymnasts [49] | o | x | o | o | o | x | o | x | o | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | −ve | x | x | x | x | x | x | x | x | x |
| Peraita-Costa et al., 2020, Spain, Tennis athletes [45] | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | −ve | x | x | x | x | x | x |
| Romero-Garcia et al., 2022, Spain, Handball athletes [55] | x | x | −ve | −ve | −ve | x | x | x | −ve | x | x | x | o | o | o | o | o | o | o | o | x | x | o | x | x | x | x | x | x | x | x | x | x | x | x | x |
| Santana et al., 2019, Spain, Gymnasts [46] | x | x | +ve | +ve | +ve | x | +ve | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x |
| Santos-Sanchez et al., 2021, Spain, Soccer athletes [47] | x | x | o | o | o | x | x | x | o | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x |
| Toti et al., 2022 Italy, Wheelchair basketball athletes [56] | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | −ve | o | +ve |
| Author, Year, Country, Athletes | MedDiet Adherence | Nutrition Knowledge | Weight | Height | BMI | Waist Circumference | Body Composition | Leg/Arm Circumference | BMR/RMR | Success/Level | 5 km Treadmill Time | Wingate Cycle | Countermovement Jump | Standing Jump | 15″ Test | Bench Test | Squat Jump | Abalakov Jump | Handgrip Strength | Heart Rate | Vo2 Max | 30 s Jump Test | Push-Up Test | Chin-Up Test | Fran Test | Cellular Fatty Acids | Antioxidant Activity | Immune Markers | Eating Behaviours | Body Image | Mood |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Baker et al., 2019, US, Runners [58] | ↑ | x | x | x | x | x | x | x | x | ↑ | ↑ | o | o | x | x | x | x | x | o | o | x | x | x | x | x | x | x | x | x | x | x |
| Caparello et al., 2023, Italy, Volleyball athletes [66] | o | x | x | x | ↑ | x | ↑ | x | ↑ | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x |
| Chilleli et al., 2016, Italy, Cyclists [59] | x | x | o | x | o | x | o | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | mo | mo | x | x | x |
| Ficarra et al., 2022, Italy, Cross-fit athletes [62] | x | x | o | x | o | o | o | ↑ | o | x | x | ↑ | o | ↑ | x | x | x | x | x | x | x | o | ↑ | ↑ | ↑ | x | x | x | x | x | x |
| Malaguti et al., 2008, Italy, Volleyball athletes [60] | x | x | x | x | o | x | o | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | o | o | x | x | x | x |
| Miralles-Amoros et al., 2023, Chile, Handball players [63] | o | x | o | o | o | x | o | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | o | o | o |
| Philippou et al., 2017, Greece, Swimmers [64] | ↑ | ↑ | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x |
| Sahnoune et al., 2020, Algeria, Athletes [65] All | x | x | o | o | o | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x |
| Male | ↑ | x | ↑ | ↑ | ↑ | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x |
| Female | ↑ | x | ↑ | ↑ | o | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x |
| Soldati et al., 2019, Italy [61] Kickboxers | x | x | x | x | x | x | ↑ | x | o | x | x | x | ↑ | o | o | o | ↑ | o | x | x | o | x | x | x | x | x | x | x | x | x | x |
| Runners | x | x | x | x | x | x | ↑ | x | o | x | x | x | ↑ | o | ↑ | o | o | o | x | x | ↑ | x | x | x | x | x | x | x | x | x | x |
| Quality Indicator of MedDiet Intervention | Baker et al., 2019 [58] | Caparello et al., 2023 [66] | Chilelli et al., 2016 [59] | Ficarra et al., 2022 [62] | Malaguti et al., 2008 [60] | Miralles-Amoros et al., 2023 [63] | Philippou et al., 2017 [64] | Sahnoune et al., 2020 [65] | Soldati et al., 2019 [61] |
|---|---|---|---|---|---|---|---|---|---|
| Diet designed and administered by dietitian | N | Y | N | Y | Y | N | Y | Y | Y |
| Minimum amounts specified to participants for identified Mediterranean foods | Y | N | N | N | N | N | N | N | N |
| Prescribed diet meets at least 8 out of 19 defined minimum criteria (Supplementary Table S6) | Y | N | N | N | N | N | N | N | N |
| Diet tolerance reported | N | N | N | N | N | N | N | N | N |
| Frequency and setting for diet instruction reported | Y | N | N | N | N | N | Y | Y | N |
| Diet compliance assessed | Y | N | N | N | N | N | Y | Y | N |
| Perception of diet burden or benefit reported | N | N | N | N | N | N | N | N | N |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mantzioris, E.; Villani, A.; Forsyth, A. The Relationship Between the Mediterranean Dietary Pattern and Exercise and Sport Performance—A Scoping Review. Nutrients 2024, 16, 4259. https://doi.org/10.3390/nu16244259
Mantzioris E, Villani A, Forsyth A. The Relationship Between the Mediterranean Dietary Pattern and Exercise and Sport Performance—A Scoping Review. Nutrients. 2024; 16(24):4259. https://doi.org/10.3390/nu16244259
Chicago/Turabian StyleMantzioris, Evangeline, Anthony Villani, and Adrienne Forsyth. 2024. "The Relationship Between the Mediterranean Dietary Pattern and Exercise and Sport Performance—A Scoping Review" Nutrients 16, no. 24: 4259. https://doi.org/10.3390/nu16244259
APA StyleMantzioris, E., Villani, A., & Forsyth, A. (2024). The Relationship Between the Mediterranean Dietary Pattern and Exercise and Sport Performance—A Scoping Review. Nutrients, 16(24), 4259. https://doi.org/10.3390/nu16244259