


Is There an Ideal Diet? Some Insights from the POUNDS Lost Study


Abstract
1. Introduction
2. The First Highly Popular Diet—The Banting Diet
3. The POUNDS (Preventing Overweight Using Novel Dietary Strategies) Lost Study
3.1. Description of the POUNDS Lost Study
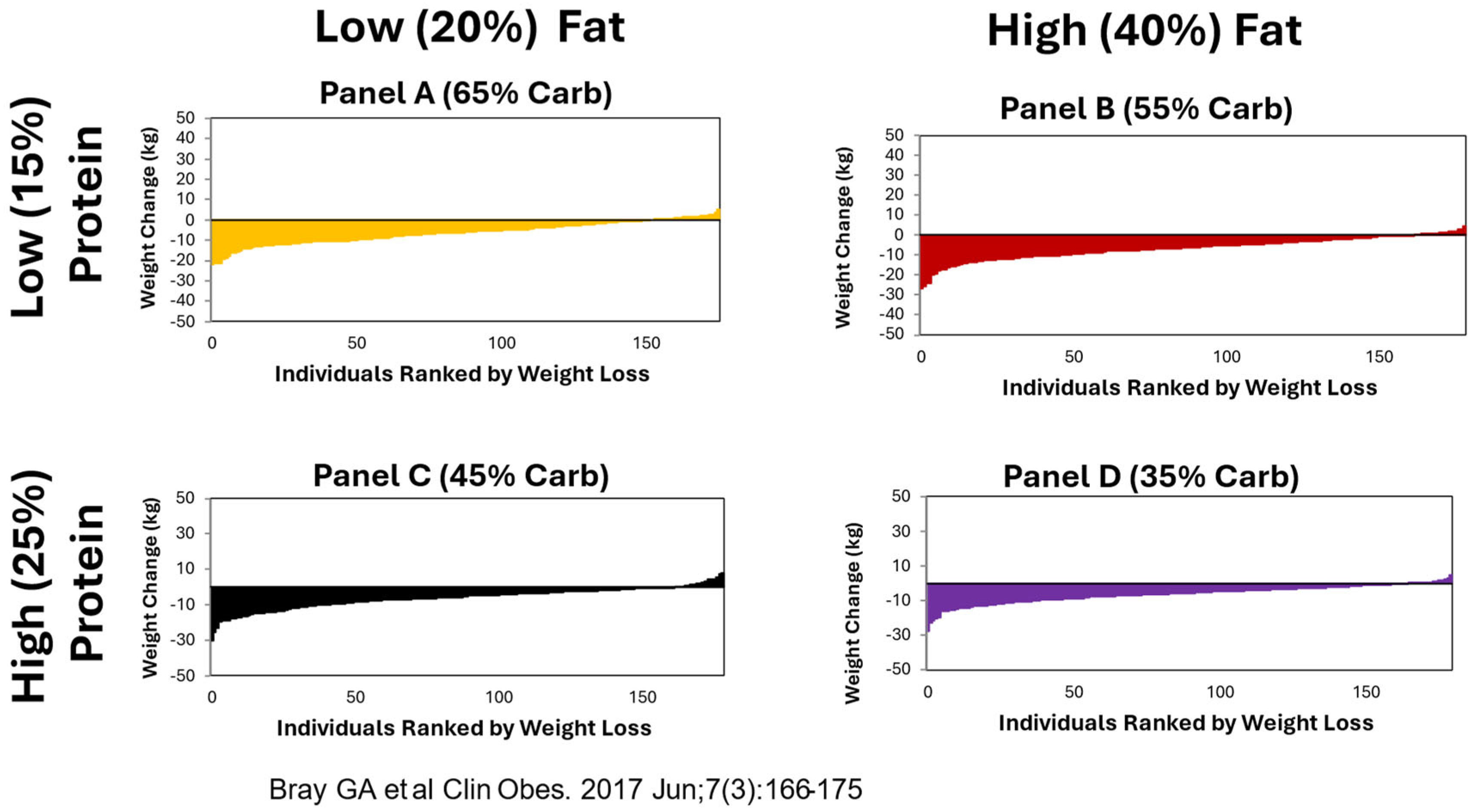
3.2. Variability of Weight Loss
4. Factors Affecting Weight Loss
4.1. Genes Interact with Diet
4.2. Combining Genes in Genetic Risk Scores for Improved Prediction
4.3. Metabolic and Behavioral Changes
4.4. Nutrient-Related Changes Alter Response to Test Diets
5. Discussion
5.1. Expert Opinions
5.2. Comparison of Diets
5.3. Adverse Effects of Some Diets
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Bray, G.A.; Suminska, M. From Hippocrates to the Obesity Society: A Brief History. In Handbook of Obesity; Bray, G.A., Bouchard, C., Katzmarzyk, P., Kirwan, J.P., Redman, L.M., Schauer, P.L., Eds.; Taylor & Francis: Boca Raton, FL, USA, 2024; Volume 2, pp. 3–16. [Google Scholar]
- Hall, K.D.; Farooqi, I.S.; Friedman, J.M.; Klein, S.; Loos, R.J.F.; Mangelsdorf, D.J.; O’Rahilly, S.; Ravussin, E.; Redman, L.M.; Ryan, D.H.; et al. The energy balance model of obesity: Beyond calories in, calories out. Am. J. Clin. Nutr. 2022, 115, 1243–1254. [Google Scholar] [CrossRef]
- Ludwig, D.S.; Aronne, L.J.; Astrup, A.; de Cabo, R.; Cantley, L.C.; Friedman, M.I.; Heymsfield, S.B.; Johnson, J.D.; King, J.C.; Krauss, R.M.; et al. The carbohydrate-insulin model: A physiological perspective on the obesity pandemic. Am. J. Clin. Nutr. 2021, 114, 1873–1885. [Google Scholar] [CrossRef] [PubMed]
- Qi, L.; Heianza, Y.; Li, X.; Sacks, F.M.; Bray, G.A. Toward Precision Weight-Loss Dietary Interventions: Findings from the POUNDS Lost Trial. Nutrients 2023, 15, 3665. [Google Scholar] [CrossRef] [PubMed]
- Banting, W. Letter on Corpulence Addressed to the Public; London, UK, 1863; (Privately printed). [Google Scholar]
- Bray, G.A. Commentary on Banting Letter. Obes. Res. 1993, 1, 148–152. [Google Scholar] [CrossRef] [PubMed]
- Harvey, W. On Corpulence in Relation to Disease: With Some Remarks of Diet; Henry Renshaw: London, UK, 1872. [Google Scholar]
- Harvey, W. De Motu Cordis & Sanguinis in Animalibus, Anatomica Exercitatio. Cum Refutationibus Aemylii Parisani et Jacob Primirosii, 2nd ed.; Joannes Maire: Leyden, The Netherlands, 1639. [Google Scholar]
- Bray, G.A.; Krauss, R.M.; Sacks, F.M.; Qi, L. Lessons Learned from the POUDS Lost Study: Genetic, Metabolic, and Behavioral Factors Affecting Changes in Body Weight, Body Composition, and Cardiometabolic Risk. Curr. Obes. Rep. 2019, 8, 262–283. [Google Scholar] [CrossRef] [PubMed]
- Sacks, F.M.; Bray, G.A.; Carey, V.J.; Smith, S.R.; Ryan, D.H.; Anton, S.D.; Katherine McManus, M.S.; Catherine, M.; Louise, M.; Bishop, M.S.; et al. Comparison of weight-loss diets with different compositions of fat, protein, and carbohydrates. N. Engl. J. Med. 2009, 360, 859–873. [Google Scholar] [CrossRef] [PubMed]
- Bray, G.A.; Ryan, D.H.; Johnson, W.; Champagne, C.M.; Johnson, C.M.; Rood, J.; Williamson, D.A.; Sacks, F.M. Markers of dietary protein intake are associated with successful weight loss in the POUNDS Lost trial. Clin. Obes. 2017, 7, 166–175. [Google Scholar] [CrossRef] [PubMed]
- Qi, Q.; Bray, G.A.; Smith, S.R.; Hu, F.B.; Sacks, F.M.; Qi, L. Insulin receptor substrate 1 (IRS1) gene variation modifies insulin resistance response to weight-loss diets in a two-year randomized trial: The Preventing Obesity by Using Novel Dietary Strategies (POUNDS LOST) Trial. Circulation 2011, 124, 563–571. [Google Scholar] [CrossRef] [PubMed]
- Qi, Q.; Bray, G.A.; Hu, F.B.; Sacks, F.M.; Qi, L. Weight Loss diets modify glucose-dependent insulinotropic polypeptide receptor rs2287019 genotype: Effects on changes in body weight, fasting glucose and insulin resistance: The Preventing Overweight Using Novel Dietary Strategies trial. Am. J. Clin. Nutr. 2012, 95, 506–513. [Google Scholar] [CrossRef]
- Zhang, X.; Qi, Q.; Zhang, C.; Hu, F.B.; Sacks, F.M.; Qi, L. FTO genotype and 2-year change in body composition and fat distribution in response to weight-loss diets: The POUNDS LOST Trial. Diabetes 2012, 61, 3005–3011. [Google Scholar] [CrossRef]
- Xu, M.; Qi, Q.; Liang, J.; Bray, G.A.; Hu, F.B.; Sacks, F.M.; Qi, L. Genetic determinant for amino acid metabolites and changes in body weight and insulin resistance in response to weight-loss diets: The Preventing Overweight Using Novel Dietary Strategies (POUNDS LOST) trial. Circulation 2013, 127, 1283–1289. [Google Scholar] [CrossRef] [PubMed]
- Heianza, Y.; Ma, W.; Huang, T.; Wang, T.; Zheng, Y.; Smith, S.R.; Bray, G.A.; Sacks, F.M.; Qi, L. Macronutrient Intake-Associated FGF21 Genotype Modifies Effects of Weight-Loss Diets on 2-Year Changes of Central Adiposity and Body Composition: The POUNDS Lost Trial. Diabetes Care 2016, 39, 1909–1914. [Google Scholar] [CrossRef] [PubMed]
- Mattei, J.; Qi, Q.; Hu, F.B.; Sacks, F.M.; Qi, L. TCF7L2 genetic variants modulate the effect of dietary fat intake on changes in body composition during a weight-loss intervention. Am. J. Clin. Nutr. 2012, 96, 1129–1136. [Google Scholar] [CrossRef] [PubMed]
- Lin, X.; Qi, Q.; Zheng, Y.; Huang, T.; Lathrop, M.; Zelenika, D.; Bray, G.A.; Sacks, F.M.; Liang, L.; Qi, L. Neuropeptide Y genotype, central obesity, and abdominal fat distribution: The POUNDS LOST trial. Am. J. Clin. Nutr. 2015, 102, 514–519. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Shao, X.; Kou, M.; Wang, X.; Ma, H.; Grundberg, E.; Bazzano, L.A.; Smith, S.R.; Bray, G.A.; Sacks, F.M.; et al. DNA Methylation at ABCG1 and Long-Term Changes in Adiposity and Fat Distribution in Response to Dietary Interventions: The POUNDS Lost Trial. Diabetes Care 2023, 46, 2201–2207. [Google Scholar] [CrossRef] [PubMed]
- Sun, D.; Heianza, Y.; Huang, T.; Ma, W.; Smith, S.R.; Bray, G.A.; Sacks, F.M.; Qi, L. Genetic, epigenetic, and transcriptional variations at NFATC2IP locus with weight loss in response to diet interventions: The POUNDS Lost Trial. Diabetes Obes. Metab. 2018, 20, 2298–2303. [Google Scholar] [CrossRef] [PubMed]
- Huang, T.; Zheng, Y.; Hruby, A.; Williamson, D.A.; Bray, G.A.; Shen, Y.; Sacks, F.M.; Qi, L. Dietary Protein Modifies the Effect of the MC4R Genotype on 2-Year Changes in Appetite and Food Craving: The POUNDS Lost Trial. J. Nutr. 2017, 147, 439–444. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Xue, Q.; Ma, H.; Champagne, C.M.; Bray, G.A.; Sacks, F.M.; Qi, L. Genetically determined gut microbial abundance and 2-year changes in central adiposity and body composition: The POUNDS lost trial. Clin. Nutr. 2022, 41, 2817–2824. [Google Scholar] [CrossRef] [PubMed]
- Heianza, Y.; Zhou, T.; Yuhang, C.; Huang, T.; Willett, W.C.; Hu, F.B.; Bray, G.A.; Sacks, F.M.; Qi, L. Starch Digestion-Related Amylase Genetic Variants, Diet, and Changes in Adiposity: Analyses in Prospective Cohort Studies and a Randomized Dietary Intervention. Diabetes 2020, 69, 1917–1926. [Google Scholar] [CrossRef]
- Li, X.; Zhou, T.; Ma, H.; Heianza, Y.; Champagne, C.M.; Williamson, D.A.; Bray, G.A.; Sacks, F.M.; Qi, L. Genetic variation of lean body mass, changes of appetite, and weight loss in response to diet interventions: The POUNDS Lost trial. Diabetes Obes. Metab. 2020, 22, 2305–2315. [Google Scholar] [CrossRef] [PubMed]
- Liu, G.; Liang, L.; Bray, G.A.; Qi, L.; Hu, F.B.; Rood, J.; Sacks, F.M.; Sun, Q. Thyroid Hormone and Changes in Body Weight and Metabolic Parameters in Response to Weight-Loss Diets: The POUNDS LOST Trial. Int. J. Obes. 2017, 41, 878–886. [Google Scholar] [CrossRef] [PubMed]
- Xue, Q.; Li, X.; Ma, H.; Zhou, T.; Heianza, Y.; Rood, J.C.; Bray, G.A.; Sacks, F.M.; Qi, L. Changes in Pedometer-measured Physical Activity are associated with Weight Loss and Changes in Body Composition and Fat Distribution in Response to Reduced Energy Diet Interventions: The POUNDS Lost trial. Diabetes Obes. Metab. 2022, 24, 1000–1009. [Google Scholar] [CrossRef] [PubMed]
- Vadiveloo, M.; Sacks, F.M.; Champagne, C.M.; Bray, G.A.; Mattei, J. Healthful dietary variety and 2-year changes in weight and adiposity among participants in the POUNDS Lost trial. J. Nutr. 2016, 146, 1552–1559. [Google Scholar] [CrossRef] [PubMed]
- Yao, Q.; de Araujo, C.D.; Juul, F.; Champagne, C.M.; Bray, G.A.; Sacks, F.M.; Vadiveloo, M.K. Isocaloric replacement of Ultra-processed Foods was associated with Greater Weight Loss in POUNDS Lost. Obesity 2024, 32, 1281–1289. [Google Scholar] [CrossRef] [PubMed]
- Li, A.; Li, X.; Zhou, T.; Ma, H.; Heianza, Y.; Williamson, D.A.; Smith, S.R.; Bray, G.A.; Sacks, F.M.; Qi, L. Sleep Disturbance, Changes in Energy Intake and Body Composition During during Weight Loss in the POUNDS Lost trial. Diabetes 2022, 71, 934–944. [Google Scholar] [CrossRef] [PubMed]
- Miketinas, D.C.; Bray, G.A.; Beyl, R.A.; Ryan, D.H.; Sacks, F.M.; Champagne, C.M. Fiber Intake Predicts Weight Loss and Dietary Adherence in Adults Consuming Calorie-Restricted Diets: The POUNDS Lost Study. J. Nutr. 2019, 149, 1742–1748. [Google Scholar] [CrossRef] [PubMed]
- Anton, S.D.; LeBlanc, H.R.; Karabetian, A.C.; Sacks, F.; Bray, G.; Williamson, D.A. Use of a Computerized Tracking System to Monitor and Provide Feedback on Dietary Goals for Calorie Restricted Diets: The POUNDS LOST Study. J. Diabetes Sci. Technol. 2012, 6, 1216–1225. [Google Scholar] [CrossRef] [PubMed]
- Williamson, D.A.; Anton, S.D.; Han, H.; Champagne, C.M.; Allen, R.; Leblanc, E.; Ryan, D.H.; McManus, K.; Laranjo, N.; Carey, V.J.; et al. Adherence is a multi-dimensional construct in the POUNDS LOST trial. J. Behav. Med. 2010, 33, 35–45. [Google Scholar] [CrossRef] [PubMed]
- Williamson, D.A.; Anton, S.D.; Han, H.; Champagne, C.M.; Allen, R.; LeBlanc, E.; Ryan, D.H.; Rood, J.; McManus, K.; Laranjo, N.; et al. Early behavioral adherence predicts short and long-term weight loss in the POUNDS LOST study. J. Behav. Med. 2010, 33, 305–314. [Google Scholar] [CrossRef]
- Thomas, D.M.; Ivanescu, A.E.; Martin, C.K.; Heymsfield, S.B.; Marshall, K.; Bodrato, V.E.; Williamson, D.A.; Anton, S.D.; Sacks, F.M.; Ryan, D.; et al. Predicting successful long-term weight loss from short-term weight-loss outcomes: New insights from a dynamic energy balance model (the POUNDS Lost study). Am. J. Clin. Nutr. 2015, 101, 449–454. [Google Scholar] [CrossRef] [PubMed]
- Hjorth, M.F.; Astrup, A.; Zohar, Y.; Urban, L.E.; Sayer, R.D.; Patterson, B.W.; Herring, S.J.; Klein, S.; Zemel, B.S.; Foster, G.D.; et al. Personalized nutrition: Pretreatment glucose metabolism determines individual long-term weight loss responsiveness in individuals with obesity on low-carbohydrate versus low-fat diet. Int. J. Obes. 2019, 43, 2037–2044. [Google Scholar] [CrossRef] [PubMed]
- Hjorth, M.F.; Zohar, Y.; Hill, J.O.; Astrup, A. Personalized Dietary Management of Overweight and Obesity Based on Measures of Insulin and Glucose. Annu. Rev. Nutr. 2018, 38, 245–272. [Google Scholar] [CrossRef] [PubMed]
- Hjorth, M.F.; Bray, G.A.; Zohar, Y.; Urban, L.; Miketinas, D.C.; Williamson, D.A.; Ryan, D.H.; Rood, J.; Champagne, C.M.; Sacks, F.M.; et al. Pretreatment Fasting Glucose and Insulin as Determinants of Weight Loss on Diets Varying in Macronutrients and Dietary Fibers-The POUNDS LOST Study. Nutrients 2019, 11, 586. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Hanseman, D.J.; Champagne, C.M.; Bray, G.A.; Qi, L.; Williamson, D.A.; Anton, S.D.; Sacks, F.M.; Tong, J. Predicting Weight Loss Using Psychological and Behavioral Factors: The POUNDS LOST Trial. J. Clin. Endocrinol. Metab. 2020, 105, 1274–1283. [Google Scholar] [CrossRef] [PubMed]
- Anton, S.D.; Gallager, J.; Carey, V.; Laranjo, N.; Cheng, J.; Champagne, C.M.; Ryan, D.H.; McManus, K.; Loria, C.M.; Bray, G.A.; et al. Diet Type and Changes in Food Cravings following Weight Loss: Findings from the POUNDS LOST Trial. Eat. Weight Disord. 2012, 17, e101-8. [Google Scholar] [CrossRef] [PubMed]
- Apolzan, J.; Myers, C.; Champagne, C.; Beyl, R.; Raynor, H.; Anton, S.; Williamson, D.A.; Sacks, F.M.; Bray, G.A.; Martin, C.K. Frequency of consuming foods predicts changes in cravings for those foods during weight loss: The POUNDS Lost Study. Obesity 2017, 25, 1343–1348. [Google Scholar] [CrossRef] [PubMed]
- Chao, A.M.; Quigley, K.M.; Wadden, T.A. Dietary interventions for obesity: Clinical and mechanistic findings. J. Clin. Investig. 2021, 131, e140065. [Google Scholar] [CrossRef] [PubMed]
- Bray, G.A.; Ryan, D.H. Evidence-Based Weight Loss Interventions: Individualized Treatment Options to Maximize Patient Outcomes. Diabetes Obes. Metab. 2021, 23 (Suppl. S1), 50–62. [Google Scholar] [CrossRef] [PubMed]
- US News and World Report Suppl 1:50-62. US News and World Report 2023. Available online: https://health.usnews.com/best-diet/best-diets-overall (accessed on 30 May 2024).
- Appel, L.J.; Moore, T.J.; Obarzanek, E.; Vollmer, W.; Svetkey, L.P.; Sacks, R.; Bray, G.A.; Vogt, T.M.; Cutler, J.A.; Windhauser, M.M.; et al. A clinical trail of the effects of dietary patterns on blood pressure. N. Engl. J. Med. 1997, 338, 1117–1124. [Google Scholar] [CrossRef] [PubMed]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.I.; Corella, D.; Arós, F.; PREDIMED Study Investigators. Primary Prevention of Cardiovascular Disease with a Mediterranean Diet Supplemented with Extra-Virgin Olive Oil or Nuts. N. Engl. J. Med. 2018, 378, e34. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, H. Never Satisfied: A Cultural History of Diets, Fantasies and Fat; The Free Press: New York, NY, USA, 1986. [Google Scholar]
- Foxcroft, L. Calories and Corsets: A History of Dieting over 2000 Years; Profile Books: London, UK, 2011. [Google Scholar]
- Gilman, S.L. Obesity: The Biography; Oxford University Press: Oxford, UK, 2010. [Google Scholar]
- Atkins, R. Dr Akins Diet Revolution. The High Calorie Way to Stay Thin Forever; David McKay: New York, NY, USA, 1972. [Google Scholar]
- Linn, R.; Stuart, S.L. The Last Chance Diet: A Revolutionary New Approach to Weight Loss; Lyle Stuart Inc.: Secaucus, NJ, USA, 1976. [Google Scholar]
- Sours, H.E.; Frattalli, V.P.; Brand, C.D.; Feldman, R.A.; Forbes, A.L.; Swanson, R.C.; Paris, A.L. Sudden death associated with very low calorie weight regimes. Am. J. Clin. Nutr. 1981, 34, 453–461. [Google Scholar] [CrossRef]

{kind=link}
| Components of Intake | Average | % as Calories |
|---|---|---|
| Energy Intake | 1714 kcal/d | |
| Protein intake | 115 g/d | 27% |
| Fat Intake | 42 g/d | 22% |
| Carbohydrate Intake | 119 g/d | 28% |
| Alcohol | 56 g/d | 23% |
| Gane Name | Genotype or Phenotype | Diet with Most Weight or Fat Loss | Ref # |
|---|---|---|---|
| Insulin receptor substrate-1 gene (IRS1) | CC genotype (rs2943641) TC and TT | Highest carbohydrate diet at 6 months lowered weight, insulin, and insulin Res (HOMA-IR) at 6 months Lowest carbohydrate diet at 6 months lowered insulin and HOMA-IR but not weight | [12] |
| Glucose-dependent insulinotropic polypeptide receptor (GIPR) | T allele (rs2287019) Changes in glucose, insulin and HOMA-IR paralleled weight changes | Low-fat diet: TT lost 8 kg; CT lost 6 kg; CC lost 4.5 kg High-fat diet: TT lost 5.5 kg; CT lost 5.8 kg and CC lost 5.9 kg | [13] |
| Fat Mass and Obesity-Associated Gene (FTO) | A allele (rs1558902) T allele | High-protein diet associated greater with loss; Low-protein diet associated with loss of fat free mass (FFM); greater loss of TAT, VAT and SAT | [14] |
| Protein phosphatase 1K mitochondrial (PPM1K) | T allele (rs1440581) | High-fat diet: TT allele lost 8 kg at 12 mos; the CT allele 6 kg and the CC allele 4+ kg | [15] |
| Fibroblast Growth Factor-21 (FGF21) | Graded response across genotypes (rs838147): C Allele T alleles | High-carbohydrate diet: C allele lost most body fat; Low-carbohydrate diet: T Allele lost most body fat | [16] |
| Transcription factor 7-like 2 (TCF7L2) | TT (rs12255372) | Low-fat diet: TT genotype had more weight and fat loss than other genotypes | [17] |
| Neuropeptide Y (NPY) | C allele (rs16147) T allele | High-fat diet: greater fat loss with C allele Low-fat diet: greater fat change with T allele | [18] |
| Baseline DNA methylation at ABCG1 (ATP-binding cassette sub-family G member 1) | Average-protein diet had significant reductions in body weight, waist circumference, TAT, VAT, SAT and dSAT at 6 months and 2 years High-protein diet did not have these effects | [19] | |
| Nuclear Factor of Activated T Cells 2 Interacting Protein (NFAT2CIP) | NFAT2CIP (rs11150675) A allele Transcriptional variations (ILMN_1725441) cis-DNA methylation at (cg26663590) | Low-fat diet: non-A allele lost more wt; lower baseline for transcriptional variant ILMN lost more weight High-fat diet: no effect of A allele on wt; higher baseline ILMN resulted in more wt loss | [20] |
| Melanocortin-4-receptor-4 (MC4R) | MC4R (rs7227255) A allele | High-protein diet: obesity-predisposing A-allele had a greater increase in appetite score and craving at 2 years than non-A allele. No interaction with fat diets | [21] |
| GRS for the relative abundance of gut microbial taxa | 20 SNPs | Average-protein diet reduced 6 mo fat mass High-protein diet: no effect | [22] |
| GRS for amylase 1 (AMY1) | 9 SNPs | 35% carbohydrate diet reduced weight and waist circumference 65% carbohydrate diet increased weight and waist circumference | [23] |
| GRS for low body mass index—(lower GRS associated with more LBM) | 5 SNPs | Low-fat diet: lower GRS for LBM resulted in a greater decrease in body weight, waist circumference, and in appetite, hunger, fullness, and prospective fullness High-fat diet: no interaction of GRS | [24] |
| Variable | Time | Tertiles 1 | Comment | Ref # | |||||
|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | |||||||
| Free-Triiodothyronine | 6 mos | 3.9 kg | 4.6 kg | 5.4 kg | Similar response for free-thyroxine; data from Model 1 | [25] | |||
| Physical Activity | 6 Mos | 6.2 kg | 7.0 kg | 9.5 kg | Measured by pedometer | [26] | |||
| Healthy Dietary Variety | 6 mos | 6.6 kg | 6.3 kg | 8.2 kg | US Healthy Food Diversity index; change at 6 mos 1 = reduced; 2 = stable; 3 = increased variety | [27] | |||
| Ultra-Professed Food | 5.3 kg | 7.5 kg | 8.3 kg | Nova 1 and 2 foods | [28] | ||||
| Quartiles | |||||||||
| 1 | 2 | 3 | 4 | ||||||
| Sleep Quality | 6 mos | 6.0 kg | 4.8 kg | 4.8 kg | 2.0 kg | Degree of sleep disturbance: 1 = no disturbance; 2 = slight; 3 = moderate; 4 = severe | [29] | ||
| Protein | 24 mos | 2.6 | 5 kg | 7.1 kg | 7.5 kg | Measured as nitrogen excretion/g creatinine; quartiles of response | [11] | ||
| Fiber | 6 mos | 5.8 kg | 5.8 kg | 7 kg | 10.3 kg | [30] | |||
| Higher Scored Diets | Score | Lower Scored Diets | Score |
|---|---|---|---|
| Mediterranean Diet | 4.6 | Zone | 2.8 |
| DASH Diet | 4.4 | Nutritarian | 2.7 |
| The Flexitarian Diet | 4.4 | Jenny Craig | 2.5 |
| MIND Diet | 4.3 | Nutrisystem | 2.5 |
| TLC Diet | 4.1 | South Beach Diet | 2.5 |
| Mayo Clinic Diet | 4.0 | Keyto Diet | 2.5 |
| Volumetrics Diet | 4.0 | Paleo Diet | 2.3 |
| Weight Watchers Diet | 3.8 | Keto Diet | 1.9 |
| Dr Weil’s Ant-inflammatory | 3.7 | Atkins Diet | 1.8 |
| Ornish Diet | 3.6 | Optavia Diet | 1.8 |
| Noom Diet | 3.5 | SlimFast Diet | 1.8 |
| Pritikin Diet | 3.5 | Raw Food Diet | 1.7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bray, G.A.; Qi, L.; Sacks, F.M. Is There an Ideal Diet? Some Insights from the POUNDS Lost Study. Nutrients 2024, 16, 2358. https://doi.org/10.3390/nu16142358
Bray GA, Qi L, Sacks FM. Is There an Ideal Diet? Some Insights from the POUNDS Lost Study. Nutrients. 2024; 16(14):2358. https://doi.org/10.3390/nu16142358
Chicago/Turabian StyleBray, George A., Lu Qi, and Frank M. Sacks. 2024. "Is There an Ideal Diet? Some Insights from the POUNDS Lost Study" Nutrients 16, no. 14: 2358. https://doi.org/10.3390/nu16142358
APA StyleBray, G. A., Qi, L., & Sacks, F. M. (2024). Is There an Ideal Diet? Some Insights from the POUNDS Lost Study. Nutrients, 16(14), 2358. https://doi.org/10.3390/nu16142358