
Reduced Taurine Serum Levels in Inflammatory Bowel Disease
 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population and Data Collection
2.2. Enzyme-Linked Immunosorbent Assay
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics
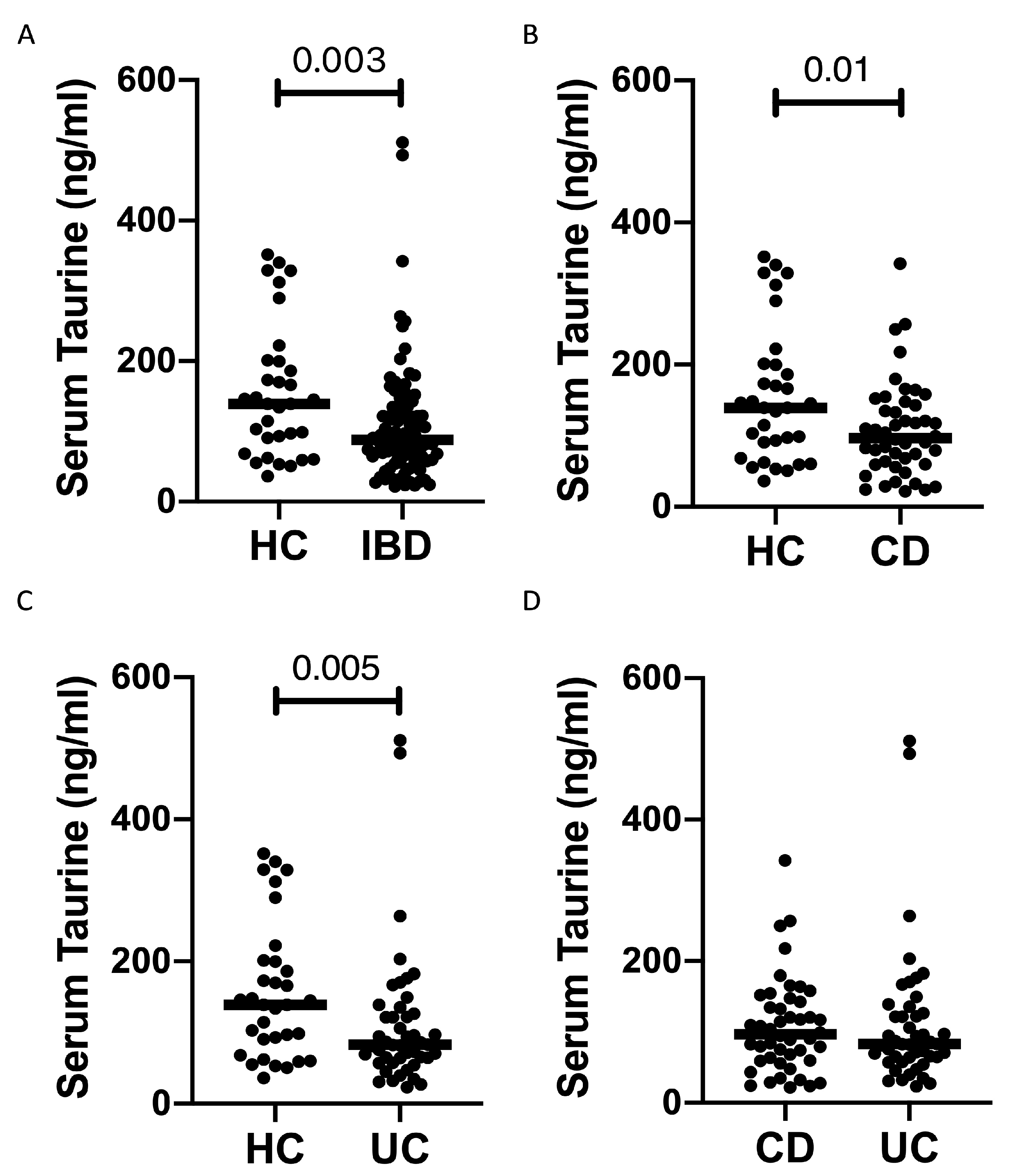
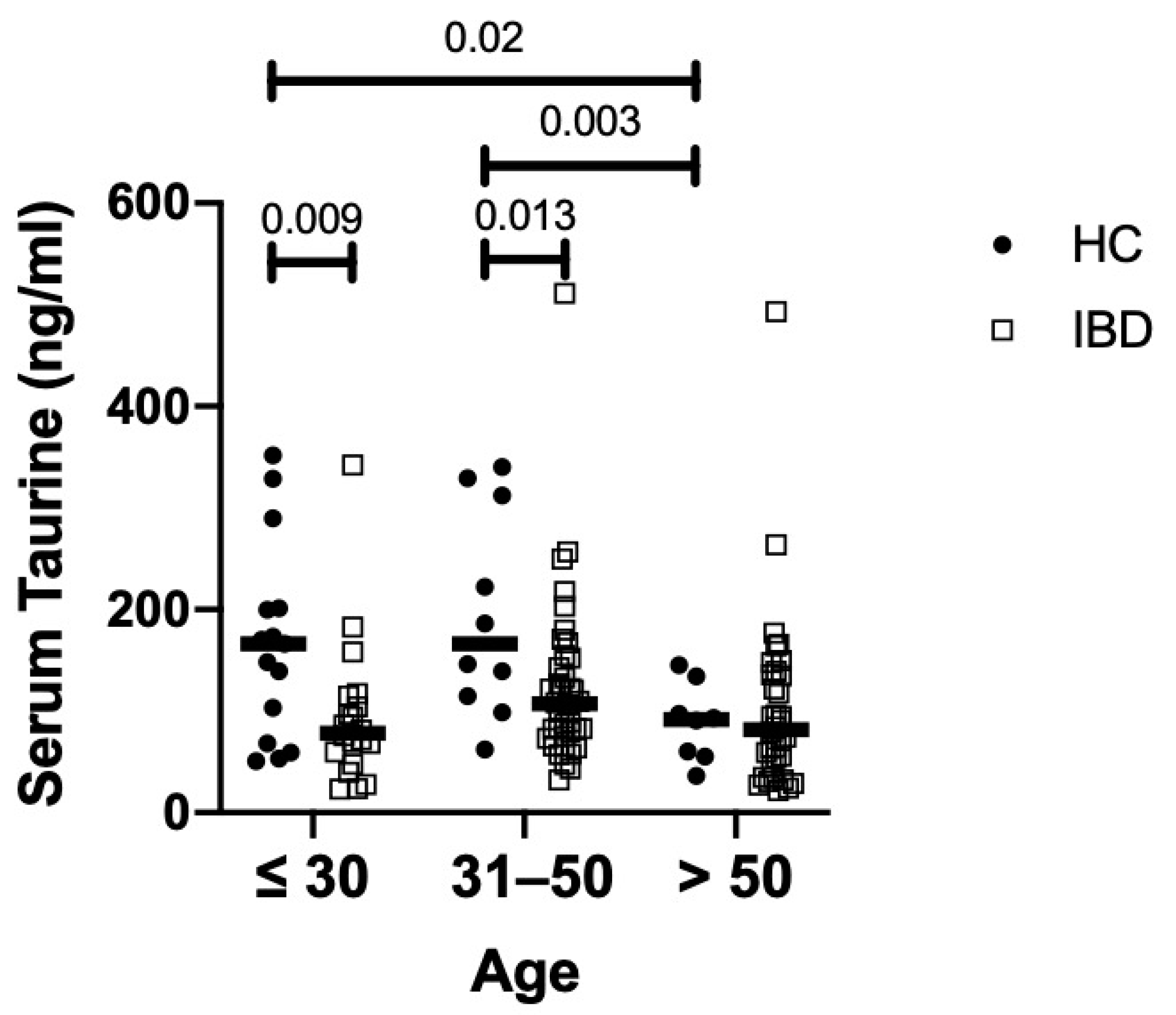
3.2. Serum Taurine Levels Are Reduced in IBD
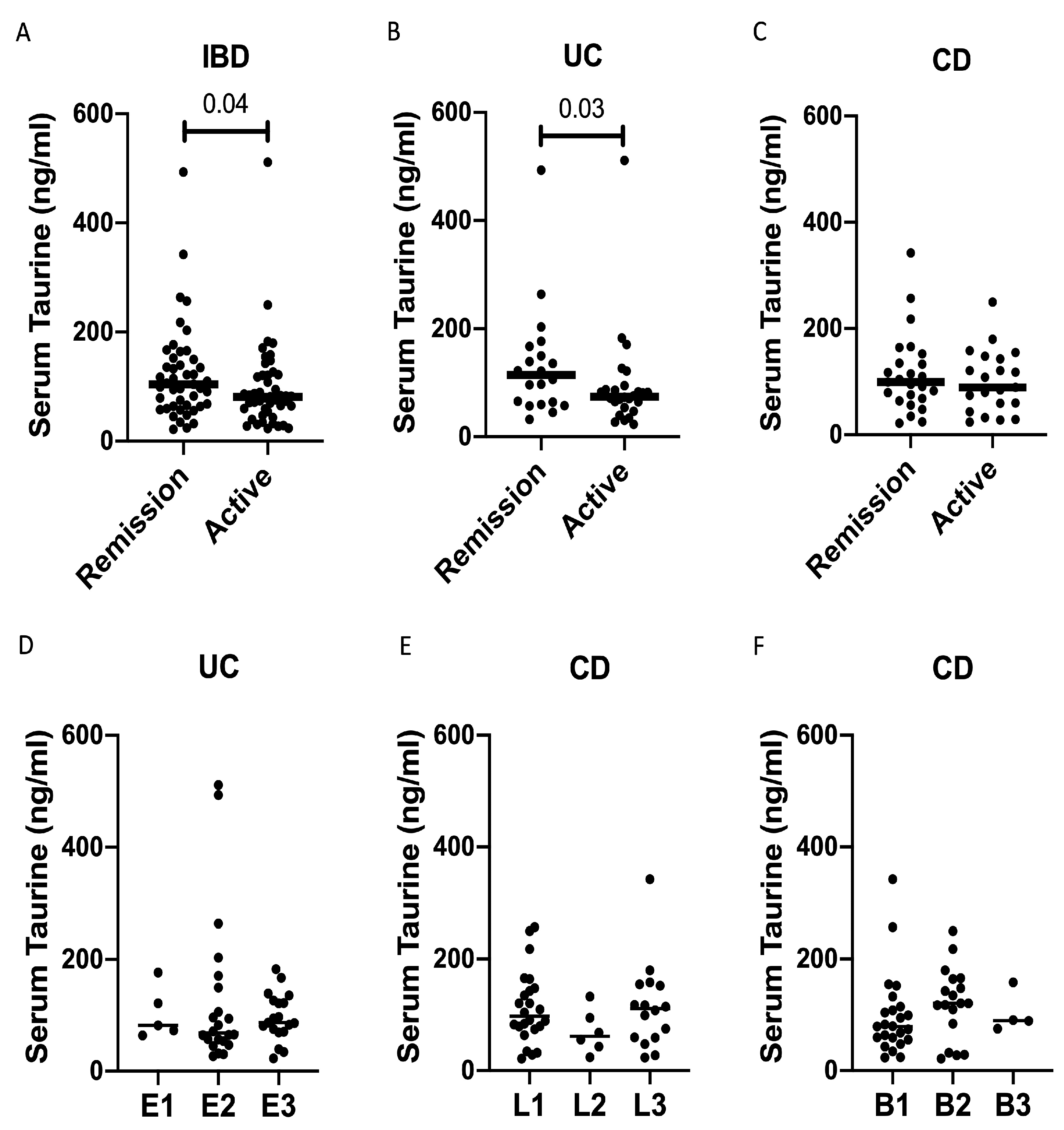
3.3. Serum Levels of Taurine Are Diminished in IBD Patients with Clinically Active Disease
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lambert, I.H.; Kristensen, D.M.; Holm, J.B.; Mortensen, O.H. Physiological Role of Taurine—From Organism to Organelle. Acta Physiol. 2015, 213, 191–212. [Google Scholar] [CrossRef]
- Caine, J.J.; Geracioti, T.D. Taurine, Energy Drinks, and Neuroendocrine Effects. CCJM 2016, 83, 895–904. [Google Scholar] [CrossRef]
- García-Ayuso, D.; Di Pierdomenico, J.; Martínez-Vacas, A.; Vidal-Sanz, M.; Picaud, S.; Villegas-Pérez, M.P. Taurine: A Promising Nutraceutic in the Prevention of Retinal Degeneration. Neural Regen. Res. 2024, 19, 606–610. [Google Scholar] [CrossRef]
- Schuller-Levis, G.B.; Park, E. Taurine and Its Chloramine: Modulators of Immunity. Neurochem. Res. 2004, 29, 117–126. [Google Scholar] [CrossRef]
- Schuller-Levis, G.B.; Park, E. Taurine: New Implications for an Old Amino Acid. FEMS Microbiol. Lett. 2003, 226, 195–202. [Google Scholar] [CrossRef]
- Faghfouri, A.H.; Seyyed Shoura, S.M.; Fathollahi, P.; Shadbad, M.A.; Papi, S.; Ostadrahimi, A.; Faghfuri, E. Profiling Inflammatory and Oxidative Stress Biomarkers Following Taurine Supplementation: A Systematic Review and Dose-Response Meta-Analysis of Controlled Trials. Eur. J. Clin. Nutr. 2022, 76, 647–658. [Google Scholar] [CrossRef]
- Marcinkiewicz, J.; Kontny, E. Taurine and Inflammatory Diseases. Amino Acids 2014, 46, 7–20. [Google Scholar] [CrossRef]
- Bartlett, D.J.; Ramos, G.P.; Fletcher, J.G.; Bruining, D.H. Imaging Evaluation of Inflammatory Bowel Disease Complications. Gastrointest. Endosc. Clin. N. Am. 2022, 32, 651–673. [Google Scholar] [CrossRef]
- MacDonald, T.T.; Monteleone, G. Immunity, Inflammation, and Allergy in the Gut. Science 2005, 307, 1920–1925. [Google Scholar] [CrossRef]
- Windsor, J.W.; Kaplan, G.G. Evolving Epidemiology of IBD. Curr. Gastroenterol. Rep. 2019, 21, 40. [Google Scholar] [CrossRef]
- Laudisi, F.; Di Fusco, D.; Dinallo, V.; Stolfi, C.; Di Grazia, A.; Marafini, I.; Colantoni, A.; Ortenzi, A.; Alteri, C.; Guerrieri, F.; et al. The Food Additive Maltodextrin Promotes Endoplasmic Reticulum Stress–Driven Mucus Depletion and Exacerbates Intestinal Inflammation. Cell. Mol. Gastroenterol. Hepatol. 2019, 7, 457–473. [Google Scholar] [CrossRef]
- Laudisi, F.; Stolfi, C.; Monteleone, G. Impact of Food Additives on Gut Homeostasis. Nutrients 2019, 11, 2334. [Google Scholar] [CrossRef]
- Ferenc, K.; Jarmakiewicz-Czaja, S.; Filip, R. Components of the Fiber Diet in the Prevention and Treatment of IBD—An Update. Nutrients 2022, 15, 162. [Google Scholar] [CrossRef]
- Zhao, Z.; Satsu, H.; Fujisawa, M.; Hori, M.; Ishimoto, Y.; Totsuka, M.; Nambu, A.; Kakuta, S.; Ozaki, H.; Shimizu, M. Attenuation by Dietary Taurine of Dextran Sulfate Sodium-Induced Colitis in Mice and of THP-1-Induced Damage to Intestinal Caco-2 Cell Monolayers. Amino Acids 2008, 35, 217–224. [Google Scholar] [CrossRef]
- Singh, P.; Gollapalli, K.; Mangiola, S.; Schranner, D.; Yusuf, M.A.; Chamoli, M.; Shi, S.L.; Lopes Bastos, B.; Nair, T.; Riermeier, A.; et al. Taurine Deficiency as a Driver of Aging. Science 2023, 380, eabn9257. [Google Scholar] [CrossRef]
- Qaradakhi, T.; Gadanec, L.K.; McSweeney, K.R.; Abraham, J.R.; Apostolopoulos, V.; Zulli, A. The Anti-Inflammatory Effect of Taurine on Cardiovascular Disease. Nutrients 2020, 12, 2847. [Google Scholar] [CrossRef]
- McGaunn, J.; Baur, J.A. Taurine Linked with Healthy Aging. Science 2023, 380, 1010–1011. [Google Scholar] [CrossRef]
- Zhang, L.; Yuan, Y.; Tong, Q.; Jiang, S.; Xu, Q.; Ding, J.; Zhang, L.; Zhang, R.; Zhang, K. Reduced Plasma Taurine Level in Parkinson’s Disease: Association with Motor Severity and Levodopa Treatment. Int. J. Neurosci. 2015, 126, 630–636. [Google Scholar] [CrossRef]
- Chesney, R.W.; Han, X.; Patters, A.B. Taurine and the Renal System. J. Biomed. Sci. 2010, 17, S4. [Google Scholar] [CrossRef]
- Mkrtchyan, G.V.; Abdelmohsen, K.; Andreux, P.; Bagdonaite, I.; Barzilai, N.; Brunak, S.; Cabreiro, F.; De Cabo, R.; Campisi, J.; Cuervo, A.M.; et al. ARDD 2020: From Aging Mechanisms to Interventions. Aging 2020, 12, 24484–24503. [Google Scholar] [CrossRef]
- Cellier, C.; Sahmoud, T.; Froguel, E.; Adenis, A.; Belaiche, J.; Bretagne, J.F.; Florent, C.; Bouvry, M.; Mary, J.Y.; Modigliani, R. Correlations between Clinical Activity, Endoscopic Severity, and Biological Parameters in Colonic or Ileocolonic Crohn’s Disease. A Prospective Multicentre Study of 121 Cases. The Groupe d’Etudes Therapeutiques Des Affections Inflammatoires Digestives. Gut 1994, 35, 231–235. [Google Scholar] [CrossRef]
- Rizzello, F.; Saracino, I.M.; Gionchetti, P.; Valerii, M.C.; Ricci, C.; Imbesi, V.; Filippone, E.; Bellocchio, I.; Dussias, N.K.; Dervieux, T.; et al. Nutritional Biomarkers for the Prediction of Response to Anti-TNF-α Therapy in Crohn’s Disease: New Tools for New Approaches. Nutrients 2024, 16, 280. [Google Scholar] [CrossRef]
- Zhou, G.; Liu, H.; Wei, P.; He, Q.; Zhang, J.; Shi, Q.; Liu, T.; Liu, S. Amino Acids-Targeted Metabolomics Reveals Novel Diagnostic Biomarkers for Ulcerative Colitis and Crohn’s Disease. Amino Acids 2023, 55, 349–358. [Google Scholar] [CrossRef]
- Pietzner, M.; Stewart, I.D.; Raffler, J.; Khaw, K.-T.; Michelotti, G.A.; Kastenmüller, G.; Wareham, N.J.; Langenberg, C. Plasma Metabolites to Profile Pathways in Noncommunicable Disease Multimorbidity. Nat. Med. 2021, 27, 471–479. [Google Scholar] [CrossRef]
- Sharma, S.; Sahoo, B.M.; Banik, B.K. Biological Effects and Mechanisms of Taurine in Various Therapeutics. CDDT 2023, 20, e250523217306. [Google Scholar] [CrossRef]
- Shimizu, M.; Zhao, Z.; Ishimoto, Y.; Satsu, H. Dietary Taurine Attenuates Dextran Sulfate Sodium (DSS)-Induced Experimental Colitis in Mice. In Taurine 7; Azuma, J., Schaffer, S.W., Ito, T., Eds.; Advances in Experimental Medicine and Biology; Springer: New York, NY, USA, 2009; Volume 643, pp. 265–271. ISBN 978-0-387-75680-6. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | UC Patients (n = 46) | CD Patients (n = 46) | p-Value |
|---|---|---|---|
| Age (years), median (range) | 46 (20–69) | 46 (19–76) | 0.832 |
| Female gender, n (%) | 25 (54.3) | 18 (39.1) | 0.210 |
| Weekly seafood consumption, n (%): 0 1 >1 | 30 (88.2) 4 (11.8) 0 (0) | 25 (86.2) 4 (13.8) 0 (0) | - |
| Weekly dark meat poultry consumption, n (%): 0 1 >1 | 15 (44.1) 13 (38.2) 6 (17.6) | 11 (37.9) 12 (41.4) 6 (20.7) | - |
| Weekly taurine-containing energy drinks, n (%): 0 1 >1 | 33 (97) 1 (3) 0 (0) | 28 (96.5) 1 (3.5) 0 (0) | - |
| IBD patients with clinically active disease, n (%) | 26 (56.5) | 21 (45.7) | 0.400 |
| Therapy with mesalamine, n (%) | 29 (63) | 15 (32.6) | 0.007 |
| Therapy with steroids, n (%) | 4 (8.7) | 8 (17.4) | 0.353 |
| Therapy with biologic agents, n (%) | 8 (17.4) | 19 (41.3) | 0.022 |
| Therapy with immunosuppressants, n (%) | 0 (0) | 5 (10.9) | - |
| UC localization, n (%): E1 E2 E3 | 5 (10.9) 22 (47.8) 19 (41.3) | - | - |
| CD localization, n (%): L1 L2 L3 | - | 24 (52.2) 6 (13) 16 (34.8) | - |
| CD phenotype, n (%): B1 B2 B3 | - | 24 (52.2) 18 (39.1) 4 (8.7) | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Frascatani, R.; Mattogno, A.; Iannucci, A.; Marafini, I.; Monteleone, G. Reduced Taurine Serum Levels in Inflammatory Bowel Disease. Nutrients 2024, 16, 1593. https://doi.org/10.3390/nu16111593
Frascatani R, Mattogno A, Iannucci A, Marafini I, Monteleone G. Reduced Taurine Serum Levels in Inflammatory Bowel Disease. Nutrients. 2024; 16(11):1593. https://doi.org/10.3390/nu16111593
Chicago/Turabian StyleFrascatani, Rachele, Adelaide Mattogno, Andrea Iannucci, Irene Marafini, and Giovanni Monteleone. 2024. "Reduced Taurine Serum Levels in Inflammatory Bowel Disease" Nutrients 16, no. 11: 1593. https://doi.org/10.3390/nu16111593
APA StyleFrascatani, R., Mattogno, A., Iannucci, A., Marafini, I., & Monteleone, G. (2024). Reduced Taurine Serum Levels in Inflammatory Bowel Disease. Nutrients, 16(11), 1593. https://doi.org/10.3390/nu16111593