
Serum Albumin and Post-Stroke Outcomes: Analysis of UK Regional Registry Data, Systematic Review, and Meta-Analysis

 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Primary Data Analysis
Study Design and Data Source
2.2. Data Extraction and Exposures
2.3. Outcomes
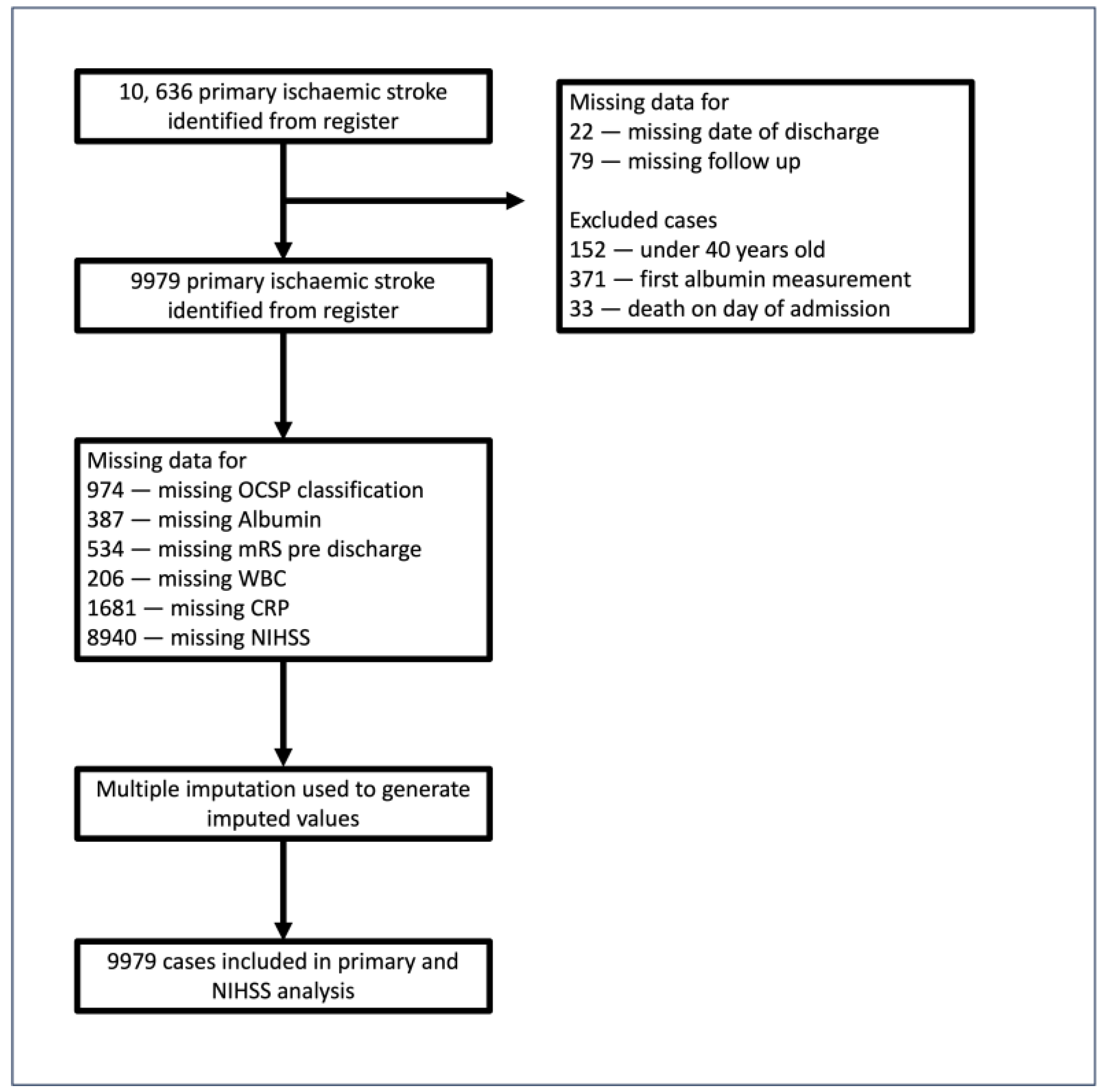
2.4. Missing Data and Exclusions
2.5. Statistical Analyses
2.6. Clinical Outcomes
2.7. Systematic Review and Meta-Analysis
3. Results
3.1. Database Study
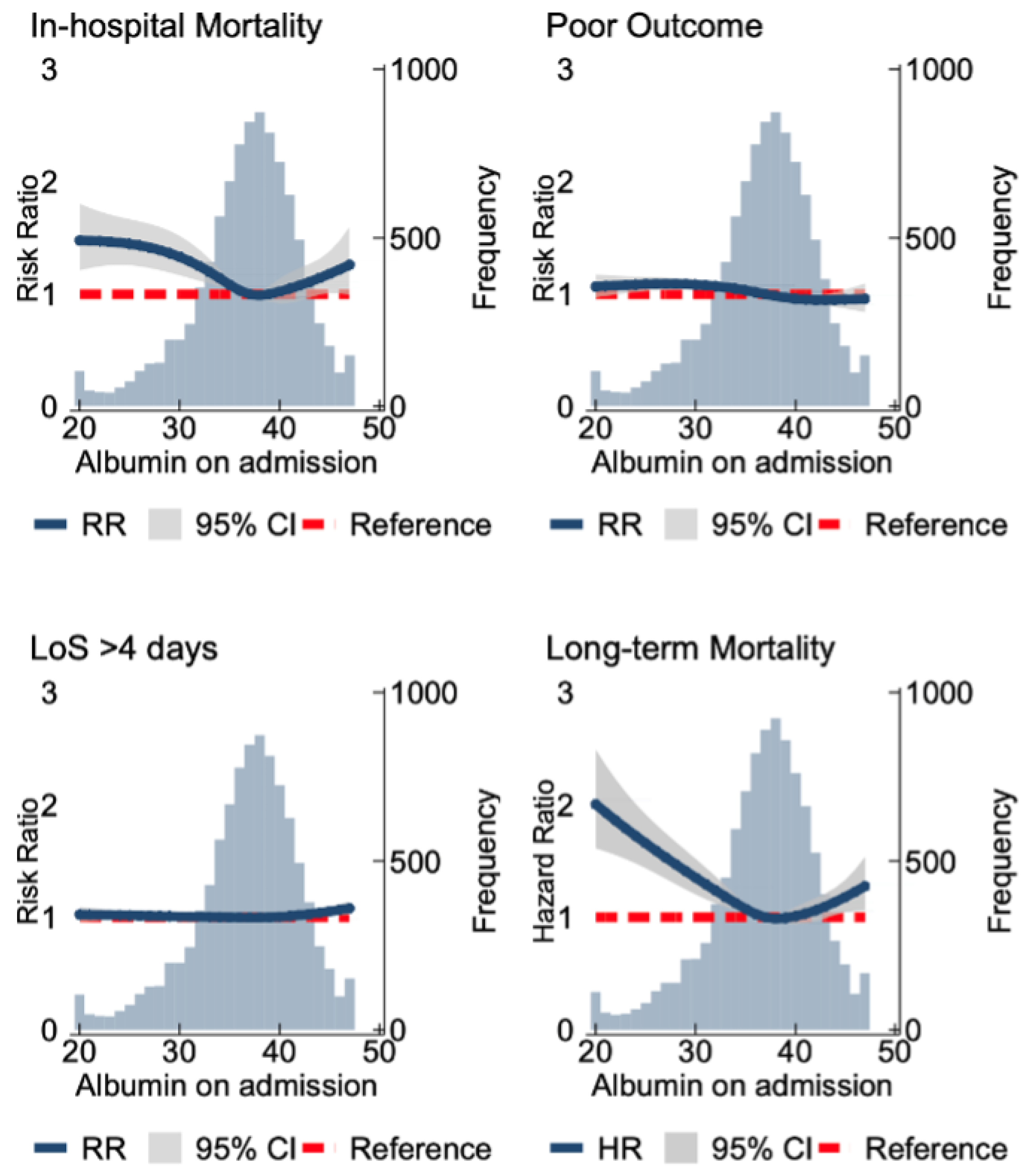
3.2. Clinical Outcomes
Albumin as a Continuous Variable
3.3. Albumin Quartiles
3.4. Systematic Review and Meta-Analysis
Search Results
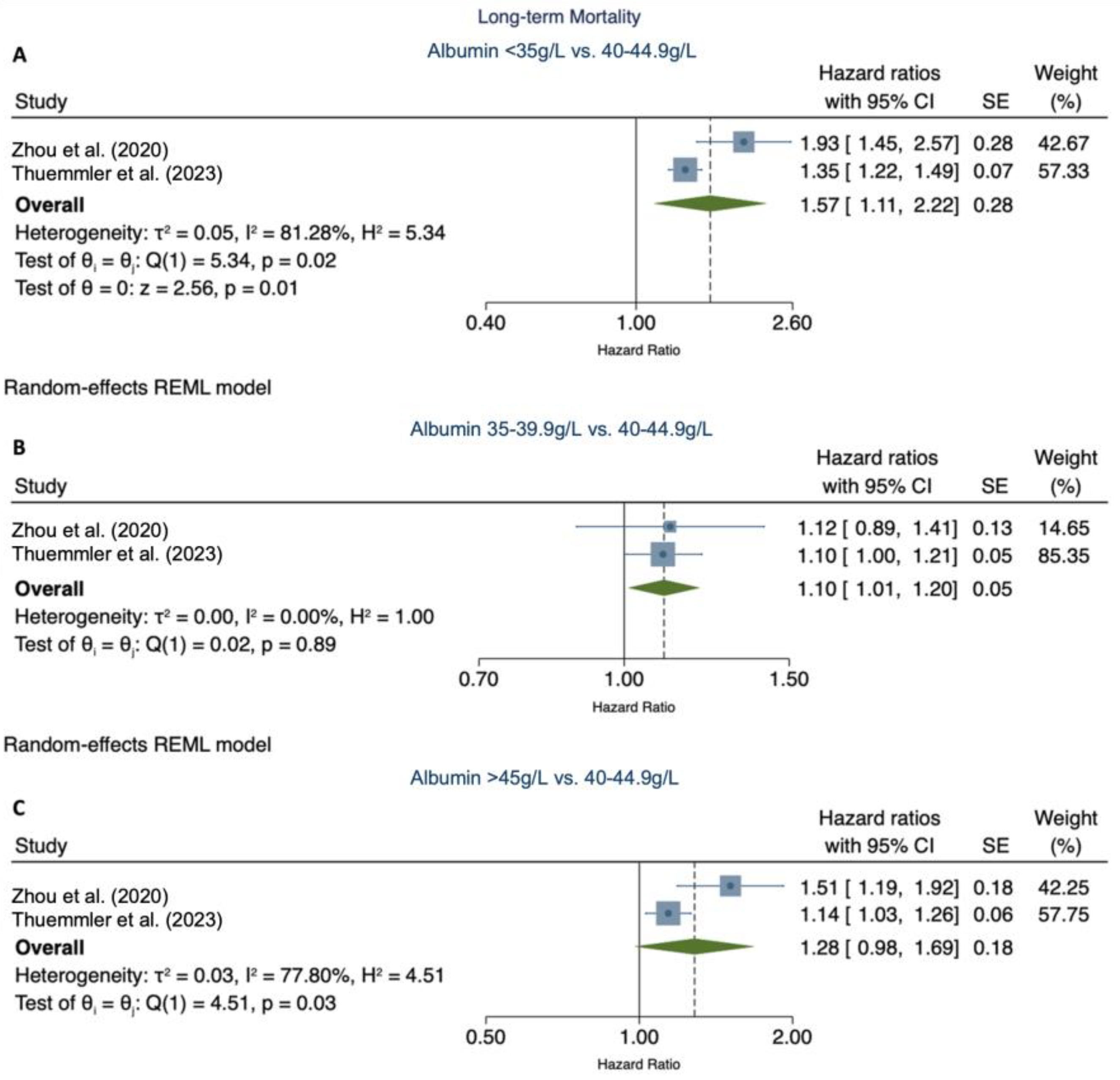
3.5. Meta-Analysis
Long-Term Mortality
3.6. Functional Outcome
3.7. Validity Assessment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Belayev, L.; Liu, Y.; Zhao, W.; Busto, R.; Ginsberg, M.D. Human Albumin Therapy of Acute Ischemic Stroke Marked Neuroprotective Efficacy at Moderate Doses and with a Broad Therapeutic Window. Stroke 2001, 32, 553–560. [Google Scholar] [CrossRef] [PubMed]
- Manolis, T.A.; Melita, H.; Mikhailidis, D.P.; Manolis, A.S. Low serum albumin: A neglected predictor in patients with cardiovascular disease. Eur. J. Intern. Med. 2022, 102, 24–39. [Google Scholar] [CrossRef] [PubMed]
- Mehta, A.; De Paola, L.; Pana, T.A.; Carter, B.; Soiza, R.L.; Kafri, M.W.; Potter, J.F.; Mamas, M.A.; Myint, P.K. The relationship between nutritional status at the time of stroke on adverse outcomes: A systematic review and meta-analysis of prospective cohort studies. Nutr. Rev. 2022, 80, 2275–2287. [Google Scholar] [CrossRef] [PubMed]
- Zhou, H.; Wang, A.; Meng, X.; Lin, J.; Jiang, Y.; Jing, J.; Zuo, Y.; Wang, Y.; Zhao, X.; Li, H.; et al. Low serum albumin levels predict poor outcome in patients with acute ischaemic stroke or transient ischaemic attack. Stroke Vasc. Neurol. 2021, 6, 458–466. [Google Scholar] [CrossRef] [PubMed]
- Gariballa, S.E.; Parker, S.G.; Taub, N.; Castleden, C.M. Influence of nutritional status on clinical outcome after acute stroke. Am. J. Clin. Nutr. 1998, 68, 275–281. [Google Scholar] [CrossRef] [PubMed]
- Dziedzic, T.; Slowik, A.; Szczudlik, A. Serum Albumin Level as a Predictor of Ischemic Stroke Outcome. Stroke 2004, 35, e156–e158. [Google Scholar] [CrossRef] [PubMed]
- Idicula, T.T.; Waje-Andreassen, U.; Brogger, J.; Naess, H.; Thomassen, L. Serum Albumin in Ischemic Stroke Patients: The Higher the BetterThe Bergen Stroke Study. Cerebrovasc. Dis. 2009, 28, 13–17. [Google Scholar] [CrossRef] [PubMed]
- Lázaro, V.A.; Del Ser Quijano, T.; Martín, R.B. Hypoalbuminemia and other prognostic factors of mortality at different time points after ischemic stroke. Nutr. Hosp. 2013, 28, 456–463. [Google Scholar] [CrossRef] [PubMed]
- Babu, M.S.; Kaul, S.; Dadheech, S.; Rajeshwar, K.; Jyothy, A.; Munshi, A. Serum albumin levels in ischemic stroke and its subtypes: Correlation with clinical outcome. Nutrition 2013, 29, 872–875. [Google Scholar] [CrossRef] [PubMed]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. PLoS Med. 2007, 4, e296. [Google Scholar] [CrossRef] [PubMed]
- Norfolk and Norwich University Hospitals NHS Foundation Trust. 2019. Available online: https://api.cqc.org.uk/public/v1/reports/5177a186-27e6-4541-82ec-8803abd597d4?20210115065848 (accessed on 12 September 2023).
- De La Iglesia, B.; Donell, S.; Rayward-Smith, V.; Bettencourt-Silva, J. On Creating a Patient-centric Database from Multiple Hospital Information Systems. Methods Inf. Med. 2012, 51, 210–220. [Google Scholar] [CrossRef] [PubMed]
- Smith, C.J.; Kishore, A.K.; Vail, A.; Chamorro, A.; Garau, J.; Hopkins, S.J. Diagnosis of Stroke-Associated Pneumonia: Recommendations From the Pneumonia in Stroke Consensus Group. Stroke 2015, 46, 2335–2340. [Google Scholar] [CrossRef] [PubMed]
- White, I.R.; Royston, P.; Wood, A.M. Multiple imputation using chained equations: Issues and guidance for practice. Stat. Med. 2011, 30, 377–399. [Google Scholar] [CrossRef] [PubMed]
- Holmberg, M.J.; Andersen, L.W. Estimating Risk Ratios and Risk Differences: Alternatives to Odds Ratios. JAMA 2020, 324, 1098–1099. [Google Scholar] [CrossRef] [PubMed]
- Risk of Bias Tools—ROBINS-E Tool, n.d. Available online: https://www.riskofbias.info/welcome/robins-e-tool (accessed on 4 August 2023).
- Yang, D.; Shen, J.; Huang, H.; Wang, J.; Sun, F.; Zeng, T.; Qiu, H.; Xie, H.; Chen, Y.; Li, S.; et al. Elevated Albumin to Globulin Ratio on Day 7 is Associated with Improved Function Outcomes in Acute Ischemic Stroke Patients with Intravenous Thrombolysis. J. Inflamm. Res. 2022, 15, 2695–2705. [Google Scholar] [CrossRef] [PubMed]
- Carter, A.M.; Catto, A.J.; Mansfield, M.W.; Bamford, J.M.; Grant, P.J. Predictive Variables for Mortality After Acute Ischemic Stroke. Stroke 2007, 38, 1873–1880. [Google Scholar] [CrossRef]
- Gabay, C.; Kushner, I. Acute-Phase Proteins and Other Systemic Responses to Inflammation. N. Engl. J. Med. 1999, 340, 448–454. [Google Scholar] [CrossRef] [PubMed]
- Zhang, G.; Pan, Y.; Zhang, R.; Wang, M.; Meng, X.; Li, Z.; Li, H.; Wang, Y.; Zhao, X.; Liu, G.; et al. Prevalence and Prognostic Significance of Malnutrition Risk in Patients With Acute Ischemic Stroke: Results From the Third China National Stroke Registry. Stroke 2022, 53, 111–119. [Google Scholar] [CrossRef] [PubMed]
- Halliwell, B.; Gutteridge, J.M. The antioxidants of human extracellular fluids. Arch. Biochem. Biophys. 1990, 280, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Arques, S. Human serum albumin in cardiovascular diseases. Eur. J. Intern. Med. 2018, 52, 8–12. [Google Scholar] [CrossRef] [PubMed]
- Watts, M.E.; Pocock, R.; Claudianos, C.; Chowen, J.A.; Arevalo, M.A.; Rosenberger, T.A. Brain Energy and Oxygen Metabolism: Emerging Role in Normal Function and Disease. Front. Mol. Neurosci. 2018, 11, 216. [Google Scholar] [CrossRef] [PubMed]
- Mikhailidis, D.P.; Mikhailidis, A.M.; Dandona, P. Effect of Human Plasma Proteins on Stabilisation of Platelet Anti-Aggregatory Activity of Prostacyclin. Ann. Clin. Biochem. Int. J. Biochem. Lab. Med. 1982, 19, 241–244. [Google Scholar] [CrossRef] [PubMed]
- Shaafi, S.; Ebrahimpour-Koujan, S.; Khalili, M.; Shamshirgaran, S.M.; Hashemilar, M.; Taheraghdam, A.; Shakouri, S.K.; Hokmabadi, E.S.; Ahmadi, Y.; Farhoudi, M.; et al. Effects of Alpha Lipoic Acid Supplementation on Serum Levels of Oxidative Stress, Inflammatory Markers and Clinical Prognosis among Acute Ischemic Stroke Patients: A Randomized, Double Blind, TNS Trial. Adv. Pharm. Bull. 2020, 10, 284–289. [Google Scholar] [CrossRef] [PubMed]
- Hashemilar, M.; Khalili, M.; Rezaeimanesh, N.; Hokmabadi, E.S.; Rasulzade, S.; Shamshirgaran, S.M.; Taheraghdam, A.; Farhoudi, M.; Shaafi, S.; Shakouri, S.K.; et al. Effect of Whey Protein Supplementation on Inflammatory and Antioxidant Markers, and Clinical Prognosis in Acute Ischemic Stroke (TNS Trial): A Randomized, Double Blind, Controlled, Clinical Trial. Adv. Pharm. Bull. 2020, 10, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Boesiger, F.; Poggioli, A.; Netzhammer, C.; Bretscher, C.; Kaegi-Braun, N.; Tribolet, P.; Wunderle, C.; Kutz, A.; Lobo, D.N.; Stanga, Z.; et al. Changes in serum albumin concentrations over 7 days in medical inpatients with and without nutritional support. A secondary post-hoc analysis of a randomized clinical trial. Eur. J. Clin. Nutr. 2023, 77, 989–997. [Google Scholar] [CrossRef] [PubMed]
- Bretscher, C.; Boesiger, F.; Kaegi-Braun, N.; Hersberger, L.; Lobo, D.N.; Evans, D.C.; Tribolet, P.; Gomes, F.; Hoess, C.; Pavlicek, V.; et al. Admission serum albumin concentrations and response to nutritional therapy in hospitalised patients at malnutrition risk: Secondary analysis of a randomised clinical trial. EClinicalMedicine 2022, 45, 101301. [Google Scholar] [CrossRef] [PubMed]
- Uchino, Y.; Watanabe, M.; Takata, M.; Amiya, E.; Tsushima, K.; Adachi, T.; Hiroi, Y.; Funazaki, T.; Komuro, I. Effect of Oral Branched-Chain Amino Acids on Serum Albumin Concentration in Heart Failure Patients with Hypoalbuminemia: Results of a Preliminary Study. Am. J. Cardiovasc. Drugs 2018, 18, 327–332. [Google Scholar] [CrossRef]
- Akirov, A.; Masri-Iraqi, H.; Atamna, A.; Shimon, I. Low Albumin Levels Are Associated with Mortality Risk in Hospitalized Patients. Am. J. Med. 2017, 130, 1465.e11–1465.e19. [Google Scholar] [CrossRef] [PubMed]
- Bucci, T.; Pastori, D.; Pignatelli, P.; Ntaios, G.; Abdul-Rahim, A.H.; Violi, F.; Lip, G.Y. Albumin Levels and Risk of Early Cardiovascular Complications After Ischemic Stroke: A Propensity-Matched Analysis of a Global Federated Health Network. Stroke 2024, 55, 604–612. [Google Scholar] [CrossRef] [PubMed]
- Makris, K.; Koniari, K.; Spanou, L.; Gialouri, E.; Evodia, E.; Lelekis, M. Prognostic significance of serum albumin level changes in acute ischemic stroke: The role of biological and analytical variation. Clin. Chem. Lab. Med. 2016, 54, 143–150. [Google Scholar] [CrossRef] [PubMed]
- Chen, N.; Li, Y.; Fang, J.; Lu, Q.; He, L. Meta-analyses Risk factors for malnutrition in stroke patients: A meta-analysis. Clin. Nutr. 2019, 38, 127–135. [Google Scholar] [CrossRef]
- Chapter 10: Analysing Data and Undertaking Meta-Analyses|Cochrane Training. Available online: https://training.cochrane.org/handbook/current/chapter-10 (accessed on 3 September 2023).



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total | Albumin QR1 | Albumin QR2 | Albumin QR3 | Albumin QR4 | p Value | |
|---|---|---|---|---|---|---|
| N | 9979 (0.00) | 2808 (28.14) | 2391 (23.96) | 2510 (25.15) | 2270 (22.75) | |
| Serum albumin, g/L, mean (SD) | 36.69 (5.38) | 30.09 (4.18) | 36.08 (0.81) | 38.95 (0.81) | 43.01 (2.13) | <0.001 |
| Age, years, mean (SD) | 78.26 (11.23) | 81.03 (10.33) | 78.84 (10.98) | 77.30 (11.07) | 75.27 (11.84) | <0.001 |
| Females | 5219 (56.62) | 1590 (56.62) | 1255 (44.69) | 1252 (44.59) | 1122 (39.96) | <0.001 |
| Comorbidities | ||||||
| Hypertension | 6138 (62.43) | 1753 (62.43) | 1485 (52.88) | 1526 (54.34) | 1374 (48.93) | 0.419 |
| Diabetes mellitus | 1806 (20.80) | 584 (20.80) | 412 (14.67) | 432 (15.38) | 378 (13.46) | <0.001 |
| Hyperlipidaemia | 1370 (11.22) | 315 (11.22) | 350 (12.46) | 374 (13.32) | 331 (11.79) | <0.001 |
| Coronary heart disease | 2792 (31.37) | 881 (31.37) | 707 (25.18) | 651 (23.18) | 553 (19.69) | <0.001 |
| Peripheral vascular disease | 659 (8.87) | 249 (8.87) | 162 (5.77) | 139 (4.95) | 109 (3.88) | <0.001 |
| Cerebrovascular disease | 9867 (98.72) | 2772 (98.72) | 2367 (84.29) | 2479 (88.28) | 2249 (80.09) | 0.566 |
| Dementia | 147 (2.35) | 66 (2.35) | 36 (1.28) | 29 (1.03) | 16 (0.57) | <0.001 |
| Cancer | 1590 (21.58) | 606 (21.58) | 373 (13.28) | 370 (13.18) | 241 (8.58) | <0.001 |
| Renal disease | 764 (12.71) | 357 (12.71) | 171 (6.09) | 143 (5.09) | 93 (3.31) | <0.001 |
| Liver disease | 151 (2.53) | 71 (2.53) | 37 (1.32) | 29 (1.03) | 14 (0.50) | <0.001 |
| Pulmonary disease | 1464 (18.41) | 517 (18.41) | 359 (12.78) | 350 (12.46) | 238 (8.48) | <0.001 |
| COPD | 826 (11.25) | 316 (11.25) | 204 (7.26) | 201 (7.16) | 105 (3.74) | <0.001 |
| Pneumonia aspiration | 845 (12.50) | 351 (12.50) | 182 (6.48) | 169 (6.02) | 143 (5.09) | <0.001 |
| Pneumonia non-aspiration | 1112 (18.27) | 513 (18.27) | 265 (9.44) | 195 (6.94) | 139 (4.95) | <0.001 |
| OCSP types, n (%) | ||||||
| Lacunar stroke (LACS) | 2554 (21.87) | 614 (21.87) | 595 (21.19) | 691 (24.61) | 654 (23.29) | <0.001 |
| Partial anterior circulation stroke (PACS) | 3791 (37.96) | 1066 (37.96) | 960 (34.19) | 962 (34.26) | 803 (28.60) | 0.010 |
| Posterior circulation syndrome (POCS) | 1651 (15.63) | 439 (15.63) | 392 (13.96) | 415 (14.78) | 405 (14.42) | 0.213 |
| Total anterior circulation stroke (TACS) | 1983 (24.54) | 689 (24.54) | 444 (15.81) | 442 (15.74) | 408 (14.53) | <0.001 |
| Pre-stroke mRs 0–2, n (%) | 1292 (25.71) | 451 (25.71) | 326 (18.59) | 296 (16.88) | 219 (12.49) | <0.001 |
| mRS at discharge, n (%) | 1893 (57.88) | 360 (57.88) | 456 (73.31) | 561 (90.19) | 516 (82.96) | <0.001 |
| Laboratory tests | ||||||
| WBC, mmol/L, mean (SD) | 8.80 (7.10–11.30) | 9.30 (7.30–12.30) | 8.40 (6.90–10.70) | 8.50 (7.00–10.80) | 9.00 (7.30–11.30) | <0.001 |
| CRP, mmol/L, mean (SD) | 11.00 (5.00–33.00) | 30.00 (10.00–75.00) | 9.00 (4.00–25.00) | 8.00 (4.00–19.00) | 8.00 (4.00–19.00) | <0.001 |
| Medication | ||||||
| Antiplatelet agents on discharge | 5894 (49.00) | 1376 (49.00) | 1460 (51.99) | 1632 (58.12) | 1426 (50.78) | <0.001 |
| Antiplatelet on admission | 3657 (36.11) | 1014 (36.11) | 889 (31.66) | 940 (33.48) | 814 (28.99) | 0.584 |
| Anticoagulants on discharge | 1200 (11.18) | 314 (11.18) | 315 (11.22) | 303 (10.79) | 268 (9.54) | 0.173 |
| Anticoagulant on admission | 120 (1.35) | 38 (1.35) | 33 (1.18) | 31 (1.10) | 18 (0.64) | 0.221 |
| Outcomes | ||||||
| Length of stay, n (IQR) | 8.00 (4.00–17.29) | 10.00 (4.21–22.00) | 8.00 (3.43–17.00) | 7.00 (3.00–15.22) | 7.00 (4.00–16.00) | <0.001 |
| NIHSS, n (IQR) | 5.00 (2.00–13.00) | 7.00 (3.00–14.00) | 5.00 (2.00–13.00) | 4.00 (2.00–12.00) | 4.00 (2.00–10.00) | <0.001 |
| Dead, n (%) | 4645 (60.40) | 1696 (60.40) | 1035 (36.86) | 953 (33.94) | 961 (34.22) | <0.001 |
| Poor outcomes (Rankin discharge ≥ 3) | 5193(65.88) | 1850(65.88) | 1242(44.23) | 1131(40.28) | 970(34.54) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thuemmler, R.J.; Pana, T.A.; Carter, B.; Mahmood, R.; Bettencourt-Silva, J.H.; Metcalf, A.K.; Mamas, M.A.; Potter, J.F.; Myint, P.K. Serum Albumin and Post-Stroke Outcomes: Analysis of UK Regional Registry Data, Systematic Review, and Meta-Analysis. Nutrients 2024, 16, 1486. https://doi.org/10.3390/nu16101486
Thuemmler RJ, Pana TA, Carter B, Mahmood R, Bettencourt-Silva JH, Metcalf AK, Mamas MA, Potter JF, Myint PK. Serum Albumin and Post-Stroke Outcomes: Analysis of UK Regional Registry Data, Systematic Review, and Meta-Analysis. Nutrients. 2024; 16(10):1486. https://doi.org/10.3390/nu16101486
Chicago/Turabian StyleThuemmler, Rosa J., Tiberiu A. Pana, Ben Carter, Ribeya Mahmood, Joao H. Bettencourt-Silva, Anthony K. Metcalf, Mamas A. Mamas, John F. Potter, and Phyo K. Myint. 2024. "Serum Albumin and Post-Stroke Outcomes: Analysis of UK Regional Registry Data, Systematic Review, and Meta-Analysis" Nutrients 16, no. 10: 1486. https://doi.org/10.3390/nu16101486
APA StyleThuemmler, R. J., Pana, T. A., Carter, B., Mahmood, R., Bettencourt-Silva, J. H., Metcalf, A. K., Mamas, M. A., Potter, J. F., & Myint, P. K. (2024). Serum Albumin and Post-Stroke Outcomes: Analysis of UK Regional Registry Data, Systematic Review, and Meta-Analysis. Nutrients, 16(10), 1486. https://doi.org/10.3390/nu16101486