

Vitamin D Supplementation at a Dose of 10 µg/Day in Institutionalized Children with Severe Motor and Intellectual Disabilities
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects (Table 1)

{kind=link}
{kind=link}
{kind=link}
| Group | Subject No. | Sex | Age (Years) † | Nutrition | Nutritional-Contents § | Diseases | Phase 2020 | Phase 2021 | UV before Phase 2020 | UV before Phase 2021 | VD Supplementation | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Phase 2020 | Phase 2021 | Intake (μg/Day) | Ratio ‡ | Serum 25(OH)D (ng/mL) | Intake (μg/Fay) | Ratio ‡ | Serum 25(OH)D (ng/mL) | |||||||||
| α-2020 | A-2021 | 1 | F | 3.25 | Tube | Blended diet | HIE | 4.5 | 1.13 | 4.3 | 15.1 | 3.78 | 23.3 | ◯ | ◯ | ◯ |
| 2 | F | 3.4 | Tube | Blended diet | Encephalopathy | 3.2 | 0.8 | 4.3 | 14.6 | 3.65 | 21 | ◯ | ◯ | ◯ | ||
| 3 | M | 4.1 | Oral | Chopped soft diet | Schizencephaly | 7.5 | 2.14 | 14.5 | 17.7 | 5.06 | 27.1 | ◯ | ◯ | ◯ | ||
| 4 | F | 6.4 | Tube | Blended diet, ENEVO® | HIE | 8.0 | 1.6 | 17.2 | 18 | 3.6 | 29.3 | ◯ | ◯ | ◯ | ||
| 5 | F | 8.5 | Oral | Chopped soft diet | HIE | 7.2 | 1.2 | 7.8 | 15.5 | 2.58 | 31.3 | ◯ | ◯ | ◯ | ||
| 6 | F | 8.0 | Oral | Regular diet | Encephalopathy | 7.9 | 1.32 | 16.5 | 18.4 | 3.07 | 34.2 | ◯ | ◯ | ◯ | ||
| 7 | F | 11.5 | Oral | Regular diet | Muscular dystrophy | 7.5 | 0.94 | 11.2 | 18 | 1.89 | 18 | ◯ | ◯ | ◯ | ||
| 8 | F | 14.2 | Oral | Chopped soft diet | Chromosomal abnormality | 9.7 | 1.02 | 5.4 | 19.7 | 2.32 | 28.1 | ◯ | ◯ | ◯ | ||
| 9 | M | 14.3 | Oral | Regular diet | Muscular dystrophy | 10.0 | 1.25 | 7 | 23.1 | 2.57 | 20 | ◯ | ◯ | ◯ | ||
| 10 | M | 14.7 | Oral | Regular diet | HIE | 14.4 | 1.8 | 12.7 | 24.4 | 2.71 | 20.5 | ◯ | ◯ | ◯ | ||
| B-2021 | 11 | M | 11.4 | Oral | Regular diet | Hydrocephalus | 6.8 | 1.05 | 11.9 | 8.1 | 1.01 | 16.8 | ◯ | ◯ | ✕ | |
| β-2020 | A-2021 | 12 | M | 1.25 | Oral | Infant formula and baby food | Chromosomal abnormality | 7.3 | 2.43 | 17 | 16.9 | 5.63 | 24.4 | ✕ | ◯ | ◯ |
| 13 | M | 1.5 | Tube | Blended diet | Subdural hematoma | 2.7 | 0.9 | 4.8 | 13.1 | 4.37 | 31.8 | ✕ | ◯ | ◯ | ||
| 14 | F | 4.5 | Tube | Blended diet, RACOL-NF® | Multiple anomaly | 4.1 | 1.03 | 6 | 15 | 3.75 | 37.7 | ✕ | ◯ | ◯ | ||
| 15 | F | 6 | Tube | Blended diet, ENEVO® | HIE | 4.5 | 0.9 | 9.4 | 17.6 | 3.52 | 27.6 | ✕ | ◯ | ◯ | ||
| 16 | M | 6.75 | Oral | Blended diet | Multiple anomaly | 6.6 | 1.47 | 7.3 | 16.7 | 3.71 | 38.4 | ✕ | ◯ | ◯ | ||
| 17 | F | 7.1 | Oral | Chopped soft diet | Congenital CMV infection | 7.7 | 1.54 | 8.4 | 18.7 | 3.12 | 23.5 | ✕ | ◯ | ◯ | ||
| 18 | F | 7.25 | Tube | RACOL-NF®, Blended diet, V CRESC® | HIE | 3.4 | 0.68 | 8.9 | 21.7 | 3.62 | 39 | ✕ | ◯ | ◯ | ||
| 19 | M | 8.4 | Oral | Chopped soft diet | Angelman syndrome | 8.8 | 1.76 | 6 | 18.8 | 3.76 | 32.7 | ✕ | ◯ | ◯ | ||
| 20 | F | 8.8 | Tube | RACOL-NF®, V CRESC® | Chromosomal abnormality | 4.4 | 0.73 | 13.2 | 21.9 | 3.65 | 30.3 | ✕ | ◯ | ◯ | ||
| 21 | F | 11 | Tube | ENEVO®, Blended diet | Bacterial meningitis | 4.2 | 0.53 | 7.6 | 15.8 | 1.66 | 22.1 | ✕ | ◯ | ◯ | ||
| 22 | F | 11.2 | Tube | ENEVO®, RACOL-NF® | HIE | 7.6 | 0.95 | 12.6 | 23.6 | 2.48 | 23 | ✕ | ◯ | ◯ | ||
| 23 | M | 12 | Combined | Blended diet, dysphagia food | Brain tumor | 7.2 | 0.9 | 8.1 | 17.8 | 2.23 | 25.7 | ✕ | ◯ | ◯ | ||
| 24 | M | 13.1 | Oral | Regular diet | Spinal muscular atrophy | 6.6 | 0.83 | 13.1 | 17.5 | 2.19 | 22.1 | ✕ | ◯ | ◯ | ||
| C-2021 | 25 | M | 2.75 | Tube | Anti-regurgitation formula | HIE | 2 | 0.67 | 10.9 | 12.5 | 3.57 | 16.8 | ✕ | ✕ | ◯ | |
| 26 | M | 4.2 | Tube | Anti-regurgitation formula | HIE | 7.9 | 2.26 | 15.2 | 19.8 | 5.66 | 19.1 | ✕ | ✕ | ◯ | ||
| D-2021 | 27 | F | 6.8 | Tube | ENEVO®, Blended diet | HIE | 2.7 | 0.54 | 6.7 | 9.1 | 1.82 | 9.1 | ✕ | ✕ | ✕ | |
| 28 | M | 14.8 | Tube | Blended diet ENEVO® | Brain malformation | 6.1 | 0.76 | 6.5 | 8.1 | 0.9 | 7.8 | ✕ | ✕ | ✕ | ||
2.2. Examinations
2.3. Statistical Analyses
3. Results
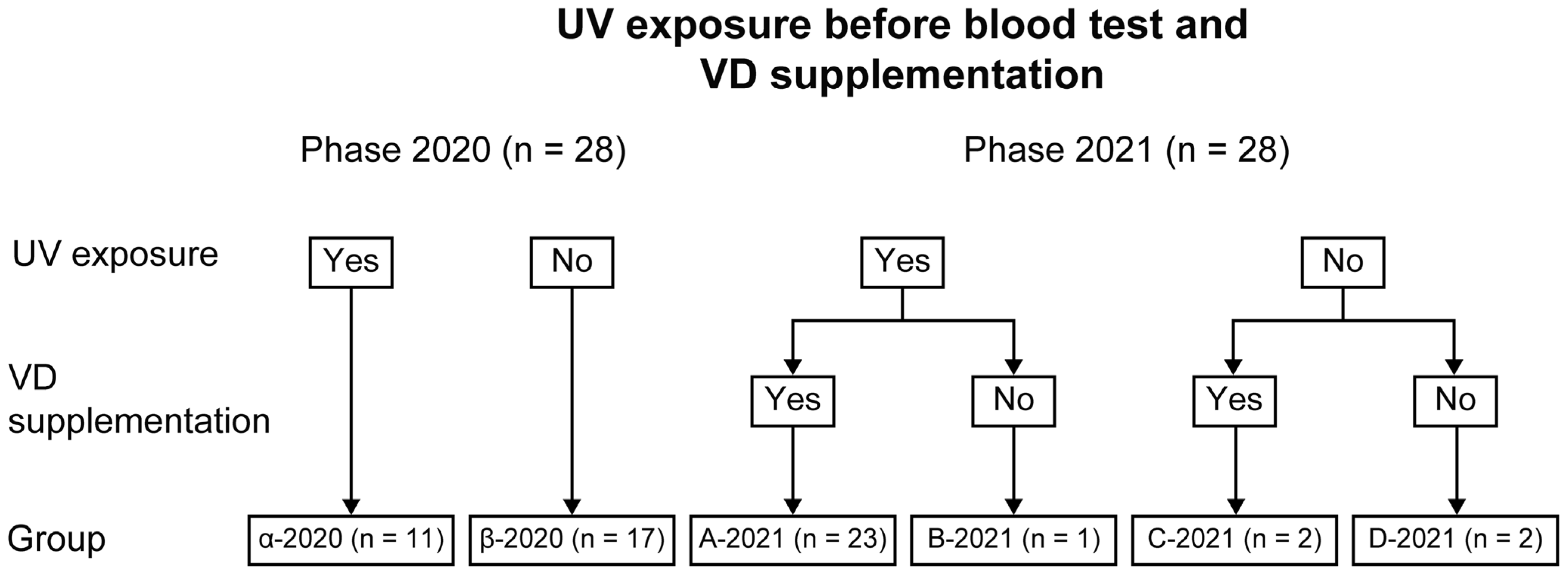
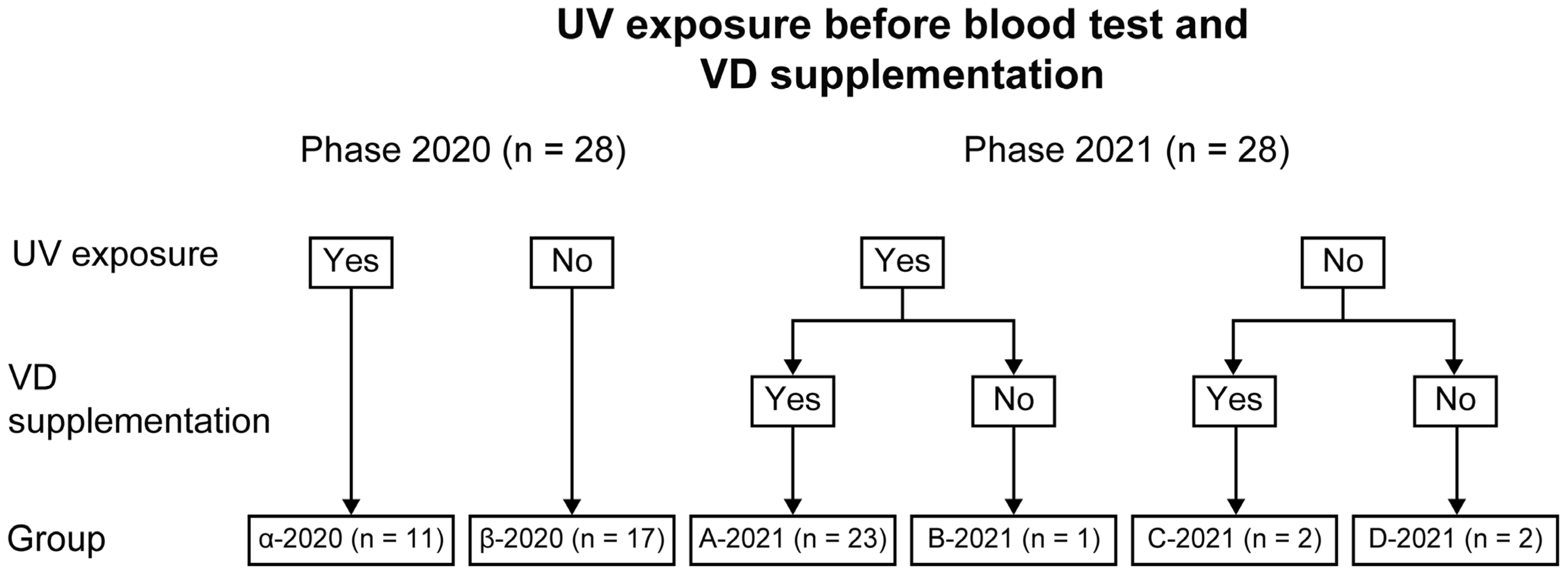
3.1. Subjects and Grouping
3.2. VD Intake, UV Exposure, and Serum 25(OH)D per Phase
3.2.1. Phase 2020
3.2.2. Phase 2021
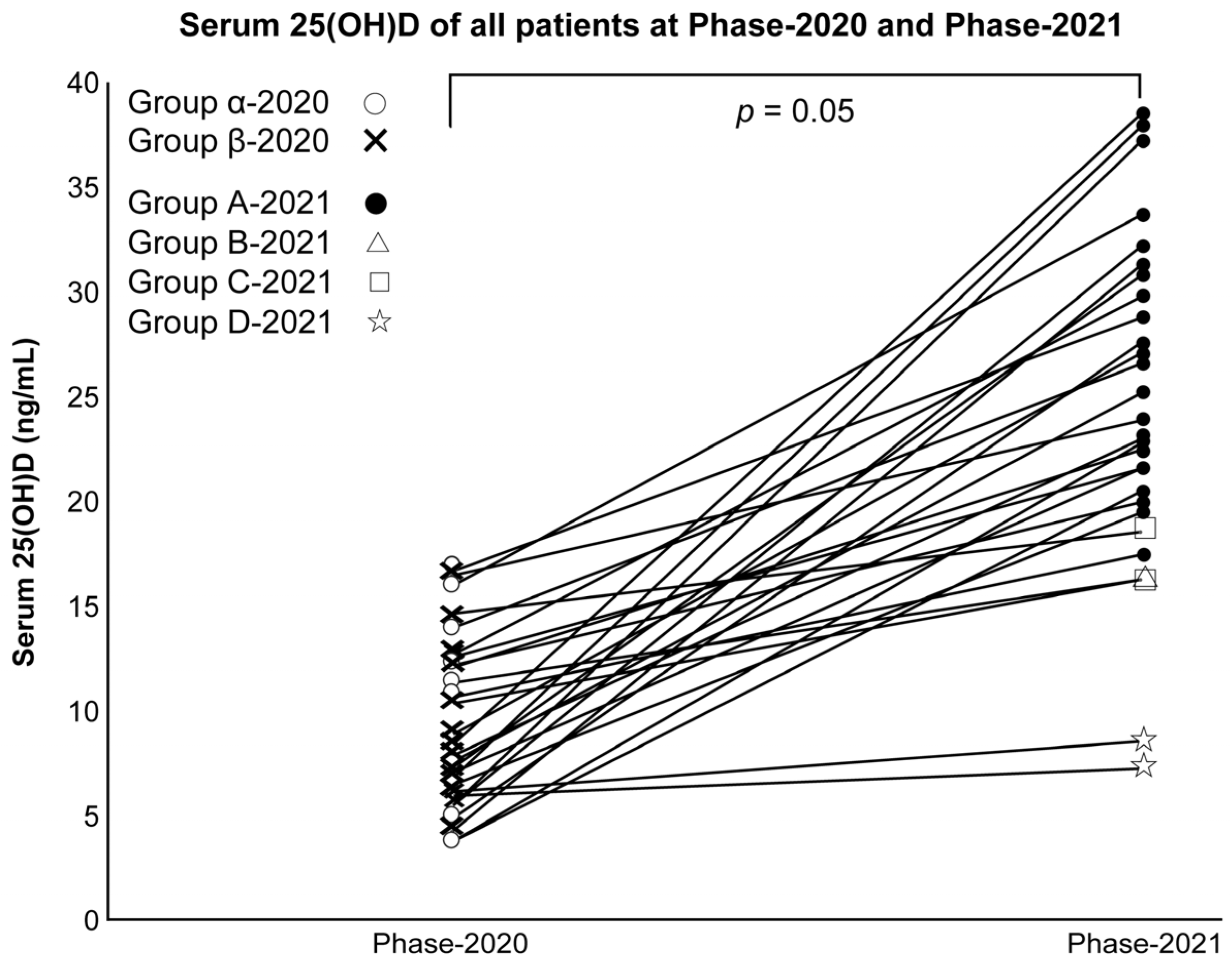
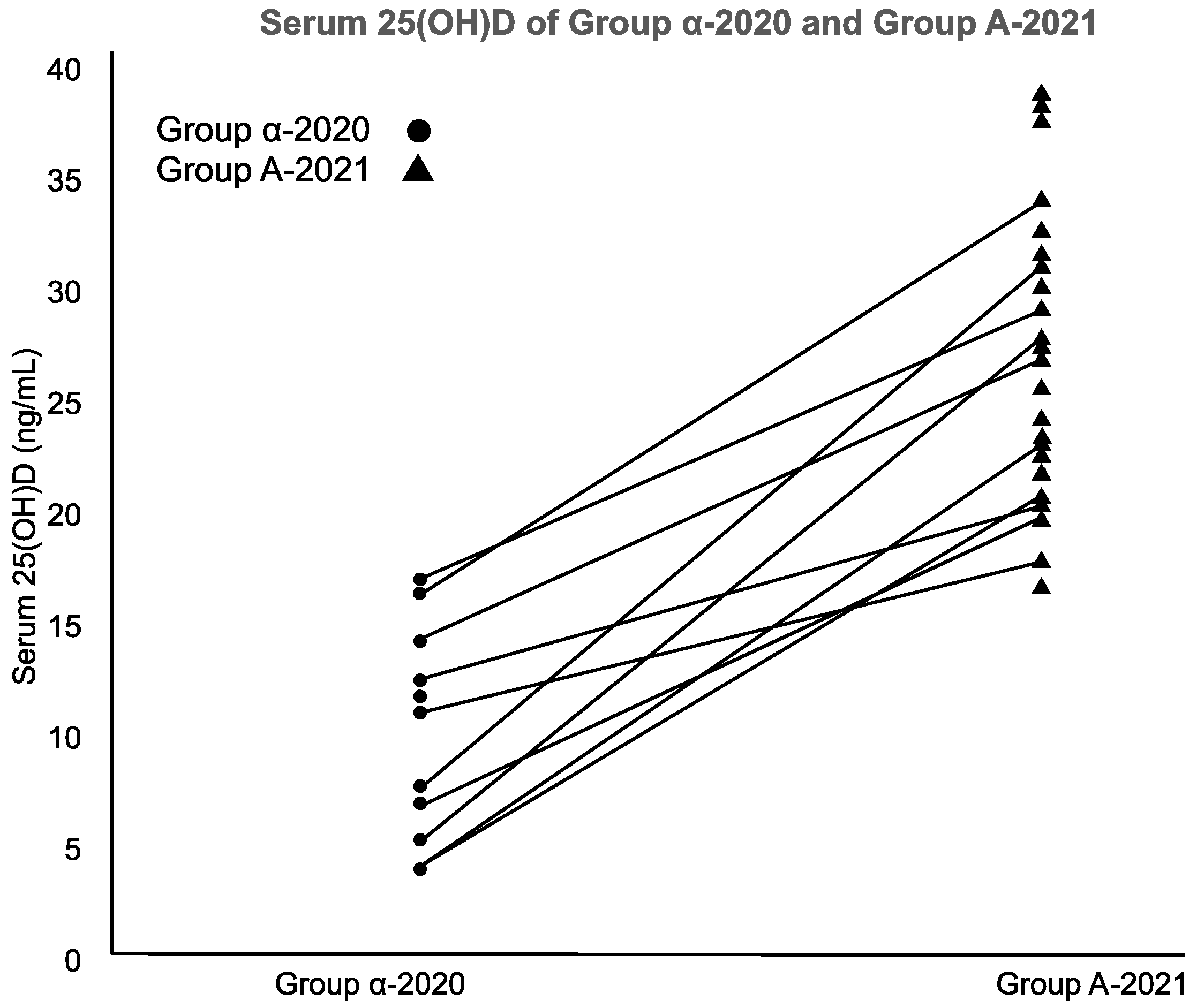
3.3. Statistical Analysis
4. Discussion
Limitation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Holick, M.F. Vitamin D Deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef] [PubMed]
- Sakai, T. Osteoporosis and fractures in patients with severe motor and intellectual disabilities. Nihon Jushoshinshinshogai Gakkaishi/Sev. Mot. J. Intellect. Disabil. 2019, 44, 99–104. (In Japanese) [Google Scholar]
- Joshi, M.; Uday, S. Vitamin D deficiency in chronic childhood disorders: Importance of screening and prevention. Nutrients 2023, 15, 2805. [Google Scholar] [CrossRef] [PubMed]
- Tomimoto, K. Assessment of vitamin D sufficiency in breastfed infants in one area in northern Japan. Nihon Shonika Gakkai Zasshi/J. Jpn. Pediatr. Soc. 2018, 122, 1563–1571. (In Japanese) [Google Scholar]
- Sato, Y.; Kamei, A.; Toda, H.; Endo, F.; Kasai, T. Vitamin D deficiency in children with severe disabilities under limited ultraviolet exposure. J. Bone Miner. Metab. 2023, 41, 52–60. [Google Scholar] [CrossRef] [PubMed]
- Bikle, D.D. Vitamin D and bone. Curr. Osteoporos. Rep. 2012, 10, 151–159. [Google Scholar] [CrossRef] [PubMed]
- Kuwabara, A.; Tsugawa, N.; Tanaka, K.; Fujii, M.; Kawai, N.; Mukae, S.; Kato, Y.; Kojima, Y.; Takahashi, K.; Omura, K.; et al. Improvement of vitamin D status in Japanese institutionalized elderly by supplementation with 800 IU of vitamin D3. J. Nutr. Sci. Vitaminol. 2009, 55, 453–458. [Google Scholar] [CrossRef]
- Duque, G.; Lord, S.R.; Mak, J.; Ganda, K.; Close, J.J.; Ebeling, P.; Papaioannou, A.; Inderjeeth, C.A. Treatment of osteoporosis in Australian residential aged care facilities: Update on consensus recommendations for fracture prevention. J. Am. Med. Dir. Assoc. 2016, 17, 852–859. [Google Scholar] [CrossRef]
- Walker, P.; Kifley, A.; Kurrle, S.; Cameron, I.D. Increasing the uptake of vitamin D supplement use in Australian residential aged care facilities: Results from the vitamin D implementation (ViDAus) study. BMC Geriatr. 2020, 20, 383. [Google Scholar] [CrossRef]
- Ministry of Health, Labour and Welfare in Japan. Dietary Reference Intakes for Japanese. 2020; Volume 2020, p. 206. Available online: https://www.mhlw.go.jp/content/10904750/000586553.pdf (accessed on 8 August 2023). (In Japanese)
- Wagner, C.L.; Greer, F.R.; American Academy of Pediatrics Section on Breastfeeding; American Academy of Pediatrics Committee on Nutrition. Prevention of rickets and vitamin D deficiency in infants, children, and adolescents. Pediatrics 2008, 122, 1142–1152. [Google Scholar] [CrossRef]
- Amrein, K.; Scherkl, M.; Hoffmann, M.; Neuwersch-Sommeregger, S.; Köstenberger, M.; Tmava Berisha, A.T.; Martucci, G.; Pilz, S.; Malle, O. Vitamin D deficiency 2.0: An update on the current status worldwide. Eur. J. Clin. Nutr. 2020, 74, 1498–1513. [Google Scholar] [CrossRef] [PubMed]
- Niedermaier, T.; Gredner, T.; Kuznia, S.; Schöttker, B.; Mons, U.; Lakerveld, J.; Ahrens, W.; Brenner, H.; PEN-Consortium. Vitamin D food fortification in European countries: The underused potential to prevent cancer deaths. Eur. J. Epidemiol. 2022, 37, 309–320. [Google Scholar] [CrossRef] [PubMed]
- De La Guía-Galipienso, F.; Martínez-Ferrán, M.; Vallecillo, N.; Lavie, C.J.; Sanchís-Gomar, F.; Pareja-Galeano, H. Vitamin D and cardiovascular health. Clin. Nutr. 2021, 40, 2946–2957. [Google Scholar] [CrossRef] [PubMed]
- Langley, C.K.; Onambélé-Pearson, G.; Sims, D.T.; Hussain, A.; Mohindra, R.K.; Kershaw, B.L.; Morse, C.I. Seasonal variations in vitamin D do not change the musculoskeletal health of physically active ambulatory men with cerebral palsy: A longitudinal cross-sectional comparison study. Nutr. Res. 2023, 111, 24–33. [Google Scholar] [CrossRef] [PubMed]
- Cutolo, M.; Smith, V.; Paolino, S.; Gotelli, E. Involvement of the secosteroid vitamin D in autoimmune rheumatic diseases and COVID-19. Nat. Rev. Rheumatol. 2023, 19, 265–287. [Google Scholar] [CrossRef] [PubMed]
- Viraraghavan, V.R.; Seth, A.; Aneja, S.; Singh, R.; Dhanwal, D. Effect of high dose vitamin D supplementation on vitamin D nutrition status of pre-pubertal children on anti-epileptic drugs—A randomized controlled trial. Clin. Nutr. ESPEN 2019, 29, 36–40. [Google Scholar] [CrossRef]
- Okazaki, R.; Ozono, K.; Fukumoto, S.; Inoue, D.; Yamauchi, M.; Minagawa, M.; Michigami, T.; Takeuchi, Y.; Matsumoto, T.; Sugimoto, T. Assessment criteria for vitamin D deficiency/insufficiency in Japan: Proposal by an expert panel supported by the Research Program of Intractable Diseases, Ministry of Health, Labour and Welfare, Japan, the Japanese Society for Bone and Mineral Research and the Japan Endocrine Society [Opinion]. J. Bone Miner. Metab. 2017, 35, 1–5. [Google Scholar] [CrossRef]
- Himeno, M.; Tsugawa, N.; Kuwabara, A.; Fujii, M.; Kawai, N.; Kato, Y.; Kihara, N.; Toyoda, T.; Kishimoto, M.; Ogawa, Y.; et al. Effect of vitamin D supplementation in the institutionalized elderly. J. Bone Miner. Metab. 2009, 27, 733–737. [Google Scholar] [CrossRef]
- Frighi, V.; Morovat, A.; Stephenson, M.T.; White, S.J.; Hammond, C.V.; Goodwin, G.M. Vitamin D deficiency in patients with intellectual disabilities: Prevalence, risk factors and management strategies. Br. J. Psychiatry 2014, 205, 458–464. [Google Scholar] [CrossRef]
- Sakai, T.; Shirai, T.; Oishi, T. Vitamins K and D deficiency in severe motor and intellectually disabled patients. Brain Dev. 2021, 43, 200–207. [Google Scholar] [CrossRef]
- Seth, A.; Aneja, S.; Singh, R.; Majumdar, R.; Sharma, N.; Gopinath, M. Effect of impaired ambulation and anti-epileptic drug intake on vitamin D status of children with cerebral palsy. Paediatr. Int. Child Health 2017, 37, 193–198. [Google Scholar] [CrossRef] [PubMed]
- Bouillon, R. Comparative analysis of nutritional guidelines for vitamin D. Nat. Rev. Endocrinol. 2017, 13, 466–479. [Google Scholar] [CrossRef] [PubMed]
- Kuwabara, A.; Nagae, A.; Kitagawa, M.; Tozawa, K.; Kumode, M.; Tanaka, K. Nutritional therapy with vitamin K is effective in the improvement of vitamin K status and bone turnover markers in patients with severe motor and intellectual disabilities. J. Nutr. Sci. Vitaminol. 2020, 66, 278–284. [Google Scholar] [CrossRef] [PubMed]
- Brustad, N.; Yousef, S.; Stokholm, J.; Bønnelykke, K.; Bisgaard, H.; Chawes, B.L. Safety of high-dose vitamin D supplementation among children aged 0 to 6 years: A systematic review and meta-analysis. JAMA Netw. Open 2022, 5, e227410. [Google Scholar] [CrossRef]
- Milart, J.; Lewicka, A.; Jobs, K.; Wawrzyniak, A.; Majder-Łopatka, M.; Kalicki, B. Effect of vitamin D treatment on dynamics of stones formation in the urinary tract and bone density in children with idiopathic hypercalciuria. Nutrients 2020, 12, 2521. [Google Scholar] [CrossRef]
- Catharine, A.R.; Taylor, C.L.; Yaktine, A.L.; Del Valle, H.B.; Institute of Medicine (US) Committee. Dietary Reference Intakes for Vitamin D and Calcium; National Academies Press: Washington, DC, USA, 2011. Available online: https://www.ncbi.nlm.nih.gov/books/NBK56070/ (accessed on 10 August 2023).
- Alonso, N.; Zelzer, S.; Eibinger, G.; Herrmann, M. Vitamin D metabolites: Analytical challenges and clinical relevance. Calcif. Tissue Int. 2022, 112, 158–177. [Google Scholar] [CrossRef]
- Asakura, K.; Etoh, N.; Imamura, H.; Michikawa, T.; Nakamura, T.; Takeda, Y.; Mori, S.; Nishiwaki, Y. Vitamin D status in Japanese adults: Relationship of serum 25-hydroxyvitamin D with simultaneously measured dietary vitamin D intake and ultraviolet ray exposure. Nutrients 2020, 12, 743. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sato, Y.; Kamei, A.; Endo, F.; Matsuyama, S.; Toda, H.; Kasai, T. Vitamin D Supplementation at a Dose of 10 µg/Day in Institutionalized Children with Severe Motor and Intellectual Disabilities. Nutrients 2024, 16, 122. https://doi.org/10.3390/nu16010122
Sato Y, Kamei A, Endo F, Matsuyama S, Toda H, Kasai T. Vitamin D Supplementation at a Dose of 10 µg/Day in Institutionalized Children with Severe Motor and Intellectual Disabilities. Nutrients. 2024; 16(1):122. https://doi.org/10.3390/nu16010122
Chicago/Turabian StyleSato, Yota, Atsushi Kamei, Fumie Endo, Sakura Matsuyama, Hiroyuki Toda, and Takeo Kasai. 2024. "Vitamin D Supplementation at a Dose of 10 µg/Day in Institutionalized Children with Severe Motor and Intellectual Disabilities" Nutrients 16, no. 1: 122. https://doi.org/10.3390/nu16010122
APA StyleSato, Y., Kamei, A., Endo, F., Matsuyama, S., Toda, H., & Kasai, T. (2024). Vitamin D Supplementation at a Dose of 10 µg/Day in Institutionalized Children with Severe Motor and Intellectual Disabilities. Nutrients, 16(1), 122. https://doi.org/10.3390/nu16010122