

Ready-to-Use Therapeutic Foods Fail to Improve Vitamin A and Iron Status Meaningfully during Treatment for Severe Acute Malnutrition in 6–59-Month-old Cambodian Children

Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Study Population
2.3. Ready-to-Use Therapeutic Foods and Treatment
2.4. Blood Sampling and Laboratory Analyses
2.5. Definition of Micronutrient and Health Status
2.6. Ethical Considerations
2.7. Statistical Analyses
3. Results
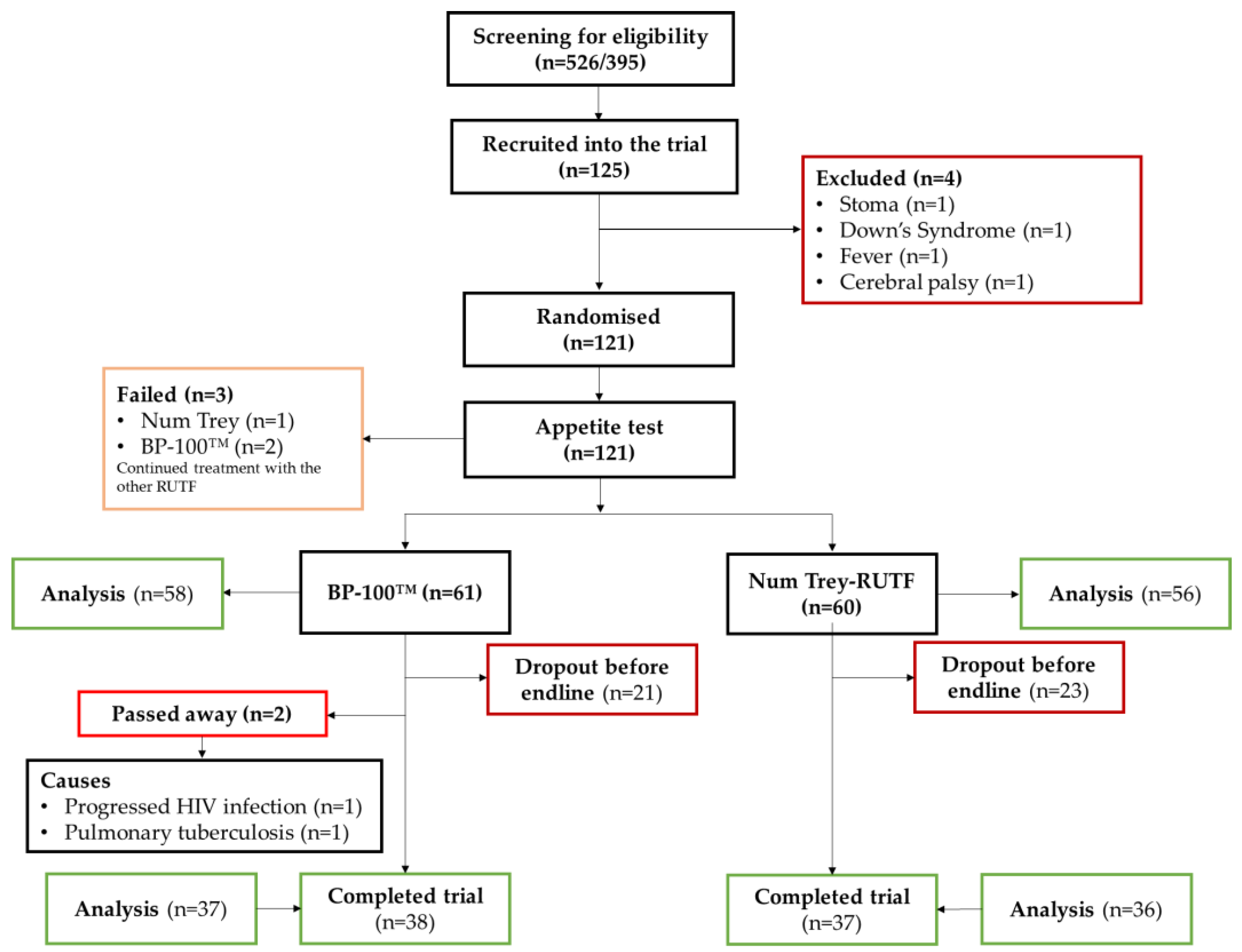
3.1. Participants’ Characteristics
3.2. Effectiveness of SAM Treatment on Micronutrient Status
3.3. Comparison between RUTFs
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AGP | α1-acid glycoprotein |
| BI | Body iron |
| CRP | C-reactive protein |
| FER | Ferritin |
| HDVAC | High-dose vitamin A capsule |
| MUAC | Mid-upper-arm circumference |
| RBP | Retinol-binding protein |
| RUTF | Ready-to-use therapeutic foods |
| SAM | Severe acute malnutrition |
| sTfR | Soluble transferrin receptor |
| SD | Standard deviation |
| WHO | World Health Organization |
| WHZ | Weight-for-height z-score |
References
- Black, R.E.; Victora, C.G.; Walker, S.P.; Bhutta, Z.A.; Christian, P.; De Onis, M.; Ezzati, M.; Grantham-Mcgregor, S.; Katz, J.; Martorell, R.; et al. Maternal and Child Undernutrition and Overweight in Low-Income and Middle-Income Countries. Lancet 2013, 382, 427–451. [Google Scholar] [CrossRef] [PubMed]
- Lapidus, N.; Luquero, F.J.; Gaboulaud, V.; Shepherd, S.; Grais, R.F. Prognostic Accuracy of WHO Growth Standards to Predict Mortality in a Large-Scale Nutritional Program in Niger. PLoS Med. 2009, 6, e1000039. [Google Scholar] [CrossRef] [PubMed]
- Saurabh, K.; Ranjan, S.; Narayan, J.P. Co-Morbidities and Micronutrient Deficiencies in Children with Severe Acute Malnutrition Fasciola Buski Infestation in Children View Project Co-Morbidities and Micronutrient Deficiencies in Children with Severe Acute Malnutrition. Int. J. Contemp. Pediatr. 2017, 44, 1225–1227. [Google Scholar] [CrossRef]
- Smit, E.N.; Muskiet, F.a.J.; Boersma, E.R. The Possible Role of Essential Fatty Acids in the Pathophysiology of Malnutrition: A Review. Prostaglandins Leukot. Essent. Fat. Acids 2004, 71, 241–250. [Google Scholar] [CrossRef]
- Bachou, H.; Tylleskär, T.; Kaddu-Mulindwa, D.H.; Tumwine, J.K. Bacteraemia among Severely Malnourished Children Infected and Uninfected with the Human Immunodeficiency Virus-1 in Kampala, Uganda. BMC Infect. Dis. 2006, 6, 160. [Google Scholar] [CrossRef]
- Babirekere-Iriso, E.; Musoke, P.; Kekitiinwa, A. Bacteraemia in Severely Malnourished Children in an HIV-Endemic Setting. Ann. Trop. Paediatr. 2006, 26, 319–328. [Google Scholar] [CrossRef]
- Jones, K.D.J.; Berkley, J.A. Severe Acute Malnutrition and Infection. Paediatr. Int. Child Health 2014, 34, S1–S29. [Google Scholar] [CrossRef]
- Jones, K.D.; Berkley, J.A. Childhood Malnutrition: Toward an Understanding of Infections, Inflammation, and Antimicrobials. Food Nutr. Bull. 2014, 35, 64–70. [Google Scholar] [CrossRef]
- Thakur, N.; Chandra, J.; Pemde, H.; Singh, V. Anemia in Severe Acute Malnutrition. Nutrition 2014, 30, 440–442. [Google Scholar] [CrossRef]
- Bailey, R.L. The Epidemiology of Global Micronutrient Deficiencies. Ann. Nutr. Metab. 2015, 66, 22–33. [Google Scholar] [CrossRef]
- Moench-Pfanner, R.; Silo, S.; Laillou, A.; Wieringa, F.; Hong, R.; Hong, R.; Poirot, E.; Bagriansky, J. The Economic Burden of Malnutrition in Pregnant Women and Children under 5 Years of Age in Cambodia. Nutrients 2016, 8, 292. [Google Scholar] [CrossRef]
- WHO. Guideline: Updates on the Management of Severe Acute Malnutrition in Infants and Children; World Health Organization: Geneva, Switzerland, 2013; pp. 1–123. [Google Scholar]
- De Pee, S.; Bloem, M.W. Current and Potential Role of Specially Formulated Foods and Food Supplements for Preventing Malnutrition among 6–23 Month Old Children and Treating Moderate Malnutrition among 6–59 Months Old Children. Food Nutr. Bull. 2009, 30, 1–40. [Google Scholar] [CrossRef]
- Manary, M.J. Local Production and Provision of Ready To Use Therapeutic Food (Rutf) Spread for the Treatment of Severe Childhood Malnutrition. Food Nutr. Bull. 2006, 27, 83–89. [Google Scholar] [CrossRef]
- Ciliberto, M.; Manary, M.; Ndekha, M.; Briend, A.; Ashorn, P. Home-Based Therapy for Oedematous Malnutrition with Ready-to-Use Therapeutic Food. Acta Paediatr. Int. J. Paediatr. 2006, 95, 1012–1015. [Google Scholar] [CrossRef]
- Ravichandra, K.R.; Behera, N. Locally Prepared Ready to Use Therapeutic Food for the Treatment of Children with Severe Acute Malnutrition: A Randomized Controlled Trial. Int J Contemp Pediatr. 2017, 4, 1491–1495. [Google Scholar]
- Diop, E.H.I.; Dossou, N.I.; Ndour, M.M.; Briend, A.; Wade, S. Comparison of the Efficacy of a Solid Ready-to-Use Food and a Liquid, Milk-Based Diet for the Rehabilitation of Severely Malnourished Children: A Randomized Trial. Am. J. Clin. Nutr. 2003, 78, 302–307. [Google Scholar] [CrossRef]
- Sandige, H.; Ndekha, M.J.; Briend, A.; Ashorn, P.; Manary, M.J. Home-Based Treatment of Malnourished Malawian Children with Locally Produced or Imported Ready-to-Use Food. J. Pediatr. Gastroenterol. Nutr. 2004, 39, 141–146. [Google Scholar] [CrossRef]
- Schoonees, A.; Mj, L.; Musekiwa, A.; Nel, E.; Volmink, J. Ready-to-Use Therapeutic Food (RUTF) for Home-Based Nutritional Rehabilitation of Severe Acute Malnutrition in Children from Six Months to Five Years of Age (Review). Cochrane 2019, 5, CD009000. [Google Scholar] [CrossRef]
- National Institute of Statistics, Directorate General for Health, and ICF International. Cambodia Demographic and Health Survey 2014; National Institute of Statistics, Directorate General for Health, and ICF International: Phnom Penh, Cambodia; Rockville, MD, USA, 2015; pp. 1–479. [Google Scholar]
- Kassebaum, N.J.; Jasrasaria, R.; Naghavi, M.; Wulf, S.K.; Johns, N.; Lozano, R.; Regan, M.; Weatherall, D.; Chou, D.P.; Eisele, T.P.; et al. A Systematic Analysis of Global Anemia Burden from 1990 to 2010. Blood 2014, 123, 615–625. [Google Scholar] [CrossRef]
- Wieringa, F.T.; Dahl, M.; Chamnan, C.; Poirot, E.; Kuong, K.; Sophonneary, P.; Sinuon, M.; Greuffeille, V.; Hong, R.; Berger, J.; et al. The High Prevalence of Anemia in Cambodian Children and Women Cannot Be Satisfactorily Explained by Nutritional Deficiencies or Hemoglobin Disorders. Nutrients 2016, 8, 348. [Google Scholar] [CrossRef]
- Karakochuk, C.D.; Whitfield, K.C.; Barr, S.I.; Lamers, Y.; Devlin, A.M.; Vercauteren, S.M.; Kroeun, H.; Talukder, A.; Mclean, J.; Green, T.J. Genetic Hemoglobin Disorders Rather Than Iron Deficiency Are a Major Predictor of Hemoglobin Concentration in Women of Reproductive Age in Rural Prey Veng, Cambodia. J. Nutr. 2015, 145, 134–142. [Google Scholar] [CrossRef] [PubMed]
- Savadogo, L.G.B.; Zoetaba, I.; Ilboudo, B.; Kinda, M.; Donnen, P. Impact of Anemia on Mortality and Nutritional Recovery among Hospitalized Severely Malnourished Children in Burkina Faso. Open J. Pediatr. 2014, 4, 115–120. [Google Scholar] [CrossRef][Green Version]
- Arya, A.K.; Kumar, P.; Midha, T.; Singh, M. Co-Morbidities in Children with Severe Acute Malnutrition—A Tertiary Care Centre Experience. Int. J. Contemp. Pediatr. 2017, 4, 1577. [Google Scholar] [CrossRef]
- Akomo, P.; Bahwere, P.; Murakami, H.; Banda, C.; Maganga, E.; Kathumba, S.; Sadler, K.; Collins, S. Soya, Maize and Sorghum Ready-to-Use Therapeutic Foods Are More Effective in Correcting Anaemia and Iron Deficiency than the Standard Ready-to-Use Therapeutic Food: Randomized Controlled Trial. BMC Public Health 2019, 19, 806. [Google Scholar] [CrossRef]
- Caminha, C.; Falbo, R.; Grande, K. Serum Retinol Concentrations in Hospitalized Severe Protein-Energy Malnourished Children. J. Trop. Pediatr. 2008, 54, 248–252. [Google Scholar] [CrossRef]
- World Health Organization; World Food Programme; United Nation System Standing Committee on Nutrition; The United Nations Children’s Fund. Community-Based Management of Severe Acute Malnutrition; World Health Organization: Geneva, Switzerland, 2007; pp. 1–8. [Google Scholar]
- Kangas, S.T.; Salpeteur, C.; Nikiema, V.; Talley, L.; Briend, A.; Ritz, C.; Friis, H.; Kaestel, P. Vitamin A and Iron Status of Children before and after Treatment of Uncomplicated Severe Acute Malnutrition. Clin. Nutr. 2020, 39, 3512–3519. [Google Scholar] [CrossRef]
- Hiffler, L.; Adamolekun, B.; Fischer, P.R.; Fattal-Vavleski, A. Thiamine Content of F-75 Therapeutic Milk for Complicated Severe Acute Malnutrition: Time for a Change? Ann. N. Y. Acad. Sci. 2017, 1404, 20–26. [Google Scholar] [CrossRef]
- Sigh, S.; Roos, N.; Chamnan, C.; Laillou, A.; Prak, S.; Wieringa, F.T. Effectiveness of a Locally Produced, Fish-Based Food Product on Weight Gain among Cambodian Children in the Treatment of Acute Malnutrition: A Randomized Controlled Trial. Nutrients 2018, 10, 909. [Google Scholar] [CrossRef]
- Sigh, S.; Roos, N.; Sok, D.; Borg, B.; Chamnan, C.; Laillou, A.; Dijkhuizen, M.A.; Wieringa, F.T. Development and Acceptability of Locally Made Fish-Based, Ready-to-Use Products for the Prevention and Treatment of Malnutrition in Cambodia. Food Nutr. Bull. 2018, 39, 420–434. [Google Scholar] [CrossRef]
- Sigh, S.; Lauritzen, L.; Wieringa, F.T.; Laillou, A.; Chamnan, C.; Angkeabos, N.; Moniboth, D.; Berger, J.; Stark, K.D.; Roos, N. Whole-Blood PUFA and Associations with Markers of Nutritional and Health Status in Acutely Malnourished Children in Cambodia. Public Health Nutr. 2020, 23, 974–986. [Google Scholar] [CrossRef]
- National Nutrition Program. National Interim Guidelines for the Manaagement of Acute Malnutrition; National Nutrition Program, Ministry of Health: Phnom Penh, Cambodia, 2011; pp. 1–77. [Google Scholar]
- Erhardt, J.G.; Estes, J.E.; Pfeiffer, C.M.; Biesalski, H.K.; Craft, N.E. Combined Measurement of Ferritin, Soluble Transferrin Receptor, Retinol Binding Protein, and C-Reactive Protein by an Inexpensive, Sensitive, and Simple Sandwich Enzyme-Linked Immunosorbent Assay Technique. J. Nutr. 2004, 134, 3127–3132. [Google Scholar] [CrossRef]
- World Health Organization. Haemoglobin Concentrations for the Diagnosis of Anaemia and Assessment of Severity; World Health Organization: Geneva, Switzerland, 2011; pp. 1–6. [Google Scholar]
- Thurnham, D.I.; Mccabe, L.D.; Haldar, S.; Wieringa, F.T.; Northrop-clewes, C.A.; Mccabe, G.P. Adjusting Plasma Ferritin Concentrations to Remove the Effects of Subclinical Inflammation in the Assessment of Iron Deficiency. Am. J. Clin. Nutr. 2010, 92, 546–555. [Google Scholar] [CrossRef]
- Thurnham, D.I.; McCabe, G.P.; Northrop-Clewes, C.A.; Nestel, P. Effects of Subclinical Infection on Plasma Retinol Concentrations and Assessment of Prevalence of Vitamin a Deficiency: Meta-Analysis. Lancet 2003, 362, 2052–2058. [Google Scholar] [CrossRef]
- De Pee, S.; Dary, O. Biochemical Indicators of Vitamin A Deficiency: Serum Retinol and Serum Retinol Binding Protein. J. Nutr. 2002, 132, 2895s–2901s. [Google Scholar] [CrossRef]
- Tanumihardjo, S.A. Vitamin A: Biomarkers of Nutrition for Development 1–4. Am. J. Clin. Nutr. 2011, 94, 658–665. [Google Scholar] [CrossRef]
- Cook, J.D.; Flowers, C.H.; Skikne, B.S. The Quantitative Assessment of Body Iron. Blood 2003, 101, 3359–3364. [Google Scholar] [CrossRef]
- Cichon, B.; Fabiansen, C.; Iuel-Brockdorf, A.S.; Yaméogo, C.W.; Ritz, C.; Christensen, V.B.; Filteau, S.; Briend, A.; Michaelsen, K.F.; Friis, H. Impact of Food Supplements on Hemoglobin, Iron Status, and Inflammation in Children with Moderate Acute Malnutrition: A 2 × 2 × 3 Factorial Randomized Trial in Burkina Faso. Am. J. Clin. Nutr. 2018, 107, 278–286. [Google Scholar] [CrossRef]
- Rosado, J.L.; González, K.E.; Caamaño, M.D.C.; García, O.P.; Preciado, R.; Odio, M. Efficacy of Different Strategies to Treat Anemia in Children: A Randomized Clinical Trial. Nutr. J. 2010, 9, 1–10. [Google Scholar] [CrossRef]
- Savage, D.; Gangaidzo, I.; Lindenbaum, J.; Kiire, C.; Mukiibi, J.M.; Moyo, A.; Gwanzura, C.; Mudenge, B.; Bennie, A.; Sitima, J.; et al. Vitamin B12 Deficiency Is the Primary Cause of Megaloblastic Anaemia in Zimbabwe. Br. J. Haematol. 1994, 86, 844–850. [Google Scholar] [CrossRef]
- Chaparro, C.M.; Suchdev, P.S. Anemia Epidemiology, Pathophysiology, and Etiology in Low- and Middle-Income Countries. Ann. N Y Acad. Sci. 2019, 1450, 15–31. [Google Scholar] [CrossRef]
- Fishman, S.M.; Christian, P.; West, K.P. The Role of Vitamins in the Prevention and Control of Anaemia. Public Health Nutr. 2000, 3, 125–150. [Google Scholar] [CrossRef] [PubMed]
- Tangpricha, E.M.S. and V. Vitamin D and Anemia: Insights into an Emerging Association. Curr. Opin. Endocrinol. Diabetes Obes. 2015, 22, 432–438. [Google Scholar] [CrossRef]
- Crane, R.J.; Jones, K.D.J.; Trust, K.-W.; Programme, R.; Kilifi, K.; Berkley, J.A. Environmental Enteric Dysfunction: An Overview. Food Nutr. Bull. 2015, 36, S76–S87. [Google Scholar] [CrossRef] [PubMed]
- Cowardin, C.A.; Syed, S.; Iqbal, N.; Jamil, Z.; Sadiq, K.; Iqbal, J.; Ali, S.A.; Moore, S.R. Environmental Enteric Dysfunction: Gut and Microbiota Adaptation in Pregnancy and Infancy. Nat. Rev. Gastroenterol. Hepatol. 2022. [Google Scholar] [CrossRef]
- Tickell, K.D.; Atlas, H.E.; Walson, J.L. Environmental Enteric Dysfunction: A Review of Potential Mechanisms, Consequences and Management Strategies. BMC Med. 2019, 17, 181. [Google Scholar] [CrossRef]
- Gilmartin, A.A.; Petri, W.A. Exploring the Role of Environmental Enteropathy in Malnutrition, Infant Development and Oral Vaccine Response. Philos. Trans. R. Soc. B Biol. Sci. 2015, 370, 20140143. [Google Scholar] [CrossRef]
- Budge, S.; Parker, A.H.; Hutchings, P.T.; Garbutt, C. Environmental Enteric Dysfunction and Child Stunting. Nutr. Rev. 2019, 77, 240–253. [Google Scholar] [CrossRef]
- Donangelo, C.M.; Woodhouse, L.R.; Mertz, S.D.; Viteri, F.E.; King, J.C. Human Nutrition and Metabolism Supplemental Zinc Lowers Measures of Iron Status in Young Women with Low Iron Reserves. J Nutr. 2002, 132, 1860–1864. [Google Scholar] [CrossRef]
- Whittae, P. Iron and Zinc interaction in humans. Am. J. Clin. Nutr. 1998, 68, 442s–446s. [Google Scholar]
- Solomons, N.W. Competitive Interaction of Iron and Zinc in the Diet: Consequences for Human Nutrition. Amr. Inst. Nutr. 1986, 116, 927–935. [Google Scholar] [CrossRef]
- Wieringa, F.T.; Dijkhuizen, M.A.; West, C.E. Iron and Zinc Interactions. Letter to Editor. Am. J. Clin. Nutr. 2004, 80, 787–788. [Google Scholar] [CrossRef]
- Lönnerdal, B. Excess Iron Intake as a Factor in Growth, Infections, and Development of Infants and Young Children. Am. J. Clin. Nutr. 2017, 106, 1681–1688. [Google Scholar] [CrossRef]
- Tanumihardjo, S.A.; Russell, R.M.; Stephensen, C.B.; Gannon, B.M.; Craft, N.E.; Haskell, M.J.; Lietz, G.; Schulze, K.; Raiten, D.J. Biomarkers of Nutrition for Development (BOND)-Iron Review. J. Nutr. 2016, 148, 1001S–1067S. [Google Scholar] [CrossRef]
- Moustiés, C.; Bourlieu-Lacanal, C.; Hemery, Y.M.; Bareá, B.; Villeneuve, P.; Servent, A.; Alter, P.; Lebrun, M.; Laillou, A.; Wieringa, F.T.; et al. Nutritional Quality of Ready-to-Use Therapeutic Foods: Focus on Lipid Composition and Vitamin Content. OCL 2022, 29, 13. [Google Scholar] [CrossRef]


{kind=link}
| Product Type | Standard RUTF | Local RUTF | UN Requirements |
|---|---|---|---|
| Energy (Kcal) | 526 | 506 | 520–550 |
| Vitamin A (mg) | 0.9 | 0.8 | 0.8–1.1 |
| Vitamin D (µg) | 18 | 11.7 | 15–20 |
| Vitamin E (mg) | 27 | 13.3 | ≥20 |
| Vitamin K (µg) | 21 | 17.4 | 15–30 |
| Thiamine (vitamin B1) (mg) | 0.5 | 0.4 | ≥0.5 |
| Riboflavin (vitamin B2) (mg) | 1.8 | 1.1 | ≥1.6 |
| Vitamin C (mg) | 54 | 39.3 | ≥50 |
| Vitamin B6 (mg) | 0.7 | 0.5 | ≥0.6 |
| Cobalamin (vitamin B12) (µg) | 1.6 | 1.1 | ≥1.6 |
| Folic acid (µg) | 225 | 249 | ≥200 |
| Niacin (mg) | 5.8 | 4.1 | ≥5 |
| Pantothenic acid (mg) | 3 | 2.7 | ≥3 |
| Biotin (vitamin B7) (µg) | 70 | 94.5 | ≥60 |
| Calcium (mg) | 470 | 219 | 300–600 |
| Sodium (mg) | <290 | 8.26 | ≤290 |
| Potassium (mg) | 1100 | 773 | 1100–1400 |
| Phosphorus (mg) | 470 | 297 | 300–600 |
| Magnesium (mg) | 110 | 88 | 80–140 |
| Iron (mg) | 10 | 5.8 | 10–14 |
| Zinc (mg) | 12 | 7.6 | 11–14 |
| Copper (mg) | 1.5 | 1.1 | 1.4–1.8 |
| Selenium (µg) | 25 | 20.5 | 20–40 |
| Iodine (µg) | 110 | 79.0 | 70–140 |
| Weight (kg) | Standard RUTF | Local RUTF | ||||||
|---|---|---|---|---|---|---|---|---|
| RUTF Quantity/Day (bar) | RUTF Quantity/Day (gram) | Iron Daily RUTF Dose (mg) | Vitamin A Daily RUTF Dose (mg) | RUTF Quantity/Day (Wafer) | RUTF Quantity/Day (gram) | Iron Daily RUTF Dose (mg) | Vitamin A Daily RUTF Dose (mg) | |
| 3.0–3.4 | 2 | ~114 | 11.4 | 1.03 | 17 | ~170 | 9.8 | 1.3 |
| 3.5–4.9 | 2.5 | ~142.5 | 14.3 | 1.3 | 20 | ~200 | 11.5 | 1.5 |
| 5.0–6.9 | 4 | ~228 | 22.8 | 2.1 | 27 | ~270 | 15.5 | 2.1 |
| 7.0–9.9 | 5 | ~285 | 28.5 | 2.6 | 40 | ~400 | 23.0 | 3.1 |
| 10.0–14.0 | 6 | ~342 | 34.2 | 3.1 | 53 | ~530 | 30.4 | 4.1 |
| Standard RUTF (n = 58) | Local RUTF (n = 56) | All Children (n = 114) | |
|---|---|---|---|
| Socio-demographic parameters | |||
| Age, months | 20.5 (12.6) | 22.6 (14.7) | 21.5 (13.6) |
| Gender | |||
| Female, % (n) | 36.2 (21) | 44.6 (25) | 40.4 (46) |
| Male, % (n) | 63.9 (37) | 55.4 (31) | 59.6 (68) |
| Anthropometrics | |||
| Weight, kg | 7.3 9 (1.6) | 7.7 (1.9) | 7.51 (1.8) |
| Height, cm | 75.1 (9.4) | 77.1 (10.2) | 76.1 (9.8) |
| MUAC, mm | 11.8 (0.9) | 11.9 (0.7) | 11.9 (0.8) |
| Weight-for-height, z-score | −3.1 (0.7) | −3.0 9 (0.5) | −3.0 (0.6) |
| Weight-for-age, z-score | −3.4 (0.9) | −3.3 (0.8) | −3.3 (0.8) |
| Height-for-age, z-score | −2.4 (1;3) | −2.2 (1.5) | −2.3 (1.4) |
| Anaemia | |||
| Haemoglobin, g/dl | 10.7 (1.7) | 10.8 (1.3) | 10.8 (1.5) |
| Anaemia, % (n) 1,* | 62.3 (33) | 51.0 (25) | 56.9 (58) |
| Haemoglobinopathy ** | |||
| Hb normal, % (n) | 58.2 (32) | 71.4 (35) | 64.4 (67) |
| Hb disorders, % (n) | 42.8 (23) | 28.6 (14) | 35.6 (37) |
| HbE-Heterozygote, % (n) | 27.3 (15) | 14.3 (7) | 21.2 (22) |
| HbE-Heterozygote/β-thalassemia, % (n) | 3.6 (2) | 4.1 (2) | 3.9 (4) |
| HbE-Homozygote, % (n) | 5.5 (3) | 4.1 (1) | 4.8 (5) |
| β-thalassemia major, % (n) | 1.8 (1) | 0.0 (0) | 1.0 (1) |
| α-thalassemia, % (n) | 0.0 (0) | 2.0 (1) | 1.0 (1) |
| α-thalassemia/Harbour spring, % (n) | 0.0 (0) | 2.0 (1) | 1.0 (1) |
| Hb-Other, % (n) | 3.6 (2) | 2.0 (1) | 3.0 (3) |
| Iron status * | |||
| Ferritin, µg/L | 40.3 (30.0) | 41.4 (28.1) | 40.8 (28.9) |
| sTfR, mg/L | 10.2 (7.4) | 10.1 (9.0) | 10.1 (8.2) |
| BI, mg/kg | 3.5 (4.6) | 4.1. (3.8) | 3.8 (4.2) |
| Iron deficiency, % (n) | 19.3 (11) | 5.7 (3) | 12.7 (14) |
| Low BI, % (n) | 17.5 (10) | 11.3 (6) | 14.5 (16) |
| Vitamin A status * | |||
| RBP, µmol/L | 1.2 (0.5) | 1.4 (0.6) | 1.3 (0.6) |
| Marginal vitamin A status, % (n) | 38.6 (22) | 24.5 (13) | 31.8 (35) |
| Vitamin A deficiency, % (n) | 7 (4) | 3.8 (2) | 5.5 (6) |
| Inflammation status * | |||
| CRP, mg/L | 4.0 (10.8) | 3.1 (5.4) | 3.6 (8.1) |
| CRP, >5 mg/L, % (n) | 12.3 (7) | 18.9 (10) | 15.5 (17) |
| AGP, g/L | 1.1 (0.9) | 1.0 (0.6) | 1.1 (0.8) |
| AGP, >1 g/L, % (n) | 38.6 (22) | 39.6 (21) | 39.1 (43) |
| 6–59-Month-Old Children Admission Mean Age of 21.5 Months | |||||
|---|---|---|---|---|---|
| Biomarker | Admission (n = 110) | Discharge (n = 75) | p-Value 1 | ||
| Mean | SD | Mean | SD | ||
| Haemoglobin, g/dl | 10.8 | 1.5 | 11.0 | 1.6 | 0.27 |
| Ferritin, µg/L | 40.8 | 28.9 | 37.0 | 23.6 | 0.74 |
| sTfR, mg/L | 10.1 | 8.2 | 9.8 | 8.6 | 0.46 |
| BI, mg/kg | 3.8 | 4.2 | 3.6 | 3.8 | 0.90 |
| RBP, µmol/L | 1.3 | 0.6 | 1.2 | 0.6 | 0.36 |
| CRP, mg/L | 3.6 | 8.6 | 2.6 | 5.7 | 0.39 |
| AGP, g/L | 0.96 | 0.69 | 0.79 | 0.57 | 0.08 |
| Iron deficiency, % | 12.5 | 9.6 | 1.00 | ||
| Low BI, % | 14.5 | 16.4 | 0.73 | ||
| Marginal vitamin A, % | 31.8 | 32.9 | 0.65 | ||
| Vitamin A deficiency, % | 5.5 | 2.7 | 1.00 | ||
| Anaemia, % | 56.9 | 52.0 | 0.55 | ||
| 6–59-Month-Old Children Admission Mean Age of 19.7 Months | |||||
|---|---|---|---|---|---|
| Biomarker | Admission (n = 31) | Discharge (n = 31) | p-Value 1 | ||
| Mean | SD | Mean | SD | ||
| Haemoglobin, g/dl | 10.7 | 1.3 | 10.9 | 1.2 | 0.25 |
| Ferritin, µg/L | 32.0 | 27.4 | 33.5 | 19.9 | 0.75 |
| sTfR, mg/L | 12.2 | 10.7 | 10.1 | 8.8 | 0.16 |
| BI, mg/kg | 2.3 | 5.0 | 3.3 | 4.1 | 0.19 |
| RBP, µmol/L | 1.24 | 0.44 | 1.33 | 0.77 | 0.55 |
| CRP, mg/L | 4.3 | 10.7 | 3.5 | 7.9 | 0.74 |
| AGP, g/L | 1.0 | 0.74 | 0.9 | 0.69 | 0.69 |
| Iron deficiency, % | 19.4 | 12.9 | 0.63 | ||
| Low BI, % | 22.6 | 19.4 | 1.00 | ||
| Marginal vitamin A, % | 32.3 | 22.5 | 0.51 | ||
| Vitamin A deficiency, % | 6.4 | 3.2 | 1.00 | ||
| Anaemia, % | 56.7 | 54.8 | 1.00 | ||
| Biomarker | Standard RUTF (n = 36) | Local RUTF (n = 33) | Difference between Treatments (Compared to Control) | ||||
|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Estimated Difference | SE | p-Value | |
| Haemoglobin, g/dl | 11.4 | 1.8 | 10.5 | 1.1 | −0.58 | 0.35 | 0.10 |
| Ferritin, µg/L | 36.5 | 24.1 | 37.2 | 24.7 | −0.20 | 5.4 | 0.98 |
| sTfR, mg/L | 9.7 | 7.2 | 10.3 | 10.4 | −0.04 | 2.1 | 0.99 |
| BI, mg/kg | 3.4 | 4.0 | 3.6 | 3.9 | +0.49 | 0.93 | 0.60 |
| RBP, µmol/L | 1.23 | 0.75 | 1.28 | 0.37 | +0.06 | 0.11 | 0.58 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sigh, S.; Roos, N.; Chhoun, C.; Laillou, A.; Wieringa, F.T. Ready-to-Use Therapeutic Foods Fail to Improve Vitamin A and Iron Status Meaningfully during Treatment for Severe Acute Malnutrition in 6–59-Month-old Cambodian Children. Nutrients 2023, 15, 905. https://doi.org/10.3390/nu15040905
Sigh S, Roos N, Chhoun C, Laillou A, Wieringa FT. Ready-to-Use Therapeutic Foods Fail to Improve Vitamin A and Iron Status Meaningfully during Treatment for Severe Acute Malnutrition in 6–59-Month-old Cambodian Children. Nutrients. 2023; 15(4):905. https://doi.org/10.3390/nu15040905
Chicago/Turabian StyleSigh, Sanne, Nanna Roos, Chamnan Chhoun, Arnaud Laillou, and Frank T. Wieringa. 2023. "Ready-to-Use Therapeutic Foods Fail to Improve Vitamin A and Iron Status Meaningfully during Treatment for Severe Acute Malnutrition in 6–59-Month-old Cambodian Children" Nutrients 15, no. 4: 905. https://doi.org/10.3390/nu15040905
APA StyleSigh, S., Roos, N., Chhoun, C., Laillou, A., & Wieringa, F. T. (2023). Ready-to-Use Therapeutic Foods Fail to Improve Vitamin A and Iron Status Meaningfully during Treatment for Severe Acute Malnutrition in 6–59-Month-old Cambodian Children. Nutrients, 15(4), 905. https://doi.org/10.3390/nu15040905