
Limited Effect of Dehydrating via Active vs. Passive Heat Stress on Plasma Volume or Osmolality, Relative to the Effect of These Stressors per Se
 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Approval
2.2. Participants
2.3. Experimental Design
2.4. Pre-Testing
2.5. Experimental Protocol
2.6. Measurements
2.7. Calculations
2.8. Statistical Analysis
3. Results
3.1. Compliance
3.2. Independent Measures (Baselines, ∆BM, Duration, Environmental Conditions)
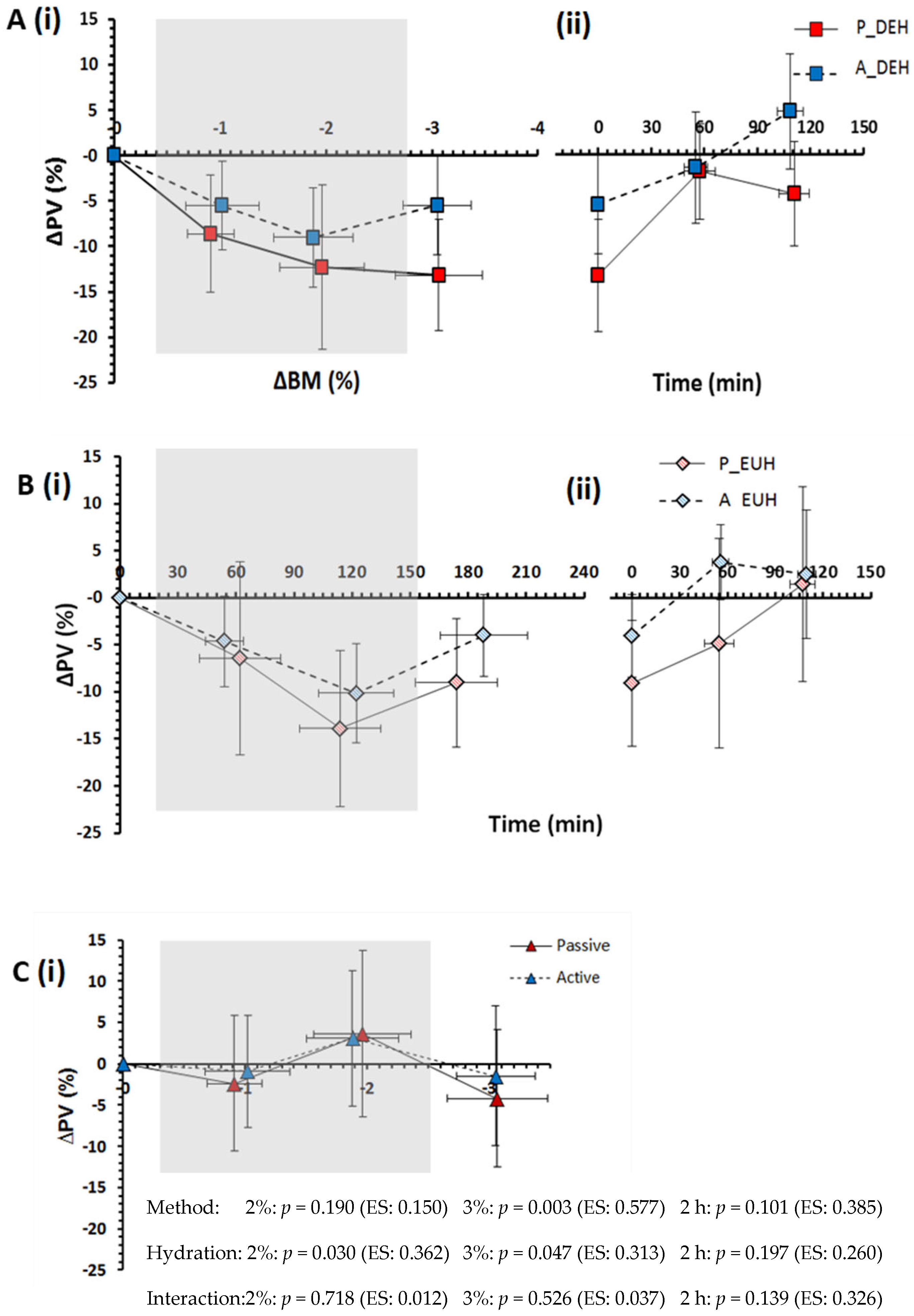
3.3. Plasma Volume and Plasma Osmolality
3.4. Substrate Oxidation and Mass Exchanges
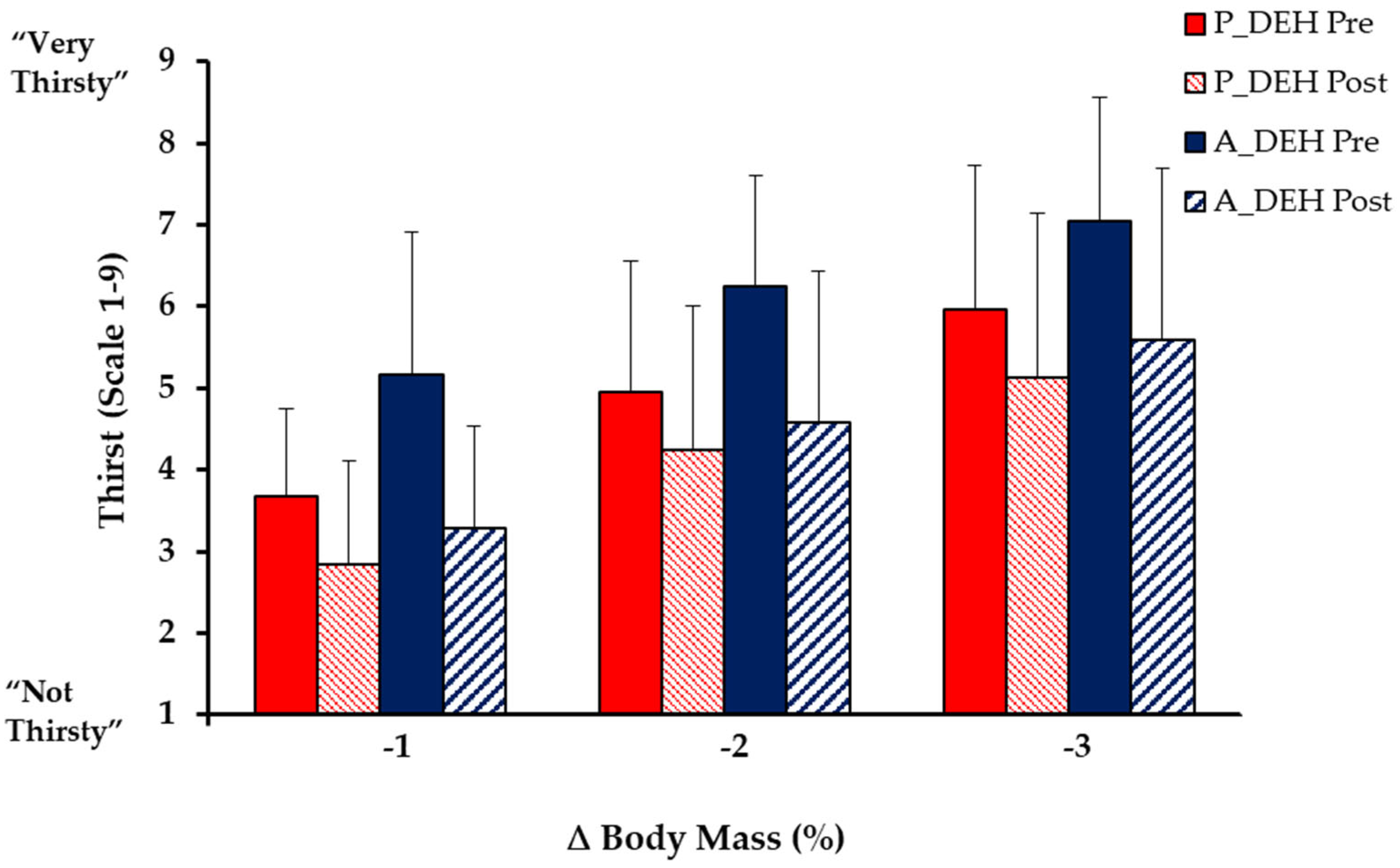
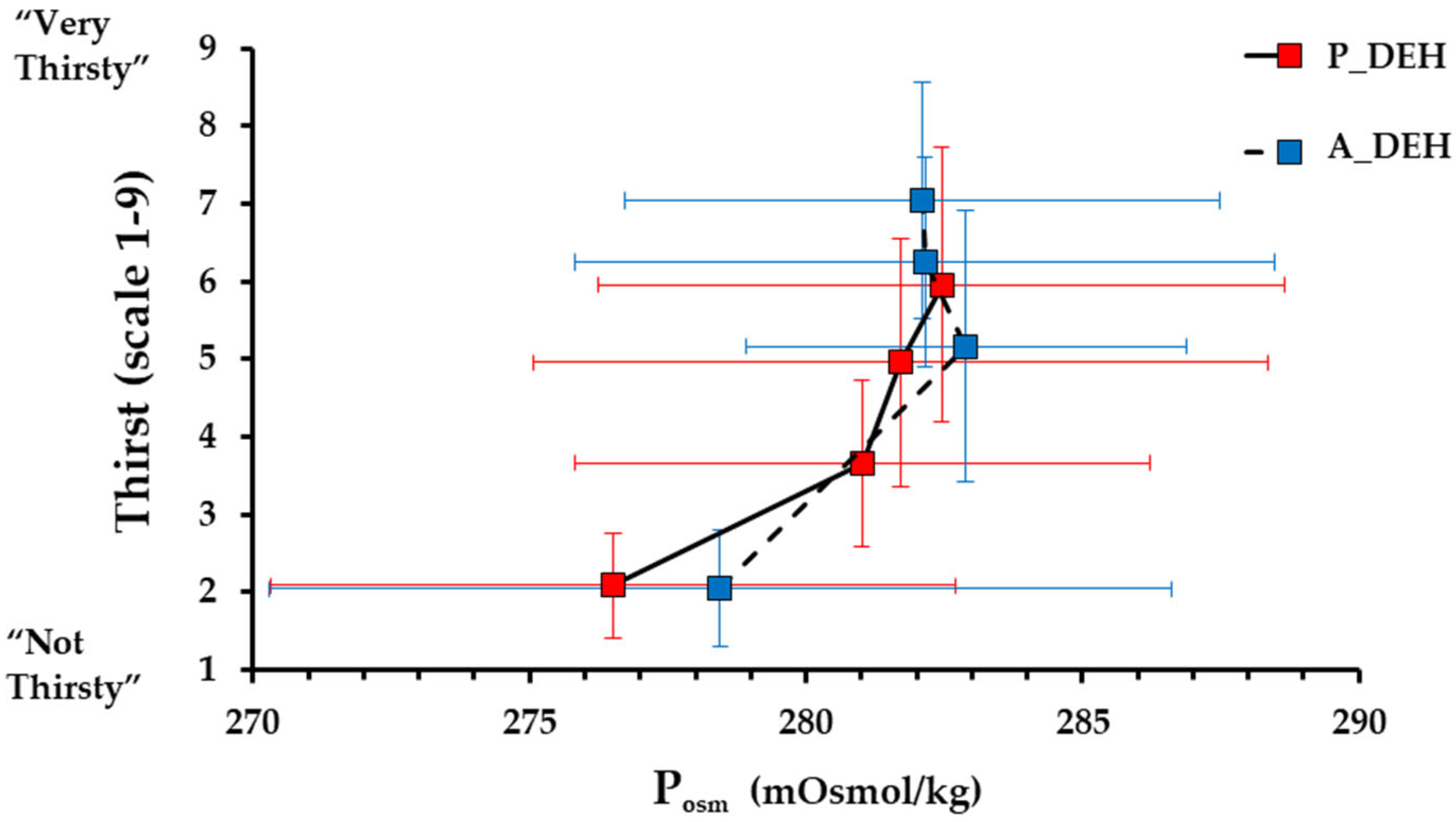
3.5. Thirst and Oral Sensations
3.6. Heart Rate, Blood Pressure and Thermal Responses
3.7. Urine Indices
3.8. Rehydration Fluid Balance
3.9. Summary of Key Findings for the Four Main Questions
3.10. Subsequent 24-h Fluid Balances and Nutrient Intakes
4. Discussion
4.1. Dehydration
4.2. Rehydration
4.3. Limitations
4.4. Perspectives
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cannon, W.B. Organization for physiological homeostasis. Physiol. Rev. 1918, 9, 399–432. [Google Scholar] [CrossRef]
- Cheuvront, S.N.; Kenefick, R.W. Dehydration: Physiology, assessment, and performance effects. Compr. Physiol. 2014, 4, 257–285. [Google Scholar] [PubMed]
- Shirreffs, S.M. Markers of hydration status. J. Sport. Med. Phys. Fit. 2000, 40, 80–84. [Google Scholar] [CrossRef] [PubMed]
- Colt, E.W.; Wang, J.; Pierson, R.N., Jr. Effect on body water of running 10 miles. J. Appl. Physiol. Respir. Environ. Exerc. Physiol. 1978, 45, 999–1001. [Google Scholar] [CrossRef]
- Tam, N.; Nolte, H.W.; Noakes, T.D. Changes in total body water content during running races of 21.1 km and 56 km in athletes drinking ad libitum. Clin. J. Sport Med. 2011, 21, 218–225. [Google Scholar] [CrossRef]
- Thomas, D.T.; Erdman, K.A.; Burke, L.M. American College of Sports Medicine Joint Position Statement. Nutrition and Athletic Performance. Med. Sci. Sport. Exerc. 2016, 48, 543–568. [Google Scholar]
- Sawka, M.N.; Burke, L.M.; Eichner, E.R.; Maughan, R.J.; Montain, S.J.; Stachenfeld, N.S. American College of Sports Medicine position stand. Exercise and fluid replacement. Med. Sci. Sport. Exerc. 2007, 39, 377–390. [Google Scholar]
- Cotter, J.D.; Thornton, S.N.; Lee, J.K.; Laursen, P.B. Are we being drowned in hydration advice? Thirsty for more? Extrem. Physiol. Med. 2014, 3, 18. [Google Scholar] [CrossRef]
- Wall, B.A.; Watson, G.; Peiffer, J.J.; Abbiss, C.R.; Siegel, R.; Laursen, P.B. Current hydration guidelines are erroneous: Dehydration does not impair exercise performance in the heat. Br. J. Sport. Med. 2013, 49, 1077–1083. [Google Scholar] [CrossRef]
- Cheuvront, S.N.; Kenefick, R.W.; Charkoudian, N.; Sawka, M.N. Physiologic basis for understanding quantitative dehydration assessment. Am. J. Clin. Nutr. 2013, 97, 455–462. [Google Scholar] [CrossRef]
- Caldwell, J.E.; Ahonen, E.; Nousiainen, U. Differential effects of sauna-, diuretic-, and exercise-induced hypohydration. J. Appl. Physiol. 1984, 57, 1018–1023. [Google Scholar] [CrossRef] [PubMed]
- Kozlowski, S.; Saltin, B. Effect of Sweat Loss on Body Fluids. J. Appl. Physiol. 1964, 19, 1119–1124. [Google Scholar] [CrossRef]
- Jimenez, C.; Melin, B.; Koulmann, N.; Allevard, A.M.; Launay, J.C.; Savourey, G. Plasma volume changes during and after acute variations of body hydration level in humans. Eur. J. Appl. Physiol. Occup. Physiol. 1999, 80, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Maw, G.J.; Mackenzie, I.L.; Taylor, N.A. Human body-fluid distribution during exercise in hot, temperate and cool environments. Acta Physiol. Scand. 1998, 163, 297–304. [Google Scholar] [CrossRef] [PubMed]
- Myhre, L.G.; Hartung, G.H.; Nunneley, S.A.; Tucker, D.M. Plasma volume changes in middle-aged male and female subjects during marathon running. J. Appl. Physiol. 1985, 59, 559–563. [Google Scholar] [CrossRef] [PubMed]
- Convertino, V.A.; Keil, L.C.; Bernauer, E.M.; Greenleaf, J.E. Plasma volume, osmolality, vasopressin, and renin activity during graded exercise in man. J. Appl. Physiol. Respir. Environ. Exerc. Physiol. 1981, 50, 123–128. [Google Scholar] [CrossRef]
- Hew-Butler, T.; Jordaan, E.; Stuempfle, K.J.; Speedy, D.B.; Siegel, A.J.; Noakes, T.D.; Soldin, S.J.; Verbalis, J.G. Osmotic and nonosmotic regulation of arginine vasopressin during prolonged endurance exercise. J. Clin. Endocrinol. Metab. 2008, 93, 2072–2078. [Google Scholar] [CrossRef]
- Maughan, R.J.; Shirreffs, S.M.; Leiper, J.B. Errors in the estimation of hydration status from changes in body mass. J. Sport. Sci. 2007, 25, 797–804. [Google Scholar] [CrossRef]
- Fernandez-Elias, V.E.; Hamouti, N.; Ortega, J.F.; Mora-Rodriguez, R. Hyperthermia, but not muscle water deficit, increases glycogen use during intense exercise. Scand. J. Med. Sci. Sport. 2015, 25 (Suppl. 1), 126–134. [Google Scholar] [CrossRef]
- Olsson, K.E.; Saltin, B. Variation in total body water with muscle glycogen changes in man. Acta Physiol. Scand. 1970, 80, 11–18. [Google Scholar] [CrossRef]
- King, R.; Jones, B.; O’Hara, J.P. The availability of water associated with glycogen during dehydration: A reservoir or raindrop? Eur. J. Appl. Physiol. 2018, 118, 283–290. [Google Scholar] [CrossRef]
- Costill, D.L.; Fink, W.J. Plasma volume changes following exercise and thermal dehydration. J. Appl. Physiol. 1974, 37, 521–525. [Google Scholar] [CrossRef] [PubMed]
- Montain, S.J.; Coyle, E.F. Influence of graded dehydration on hyperthermia and cardiovascular drift during exercise. J. Appl. Physiol. 1992, 73, 1340–1350. [Google Scholar] [CrossRef] [PubMed]
- Harrison, M.H. Effects of thermal stress and exercise on blood volume in humans. Physiol. Rev. 1985, 65, 149–209. [Google Scholar] [CrossRef] [PubMed]
- Sawka, M.N.; Montain, S.J. Fluid and electrolyte supplementation for exercise heat stress. Am. J. Clin. Nutr. 2000, 72, 564S–572S. [Google Scholar] [CrossRef]
- Valtin, H. “Drink at least eight glasses of water a day.” Really? Is there scientific evidence for “8 × 8”? Am. J. Physiol. Regul. Integr. Comp. Physiol. 2002, 283, R993–R1004. [Google Scholar] [CrossRef] [PubMed]
- Hew-Butler, T.; Verbalis, J.G.; Noakes, T.D. Updated fluid recommendation: Position statement from the International Marathon Medical Directors Association (IMMDA). Clin. J. Sport Med. 2006, 16, 283–292. [Google Scholar] [CrossRef]
- Ichinose, T.; Okazaki, K.; Masuki, S.; Mitono, H.; Chen, M.; Endoh, H.; Nose, H. Ten-day endurance training attenuates the hyperosmotic suppression of cutaneous vasodilation during exercise but not sweating. J. Appl. Physiol. 1985 2005, 99, 237–243. [Google Scholar] [CrossRef]
- Phillips, P.A.; Rolls, B.J.; Ledingham, J.G.; Morton, J.J. Body fluid changes, thirst and drinking in man during free access to water. Physiol. Behav. 1984, 33, 357–363. [Google Scholar] [CrossRef]
- Rehrer, N.J.; Burke, L.M. Sweat losses during various sports. Aust. J. Nutr. Diet. 1996, 53, S13. [Google Scholar]
- Akerman, A.P.; Tipton, M.; Minson, C.T.; Cotter, J.D. Heat stress and dehydration in adapting for performance: Good, bad, both, or neither? Temperature 2016, 3, 412–436. [Google Scholar] [CrossRef]
- Stachenfeld, N.S. Sex hormone effects on body fluid regulation. Exerc. Sport Sci. Rev. 2008, 36, 152–159. [Google Scholar] [CrossRef]
- Refinetti, R.; Menaker, M. The circadian rhythm of body temperature. Physiol. Behav. 1992, 51, 613–637. [Google Scholar] [CrossRef]
- Hagan, R.D.; Diaz, F.J.; Horvath, S.M. Plasma volume changes with movement to supine and standing positions. J. Appl. Physiol. Respir. Environ. Exerc. Physiol. 1978, 45, 414–417. [Google Scholar] [CrossRef]
- Ramanathan, N.L. A new weighting system for mean surface temperature of the human body. J. Appl. Physiol. 1964, 19, 531–533. [Google Scholar] [CrossRef]
- Riebe, D.; Maresh, C.M.; Armstrong, L.E.; Kenefick, R.W.; Castellani, J.W.; Echegaray, M.E.; Clark, B.A.; Camaione, D.N. Effects of oral and intravenous rehydration on ratings of perceived exertion and thirst. Med. Sci. Sport. Exerc. 1997, 29, 117–124. [Google Scholar] [CrossRef]
- Engell, D.B.; Maller, O.; Sawka, M.N.; Francesconi, R.N.; Drolet, L.; Young, A.J. Thirst and fluid intake following graded hypohydration levels in humans. Physiol. Behav. 1987, 40, 229–236. [Google Scholar] [CrossRef] [PubMed]
- Weir, J.d.V. New methods for calculating metabolic rate with special reference to protein metabolism. J. Physiol. 1949, 109, 1. [Google Scholar] [CrossRef] [PubMed]
- Rogers, G.; Goodman, C.; Rosen, C. Water budget during ultra-endurance exercise. Med. Sci. Sport. Exerc. 1997, 29, 1477–1481. [Google Scholar] [CrossRef]
- Mitchell, J.W.; Nadel, E.R.; Stolwijk, J.A. Respiratory weight losses during exercise. J. Appl. Physiol. 1972, 32, 474–476. [Google Scholar] [CrossRef] [PubMed]
- King, R.F.G.J.; Cooke, C.; Carroll, S.; O’Hara, J. Estimating changes in hydration status from changes in body mass: Considerations regarding metabolic water and glycogen storage. J. Sport. Sci. 2008, 26, 1361–1363. [Google Scholar] [CrossRef]
- Dill, D.B.; Costill, D.L. Calculation of percentage changes in volumes of blood, plasma, and red cells in dehydration. J. Appl. Phsyiol. 1974, 37, 247–248. [Google Scholar] [CrossRef] [PubMed]
- Strauss, M.B.; Davis, R.K.; Rosenbaum, J.D.; Rossmeisl, E.C. Water diuresis produced during recumbency by the intravenous infusion of isotonic saline solution. J. Clin. Investig. 1951, 30, 862–868. [Google Scholar] [CrossRef]
- Hinghofer-Szalkay, H.; Harrison, M.H.; Greenleaf, J.E. Early fluid and protein shifts in men during water immersion. Eur. J. Appl. Physiol. Occup. Physiol. 1987, 56, 673–678. [Google Scholar] [CrossRef]
- Li, T.L.; Gleeson, M. The effect of single and repeated bouts of prolonged cycling and circadian variation on saliva flow rate, immunoglobulin A and alpha-amylase responses. J. Sport. Sci. 2004, 22, 1015–1024. [Google Scholar] [CrossRef] [PubMed]
- Verbalis, J.G. Inhibitory Controls of Drinking: Satiation of Thirst; Springer: London, UK, 1991; pp. 313–334. [Google Scholar]
- Costill, D. Sweating: Its composition and effects on body fluids. Ann. New York Acad. Sci. 1977, 301, 160–174. [Google Scholar] [CrossRef]
- Astrand, P.O.; Saltin, B. Plasma and Red Cell Volume after Prolonged Severe Exercise. J. Appl. Physiol. 1964, 19, 829–832. [Google Scholar] [CrossRef] [PubMed]
- Pastene, J.; Germain, M.; Allevard, A.; Gharib, C.; Lacour, J. Water balance during and after marathon running. Eur. J. Appl. Physiol. O 1996, 73, 49–55. [Google Scholar] [CrossRef]
- Ladell, W.S.S. The Effects of Water and Salt Intake upon the Performance of Men Working in Hot and Humid Environments. J. Physiol. 1955, 127, 11–46. [Google Scholar] [CrossRef]
- Hew-Butler, T.; Collins, M.; Bosch, A.; Sharwood, K.; Wilson, G.; Armstrong, M.; Jennings, C.; Swart, J.; Noakes, T. Maintenance of plasma volume and serum sodium concentration despite body weight loss in Ironman triathletes. Clin. J. Sport Med. 2007, 17, 116–122. [Google Scholar] [CrossRef]
- Benias, P.C.; Wells, R.G.; Sackey-Aboagye, B.; Klavan, H.; Reidy, J.; Buonocore, D.; Miranda, M.; Kornacki, S.; Wayne, M.; Carr-Locke, D.L.; et al. Structure and Distribution of an Unrecognized Interstitium in Human Tissues. Sci. Rep. 2018, 8, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Noakes, T.D. The hyponatremia of exercise. Int. J. Sport Nutr. 1992, 2, 205–228. [Google Scholar] [CrossRef] [PubMed]
- Floyer, M.A.; Morris, D.V. The effect of arginine vasopressin (AVP) on the distribution of fluid in the rat [proceedings]. J. Physiol. 1976, 263, 157P–158P. [Google Scholar] [PubMed]
- Kosunen, K.J.; Pakarinen, A.J. Plasma renin, angiotensin II, and plasma and urinary aldosterone in running exercise. J. Appl. Physiol. 1976, 41, 26–29. [Google Scholar] [CrossRef] [PubMed]
- Kotchen, T.A.; Hartley, L.H.; Rice, T.W.; Mougey, E.H.; Jones, L.G.; Mason, J.W. Renin, norepinephrine, and epinephrine responses to graded exercise. J. Appl. Physiol. 1971, 31, 178–184. [Google Scholar] [CrossRef]
- Melin, B.; Koulmann, N.; Jimenez, C.; Savourey, G.; Launay, J.C.; Cottet-Emard, J.M.; Pequignot, J.M.; Allevard, A.M.; Gharib, C. Comparison of passive heat or exercise-induced dehydration on renal water and electrolyte excretion: The hormonal involvement. Eur. J. Appl. Physiol. 2001, 85, 250–258. [Google Scholar] [CrossRef]
- Robertson, G.L.; Shelton, R.L.; Athar, S. The osmoregulation of vasopressin. Kidney Int. 1976, 10, 25–37. [Google Scholar] [CrossRef]
- Brandenberger, G.; Candas, V.; Follenius, M.; Libert, J.; Kahn, J. Vascular fluid shifts and endocrine responses to exercise in the heat. Eur. J. Appl. Physiol. 1986, 55, 123–129. [Google Scholar] [CrossRef]
- Brenner, I.K.; Thomas, S.; Shephard, R.J. Spectral analysis of heart rate variability during heat exposure and repeated exercise. Eur. J. Appl. Physiol. 1997, 76, 145–156. [Google Scholar] [CrossRef]
- Stachenfeld, N.S.; Taylor, H.S. Effects of estrogen and progesterone administration on extracellular fluid. J. Appl. Physiol. 2004, 96, 1011–1018. [Google Scholar] [CrossRef]
- Hellmig, S.; Von Schoning, F.; Gadow, C.; Katsoulis, S.; Hedderich, J.; Folsch, U.R.; Stuber, E. Gastric emptying time of fluids and solids in healthy subjects determined by 13C breath tests: Influence of age, sex and body mass index. J. Gastroenterol. Hepatol. 2006, 21, 1832–1838. [Google Scholar] [CrossRef] [PubMed]
- Rosner, M.H.; Kirven, J. Exercise-associated hyponatremia. Clin. J. Am. Soc. Nephrol. 2007, 2, 151–161. [Google Scholar] [CrossRef] [PubMed]
- Heaps, C.L.; Gonzalezalonso, J.; Coyle, E.F. Hypohydration Causes Cardiovascular Drift without Reducing Blood-Volume. Int. J. Sport. Med. 1994, 15, 74–79. [Google Scholar] [CrossRef] [PubMed]
- Poortmans, J.R. Exercise and renal function. Exerc. Sport Sci. Rev. 1977, 5, 255–294. [Google Scholar] [CrossRef] [PubMed]
- Montain, S.J.; Sawka, M.N.; Latzka, W.A.; Valeri, C.R. Thermal and cardiovascular strain from hypohydration: Influence of exercise intensity. Int. J. Sport. Med. 1998, 19, 87–91. [Google Scholar] [CrossRef]
- Hamilton, M.T.; Gonzalez-Alonso, J.; Montain, S.J.; Coyle, E.F. Fluid replacement and glucose infusion during exercise prevent cardiovascular drift. J. Appl. Physiol. 1991, 71, 871–877. [Google Scholar] [CrossRef] [PubMed]
- Shaffrath, J.D.; Adams, W.C. Effects of airflow and work load on cardiovascular drift and skin blood flow. J. Appl. Physiol. Respir. Environ. Exerc. Physiol. 1984, 56, 1411–1417. [Google Scholar] [CrossRef]
- Adolph, E.F. (Ed.) Physiology of Man in the Desert; Interscience: New York, NY, USA, 1947. [Google Scholar]
- Greenleaf, J.E.; Sargent, F., II. Voluntary dehydration in man. J. Appl. Physiol. 1965, 20, 719–724. [Google Scholar] [CrossRef] [PubMed]
- Vernon, H.M.; Warner, C.G. The influence of the humidity of the air on capacity for work at high temperatures. J. Hyg. Camb. 1932, 32, 431–463. [Google Scholar] [CrossRef]
- Figaro, M.K.; Mack, G.W. Regulation of fluid intake in dehydrated humans: Role of oropharyngeal stimulation. Am. J. Physiol. Regul. 1997, 272, R1740–R1746. [Google Scholar] [CrossRef]
- Convertino, V.A.; Armstrong, L.E.; Coyle, E.F.; Mack, G.W.; Sawka, M.N.; Senay, L.C., Jr.; Sherman, W.M. American College of Sports Medicine position stand. Exercise and fluid replacement. Med. Sci. Sport. Exerc. 1996, 28, i–vii. [Google Scholar] [CrossRef] [PubMed]
- Vrijens, D.M.; Rehrer, N.J. Sodium-free fluid ingestion decreases plasma sodium during exercise in the heat. J. Appl. Physiol. 1999, 86, 1847–1851. [Google Scholar] [CrossRef] [PubMed]
- Robinson, T.A.; Hawley, J.A.; Palmer, G.S.; Wilson, G.R.; Gray, D.A.; Noakes, T.D.; Dennis, S.C. Water Ingestion Does Not Improve 1-H Cycling Performance in Moderate Ambient-Temperatures. Eur. J. Appl. Physiol. O 1995, 71, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Goulet, E.D.B.; Hoffman, M.D. Impact of Ad Libitum Versus Programmed Drinking on Endurance Performance: A Systematic Review with Meta-Analysis. Sport. Med. 2019, 49, 221–232. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N | Age (y) | Height (cm) | Body Mass (kg) | Body Fat a (%) | O2peakb (mL/min/kg) | |
|---|---|---|---|---|---|---|
| All | 12 | 33.5 ± 11.6 | 172 ± 7 | 74.4 ± 13.4 | 20 ± 7 | 50.7 ± 9.0 |
| Female | 5 | 27.2 ± 8.0 | 167 ± 5 | 66.2 ± 6.0 | 24 ± 6 | 48.4 ± 5.1 |
| Male | 7 | 38.0 ± 12.2 | 176 ± 5 | 80.3 ± 14.5 | 17 ± 7 | 52.6 ± 11.4 |
| Trial | ||||
|---|---|---|---|---|
| Passive Heat DEHhydration | Active Heat DEHydration | Passive Heat EUHydration | Active Heat EUHydration | |
| Total duration (min) | 179 ± 36 | 185 ± 12 | 175 ± 43 | 187 ± 29 |
| Post BM (kg) | 72.6 ± 12.2 | 72.3 ± 14.3 | 74.0 ± 15.1 | 74.6 ± 13.5 |
| Gross ∆BM a (%) | −3.1 ± 0.6 | −3.1 ± 0.3 | −3.1 ± 0.5 | −3.2 ± 0.5 |
| Net ∆BM a (%) | −3.1 ± 0.6 | −3.1 ± 0.3 | −0.1 ± 0.6 | −0.0 ± 0.3 |
| Research Question | Comparison | Findings | |||
|---|---|---|---|---|---|
| ΔPosm | ΔPV | Thirst | Uvol | ||
| 1: Are physiological and psychophysical strains greater when a realistic mild-moderate dehydration is induced via passive, more so than active heat stress, and still in those exposures? | 0 vs. −2% BM in respective stressor (e.g., Figure 2A and Figure 3A) | P ≈ A | P ≈ A | P ≈ A | P ≈ A |
| 2: Are fluid-regulatory responses greater when moderately hypohydrated via passive, more so than active heat stress, and now in a non-stressful environment? | 0 vs. −3% BM, in a matched setting; resting in a temperate environ. (e.g., Figure 2A and Figure 3A) | P ≈ A | P > A | P ≈ A | P ≈ A |
| 3: What are the effects of these stressors per se? (i.e., by comparing with a BM-neutral condition under the same stressor) | Compare effects across hydration states within each form of heat stress. (e.g., Figure 2B,C and Figure 3B,C) | D < P ≈ A | D < P ≈ A | P < A | D > P ≈ A |
| 4: Does rehydration recovery behaviour or efficacy depend on the method of dehydration? | −3% BM vs. 2 h rehydrate | P ≈ A | P ≈ A | P ≈ A | P ≈ A |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Davies, A.; Akerman, A.P.; Rehrer, N.J.; Thornton, S.N.; Cotter, J.D. Limited Effect of Dehydrating via Active vs. Passive Heat Stress on Plasma Volume or Osmolality, Relative to the Effect of These Stressors per Se. Nutrients 2023, 15, 904. https://doi.org/10.3390/nu15040904
Davies A, Akerman AP, Rehrer NJ, Thornton SN, Cotter JD. Limited Effect of Dehydrating via Active vs. Passive Heat Stress on Plasma Volume or Osmolality, Relative to the Effect of These Stressors per Se. Nutrients. 2023; 15(4):904. https://doi.org/10.3390/nu15040904
Chicago/Turabian StyleDavies, Alexandria, Ashley Paul Akerman, Nancy Jane Rehrer, Simon N. Thornton, and James David Cotter. 2023. "Limited Effect of Dehydrating via Active vs. Passive Heat Stress on Plasma Volume or Osmolality, Relative to the Effect of These Stressors per Se" Nutrients 15, no. 4: 904. https://doi.org/10.3390/nu15040904
APA StyleDavies, A., Akerman, A. P., Rehrer, N. J., Thornton, S. N., & Cotter, J. D. (2023). Limited Effect of Dehydrating via Active vs. Passive Heat Stress on Plasma Volume or Osmolality, Relative to the Effect of These Stressors per Se. Nutrients, 15(4), 904. https://doi.org/10.3390/nu15040904