

Unveiling Lived Experiences: Exploring the Health and Lifestyle Effects of COVID-19 on Healthcare Workers


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Measures
2.4. Analytic Strategy
3. Results
3.1. Open-Ended Questions
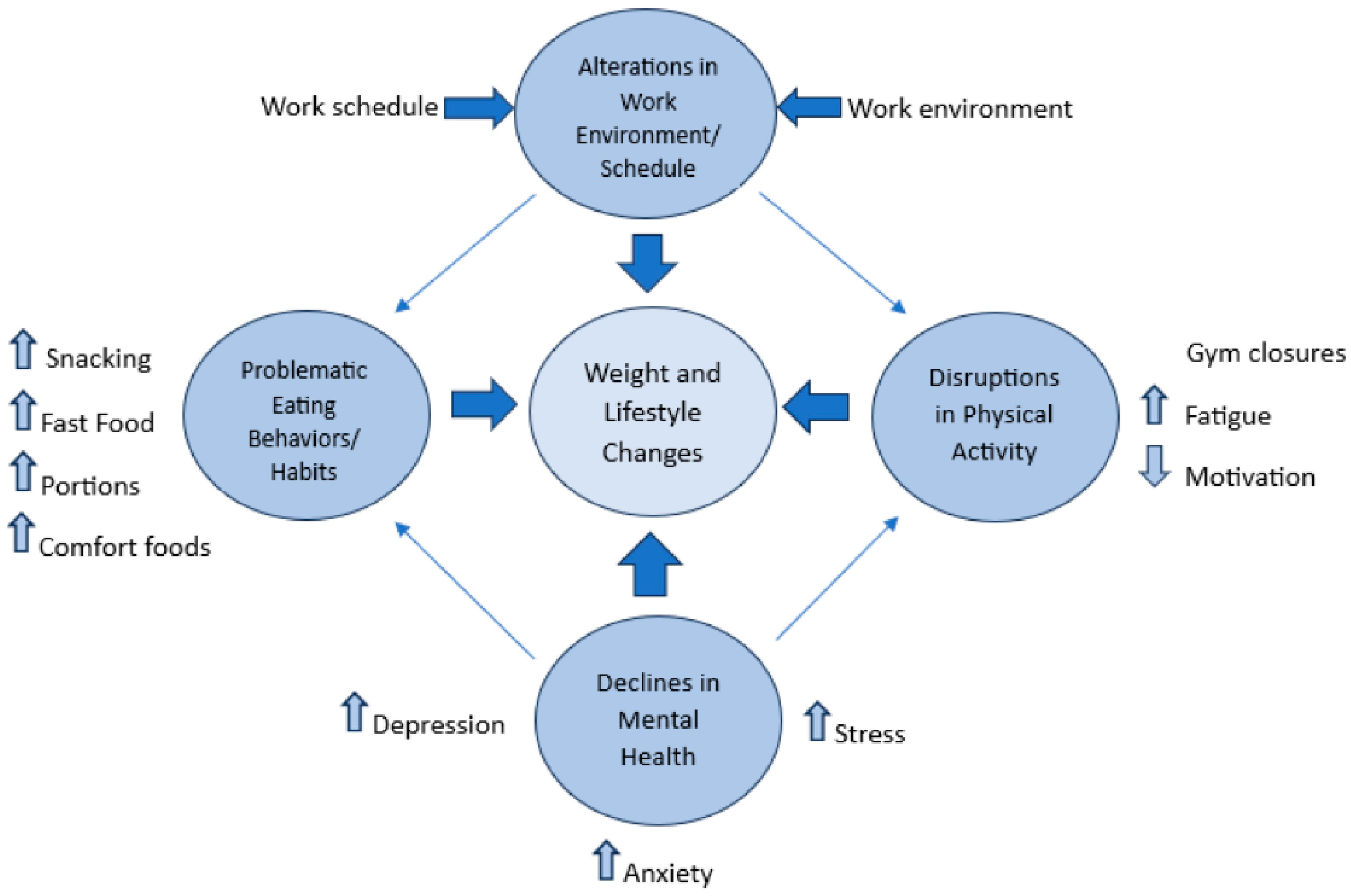
3.2. Primary Themes
3.2.1. Problematic Eating Patterns and Habits
“I was consistently plant-based prior to COVID. Then ice cream and chips became the only way I could tolerate my grief and fear. I recently regained my control over sugar consumption. I still struggle to reduce consumption of salty crunchy snacks.”(M12 participant)
“There was a lot of free food offered to my unit. Also, I stress eat.”(M0 participant)
“At the beginning of the pandemic, my husband and I were ordering out a lot due to work, exhaustion, wanting to help the community, and we were in the process of moving.”(M12 participant)
“At first I was trying to lose weight, binge eating, lots of take out due to social isolation and being bored, rewarding myself, so I gained 10–15 pounds.”(M24 participant)
“Prior to the pandemic, I ate pretty healthy meals and portion sizes were appropriate. Al-though not often, now less of an ability to control eating habits, sometimes overeating or eating larger portions.”(M12 participant)
“I used food for comfort and pleasure because experiencing so little of either due to social isolation of pandemic.”(M0 participant)
3.2.2. Disruptions in Physical Activity
“I ate more junk and gave up completely on exercising mostly due to overall fatigue, physical and emotional and also because I was showering before and after work and did not want to shower a third time during the day.”(M0 participant)
“The gym I attended decided to require everyone to wear masks while they worked out. I could not wear a mask while doing my HIIT/cardio routine and I was “mask-shamed”… I wanted to put my membership on hold, but the gym just canceled my membership instead.”(M12 participant)
“I was working out less… too mentally and physically exhausted.”(M12 participant)
“I was more active before the pandemic, going to the gym. Now I don’t do anything.”(M24 participant)
3.2.3. Declines in Mental Health
“Constant stress distracted me constantly from my goals. Everyday adaptations to what is going on with COVID has had a huge impact on my ability to focus and perform.”(M0 participant)
3.2.4. Alterations in Work Environment or Schedule
“Prior to COVID I ate a great diet. Mostly homecooked meals, fruit, veggies. In the past 6 months I have been working more hours and unpredictable hours and I just ate what is available to eat which is usually not good stuff and I have less time to cook.”(M0 participant)
“I had difficulty staying motivated due to job stress and exhaustion. We were short staffed, working harder and longer hours.”(M12 participant)
3.3. Secondary Themes
3.3.1. Improvements in Physical Activity
“My activity level has varied. Initially slowed due to a fear of going to the gym and closures. Found alternative ways to exercise, some have sustained.”(M12 participant)
“I have more structured meals and a bit more flexibility to go for walks mid-day.”(M12 participant)
3.3.2. Intentional Healthier Lifestyle Habits
“We have been more focused on meal prepping and eating healthier at home. Some weeks are better than others.”(M12 participant)
“Since I stopped exercising, I have snacked more, but I try to keep the snacks healthy, such as carrot sticks, nuts, fruit. I noticed weight gain and I increased my water intake. Instead of cutting my tea with water, I just drink plain water. I am making more salads. If I have a calorie heavy meal one day the next day, I try to have a salad.”(M12 participant)
“There were times during the pandemic that we had increased take out. That has decreased to about 1 time per week. Now that our daughter is starting to try foods, we have a lot more fruits and vegetables in the home. That is helping keep us healthier too.”(M24 participant)
“Before I drank a soda daily and would have a bite size piece of candy. But since I have gained weight, I cut out soda and candy.”(M24 participant)
3.3.3. Changes in Sleep/Fatigue
“(I think my weight changed) because of the stress and working too much and not enough sleeping due to working both day and night.”(M0 participant)
“Lack of sleep and lack of time caused me to eat out frequently and eat far less healthy than if I cooked myself.”(M12 participant)
3.3.4. Other
“I had a concussion during the first part of the pandemic and after PT I never really resumed regular exercise.”(M12 participant)
“I lost 25 pounds after the first COVID diagnosis. Loss of taste and smell for a few months really curbed appetite and intake. But all the weight returned over the last 20 months and my second bout with COVID did not result in any loss of senses.”(M24 participant)
3.4. Final Thoughts Related to Changes in Lifestyle Habits
4. Discussion
4.1. Next Steps
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Carroll, N.; Sadowski, A.; Laila, A.; Hruska, J.; Nixon, M.; Ma, D.W.L.; Haines, J. The Impact of COVID-19 on Health Behavior, Stress, Financial and Food Security among Middle to High Income Canadian Families with Young Children. Nutrients 2020, 12, 2352. [Google Scholar] [CrossRef]
- Di Renzo, L.; Gualtieri, P.; Pivari, F.; Soldati, L.; Attina, A.; Cinelli, G.; Leggeri, C.; Caparello, G.; Barrea, L.; Scerbo, F.; et al. Eating habits and lifestyle changes during COVID-19 lockdown: An Italian survey. J. Transl. Med. 2020, 8, 229. [Google Scholar] [CrossRef]
- Oni, T.; Micklesfield, L.K.; Wadende, P.; Obonyo, C.O.; Woodcock, J.; Mogo, E.R.I.; Odunitan-Wayas, F.A.; Assah, F.; Tatah, L.; Foley, L.; et al. Implications of COVID-19 control measures for diet and physical activity, and lessons for addressing other pandemics facing rapidly urbanising countries. Glob. Health Action 2020, 13, 1810415. [Google Scholar] [CrossRef]
- Puhl, R.; Lessard, L.; Larson, N.; Eisenberg, M.; Neumark-Stzainer, D. Weight Stigma as a Predictor of Distress and Maladaptive Eating Behaviors During COVID-19: Longitudinal Findings From the EAT Study. Ann. Behav. Med. 2020, 54, 738–746. [Google Scholar] [CrossRef]
- Stockwell, S.; Trott, M.; Tully, M.; Shin, J.; Barnett, Y.; Butler, L.; McDermott, D.; Schuch, F.; Smith, L. Changes in physical activity and sedentary behaviours from before to during the COVID-19 pandemic lockdown: A systematic review. BMJ Open Sport Exerc. Med. 2021, 7, e000960. [Google Scholar] [CrossRef]
- Chew, H.S.J.; Lopez, V. Global Impact of COVID-19 on Weight and Weight-Related Behaviors in the Adult Population: A Scoping Review. Int. J. Environ. Res. Public Health 2021, 18, 1876. [Google Scholar] [CrossRef]
- Kazmierski, K.F.M.; Gillespie, M.L.; Kuo, S. Stress-Induced eating among racial/ethnic groups in the United States: A Systematic Review. J. Racial Ethn. Health Disparities 2020, 8, 912–926. [Google Scholar] [CrossRef]
- Khaled, K.; Tsofliou, F.; Hundley, V.; Helmreich, R.; Almilaji, O. Perceived stress and diet quality in women of reproductive age: A systematic review and meta-analysis. Nutr. J. 2020, 19, 92. [Google Scholar] [CrossRef]
- Neill, E.; Meyer, D.; Toh, W.L.; van Rheenen, T.E.; Phillipou, A.; Tan, E.J.; Rossell, S.L. Alcohol use in Australia during the early days of the COVID-19 pandemic: Initial results from the COLLATE project. Psychiatry Clin. Neurosci. 2020, 74, 542–549. [Google Scholar] [CrossRef]
- Shaukat, N.; Ali, D.M.; Razzak, J. Physical and mental health impacts of COVID-19 on healthcare workers: A scoping review. Int. J. Emerg. Med. 2020, 13, 40. [Google Scholar] [CrossRef]
- Gupta, N.; Dhamija, S.; Patil, J.; Chaudhari, B. Impact of COVID-19 pandemic on healthcare workers. Ind. Psychiatry J. 2021, 30 (Suppl. 1), S282–S284. [Google Scholar] [CrossRef]
- Shreffler, J.; Petrey, J.; Huecker, M. The Impact of COVID-19 on Healthcare Worker Wellness: A Scoping Review. West. J. Emerg. Med. 2020, 21, 1059–1066. [Google Scholar] [CrossRef]
- Melnyk, B.M.; Kelly, S.A.; Stephens, J.; Dhakal, K.; McGovern, C.; Tucker, S.; Hoying, J.; McRae, K.; Ault, S.; Spurlock, E.; et al. Interventions to Improve Mental Health, Well-Being, Physical Health, and Lifestyle Behaviors in Physicians and Nurses: A Systematic Review. Am. J. Health Promot. 2020, 34, 929–941. [Google Scholar] [CrossRef]
- Durand-Sanchez, E.; Ruiz-Alvarado, C.; Contreras-Valderrama, R.; Morales-García, W.C.; Mamani-Benito, O.; Huancahuire-Vega, S.; Saintila, J.; Morales-García, M.; Ruiz Mamani, P.G. Sociodemographic Aspects and Healthy Behaviors Associated With Perceived Life Satisfaction in Health Professionals. J. Prim. Care Community Health 2023, 14, 21501319221148332. [Google Scholar] [CrossRef]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef]
- Braden, A.; Musher-Eisenman, D.; Watford, T.; Emley, E. Eating when depressed, anxious, bored, or happy: Are emotional eating types associated with unique psychological and physical health correlates? Appetite 2018, 125, 410–417. [Google Scholar] [CrossRef]
- Evers, C.; Dingemans, A.; Junghans, A.F.; Boevé, A. Feeling bad or feeling good, does emotion affect your consumption of food? A meta-analysis of the experimental evidence. Neurosci. Biobehav. Rev. 2018, 92, 195–208. [Google Scholar] [CrossRef]
- Buss, J. Associations between obesity and stress and shift work among nurses. Workplace Health Saf. 2012, 60, 453–458. [Google Scholar] [CrossRef]
- Antentas, J.M.; Vivas, E. Impact of the economic crisis on the right to a healthy diet. SESPAS report 2014. Gac. Sanit. 2014, 28, 58–61. [Google Scholar] [CrossRef]
- Epel, E.; Lapidus, R.; McEwen, B.; Brownell, K. Stress may add bite to appetite in women: A laboratory study of stress-induced cortisol and eating behavior. Psychoneuroendocrinology 2001, 26, 37–49. [Google Scholar] [CrossRef]
- O’Connor, D.B.; Jones, F.; Conner, M.; McMillan, B.; Ferguson, E. Effects of daily hassles and eating style on eating behavior. Health Psychol. 2008, 27 (Suppl. 1), S20–S31. [Google Scholar] [CrossRef]
- González-Monroy, C.; Gómez-Gómez, I.; Olarte-Sánchez, C.M.; Motrico, E. Eating behaviour changes during the COVID-19 pandemic: A systematic review of longitudinal studies. Int. J. Environ. Res. Public Health 2021, 18, 11130. [Google Scholar] [CrossRef]
- Griffin, T.; Grey, E.; Lambert, J.; Gillison, F.; Townsend, N.; Solomon-Moore, E. Life in lockdown: A qualitative study exploring the experience of living through the initial COVID-19 lockdown in the UK and its impact on diet, physical activity and mental health. BMC Public Health 2023, 23, 588. [Google Scholar] [CrossRef]
- Scarmozzino, F.; Visioli, F. COVID-19 and the Subsequent Lockdown Modified Dietary Habits of Almost Half the Population in an Italian Sample. Foods 2020, 9, 675. [Google Scholar] [CrossRef]
- Oliver, T.L.; Shenkman, R.; Diewald, L.K.; Bernhardt, P.W.; Chen, M.H.; Moore, C.H.; Kaufmann, P.G. A Year in the Life of U.S. Frontline Health Care Workers: Impact of COVID-19 on Weight Change, Physical Activity, Lifestyle Habits, and Psychological Factors. Nutrients 2022, 14, 4865. [Google Scholar] [CrossRef]
- Johnson, A.N.; Clockston, R.L.M.; Fremling, L.; Clark, E.; Lundeberg, P.; Mueller, M.; Graham, D.J. Changes in Adults’ eating behaviors during the initial months of the COVID-19 pandemic: A narrative review. J. Acad. Nutr. Diet. 2022, 123, 144–194. [Google Scholar] [CrossRef]
- Kaufmann, P.G.; Havens, D.S.; Mensinger, J.L.; Bradley, P.K.; Brom, H.M.; Copel, L.C.; Costello, A.; D’Annunzio, C.; Dean Durning, J.; Maldonado, L.; et al. The COVID-19 Study of Healthcare and Support Personnel (CHAMPS): Objectives and Design. JMIR Res. Protoc. 2021, 10, e30757. [Google Scholar] [CrossRef]
- Vaismoradi, M. Content analysis and thematic analysis: Implications for conducting a qualitative descriptive study. Nurs. Health Sci. 2013, 15, 398–405. [Google Scholar] [CrossRef]
- Zachary, Z.; Forbes, B.; Lopez, B.; Pederson, G.; Welty, J.; Deyo, A.; Kerekes, M. Self-quarantine and weight gain related risk factors during the COVID-19 pandemic. Obes. Res. Clin. Pract. 2020, 14, 210–216. [Google Scholar] [CrossRef]
- Herle, M.; Smith, A.D.; Bu, F.; Steptoe, A.; Fancourt, D. Trajectories of eating behavior during COVID-19 lockdown: Longitudinal analyses of 22,374 adults. Clin. Nutr. ESPEN 2021, 42, 158–165. [Google Scholar] [CrossRef]
- Cecchetto, C.; Aiello, M.; Gentili, C.; Ionta, S.; Osimo, S.A. Increased emotional eating during COVID-19 associated with lockdown, psychological and social distress. Appetite 2021, 160, 105122. [Google Scholar] [CrossRef]
- Mota, I.A.; Oliveira Sobrinho, G.D.; Morais, I.P.S.; Dantas, T.F. Impact of COVID-19 on eating habits, physical activity and sleep in Brazilian healthcare professionals. Arq. Neuro-Psiquiatr. 2021, 79, 429–436. [Google Scholar] [CrossRef]
- Yaman, G.B.; Hocaoğlu, Ç. Examination of eating and nutritional habits in health care workers during the COVID-19 pandemic. Nutrition 2023, 105, 111839. [Google Scholar] [CrossRef]
- Lopez-Minguez, J.; Gómez-Abellán, P.; Garaulet, M. Timing of Breakfast, Lunch, and Dinner. Effects on Obesity and Metabolic Risk. Nutrients 2019, 11, 2624. [Google Scholar] [CrossRef]
- Manoogian, E.N.C.; Chaix, A.; Panda, S. When to Eat: The Importance of Eating Patterns in Health and Disease. J. Biol. Rhythm. 2019, 34, 579–581. [Google Scholar] [CrossRef]
- Yao, Z.; Xie, X.; Bai, R.; Li, L.; Zhang, X.; Li, S.; Ma, Y.; Hui, Z.; Chen, J. The impact of eating behaviors during COVID-19 in health-care workers: A conditional process analysis of eating, affective disorders, and PTSD. Heliyon 2022, 8, e10892. [Google Scholar] [CrossRef]
- Di Giuseppe, M.; Nepa, G.; Prout, T.A.; Albertini, F.; Marcelli, S.; Orrù, G.; Conversano, C. Stress, Burnout, and Resilience among Healthcare Workers during the COVID-19 Emergency: The Role of Defense Mechanisms. Int. J. Environ. Res. Public Health 2021, 18, 5258. [Google Scholar] [CrossRef]
- Leo, C.G.; Sabina, S.; Tumolo, M.R.; Bodini, A.; Ponzini, G.; Sabato, E.; Mincarone, P. Burnout Among Healthcare Workers in the COVID 19 Era: A Review of the Existing Literature. Front. Public Health 2021, 9, 750529. [Google Scholar] [CrossRef]
- Sahebi, A.; Nejati-Zarnaqi, B.; Moayedi, S.; Yousefi, K.; Torres, M.; Golitaleb, M. The prevalence of anxiety and depression among healthcare workers during the COVID-19 pandemic: An umbrella review of meta-analyses. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2021, 107, 110247. [Google Scholar] [CrossRef]
- Marvaldi, M.; Mallet, J.; Dubertret, C.; Moro, M.R.; Guessoum, S.B. Anxiety, depression, trauma-related, and sleep disorders among healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis. Neurosci. Biobehav. Rev. 2021, 126, 252–264. [Google Scholar] [CrossRef]
- Esquivel, M.K. Nutrition Strategies for Reducing Risk of Burnout Among Physicians and Health Care Professionals. Am. J. Lifestyle Med. 2020, 15, 126–129. [Google Scholar] [CrossRef]
- Naczenski, L.M.; Vries, J.D.; Hooff, M.L.M.V.; Kompier, M.A.J. Systematic review of the association between physical activity and burnout. J. Occup. Health 2017, 59, 477–494. [Google Scholar] [CrossRef]
- Caldiroli, A.; La Tegola, D.; Manzo, F.; Scalia, A.; Affaticati, L.M.; Capuzzi, E.; Colmegna, F.; Argyrides, M.; Giaginis, C.; Mendolicchio, L.; et al. The Impact of the COVID-19 Pandemic on Binge Eating Disorder: A Systematic Review. Nutrients 2023, 15, 3777. [Google Scholar] [CrossRef]
- Miskovic-Wheatley, J.; Koreshe, E.; Kim, M.; Simeone, R.; Maguire, S. The impact of the COVID-19 pandemic and associated public health response on people with eating disorder symptomatology: An Australian study. J. Eat. Disord. 2022, 10, 9. [Google Scholar] [CrossRef]


{kind=link}
| Variables | Baseline/M0 (n = 234) | M12 (n = 127) | M24 (n = 80) |
|---|---|---|---|
| Gender | |||
| Men, n (%) | 30 (12.8) | 15 (12%) | 9 (11%) |
| Women, n (n%) | 203 (86.8) | 112 (88%) | 71 (89%) |
| Gender non-conforming individuals, n (%) | 1 (0.4) | ||
| Age, mean (SD), years | 38.69 (12) | 38.94 (12.1) | 37.96 (11.9) |
| Race | n (%) | n (%) | n (%) |
| Black/African American | 6 (2.6) | 4 (3.1) | 3 (3.8) |
| Latinx/Hispanic | 2 (0.9) | 0 (0) | 0 (0) |
| White/Non-Hispanic | 215 (91.9) | 119 (93.7) | 73 (91.3) |
| Asian/Pacific Islander | 4 (1.7) | 1 (0.8) | 1 (1.2) |
| Multi-racial/Mixed ethnicities | 5 (2.1) | 2 (1.6) | 2 (2.5) |
| Other | 2 (0.9) | 1 (0.8) | 1 (1.2) |
| Body Mass Index | (n = 189) * | (n = 120) * | (n = 75) * |
| n (%) | n (%) | n (%) | |
| Underweight | 2 (1.1) | 3 (2.5) | 1 (1.3) |
| Normal | 80 (42.8) | 53 (44.2) | 31 (41.3) |
| Overweight | 67 (35.8) | 35 (29.2) | 21 (28) |
| Obesity | 38 (20.3) | 29 (24.2) | 22 (29.3) |
| BMI, mean (SD) | 26.64 (6.29) | 27.00 (6.98) | 27.62 (6.82) |
| Job Role | n (%) | n (%) | n (%) |
| Nurse (e.g., including RN, CRNP, CRNA, Nursing Assistant, LPN) | 151 (64.5) | 85 (66.9) | 51 (63.75) |
| Aide or Medical Assistant | 5 (2.1) | 3 (2.4) | 2 (2.5) |
| Emergency Services (including Police Officers, Paramedics, EMTs, AEMTs, and EMRs) | 21 (9.0) | 9 (7.1) | 7 (8.75) |
| Therapists (including PT, OT) | 9 (3.9) | 6 (4.7) | 4 (5.0) |
| Pharmacist/Pharmacy technician | 7 (3.0) | 7 (5.5) | 6 (7.5) |
| Physician/Physician Assistant | 9 (3.8) | 6 (4.7) | 2 (2.5) |
| Staff (Reception/Unit Clerk/Administrative Assistant/Housekeeping) | 2 (0.8) | 1 (0.8) | 0 (0) |
| Registered Dietitian | 4 (1.7) | 2 (1.6) | 2 (2.5) |
| Social Work | 10 (4.3) | 5 (3.9) | 3 (3.75) |
| Other (please describe) | 16 (6.8) | 3 (2.4) | 3 (3.75) |
| Theme | Description | M0 n | M12 n | M24 n | % of Total Response (n = 157) |
|---|---|---|---|---|---|
| Problematic eating behaviors and habits * | Emotional/stress eating, eating for comfort | 18 | 19 | 5 | 26.8% |
| Disruptions in physical activity * | Gyms closed; schedule disruptions | 14 | 11 | 6 | 19.7.% |
| Declines in mental health * | Increase in stress, depression, anxiety | 12 | 8 | 2 | 14% |
| Alterations in Work Environment or Schedule * | Change in work environment/ location | 10 | 6 | 1 | 10.8% |
| Improvements in physical activity | Schedule permitted more physical activity; motivation | 5 | 2 | 4 | 7% |
| Intentional healthier lifestyle habits | Purposeful introduction of healthier eating and lifestyle habits | 4 | 5 | 1 | 6.4% |
| Change in sleep/fatigue | Disruptions in normal sleep habits | 3 | 5 | 1 | 5.7% |
| Other | Medical changes, pregnancy, breastfeeding | 4 | 4 | 7 | 9.6% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shenkman, R.; Diewald, L.; Murray, M.B.; Oliver, T.L. Unveiling Lived Experiences: Exploring the Health and Lifestyle Effects of COVID-19 on Healthcare Workers. Nutrients 2023, 15, 4857. https://doi.org/10.3390/nu15234857
Shenkman R, Diewald L, Murray MB, Oliver TL. Unveiling Lived Experiences: Exploring the Health and Lifestyle Effects of COVID-19 on Healthcare Workers. Nutrients. 2023; 15(23):4857. https://doi.org/10.3390/nu15234857
Chicago/Turabian StyleShenkman, Rebecca, Lisa Diewald, Mary Beth Murray, and Tracy L. Oliver. 2023. "Unveiling Lived Experiences: Exploring the Health and Lifestyle Effects of COVID-19 on Healthcare Workers" Nutrients 15, no. 23: 4857. https://doi.org/10.3390/nu15234857
APA StyleShenkman, R., Diewald, L., Murray, M. B., & Oliver, T. L. (2023). Unveiling Lived Experiences: Exploring the Health and Lifestyle Effects of COVID-19 on Healthcare Workers. Nutrients, 15(23), 4857. https://doi.org/10.3390/nu15234857