
Development of a Semi-Quantitative Food-Frequency Questionnaire for Korean Adults with Obesity

Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source and Participants for Determining the FFQ Dish/Food List
2.2. Selection of Dish/Food List
2.3. Response Options for Intake Frequency
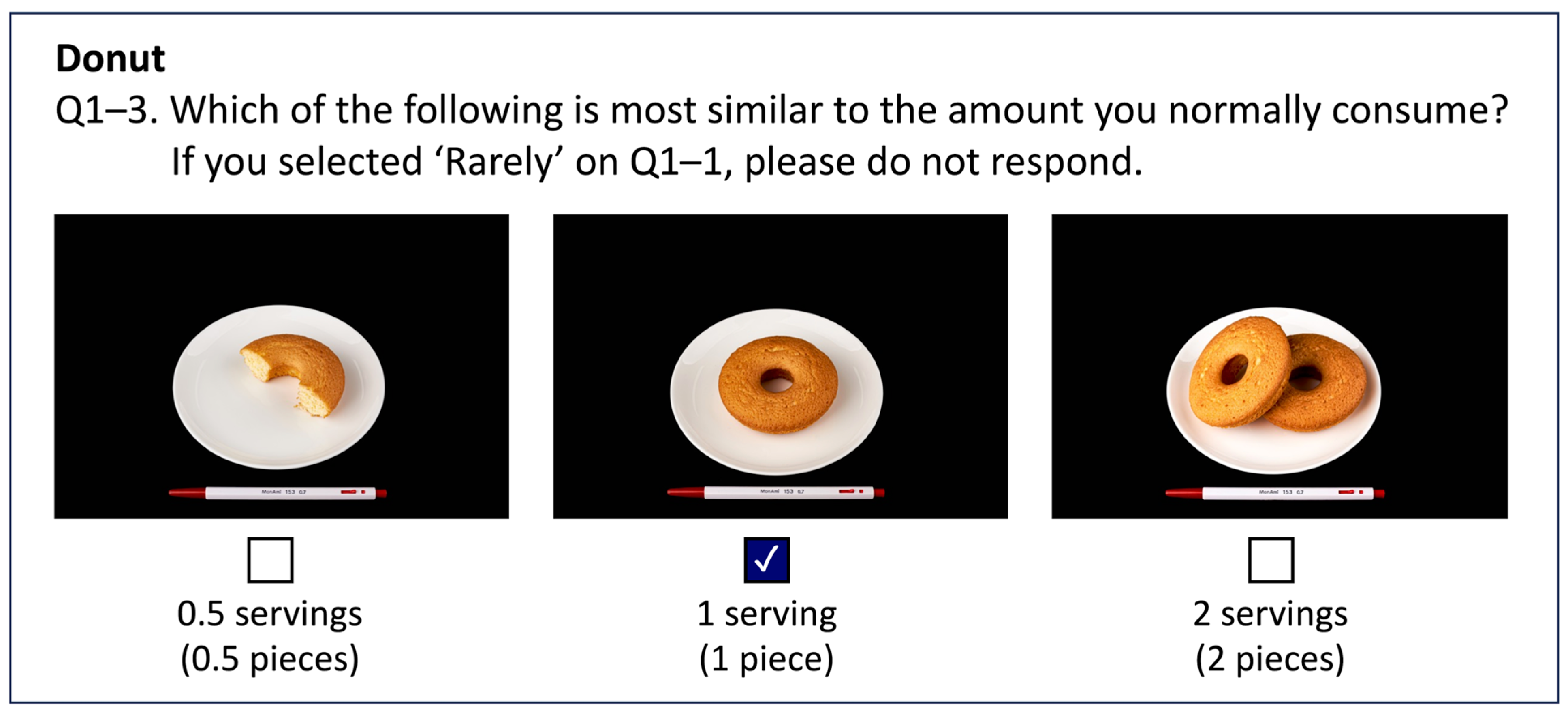
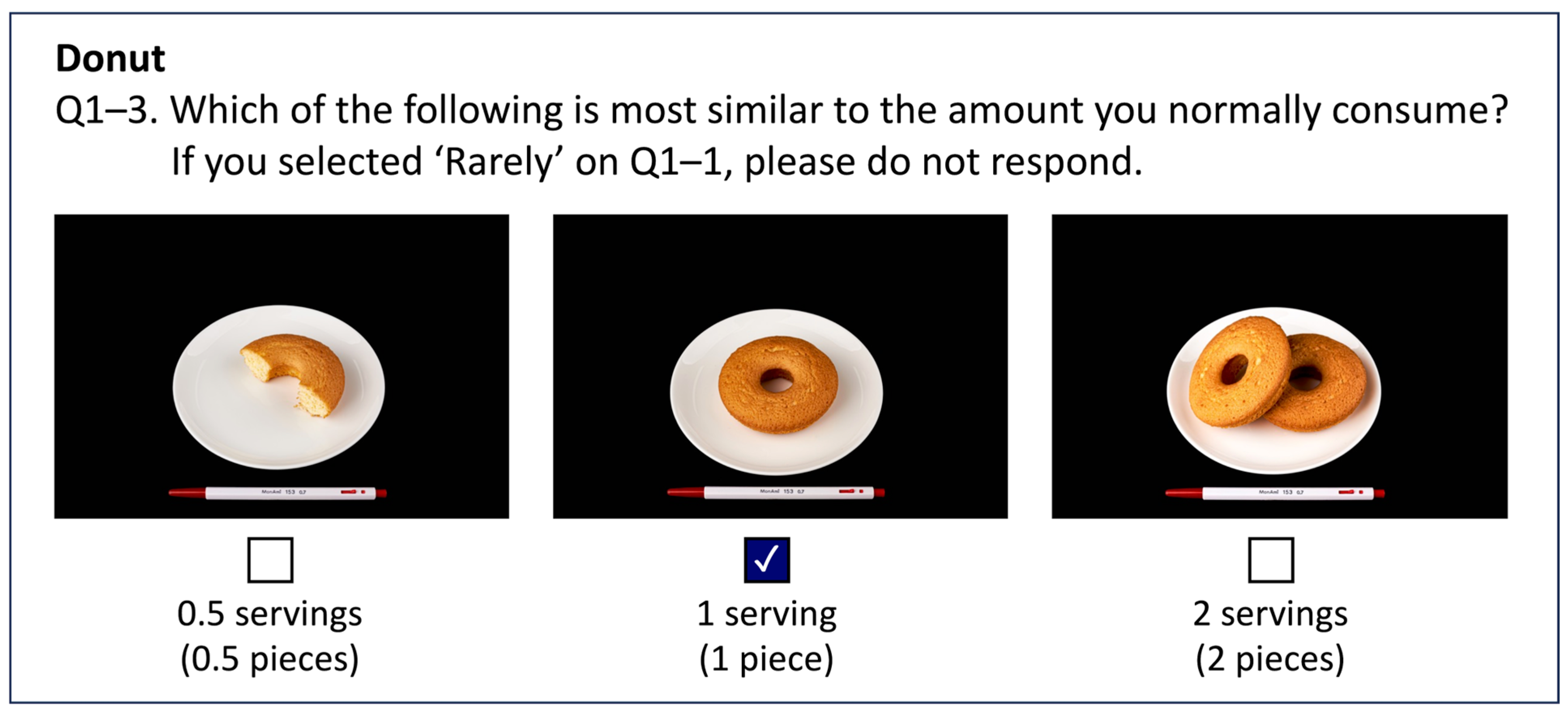
2.4. Response Options for Portion Size
2.5. Preliminary Surveys
2.6. Development of a Nutrient Database for Dish/Food Items
3. Results
3.1. Dish/Food List of the FFQ
3.2. Question and Response Options for Intake Frequency
3.3. Question and Response Options for Portion Size
3.4. Preliminary Survey and Revision of the FFQ
3.5. Nutrient Database for the FFQ
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ritchie, H.; Roser, M. Obesity. Available online: https://ourworldindata.org/obesity (accessed on 26 September 2023).
- World Health Organization. The Asia-Pacific perspective: Redefining Obesity and Its Treatment. 2000. Available online: chrome-extension://hmigninkgibhdckiaphhmbgcghochdjc/pdfjs/web/viewer.html?file=https://www.vepachedu.org/TSJ/BMI-Guidelines.pdf (accessed on 17 November 2023).
- Haam, J.-H.; Kim, B.T.; Kim, E.M.; Kwon, H.; Kang, J.-H.; Park, J.H.; Kim, K.-K.; Rhee, S.Y.; Kim, Y.-H.; Lee, K.Y. Diagnosis of Obesity: 2022 Update of Clinical Practice Guidelines for Obesity by the Korean Society for the Study of Obesity. JOMES 2023, 32, 121–129. [Google Scholar] [CrossRef] [PubMed]
- Korean Society for the Study of Obesity. Clinical Practice Guidelines for Obesity 2022; Korean Society for the Study of Obesity: Seoul, Republic of Korea, 2023. [Google Scholar]
- Korea Disease Control and Prevention Agency. Korea Health Statistics 2021: Korea National Health and Nutrition Examination Survey (KNHANES VIII-3); Korea Disease Control and Prevention Agency: Chungcheongbuk-do, Republic of Korea, 2022.
- Mohajan, D.; Mohajan, H.K. Obesity and Its Related Diseases: A New Escalating Alarming in Global Health. J. Innov. Med. Res. 2023, 2, 12–23. [Google Scholar] [CrossRef]
- Okunogbe, A.; Nugent, R.; Spencer, G.; Powis, J.; Ralston, J.; Wilding, J. Economic impacts of overweight and obesity: Current and future estimates for 161 countries. BMJ Glob. Health 2022, 7, e009773. [Google Scholar] [CrossRef] [PubMed]
- Bray, G.A.; Frühbeck, G.; Ryan, D.H.; Wilding, J.P. Management of obesity. Lancet 2016, 387, 1947–1956. [Google Scholar] [CrossRef] [PubMed]
- Yun, S.; Shim, J.; Kweon, S.; Oh, K. Development of a food frequency questionnaire for the Korea National Health and Nutrition Examination Survey: Data from the fourth Korea National Health and Nutrition Examination Survey (KNHANES IV). Korean J. Nutr. 2013, 46, 186–196. [Google Scholar] [CrossRef]
- Kim, D.W.; Song, S.; Lee, J.E.; Oh, K.; Shim, J.; Kweon, S.; Paik, H.Y.; Joung, H. Reproducibility and validity of an FFQ developed for the Korea National Health and Nutrition Examination Survey (KNHANES). Public Health Nutr. 2015, 18, 1369–1377. [Google Scholar] [CrossRef]
- Ahn, Y.; Lee, J.; Paik, H.; Lee, H.; Jo, I.; Kimm, K. Development of a semi-quantitative food frequency questionnaire based on dietary data from the Korea National Health and Nutrition Examination Survey. Nutr. Sci. 2003, 6, 173–184. [Google Scholar]
- Ahn, Y.; Kwon, E.; Shim, J.E.; Park, M.K.; Joo, Y.; Kimm, K.; Park, C.; Kim, D.H. Validation and reproducibility of food frequency questionnaire for Korean genome epidemiologic study. Eur. J. Clin. Nutr. 2007, 61, 1435–1441. [Google Scholar] [CrossRef]
- Willett, W. Nutritional Epidemiology; Oxford University Press: Oxford, UK, 1998. [Google Scholar]
- Bang, S.; Hyeon, S. Comparison of physical activity and dietary patterns according to the degree of obesity in Korean men and women: Data from the Seventh Korea National Health and Nutrition Examination Survey VII-1 (2016). J. Digit. Contents Soc. 2018, 19, 1527–1534. [Google Scholar] [CrossRef]
- Kim, M.; Yun, Y.; Kim, Y. Developing Dish-based Food Frequency Questionnaire for the Epidemiology Study of Hypertension Among Korean. Korean J. Community Nutr. 2008, 13, 701–712. [Google Scholar]
- Hong, S.; Choi, Y.; Lee, H.J.; Kim, S.H.; Oe, Y.; Lee, S.Y.; Nam, M.; Kim, Y.S. Development and validation of a semi-quantitative food frequency questionnaire to assess diets of Korean type 2 diabetic patients. Korean Diabetes J. 2010, 34, 32–39. [Google Scholar] [CrossRef] [PubMed]
- Bentzen, S.M.; Knudsen, V.K.; Christiensen, T.; Ewers, B. Relative validity of a web-based food frequency questionnaire for patients with type 1 and type 2 diabetes in Denmark. Nutr. Diabetes 2016, 6, e232. [Google Scholar] [CrossRef] [PubMed]
- Sarmento, R.A.; Riboldi, B.P.; da Costa Rodrigues, T.; de Azevedo, M.J.; de Almeida, J.C. Development of a quantitative food frequency questionnaire for Brazilian patients with type 2 diabetes. BMC Public Health 2013, 13, 740. [Google Scholar] [CrossRef] [PubMed]
- Amsah, N.; Md Isa, Z.; Ahmad, N. Development of a Semi-Quantitative Food Frequency Questionnaire to Estimate Macronutrient Intake among Type 2 Diabetes Mellitus Patients in Malaysia. Nutrients 2023, 15, 506. [Google Scholar] [CrossRef]
- Nirdnoy, N.; Sranacharoenpong, K.; Surawit, A.; Pinsawas, B.; Mongkolsucharitkul, P.; Pongkunakorn, T.; Manosan, T.; Ophakas, S.; Suta, S.; Pumeiam, S.; et al. Validation of a Thai semiquantitative food frequency questionnaire (semi-FFQ) for people at risk of metabolic syndrome. J. Health Popul. Nutr. 2023, 42, 13. [Google Scholar] [CrossRef]
- Béliard, S.; Coudert, M.; Valéro, R.; Charbonnier, L.; Duchêne, E.; Allaert, F.A.; Bruckert, É. Validation of a short food frequency questionnaire to evaluate nutritional lifestyles in hypercholesterolemic patients. Ann. Endocrinol. 2012, 73, 523–529. [Google Scholar] [CrossRef]
- Bredin, C.; Naimimohasses, S.; Norris, S.; Wright, C.; Hancock, N.; Hart, K.; Moore, J.B. Development and relative validation of a short food frequency questionnaire for assessing dietary intakes of non-alcoholic fatty liver disease patients. Eur. J. Nutr. 2020, 59, 571–580. [Google Scholar] [CrossRef]
- Kweon, S.; Kim, Y.; Jang, M.-J.; Kim, Y.; Kim, K.; Choi, S.; Chun, C.; Khang, Y.-H.; Oh, K. Data Resource Profile: The Korea National Health and Nutrition Examination Survey (KNHANES). Int. J. Epidemiol. 2014, 43, 69–77. [Google Scholar] [CrossRef]
- Park, M.K.; Kim, D.W.; Kim, J.; Park, S.; Joung, H.; Song, W.O.; Paik, H.Y. Development of a dish-based, semi-quantitative FFQ for the Korean diet and cancer research using a database approach. Br. J. Nutr. 2011, 105, 1065–1072. [Google Scholar] [CrossRef]
- Ministry of Food and Drug Safety. Food Nutrient Database; Ministry of Food and Drug Safety: Chungcheongbuk-do, Republic of Korea, 2020.
- Ministry of Food and Drug Safety. Dining out Nutritional Ingredient Database (2012–2017); Ministry of Food and Drug Safety: Chungcheongbuk-do, Republic of Korea, 2019.
- Ministry of Health and Welfare; Korea Health Industry Development Institute. Development of Food and Nutrient Database: Food Portion/Weight Database; Ministry of Health and Welfare; Korea Health Industry Development Institute: Sejong City, Republic of Korea, 2007.
- Ministry of Health and Welfare. Database of Food Ingredient Amounts by Food; Ministry of Health and Welfare: Chungcheongbuk-do, Republic of Korea, 2019.
- MenuGen. Available online: https://koreanfood.rda.go.kr/kfi/mgnNewmealinfoMealquery/list (accessed on 11 November 2023).
- CAN-Pro 6.0. Available online: http://canpro6.kns.or.kr/ (accessed on 11 November 2023).
- Rural Development Administration. Food Composition Database; Rural Development Administration National Institute of Agriculture Sciences: Jeollabuk-do, Republic of Korea, 2022. [Google Scholar]
- Jun, S.; Shin, S.; Joung, H. Estimation of dietary flavonoid intake and major food sources of Korean adults. Br. J. Nutr. 2016, 115, 480–489. [Google Scholar] [CrossRef]
- Olariike Oyindasola, K. Diet and Obesity. In Psychology and Pathophysiological Outcomes of Eating; Akikazu, T., Hubertus, H., Eds.; IntechOpen: Rijeka, Croatia, 2021. [Google Scholar]
- Ministry of Health and Welfare; The Korean Nutrition Society. Dietary Reference Intakes for Koreans 2020; Ministry of Health and Welfare, The Korean Nutrition Society: Sejong, Republic of Korea, 2020.
- Shim, J.S.; Shim, S.Y.; Cha, H.J.; Kim, J.; Kim, H.C. Socioeconomic Characteristics and Trends in the Consumption of Ultra-Processed Foods in Korea from 2010 to 2018. Nutrients 2021, 13, 1120. [Google Scholar] [CrossRef] [PubMed]
- Shim, J.S.; Shim, S.Y.; Cha, H.J.; Kim, J.; Kim, H.C. Association between Ultra-processed Food Consumption and Dietary Intake and Diet Quality in Korean Adults. J. Acad. Nutr. Diet. 2022, 122, 583–594. [Google Scholar] [CrossRef]
- Shim, J.S. Ultra-processed foods and total sugars intake in Korea: Evidence from the Korea National Health and Nutrition Examination Survey 2016-2018. Nutr. Res. Pract. 2022, 16, 476–488. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.; Park, J.M.; Oh, S.U.; Ha, K.; Joung, H. Consumption of Ultra-Processed Foods Increases the Likelihood of Having Obesity in Korean Women. Nutrients 2021, 13, 698. [Google Scholar] [CrossRef]
- Shim, J.S.; Ha, K.H.; Kim, D.J.; Kim, H.C. Ultra-Processed Food Consumption and Obesity in Korean Adults. Diabetes Metab. J. 2023, 47, 547–558. [Google Scholar] [CrossRef] [PubMed]
- Shim, J.S.; Ha, K.H.; Kim, D.J.; Kim, H.C. Diet quality partially mediates the association between ultraprocessed food consumption and adiposity indicators. Obesity (Silver Spring) 2023, 31, 2430–2439. [Google Scholar] [CrossRef] [PubMed]
- Tan, L.J.; Hwang, S.B.; Shin, S. The Longitudinal Effect of Ultra-Processed Food on the Development of Dyslipidemia/Obesity as Assessed by the NOVA System and Food Compass Score. Mol. Nutr. Food Res. 2023, 67, e2300003. [Google Scholar] [CrossRef]
- FAO Statistical Databases (FAOSTAT). Available online: https://www.fao.org/faostat/en/#data (accessed on 26 September 2023).
- Frequently Consumed Foods. Available online: https://www.khidi.or.kr/kps (accessed on 26 September 2023).
- Block, G.; Hartman, A.M.; Dresser, C.M.; Carroll, M.D.; Gannon, J.; Gardner, L. A data-based approach to diet questionnaire design and testing. Am. J. Epidemiol. 1986, 124, 453–469. [Google Scholar] [CrossRef]
- Kim, J.; Jo, I.; Joung, H. A rice-based traditional dietary pattern is associated with obesity in Korean adults. J. Acad. Nutr. Diet. 2012, 112, 246–253. [Google Scholar] [CrossRef]

{kind=link}
| Total (n = 8450) | Men (n = 4515) | Women (n = 3935) | |
|---|---|---|---|
| Median age (years) | 47 (37–56) 1 | 44 (35–55) | 50 (40–58) |
| Age distribution, n (%) | |||
| 19–29 years | 960 (11.4) | 630 (7.5) | 330 (3.9) |
| 30–49 years | 3783 (44.8) | 2202 (26.1) | 1581 (18.7) |
| 50–64 years | 3707 (43.9) | 1683 (19.9) | 2024 (24.0) |
| Median BMI (kg/m2) | 27.1 (25.9–29.0) | 27.0 (25.9–28.8) | 27.1 (26.0–29.1) |
| BMI distribution, n (%) | |||
| 25 to <30 kg/m2 | 7068 (83.6) | 3856 (45.6) | 3212 (38.1) |
| 30 to <35 kg/m2 | 1169 (13.8) | 562 (6.7) | 607 (7.2) |
| ≥35 kg/m2 | 213 (2.5) | 97 (1.2) | 116 (1.4) |
| Cumulative Contribution Rate (%) | Cumulative R2 of between-Individual Variation | |
|---|---|---|
| Energy | 84.4 | 81.2 |
| Carbohydrate | 85.2 | 79.3 |
| Sugar | 83.2 | 86.9 |
| Dietary fiber | 82.6 | 83.0 |
| Protein | 79.2 | 73.3 |
| Fat | 80.3 | 81.2 |
| Saturated fat | 82.5 | 83.9 |
| Sodium | 78.3 | 77.0 |
| Vitamin A | 74.9 | 52.2 |
| Vitamin E | 78.9 | 75.2 |
| Flavonoids | 77.2 | 43.6 |
| Average | 80.6 | 74.2 |
| Dish/Food Category (n = 12) | Numbers of Dish/Food Items (n = 129) |
|---|---|
| Rice | 7 |
| Noodle and dumplings | 6 |
| Bread, rice cakes, and cereal | 10 |
| Soup and stews | 12 |
| Eggs, pulses, meats, and fishes | 28 |
| Vegetable and kimchi | 31 |
| Fruits | 14 |
| Snack | 4 |
| Milk and dairy products | 4 |
| Beverage | 9 |
| Alcohol | 3 |
| Water | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chung, J.; Ahn, S.; Joung, H.; Shin, S. Development of a Semi-Quantitative Food-Frequency Questionnaire for Korean Adults with Obesity. Nutrients 2023, 15, 4848. https://doi.org/10.3390/nu15224848
Chung J, Ahn S, Joung H, Shin S. Development of a Semi-Quantitative Food-Frequency Questionnaire for Korean Adults with Obesity. Nutrients. 2023; 15(22):4848. https://doi.org/10.3390/nu15224848
Chicago/Turabian StyleChung, Jina, Seoeun Ahn, Hyojee Joung, and Sangah Shin. 2023. "Development of a Semi-Quantitative Food-Frequency Questionnaire for Korean Adults with Obesity" Nutrients 15, no. 22: 4848. https://doi.org/10.3390/nu15224848
APA StyleChung, J., Ahn, S., Joung, H., & Shin, S. (2023). Development of a Semi-Quantitative Food-Frequency Questionnaire for Korean Adults with Obesity. Nutrients, 15(22), 4848. https://doi.org/10.3390/nu15224848