
The Role of Vitamin D in Patients with Inflammatory Bowel Disease Treated with Vedolizumab

 ,
,
Abstract
:1. Introduction
2. Methods
3. Results
3.1. Patient Characteristics
3.2. Pre-Treatment Vitamin D Levels and Ulcerative Colitis Outcomes
3.3. Pre-Treatment Vitamin D Levels and Crohn’s Disease Outcomes
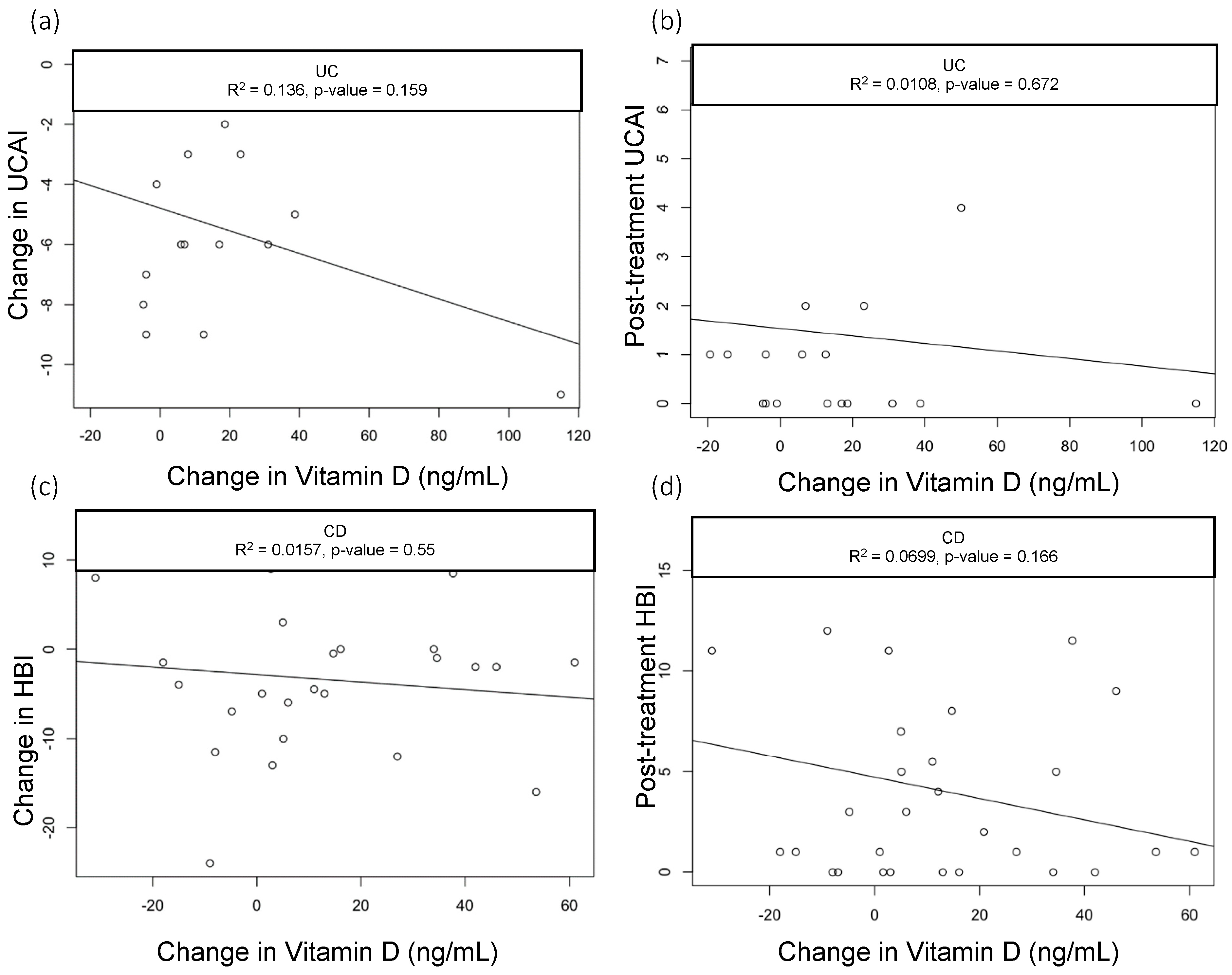
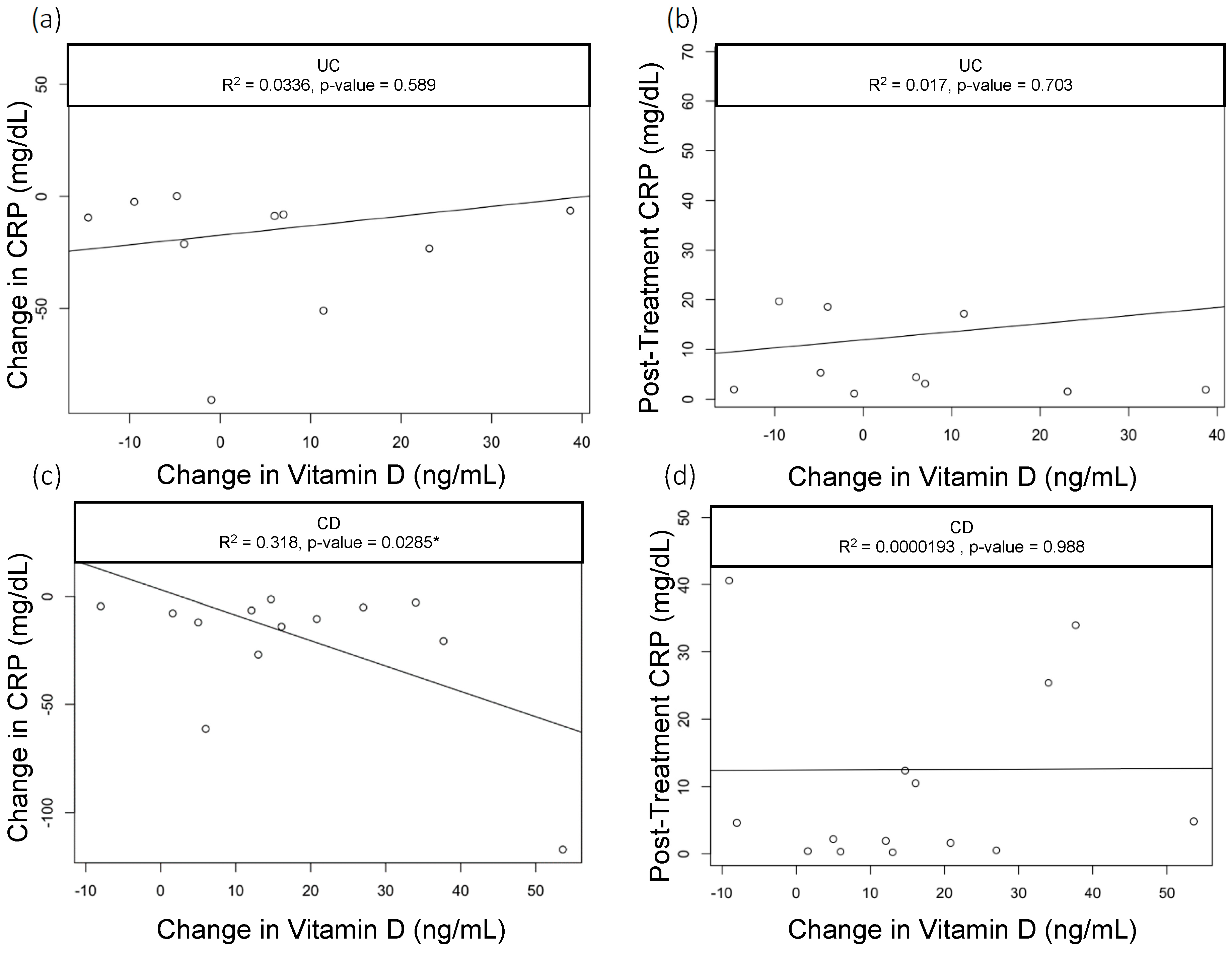
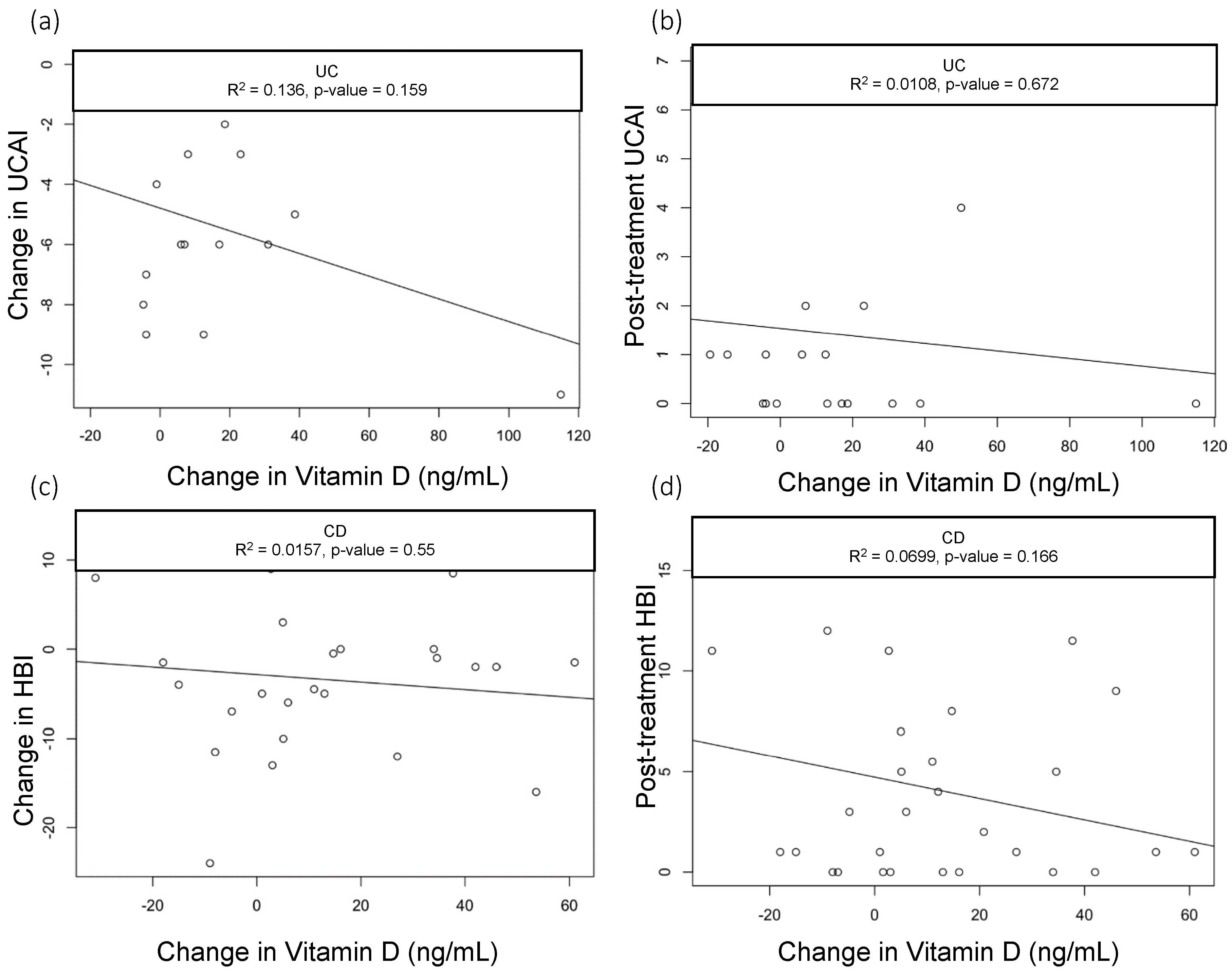
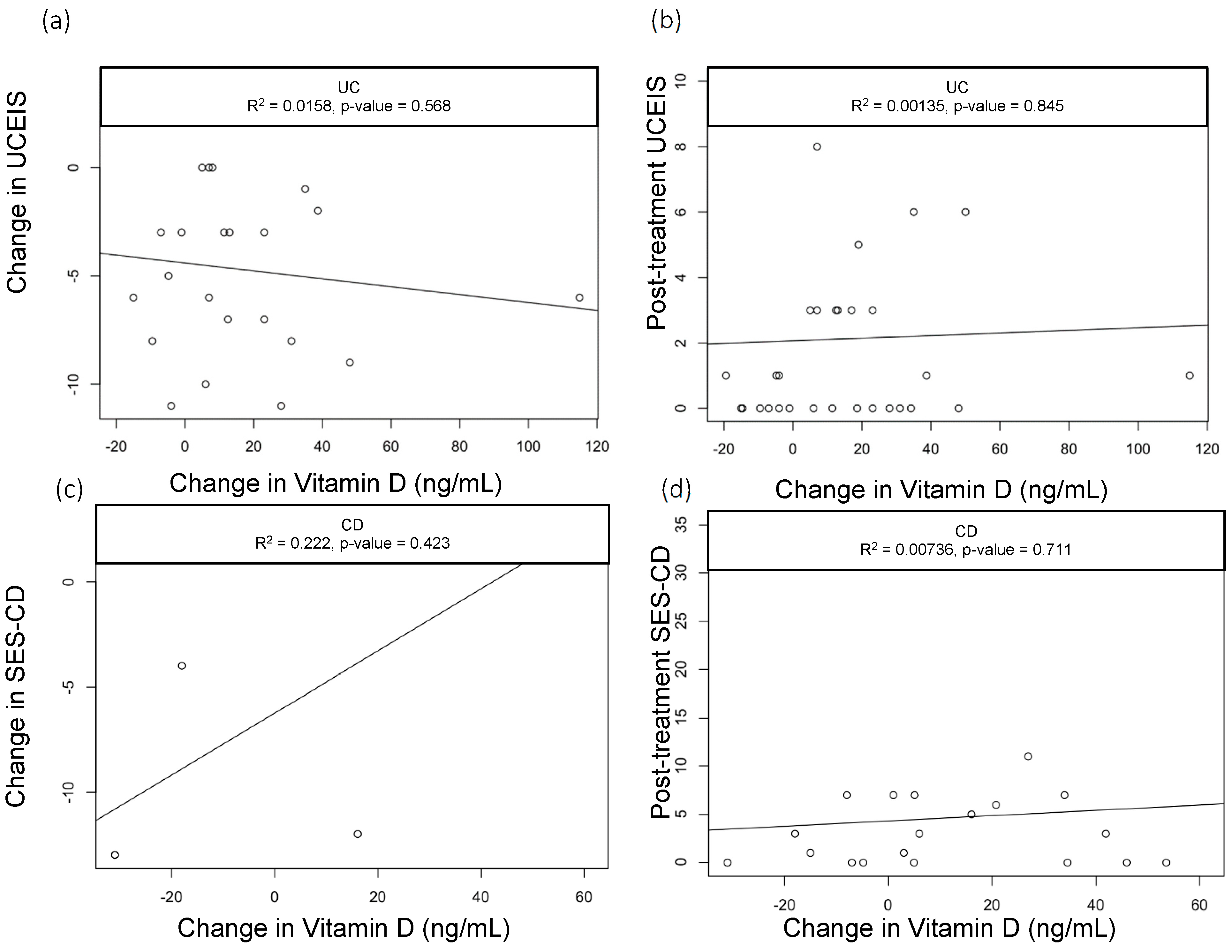
3.4. Change in Vitamin D Levels and Outcomes
3.5. Pre- and Post-Vedolizumab Therapy Outcomes
Ulcerative Colitis Outcomes
3.6. Crohn’s Disease Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pilon, D.; Ding, Z.; Muser, E.; Obando, C.; Voelker, J.; Manceur, A.M.; Kinkead, F.; Lafeuille, M.H.; Lefebvre, P. Long-term direct and indirect costs of ulcerative colitis in a privately-insured United States population. Curr. Med. Res. Opin. 2020, 36, 1285–1294. [Google Scholar] [CrossRef] [PubMed]
- Volk, N.; Siegel, C.A. Defining Failure of Medical Therapy for Inflammatory Bowel Disease. Inflamm. Bowel Dis. 2019, 25, 74–77. [Google Scholar] [CrossRef]
- Nemes, R.M.; Pop, C.S.; Calagiu, D.; Dobrin, D.; Chetroiu, D.; Jantea, P.; Postolache, P. Anemia in inflammatory bowel disease: More than just a supplement. Curr. Opin. Gastroenterol. Jul. 2018, 34, 217–225. [Google Scholar] [CrossRef]
- Bernstein, C.N.; Leslie, W.D. Review article: Osteoporosis and inflammatory bowel disease. Aliment. Pharmacol. Ther. 2004, 19, 941–952. [Google Scholar] [CrossRef]
- Ardizzone, S.; Bollani, S.; Bettica, P.; Bevilacqua, M.; Molteni, P.; Bianchi Porro, G. Altered bone metabolism in inflammatory bowel disease: There is a difference between Crohn’s disease and ulcerative colitis. J. Intern. Med. 2000, 247, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Siffledeen, J.S.; Fedorak, R.N.; Siminoski, K.; Jen, H.; Vaudan, E.; Abraham, N.; Seinhart, H.; Greenberg, G. Bones and Crohn’s: Risk factors associated with low bone mineral density in patients with Crohn’s disease. Inflamm. Bowel Dis. 2004, 10, 220–228. [Google Scholar] [CrossRef]
- Lewandowski, K.; Kaniewska, M.; Więcek, M.; Szwarc, P.; Panufnik, P.; Tulewicz-Marti, E.; Walicka, M.; Franek, E.; Rydzewska, G. Risk Factors for Osteoporosis among Patients with Inflammatory Bowel Disease-Do We Already Know Everything? Nutrients 2023, 15, 1151. [Google Scholar] [CrossRef]
- Topalova-Dimitrova, A.; Dimitrov, I.V.; Nikolov, R. Lower vitamin D levels are associated with the pathogenesis of inflammatory bowel diseases. Medicine 2023, 102, e35505. [Google Scholar] [CrossRef]
- Liu, C.; Liu, X.; Shi, H.; Chen, F.; Sun, L.; Gao, X.; Wang, Y. The correlation between serum 25-hydroxyvitamin D level and ulcerative colitis: A systematic review and meta-analysis. Eur. J. Gastroenterol. Hepatol. 2023, 35, 1375–1381. [Google Scholar] [CrossRef]
- Rizvi, A.; Trivedi, P.; Bar-Mashiah, A.; Plietz, M.; Khaitov, S.; Sylla, P.; Greenstein, A.; Dubinsky, M.C.; Kayal, M. Vitamin d Deficiency is Common in Patients with Ulcerative Colitis After Total Proctocolectomy with Ileal Pouch Anal Anastomosis. Inflamm. Bowel Dis. 2022, 28, 1924–1926. [Google Scholar] [CrossRef]
- Mouli, V.P.; Ananthakrishnan, A.N. Review article: Vitamin D and inflammatory bowel diseases. Aliment. Pharmacol. Ther. 2014, 39, 125–136. [Google Scholar] [CrossRef]
- Dan, L.; Chen, X.; Xie, Y.; Sun, Y.; Hesketh, T.; Wang, X.; Chen, J. Nonlinear Association between Serum 25-Hydroxyvitamin D and All-Cause Mortality in Adults with Inflammatory Bowel Disease in a Prospective Cohort Study. J. Nutr. 2022, 152, 2125–2134. [Google Scholar] [CrossRef] [PubMed]
- Gubatan, J.; Rubin, S.J.; Bai, L.; Haileselassie, Y.; Levitte, S.; Balabanis, T.; Patel, A.; Sharma, A.; Sinha, S.R.; Habtezion, A. Vitamin D Is Associated with alpha4beta7+ Immunophenotypes and Predicts Vedolizumab Therapy Failure in Patients with Inflammatory Bowel Disease. J. Crohn’s Colitis 2021, 15, 1980–1990. [Google Scholar] [CrossRef]
- Gubatan, J.; Chou, N.D.; Nielsen, O.H.; Moss, A.C. Systematic review with meta-analysis: Association of vitamin D status with clinical outcomes in adult patients with inflammatory bowel disease. Aliment. Pharmacol. Ther. 2019, 50, 1146–1158. [Google Scholar] [CrossRef] [PubMed]
- Hausmann, J.; Kubesch, A.; Amiri, M.; Filmann, N.; Blumenstein I Vitamin, D. Deficiency is Associated with Increased Disease Activity in Patients with Inflammatory Bowel Disease. J. Clin. Med. 2019, 8, 1319. [Google Scholar] [CrossRef]
- Gordon, R.J.; Wells, R.; Johansen, C.; Liu, S.; Dahlberg, S.E.; Snapper, S.B.; Rufo, P.A. Efficacy and Safety of High-dose Cholecalciferol in Patients with Inflammatory Bowel Disease Receiving Infliximab. J. Pediatr. Gastroenterol. Nutr. 2022, 74, 476–483. [Google Scholar] [CrossRef]
- Guzman-Prado, Y.; Samson, O.; Segal, J.P.; Limdi, J.K.; Hayee, B. Vitamin D Therapy in Adults with Inflammatory Bowel Disease: A Systematic Review and Meta-Analysis. Inflamm. Bowel Dis. 2020, 26, 1819–1830. [Google Scholar] [CrossRef] [PubMed]
- Gudsoorkar, V.; Chaikriangkrai, K.; Abraham, B. Vitamin D Deficiency Is Associated with Persistent CRP Elevation and a Lower Clinical Response to Vedolizumab Treatment in Crohn’s Disease Patients. Am. J. Gastroenterol. 2015, 110, S844–S845. [Google Scholar] [CrossRef]
- Gubatan, J.; Mitsuhashi, S.; Zenlea, T.; Rosenberg, L.; Robson, S.; Moss, A.C. Low Serum Vitamin D During Remission Increases Risk of Clinical Relapse in Patients with Ulcerative Colitis. Clin. Gastroenterol. Hepatol. 2017, 15, 240–246. [Google Scholar] [CrossRef]
- Gasche, C.; Evstatiev, R.; Haas, T.; Kaser, A.; Knoflach, P.; Petritsch, W.; Weiss, G.; Reinisch, W. Diagnosis and treatment of iron deficiency and anaemia in inflammatory bowel diseases. Consensus of the Austrian IBD Working Party. Z. Gastroenterol. 2011, 49, 627–632. [Google Scholar] [CrossRef]
- Xue, L.N.; Xu, K.Q.; Zhang, W.; Wang, Q.; Wu, J.; Wang, X.Y. Associations between vitamin D receptor polymorphisms and susceptibility to ulcerative colitis and Crohn’s disease: A meta-analysis. Inflamm. Bowel Dis. 2013, 19, 54–60. [Google Scholar] [CrossRef] [PubMed]
- Opstelten, J.L.; Chan, S.S.; Hart, A.R.; Van Schaik, F.D.; Siersema, P.D.; Lentjes, E.G.; Khaw, K.T.; Luben, R.; Key, T.J.; Boeing, H. Prediagnostic Serum Vitamin D Levels and the Risk of Crohn’s Disease and Ulcerative Colitis in European Populations: A Nested Case-Control Study. Inflamm. Bowel Dis. 2018, 24, 633–640. [Google Scholar] [CrossRef] [PubMed]
- Gao, H.; Zhou, H.; Zhang, Z.; Gao, J.; Li, J.; Li, X. Vitamin D3 alleviates inflammation in ulcerative colitis by activating the VDR-NLRP6 signaling pathway. Front. Immunol. 2023, 14, 1135930. [Google Scholar] [CrossRef] [PubMed]
- Triantos, C.; Aggeletopoulou, I.; Mantzaris, G.J.; Mouzaki, A. Molecular basis of vitamin D action in inflammatory bowel disease. Autoimmun. Rev. 2022, 21, 103136. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, J.; Cooper, S.C.; Ghosh, S.; Hewison, M. The Role of Vitamin D in Inflammatory Bowel Disease: Mechanism to Management. Nutrients 2019, 11, 1019. [Google Scholar] [CrossRef] [PubMed]
- Schardey, J.; Globig, A.M.; Janssen, C.; Hofmann, M.; Manegold, P.; Thimme, R.; Hasselblatt, P. Vitamin D Inhibits Pro-Inflammatory T Cell Function in Patients with Inflammatory Bowel Disease. J. Crohn’s Colitis 2019, 13, 1546–1557. [Google Scholar] [CrossRef]
- Ananthakrishnan, A.N. Vitamin D and Inflammatory Bowel Disease. Gastroenterol. Hepatol. 2016, 12, 513–515. [Google Scholar]
- Valvano, M.; Magistroni, M.; Cesaro, N.; Carlino, G.; Monaco, S.; Fabiani, S.; Vinci, A.; Vernia, F.; Viscido, A.; Latella, G. Effectiveness of Vitamin D Supplementation on Disease Course in Inflammatory Bowel Disease Patients: Systematic Review with Meta-Analysis. Inflamm. Bowel Dis. 2022, XX, 1–11. [Google Scholar] [CrossRef]
- Garg, M.; Hendy, P.; Ding, J.N.; Shaw, S.; Hold, G.; Hart, A. The Effect of Vitamin D on Intestinal Inflammation and Faecal Microbiota in Patients with Ulcerative Colitis. J. Crohn’s Colitis 2018, 12, 963–972. [Google Scholar] [CrossRef]
- Wallace, C.; Gordon, M.; Sinopoulou, V.; Limketkai, B.N. Vitamin D for the treatment of inflammatory bowel disease. Cochrane Database Syst. Rev. 2023, 10, Cd011806. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Combined (n = 88) | CD (n = 44) | UC (n = 44) | p-Value | |
|---|---|---|---|---|
| Age (median (IQR)) | 39.5 [31.0, 53.3] | 41.0 [29.0, 59.3] | 38.00 [31.0, 50.3] | 0.251 |
| Gender = Male (%) | 30 (34.1) | 13 (29.5) | 17 (38.6) | 0.5 |
| Race (%) | 0.68 | |||
| Asian | 6 (6.8) | 2 (4.5) | 4 (9.1) | |
| Black | 11 (12.5) | 6 (13.6) | 5 (11.4) | |
| Caucasian | 71 (80.7) | 36 (81.8) | 35 (79.5) | |
| Disease Duration (years) | 10.5 [5.1, 17.3] | 11.5 [5.7, 21.8] | 8.93 [5.1, 13.0] | 0.069 |
| Location of Disease | <0.001 | |||
| Colonic | 60 (68.2) | 17 (38.6) | 44 (100) | |
| Proximal | 9 (10.2) | 9 (20.5) | 0 (0.0) | |
| Colonic + Proximal | 19 (21.6) | 18 (40.9) | 0 (0.0) | |
| # Prior Therapies | 1.0 [1.0, 2.0] | 1.0 [1.0, 2.25] | 1.0 [1.0, 2.0] | 0.077 |
| # Prior Surgeries | 1.0 [1.0, 2.0] | 1.0 [1.0, 2.0] | 2.0 [1.5, 2.5] | 0.487 |
| # Baseline Endoscopic Score (UC = UCEIS, CD = SES-CD) (median [IQR]) | 15.00 [12.25, 23.25] | 6.00 [3.00, 8.75] | N/A |
| Vitamin D < 30 ng/mL (n = 16) | Vitamin D ≥ 30 ng/mL (n = 18) | p-Value | |
|---|---|---|---|
| Age (years) | 42.50 [33.25, 56.0] | 39.50 [34.75, 48.0] | 0.534 |
| Male (%) | 8 (50.0) | 5 (27.8) | 0.328 |
| Race (%) | 0.987 | ||
| Asian | 1 (6.2) | 1 (5.6) | |
| Black | 2 (12.5) | 2 (11.1) | |
| Caucasian | 13 (81.2) | 15 (83.3) | |
| Disease Duration (years) | 12.4 [6.2, 15.8] | 9.4 [5.0, 13.1] | 0.293 |
| Vedolizumab Dose Escalation (n (%)) | 10 (62.5) | 14 (77.8) | 0.549 |
| Iron Supplementation | 1 (6.2) | 1 (5.6) | 1.00 |
| Pre-Treatment Scores | |||
| UCAI score | 6.5 [4.0, 9.25] | 6.0 [1.5, 8.0] | 0.641 |
| CRP (mg/dL) | 4.0 [0.5 11.32] | 1.5 [0.9, 5.2] | 0.734 |
| ESR (mm/h) | 11.0 [6.0, 47.0] | 6.0 [2.0, 11.0] | 0.073 |
| Fecal Calprotectin (μg/mg) (median (IQR)) | 299.0 [149.0, 844.0] | 1377.9 [1313.9, 1441.8] | 0.245 |
| Fecal Lactoferrin (μg/g) | 400.2 [400.2, 400.2] | 71.7 [30.0, 130.9] | 0.143 |
| UCEIS Score (median (IQR)) | 7.0 [3.0, 9.0] | 8.0 [4.5, 9.5] | 0.716 |
| BMI | 24.6 [23.6, 29.1] | 24.5 [22.1, 30.6] | 0.72 |
| Vitamin D (ng/mL) | 22.5 [17.5, 26.5] | 38.7 [35.3, 48.6] | <0.001 |
| Albumin (g/dL) | 3.7 [2.7, 3.9] | 3.9 [3.1, 4.0] | 0.533 |
| Iron (umol/L) | 62.0 [22.5, 100.5] | 94.0 [58.0, 110.5] | 0.11 |
| TIBC (μg/dL) | 311.0 [285.0, 361.0] | 335.0 [293.5, 380.5] | 0.42 |
| Ferritin (μg/L) | 38.0 [22.5, 115.5] | 60.0 [29.5, 104.5] | 0.575 |
| Iron Sat (%) | 20.5 [10.3, 28.0] | 27.5 [21.0, 33.0] | 0.164 |
| Vitamin B12 (pg/mL) | 526.5 [357.5, 825.3] | 701.0 [414.3, 898.5] | 0.378 |
| Folate (ng/mL) | 13.4 [10.6, 14.9] | 12.2 [11.2, 18.1] | 0.979 |
| Zinc (μg/dL) (mean [SD]) | 68.7 (12.7) | 82.7 (21.6) | 0.173 |
| # Prior Advanced Therapies (mean (SD)) | 1.00 [0.00, 1.00] | 1.00 [1.00, 2.00] | 0.199 |
| Post-Treatment Scores | |||
| UCAI core | 0.5 [0.0, 3.3] | 1.0 [0.0, 1.3] | 0.838 |
| CRP (mg/dL) | 2.8 [1.1, 8.1] | 2.1 [1.0, 4.6] | 0.651 |
| ESR (mm/h) | 11.0 [5.8, 19.0] | 6.0 [2.0, 11.0] | 0.103 |
| Fecal Calprotectin (μg/mg) | 1026.0 [41.8, 2527.5] | 1670.8 [1050.4, 2291.2] | 0.643 |
| Fecal Lactoferrin (μg/g) | 37.0 [21.7, 58.8] | 69.8 [50.2, 96.3] | 0.564 |
| UCEIS score (mean (SD)) | 3.87 (3.7) | 1.5 (2.5) | 0.037 |
| Vedolizumab Level (μg/mL) | 19.9 [11.4, 28.9] | 25.4 [14.1, 34.5] | 0.27 |
| Vedolizumab Replacement Medication | 0.459 | ||
| Infliximab | 1 (33.3) | 2 (50.0) | |
| Ustekinumab | 1 (33.3) | 2 (50.0) | |
| Tofacitinib | 1 (33.3) | 0 (0.0) | |
| BMI | 25.8 [24.3, 29.5] | 24.8 [22.1, 28.8] | 0.541 |
| Vitamin D (ng/mL) | 31.0 [24.5, 49.5] | 56.0 [46.0, 66.0] | 0.007 |
| Albumin (g/dL) | 3.8 [3.3, 4.0] | 3.9 [3.7, 4.2] | 0.338 |
| Iron (umol/L) | 79.5 [53.5, 87.0] | 89.5 [54.3, 110.8] | 0.351 |
| TIBC (μg/dL) | 328.0 [294.3, 360.3] | 326.5 [299.3, 346.0] | 1 |
| Ferritin (μg/L) | 54.0 [25.3, 122.5] | 50.0 [25.0, 126.0] | 0.885 |
| Iron Sat (%) | 24.50 [17.50, 33.00] | 27.5 [17.3, 37.8] | 0.809 |
| Vitamin B12 (pg/mL) | 556.0 [462.0, 606.5] | 548.0 [469.0, 1093.0] | 0.571 |
| Folate (ng/mL) | 12.6 [10.4, 18.5] | 10.5 [7.5, 20.0] | 0.321 |
| Zinc (μg/dL) (mean (SD)) | 83.53 (9.99) | 73.00 (5.66) | 0.253 |
| Vitamin D < 30 ng/mL (n = 19) | Vitamin D ≥ 30 ng/mL (n = 12) | p-Value | |
|---|---|---|---|
| Age (years) | 41.0 [30.5, 57.5] | 43.5 [31.8, 62.0] | 0.776 |
| Male (%) | 5 (26.3) | 2 (16.7) | 0.853 |
| Race (%) | 0.111 | ||
| Asian | 0 (0.0) | 2 (16.7) | |
| Black | 5 (26.3) | 1 (8.3) | |
| Caucasian | 14 (73.7) | 9 (75.0) | |
| Disease Duration (years) | 14.2 [4.5, 20.6] | 14.4 [8.2, 25.4] | 0.273 |
| Disease Location (%) | 0.339 | ||
| 1 Colon Only | 8 (42.1) | 3 (25.0) | |
| 2 Proximal (Gastric ± Small bowel) | 5 (26.3) | 2 (16.7) | |
| 3 Proximal and Colon | 6 (31.6) | 7 (58.3) | |
| Vedolizumab Dose Escalation (%) | 8 (42.1) | 8 (66.7) | 0.335 |
| Iron Supplementation | 0 (0) | 1 (8.3) | 0.814 |
| Pre-Treatment Scores | |||
| HBI score | 6.0 [3.0, 11.5] | 5.0 [3.0, 10.0] | 0.725 |
| CRP (mg/dL) | 8.2 [2.0, 21.8] | 2.6 [0.6, 12.1] | 0.212 |
| ESR (mm/h) | 25.0 [13.0, 50.0] | 16.0 [5.0, 31.0] | 0.403 |
| Fecal Calprotectin (μg/mg) | N/A | 272.5 [171.7, 373.2] | N/A |
| Fecal Lactoferrin (μg/g) | 252.5 [252.5, 252.5] | 52.5 [29.3, 75.7] | 0.221 |
| SES-CD score | 17.0 [13.5, 22.0] | 13.0 [11.5, 17.8] | 0.721 |
| # Prior Surgeries | 1.0 [1.0, 1.0] | 2.0 [1.0, 2.0] | 0.129 |
| BMI (kg/m2) | 24.1 [19.3, 30.4] | 22.4 [21.5, 24.2] | 0.525 |
| Vitamin D (ng/mL) | 17.4 [14.7, 22.0] | 40.0 [33.8, 49.8] | <0.001 |
| Albumin (g/dL) | 3.0 [2.5, 4.0] | 3.6 [3.3, 4.1] | 0.451 |
| Iron (umol/L) | 35.5 [25.0, 57.8] | 81.0 [26.0, 90.5] | 0.132 |
| TIBC (μg/dL) | 301.0 [266.5, 383.5] | 323.0 [247.0, 327.0] | 0.586 |
| Ferritin (μg/L) | 58.0 [14.0, 141.0] | 82.0 [60.0, 122.0] | 0.35 |
| Iron Sat (%) | 12.0 [6.25, 17.25] | 25.0 [17.5, 28.5] | 0.008 |
| Vitamin B12 (pg/mL) | 433.5 [378.5, 551.0] | 885.0 [645.5, 1285.3] | 0.003 |
| Folate (ng/mL) | 9.6 [6.8, 13.7] | 18.6 [10.2, 20.7] | 0.054 |
| Zinc (μg/dL) (mean (SD)) | 66.9 (20.0) | 73.8 (17.6) | 0.521 |
| Prior Biologics | 1.00 [1.00, 2.00] | 2.00 [1.00, 3.00] | 0.13 |
| Post-Treatment Scores | |||
| HBI score | 1.0 [0.0, 5.0] | 5.5 [1.0, 10.0] | 0.163 |
| CRP (mg/dL) | 1.6 [0.4, 4.3] | 3.0 [1.5, 18.7] | 0.101 |
| ESR (mm/h) | 7.5 [2.0, 21.3] | 9.0 [2.0, 11.0] | 0.692 |
| Fecal Calprotectin (μg/mg) | 24.0 [12.3, 702.0] | 2.5 [2.5, 156.7] | 0.825 |
| Fecal Lactoferrin (μg/g) | 194.0 [29.3, 737.3] | 30.0 [30.0, 58.6] | 0.793 |
| SES-CD Score (mean (SD)) | 3.6 (3.8) | 6.3 (12.9) | 0.539 |
| Vedolizumab level (μg/mL) | 14.4 [11.1, 23.0] | 27.4 [22.4, 42.7] | 0.045 |
| Vedo Replacement Drug | 0.189 | ||
| Infliximab | 1 (33.3) | 2 (66.7) | |
| Ustekinumab | 2 (66.7) | 0 (0.0) | |
| Tofacitinib | 0 (0.0) | 1 (33.3) | |
| BMI (kg/m2) | 24.7 [21.6, 33.5] | 24.4 [22.3, 26.5] | 0.446 |
| Vitamin D (ng/mL) | 27.0 [22.0, 50.5] | 31.0 [29.5, 64.4] | 0.081 |
| Albumin (g/dL) | 3.5 [2.7, 3.9] | 3.5 [3.3, 4.1] | 0.602 |
| Iron (umol/L) | 65.0 [54.0, 86.0] | 96.5 [77.0, 116.3] | 0.025 |
| TIBC (μg/dL) | 305.0 [278.0, 374.0] | 266.5 [255.5, 338.0] | 0.335 |
| Ferritin (μg/L) | 83.0 [52.5, 300.0] | 144.0 [61.5, 256.0] | 0.621 |
| Iron Sat (%) | 24.0 [17.0, 30.0] | 35.5 [33.5, 40.8] | 0.007 |
| Vitamin B12 (pg/mL) | 572.0 [445.5, 718.5] | 598.0 [473.0, 1243.0] | 0.445 |
| Folate (ng/mL) | 10.7 [9.6, 19.2] | 17.1 [10.4, 19.3] | 0.631 |
| Zinc (μg/dL) (mean (SD)) | 71.13 (10.59) | 77.40 (13.56) | 0.411 |
| Pre-Vedolizumab | Post-Vedolizumab | p | |
|---|---|---|---|
| UC Activity Index | 6.0 [2.3, 8.0] | 1.0 [0.0, 2.5] | <0.001 |
| CRP (mg/dL) | 3.2 [0.9, 11.3] | 2.5 [1.1, 6.7] | 0.777 |
| ESR (mm/h) | 11.0 [6.0, 27.0] | 7.5 [2.0, 16.8] | 0.245 |
| Fecal Calprotectin (μg/mg) | 1250.0 [299.0, 1250.0] | 196.0 [52.0, 2000.0] | 0.479 |
| Fecal Lactoferrin (μg/g) | 130.9 [50.9, 276.1] | 49.0 [28.2, 81.1] | 0.134 |
| UCEIS | 6.0 [3.0, 8.8] | 1.0 [0.0, 5.0] | <0.001 |
| BMI (kg/m2) | 24.4 [21.3, 28.7] | 25.87 [23.1, 29.9] | 0.337 |
| Vitamin D (ng/mL) | 33.2 [25.0, 38.8] | 45.0 [29.5, 60.0] | 0.008 |
| Albumin (g/dL) | 3.9 [3.0, 4.1] | 3.9 [3.6, 4.2] | 0.484 |
| Iron (umol/L) | 65.0 [34.0, 101.0] | 83.0 [52.3, 102.3] | 0.423 |
| TIBC (μg/dL) | 322.0 [283.5, 361.8] | 324.5 [295.0 353.0] | 0.563 |
| Ferritin (μg/L) | 54.5 [23.3, 135.0] | 55.0 [26.0, 122.0] | 0.766 |
| Iron Sat (%) | 27.0 [12.8, 29.0] | 25.5 [16.8, 32.3] | 0.477 |
| Vitamin B12 (pg/mL) | 619.0 [404.8, 840.8] | 548.0 [440.0, 687.0] | 0.637 |
| Folate (ng/mL) | 12.5 [10.7, 15.4] | 11.3 [9.2, 19.9] | 0.942 |
| Zinc (μg/dL) (mean (SD)) | 77.4 (19.6) | 79.9 (8.8) | 0.741 |
| Pre-Vedolizumab | Post-Vedolizumab | p | |
|---|---|---|---|
| Harvey–Bradshaw Index | 6.0 [3.0, 10.0] | 2.5 [1.0, 6.9] | 0.002 |
| CRP (mg/dL) | 3.4 [0.9, 13.5] | 2.7 [0.6, 6.7] | 0.44 |
| ESR (mm/h) | 16.5 [6.8, 46.3] | 6.0 [2.00, 19.8] | 0.004 |
| Fecal Calprotectin (μg/mg) | 326.5 [152.0, 495.7] | 80.5 [2.5, 235.3] | 0.234 |
| Fecal Lactoferrin (μg/g) | 98.9 [52.5, 175.7] | 30.0 [29.0, 96.2] | 0.735 |
| SES-CD | 15.0 [12.3, 23.3] | 3.0 [0.0, 8.5] | 0.002 |
| BMI (kg/m2) | 22.7 [19.7, 28.0] | 24.0 [21.6, 29.7] | 0.154 |
| Vitamin D (ng/mL) | 23.0 [17.0, 36.0] | 31.0 [24.0, 51.7] | 0.007 |
| Albumin (g/dL) | 3.3 [2.6, 4.2] | 3.5 [3.1, 4.1] | 0.658 |
| Iron (umol/L) | 41.0 [25.3, 75.8] | 82.5 [62.0, 107.3] | <0.001 |
| TIBC (μg/dL) | 297.0 [256.0, 330.5] | 312.0 [270.0, 344.3] | 0.305 |
| Ferritin (μg/L) | 74.0 [26.0, 141.0] | 117.0 [54.0, 273.5] | 0.064 |
| Iron Sat (%) | 15.0 [9.0, 25.0] | 27.0 [21.8, 36.3] | <0.001 |
| Vitamin B12 (pg/mL) | 545.0 [407.0, 969.0] | 572.0 [443.0, 946.3] | 0.55 |
| Folate (ng/mL) | 11.0 [6.8, 18.0] | 11.7 [8.9, 19.3] | 0.462 |
| Zinc (μg/dL) (mean (SD)) | 70.1 (18.5) | 74.3 (11.7) | 0.446 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abraham, B.P.; Fan, C.; Thurston, T.; Moskow, J.; Malaty, H.M. The Role of Vitamin D in Patients with Inflammatory Bowel Disease Treated with Vedolizumab. Nutrients 2023, 15, 4847. https://doi.org/10.3390/nu15224847
Abraham BP, Fan C, Thurston T, Moskow J, Malaty HM. The Role of Vitamin D in Patients with Inflammatory Bowel Disease Treated with Vedolizumab. Nutrients. 2023; 15(22):4847. https://doi.org/10.3390/nu15224847
Chicago/Turabian StyleAbraham, Bincy P., Christopher Fan, Theresa Thurston, Joshua Moskow, and Hoda M. Malaty. 2023. "The Role of Vitamin D in Patients with Inflammatory Bowel Disease Treated with Vedolizumab" Nutrients 15, no. 22: 4847. https://doi.org/10.3390/nu15224847
APA StyleAbraham, B. P., Fan, C., Thurston, T., Moskow, J., & Malaty, H. M. (2023). The Role of Vitamin D in Patients with Inflammatory Bowel Disease Treated with Vedolizumab. Nutrients, 15(22), 4847. https://doi.org/10.3390/nu15224847