
Influence of Diet, Dietary Products and Vitamins on Age-Related Cataract Incidence: A Systematic Review

 , ,
, ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
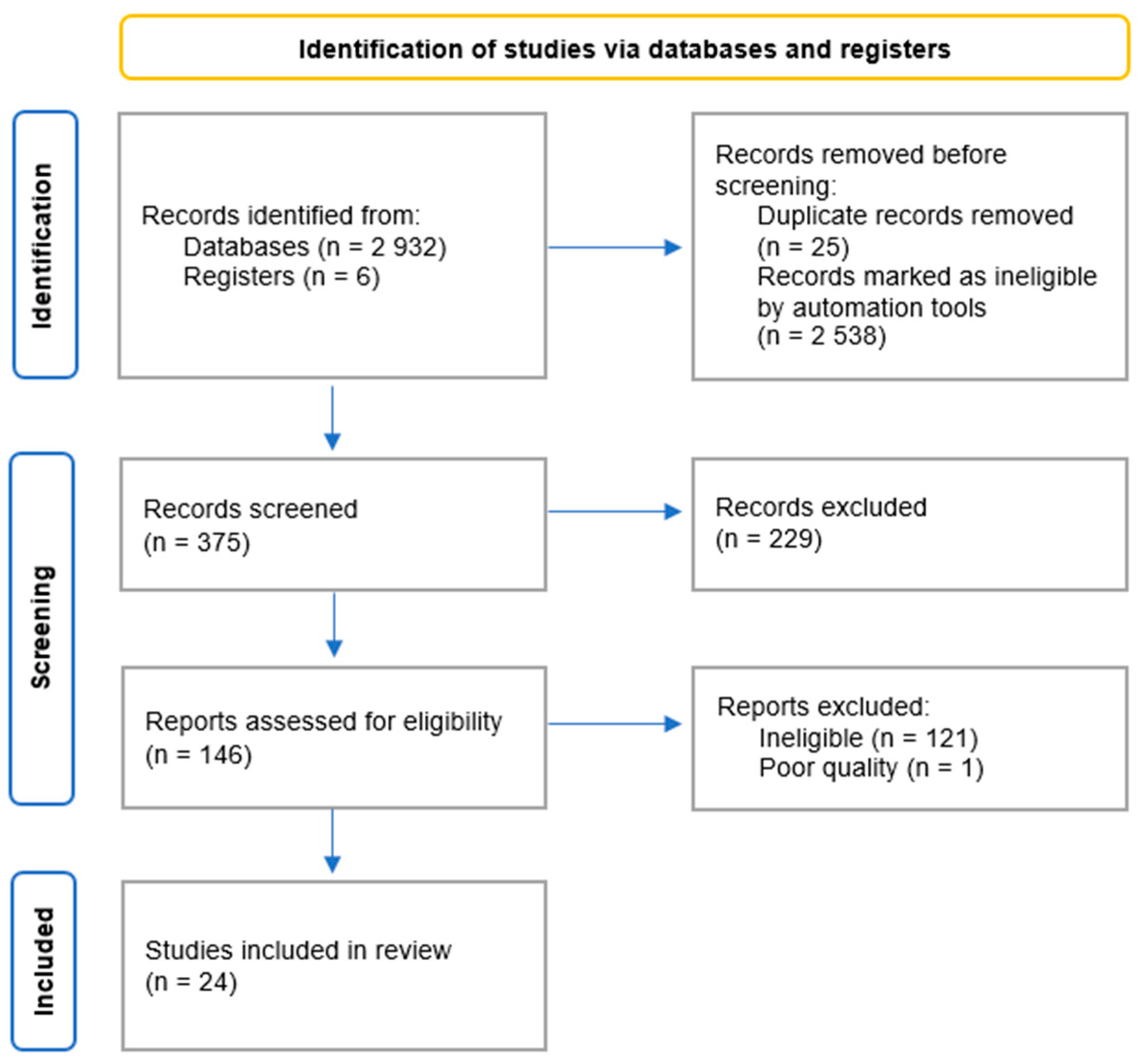
2.1. Search Strategy and Eligibility Criteria
2.2. Data Extraction and Assessment of Study Quality
3. Results
3.1. ARC and Different Types of Diets
3.1.1. Mediterranean Diet (MedDiet)
3.1.2. Traditional Korean Balanced Diet
3.1.3. Traditional and Dairy-Products-and-Vegetables Dietary Patterns
3.1.4. Vegetarian Diet
3.1.5. Nutrient Patterns
3.1.6. Pro-Inflammatory Diet
3.2. ARC and Different Types of Dietary Products
3.2.1. Fruit and Vegetables
3.2.2. Dairy Products
3.2.3. Wholegrain and Legume Foods
3.2.4. Coffee
3.2.5. Meat and Fish
3.3. ARC and Vitamins, Minerals and Carotenoids
3.3.1. Antioxidants
3.3.2. B-Group Vitamins
3.3.3. Vitamin K
3.3.4. Others
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Thompson, J.; Lakhani, N. Cataracts. Prim. Care 2015, 42, 409–423. [Google Scholar] [CrossRef]
- GBD 2019 Blindness and Vision Impairment Collaborators. Causes of blindness and vision impairment in 2020 and trends over 30 years, and prevalence of avoidable blindness in relation to VISION 2020: The Right to Sight: An analysis for the Global Burden of Disease Study. Lancet Glob. Health 2021, 9, e144–e160. [Google Scholar] [CrossRef] [PubMed]
- Chylack, L.T., Jr.; Wolfe, J.K.; Singer, D.M.; Leske, M.C.; Bullimore, M.A.; Bailey, I.L.; Friend, J.; McCarthy, D.; Wu, S.Y. The Lens Opacities Classification System III. The Longitudinal Study of Cataract Study Group. Arch. Ophthalmol. 1993, 111, 831–836. [Google Scholar] [CrossRef] [PubMed]
- Hashemi, H.; Pakzad, R.; Yekta, A.; Aghamirsalim, M.; Pakbin, M.; Ramin, S.; Khabazkhoob, M. Global and regional prevalence of age-related cataract: A comprehensive systematic review and meta-analysis. Eye 2020, 34, 1357–1370. [Google Scholar] [CrossRef]
- Ruan, X.; Liu, Z.; Luo, L.; Liu, Y. The Structure of the Lens and Its Associations with the Visual Quality. BMJ Open Ophthalmol. 2020, 5, e000459. [Google Scholar] [CrossRef] [PubMed]
- Pesudovs, K.; Lansingh, V.C.; Kempen, J.H.; Steinmetz, J.D.; Briant, P.S.; Varma, R.; Wang, N.; Jonas, J.; Resnikoff, S.; Taylor, H.R.; et al. Cataract-related blindness and vision impairment in 2020 and trends over time in relation to VISION 2020: The Right to Sight: An analysis for the Global Burden of Disease Study. Investig. Ophthalmol. Vis. Sci. 2021, 62, 3523. [Google Scholar]
- Lee, C.M.; Afshari, N.A. The global state of cataract blindness. Curr. Opin. Ophthalmol. 2017, 28, 98–103. [Google Scholar] [CrossRef]
- Lansingh, V.C.; Eckert, K.A. VISION 2020: The Right to Sight in 7 Years? Med. Hypothesis Discov. Innov. Ophthalmol. 2013, 2, 26–29. [Google Scholar]
- Ang, M.J.; Afshari, N.A. Cataract and systemic disease: A review. Clin. Exp. Ophthalmol. 2021, 49, 118–127. [Google Scholar] [CrossRef]
- Smeeth, L.; Boulis, M.; Hubbard, R.; Fletcher, A.E. A population based case-control study of cataract and inhaled corticosteroids. Br. J. Ophthalmol. 2003, 87, 1247–1251. [Google Scholar] [CrossRef]
- Ruigómez, A.; García Rodríguez, L.A.; Dev, V.J.; Arellano, F.; Raniwala, J. Are schizophrenia or antipsychotic drugs a risk factor for cataracts? Epidemiology 2000, 11, 620–623. [Google Scholar] [CrossRef]
- Prokofyeva, E.; Wegener, A.; Zrenner, E. Cataract prevalence and prevention in Europe: A literature review. Acta Ophthalmol. 2013, 91, 395–405. [Google Scholar] [CrossRef] [PubMed]
- Upaphong, P.; Thonusin, C.; Choovuthayakorn, J.; Chattipakorn, N.; Chattipakorn, S.C. The Possible Positive Mechanisms of Pirenoxine in Cataract Formation. Int. J. Mol. Sci. 2022, 23, 9431. [Google Scholar] [CrossRef] [PubMed]
- Muranov, K.; Poliansky, N.; Winkler, R.; Rieger, G.; Schmut, O.; Horwath-Winter, J. Protection by iodide of lens from selenite-induced cataract. Graefes Arch. Clin. Exp. Ophthalmol. 2004, 242, 146–151. [Google Scholar] [CrossRef] [PubMed]
- Cicinelli, M.V.; Buchan, J.C.; Nicholson, M.; Varadaraj, V.; Khanna, R.C. Cataracts. Lancet 2023, 401, 377–389. [Google Scholar] [CrossRef]
- Rautiainen, S.; Lindblad, B.E.; Morgenstern, R.; Wolk, A. Total antioxidant capacity of the diet and risk of age-related cataract: A population-based prospective cohort of women. JAMA Ophthalmol. 2014, 132, 247–252. [Google Scholar] [CrossRef]
- Tan, A.G.; Mitchell, P.; Flood, V.M.; Burlutsky, G.; Rochtchina, E.; Cumming, R.G.; Wang, J.J. Antioxidant nutrient intake and the long-term incidence of age-related cataract: The Blue Mountains Eye Study. Am. J. Clin. Nutr. 2008, 87, 1899–1905. [Google Scholar] [CrossRef]
- Christen, W.G.; Liu, S.; Glynn, R.J.; Gaziano, J.M.; Buring, J.E. Dietary carotenoids, vitamins C and E, and risk of cataract in women: A prospective study. Arch. Ophthalmol. 2008, 126, 102–109. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- García-Layana, A.; Ciufo, G.; Toledo, E.; Martínez-González, M.A.; Corella, D.; Fitó, M.; Estruch, R.; Gómez-Gracia, E.; Fiol, M.; Lapetra, J.; et al. The Effect of a Mediterranean Diet on the Incidence of Cataract Surgery. Nutrients 2017, 9, 453. [Google Scholar] [CrossRef]
- Jee, D.; Park, S. Hyperglycemia and Hypo-HDL-cholesterolemia Are Primary Risk Factors for Age-related Cataract, and a Korean-style Balanced Diet has a Negative Association, based on the Korean Genome and Epidemiology Study. J. Korean Med. Sci. 2021, 36, e155. [Google Scholar] [CrossRef] [PubMed]
- Amini, S.; Jafarirad, S.; Abiri, B.; Delgarm, P.; Mohamad-Zadeh, Y.; Ghomi, M.R.; Jahangirimehr, A. Traditional and Dairy Products and Vegetables Dietary Patterns Are Inversely Associated with the Risk of Cataract in the Middle Age and Aged Population: A Case-Control Study. J. Nutr. Health Aging 2021, 25, 1248–1254. [Google Scholar] [CrossRef]
- Chiu, T.H.T.; Chang, C.C.; Lin, C.L.; Lin, M.N. A Vegetarian Diet Is Associated with a Lower Risk of Cataract, Particularly Among Individuals with Overweight: A Prospective Study. J. Acad. Nutr. Diet 2021, 121, 669–677.E1. [Google Scholar] [CrossRef] [PubMed]
- Sedaghat, F.; Ghanavati, M.; Nezhad Hajian, P.; Hajishirazi, S.; Ehteshami, M.; Rashidkhani, B. Nutrient patterns and risk of cataract: A case-control study. Int. J. Ophthalmol. 2017, 10, 586–592. [Google Scholar] [CrossRef] [PubMed]
- Shivappa, N.; Hébert, J.R.; Rashidkhani, B.; Ghanavati, M. Inflammatory Potential of Diet is Associated with Increased Odds of Cataract in a Case-Control Study from Iran. Int. J. Vitam. Nutr. Res. 2017, 87, 17–24. [Google Scholar] [CrossRef]
- Pastor-Valero, M. Fruit and vegetable intake and vitamins C and E are associated with a reduced prevalence of cataract in a Spanish Mediterranean population. BMC Ophthalmol. 2013, 13, 52. [Google Scholar] [CrossRef]
- Theodoropoulou, S.; Samoli, E.; Theodossiadis, P.G.; Papathanassiou, M.; Lagiou, A.; Lagiou, P.; Tzonou, A. Diet and cataract: A case-control study. Int. Ophthalmol. 2014, 34, 59–68. [Google Scholar] [CrossRef]
- Huang, G.; Wu, L.; Qiu, L.; Lai, J.; Huang, Z.; Liao, L. Association between vegetables consumption and the risk of age-related cataract: A meta-analysis. Int. J. Clin. Exp. Med. 2015, 8, 18455–18461. [Google Scholar]
- Adachi, S.; Sawada, N.; Yuki, K.; Uchino, M.; Iwasaki, M.; Tsubota, K.; Tsugane, S. Intake of Vegetables and Fruits and the Risk of Cataract Incidence in a Japanese Population: The Japan Public Health Center-Based Prospective Study. J. Epidemiol. 2021, 31, 21–29. [Google Scholar] [CrossRef]
- Camacho-Barcia, L.; Bulló, M.; García-Gavilán, J.F.; Martínez-González, M.A.; Corella, D.; Estruch, R.; Fitó, M.; Gómez-Gracia, E.; Arós, F.; Fiol, M.; et al. Dairy products intake and the risk of incident cataracts surgery in an elderly Mediterranean population: Results from the PREDIMED study. Eur. J. Nutr. 2019, 58, 619–627. [Google Scholar] [CrossRef]
- Tan, A.G.; Flood, V.M.; Kifley, A.; Russell, J.; Cumming, R.G.; Mitchell, P.; Wang, J.J. Wholegrain and legume consumption and the 5-year incidence of age-related cataract in the Blue Mountains Eye Study. Br. J. Nutr. 2020, 124, 306–315. [Google Scholar] [CrossRef]
- Jiang, H.; Yin, Y.; Wu, C.R.; Liu, Y.; Guo, F.; Li, M.; Ma, L. Dietary vitamin and carotenoid intake and risk of age-related cataract. Am. J. Clin. Nutr. 2019, 109, 43–54. [Google Scholar] [CrossRef]
- Zhang, Y.; Jiang, W.; Xie, Z.; Wu, W.; Zhang, D. Vitamin E and risk of age-related cataract: A meta-analysis. Public Health Nutr. 2015, 18, 2804–2814. [Google Scholar] [CrossRef]
- Wei, L.; Liang, G.; Cai, C.; Lv, J. Association of vitamin C with the risk of age-related cataract: A meta-analysis. Acta Ophthalmol. 2016, 94, e170–e176. [Google Scholar] [CrossRef] [PubMed]
- Wang, A.; Han, J.; Jiang, Y.; Zhang, D. Association of vitamin A and β-carotene with risk for age-related cataract: A meta-analysis. Nutrition 2014, 30, 1113–1121. [Google Scholar] [CrossRef] [PubMed]
- Zheng Selin, J.; Rautiainen, S.; Lindblad, B.E.; Morgenstern, R.; Wolk, A. High-dose supplements of vitamins C and E, low-dose multivitamins, and the risk of age-related cataract: A population-based prospective cohort study of men. Am. J. Epidemiol. 2013, 177, 548–555. [Google Scholar] [CrossRef] [PubMed]
- Glaser, T.S.; Doss, L.E.; Shih, G.; Nigam, D.; Sperduto, R.D.; Ferris, F.L., 3rd; Agrón, E.; Clemons, T.E.; Chew, E.Y. The Association of Dietary Lutein plus Zeaxanthin and B Vitamins with Cataracts in the Age-Related Eye Disease Study: AREDS Report No. 37. Ophthalmology 2015, 122, 1471–1479. [Google Scholar] [CrossRef]
- Selin, J.Z.; Lindblad, B.E.; Bottai, M.; Morgenstern, R.; Wolk, A. High-dose B-vitamin supplements and risk for age-related cataract: A population-based prospective study of men and women. Br. J. Nutr. 2017, 118, 154–160. [Google Scholar] [CrossRef]
- Camacho-Barcia, M.L.; Bulló, M.; Garcia-Gavilán, J.F.; Ruiz-Canela, M.; Corella, D.; Estruch, R.; Fitó, M.; García-Layana, A.; Arós, F.; Fiol, M.; et al. Association of Dietary Vitamin K1 Intake With the Incidence of Cataract Surgery in an Adult Mediterranean Population: A Secondary Analysis of a Randomized Clinical Trial. JAMA Ophthalmol. 2017, 135, 657–661. [Google Scholar] [CrossRef]
- Bae, J.H.; Shin, D.S.; Lee, S.C.; Hwang, I.C. Sodium Intake and Socioeconomic Status as Risk Factors for Development of Age-Related Cataracts: The Korea National Health and Nutrition Examination Survey. PLoS ONE 2015, 10, e0136218. [Google Scholar] [CrossRef]
- Jee, D.; Kang, S.; Huang, S.; Park, S. Polygenetic-Risk Scores Related to Crystallin Metabolism Are Associated with Age-Related Cataract Formation and Interact with Hyperglycemia, Hypertension, Western-Style Diet, and Na Intake. Nutrients 2020, 12, 3534. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Jeong, M.; Jung, S.; Lee, M.; Yoo, S. The Relationship between Nutrient Intake and Cataracts in the Older Adult Population of Korea. Nutrients 2022, 14, 4962. [Google Scholar] [CrossRef] [PubMed]
- Yonova-Doing, E.; Forkin, Z.A.; Hysi, P.G.; Williams, K.M.; Spector, T.D.; Gilbert, C.E.; Hammond, C.J. Genetic and Dietary Factors Influencing the Progression of Nuclear Cataract. Ophthalmology 2016, 123, 1237–1244. [Google Scholar] [CrossRef] [PubMed]
- National Institutes of Health (NIH). Study Quality Assessment Tools. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 1 August 2023).
- Rishor-Olney, C.R.; Hinson, M.R. Mediterranean Diet. In StatPearls; StatPearls Publishing Copyright © 2023; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2023. [Google Scholar]
- Davis, C.; Bryan, J.; Hodgson, J.; Murphy, K. Definition of the Mediterranean Diet; A Literature Review. Nutrients 2015, 7, 9139–9153. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.-W. A journey to explore the health properties of traditional Korean diet: A commentary. J. Ethn. Foods 2023, 10, 9. [Google Scholar] [CrossRef]
- Kim, S.H.; Kim, M.S.; Lee, M.S.; Park, Y.S.; Lee, H.J.; Kang, S.-A.; Lee, H.S.; Lee, K.-E.; Yang, H.J.; Kim, M.J.; et al. Korean diet: Characteristics and historical background. J. Ethn. Foods 2016, 3, 26–31. [Google Scholar] [CrossRef]
- Hargreaves, S.M.; Raposo, A.; Saraiva, A.; Zandonadi, R.P. Vegetarian Diet: An Overview through the Perspective of Quality of Life Domains. Int. J. Environ. Res. Public Health 2021, 18, 4067. [Google Scholar] [CrossRef]
- Heidari, N.; Nabie, R.; Jabbari, M.; Irannejad Niri, Z.; Zeinalian, R.; Asghari Jafarabadi, M.; Arefhosseini, S.R. The association between food diversity and serum antioxidant indices in cataract patients compared to healthy subjects. J. Res. Med. Sci. 2021, 26, 59. [Google Scholar] [CrossRef]
- Pitsavos, C.; Panagiotakos, D.B.; Tzima, N.; Chrysohoou, C.; Economou, M.; Zampelas, A.; Stefanadis, C. Adherence to the Mediterranean diet is associated with total antioxidant capacity in healthy adults: The ATTICA study2. Am. J. Clin. Nutr. 2005, 82, 694–699. [Google Scholar] [CrossRef]
- Ghanavati, M.; Behrooz, M.; Rashidkhani, B.; Ashtray-Larky, D.; Zameni, S.D.; Alipour, M. Healthy Eating Index in Patients With Cataract: A Case-Control Study. Iran. Red. Crescent Med. J. 2015, 17, e22490. [Google Scholar] [CrossRef]
- Golafrouz, H.; Moghadam, F.A.; Eghtesadi, S. The association between Dietary Phytochemical Index and Mediterranean-style Dietary Pattern Score with the risk of cataract. PharmaNutrition 2023, 25, 100349. [Google Scholar] [CrossRef]
- Moïse, M.M.; Benjamin, L.M.; Doris, T.M.; Dalida, K.N.; Augustin, N.O. Role of Mediterranean diet, tropical vegetables rich in antioxidants, and sunlight exposure in blindness, cataract and glaucoma among African type 2 diabetics. Int. J. Ophthalmol. 2012, 5, 231–237. [Google Scholar] [CrossRef]
- Fan, H.; Han, X.; Shang, X.; Zhu, Z.; He, M.; Xu, G.; Chen, Z.; Deng, R. Fruit and vegetable intake and the risk of cataract: Insights from the UK Biobank study. Eye 2023, 37, 3234–3242. [Google Scholar] [CrossRef]
- Pearson, T.A.; Blair, S.N.; Daniels, S.R.; Eckel, R.H.; Fair, J.M.; Fortmann, S.P.; Franklin, B.A.; Goldstein, L.B.; Greenland, P.; Grundy, S.M.; et al. AHA Guidelines for Primary Prevention of Cardiovascular Disease and Stroke: 2002 Update. Circulation 2002, 106, 388–391. [Google Scholar] [CrossRef]
- Lăcătușu, C.M.; Grigorescu, E.D.; Floria, M.; Onofriescu, A.; Mihai, B.M. The Mediterranean Diet: From an Environment-Driven Food Culture to an Emerging Medical Prescription. Int. J. Environ. Res. Public Health 2019, 16, 942. [Google Scholar] [CrossRef] [PubMed]
- Haile, B.; Neme, K.; Belachew, T. Evolution of human diet and effect of globalization on regional diet with emphasis to the Mediterranean diet. Nutr. Food Sci. 2017, 47, 869–883. [Google Scholar] [CrossRef]


{kind=link}
| First Author, Date (Quality) | Design | Location | Sample Characteristic | ARC Type | Key Findings |
|---|---|---|---|---|---|
| ARC VS. DIETARY PATTERNS | |||||
| Mediterranean Diet (MedDiet) | |||||
| García-Layana et al. [20], 2017 (good) | Randomized Controlled Trial (RCT) | Spain | 5802 participants, from 55 to 80 years old | the type of cataract was not distinguished | The study did not reveal any significant difference between the MedDiet groups and the control group. Moreover, there was no decrease in the frequency of cataract surgery between the groups assigned to the MedDiet versus the control group. The observed rates (per 1000 person-years) were 16.9, 17.6, and 16.2 for the MedDiet + EVOO, MedDiet + Nuts, and control groups, respectively. |
| Traditional Korean balanced diet (KBD) | |||||
| Jee D, Park S. [21], 2021 (fair) | Cohort study | Korea | 40,262 participants (1972 ARC patients and 38,290 healthy controls), from 51 to 77 years old | the type of cataract was not distinguished | The study showed that in the MS groups only KBD consumption was inversely associated with the risk of ARC. Moreover, participants with a high KBD diet in the MS group had significantly lower ORs for ARC risk compared to those with a low KBD diet. Irrespective of MS, neither the rice-based diet or the WD diet patterns affected ARC risk. |
| Traditional and Dairy Products and Vegetable Dietary Patterns | |||||
| Amini et al. [22], 2021 (good) | Case-control study | Iran | 336 participants (168 patients with ARC and 168 healthy ones), from 40 to 80 years old | the type of cataract was not distinguished | The study demonstrated that dietary patterns referred to as “dairy products and vegetables” and “traditional” were inversely associated with cataracts. Participants who consumed a high “carbohydrate and simple sugar” diet had higher ORs for risk of cataracts compared to those with a low intake. There was no significant association between the “nuts, seeds and simple sugar” dietary pattern and cataracts. |
| Vegetarian diet | |||||
| Chiu et al. [23], 2020 (good) | Cohort study | Taiwan | 4436 participants (1341 vegetarians and 3095 nonvegetarian), aged over 40 | the type of cataract was not distinguished | The study found that a vegetarian diet was associated with a 20% reduced risk of cataracts. This association was more pronounced among individuals who were overweight. |
| Nutrient patterns | |||||
| Sedaghat et al. [24], 2017 (good) | Case-control study | Iran | 295 participants (97 cataract patients and 198 matched controls), from 48 to 67 years old | the type of cataract was not distinguished | The study indicated that participants who consumed high “sodium pattern” and high “fatty acid pattern” diets had higher ORs for risk of cataract compared to subjects with low consumption. No significant association was observed between the “mixed pattern” diet and cataracts. Both “antioxidant pattern” and “omega-3 pattern” diets were negatively associated with the prevalence of cataracts. |
| Pro-inflammatory diet | |||||
| Shivappa et al. [25], 2017 (good) | Case-control study | Iran | 295 participants (97 cataract cases and 198 healthy controls), from 48 to 67 years old | the type of cataract was not distinguished | The study showed a positive association between DII and cataract incidence as well as E-DII and the risk of cataracts. |
| CATARACT VS. DIETARY PRODUCTS | |||||
| Fruit and vegetable | |||||
| Pastor-Valero [26], 2013 (good) | Cross-sectional study | Spain | 593 participants (274 men and 319 women) enrolled in the EUREYE study, aged over 65 | the type of cataract was not distinguished | The study showed that a higher combined consumption of fruit and vegetables was significantly and negatively associated with the odds of cataract development. No association was found in separate analyses of the intake of fruit or vegetables and prevalence of cataracts. |
| Theodoropoulou et al. [27], 2014 (good) | Case–control study | Greece | 628 participants (314 cataract cases and 314 controls), from 45 to 85 years old | nuclear, cortical, posterior subcapsular cataract | The study found that, unlike higher meat intake, increased consumption of plant-based products, such as vegetables, fruit, starchy products, legumes, nuts, and fish was significantly and negatively associated with the risk of cataracts. There was no significant association between the consumption of cereals, dairy products, added lipids and cataract risk. |
| Huang et al. [28], 2015 (good) | Meta-analysis | USA, Nigeria, Spain, Australia, Italy, Greece | 9 articles involving 6464 cataract cases and 11,2447 participants | the type of cataract was not distinguished | The study showed that the highest vegetable intake, when compared to the lowest, was significantly and negatively associated with the risk of cataracts. In a stratified analysis of research design, relationships were also discovered in case–control studies and cohort studies. The highest vegetable consumption, as opposed to the lowest consumption, was significantly related to the risk of ARC in America and Europe, but not in other regions of the world. |
| Adachi et al. [29], 2021 (good) | Cohort study | Japan | 71,720 participants (32,387 men and 39,333 women) from 45 to 74 years old | the type of cataract was not distinguished | The study revealed that male participants who consumed high rather than low amounts of total vegetables and cruciferous vegetables had a significantly lower prevalence of ARC. This association was more pronounced in men over 60 years old than in younger men. In female participants, the opposite results were observed. |
| Dairy products | |||||
| Camacho-Barcia et al. [30], 2019 (fair) | RCT | Spain | 5860 participants, men from 55 to 80 years old and women from 60 to 80 years old, enrolled in the PREDIMED Study | the type of cataract was not distinguished | The study showed that participants with a higher intake of skimmed yoghurt had an inverse association with the risk of cataract surgery. The second tertile of total yogurt intake also indicated a negative association with cataract risk. |
| Wholegrain and legume foods | |||||
| Tan et al. [31], 2020 (good) | Cohort study | Australia | the baseline: 3654 participants; five years later: 2334 participants; ten years later: 1952 participants from BMES, aged over 49 years old | nuclear, cortical, posterior subcapsular cataract | The study did not find any significant associations between total wholegrain consumption or the consumption of any specific source of whole grain and any type of cataract incidence. There was no significant trend of a relationship between the highest and the lowest intake of legumes for PSC cataract incidence. No associations were found between pulse consumption and the incidence of cortical or nuclear cataract. |
| CATARACT VS. VITAMINS, MINERALS AND CAROTENOIDS | |||||
| Antioxidants | |||||
| Jiang et al. [32], 2019 (good) | Meta-analysis | USA, Australia, Finland, Canada, Puerto Rico, Japan, | 8 RCTs and 12 cohort studies in total including 385,107 participants, aged over 40 | nuclear, cortical, posterior subcapsular cataract | The study demonstrated that in RCTs, neither vitamin E or β-carotene supplements, when compared with the placebo, had any significant beneficial effect on the risk of ARC. Analyses of cohort studies showed that the highest levels of vitamins A and E, as compared with the lowest levels, were associated with a 19% and 10% decrease in the risk of ARC. An increase in vitamin A intake of 5 mg per day was associated with a 6% decrease in the risk of ARC. An increase in vitamin C consumption of 500 mg per day was significantly associated with an 18% decrease in the risk of ARC. The highest intake of β-carotene, as well as lutein or zeaxanthin, as opposed to the lowest intake, was associated with a 10% and 19% decrease in the risk of ARC. An increase in β-carotene consumption of 5 mg per day and in lutein or zeaxanthin consumption of 10 mg per day was significantly associated with an 8% and 26% decrease in the risk of ARC. No significant association was found between total carotenoid, α-carotene, and β-cryptoxantin intake and the risk of ARC. |
| Zhang et al. [33], 2015 (good) | Meta-analysis | USA, Australia, Finland, Sweden, Italy, Greece, Spain | 18 articles (8 case-control studies, 5 RCTs, 4 cohort studies, 1 cross-sectional study) including 12,542 cataract cases | nuclear, cortical, posterior subcapsular cataract | The study showed that the highest compared to the lowest dietary vitamin E intake, as well as combined dietary and supplemental vitamin E intake, were statistically significantly associated with the risk of ARC. There was no significant association between solely supplemental vitamin E intake and risk of ARC. Dose-response analysis of dietary vitamin E intake and ARC risk found a statistically significant decreased risk of developing ARC with increasing dietary vitamin E intake from 7 mg/d. |
| Wei et al. [34], 2016 (good) | Meta-analysis | USA, Spain, Japan, Sweden, Italy, India, Australia | 15 articles (11 prospective studies, 7 case-control studies, 1 RCT and 1 cross-sectional study) including 16,205 cataract cases | nuclear, cortical, posterior subcapsular cataract | The study revealed that the highest dietary vitamin C intake, as compared to the lowest intake of this vitamin, was significantly associated with the risk of cataracts. Subgroup analyses by study design suggest that the association between the highest compared to the lowest consumption of vitamin C and cataract risk was significant in the case-control studies only. In subgroup analyses based on geographic locations, significant associations were observed in both Asia and America, but not in Europe. In the subgroup analysis by cataract type, a significant association was found only in nuclear cataract. |
| Wang et al. [35], 2014 (good) | Meta-analysis | USA, Finland, Australia, Spain and Italy | - 12 articles with 17 studies including 7038 cataract cases for β-carotene intake - 6 articles with 11 studies including 5553 cataract cases for vitamin A intake | nuclear, cortical, posterior subcapsular cataract | The study showed that the highest consumption of β-carotene as well as vitamin A, as compared to the lowest consumption of these vitamins, was significantly associated with the risk of cataracts. For both β-carotene and vitamin A, the association was significant only in prospective studies. In the subgroup analysis by cataract type, a significant association was found only between β-carotene consumption and PSC. The study found no significant association between vitamin A intake and the risk of any specific type of cataract. |
| Zheng Selin et al. [36], 2013 (good) | Cohort study | Sweden | 31,120 Swedish men, from 45 to 79 years old | the type of cataract was not distinguished | The study demonstrated that in the multivariable analysis, the use of only vitamin C and the use of only vitamin E supplements, when compared to non-supplement-use, were associated with a higher risk of cataracts. The multivariable-adjusted hazard ratios for male participants who took other supplements in addition to vitamin C or vitamin E, in contrast to non-supplement-users, were also associated with a higher risk of cataracts. Vitamin C or vitamin E from the diet were not associated with cataract risk. |
| Vitamin B | |||||
| Glaser et al. [37], 2015 (good) | Baseline cross-sectional and prospective cohort study | USA | 3115 patients (6129 eyes) enrolled in the Age-Related Eye Disease Study, from 55 to 80 years old, followed up for mean of 9.6 years | nuclear, cortical, posterior subcapsular cataract | The study showed that the highest dietary consumption of vitamin B2, compared to the lowest, was associated with a 22% and 38% lower prevalence of mild and moderate nuclear cataracts and a 20% lower prevalence of mild cortical cataract, respectively. The highest dietary consumption of vitamin B12, compared to the lowest, was associated with a 22% and 38% lower prevalence of mild and moderate nuclear cataracts and a 23% lower prevalence of mild cortical cataract. A 33% decrease in the prevalence of moderate nuclear cataract was found in the highest quintile of vitamin B6 consumption. Niacin was linked to a 31% lower risk of mild nuclear cataract in Centrum® non-users, and vitamin B12 was linked to a 44% lower risk of mild cortical cataract. Users of Centrum® who reported consuming the most folate had a 61% higher chance of developing at least a mild PSC cataract compared to those who consumed the least folate. |
| Selin et al. [38], 2017 (good) | Cohort study | Sweden | 13,757 women from the Swedish Mammography Cohort, from 48 to 83 years old and 22,823 men from the Cohort of Swedish Men, from 45 to 79 years old | the type of cataract was not distinguished | Participants who used supplements of vitamin B, either separately or in combination with other supplements, had a significantly higher risk of cataract incidence than non-supplement-users. In the youngest age group (under 60 years old), the use of B vitamins alone was related to a significantly increased risk of cataract incidence. |
| Vitamin K | |||||
| Camacho-Barcia et al. [39], 2017 (fair) | Secondary analysis of an RCT | Spain | 5860 participants (2590 men and 3270 women), from 60 to 72 years old | the type of cataract was not distinguished | The study showed that the highest dietary intake of vitamin K1, when compared to the lowest, was associated with a 25% lower risk of cataract surgery. |
| Others | |||||
| Bae et al. [40], 2015 (fair) | Cross-sectional case-control study | Korea | 12,693 participants, (2687 with cataracts aged from 51 years old and 10,006 controls) from KNHANES | nuclear, cortical, posterior subcapsular cataract | The study demonstrated that the prevalence of cataract incidence was significantly associated with high U[Na+] to Cr ratio in participants over 50. |
| Jee et al. [41], 2020 (fair) | Cohort study | Korea | 41,067 participants (1972 with cataracts and 39,095 controls) aged over 50 years old | the type of cataract was not distinguished | The study revealed an association between sodium and coffee intake, as well as a Western-style diet and genetic risk in ARC development. |
| Lee et al. [42], 2022 (fair) | Cross-sectional study | Korea | 5634 participants among whom 2137 had cataracts and 3497 did not, aged over 60 years old | the type of cataract was not distinguished | The study indicated that in male participants, higher consumption of both vitamin B1 and water was associated with a lower prevalence of cataracts. Among female participants, consumption of polyunsaturated fatty acids and vitamin A was inversely associated with the prevalence of cataracts. Likewise, lower consumption of vitamin B3 and sugar was linked to a higher prevalence of cataracts. Moreover, an increase in vitamin B2 consumption was correlated with an increase in the prevalence of cataracts. |
| Yonova-Doing et al. [43], 2016 (fair) | Cohort study | United Kingdom | 324 female twin participants (151 monozygotic and 173 dizygotic twins), from 58 to 83 years old | nuclear cataract | The study showed that at baseline, NDS was significantly related to vitamin C and manganese. However, the association with cataract progression was only found for vitamin C. The highest consumption of vitamin C and manganese, as compared to the lowest, was associated with a 19% and 20% risk reduction at baseline, respectively. The highest consumption of vitamin C, compared to the lowest, was also associated with a 33% risk reduction in cataract progression. Only micronutrient supplements remained significant in the multivariate model, and their intake led to an 18% risk reduction in people within the highest tertile of nutrient intake, compared with the lowest. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Falkowska, M.; Młynarczyk, M.; Micun, Z.; Konopińska, J.; Socha, K. Influence of Diet, Dietary Products and Vitamins on Age-Related Cataract Incidence: A Systematic Review. Nutrients 2023, 15, 4585. https://doi.org/10.3390/nu15214585
Falkowska M, Młynarczyk M, Micun Z, Konopińska J, Socha K. Influence of Diet, Dietary Products and Vitamins on Age-Related Cataract Incidence: A Systematic Review. Nutrients. 2023; 15(21):4585. https://doi.org/10.3390/nu15214585
Chicago/Turabian StyleFalkowska, Martyna, Maryla Młynarczyk, Zuzanna Micun, Joanna Konopińska, and Katarzyna Socha. 2023. "Influence of Diet, Dietary Products and Vitamins on Age-Related Cataract Incidence: A Systematic Review" Nutrients 15, no. 21: 4585. https://doi.org/10.3390/nu15214585
APA StyleFalkowska, M., Młynarczyk, M., Micun, Z., Konopińska, J., & Socha, K. (2023). Influence of Diet, Dietary Products and Vitamins on Age-Related Cataract Incidence: A Systematic Review. Nutrients, 15(21), 4585. https://doi.org/10.3390/nu15214585