
Omega-3 Polyunsaturated Fatty Acid Levels in Maternal and Cord Plasma Are Associated with Maternal Socioeconomic Status

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participant Recruitment and Biological Sample Collection
2.2. Polyunsaturated Fatty Acid Laboratory Analysis
2.3. Demographic Data and Questionnaires
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
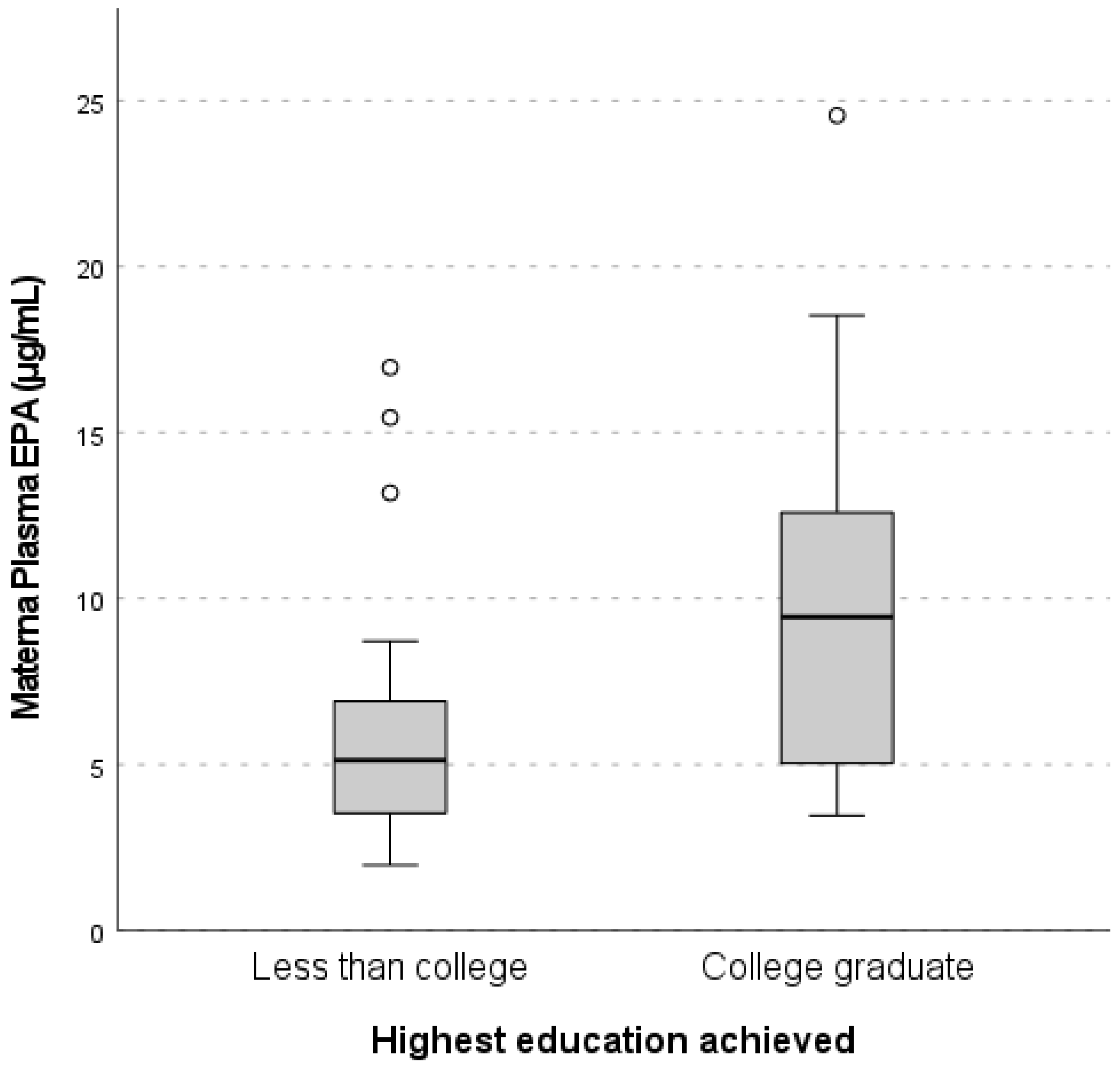
3.2. Maternal Education Level, and Plasma n-3 and n-6 PUFA Concentrations
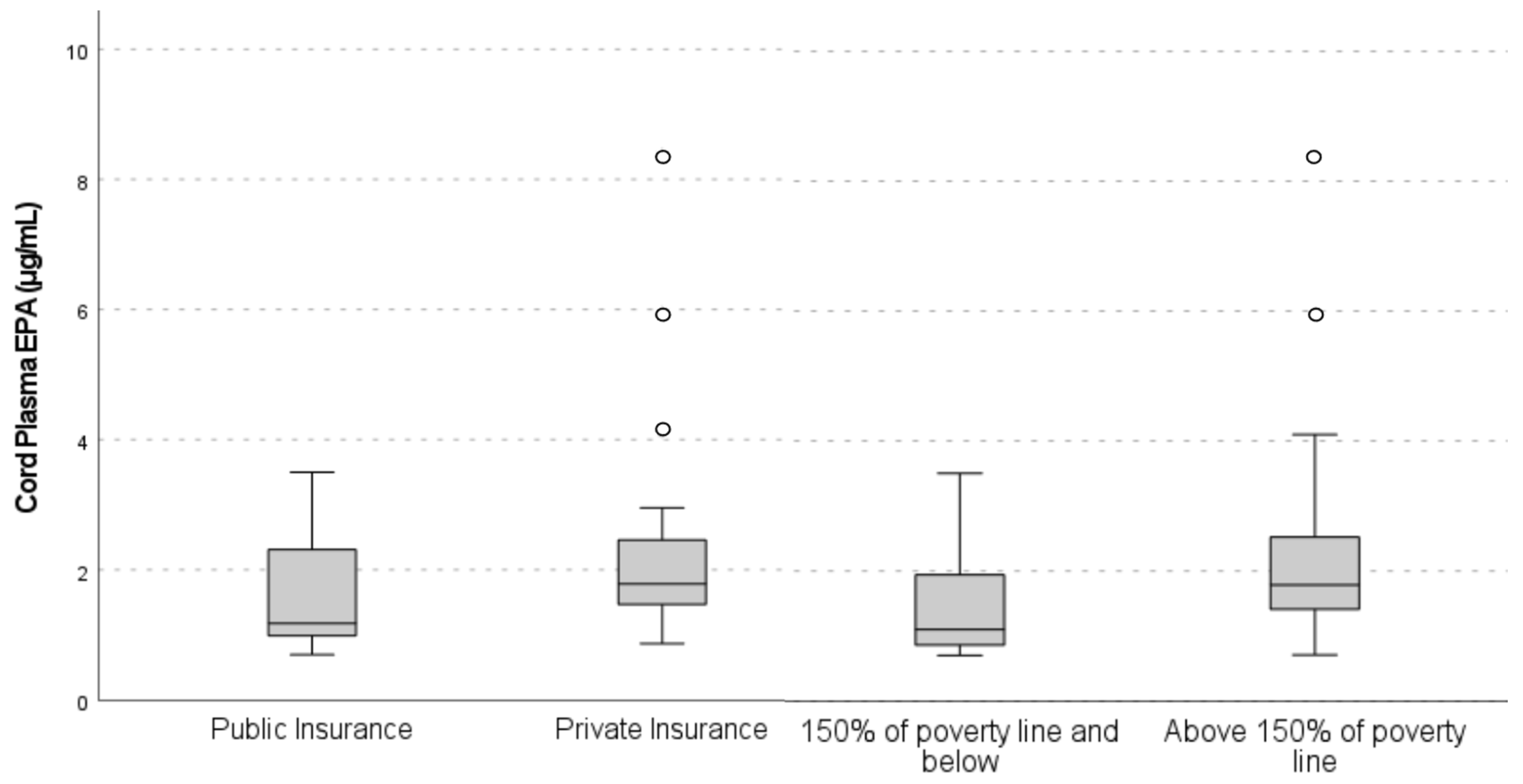
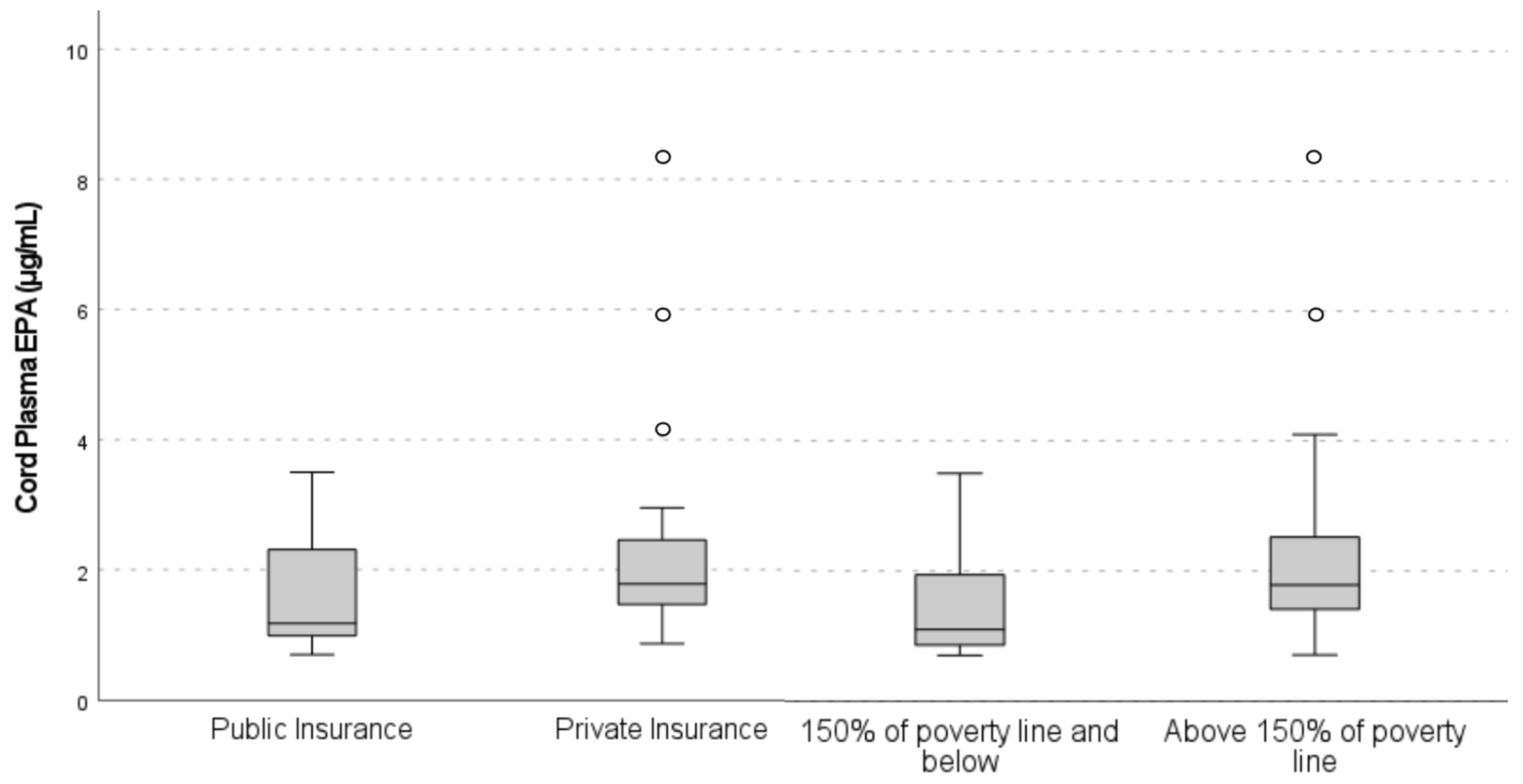
3.3. Maternal Economic Level, and Plasma n-3 and n-6 PUFA Concentrations
3.4. Maternal Dietary Intake of n-3 and n-6 PUFAs, and Intake Comparison among SES Categories
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mallick, R.; Basak, S.; Duttaroy, A.K. Docosahexaenoic acid,22:6n-3: Its roles in the structure and function of the brain. Int. J. Dev. Neurosci. 2019, 79, 21–31. [Google Scholar] [CrossRef]
- Cave, C.; Hein, N.; Smith, L.M.; Anderson-Berry, A.; Richter, C.K.; Bisselou, K.S.; Appiah, A.K.; Kris-Etherton, P.; Skulas-Ray, A.C.; Thompson, M.; et al. Omega-3 Long-Chain Polyunsaturated Fatty Acids Intake by Ethnicity, Income, and Education Level in the United States: NHANES 2003–2014. Nutrients 2020, 12, 2045. [Google Scholar] [CrossRef]
- Shrestha, N.; Sleep, S.L.; Cuffe, J.S.; Holland, O.J.; Perkins, A.V.; Yau, S.Y.; McAinch, A.J.; Hryciw, D.H. Role of omega-6 and omega-3 fatty acids in fetal programming. Clin. Exp. Pharmacol. Physiol. 2020, 47, 907–915. [Google Scholar] [CrossRef]
- Middleton, P.; Gomersall, J.C.; Gould, J.F.; Shepherd, E.; Olsen, S.F.; Makrides, M. Omega-3 fatty acid addition during pregnancy. Cochrane Database Syst. Rev. 2018, 11, Cd003402. [Google Scholar] [CrossRef]
- Van Dael, P. Role of n-3 long-chain polyunsaturated fatty acids in human nutrition and health: Review of recent studies and recommendations. Nutr. Res. Pract. 2021, 15, 137–159. [Google Scholar] [CrossRef]
- Hsu, M.-C.; Tung, C.-Y.; Chen, H.-E. Omega-3 polyunsaturated fatty acid supplementation in prevention and treatment of maternal depression: Putative mechanism and recommendation. J. Affect. Disord. 2018, 238, 47–61. [Google Scholar] [CrossRef]
- Oken, E.; Ning, Y.; Rifas-Shiman, S.L.; Rich-Edwards, J.W.; Olsen, S.F.; Gillman, M.W. Diet during pregnancy and risk of preeclampsia or gestational hypertension. Ann. Epidemiol. 2007, 17, 663–668. [Google Scholar] [CrossRef] [PubMed]
- Szczuko, M.; Kikut, J.; Komorniak, N.; Bilicki, J.; Celewicz, Z.; Ziętek, M. The Role of Arachidonic and Linoleic Acid Derivatives in Pathological Pregnancies and the Human Reproduction Process. Int. J. Mol. Sci. 2020, 21, 9628. [Google Scholar] [CrossRef]
- Perucci, L.O.; Santos, T.A.P.; Santos, P.C.; Teixeira, L.C.R.; Alpoim, P.N.; Gomes, K.B.; Sousa, L.P.; Dusse, L.M.S.; Talvani, A. Pre-eclampsia is associated with reduced resolvin D1 and maresin 1 to leukotriene B4 ratios in the plasma. Am. J. Reprod. Immunol. 2020, 83, e13206. [Google Scholar] [CrossRef]
- Burdge, G.C.; Calder, P.C. Conversion of alpha-linolenic acid to longer-chain polyunsaturated fatty acids in human adults. Reprod. Nutr. Dev. 2005, 45, 581–597. [Google Scholar] [CrossRef]
- Omega-3 Fatty Acids. Fact Sheet for Health Professionals. 15 February 2023. Available online: https://ods.od.nih.gov/factsheets/Omega3FattyAcids-HealthProfessional/ (accessed on 10 July 2023).
- Wall, R.; Ross, R.P.; Fitzgerald, G.F.; Stanton, C. Fatty acids from fish: The anti-inflammatory potential of long-chain omega-3 fatty acids. Nutr. Rev. 2010, 68, 280–289. [Google Scholar] [CrossRef]
- Mariamenatu, A.H.; Abdu, E.M. Overconsumption of Omega-6 Polyunsaturated Fatty Acids (PUFAs) versus Deficiency of Omega-3 PUFAs in Modern-Day Diets: The Disturbing Factor for Their “Balanced Antagonistic Metabolic Functions” in the Human Body. J. Lipids 2021, 2021, 8848161. [Google Scholar] [CrossRef] [PubMed]
- Meyer, B.J.; Mann, N.J.; Lewis, J.L.; Milligan, G.C.; Sinclair, A.J.; Howe, P.R.C. Dietary intakes and food sources of omega-6 and omega-3 polyunsaturated fatty acids. Lipids 2003, 38, 391–398. [Google Scholar] [CrossRef]
- Burdge, G.C. Metabolism of alpha-linolenic acid in humans. Prostaglandins Leukot Essent Fat. Acids 2006, 75, 161–168. [Google Scholar] [CrossRef]
- Burdge, G.C.; Wootton, S.A. Conversion of alpha-linolenic acid to eicosapentaenoic, docosapentaenoic and docosahexaenoic acids in young women. Br. J. Nutr. 2002, 88, 411–420. [Google Scholar] [CrossRef] [PubMed]
- Cholewski, M.; Tomczykowa, M.; Tomczyk, M. A Comprehensive Review of Chemistry, Sources and Bioavailability of Omega-3 Fatty Acids. Nutrients 2018, 10, 1662. [Google Scholar] [CrossRef] [PubMed]
- Thompson, M.; Hein, N.; Hanson, C.; Smith, L.M.; Anderson-Berry, A.; Richter, C.K.; Bisselou, K.S.; Appiah, A.K.; Kris-Etherton, P.; Skulas-Ray, A.C.; et al. Omega-3 Fatty Acid Intake by Age, Gender, and Pregnancy Status in the United States: National Health and Nutrition Examination Survey 2003–2014. Nutrients 2019, 11, 177. [Google Scholar] [CrossRef]
- Kim, K.-B.; Nam, Y.A.; Kim, H.S.; Hayes, A.W.; Lee, B.-M. α-Linolenic acid: Nutraceutical, pharmacological and toxicological evaluation. Food Chem. Toxicol. 2014, 70, 163–178. [Google Scholar] [CrossRef] [PubMed]
- Dwarkanath, P.; Muthayya, S.; Thomas, T.; Vaz, M.; Parikh, P.; Mehra, R.; Kurpad, A.V. Polyunsaturated fatty acid consumption and concentration among South Indian women during pregnancy. Asia Pac. J. Clin. Nutr. 2009, 18, 389–394. [Google Scholar]
- Richter, C.K.; Bisselou, K.S.; Nordgren, T.M.; Smith, L.; Appiah, A.K.; Hein, N.; Anderson-Berry, A.; Kris-Etherton, P.; Hanson, C.; Skulas-Ray, A.C. n-3 Docosapentaenoic Acid Intake and Relationship with Plasma Long-Chain n-3 Fatty Acid Concentrations in the United States: NHANES 2003–2014. Lipids 2019, 54, 221–230. [Google Scholar] [CrossRef]
- Nordgren, T.M.; Lyden, E.; Anderson-Berry, A.; Hanson, C. Omega-3 Fatty Acid Intake of Pregnant Women and Women of Childbearing Age in the United States: Potential for Deficiency? Nutrients 2017, 9, 197. [Google Scholar] [CrossRef]
- Richter, C.K.; Bowen, K.J.; Mozaffarian, D.; Kris-Etherton, P.M.; Skulas-Ray, A.C. Total Long-Chain n-3 Fatty Acid Intake and Food Sources in the United States Compared to Recommended Intakes: NHANES 2003–2008. Lipids 2017, 52, 917–927. [Google Scholar] [CrossRef]
- Xie, L.; Innis, S.M. Genetic variants of the FADS1 FADS2 gene cluster are associated with altered (n-6) and (n-3) essential fatty acids in plasma and erythrocyte phospholipids in women during pregnancy and in breast milk during lactation. J. Nutr. 2008, 138, 2222–2228. [Google Scholar] [CrossRef]
- Simopoulos, A.P. Evolutionary aspects of diet, the omega-6/omega-3 ratio and genetic variation: Nutritional implications for chronic diseases. Biomed. Pharmacother. 2006, 60, 502–507. [Google Scholar] [CrossRef] [PubMed]
- Pinto, T.J.P.; Farias, D.R.; Rebelo, F.; Lepsch, J.; Vaz, J.S.; Moreira, J.D.; Cunha, G.M.; Kac, G. Lower inter-partum interval and unhealthy life-style factors are inversely associated with n-3 essential fatty acids changes during pregnancy: A prospective cohort with Brazilian women. PLoS ONE 2015, 10, e0121151. [Google Scholar] [CrossRef]
- Woodard, V.; Thoene, M.; Van Ormer, M.; Thompson, M.; Hanson, C.; Natarajan, S.K.; Mukherjee, M.; Yuil-Valdes, A.; Nordgren, T.M.; Ulu, A.; et al. Intrauterine Transfer of Polyunsaturated Fatty Acids in Mother-Infant Dyads as Analyzed at Time of Delivery. Nutrients 2021, 13, 996. [Google Scholar] [CrossRef]
- Aparicio, E.; Martín-Grau, C.; Bedmar, C.; Orus, N.S.; Basora, J.; Arija, V.; The ECLIPSES Study Group. Maternal Factors Associated with Levels of Fatty Acids, Specifically n-3 PUFA during Pregnancy: ECLIPSES Study. Nutrients 2021, 13, 317. [Google Scholar] [CrossRef]
- Stark, K.D.; Beblo, S.; Murthy, M.; Whitty, J.E.; Buda-Abela, M.; Janisse, J.; Rockett, H.; Martier, S.S.; Sokol, R.J.; Hannigan, J.H.; et al. Alcohol Consumption in Pregnant, Black Women Is Associated With Decreased Plasma and Erythrocyte Docosahexaenoic Acid. Alcohol Clin. Exp. Res. 2005, 29, 130–140. [Google Scholar] [CrossRef] [PubMed]
- Cohen, B.E.; Garg, S.K.; Ali, S.; Harris, W.S.; Whooley, M.A. Red Blood Cell Docosahexaenoic Acid and Eicosapentaenoic Acid Concentrations Are Positively Associated with Socioeconomic Status in Patients with Established Coronary Artery Disease: Data from the Heart and Soul Study12. J. Nutr. 2008, 138, 1135–1140. [Google Scholar] [CrossRef]
- Lim, S.; Beauchamp, A.; Dodson, S.; O’Hara, J.; McPhee, C.; Fulton, A.; Wildey, C.; Osborne, R.H. Health literacy and fruit and vegetable intake in rural Australia. Public Health Nutr. 2017, 20, 2680–2684. [Google Scholar] [CrossRef] [PubMed]
- Conway, M.C.; McSorley, E.M.; Mulhern, M.S.; Strain, J.J.; van Wijngaarden, E.; Yeates, A.J. Influence of fatty acid desaturase (FADS) genotype on maternal and child polyunsaturated fatty acids (PUFA) status and child health outcomes: A systematic review. Nutr. Rev. 2020, 78, 627–646. [Google Scholar] [CrossRef] [PubMed]
- Schuchardt, J.P.; Hahn, A. Bioavailability of long-chain omega-3 fatty acids. Prostaglandins Leukot. Essent. Fat. Acids 2013, 89, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Simopoulos, A.P. Genetic variants in the metabolism of omega-6 and omega-3 fatty acids: Their role in the determination of nutritional requirements and chronic disease risk. Exp. Biol. Med. 2010, 235, 785–795. [Google Scholar] [CrossRef]
- Cole, S.W. Social Regulation of Human Gene Expression. Curr. Dir. Psychol. Sci. 2009, 18, 132–137. [Google Scholar] [CrossRef]
- Chen, E.; E Miller, G.; A Walker, H.; Arevalo, J.M.; Sung, C.Y.; Cole, S.W. Genome-wide transcriptional profiling linked to social class in asthma. Thorax 2009, 64, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Koletzko, B.; Demmelmair, H.; Schaeffer, L.; Illig, T.; Heinrich, J. Genetically determined variation in polyunsaturated fatty acid metabolism may result in different dietary requirements. Nestle Nutr. Workshop Ser. Pediatr. Program 2008, 62, 35–44; discussion 44–49. [Google Scholar]
- Haggarty, P. Fatty Acid Supply to the Human Fetus. Annu. Rev. Nutr. 2010, 30, 237–255. [Google Scholar] [CrossRef] [PubMed]
- McKinnon, L.; Giskes, K.; Turrell, G. The contribution of three components of nutrition knowledge to socio-economic differences in food purchasing choices. Public Health Nutr. 2014, 17, 1814–1824. [Google Scholar] [CrossRef]
- Hakli, G.; Asil, E.; Ucar, A.; Ozdogan, Y.; Yilmaz, M.V.; Ozcelik, A.O.; Surucuoglu, M.S.; Cakiroglu, F.P.; Akan, L.S. Nutritional knowledge and behavior of adults: Their relations with sociodemographic factors. Pak. J. Nutr. 2016, 15, 532. [Google Scholar] [CrossRef]
- Jahns, L.; Raatz, S.K.; Johnson, L.K.; Kranz, S.; Silverstein, J.T.; Picklo, M.J. Intake of Seafood in the US Varies by Age, Income, and Education Level but Not by Race-Ethnicity. Nutrients 2014, 6, 6060–6075. [Google Scholar] [CrossRef]
- Hoge, A.; Bernardy, F.; Donneau, A.-F.; Dardenne, N.; Degée, S.; Timmermans, M.; Nisolle, M.; Guillaume, M.; Castronovo, V. Low omega-3 index values and monounsaturated fatty acid levels in early pregnancy: An analysis of maternal erythrocytes fatty acids. Lipids Health Dis. 2018, 17, 63. [Google Scholar] [CrossRef] [PubMed]
- Medicine, I.O. Dietary Reference Intakes (DRIs): Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein, and Amino Acids (Macronutrients); National Academies Press Washington: Washington, DC, USA, 2004. [Google Scholar]
- Food and Agriculture Organization of the United Nations. Fats and fatty acids in human nutrition. Report of an expert consultation. FAO Food Nutr. Pap. 2010, 91, 1–166. [Google Scholar]
- Zahn, C.M.; Zahn, J.R.W.; El-Sayed, Y.Y.; Ecker, J.L. Update on Seafood Consumption during Pregnancy. March 2020. [Practice Advisory]. Available online: https://www.acog.org/clinical/clinical-guidance/practice-advisory/articles/2017/01/update-on-seafood-consumption-during-pregnancy# (accessed on 21 July 2023).
- Schuchardt, J.P.; Cerrato, M.; Ceseri, M.; DeFina, L.F.; Delgado, G.E.; Gellert, S.; Hahn, A.; Howard, B.V.; Kadota, A.; Kleber, M.E.; et al. Red blood cell fatty acid patterns from 7 countries: Focus on the Omega-3 index. Prostaglandins Leukot Essent Fat. Acids 2022, 179, 102418. [Google Scholar] [CrossRef] [PubMed]
- Sedgwick, P. Non-response bias versus response bias. BMJ Br. Med. J. 2014, 348, g2573. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Participant Characteristic | N | Median (IQR) |
|---|---|---|
| Maternal age (years) | 55 | 30 (24–34) |
| Corrected gestational age at birth (weeks) | 55 | 39.3 (36.7–40) |
| Infant birth weight (g) | 55 | 3313 (2540–2714) |
| Infant birth head circumference (cm) | 55 | 33.7 (32.4–35.6) |
| Infant birth length (cm) | 54 | 49.0 (46.7–50.8) |
| Maternal pre-pregnancy BMI (kg/m2) | 51 | 27.5 (22.0–33.0) |
| N | % | |
| Infant sex | ||
| Male | 28 | 50.9 |
| Female | 27 | 49.1 |
| Maternal race | ||
| White | 32 | 58.2 |
| African American | 11 | 20.0 |
| Hispanic | 6 | 10.9 |
| Asian or Pacific Islander | 1 | 1.8 |
| Other/unknown | 5 | 9.1 |
| Pre-eclampsia | ||
| Yes | 8 | 14.5 |
| No | 47 | 85.5 |
| Maternal diabetes | ||
| Yes | 5 | 9.1 |
| No | 50 | 90.9 |
| Infant NICU admission | ||
| Yes | 17 | 30.9 |
| No | 38 | 69.1 |
| Maternal smoking status | ||
| Never smoked | 44 | 80.0 |
| Current smoker | 1 | 1.8 |
| Former smoker | 10 | 18.2 |
| Maternal Insurance Type | ||
| Public | 25 | 45.5 |
| Private | 30 | 54.5 |
| Maternal highest education | ||
| Less than college | 26 | 47.3 |
| College graduate | 22 | 40.0 |
| Did not complete survey | 7 | 12.7 |
| Maternal annual income | ||
| ≤150% of poverty line | 10 | 18.2 |
| >150% of poverty line | 26 | 47.3 |
| “Unknown” | 12 | 21.8 |
| Did not complete survey | 7 | 12.7 |
| Nutrient | N | Median Plasma Level (µg/mL; IQR)—Entire Cohort | N | Median Plasma Level (µg/mL; IQR)—Higher-Education Group | N | Median Plasma Level (µg/mL; IQR)—Lower-Education Group | ||
|---|---|---|---|---|---|---|---|---|
| α-Linolenic acid (ALA) | 55 | 30.7 (25.6–39.5) | 22 | 29.59 (25.21–39.41) | 26 | 33.87 (26.83–41.29) | ||
| Arachidonic acid (AA) | 55 | 242.4 (25.6–39.5) | 22 | 253.64 (217.79–288.36) | 26 | 219.28 (195.64–295.71) | ||
| Docosahexaenoic acid (DHA) | 55 | 62.5 (51.3–80.6) | 22 | 66.84 (58.11–86.95) | 26 | 59.56 (46.97–75.59) | ||
| Docosapentaenoic-n3 acid (DPA) | 55 | 9.3 (7.4–12.2) | 22 | 9.90 (8.33–12.77) | 26 | 9.36 (6.96–11.97) | ||
| Eicosapentaenoic acid (EPA) | 55 | 5.57 (3.9–9.5) | 22 | 9.44 (5.02–12.60) | 26 | 5.13 (3.45–6.98) | ||
| Linoleic acid (LA) | 55 | 1349.6 (1191.2–1594.9) | 22 | 1331.41 (1208.76–1617.27) | 26 | 1341.01 (1180.72–1586.98) | ||
| n-6:n-3 PUFA ratio | 55 | 15.32 (13.4–17.6) | 22 | 14.80 (12.43–16.55) | 26 | 15.83 (13.42–19.10) | ||
| Total n-3 PUFAs | 55 | 114.6 (90.1–139.5) | 22 | 125.96 (99.03–148.03) | 26 | 109.81 (86.47–125.83) | ||
| Total n-6 PUFAs | 55 | 1733.1 (1480.9–1989.2) | 22 | 1753.66 (1503.00–2030.11) | 26 | 1709.08 (1476.47–1911.24) | ||
| Nutrient | N | Median Plasma Level (µg/mL; IQR)—Higher-Income Group | N | Median Plasma Level (µg/mL; IQR)—Lower-Income Group | N | Median Plasma Level (µg/mL; IQR)—Private Insurance | N | Median Plasma Level (µg/mL; IQR)—Public Insurance |
| ALA | 26 | 29.59 (25.21–39.41) | 10 | 36.75 (30.04–40.96) | 30 | 28.70 (23.53–40.32) | 25 | 34.65 (28.30–40.08) |
| AA | 26 | 244.19 (199.90–302.93) | 10 | 261.13 (192.78–387.89) | 30 | 237.17 (193.92–288.36) | 25 | 259.87 (204.23–302.36) |
| DHA | 26 | 62.44 (55.93–83.28) | 10 | 65.07 (41.17–95.02) | 30 | 62.16 (50.87–83.28) | 25 | 68.56 (53.01–80.41) |
| DPA | 26 | 10.12 (8.27–12.64) | 10 | 8.03 (7.28–12.57) | 30 | 9.15 (7.20–12.10) | 25 | 9.86 (7.27–12.58) |
| EPA | 26 | 7.53 (4.88–11.77) | 10 | 4.22 (2.92–8.48) | 30 | 5.68 (4.33–11.44) | 25 | 5.55 (3.62–7.81) |
| LA | 26 | 1331.41 (1208.76–1596.27) | 10 | 1472.69 (1290.51–1807.67) | 30 | 1331.41 (1119.97–1617.27) | 25 | 1443.15 (1217.03–1589.63) |
| n-6:n-3 PUFA ratio | 26 | 15.08 (12.43–17.00) | 10 | 17.85 (11.75–20.08) | 30 | 15.38 (13.28–17.32) | 25 | 15.28 (13.28–18.15) |
| Total n-3 PUFAs | 26 | 118.89 (93.68–146.20) | 10 | 108.94 (86.23–152.86) | 30 | 110.84 (88.47–141.15) | 25 | 118.09 (91.05–142.39) |
| Total n-6 PUFAs | 26 | 1753.66 (1503.00–1993.82) | 10 | 1795.99 (1652.90–2268.38) | 30 | 1678.78 (1446.64–2030.11) | 25 | 1769.63 (1607.94–1953.95) |
| Nutrient | N | Median Plasma Level (µg/mL; IQR)— Entire Cohort | N | Median Plasma Level (µg/mL; IQR)—Higher Education-Group | N | Median Plasma Level (µg/mL; IQR)—Lower-Education Group | ||
|---|---|---|---|---|---|---|---|---|
| ALA | 55 | 1.9 (1.2–3.1) | 22 | 2.05 (1.28–2.96) | 26 | 1.82 (0.95–3.07) | ||
| AA | 55 | 154.6 (127.7–178.3) | 22 | 157.79 (130.59–179.47) | 26 | 141.84 (124.19–176.68) | ||
| DHA | 55 | 34.9 (28.3–42.6) | 22 | 37.96 (34.31–49.69) | 26 | 32.80 (25.59–37.68) | ||
| DPA | 55 | 2.5 (1.8–3.5) | 22 | 2.69 (2.15–4.64) | 26 | 2.37 (1.58–3.07) | ||
| EPA | 55 | 1.6 (1.1–2.4) | 22 | 1.88 (1.41–2.63) | 26 | 1.40 (1.00–1.81) | ||
| LA | 55 | 135.4 (135.4–166.3) | 22 | 135.61 (117.26–190.70) | 26 | 122.42 (98.72–161.52) | ||
| n-6:n-3 ratio | 55 | 8.6 (6.8–9.6) | 22 | 7.92 (6.52–9.07) | 26 | 8.77 (6.96–9.65) | ||
| Total n-3 PUFAs | 55 | 40.4 (32.9–53.5) | 22 | 44.23 (39.29–59.19) | 26 | 39.34 (29.67–44.74) | ||
| Total n-6 PUFAs | 55 | 347.9 (283.2–400.7) | 22 | 349.63 (308.21–402.99) | 26 | 321.34 (269.51–388.93) | ||
| Nutrient | N | Median Plasma Level (µg/mL; IQR)— Private Insurance | N | Median Plasma Level (µg/mL; IQR)—Public Insurance | N | Median Plasma Level (µg/mL; IQR)— Higher-Income Group | N | Median Plasma Level (µg/mL; IQR)— Lower-Income Group |
| ALA | 30 | 1.84 (1.28–3.31) | 25 | 2.06 (1.05–2.93) | 26 | 2.05 (1.26–2.78) | 10 | 1.78 (1.17–3.13) |
| AA | 30 | 158.82 (133.09–184.10) | 25 | 142.06 (126.61–176.98) | 26 | 157.79 (127.64–178.75) | 10 | 140.16 (117.95–177.71) |
| DHA | 30 | 35.08 (31.03–49.28) | 25 | 33.47 (25.81–40.03) | 26 | 36.23 (32.40–49.29) | 10 | 36.27 (24.08–43.15) |
| DPA | 30 | 2.47 (1.91–3.75) | 25 | 2.55 (1.55–3.63) | 26 | 2.56 (2.02–4.64) | 10 | 2.89 (2.31–3.36) |
| EPA | 30 | 1.79 (1.46–2.48) | 25 | 1.18 (0.99–2.32) | 26 | 1.79 (1.40–2.58) | 10 | 1.10 (0.83–1.96) |
| LA | 30 | 135.61 (106.61–190.70) | 25 | 124.72 (98.26–157.38) | 26 | 135.48 (109.56–168.67) | 10 | 122.41 (102.97–138.95) |
| n-6:n-3 ratio | 30 | 8.55 (6.78–10.55) | 25 | 8.78 (7.10–9.50) | 26 | 8.42 (6.64–9.10) | 10 | 7.87 (5.92–9.65) |
| Total n-3 PUFAs | 30 | 41.28 (36.73–57.15) | 25 | 39.47 (30.28–48.86) | 26 | 43.73 (37.72–59.19) | 10 | 42.19 (29.55–49.14) |
| Total n-6 PUFAs | 30 | 349.02 (308.21–418.42) | 25 | 331.83 (272.21–386.48) | 26 | 349.02 (305.67–401.08) | 10 | 299.40 (275.61–379.95) |
| Nutrient | N | Median Intake (g/day; IQR) for Entire Cohort | N | Median Intake (g/day; IQR) for Higher-Education Group | N | Median Intake (g/day; IQR) for Lower-Education Group | p-Value |
|---|---|---|---|---|---|---|---|
| ALA intake | 48 | 1.29 (0.94–1.74) | 22 | 1.26 (1.12–1.56) | 26 | 1.35 (0.88–1.95) | 0.61 |
| AA intake | 48 | 0.14 (0.09–0.18) | 22 | 0.14 (0.10–0.19) | 26 | 0.14 (0.09–0.18) | 0.84 |
| DHA intake | 48 | 0.07 (0.03–0.17) | 22 | 0.07 (0.03–0.19) | 26 | 0.07 (0.03–0.17) | 0.79 |
| DPA intake | 48 | 0.02 (0.01–0.03) | 22 | 0.02 (0.01–0.03) | 26 | 0.02 (0.01–0.03) | 0.77 |
| EPA intake | 48 | 0.02 (0.00–0.06) | 22 | 0.03 (0.01–0.14) | 26 | 0.02 (0.00–0.06) | 0.33 |
| LA intake | 48 | 11.99 (8.86–15.60) | 22 | 10.88 (9.07–13.34) | 26 | 12.86 (7.93–19.00) | 0.41 |
| n-6:n-3 PUFA intake ratio (no supplementation) | 48 | 9.12 (8.22–10.08) | 22 | 9.19 (8.21–10.06) | 26 | 9.08 (8.51–10.21) | 0.80 |
| n-6:n-3 PUFA intake ratio (with supplementation) | 48 | 8.95 (7.29–10.06) | 22 | 8.21 (6.67–9.89) | 26 | 9.08 (8.14–10.21) | 0.15 |
| Total n-3 PUFA intake (no supplementation) | 48 | 1.43 (1.07–1.84) | 22 | 1.30 (1.10–1.54) | 26 | 1.53 (0.94–2.06) | 0.33 |
| Total n-3 PUFA intake (with supplementation) | 48 | 1.53 (1.09–1.98) | 22 | 1.47 (1.18–1.94) | 26 | 1.61 (0.94–2.06) | 0.98 |
| Total n-6 PUFA intake (no supplementation) | 48 | 13.09 (9.72–17.11) | 22 | 11.61 (10.09–14.61) | 26 | 14.57 (8.74–21.15) | 0.35 |
| Total n-6 PUFA intake (with supplementation) | 48 | 13.09 (9.72–17.11) | 22 | 11.61 (10.09–14.61) | 26 | 14.57 (8.74–21.15) | 0.36 |
| Nutrient | N | Median Intake (g/day; IQR) for Higher-Income Group | N | Median Intake (g/day; IQR) for Lower-Income Group | p-Value | ||
| ALA intake | 26 | 1.26 (1.05–1.72) | 10 | 1.55 (1.28–1.78) | 0.19 | ||
| AA intake | 26 | 0.14 (0.09–0.18) | 10 | 0.15 (0.11–0.27) | 0.43 | ||
| DHA intake | 26 | 0.09 (0.03–0.23) | 10 | 0.07 (0.06–0.25) | 0.48 | ||
| DPA intake | 26 | 0.02 (0.01–0.03) | 10 | 0.02 (0.01–0.03) | 0.90 | ||
| EPA intake | 26 | 0.03 (0.01–0.14) | 10 | 0.03 (0.01–0.08) | 0.88 | ||
| LA intake | 26 | 10.87 (8.99–15.36) | 10 | 13.73 (11.24–15.46) | 0.21 | ||
| n-6:n-3 PUFA intake ratio (no supplementation) | 26 | 9.01 (8.21–10.06) | 10 | 8.80 (7.94–9.89) | 0.72 | ||
| n-6:n-3 PUFA intake ratio (with supplementation) | 26 | 8.21 (6.76–9.85) | 10 | 8.80 (7.94–9.89) | 0.48 | ||
| Total n-3 PUFA intake (no supplementation) | 26 | 1.30 (1.09–1.75) | 10 | 1.75 (1.45–1.88) | 0.07 | ||
| Total n-3 PUFA intake (with supplementation) | 26 | 1.47 (1.15–2.02) | 10 | 1.75 (1.51–1.88) | 0.57 | ||
| Total n-6 PUFA intake (no supplementation) | 26 | 11.61 (10.02–16.65) | 10 | 15.49 (12.29–17.09) | 0.18 | ||
| Total n-6 PUFA intake (with supplementation) | 26 | 11.61 (10.02–16.65) | 10 | 15.49 (12.29–17.09) | 0.19 | ||
| Nutrient | N | Median Intake (g/day; IQR) for Private Insurance | N | Median Intake (g/day; IQR) for Public Insurance | p-Value | ||
| ALA intake | 26 | 1.26 (1.05–1.83) | 22 | 1.35 (0.84–1.73) | 0.98 | ||
| AA intake | 26 | 0.14 (0.10–0.19) | 22 | 0.14 (0.09–0.18) | 0.66 | ||
| DHA intake | 26 | 0.07 (0.03–0.23) | 22 | 0.07 (0.03–0.16) | 0.73 | ||
| DPA intake | 26 | 0.02 (0.01–0.03) | 22 | (0.02 (0.01–0.03) | 0.63 | ||
| EPA intake | 26 | 0.02 (0.00–0.11) | 22 | 0.01 (0.00–0.07) | 0.59 | ||
| LA intake | 26 | 11.01 (9.07–15.36) | 22 | 12.96 (7.58–16.42) | 0.85 | ||
| n-6:n-3 PUFA intake ratio (no supplementation) | 26 | 9.05 (10.09–8.20) | 22 | 9.17 (8.49–9.98) | 0.90 | ||
| n-6:n-3 PUFA intake ratio (with supplementation) | 26 | 8.21 (6.76–10.07) | 22 | 9.17 (8.49–9.98) | 0.17 | ||
| Total n-3 PUFA intake (no supplementation) | 26 | 1.30 (1.09–1.75) | 22 | 1.53 (0.93–1.87) | 0.61 | ||
| Total n-3 PUFA intake (with supplementation) | 26 | 1.47 (1.15–2.12) | 22 | 1.61 (0.93–1.87) | 0.56 | ||
| Total n-6 PUFA intake (no supplementation) | 26 | 11.91 (10.09–16.65) | 22 | 14.57 (8.20–18.08) | 0.76 | ||
| Total n-6 PUFA intake (with supplementation) | 26 | 11.91 (10.09–16.65) | 22 | 14.57 (8.20–18.08) | 0.77 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hergenrader, A.; VanOrmer, M.; Slotkowski, R.; Thompson, M.; Freeman, A.; Paetz, O.; Sweeney, S.; Wegner, L.; Ali, K.; Bender, N.; et al. Omega-3 Polyunsaturated Fatty Acid Levels in Maternal and Cord Plasma Are Associated with Maternal Socioeconomic Status. Nutrients 2023, 15, 4432. https://doi.org/10.3390/nu15204432
Hergenrader A, VanOrmer M, Slotkowski R, Thompson M, Freeman A, Paetz O, Sweeney S, Wegner L, Ali K, Bender N, et al. Omega-3 Polyunsaturated Fatty Acid Levels in Maternal and Cord Plasma Are Associated with Maternal Socioeconomic Status. Nutrients. 2023; 15(20):4432. https://doi.org/10.3390/nu15204432
Chicago/Turabian StyleHergenrader, Alexandra, Matthew VanOrmer, Rebecca Slotkowski, Maranda Thompson, Alyssa Freeman, Olivia Paetz, Sarah Sweeney, Lauren Wegner, Khadijjta Ali, Nicole Bender, and et al. 2023. "Omega-3 Polyunsaturated Fatty Acid Levels in Maternal and Cord Plasma Are Associated with Maternal Socioeconomic Status" Nutrients 15, no. 20: 4432. https://doi.org/10.3390/nu15204432
APA StyleHergenrader, A., VanOrmer, M., Slotkowski, R., Thompson, M., Freeman, A., Paetz, O., Sweeney, S., Wegner, L., Ali, K., Bender, N., Chaudhary, R., Thoene, M., Hanson, C., & Anderson-Berry, A. (2023). Omega-3 Polyunsaturated Fatty Acid Levels in Maternal and Cord Plasma Are Associated with Maternal Socioeconomic Status. Nutrients, 15(20), 4432. https://doi.org/10.3390/nu15204432