
Is Curcumine Useful in the Treatment and Prevention of the Tendinopathy and Myotendinous Junction Injury? A Scoping Review

 ,
, 
 ,
,  and
and 
Abstract
1. Introduction
- (a)
- Reactive tendinopathy (mechanical) is usually the consequence of an acute overload on the tendon due to tension or compression. In this type, the immune system plays a key role in tissue regeneration and maintenance processes. In this event, tendinopathy sometimes coincides with an episode of a cold or after oral surgery. From a microscopic point of view, cellular hyperactivity of the tendon can be observed after physical stress in reactive tendinopathy. The number of tendon cells increases greatly, the cells become rounded and the tissue attracts water due to the presence of hydrophilic molecules (i.e., proteoglycans). These machromolecules (proteoglycans and glycosaminoglycans) are important for water retention and improve the biomechanical properties (elasticity) in the tendon against shear and compression forces [33].
- (b)
- Degenerative tendinopathy is characterised by a progression of ECM and collagen disorganisation. Cellular damage is accompanied by alterations in tendon vascularization, being unable to withstand any tensional stress, and evolving to be mechanically useless. In addition, the tissue begins to produce pain-related substances and activates the peripheral nerve, causing hypersensitivity [34].
1.1. The Inflammatory Process in Tendinopathies
1.2. Therapeutic Management of Tendinopathies
1.3. Nutritional Approach to Tendinopathy
1.4. Curcumin as a Therapeutic Adjuvant in Tendinopathy
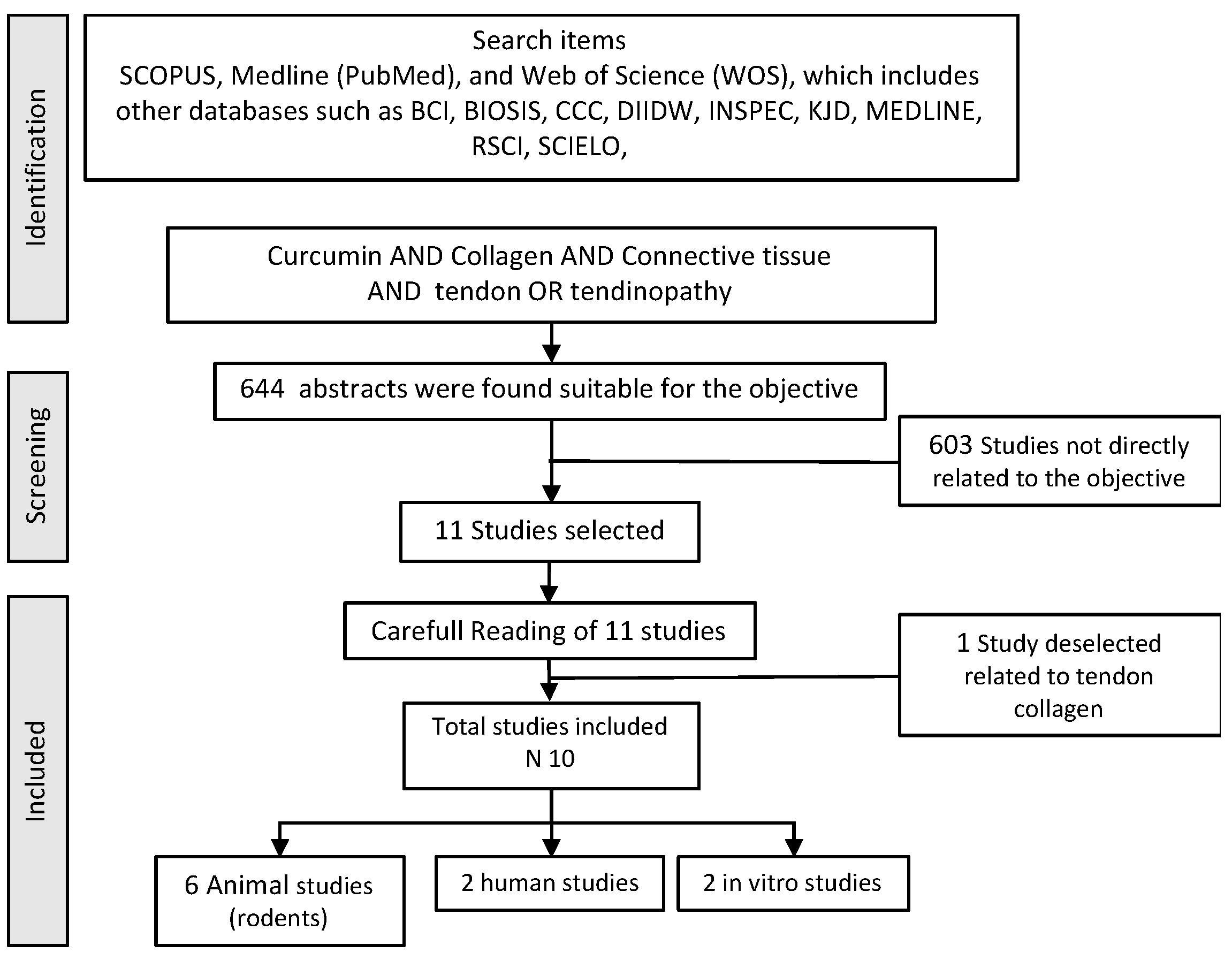
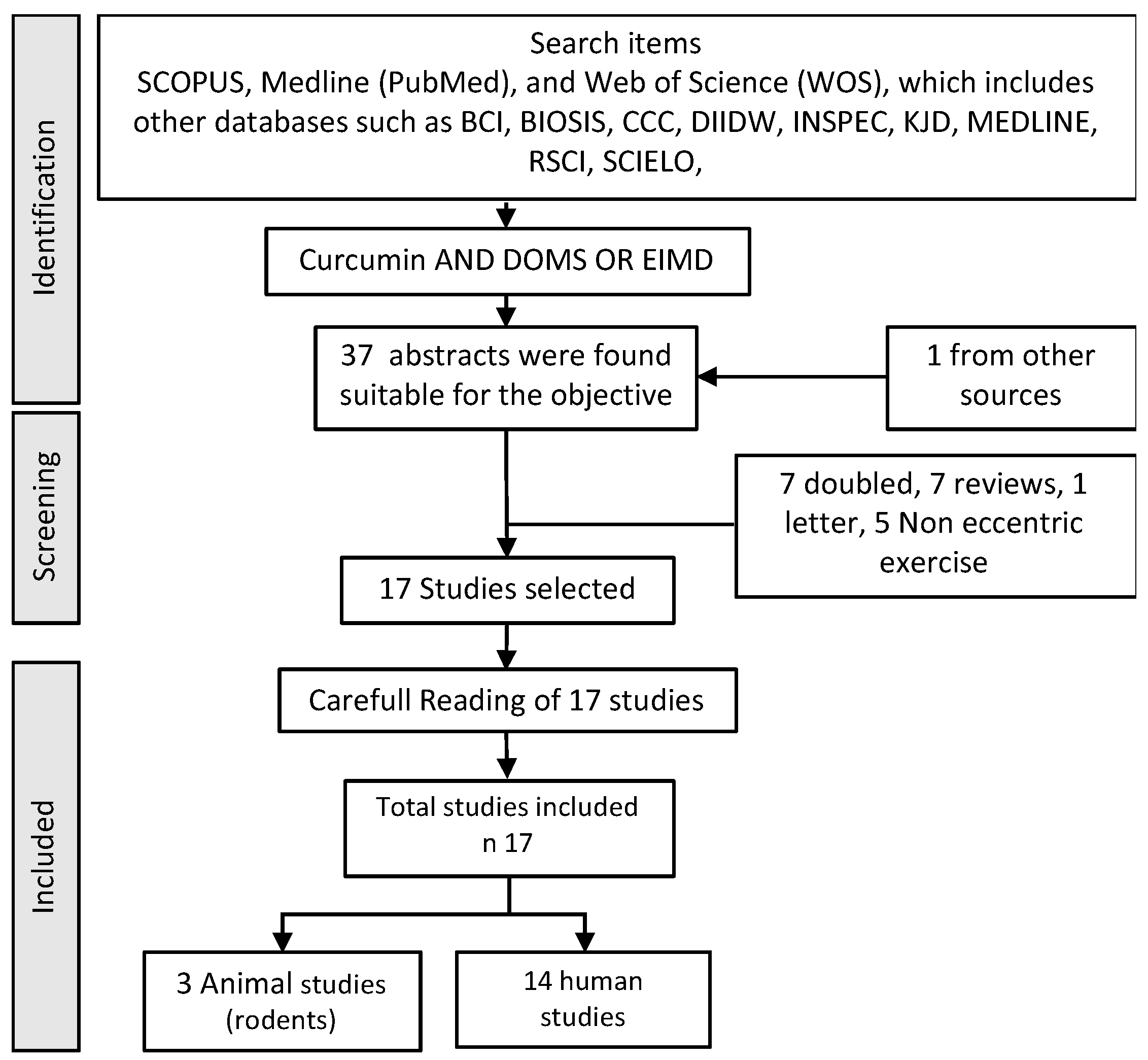
2. Methodology
Study Analysis and Search Strategy
3. Results
4. Discussion
4.1. Curcumin as Anti-Inflammatory and Immunomodulatory Agent
Pharmacological Action of Curcumin
- Antioxidant
- Collagen organisation
- Analgesic
- Biostimulator
4.2. Therapeutic Guidance
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Maffulli, N.; Barrass, V.; Ewen, S.W.B. Light Microscopic Histology of Achilles Tendon Ruptures: A Comparison with Unruptured Tendons. Am. J. Sports Med. 2000, 28, 857–863. [Google Scholar] [CrossRef] [PubMed]
- Loiacono, C.; Palermi, S.; Massa, B.; Belviso, I.; Romano, V.; Di Gregorio, A.; Sirico, F.; Sacco, A.M. Tendinopathy: Pathophysiology, Therapeutic Options, and Role of Nutraceutics. A Narrative Literature Review. Medicina 2019, 55, 447. [Google Scholar] [CrossRef] [PubMed]
- Maffulli, N.; Wong, J.; Almekinders, L.C. Types and epidemiology of tendinopathy. Clin. Sports Med. 2003, 22, 675–692. [Google Scholar] [CrossRef]
- Albers, I.S.; Zwerver, J.; Diercks, R.L.; Dekker, J.H.; Van den Akker-Scheek, I. Incidence and prevalence of lower extremity tendinopathy in a Dutch general practice population: A cross sectional study. BMC Musculoskelet. Disord. 2016, 17, 16. [Google Scholar] [CrossRef] [PubMed]
- Jakobsen, J.R.; Mackey, A.L.; Koch, M.; Imhof, T.; Hannibal, J.; Kjær, M.; Krogsgaard, M.R. Larger interface area at the human myotendinous junction in type 1 compared with type 2 muscle fibers. Scand. J. Med. Sci. Sports 2023, 33, 136–145. [Google Scholar] [CrossRef] [PubMed]
- Huijing, P.A. Muscle as a collagen fiber reinforced composite: A review of force transmission in muscle and whole limb. J. Biomech. 1999, 32, 329–345. [Google Scholar] [CrossRef]
- Garrett, W.E. Muscle strain injuries. Am. J. Sports Med. 1996, 24, S2–S8. [Google Scholar] [CrossRef]
- Orchard, J.; Seward, H. Epidemiology of injuries in the Australian Football League, seasons 1997–2000. Br. J. Sports Med. 2002, 36, 39–44. [Google Scholar] [CrossRef]
- Altarriba-Bartes, A.; Drobnic, F.; Til, L.; Malliaropoulos, N.; Montoro, J.B.; Irurtia, A. Epidemiology of injuries in elite taekwondo athletes: Two Olympic periods cross-sectional retrospective study. BMJ Open 2014, 4, e004605. [Google Scholar] [CrossRef]
- Tidball, J.G.; Chan, M. Adhesive strength of single muscle cells to basement membrane at myotendinous junctions. J. Appl. Physiol. 1989, 67, 1063–1069. [Google Scholar] [CrossRef]
- Jakobsen, J.R.; Krogsgaard, M.R. The Myotendinous Junction—A Vulnerable Companion in Sports. A Narrative Review. Front. Physiol. 2021, 12, 635561. [Google Scholar] [CrossRef] [PubMed]
- Schmid, M.R.; Hodler, J.; Cathrein, P.; Duewell, S.; Jacob, H.A.C.; Romero, J. Is Impingement the Cause of Jumper’s Knee?: Dynamic and Static Magnetic Resonance Imaging of Patellar Tendinitis in an Open-Configuration System. Am. J. Sports Med. 2002, 30, 388–395. [Google Scholar] [CrossRef] [PubMed]
- Peace, K.A.L.; Lee, J.C.; Healy, J. Imaging the infrapatellar tendon in the elite athlete. Clin. Radiol. 2006, 61, 570–578. [Google Scholar] [CrossRef] [PubMed]
- Couppé, C.; Kongsgaard, M.; Aagaard, P.; Vinther, A.; Boesen, M.; Kjaer, M.; Magnusson, S.P. Differences in tendon properties in elite badminton players with or without patellar tendinopathy. Scand. J. Med. Sci. Sports 2013, 23, e89–e95. [Google Scholar] [CrossRef]
- Irby, A.; Gutierrez, J.; Chamberlin, C.; Thomas, S.J.; Rosen, A.B. Clinical management of tendinopathy: A systematic review of systematic reviews evaluating the effectiveness of tendinopathy treatments. Scand. J. Med. Sci. Sports 2020, 30, 1810–1826. [Google Scholar] [CrossRef]
- Abate, M.; Gravare-Silbernagel, K.; Siljeholm, C.; Di Iorio, A.; De Amicis, D.; Salini, V.; Werner, S.; Paganelli, R. Pathogenesis of tendinopathies: Inflammation or degeneration? Arthritis Res. Ther. 2009, 11, 235. [Google Scholar] [CrossRef] [PubMed]
- Cook, J.L.; Khan, K.M. Etiology of Tendinopathy. In Tendinopathy in Athletes; Woo, S.L.Y., Renstrm, P.A.F.H., Arnoczky, S.P., Eds.; Blackwell Publishing Ltd.: Oxford, UK, 2007; pp. 10–28. [Google Scholar]
- Knobloch, K. Drug-Induced Tendon Disorders. In Metabolic Influences on Risk for Tendon Disorders; Ackermann, P.W., Hart, D.A., Eds.; Springer International Publishing: New York, NY, USA, 2016; Volume 920, pp. 229–238. [Google Scholar]
- Abate, M.; Schiavone, C.; Salini, V.; Andia, I. Occurrence of tendon pathologies in metabolic disorders. Rheumatology 2013, 52, 599–608. [Google Scholar] [CrossRef]
- Li, Y.; Fessel, G.; Georgiadis, M.; Snedeker, J.G. Advanced glycation end-products diminish tendon collagen fiber sliding. Matrix Biol. 2013, 32, 169–177. [Google Scholar] [CrossRef]
- Couppé, C.; Svensson, R.B.; Kongsgaard, M.; Kovanen, V.; Grosset, J.F.; Snorgaard, O.; Bencke, J.; Larsen, J.O.; Bandholm, T.; Christensen, T.M.; et al. Human Achilles tendon glycation and function in diabetes. J. Appl. Physiol. 2016, 120, 130–137. [Google Scholar] [CrossRef]
- Schwarz, R.I.; Kleinman, P.; Owens, N. Ascorbate Can Act as an Inducer of the Collagen Pathway Because Most Steps Are Tightly Coupled. Ann. N. Y. Acad. Sci. 1987, 498, 172–185. [Google Scholar] [CrossRef]
- Sajithlal, G.B.; Chithra, P.; Chandrakasan, G. Effect of curcumin on the advanced glycation and cross-linking of collagen in diabetic rats. Biochem. Pharm. 1998, 56, 1607–1614. [Google Scholar] [CrossRef] [PubMed]
- Arbiser, J.L.; Klauber, N.; Rohan, R.; van Leeuwen, R.; Huang, M.T.; Fisher, C.; Flynn, E.; Byers, H.R. Curcumin is an in vivo inhibitor of angiogenesis. Mol. Med. 1998, 4, 376–483. [Google Scholar] [CrossRef]
- Minaguchi, J.; Koyama, Y.-i.; Meguri, N.; Hosaka, Y.; Ueda, H.; Kusubata, M.; Hirota, A.; Irie, S.; Mafune, N.; Takehana, K. Effects of Ingestion of Collagen Peptide on Collagen Fibrils and Glycosaminoglycans in Achilles Tendon. J. Nutr. Sci. Vitam. 2005, 51, 169–174. [Google Scholar] [CrossRef] [PubMed]
- Lippiello, L. Collagen Synthesis in Tenocytes, Ligament Cells and Chondrocytes Exposed to a Combination of Glucosamine HCl and Chondroitin Sulfate. Evid. Based Complement. Altern. Med. 2007, 4, 219–224. [Google Scholar] [CrossRef] [PubMed]
- Oryan, A.; Goodship, A.E.; Silver, I.A. Response of a Collagenase-Induced Tendon Injury to Treatment with a Polysulphated Glycosaminoglycan (Adequan). Connect. Tissue Res. 2008, 49, 351–360. [Google Scholar] [CrossRef]
- Fusini, F.; Bisicchia, S.; Bottegoni, C.; Gigante, A.; Zanchini, F.; Busilacchi, A. Nutraceutical supplement in the management of tendinopathies: A systematic review. Muscles Ligaments Tendons J. 2019, 6, 48. [Google Scholar] [CrossRef]
- O’Brien, M. Structure and metabolism of tendons. Scand. J. Med. Sci. Sports 2007, 7, 55–61. [Google Scholar] [CrossRef]
- Cerciello, S.; Neyret, P. Ligament Tissue Pathology. In General Orthopaedics and Basic Science; Paschos, N.K., Bentley, G., Eds.; Springer International Publishing: New York, NY, USA, 2019; pp. 57–61. [Google Scholar]
- Calve, S.; Dennis, R.G.; Kosnik, P.E.; Baar, K.; Grosh, K.; Arruda, E.M. Engineering of Functional Tendon. Tissue Eng. 2004, 10, 755–761. [Google Scholar] [CrossRef]
- Bard, H. Tendinopatías: Etiopatogenia, diagnóstico y tratamiento. EMC Apar. Locomot. 2012, 45, 1–20. [Google Scholar] [CrossRef]
- Giffin, J.R.; Stanish, W.D. Overuse tendonitis and rehabilitation. Can. Fam. Physician 1993, 39, 1762–1769. [Google Scholar]
- Smith, R.K.W.; McIlwraith, C.W. “One Health” in tendinopathy research: Current concepts. J. Orthop. Res. 2021, 39, 1596–1602. [Google Scholar] [CrossRef] [PubMed]
- Millar, N.L.; Silbernagel, K.G.; Thorborg, K.; Kirwan, P.D.; Galatz, L.M.; Abrams, G.D.; Murrell, G.A.C.; McInnes, I.B.; Rodeo, S.A. Tendinopathy. Nat. Rev. Dis. Prim. 2021, 7, 1. [Google Scholar] [CrossRef] [PubMed]
- Yao, L.; Bestwick, C.S.; Bestwick, L.A.; Aspden, R.M.; Maffulli, N. Non-immortalized human tenocyte cultures as a vehicle for understanding cellular aspects to tendinopathy. Transl. Med. UniSa 2011, 1, 173–194. [Google Scholar] [PubMed]
- Millar, N.L.; Murrell, G.A.C.; McInnes, I.B. Alarmins in tendinopathy: Unravelling new mechanisms in a common disease. Rheumatology 2013, 52, 769–779. [Google Scholar] [CrossRef]
- Del Buono, A.; Battery, L.; Denaro, V.; Maccauro, G.; Maffulli, N. Tendinopathy and Inflammation: Some Truths. Int. J. Immunopathol. Pharm. 2011, 24, 45–50. [Google Scholar] [CrossRef]
- Legerlotz, K.; Jones, E.R.; Screen, H.R.C.; Riley, G.P. Increased expression of IL-6 family members in tendon pathology. Rheumatology 2012, 51, 1161–1165. [Google Scholar] [CrossRef]
- Al-Sadi, O.; Schulze-Tanzil, G.; Kohl, B.; Lohan, A.; Lemke, M.; Ertel, W.; John, T. Tenocytes, pro-inflammatory cytokines and leukocytes: A relationship? Muscles Ligaments Tendons J. 2011, 1, 68–76. [Google Scholar]
- Chaudhury, S.; Carr, A.J. Lessons we can learn from gene expression patterns in rotator cuff tears and tendinopathies. J. Shoulder Elb. Surg. 2012, 21, 191–199. [Google Scholar] [CrossRef]
- Yang, G.; Im, H.J.; Wang, J.H.C. Repetitive mechanical stretching modulates IL-1β induced COX-2, MMP-1 expression, and PGE2 production in human patellar tendon fibroblasts. Gene 2005, 363, 166–172. [Google Scholar] [CrossRef]
- Welc, S.S.; Clanton, T.L. The regulation of interleukin-6 implicates skeletal muscle as an integrative stress sensor and endocrine organ: Interleukin-6 produced by skeletal muscle during stress. Exp. Physiol. 2013, 98, 359–371. [Google Scholar] [CrossRef]
- D’Addona, A.; Maffulli, N.; Formisano, S.; Rosa, D. Inflammation in tendinopathy. Surgeon 2017, 15, 297–302. [Google Scholar] [CrossRef] [PubMed]
- Leadbetter, W.B. Cell-matrix response in tendon injury. Clin. Sports Med. 1992, 11, 533–578. [Google Scholar] [CrossRef] [PubMed]
- Sharma, P.; Maffulli, N. Biology of tendon injury: Healing, modeling and remodeling. J. Musculoskelet. Neuronal Interact. 2006, 6, 181–190. [Google Scholar]
- Daley, W.P.; Peters, S.B.; Larsen, M. Extracellular matrix dynamics in development and regenerative medicine. J. Cell Sci. 2008, 121, 255–264. [Google Scholar] [CrossRef]
- Lu, P.; Takai, K.; Weaver, V.M.; Werb, Z. Extracellular Matrix Degradation and Remodeling in Development and Disease. Cold Spring Harb. Perspect. Biol. 2011, 3, a005058. [Google Scholar] [CrossRef] [PubMed]
- Killian, M.L.; Cavinatto, L.; Galatz, L.M.; Thomopoulos, S. The role of mechanobiology in tendon healing. J. Shoulder Elb. Surg. 2012, 21, 228–237. [Google Scholar] [CrossRef] [PubMed]
- Ackermann, P.W.; Domeij-Arverud, E.; Leclerc, P.; Amoudrouz, P.; Nader, G.A. Anti-inflammatory cytokine profile in early human tendon repair. Knee Surg. Sports Traumatol. Arthrosc. 2013, 21, 1801–1806. [Google Scholar] [CrossRef]
- Fedorczyk, J.M.; Barr, A.E.; Rani, S.; Gao, H.G.; Amin, M.; Amin, S.; Litvin, J.; Barbe, M.F. Exposure-dependent increases in IL-1β, substance P, CTGF, and tendinosis in flexor digitorum tendons with upper extremity repetitive strain injury. J. Orthop. Res. 2010, 28, 298–307. [Google Scholar] [CrossRef]
- Sharma, P.; Maffulli, N. Tendon Injury and Tendinopathy: Healing and Repair. J. Bone Jt. Surg. Am. 2005, 87, 187–202. [Google Scholar] [CrossRef]
- Thampatty, B.P.; Li, H.; Im, H.J.; Wang, J.H.C. EP4 receptor regulates collagen type-I, MMP-1, and MMP-3 gene expression in human tendon fibroblasts in response to IL-1β treatment. Gene 2007, 386, 154–161. [Google Scholar] [CrossRef]
- Dinesh, P.; Rasool, M. Berberine mitigates IL-21/IL-21R mediated autophagic influx in fibroblast-like synoviocytes and regulates Th17/Treg imbalance in rheumatoid arthritis. Apoptosis 2019, 24, 644–661. [Google Scholar] [CrossRef] [PubMed]
- Riley, G.P.; Curry, V.; DeGroot, J.; van El, B.; Verzijl, N.; Hazleman, B.L.; Bank, R.A. Matrix metalloproteinase activities and their relationship with collagen remodelling in tendon pathology. Matrix Biol. 2002, 21, 185–195. [Google Scholar] [CrossRef] [PubMed]
- Nagase, H.; Visse, R.; Murphy, G. Structure and function of matrix metalloproteinases and TIMPs. Cardiovasc. Res. 2006, 69, 562–573. [Google Scholar] [CrossRef]
- Paoloni, J.A.; Appleyard, R.C.; Nelson, J.; Murrell, G.A.C. Topical Glyceryl Trinitrate Treatment of Chronic Noninsertional Achilles Tendinopathy: A Randomized, Double-Blind, Placebo-Controlled Trial. J. Bone Jt. Surg. Am. 2004, 86, 916–922. [Google Scholar] [CrossRef] [PubMed]
- Xia, W.; Szomor, Z.; Wang, Y.; Murrell, G.A.C. Nitric oxide enhances collagen synthesis in cultured human tendon cells. J. Orthop. Res. 2006, 24, 159–172. [Google Scholar] [CrossRef]
- Murrell, G.A.C. Oxygen free radicals and tendon healing. J. Shoulder Elb. Surg. 2007, 16, S208–S214. [Google Scholar] [CrossRef]
- Semis, H.S.; Gur, C.; Ileriturk, M.; Kandemir, F.M.; Kaynar, O. Evaluation of Therapeutic Effects of Quercetin Against Achilles Tendinopathy in Rats via Oxidative Stress, Inflammation, Apoptosis, Autophagy, and Metalloproteinases. Am. J. Sports Med. 2022, 50, 486–498. [Google Scholar] [CrossRef]
- Maffulli, N.; Walley, G.; Sayana, M.K.; Longo, U.G.; Denaro, V. Eccentric calf muscle training in athletic patients with Achilles tendinopathy. Disabil. Rehabil. 2008, 30, 1677–1684. [Google Scholar] [CrossRef]
- Medina, D. Guia de la pràctica clínica de les tendinopaties: Diagnòstic, tractament i prevenció. Apunt. Med. l’Esport 2012, 47, 143–168. [Google Scholar]
- Rees, J.D.; Wilson, A.M.; Wolman, R.L. Current concepts in the management of tendon disorders. Rheumatology 2006, 45, 508–521. [Google Scholar] [CrossRef]
- Molnar, J.A.; Underdown, M.J.; Clark, W.A. Nutrition and Chronic Wounds. Adv. Wound Care 2014, 3, 663–681. [Google Scholar] [CrossRef] [PubMed]
- DePhillipo, N.N.; Aman, Z.S.; Kennedy, M.I.; Begley, J.P.; Moatshe, G.; LaPrade, R.F. Efficacy of Vitamin C Supplementation on Collagen Synthesis and Oxidative Stress After Musculoskeletal Injuries: A Systematic Review. Orthop. J. Sports Med. 2018, 6, 232596711880454. [Google Scholar] [CrossRef] [PubMed]
- Tuero, B. Funciones de la vitamina C en el metabolismo del colágeno. Rev. Cuba. Aliment. Nutr. 2000, 1, 46–54. [Google Scholar]
- Kipp, D.E.; McElvain, M.; Kimmel, D.B.; Akhter, M.P.; Robinson, R.G.; Lukert, B.P. Scurvy results in decreased collagen synthesis and bone density in the guinea pig animal model. Bone 1996, 18, 281–288. [Google Scholar] [CrossRef] [PubMed]
- Poulsen, R.; Zarei, A.; Sabokbar, A.; Hulley, P. Tendon, a Vitamin D-Responsive Tissue—Why the British Weather May Not Just Be Bad for Your Bones. Int. J. Exp. Pathol. 2013, 94, A20. [Google Scholar]
- Agrawal, D.; Dougherty, K.; Dilisio, M. Vitamin D and the immunomodulation of rotator cuff injury. J. Inflamm. Res. 2016, 9, 123–131. [Google Scholar] [CrossRef]
- Angeline, M.E.; Ma, R.; Pascual-Garrido, C.; Voigt, C.; Deng, X.H.; Warren, R.F.; Rodeo, S.A. Effect of Diet-Induced Vitamin D Deficiency on Rotator Cuff Healing in a Rat Model. Am. J. Sports Med. 2014, 42, 27–34. [Google Scholar] [CrossRef]
- Nossov, S.; Dines, J.S.; Murrell, G.A.C.; Rodeo, S.A.; Bedi, A. Biologic augmentation of tendon-to-bone healing: Scaffolds, mechanical load, vitamin D, and diabetes. Instr. Course Lect. 2014, 63, 451–462. [Google Scholar]
- Barbosa, A.W.C.; Benevides, G.P.; Alferes, L.M.T.; Salomão, E.M.; Gomes-Marcondes, M.C.C.; Gomes, L. A leucine-rich diet and exercise affect the biomechanical characteristics of the digital flexor tendon in rats after nutritional recovery. Amino Acids 2012, 42, 329–336. [Google Scholar] [CrossRef]
- Vieira, C.P.; Oliveira, L.P.D.; Guerra, F.D.R.; Almeida, M.D.S.D.; Marcondes, M.C.C.G.; Pimentel, E.R. Glycine Improves Biochemical and Biomechanical Properties Following Inflammation of the Achilles Tendon: Glycine Improves the Tendon Inflammation. Anat. Rec. 2015, 298, 538–545. [Google Scholar] [CrossRef]
- Noorafshan, A.; Ashkani-Esfahani, S. A Review of Therapeutic Effects of Curcumin. Curr. Pharm. Des. 2013, 19, 2032–2046. [Google Scholar] [PubMed]
- Witkin, J.; Li, X. Curcumin, an Active Constiuent of the Ancient Medicinal Herb Curcuma longa L.: Some Uses and the Establishment and Biological Basis of Medical Efficacy. CNS Neurol. Disord. Drug Targets 2013, 12, 487–497. [Google Scholar] [CrossRef] [PubMed]
- Fujisawa, S.; Atsumi, T.; Ishihara, M.; Kadoma, Y. Cytotoxicity, ROS-generation activity and radical-scavenging activity of curcumin and related compounds. Anticancer Res. 2004, 24, 563–569. [Google Scholar] [PubMed]
- Augustyniak, A.; Bartosz, G.; Čipak, A.; Duburs, G.; Horáková, L.; Łuczaj, W.; Majekova, M.; Odysseos, A.D.; Rackova, L.; Skrzydlewska, E.; et al. Natural and synthetic antioxidants: An updated overview. Free Radic. Res. 2010, 44, 1216–1262. [Google Scholar] [CrossRef] [PubMed]
- Dinkova-Kostova, A.T.; Talalay, P. Relation of structure of curcumin analogs to their potencies as inducers of Phase 2 detoxification enzymes. Carcinogenesis 1999, 20, 911–914. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, B.B.; Harikumar, K.B. Potential therapeutic effects of curcumin, the anti-inflammatory agent, against neurodegenerative, cardiovascular, pulmonary, metabolic, autoimmune and neoplastic diseases. Int. J. Biochem. Cell Biol. 2009, 41, 40–59. [Google Scholar] [CrossRef]
- Shehzad, A.; Lee, J.; Lee, Y.S. Curcumin in various cancers. BioFactors 2013, 39, 56–68. [Google Scholar] [CrossRef]
- Shishodia, S. Molecular mechanisms of curcumin action: Gene expression. BioFactors 2013, 39, 37–55. [Google Scholar] [CrossRef]
- Harbour, R.; Miller, J. A new system for grading recommendations in evidence based guidelines. BMJ 2001, 323, 334–336. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J.; GRADE Working Group. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [CrossRef]
- Cumpston, M.; Li, T.; Page, M.J.; Chandler, J.; Welch, V.A.; Higgins, J.P.; Thomas, J. Updated Guidance for Trusted Systematic Reviews: A New Edition of the Cochrane Handbook for Systematic Reviews of Interventions; Cochrane Editorial Unit; Wiley: Hoboken, NJ, USA, 2019. [Google Scholar]
- Hutton, B.; Catalá-López, F.; Moher, D. La extensión de la declaración PRISMA para revisiones sistemáticas que incorporan metaanálisis en red: PRISMA-NMA. Med. Clín. 2016, 147, 262–266. [Google Scholar] [CrossRef]
- Peters, M.D.; Godfrey, C.M.; Khalil, H.; McInerney, P.; Parker, D.; Soares, C.B. Guidance for conducting systematic scoping reviews. Int. J. Evid.-Based Healthc. 2015, 13, 141–146. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed]
- Güleç, A.; Türk, Y.; Aydin, B.K.; Erkoçak, Ö.F.; Safalı, S.; Ugurluoglu, C. Effect of curcumin on tendon healing: An experimental study in a rat model of Achilles tendon injury. Int. Orthop. 2018, 42, 1905–1910. [Google Scholar] [CrossRef] [PubMed]
- Jiang, D.; Gao, P.; Lin, H.; Geng, H. Curcumin improves tendon healing in rats: A histological, biochemical, and functional evaluation. Connect. Tissue Res. 2016, 57, 20–27. [Google Scholar] [CrossRef]
- Zhang, J.; Xiao, C.; Zhang, X.; Lin, Y.; Yang, H.; Zhang, Y.S.; Ding, J. An oxidative stress-responsive electrospun polyester membrane capable of releasing anti-bacterial and anti-inflammatory agents for postoperative anti-adhesion. J. Control Release 2021, 335, 359–368. [Google Scholar] [CrossRef]
- Li, Y.; Zhang, W.; Li, X.; Comes Franchini, M.; Xu, K.; Locatelli, E.; Martin, R.C.; Monaco, I.; Li, Y.; Cui, S. Controlled release of curcumin from curcumin-loaded nanomicelles to prevent peritendinous adhesion during Achilles tendon healing in rats. Int. J. Nanomed. 2016, 11, 2873–2881. [Google Scholar] [CrossRef]
- Merolla, G.; Dellabiancia, F.; Ingardia, A.; Paladini, P.; Porcellini, G. Co-analgesic therapy for arthroscopic supraspinatus tendon repair pain using a dietary supplement containing Boswellia serrata and Curcuma longa: A prospective randomized placebo-controlled study. Musculoskelet. Surg. 2015, 99, 43–52. [Google Scholar] [CrossRef]
- Buhrmann, C.; Mobasheri, A.; Busch, F.; Aldinger, C.; Stahlmann, R.; Montaseri, A.; Shakibaei, M. Curcumin Modulates Nuclear Factor κB (NF-κB)-mediated Inflammation in Human Tenocytes in Vitro. J. Biol. Chem. 2011, 286, 28556–28566. [Google Scholar] [CrossRef]
- Mueller, A.L.; Brockmueller, A.; Kunnumakkara, A.B.; Shakibaei, M. Calebin A, a Compound of Turmeric, Down-Regulates Inflammation in Tenocytes by NF-κB/Scleraxis Signaling. Int. J. Mol. Sci. 2022, 23, 1695. [Google Scholar] [CrossRef] [PubMed]
- Chen, B.; Liang, Y.; Zhang, J.; Bai, L.; Xu, M.; Han, Q.; Han, X.; Xiu, J.; Li, M.; Zhou, X.; et al. Synergistic enhancement of tendon-to-bone healing via anti-inflammatory and pro-differentiation effects caused by sustained release of Mg2+/curcumin from injectable self-healing hydrogels. Theranostics 2021, 11, 5911–5925. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Xie, Y.; Liu, M.; Hu, J.; Tang, C.; Huang, J.; Qin, T.; Chen, X.; Chen, W.; Shen, W.; et al. Controlled-release curcumin attenuates progression of tendon ectopic calcification by regulating the differentiation of tendon stem/progenitor cells. Mater. Sci. Eng. C Mater. Biol. Appl. 2019, 103, 109711. [Google Scholar] [CrossRef] [PubMed]
- Henrotin, Y.; Dierckxsens, Y.; Delisse, G.; Seidel, L.; Albert, A. Curcuminoids and Boswellia serrata extracts combination decreases tendinopathy symptoms: Findings from an open-label post-observational study. Curr. Med. Res. Opin. 2021, 37, 423–430. [Google Scholar] [CrossRef] [PubMed]
- Davis, J.M.; Murphy, E.A.; Carmichael, M.D.; Zielinski, M.R.; Groschwitz, C.M.; Brown, A.S.; Gamgemi, J.D.; Ghaffar, A.; Mayer, E.P. Curcumin effects on inflammation and performance recovery following eccentric exercise-induced muscle damage. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2007, 292, R2168–R2173. [Google Scholar] [CrossRef]
- Kawanishi, N.; Kato, K.; Takahashi, M.; Mizokami, T.; Otsuka, Y.; Imaizumi, A.; Shiva, D.; Yano, H.; Suzuki, K. Curcumin attenuates oxidative stress following downhill running-induced muscle damage. Biochem. Biophys. Res. Commun. 2013, 441, 573–578. [Google Scholar] [CrossRef] [PubMed]
- Boz, I.; Belviranli, M.; Okudan, N. Curcumin Modulates Muscle Damage but not Oxidative Stress and Antioxidant Defense Following Eccentric Exercise in Rats. Int. J. Vitam Nutr. Res. 2014, 84, 163–172. [Google Scholar] [CrossRef]
- Drobnic, F.; Riera, J.; Appendino, G.; Togni, S.; Franceschi, F.; Valle, X.; Pons, A.; Tur, J. Reduction of delayed onset muscle soreness by a novel curcumin delivery system (Meriva®): A randomised, placebo-controlled trial. J. Int. Soc. Sports Nutr. 2014, 11, 31. [Google Scholar] [CrossRef]
- Tanabe, Y.; Maeda, S.; Akazawa, N.; Zempo-Miyaki, A.; Choi, Y.; Ra, S.G.; Imaizumi, A.; Otsuka, Y.; Nosaka, K. Attenuation of indirect markers of eccentric exercise-induced muscle damage by curcumin. Eur. J. Appl. Physiol. 2015, 115, 1949–1957. [Google Scholar] [CrossRef]
- Nicol, L.M.; Rowlands, D.S.; Fazakerly, R.; Kellett, J. Curcumin supplementation likely attenuates delayed onset muscle soreness (DOMS). Eur. J. Appl. Physiol. 2015, 115, 1769–1777. [Google Scholar] [CrossRef]
- McFarlin, B.K.; Venable, A.S.; Henning, A.L.; Sampson, J.N.B.; Pennel, K.; Vingren, J.L.; Hill, D.W. Reduced inflammatory and muscle damage biomarkers following oral supplementation with bioavailable curcumin. BBA Clin. 2016, 5, 72–78. [Google Scholar] [CrossRef] [PubMed]
- Nakhostin-Roohi, B. The Effect of Curcumin Supplementation on Selected Markers of Delayed Onset Muscle Soreness (DOMS). Ann. Appl. Sport Sci. 2016, 4, 25–31. [Google Scholar] [CrossRef]
- Delecroix, B.; Abaïdia, A.E.; Leduc, C.; Dawson, B.; Dupont, G. Curcumin and Piperine Supplementation and Recovery Following Exercise Induced Muscle Damage: A Randomized Controlled Trial. J. Sports Sci. Med. 2017, 16, 147–153. [Google Scholar] [PubMed]
- Tanabe, Y.; Chino, K.; Ohnishi, T.; Ozawa, H.; Sagayama, H.; Maeda, S.; Takahashi, H. Effects of oral curcumin ingested before or after eccentric exercise on markers of muscle damage and inflammation. Scand. J. Med. Sci. Sports 2019, 29, 524–534. [Google Scholar] [CrossRef]
- Jäger, R.; Purpura, M.; Kerksick, C.M. Eight Weeks of a High Dose of Curcumin Supplementation May Attenuate Performance Decrements Following Muscle-Damaging Exercise. Nutrients 2019, 11, 1692. [Google Scholar] [CrossRef] [PubMed]
- Jäger, R.; Kerksick, C.M.; Campbell, B.I.; Cribb, P.J.; Wells, S.D.; Skwiat, T.M.; Purpura, M.; Ziegenfuss, T.N.; Ferrando, A.A.; Arent, A.S.; et al. International Society of Sports Nutrition Position Stand: Protein and exercise. J. Int. Soc. Sports Nutr. 2017, 14, 20. [Google Scholar] [CrossRef]
- Tanabe, Y.; Chino, K.; Sagayama, H.; Lee, H.J.; Ozawa, H.; Maeda, S.; Takahashi, H. Effective Timing of Curcumin Ingestion to Attenuate Eccentric Exercise-Induced Muscle Soreness in Men. J. Nutr. Sci. Vitam. 2019, 65, 82–89. [Google Scholar] [CrossRef] [PubMed]
- Basham, S.A.; Waldman, H.S.; Krings, B.M.; Lamberth, J.; Smith, J.W.; McAllister, M.J. Effect of Curcumin Supplementation on Exercise-Induced Oxidative Stress, Inflammation, Muscle Damage, and Muscle Soreness. J. Diet. Suppl. 2020, 17, 401–414. [Google Scholar] [CrossRef]
- Cardaci, T.D.; Machek, S.B.; Wilburn, D.T.; Hwang, P.S.; Willoughby, D.S. Ubiquitin Proteasome System Activity is Suppressed by Curcumin following Exercise-Induced Muscle Damage in Human Skeletal Muscle. J. Am. Coll. Nutr. 2021, 40, 401–411. [Google Scholar] [CrossRef]
- Mallard, A.R.-; Briskey, D.; Richards BExSSc, A.; Rao, A. Curcumin Improves Delayed Onset Muscle Soreness and Postexercise Lactate Accumulation. J. Diet. Suppl. 2021, 18, 531–542. [Google Scholar] [CrossRef]
- Amalraj, A.; Divya, C.; Gopi, S. The Effects of Bioavailable Curcumin (Cureit) on Delayed Onset Muscle Soreness Induced By Eccentric Continuous Exercise: A Randomized, Placebo-Controlled, Double-Blind Clinical Study. J. Med. Food 2020, 23, 545–553. [Google Scholar] [CrossRef] [PubMed]
- Hillman, A.R.; Gerchman, A.; O’Hora, E. Ten Days of Curcumin Supplementation Attenuates Subjective Soreness and Maintains Muscular Power Following Plyometric Exercise. J. Diet. Suppl. 2022, 19, 303–317. [Google Scholar] [CrossRef] [PubMed]
- Srimal, R.C.; Dhawan, B.N. Pharmacology of diferuloyl methane (curcumin), a non-steroidal anti-inflammatory agent. J. Pharm. Pharm. 1973, 25, 447–452. [Google Scholar] [CrossRef] [PubMed]
- Ammon, H.; Anazodo, M.; Safayhi, H.; Dhawan, B.; Srimal, R. Curcumin: A Potent Inhibitor of Leukotriene B4 Formation in Rat Peritoneal Polymorphonuclear Neutrophils (PMNL). Planta Med. 1992, 58, 226. [Google Scholar] [CrossRef]
- Shishodia, S. Curcumin: Getting Back to the Roots. Ann. N. Y. Acad. Sci. 2005, 1056, 206–217. [Google Scholar] [CrossRef] [PubMed]
- Amit, S.; Ben-Neriah, Y. NF-κB activation in cancer: A challenge for ubiquitination- and proteasome-based therapeutic approach. Semin. Cancer Biol. 2003, 13, 15–28. [Google Scholar] [CrossRef] [PubMed]
- Hatcher, H.; Planalp, R.; Cho, J.; Torti, F.M.; Torti, S.V. Curcumin: From ancient medicine to current clinical trials. Cell Mol. Life Sci. 2008, 65, 1631–1652. [Google Scholar] [CrossRef] [PubMed]
- Gao, X.; Kuo, J.; Jiang, H.; Deeb, D.; Liu, Y.; Divine, G.; Chapman, R.A.; Dulchavsky, S.A.; Gautam, S.C. Immunomodulatory activity of curcumin: Suppression of lymphocyte proliferation, development of cell-mediated cytotoxicity, and cytokine production in vitro. Biochem. Pharm. 2004, 68, 51–61. [Google Scholar] [CrossRef]
- Surh, Y.J. Anti-tumor promoting potential of selected spice ingredients with antioxidative and anti-inflammatory activities: A short review. Food Chem. Toxicol. 2002, 40, 1091–1097. [Google Scholar] [CrossRef]
- Hanai, H.; Sugimoto, K. Curcumin has Bright Prospects for the Treatment of Inflammatory Bowel Disease. Curr. Pharm. Des. 2009, 15, 2087–2094. [Google Scholar] [CrossRef]
- Chan, M.M.Y.; Huang, H.I.; Fenton, M.R.; Fong, D. In Vivo Inhibition of Nitric Oxide Synthase Gene Expression by Curcumin, a Cancer Preventive Natural Product with Anti-Inflammatory Properties. Biochem. Pharm. 1998, 55, 1955–1962. [Google Scholar] [CrossRef] [PubMed]
- Hewlings, S.; Kalman, D. Curcumin: A Review of Its Effects on Human Health. Foods 2017, 6, 92. [Google Scholar] [CrossRef]
- Derosa, G.; Maffioli, P.; Simental-Mendía, L.E.; Bo, S.; Sahebkar, A. Effect of curcumin on circulating interleukin-6 concentrations: A systematic review and meta-analysis of randomized controlled trials. Pharm. Res. 2016, 111, 394–404. [Google Scholar] [CrossRef] [PubMed]
- Sahebkar, A.; Cicero, A.F.G.; Simental-Mendía, L.E.; Aggarwal, B.B.; Gupta, S.C. Curcumin downregulates human tumor necrosis factor-α levels: A systematic review and meta-analysis ofrandomized controlled trials. Pharm. Res. 2016, 107, 234–242. [Google Scholar] [CrossRef]
- Kahkhaie, K.R.; Mirhosseini, A.; Aliabadi, A.; Mohammadi, A.; Mousavi, M.J.; Haftcheshmeh, S.M.; Sathyapalan, T.; Sahebkar, A. Curcumin: A modulator of inflammatory signaling pathways in the immune system. Inflammopharmacol 2019, 27, 885–900. [Google Scholar] [CrossRef]
- Kumar, D.; Kumar, M.; Saravanan, C.; Singh, S.K. Curcumin: A potential candidate for matrix metalloproteinase inhibitors. Expert. Opin. Ther. Targets 2012, 16, 959–972. [Google Scholar] [CrossRef]
- Ebrahimi, S.; Esfahani, S.A.; Kohkiloezadeh, M.; Moghaddam, B.H.; Askarian, S.; Tanideh, N.; Tamadon, A. A model of cerebral ischemia induction in neonatal rabbits. J. Appl. Anim. Res. 2012, 40, 37–42. [Google Scholar] [CrossRef]
- Sies, H. Oxidative stress: A concept in redox biology and medicine. Redox Biol. 2015, 4, 180–183. [Google Scholar] [CrossRef]
- Sreejayan, M.N.R. Nitric oxide scavenging by curcuminoids. J. Pharm. Pharm. 1997, 49, 105–107. [Google Scholar] [CrossRef]
- Joe, B.; Lokesh, B.R. Role of capsaicin, curcumin and dietary n—3 fatty acids in lowering the generation of reactive oxygen species in rat peritoneal macrophages. Biochim. Biophys. Acta 1994, 1224, 255–263. [Google Scholar] [CrossRef]
- Lin, J.K.; Shih, C.A. Inhibitory effect of curcumin on xanthine dehydrogenase/oxidase induced by phorbol-12-myristate-13-acetate in NJH3T3 cells. Carcinogenesis 1994, 15, 1717–1721. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Lázaro, D.; Mielgo-Ayuso, J.; Seco-Calvo, J.; Córdova-Martínez, A.; Caballero-García, A.; Fernandez-Lazaro, C. Modulation of Exercise-Induced Muscle Damage, Inflammation, and Oxidative Markers by Curcumin Supplementation in a Physically Active Population: A Systematic Review. Nutrients 2020, 12, 501. [Google Scholar] [CrossRef] [PubMed]
- Matteucci, A.; Cammarota, R.; Paradisi, S.; Varano, M.; Balduzzi, M.; Leo, L.; Bellenchi, G.C.; Nuccio, C.D.; Carnovale-Scalzo, G.; Scorcia, G.; et al. Curcumin Protects against NMDA-Induced Toxicity: A Possible Role for NR2A Subunit. Investig. Ophthalmol. Vis. Sci. 2011, 52, 1070–1077. [Google Scholar] [CrossRef] [PubMed]
- Bright, J.J. Curcumin and autoimmune disease. In The Molecular Targets and Therapeutic Uses of Curcumin in Health and Disease; Aggarwal, B.B., Surh, Y.J., Shishodia, S., Eds.; Springer: Boston, MA, USA, 2007; pp. 425–451. [Google Scholar]
- Xie, L.; Li, X.K.; Takahara, S. Curcumin has bright prospects for the treatment of multiple sclerosis. Int. Immunopharmacol. 2011, 11, 323–330. [Google Scholar] [CrossRef]
- Chandran, B.; Goel, A. A Randomized, Pilot Study to Assess the Efficacy and Safety of Curcumin in Patients with Active Rheumatoid Arthritis. Phytother. Res. 2012, 26, 1719–1725. [Google Scholar] [CrossRef]
- Pari, L.; Murugan, P. Influence of tetrahydrocurcumin on tail tendon collagen contents and its properties in rats with streptozotocin–nicotinamide-induced type 2 diabetes. Fundam. Clin. Pharm. 2007, 21, 665–671. [Google Scholar] [CrossRef]
- Johansson, H.; Sojka, P. Pathophysiological mechanisms involved in genesis and spread of muscular tension in occupational muscle pain and in chronic musculoskeletal pain syndromes: A hypothesis. Med. Hypotheses 1991, 35, 196–203. [Google Scholar] [CrossRef]
- Birznieks, I.; Burton, A.R.; Macefield, V.G. The effects of experimental muscle and skin pain on the static stretch sensitivity of human muscle spindles in relaxed leg muscles: Effect of pain on muscle spindle stretch sensitivity. J. Physiol. 2008, 586, 2713–2723. [Google Scholar] [CrossRef]
- Lund, J.P.; Donga, R.; Widmer, C.G.; Stohler, C.S. The pain-adaptation model: A discussion of the relationship between chronic musculoskeletal pain and motor activity. Can. J. Physiol. Pharm. 1991, 69, 683–694. [Google Scholar] [CrossRef]
- Sahebkar, A.; Henrotin, Y. Analgesic Efficacy and Safety of Curcuminoids in Clinical Practice: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Pain Med. 2015, 17, 1192–1202. [Google Scholar] [CrossRef]
- Drobnic, F. Curcumin reduces pain in DOMS. Pain 2016, 157, 2390–2391. [Google Scholar] [CrossRef] [PubMed]
- Moini Zanjani, T.; Ameli, H.; Labibi, F.; Sedaghat, K.; Sabetkasaei, M. The Attenuation of Pain Behavior and Serum COX-2 Concentration by Curcumin in a Rat Model of Neuropathic Pain. Korean J. Pain 2014, 27, 246–252. [Google Scholar] [CrossRef] [PubMed]
- Enyeart, J.A.; Liu, H.; Enyeart, J.J. Curcumin inhibits bTREK-1 K+ channels and stimulates cortisol secretion from adrenocortical cells. Biochem. Biophys. Res. Commun. 2008, 370, 623–628. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Wei, S.; Xu, H.; Xia, D.; Zhao, R. Curcumin attenuates the effects of transport stress on serum cortisol concentration, hippocampal NO production, and BDNF expression in the pig. Domest. Anim. Endocrinol. 2010, 39, 231–239. [Google Scholar] [CrossRef]
- Marchesi, N.; Govoni, S.; Allegri, M. Non-drug pain relievers active on non-opioid pain mechanisms. Pain Pract. 2021, 22, 255–275. [Google Scholar] [CrossRef] [PubMed]
- Hasriadi; Dasuni Wasana, P.W.; Vajragupta, O.; Rojsitthisak, P.; Towiwat, P. Mechanistic Insight into the Effects of Curcumin on Neuroinflammation-Driven Chronic Pain. Pharmaceuticals 2021, 14, 777. [Google Scholar] [CrossRef]
- Leamy, A.W.; Shukla, P.; McAlexander, M.A.; Carr, M.J.; Ghatta, S. Curcumin ((E,E)-1,7-bis(4-hydroxy-3-methoxyphenyl)-1,6-heptadiene-3,5-dione) activates and desensitizes the nociceptor ion channel TRPA1. Neurosci. Lett. 2011, 503, 157–162. [Google Scholar] [CrossRef]
- Yeon, K.Y.; Kim, S.A.; Kim, Y.H.; Lee, M.K.; Ahn, D.K.; Kim, H.J.; Kim, J.S.; Jung, S.J.; Oh, S.B. Curcumin Produces an Antihyperalgesic Effect via Antagonism of TRPV1. J. Dent. Res. 2010, 89, 170–174. [Google Scholar] [CrossRef]
- Bahramsoltani, R.; Rahimi, R.; Farzaei, M.H. Pharmacokinetic interactions of curcuminoids with conventional drugs: A review. J. Ethnopharmacol. 2017, 209, 1–12. [Google Scholar] [CrossRef]
- Williams, J.A.; Hyland, R.; Jones, B.C.; Smith, D.A.; Hurst, S.; Goosen, T.C.; Peterkin, V.; Koup, J.R.; Ball, S.E. Drug-drug interactions for UDP-glucuronosyltransferase substrates: A pharmacokinetic explanation for typically observed low exposure (AUCi/AUC) ratios. Drug Metab. Dispos. 2004, 32, 1201–1208. [Google Scholar] [CrossRef]
- Barua, N.; Buragohain, A.K. Therapeutic Potential of Curcumin as an Antimycobacterial Agent. Biomolecules 2021, 11, 1278. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Lim, L.Y. Effects of Spice Constituents on P-Glycoprotein-Mediated Transport and CYP3A4-Mediated Metabolism in Vitro. Drug Metab. Dispos. 2008, 36, 1283–1290. [Google Scholar] [CrossRef] [PubMed]
- Leynadier, F.; Duarte-Risselin, C.; Murrieta, M. Comparative therapeutic effect and safety of mizolastine and loratadine in chronic idiopathic urticaria. URTILOR study group. Eur. J. Derm. 2000, 10, 205–211. [Google Scholar]
- Pavithra, B.H.; Prakash, N.; Jayakumar, K. Modification of pharmacokinetics of norfloxacin following oral administration of curcumin in rabbits. J. Vet. Sci. 2009, 10, 293. [Google Scholar] [CrossRef] [PubMed]
- Johnson, M.D.; Perfect, J.R. Use of Antifungal Combination Therapy: Agents, Order, and Timing. Curr. Fungal Infect. Rep. 2010, 4, 87–95. [Google Scholar] [CrossRef]
- Fredriksson, M.; Li, Y.; Stålman, A.; Haldosén, L.A.; Felländer-Tsai, L. Diclofenac and triamcinolone acetonide impair tenocytic differentiation and promote adipocytic differentiation of mesenchymal stem cells. J. Orthop. Surg. Res. 2013, 8, 30. [Google Scholar] [CrossRef]
- Ghosh, N.; Kolade, O.O.; Shontz, E.; Rosenthal, Y.; Zuckerman, J.D.; Bosco, J.A.; Virk, M.S. Nonsteroidal Anti-Inflammatory Drugs (NSAIDs) and Their Effect on Musculoskeletal Soft-Tissue Healing: A Scoping Review. JBJS Rev. 2019, 7, e4. [Google Scholar] [CrossRef]
- Schug, S.A. Do NSAIDs Really Interfere with Healing after Surgery? J. Clin. Med. 2021, 10, 2359. [Google Scholar] [CrossRef]
- Duchman, K.R.; Lemmex, D.B.; Patel, S.H.; Ledbetter, L.; Garrigues, G.E.; Riboh, J.C. The Effect of Non-Steroidal Anti-Inflammatory Drugs on Tendon-to-Bone Healing: A Systematic Review with Subgroup Meta-Analysis. Iowa Orthop. J. 2019, 39, 107–119. [Google Scholar]
- Tang, W. The Metabolism of Diclofenac—Enzymology and Toxicology Perspectives. Curr Drug Metab. 2003, 4, 319–329. [Google Scholar] [CrossRef]
- Lynch, T.; Price, A. The effect of cytochrome P450 metabolism on drug response, interactions, and adverse effects. Am. Fam. Physician 2007, 76, 391–396. [Google Scholar] [PubMed]
- Anand, P.; Kunnumakkara, A.B.; Newman, R.A.; Aggarwal, B.B. Bioavailability of Curcumin: Problems and Promises. Mol. Pharm. 2007, 4, 807–818. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.C.; Prasad, S.; Kim, J.H.; Patchva, S.; Webb, L.J.; Priyadarsini, I.K.; Aggarwal, B.B. Multitargeting by curcumin as revealed by molecular interaction studies. Nat. Prod. Rep. 2011, 28, 1937. [Google Scholar] [CrossRef] [PubMed]
- Dei Cas, M.; Ghidoni, R. Dietary Curcumin: Correlation between Bioavailability and Health Potential. Nutrients 2019, 11, 2147. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Lu, Y.; Lee, R.J.; Xiang, G. Nano Encapsulated Curcumin: And Its Potential for Biomedical Applications. Int. J. Nanomed. 2020, 15, 3099–3120. [Google Scholar] [CrossRef] [PubMed]
- Bresciani, L.; Favari, C.; Calani, L.; Francinelli, V.; Riva, A.; Petrangolini, G.; Allegrini, P.; Mena, P.; Del Rio, D. The Effect of Formulation of Curcuminoids on Their Metabolism by Human Colonic Microbiota. Molecules 2020, 25, 940. [Google Scholar] [CrossRef] [PubMed]
- Slika, L.; Patra, D. A short review on chemical properties, stability and nano-technological advances for curcumin delivery. Expert. Opin. Drug Deliv. 2020, 17, 61–75. [Google Scholar] [CrossRef]
- Witika, B.A.; Makoni, P.A.; Matafwali, S.K.; Mweetwa, L.L.; Shandele, G.C.; Walker, R.B. Enhancement of Biological and Pharmacological Properties of an Encapsulated Polyphenol: Curcumin. Molecules 2021, 26, 4244. [Google Scholar] [CrossRef]
- Gupta, S.C.; Patchva, S.; Aggarwal, B.B. Therapeutic Roles of Curcumin: Lessons Learned from Clinical Trials. AAPS J. 2013, 15, 195–218. [Google Scholar] [CrossRef]
- Cheng, A.L.; Hsu, C.H.; Lin, J.K.; Hsu, M.M.; Ho, Y.F.; Shen, T.S.; Ko, J.Y.; Lin, J.T.; Lin, B.R.; Ming-Shiang, W.; et al. Phase I clinical trial of curcumin, a chemopreventive agent, in patients with high-risk or pre-malignant lesions. Anticancer Res. 2001, 21, 2895–2900. [Google Scholar]
- Sharma, R.A.; Steward, W.P.; Gescher, A.J. Pharmacokinetics and Pharmacodynamics of circumin. In The Molecular Targets and Therapeutic Uses of Curcumin in Health and Disease; Aggarwal, B.B., Surh, Y.J., Shishodia, S., Eds.; Springer: Boston, MA, USA, 2007; Volume 595, pp. 453–470. [Google Scholar]
- Heger, M.; van Golen, R.F.; Broekgaarden, M.; Michel, M.C. The Molecular Basis for the Pharmacokinetics and Pharmacodynamics of Curcumin and Its Metabolites in Relation to Cancer. Pharm. Rev. 2014, 66, 222–307. [Google Scholar] [CrossRef] [PubMed]
- Coleman, B.D.; Khan, K.M.; Maffulli, N.; Cook, J.L.; Wark, J.D. Studies of surgical outcome after patellar tendinopathy: Clinical significance of methodological deficiencies and guidelines for future studies: Surgical outcome of patellar tendinopathy. Scand. J. Med. Sci. Sports 2000, 10, 2–11. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference | Molecule/s | Dosage | Route | Days | Placebo/Control | n | Type of Subjects | Type Injury | Tests | Impact on Resolution. | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Davis JM et al. (2007) | [99] | Curcumin | 10 mg (≈40 mg/kg) | Oral (pellets) | 3 | P | 64 | Rodents | Eccentric exercise or Concentric exercise | Blood analysis (CK, Inflamation), FP | ⊕ Running time to fatigue, running distance, IL-1β, IL-6, TNF-α, in the eccentric exercise working set of animals. |
| Kawanishi N et al. (2013) | [100] | Curcumin (Theracurmin®) | 3 mg | Oral (after injury) | 1 | P | 52 | Rodents | Eccentric exercise | Blood analysis (M Injury, Inflamation pattern) muscle immunohisyology | ⊕ NADPH oxidase, MCP-1 and F4/80 mRNA expression, H2O2, attenuated oxidative stress ≈ CK, LDH, COX2 expression., |
| Boz I et al. (2014) | [101] | Curcumin | 200 mg/kg | Oral gavage | 20 | P | 30 | Rodents | Eccentric exercise | Blood analysis (M Injury, Inflamation pattern, oxidative pattern) Muscle histology,. | ⊕ CK, Mb ≈ MDA, SOD, GPx |
| Drobnic F et al. (2014) | [102] | Curcumin (Meriva®) | 200 mg/day (2 g Meriva®) | Oral | 4 | P | 20 | Human | Eccentric exercise | Blood analysis (CK, Inflamation, oxidative pattern), VAS. | ⊕ IL-8, VAS; ≈ CRP, MCP1, CK, TAC. |
| Tanabe et al. (2015) | [103] | Curcumin (Theracurmin®) | 150 mg/day | Oral | 1 | P | 14 | Human | Eccentric exercise | Blood analysis (M Injury, Inflamation pattern), VAS, FP, Arm circumference | ⊕ CK, MVIC ≈ ROM, VAS, IL-6, TNF-α, Arm circumference |
| Nicol et al. (2015) | [104] | Curcumin (Eurofins Scientific Inc) | 2.5 g/12 h | Oral | 5 | P | 19 | Human | Eccentric exercise | Blood analysis (M Injury, Inflamation pattern), VAS, FP | ⊕ VAS, CK, IL-6, Exercise performance. ≈ Swelling, TNF-α |
| McFarlin et al. (2016) | [105] | Curcumin (Longvida®) | 400 mg/day | Oral | 6 | P | 28 | Human | Eccentric exercise | Blood analysis (CK, Inflamation, oxidative pattern), VAS, FP | ⊕, CK, IL-8, TNF-α. ≈ VAS, IL-6, IL-10 |
| Nakhostin-Roohi B et al. (2016) | [106] | Curcumin (Theracurmin®) | 1150 mg | Oral (after injury) | 1 | P | 10 | Human | Eccentric exercise | Blood analysis (M Injury, Inflamation pattern), VAS. | ⊕ VAS, CK, ALT, AST, TAC |
| Delecroix B et al. (2017) | [107] | Curcumin + Piperine (*) | 2 g/8 h | Oral | 4 | P | 10 | Human | Eccentric exercise | Blood analysis (M Injury, Inflamation, oxidative pattern), VAS, FP | ⊕ Exercise performance. ≈ VAS, CK. |
| Tanabe Y et al. (2019) | [108] | Curcumin (Theracurmin®) | 90 mg/12 h | Oral | 11 | P | 24 | Human | Eccentric exercise | Blood analysis (CK), VAS, FP | ⊕ VAS, ROM ≈ MVIC, CK. |
| Reference | Molecule/s | Dosage | Route | Days | Placebo/Control | n | Type of Subjects | Type Injury | Tests | Impact on Resolution. | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Jäger R et al. (2019) | [109] | Curcumin (CurcuWIN®) | 50 or 200 mg/day | Oral | 56 | P | 74 | Humans | Eccentric exercise | VAS, FP (Isokinetic and isometric test) | ≈ VAS, isokinetic strength tests. ⊕ tendency in VAS and some isokinetic test for the 200 mg dosage. |
| Tanabe Y et al. (2019) Ex I | [110] | Curcumin (Theracurmin®) | 90 mg/12 h | Oral Before injury | 7 | P | 10 | Human | Eccentric exercise | Blood analysis (M Injury, Inflamation, oxidative pattern), VAS, FP | ⊕ IL-8, ≈ VAS, Swelling, CK, MVIC, ROM, TNF-α, BAP, |
| Tanabe Y et al. (2019) Ex II | Oral After injury | 10 | ⊕ VAS, CK, MVIC, ROM, d-ROMs. ≈ Swelling, IL-8,, TNF-α, BAP, d-ROMs. | ||||||||
| Basham SA et al. (2020) | [111] | Curcumin (CurcuFresh®) | 1.5 g/day | Oral | 28 | P | 20 | Human | Eccentric exercise | Blood analysis (M Injury, Inflamation pattern, oxidative pattern), VAS | ⊕ CK, VAS, TAC, MDA, TNFα, |
| Cardaci TD et al. (2020) | [113] | Curcumin + Piperine (*) | 2 g/day | Oral | 11 | P (Piperine) | 23 | Human | Eccentric exercise | Muscle biopsy, VAS, | ⊕ Ubiquitin, MAFbx/Atrogin-1. UPS dysregulation is mediated by downregulation of proteasome catalytic enzymes. ≈ USP19, VAS. |
| Mallard AR et al. (2020) | [114] | Curcumin (+LipiSperse) | 450 mg/day | Oral | 1 | P | 27 | Human | Eccentric exercise | Blood analysis (CK, Inflamation, oxidative pattern), VAS, FP | ⊕, VAS, Swelling (TC), Lac, IL-10, IL-6, IL-8, ≈ CK, LDH, CRP-Hs, Mb, TNF-α, |
| Amalraj A et al. (2020) | [115] | Curcumin (Cureit®) | 500 mg/day | Oral | 4 | P | 30 | Human | Eccentric exercise | Blood analysis (CK), VAS, FP (maximal aerobic exercise testing) | ⊕ VAS, ≈ CK, VO2 max |
| Hillman AR et al. (2021) | [116] | Curcumin (CLE) | 475 mg/day | Oral | 10 | P | 22 | Humans | Eccentric exercise | Blood analysis (CK, ESRVAS, FP (vertical jump) | ⊕ VAS, Vertical jump ≈ CK, ESR |
| Reference | Molecule/s | Dosage | Route | Days | Placebo/Control | n | Type of Subjects | Type Injury | Tests | Impact on Resolution. | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Buhrmann et al. (2011) | [94] | Curcumin | 5–20 μM | Tenocytes culture in vitro | 12 h, 24 h, 48 h | C | - | Human tenocytes monolayer cultures | IL-1β stimulated tenocytes | Histology, Immunology | ⊕ modulation of NF-κB signaling, inhibited IL-1β-induced inflammation and apoptosis. Any toxicity on the cells |
| Mueller AL et al. (2022) | [95] | Calebin A | 5000 μM DMSO (<0.1%)). | Tenocytes culture in vitro | 18 h | C | - | Canine tenocytes monolayer cultures | Tendinitis μenvironment | Histology, Immunology | ⊕ inflammatory and degradative processes by blocking TNF-β, TNF-α-induced adhesiveness and T-lymphocytes facilitating down-regulation of Collagen I, Tenomodulin, tenocyte-specific transcription factor and the up-regulation of NF-κB phosphorylation;. |
| Chen B et al. (2021) | [96] | Curcumin, Mg, Chitosan | Hydrogel locally applied during surgery | 3–4–21 | C | Rodents | Rotator cuff C/R | Histology, Immunology, Biomechanical. | Promote rotator cuff tendon-to-bone healing ⊕ anti-inflammatory and antioxidation effects, ⊕ biomechanical tests and histological results | ||
| Chen Y et al. (2019) | [88] | Curcumin, Chitosan | 135 mg/mL | Hydrogel locally applied during surgery | Every 3 d/4 weeks | C | 21 | Rodents | Achilles tendon ectopic calcification model | Imaging (xR), Histology, Immunology. | ⊕ Partially reversed tendon calcification and enhanced tendon regeneration |
| Güleç A et al. (2018) | [89] | Curcumin | 200 mg/kg | Oral gavage | 28 | C | 18 | Rodents | Achilles tendon C/R | Histology and Biomechanical | ⊕ Tenocyte morphology, collagen, and ground substance scores, ⊕ Biomechanical parameters (failure load, cross-sectional area, length, ultimate stress, strain), ↔ Vascularization, |
| Jiang D et al. (2016) | [90] | Curcumin | 100 mg/kg | Oral gavage | 14 | C | 64 | Rodents | Patellar tendon | Histology, Immunology Gene expression, Biomechanical | ⊕ Organized collagen fiber, alignment, ⊕ collagen I, ⊕ biomechanical properties and ↑SOD, ↓MDA. |
| Zhang J et al. (2021) | [91] | Curcumin Celecoxib | - | Electrospun polyester membrane (EPM) | 3 | C | 40 | Rodents | Achilles tendon C/R | Histology, Immunology | The EPM with Curcumin and Celecoxib acts synergistically preventing peritendinous adhesion and inflammation. |
| Li Y et al. (2016) | [92] | Curcumin | 0.44 mg/kg/0.1 mL saline | Polymeric nanomicelles applied locally | 28 | C | 36 | Rodents | Achilles tendon C/R | Histology, Biomechanical | ⊕ inflammatory adhesion, ⊕ collagen fiber orientation ⊕ tendon strength |
| Merolla et al. (2015) | [97] | Curcuma, MSM, Boswellia, Vit C, Glucosamin, CS, Collagen, Arginin | 200 mg | Oral | 168 | P | 50 | Human | Rotator cuff surgery | VAS, PGAS, Constant–Murley Score, Biomechanical. | ⊕ postoperative rotator cuff short and partially mid-term pain, while longterm pain was unchanged, ⊕ concomitant treatment |
| Henrotin Y et al. (2021) | [98] | Curcumin, Boswellia | 144 mg | Oral | 30 | No | 670 | Human | Diverse tendinopathies | Analog visual scale (VAS), patien satisfaction | ⊕ pain score, concomitant treatment and patient satisfaction |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Córdova, A.; Drobnic, F.; Noriega-González, D.; Caballero-García, A.; Roche, E.; Alvarez-Mon, M. Is Curcumine Useful in the Treatment and Prevention of the Tendinopathy and Myotendinous Junction Injury? A Scoping Review. Nutrients 2023, 15, 384. https://doi.org/10.3390/nu15020384
Córdova A, Drobnic F, Noriega-González D, Caballero-García A, Roche E, Alvarez-Mon M. Is Curcumine Useful in the Treatment and Prevention of the Tendinopathy and Myotendinous Junction Injury? A Scoping Review. Nutrients. 2023; 15(2):384. https://doi.org/10.3390/nu15020384
Chicago/Turabian StyleCórdova, Alfredo, Franchek Drobnic, David Noriega-González, Alberto Caballero-García, Enrique Roche, and Melchor Alvarez-Mon. 2023. "Is Curcumine Useful in the Treatment and Prevention of the Tendinopathy and Myotendinous Junction Injury? A Scoping Review" Nutrients 15, no. 2: 384. https://doi.org/10.3390/nu15020384
APA StyleCórdova, A., Drobnic, F., Noriega-González, D., Caballero-García, A., Roche, E., & Alvarez-Mon, M. (2023). Is Curcumine Useful in the Treatment and Prevention of the Tendinopathy and Myotendinous Junction Injury? A Scoping Review. Nutrients, 15(2), 384. https://doi.org/10.3390/nu15020384