Consumption of Eggs Alone or Enriched with Annatto (Bixa orellana L.) Does Not Increase Cardiovascular Risk in Healthy Adults—A Randomized Clinical Trial, the Eggant Study

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
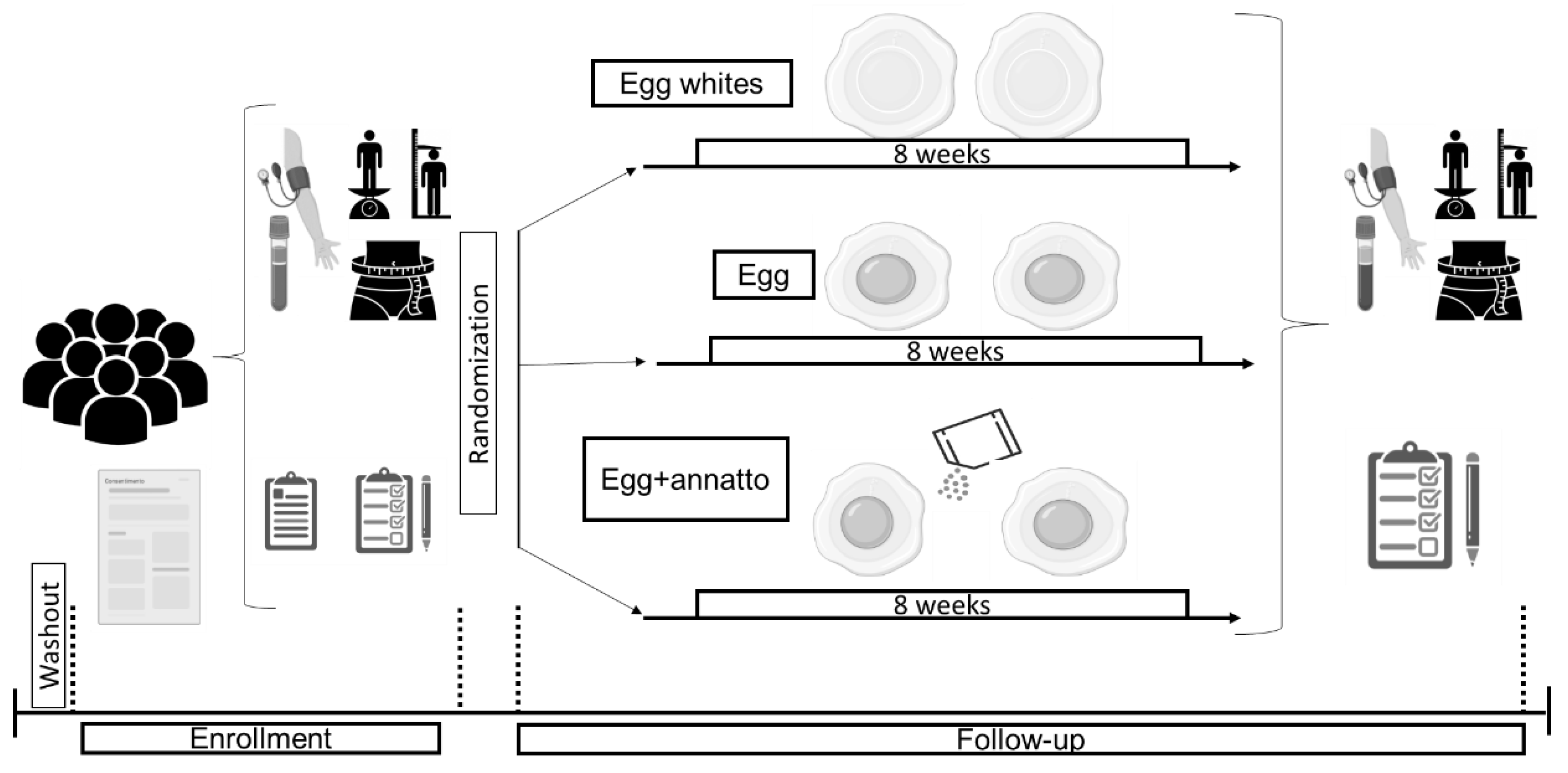
2.1. Intervention
2.2. Blood Collection
2.3. Anthropometric Measurements
2.4. Blood Lipid Profile, Glucose, and Liver Enzymes
2.5. Lipoproteins and Apolipoproteins
2.6. Diet Analysis
2.7. Statistical Analysis
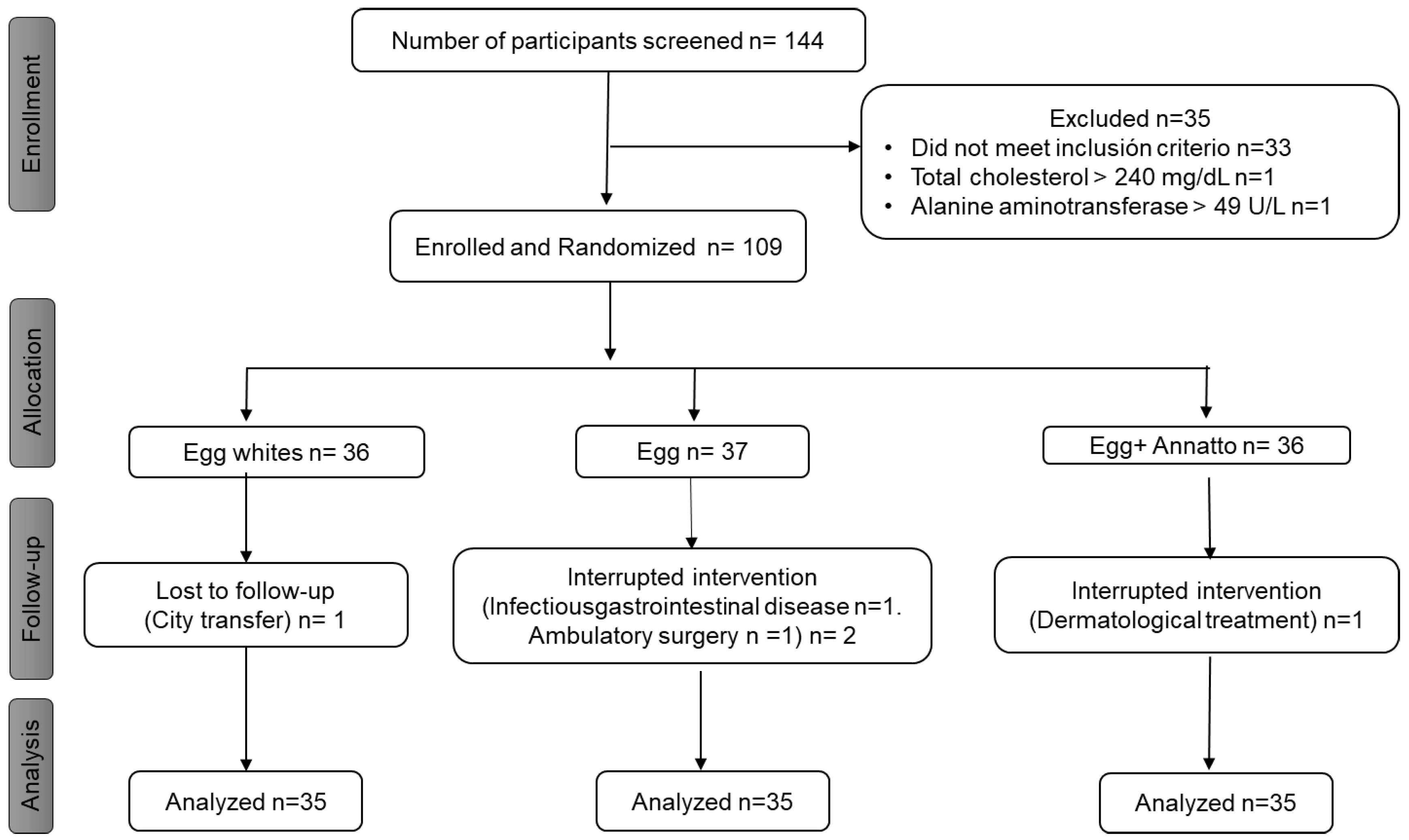
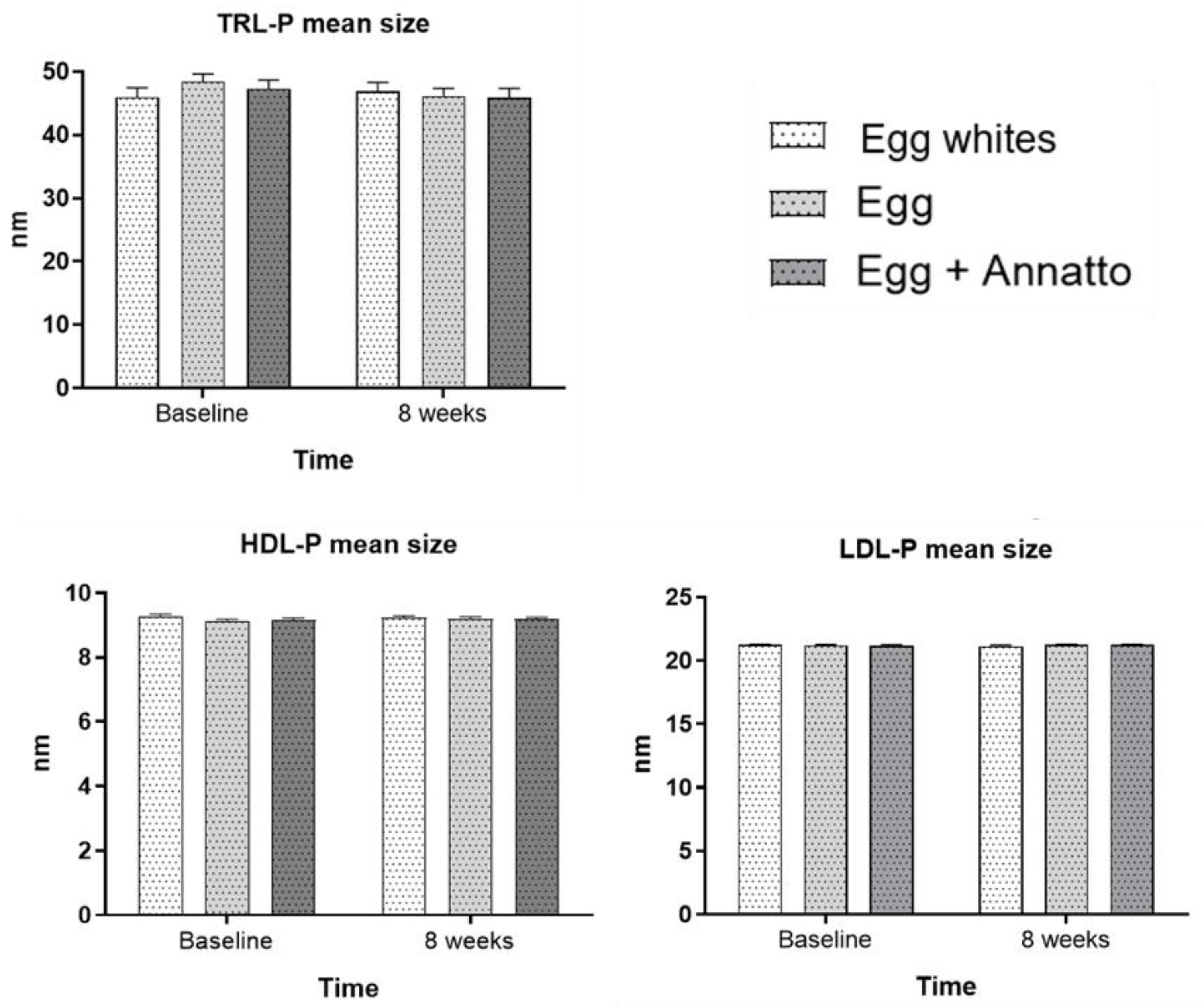
3. Results
4. Discussion
5. Conclusions
6. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vassilaki, M.; Linardakis, M.; Polk, D.M.; Philalithis, A. The burden of behavioral risk factors for cardiovascular disease in Europe. A significant prevention deficit. Prev. Med. 2015, 81, 326–332. [Google Scholar] [CrossRef] [PubMed]
- Powell-Wiley, T.M.; Poirier, P.; Burke, L.E.; Després, J.-P.; Gordon-Larsen, P.; Lavie, C.J.; Lear, S.A.; Ndumele, C.E.; Neeland, I.J.; Sanders, P.; et al. Obesity and Cardiovascular Disease A Scientific Statement From the American Heart Association. Circulation 2021, 143, E984–E1010. [Google Scholar] [CrossRef] [PubMed]
- Ministerio de Salud y Protección Social; Instituto Colombiano de Bienestar Familiar (ICBF); Instituto Nacional de Salud. Encuesta Nacional de la Situación Nutricional en Colombia-ENSIN 2010; Da Vinci Editores & CÍA S N C: Bogotá, Colombia, 2011; p. 365.
- Ministerio de Salud y Protección Social; Instituto Nacional de Salud; Instituto Colombiano de Bienestar Familiar (ICBF); Universidad Nacional de Colombia. Encuesta Nacional de la Situación Nutricional—ENSIN 2015; Editores & CÍA S N C: Bogotá, Colombia, 2020; p. 683.
- Chacón, C.; Ramírez, M. Poverty in Colombia, in times of COVID-19. Munich Pers RePEc Arch. 2020, 11, 1–14. [Google Scholar]
- Puglisi, M.J.; Fernandez, M.L. The Health Benefits of Egg Protein. Nutrients 2022, 14, 2904. [Google Scholar] [CrossRef] [PubMed]
- Kanter, M.M.; Kris-Etherton, P.M.; Fernandez, M.L.; Vickers, K.C.; Katz, D.L. Exploring the Factors That Affect Blood Cholesterol and Heart Disease Risk: Is Dietary Cholesterol as Bad for You as History Leads Us to Believe? Adv. Nutr. Int. Rev. J. 2012, 3, 711–717. [Google Scholar] [CrossRef]
- McNamara, D.J. The fifty year rehabilitation of the egg. Nutrients 2015, 7, 8716–8722. [Google Scholar] [CrossRef]
- Berger, S.; Raman, G.; Vishwanathan, R.; Jacques, P.F.; Johnson, E.J. Dietary cholesterol and cardiovascular disease: A systematic review. Am. J. Clin. Nutr. 2015, 102, 276–294. [Google Scholar] [CrossRef]
- Barona, J.; Fernandez, L. Dietary cholesterol affects plasma lipid levels, the intravascular processing of lipoproteins and reverse cholesterol transport without increasing the risk for heart disease. Nutrients 2012, 4, 1015–1025. [Google Scholar] [CrossRef]
- Dehghan, M.; Mente, A.; Rangarajan, S.; Mohan, V.; Lear, S.; Swaminathan, S.; Wielgosz, A.; Seron, P.; Avezum, A.; Lopez-Jaramillo, P.; et al. Association of egg intake with blood lipids, cardiovascular disease, and mortality in 177,000 people in 50 countries. Am. J. Clin. Nutr. 2020, 111, 795–803. [Google Scholar] [CrossRef]
- Mutungi, G.; Waters, D.; Ratliff, J.; Puglisi, M.; Clark, R.M.; Volek, J.S.; Fernandez, M.L. Eggs distinctly modulate plasma carotenoid and lipoprotein subclasses in adult men following a carbohydrate-restricted diet. J. Nutr. Biochem. 2010, 21, 261–267. [Google Scholar] [CrossRef]
- Chung, H.; Rasmussen, H.M.; Johnson, E.J. Lutein Bioavailability Is Higher from Lutein-Enriched Eggs than from Supplements and Spinach in Men. Hum. Nutr. Metab. 2004, 134, 1887–1893. [Google Scholar] [CrossRef] [PubMed]
- Khoo, H.E.; Prasad, K.N.; Kong, K.W.; Jiang, Y.; Ismail, A. Carotenoids and their isomers: Color pigments in fruits and vegetables. Molecules 2011, 16, 1710–1738. [Google Scholar] [CrossRef] [PubMed]
- Ciccone, M.; Cortese, F.; Gesualdo, M.; Carbonara, S.; Zito, A.; Ricci, G.; De Pascalis, F.; Scicchitano, P.; Riccioni, G. Dietary Intake of Carotenoids and Their Antioxidant and Anti-Inflammatory Effects in Cardiovascular Care. Mediat. Inflamm. 2013, 2013, 1–11. [Google Scholar] [CrossRef]
- Chen, J.; Song, Y.; Zhang, L. Effect of lycopene supplementation on oxidative stress: An exploratory systematic review and meta-analysis of randomized controlled trials. J. Med. Food 2013, 16, 361–374. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, M. Estudio de la irritación dérmica primaria en piel dañada de conejos tras la exposición a un extracto alcohólico de Bixa orellana lin. Rev. Cuba Estomatol. 2003, 34, 25–30. [Google Scholar]
- Bell, G.A.S.; Shamna, R.; Sangeetha, B.S.J. In Vivo antioxidant activity of bark extract of Bixa orellana L. against acetaminophen–induced oxidative stress. Asian Pac. J. Trop. Biomed. 2012, 2, S700–S705. [Google Scholar] [CrossRef]
- Gómez, G.C.; Castillo, J.C.Q.; Pérez, J.C.A.; Montoya, J.E.Z. Ethanolic extract from leaves of Bixa orellana L.: A potential natural food preservative. Interciencia 2012, 37, 547–551. [Google Scholar]
- Rivera-Madrid, R.; Aguilar-Espinosa, M.; Cárdenas-Conejo, Y.; Garza-Caligaris, L.E. Carotenoid Derivates in Achiote (Bixa orellana) Seeds: Synthesis and Health Promoting Properties. Front. Plant Sci. 2016, 7, 1–7. [Google Scholar] [CrossRef]
- da Silva, J.A.T.; Zeng, S.; Godoy-Hernández, G.; Rivera-Madrid, R.; Dobránszki, J. Bixa orellana L. (achiote) tissue culture: A review. Vitr. Cell Dev. Biol.-Plant 2019, 55, 231–241. [Google Scholar] [CrossRef]
- Pacheco, T.G.; Lopes, A.D.S.; Viana, G.D.M.; da Silva, O.N.; da Silva, G.M.; Vieira, L.D.N.; Guerra, M.P.; Nodari, R.O.; de Souza, E.M.; Pedrosa, F.D.O.; et al. Genetic, evolutionary and phylogenetic aspects of the plastome of annatto (Bixa orellana L.), the Amazonian commercial species of natural dyes. Planta 2019, 249, 563–582. [Google Scholar] [CrossRef]
- Kelly, E.R.; Plat, J.; Haenen, G.R.M.M.; Kijlstra, A.; Berendschot, T.T.J.M. The effect of modified eggs and an egg-yolk based beverage on serum lutein and zeaxanthin concentrations and macular pigment optical density: Results from a randomized trial. PLoS ONE 2014, 9, e92659. [Google Scholar] [CrossRef] [PubMed]
- Perez, A.; Rodriguez, M.; Gil, J.R.G.; Ramírez, G. Tamaño de Muestra Versión 1.1; Pontificia Universidad Javeriana: Bogotá, Colombia, 2001; p. 1. [Google Scholar]
- Abramson, J.H. WINPEPI updated: Computer programs for epidemiologists, and their teaching potential. Epidemiol. Perspect. Innov. 2011, 8, 1. [Google Scholar] [CrossRef] [PubMed]
- Scotter, M.J.; Castle, L.; Appleton, G.P. Kinetics and yields for the formation of coloured and aromatic thermal degradation products of annatto in foods. Food Chem. 2001, 74, 365–375. [Google Scholar] [CrossRef]
- Roehrs, M.; Conte, L.; da Silva, D.T.; Duarte, T.; Maurer, L.H.; de Carvalho, J.A.M.; Moresco, R.N.; Somacal, S.; Emanuelli, T. Annatto carotenoids attenuate oxidative stress and inflammatory response after high-calorie meal in healthy subjects. Food Res. Int. 2017, 100, 771–779. [Google Scholar] [CrossRef]
- Instituto Colombiano de Bienestar Familiar-ICBF; Universidad nacional de Colombia. Tabla de Composición de Alimentos Colombianos-TCAC, 1st ed.; ICBF: Bogotá, Colombia, 2018; p. 147.
- Monsalve, J.M.; González, L.I. Diseño de un cuestionario de frecuencia para evaluar ingesta alimentaria en la Universidad de Antioquia, Colombia. Nutr. Hosp. 2011, 26, 1333–1344. [Google Scholar]
- Marín-Echeverri, C.; Piedrahita-Blandón, M.; Galvis-Pérez, Y.; Blesso, B.; María-Luz Fernández, M.; Nuñez-Rangel, V.; Barona-Acevedo, J. Improvements in antioxidant status after agraz consumption was associated to reductions in cardiovascular risk factors in women with metabolic syndrome. CyTA-J. Food 2021, 19, 238–246. [Google Scholar] [CrossRef]
- Aristizabal, C.; Barona, J.; Gonzalez, L.; Deossa, G.; Estrada, A. Fatty acid content of plasma triglycerides may contribute to the heterogeneity in the relationship between abdominal obesity and the metabolic syndrome. Metab. Syndr. Relat. Disord. 2016, 14, 311–317. [Google Scholar] [CrossRef]
- Arnett, D.K.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; et al. ACC/AHA guideline on the primary prevention of cardiovascular disease: A report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019, 140, e596–e646. [Google Scholar]
- Khan, S.U.; Khan, M.Z.; Subramanian, C.R.; Riaz, H.; Khan, M.U.; Lone, A.N.; Khan, M.S.; Benson, E.M.; Alkhouli, M.; Blaha, M.J.; et al. Participation of Women and Older Participants in Randomized Clinical Trials of Lipid-Lowering Therapies: A Systematic Review. JAMA Netw Open. 2020, 3, 1–12. [Google Scholar] [CrossRef]
- Jin, X.; Chandramouli, C.; Allocco, B.; Gong, E.; Lam, C.S.P.; Yan, L.L. Women’s participation in cardiovascular clinical trials from 2010 to 2017. Circulation 2020, 141, 540–548. [Google Scholar] [CrossRef]
- Liu, K.A.; Mager, N.A.D. Women’s involvement in clinical trials: Historical perspective and future implications. Pharm Pract. 2016, 14, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Departamento Administrativo Nacional de Estadistica-DANE. Mercado Laboral de la Juventud Trimestre Móvil Junio-Agosto 2020; Boletín Técnico; DANE: Bogotá, Colombia, 2020; pp. 1–14.
- Nugent, R.; Levin, C.; Hale, J.; Hutchinson, B. Economic effects of the double burden of malnutrition. Lancet 2020, 395, 156–164. [Google Scholar] [CrossRef] [PubMed]
- Wells, J.C.; Sawaya, A.L.; Wibaek, R.; Mwangome, M.; Poullas, M.S.; Yajnik, C.S.; Demaio, A. The double burden of malnutrition: Aetiological pathways and consequences for health. Lancet 2020, 395, 75–88. [Google Scholar] [CrossRef] [PubMed]
- W Weintraub, W.S.; Daniels, S.R.; Burke, L.E.; Franklin, B.A.; Goff, D.C., Jr.; Hayman, L.L.; Lloyd-Jones, D.; Pandey, D.K.; Sanchez, E.J.; Schram, A.P.; et al. Value of primordial and primary prevention for cardiovascular disease: A policy statement from the American Heart Association. Circulation 2011, 124, 967–990. [Google Scholar] [CrossRef]
- Ratliff, J.; Leite, J.O.; de Ogburn, R.; Puglisi, M.J.; VanHeest, J.; Fernandez, M.L. Consuming eggs for breakfast influences plasma glucose and ghrelin, while reducing energy intake during the next 24 hours in adult men. Nutr Res. 2010, 30, 96–103. [Google Scholar] [CrossRef]
- Missimer, A.; Dimarco, D.M.; Andersen, C.J.; Murillo, A.G.; Vergara-Jimenez, M.; Fernandez, M.L. Consuming two eggs per day, as compared to an oatmeal breakfast, increases plasma ghrelin while maintaining the LDL/HDL ratio. Nutrients 2017, 9, 89. [Google Scholar] [CrossRef]
- Blesso, C.N.; Andersen, C.J.; Bolling, B.W.; Fernandez, M.L. Egg intake improves carotenoid status by increasing plasma HDL cholesterol in adults with metabolic syndrome. Food Funct. 2013, 4, 213–221. [Google Scholar] [CrossRef]
- Njike, V.; Faridi, Z.; Dutta, S.; Gonzalez-Simon, A.L.; Katz, D.L. Daily egg consumption in hyperlipidemic adults—Effects on endothelial function and cardiovascular risk. Nutr. J. 2010, 9, 1–9. [Google Scholar] [CrossRef]
- Zhong, V.W.; Van Horn, L.; Cornelis, M.C.; Wilkins, J.T.; Ning, H.; Carnethon, M.; Greenland, P.; Mentz, R.J.; Tucker, K.L.; Zhao, L.; et al. Associations of Dietary Cholesterol or Egg Consumption With Incident Cardiovascular Disease and Mortality. Jama 2019, 321, 1081–1095. [Google Scholar] [CrossRef]
- Akici, N.; Onal, Z.E.; Gürbüz, T.; Sağ, C.; Kilinç, S. Atherogenic indices in the assessment of cardiovascular disease risk in children with obesity and subclinical hypothyroidism. Acta Endocrinol. 2020, 16, 334–338. [Google Scholar] [CrossRef]
- Kazemi, T.; Hajihosseini, M.; Moossavi, M.; Hemmati, M.; Ziaee, M. Cardiovascular Risk Factors and Atherogenic Indices in an Iranian Population: Birjand East of Iran. Clin. Med. Insights Cardiol. 2018, 12, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Lemos, B.S.; Medina-Vera, I.; Blesso, C.N.; Fernandez, M.L. Intake of 3 eggs per day when compared to a choline bitartrate supplement, downregulates cholesterol synthesis without changing the LDL/HDL ratio. Nutrients 2018, 10, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Mutungi, G.; Ratliff, J.; Puglisi, M.; Torres-Gonzalez, M.; Vaishnav, U.; Leite, J.O.; Quann, E.; Volek, J.S.; Fernandez, M.L. Dietary cholesterol from eggs increases plasma HDL cholesterol in overweight men consuming a carbohydrate-restricted diet. J. Nutr. 2008, 138, 272–276. [Google Scholar] [CrossRef]
- Decewicz, D.J.; Neatrour, D.M.; Burke, A.; Haberkorn, M.J.; Patney, H.L.; Vernalis, M.N.; Ellsworth, D.L. Effects of cardiovascular lifestyle change on lipoprotein subclass profiles defined by nuclear magnetic resonance spectroscopy. Lipids Health Dis. 2009, 8, 26. [Google Scholar] [CrossRef] [PubMed]
- Johannesen, C.D.L.; Mortensen, M.B.; Langsted, A.; Nordestgaard, B.G. Apolipoprotein B and Non-HDL Cholesterol Better Reflect Residual Risk Than LDL Cholesterol in Statin-Treated Patients. J. Am. Coll. Cardiol. 2021, 77, 1439–1450. [Google Scholar] [CrossRef] [PubMed]
- de Lima Albuquerque, M.N.; da Silva Diniz, A.; de Arruda, I.K.G. Apolipoproteínas y su asociación con biomarcadores de riesgo cardiometabólico en adolescentes. Nutr. Hosp. 2015, 32, 2674–2683. [Google Scholar]
- Dominiczak, M.H.; Caslake, M.J. Apolipoproteins: Metabolic role and clinical biochemistry applications. Ann. Clin. Biochem. Int. J. Biochem. Lab. Med. 2011, 48, 498–515. [Google Scholar] [CrossRef]
- Behbodikhah, J.; Ahmed, S.; Elyasi, A.; Kasselman, L.J.; De Leon, J.; Glass, A.D.; Reiss, A.B. Apolipoprotein b and cardiovascular disease: Biomarker and potential therapeutic target. Metabolites 2021, 11, 690. [Google Scholar] [CrossRef]
- Manjunath, C.N.; Rawal, R.; Irani, P.M.; Madhu, K. Atherogenic dyslipidemia. Indian J. Endocrinol. Metab. 2013, 17, 969. [Google Scholar]
- Van der Made, S.M.; Kelly, E.R.; Berendschot, T.T.J.M.; Kijlstra, A.; Lu¨tjohann, D.; Plat, J. Consuming a buttermilk drink containing lutein-enriched egg yolk daily for 1 year increased plasma lutein but did not affect serum lipid or lipoprotein concentrations in adults with early signs of age-related macular degeneration. J. Nutr. 2014, 144, 1370–1377. [Google Scholar] [CrossRef]
- Ballesteros, M.N.; Valenzuela, F.; Robles, A.E.; Artalejo, E.; Aguilar, D.; Andersen, C.J.; Valdez, H.; Fernandez, M.L. One egg per day improves inflammation when compared to an oatmeal-based breakfast without increasing other cardiometabolic risk factors in diabetic patients. Nutrients 2015, 7, 3449–3463. [Google Scholar] [CrossRef] [PubMed]
- Blesso, C.N.; Andersen, C.J.; Barona, J.; Volek, J.S.; Fernandez, M.L. Whole egg consumption improves lipoprotein profiles and insulin sensitivity to a greater extent than yolk-free egg substitute in individuals with metabolic syndrome. Metabolism 2013, 62, 400–410. [Google Scholar] [CrossRef] [PubMed]
- DiMarco, D.M.; Norris, G.H.; Millar, C.L.; Blesso, C.N.; Fernandez, M.L. Intake of up to 3 Eggs per Day Is Associated with Changes in HDL Function and Increased Plasma Antioxidants in Healthy, Young Adults. J. Nutr. 2017, 147, 323–329. [Google Scholar] [CrossRef] [PubMed]
- Mota, D.R.; Perez, L.; Carrari, F.; Mendoza, J.; Díaz, F.; Pinzon, L.; Godoy, G.; Rivera, F. Achiote (Bixa orellana L.): A natural source of pigment and vitamin E. J. Food Sci. Technol. 2017, 54, 1729–1741. [Google Scholar] [CrossRef] [PubMed]
- Böhm, V.; Lietz, G.; Olmedilla, B.; Phelan, D.; Reboul, E.; Bánati, D.; Borel, P.; Corte, J. From carotenoid intake to carotenoid blood and tissue concentrations–implications for dietary intake recommendations. Nutr. Rev. 2021, 79, 544–573. [Google Scholar] [CrossRef]
- Blesso, C.N.; Andersen, C.J.; Barona, J.; Volk, B.; Volek, J.S.; Fernandez, M.L. Effects of carbohydrate restriction and dietary cholesterol provided by eggs on clinical risk factors in metabolic syndrome. J. Clin. Lipidol. 2013, 7, 463–471. [Google Scholar] [CrossRef]
- Dietary Guidelines Advisory Committee. Scientific Report of the 2015 Dietary Guidelines Advisory Committee. Wash. USDA US Dep. Health Hum. Serv. 2015, 53, 1689–1699. [Google Scholar]
- Instituto Colombiano de Bienestar Familiar-ICBF-Organización para las Naciones Unidas para la Aliemntación y la Agricultura-FAO. Guías Alimentarias Basadas en Alimentos Para la Población Colombiana Mayor de 2 Años, 2nd ed.; Taller Creativo de Aleida Sánchez B. Ltda.: Bogotá, Colombia, 2018; p. 320. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Egg Whites (Control) | Egg | Egg + Annatto | p-Value | |||
|---|---|---|---|---|---|---|
| n (%) | n (%) | n (%) | ||||
| Sex | Women | 24 (22.8) | 23 (21.9) | 22 (20.9) | 0.88 | |
| Men | 11 (10.5) | 12 (11.4) | 13 (12.4) | |||
| Age | Young adult (≥18 to ≤26 years) | 12 (11.4) | 12 (11.4) | 11 (10.5) | 0.958 | |
| Adult (≥27 years) | 23 (21.9) | 23 (21.9) | 24 (22.9) | |||
| Socioeconomic level | 1 | 2 (1.9) | 0 (0.0) | 0 (0.0) | 0.251 * | |
| 2 | 9 (8.6) | 4 (3.8) | 5 (4.8) | |||
| 3 | 15 (14.2) | 21 (20.0) | 24 (22.9) | |||
| 4 | 8 (7.6) | 8 (7.6) | 6 (5.7) | |||
| 5 | 1 (0.9) | 2 (1.9) | 0 (0.0) | |||
| Education level | High school | 9 (8.6) | 5 (4.8) | 10 (9.5) | 0.509 | |
| Technical or technological | 8 (7.6) | 4 (3.8) | 4 (3.8) | |||
| Professional | 12 (12.5) | 17 (17.7) | 14 (14.5) | |||
| Postgraduate | 6 (5.7) | 9 (8.6) | 7 (6.7) | |||
| Body mass index (BMI) | Baseline | Normal (≥18.5 to ≤24.9 kg/m2) | 24 (22.9) | 19 (18.1) | 21 (20.0) | 0.467 |
| Overweight (≥25 kg/m2) | 11 (10.4) | 16 (15.2) | 14 (13.3) | |||
| Week 8th | Normal (≥18.5 to ≤24.9 kg/m2) | 25 (23.8) | 20 (19.0) | 21 (20.0) | 0.424 | |
| Overweight (≥25 kg/m2) | 10 (9.5) | 15 (14.3) | 14 (13.3) | |||
| Egg Whites (Control) | Egg | Egg + Annatto | Value | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Median (±SD) | Median (±SD) | Median (±SD) | p1 | p2 | p3 | ||||
| Baseline | Week 8 | Baseline | Week 8 | Baseline | Week 8 | ||||
| Total Cholesterol (mg/dL) | 182 (32.2) | 183 (36.9) | 180 (37.2) | 185 (37.4) | 172 (32.4) | 178 (36.2) | 0.449 | 0.352 | 0.866 |
| HDL Cholesterol (mg/dL) | 52.1 (15) | 51.1 (14.9) | 53.7 (13.5) | 52.8 (12) | 50 (10) | 50.2 (9.1) | 0.697 | 0.441 | 0.855 |
| LDL Cholesterol (mg/dL) | 118 (30.8) | 118 (28.9) | 114 (32.4) | 120 (33.3) | 111 (33.1) | 116 (36.6) | 0.599 | 0.418 | 0.807 |
| Triglycerides (mg/dL) | 106 (53.6) | 112 (69.5) | 106 (40.8) | 107 (39.4) | 110 (60.8) | 105 (57.7) | 0.981 | 0.797 | 0.892 |
| Glucose (mg/dL) | 84.2 (7.8) | 85.2 (10.6) | 83.6 (6.9) | 85.4 (5.4) | 83.8 (5.8) | 83.6 (5.9) | 0.398 | 0.674 | 0.721 |
| Egg Whites (Control) | Egg | Egg + Annatto | Value | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Median (±SD) | Median (±SD) | Median (±SD) | p1 | p2 | p3 | ||||
| Baseline | Week 8 | Baseline | Week 8 | Baseline | Week 8 | ||||
| TC/HDLc | 3.67 (1.1) | 3.82 (1.2) | 3.49 (0.9) | 3.61 (0.8) | 3.57 (0.9) | 3.64 (0.9) | 0.363 | 0.719 | 0.981 |
| LDL-C/HDL-C | 2.45 (1.0) | 2.5 (0.9) | 2.24 (0.8) | 2.36 (0.7) | 2.35 (0.9) | 2.4 (0.9) | 0.428 | 0.623 | 0.959 |
| Non-HDLC | 129 (34.2) | 132 (37.9) | 126 (33.8) | 132 (33.3) | 122 (32.1) | 128 (35.3) | 0.333 | 0.585 | 0.922 |
| TG/HDL-C | 2.27 (1.6) | 2.56 (2.2) | 2.12 (1.0) | 2.14 (0.9) | 2.35 (1.4) | 2.19 (1.4) | 0.807 | 0.527 | 0.663 |
| Apo B (mg/dL) | 73.5 (19.5) | 74.3 (22.5) | 73.4 (23.3) | 72.9 (24.5) | 72.9 (24.5) | 69.5 (22.9) | 0.487 | 0.544 | 0.903 |
| ApoA1 (mg/dL) | 137 (21.9) | 131 (23.3) | 137 (26.1) | 138 (24.1) | 131 (17.7) | 132 (18.2) | 0.565 | 0.341 | 0.458 |
| LDLc/ApoB | 1.63 (0.22) | 1.63 (0.23) | 1.58 (0.20) | 1.60 (0.19) | 1.64 (0.22) | 1.62 (0.16) | 0.895 | 0.493 | 0.804 |
| ApoB/ApoA1 | 0.54 (0.15) | 0.59 (0.21) | 0.55 (0.19) | 0.56 (0.16) | 0.54 (0.18) | 0.56 (0.20) | 0.345 | 0.840 | 0.949 |
| Egg Whites | Egg | Egg + Annatto | Value | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Median (±SD) | Median (±SD) | Median (±SD) | p1 | p2 | p3 | ||||
| Baseline | Week 8 | Baseline | Week 8 | Baseline | Week 8 | ||||
| Total Triglyceride-Rich Lipoprotein Particle (TRLP, nmol/L) | 130 (44.2) | 125 (43.9) | 147 (47) | 148 (38.1) | 134 (45.9) | 136 (49.9) | 0.991 | 0.866 | 0.133 |
| Very Large TRLP (nmol/L) | 0.34 (0.5) | 0.42 (0.5) | 0.39 (0.5) | 0.28 (0.3) | 0.38 (0.4) | 0.33 (0.3) | 0.969 | 0.378 | 0.636 |
| Large TRLP (nmol/L) | 2.63 (1.5) | 2.95 (2.0) | 3.03 (1.6) | 3.15 (2.2) | 2.90 (1.9) | 2.66 (2.0) | 0.743 | 0.517 | 0.611 |
| Medium TRLP (nmol/L) | 13.5 (9.0) | 15.4 (9.2) | 12.2 (4.7) | 13.2 (6.8) | 12.1 (6.3) | 11.6 (5.3) | 0.374 | 0.511 | 0.670 |
| Small TRLP (nmol/L) | 54.8 (27.8) | 53.7 (33.9) | 56 (32.7) | 63.9 (35.4) | 54.9 (33.7) | 65 (34) | 0.295 | 0.571 | 0.483 |
| Very Small TRLP (nmol/L) | 59.2 (37.3) | 66.9 (54.2) | 71.0 (34.1) | 57.3 (28.1) | 56.1 (27.4) | 49.2 (29.2) | 0.264 | 0.176 | 0.363 |
| Total LDL Particle (LDL-P, nmol/L) | 1154 (290) | 1217 (382) | 1121 (317) | 1157 (284) | 1098 (371) | 1104 (302) | 0.447 | 0.318 | 0.876 |
| Large LDL-P (nmol/L) | 401 (190) | 365 (182) | 335 (129) | 373 (112) | 358 (175) | 365 (182) | 0.882 | 0.547 | 0.404 |
| Medium LDL-P (nmol/L) | 332 (1629 | 340 (181) | 350 (267) | 260 (162) | 298 (167) | 313 (180) | 0.466 | 0.366 | 0.353 |
| Small LDL-P (nmol/L) | 361 (166) | 477 (273) | 377 (98) | 468 (210) | 386 (180) | 449 (227) | 0.959 | 0.235 | 0.898 |
| Total Calibrated HDL Particle (cHDL-P, μmol/L) | 20.3 (2.8) | 19.3 (1.6) | 20.5 (3.2) | 20.3 (2.9) | 19.9 (2.1) | 19.8 (1.9) | 0.326 | 0.365 | 0.422 |
| Large cHDL-P (μmol/L) | 2.52 (1.6) | 1.81 (1.1) | 1.83 (1.2) | 2.12 (1.1) | 2.13 (1.4) | 2.16 (1.3) | 0.975 | 0.873 | 0.155 |
| Medium cHDL-P (μmol/L) | 5.93 (2.6) | 5.87 (1.9) | 6.01 (1.7) | 6.29 (2.0) | 5.71 (1.7) | 5.82 (1.7) | 0.619 | 0.479 | 0.959 |
| Small cHDL-P (μmol/L) | 11.9 (3.3) | 11.5 (2.9) | 12 (3.3) | 11.6 (3.0) | 11.7 (2.1) | 11.7 (2.3) | 0.957 | 0.515 | 0.910 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Galvis, Y.; Pineda, K.; Zapata, J.; Aristizabal, J.; Estrada, A.; Fernandez, M.L.; Barona-Acevedo, J. Consumption of Eggs Alone or Enriched with Annatto (Bixa orellana L.) Does Not Increase Cardiovascular Risk in Healthy Adults—A Randomized Clinical Trial, the Eggant Study. Nutrients 2023, 15, 369. https://doi.org/10.3390/nu15020369
Galvis Y, Pineda K, Zapata J, Aristizabal J, Estrada A, Fernandez ML, Barona-Acevedo J. Consumption of Eggs Alone or Enriched with Annatto (Bixa orellana L.) Does Not Increase Cardiovascular Risk in Healthy Adults—A Randomized Clinical Trial, the Eggant Study. Nutrients. 2023; 15(2):369. https://doi.org/10.3390/nu15020369
Chicago/Turabian StyleGalvis, Yeisson, Keilly Pineda, Juliana Zapata, Juan Aristizabal, Alejandro Estrada, María Luz Fernandez, and Jacqueline Barona-Acevedo. 2023. "Consumption of Eggs Alone or Enriched with Annatto (Bixa orellana L.) Does Not Increase Cardiovascular Risk in Healthy Adults—A Randomized Clinical Trial, the Eggant Study" Nutrients 15, no. 2: 369. https://doi.org/10.3390/nu15020369
APA StyleGalvis, Y., Pineda, K., Zapata, J., Aristizabal, J., Estrada, A., Fernandez, M. L., & Barona-Acevedo, J. (2023). Consumption of Eggs Alone or Enriched with Annatto (Bixa orellana L.) Does Not Increase Cardiovascular Risk in Healthy Adults—A Randomized Clinical Trial, the Eggant Study. Nutrients, 15(2), 369. https://doi.org/10.3390/nu15020369