
Associations between Sleep-Disordered Breathing and Serum Uric Acid and Their Sex Differences: The Nagahama Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Assessment of SDB
2.3. Definition of Confounders and Noncommunicable Diseases
2.4. Statistics
3. Results
3.1. Study Participants
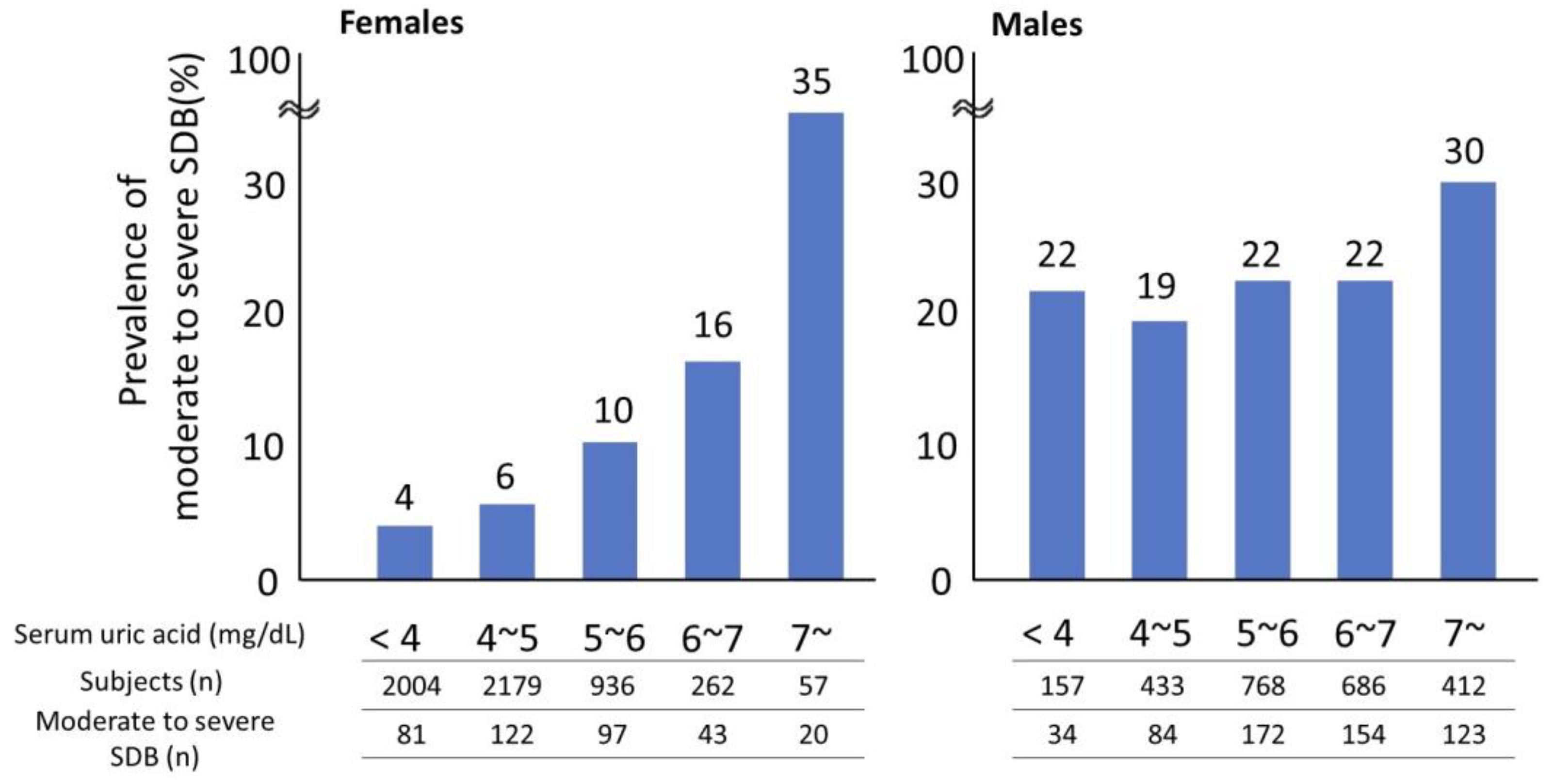
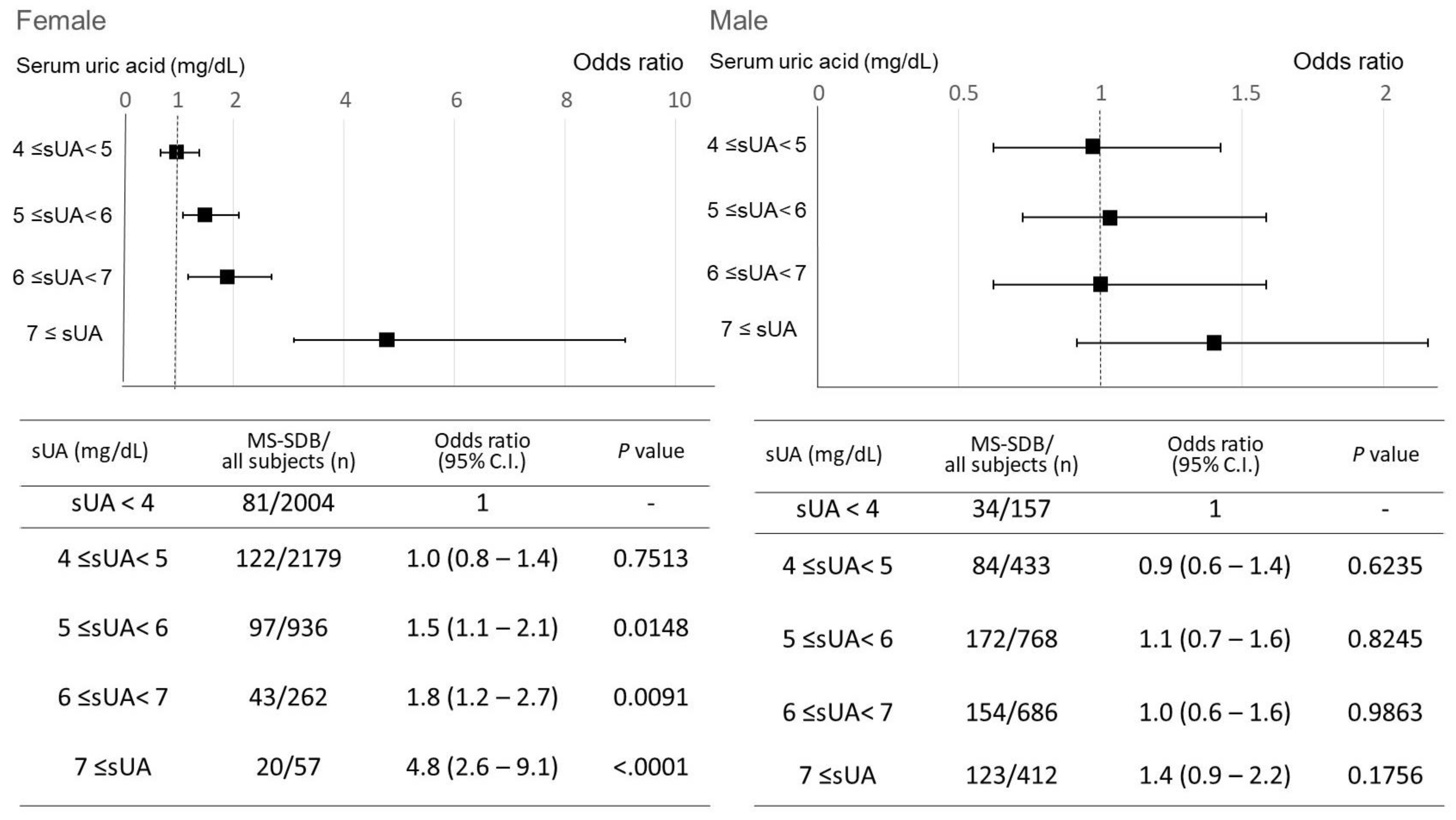
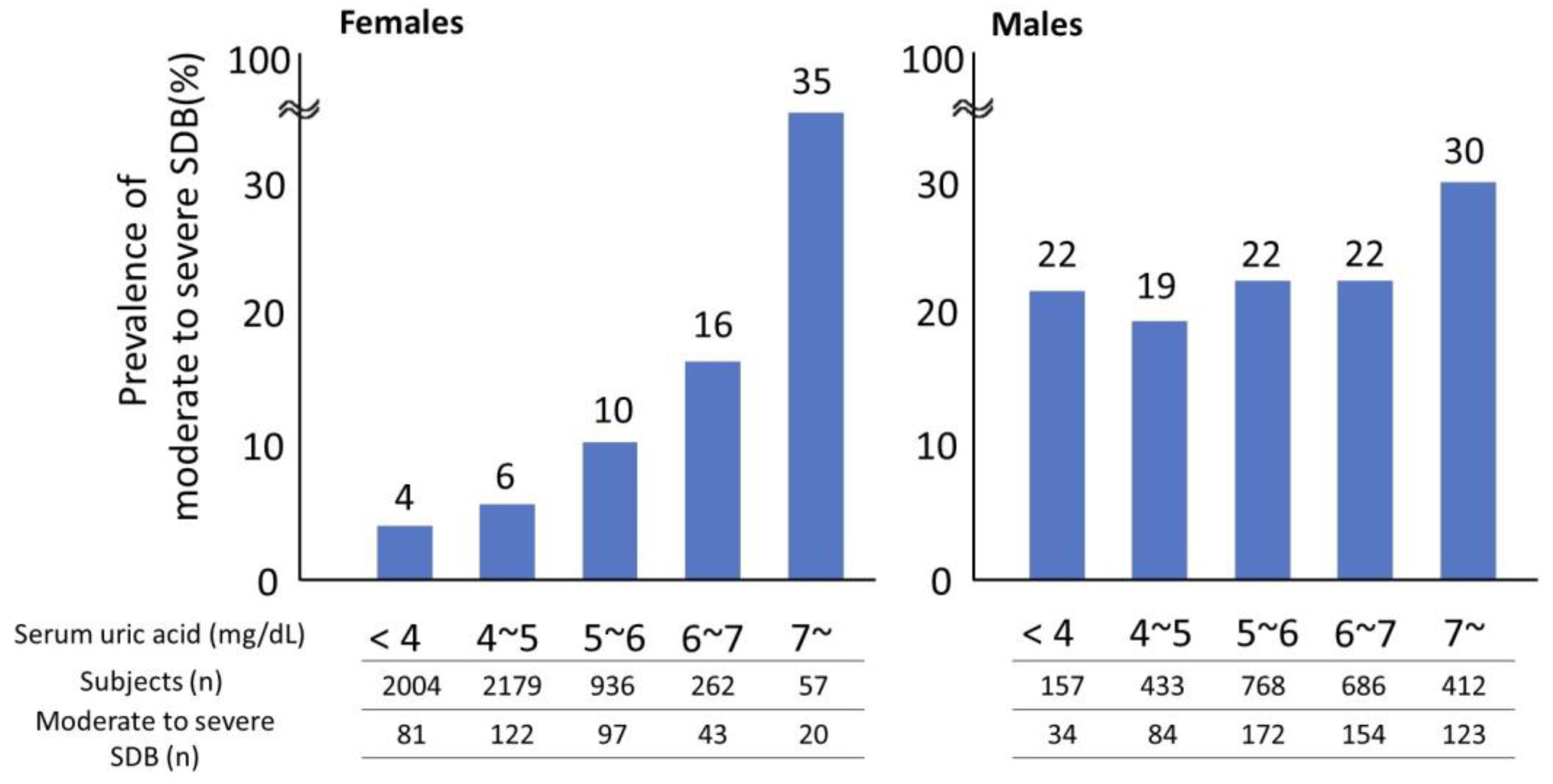
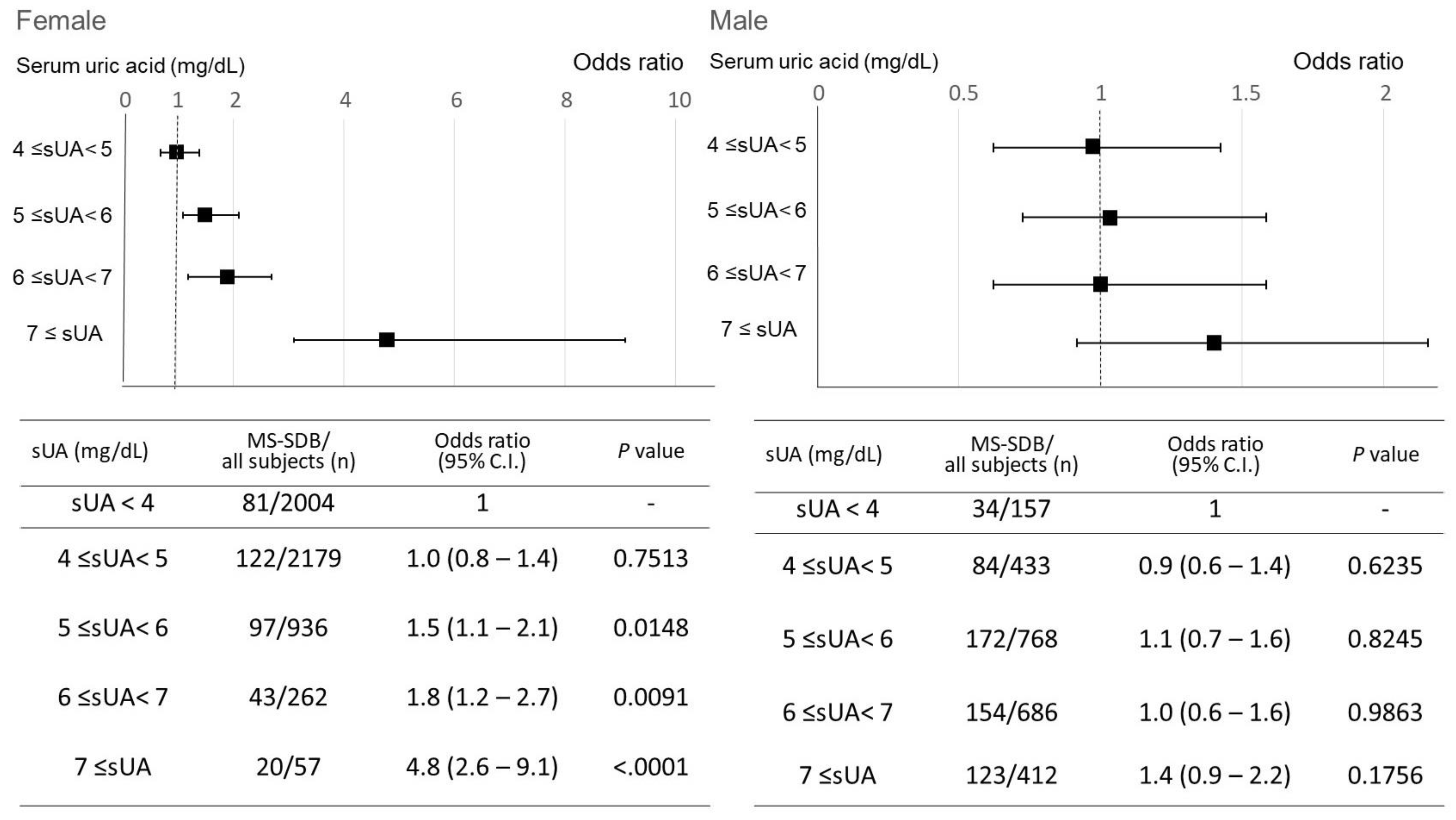
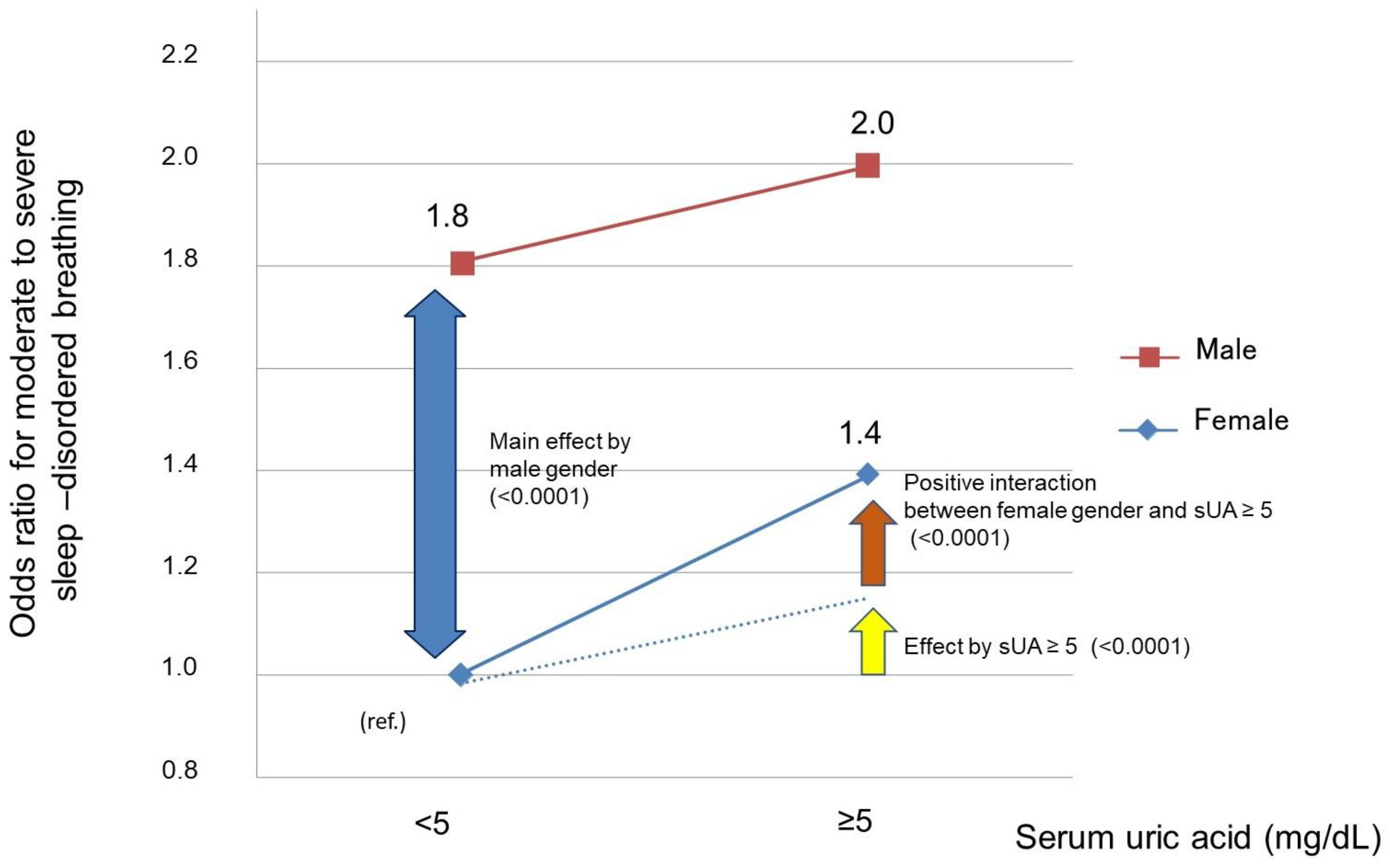
3.2. Impact of Serum Uric Acid Elevation on Moderate to Severe Sleep-Disordered Breathing
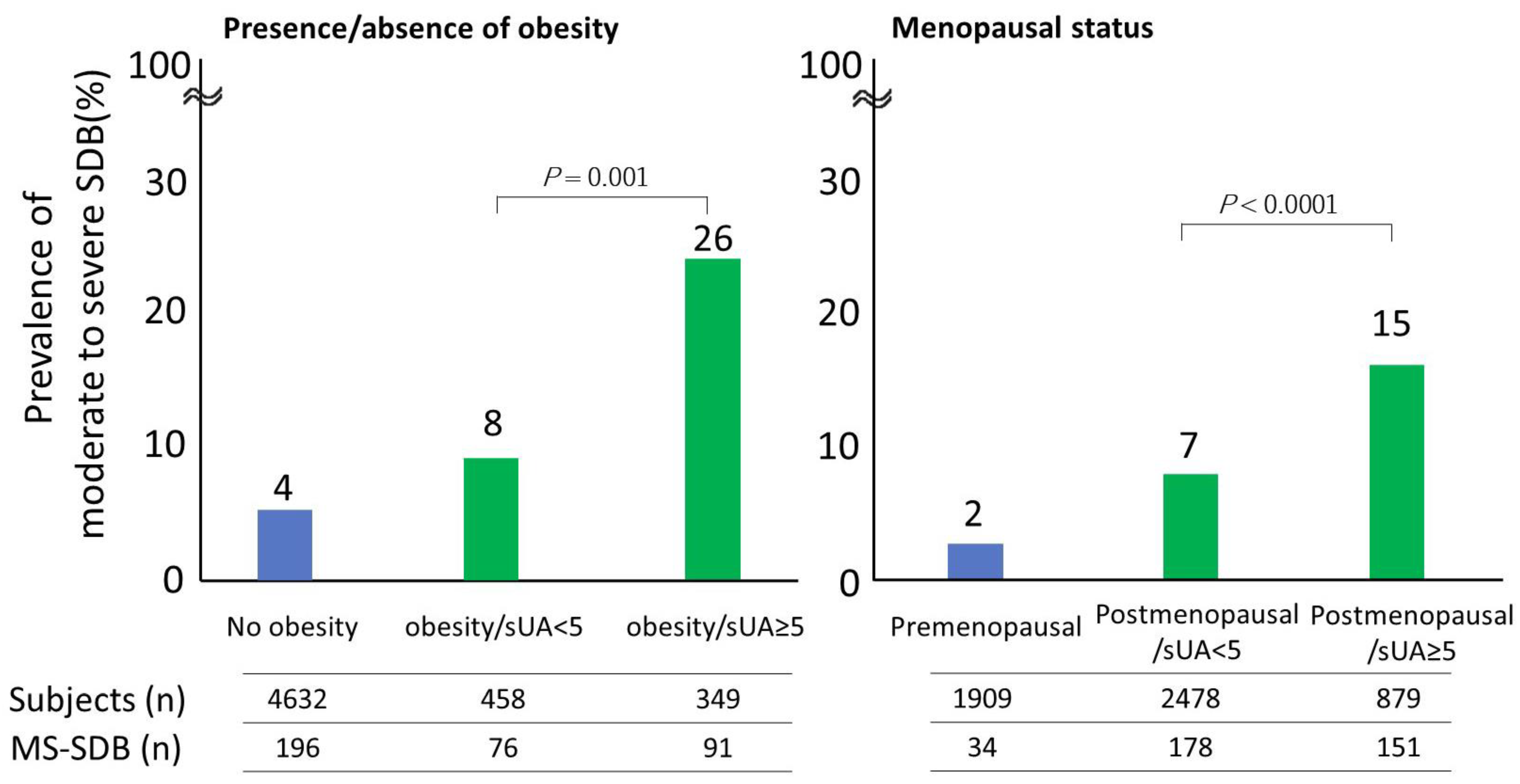
3.3. Association between Serum Uric Acid Elevation within the Normal Range and Moderate to Severe Sleep-Disordered Breathing in Females
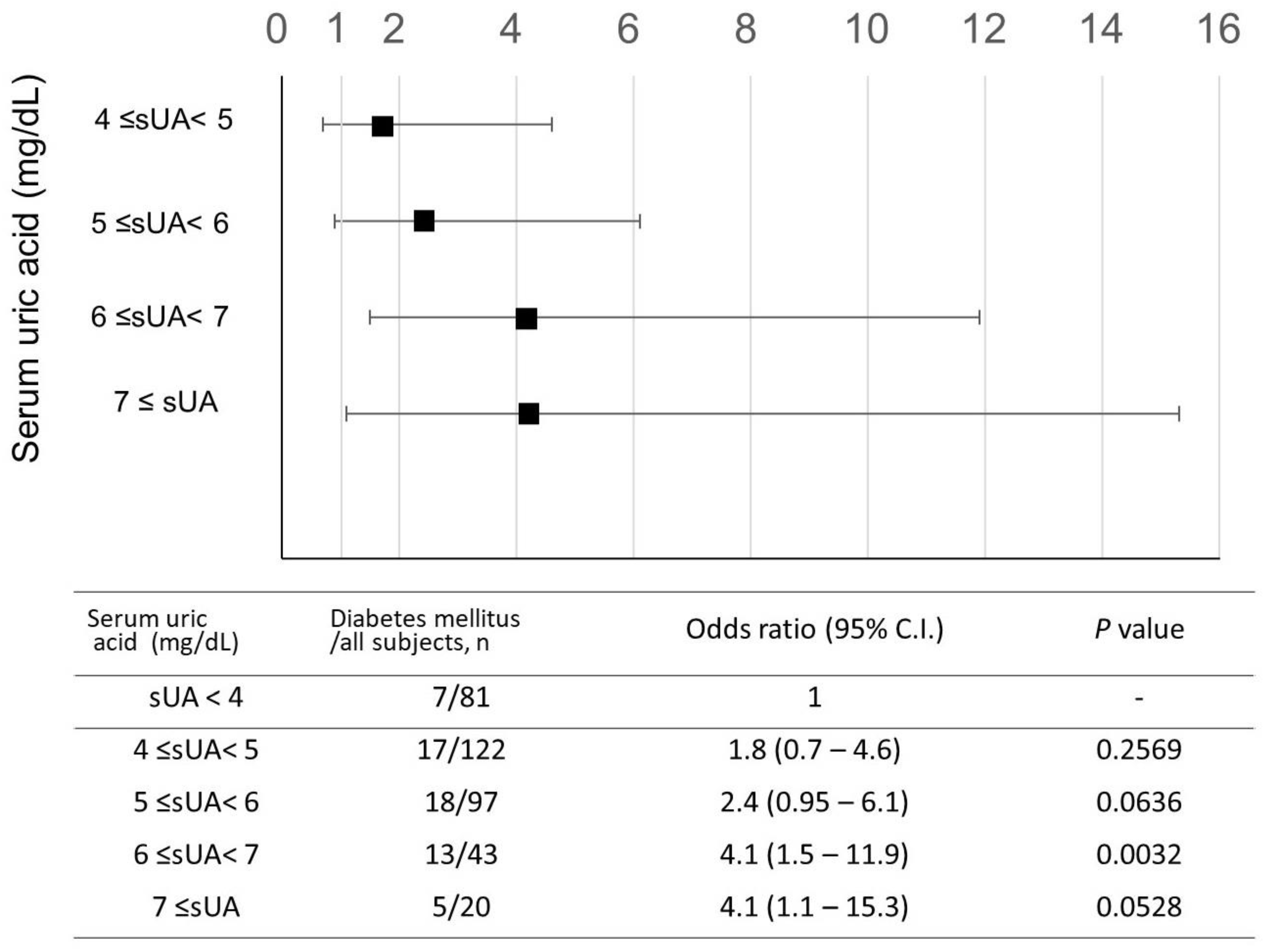
3.4. Clinical Features of Females with Moderate-to-Severe Sleep-Disordered Breathing and Serum Uric Acid ≥ 5 mg/dL
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Ejaz, S.M.; Khawaja, I.S.; Bhatia, S.; Hurwitz, T.D. Obstructive sleep apnea and depression: A review. Innov. Clin. Neurosci. 2011, 8, 17–25. [Google Scholar] [PubMed]
- Blagojevic-Bucknall, M.; Mallen, C.; Muller, S.; Hayward, R.; West, S.; Choi, H.; Roddy, E. The risk of gout among patients with sleep apnea: A matched cohort study. Arthritis Rheumatol. 2019, 71, 154–160. [Google Scholar] [CrossRef] [PubMed]
- Shi, T.; Min, M.; Sun, C.; Cheng, C.; Zhang, Y.; Liang, M.; Rizeq, F.K.; Sun, Y. A meta-analysis of the association between gout, serum uric acid level, and obstructive sleep apnea. Sleep Breath. 2019, 23, 1047–1057. [Google Scholar] [CrossRef] [PubMed]
- Jennum, P.; Riha, R.L. Epidemiology of sleep apnoea/hypopnoea syndrome and sleep-disordered breathing. Eur. Respir. J. 2009, 33, 907–914. [Google Scholar] [CrossRef] [PubMed]
- Heinzer, R.; Marti-Soler, H.; Haba-Rubio, J. Prevalence of sleep apnoea syndrome in the middle to old age general population. Lancet Respir. Med. 2016, 4, e5–e6. [Google Scholar] [CrossRef] [PubMed]
- Larsson, S.C.; Burgess, S.; Michaëlsson, K. Genetic association between adiposity and gout: A Mendelian randomization study. Rheumatology 2018, 57, 2145–2148. [Google Scholar] [CrossRef] [PubMed]
- Singh, J.A.; Cleveland, J.D. Gout and the Risk of Incident Obstructive Sleep Apnea in Adults 65 Years or Older: An Observational Study. J. Clin. Sleep Med. 2018, 14, 1521–1527. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.K.; Ford, E.S.; Li, C.; Curhan, G. Prevalence of the metabolic syndrome in patients with gout: The Third National Health and Nutrition Examination Survey. Arthritis Rheumatol. 2007, 57, 109–115. [Google Scholar] [CrossRef]
- Evans, P.L.; Prior, J.A.; Belcher, J.; Mallen, C.D.; Hay, C.A.; Roddy, E. Obesity, hypertension and diuretic use as risk factors for incident gout: A systematic review and meta-analysis of cohort studies. Arthritis Res. Ther. 2018, 20, 136. [Google Scholar] [CrossRef]
- Hirotsu, C.; Tufik, S.; Guindalini, C.; Mazzotti, D.R.; Bittencourt, L.R.; Andersen, M.L. Association between uric acid levels and obstructive sleep apnea syndrome in a large epidemiological sample. PLoS ONE 2013, 8, e66891. [Google Scholar] [CrossRef]
- Fleming, W.E.; Holty, J.-E.C.; Bogan, R.K.; Hwang, D.; Ferouz-Colborn, A.S.; Budhiraja, R.; Redline, S.; Mensah-Osman, E.; Osman, N.I.; Li, Q.; et al. Use of blood biomarkers to screen for obstructive sleep apnea. Nat. Sci. Sleep 2018, 10, 159–167. [Google Scholar] [CrossRef] [PubMed]
- Chen, Q.; Lin, G.; Chen, L.; Huang, J.; Huang, Y.; Li, P.; Chen, M.; Lin, Q. Does Continuous Positive Airway Pressure Therapy in Patients with Obstructive Sleep Apnea Improves Uric Acid? A Meta-Analysis. Oxid. Med. Cell. Longev. 2019, 2019, 4584936. [Google Scholar] [CrossRef] [PubMed]
- Sui, X.; Church, T.S.; Meriwether, R.A.; Lobelo, F.; Blair, S.N. Uric acid and the development of metabolic syndrome in women and men. Metabolism 2008, 57, 845–852. [Google Scholar] [CrossRef] [PubMed]
- Netzer, N.C.; Eliasson, A.H.; Strohl, K.P. Women with sleep apnea have lower levels of sex hormones. Sleep Breath. 2003, 7, 25–29. [Google Scholar] [CrossRef] [PubMed]
- Behan, M.; Wenninger, J.M. Sex steroidal hormones and respiratory control. Respir. Physiol. Neurobiol. 2008, 164, 213–221. [Google Scholar] [CrossRef] [PubMed]
- Neugarten, J. Gender and the progression of renal disease. J. Am. Soc. Nephrol. 2002, 13, 2807–2809. [Google Scholar] [CrossRef] [PubMed]
- Abd El-Lateef, S.M.; El-Sayed, E.-S.M.; Mansour, A.M.; Salama, S.A. The protective role of estrogen and its receptors in gentamicin-induced acute kidney injury in rats. Life Sci. 2019, 239, 117082. [Google Scholar] [CrossRef]
- Lima-Posada, I.; Bobadilla, N.A. Understanding the opposite effects of sex hormones in mediating renal injury. Nephrology 2021, 26, 217–226. [Google Scholar] [CrossRef]
- Elliot, S.J.; Berho, M.; Korach, K.; Doublier, S.; Lupia, E.; Striker, G.E.; Karl, M. Gender-specific effects of endogenous testosterone: Female alpha-estrogen receptor-deficient C57Bl/6J mice develop glomerulosclerosis. Kidney Int. 2007, 72, 464–472. [Google Scholar] [CrossRef]
- Doublier, S.; Lupia, E.; Catanuto, P.; Periera-Simon, S.; Xia, X.; Korach, K.; Berho, M.; Elliot, S.J.; Karl, M. Testosterone and 17β-estradiol have opposite effects on podocyte apoptosis that precedes glomerulosclerosis in female estrogen receptor knockout mice. Kidney Int. 2011, 79, 404–413. [Google Scholar] [CrossRef]
- Murase, K.; Matsumoto, T.; Tabara, Y.; Ohler, A.; Gozal, D.; Minami, T.; Kanai, O.; Takeyama, H.; Takahashi, N.; Hamada, S.; et al. Association of Sleep-disordered Breathing and Blood Pressure with Albuminuria; The Nagahama Study. Ann. Am. Thorac. Soc. 2022, 19, 451–461. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, T.; Murase, K.; Tabara, Y.; Minami, T.; Kanai, O.; Takeyama, H.; Chin, K. Sleep disordered breathing and metabolic comorbidities across sex and menopausal status in East Asians: The Nagahama Study. Eur. Respir. J. 2020, 56, 1902251. [Google Scholar] [CrossRef] [PubMed]
- Glantzounis, G.; Tsimoyiannis, E.; Kappas, A.; Galaris, D. Uric Acid and Oxidative Stress. Curr. Pharm. Des. 2005, 11, 4145–4151. [Google Scholar] [CrossRef] [PubMed]
- Kapetanovic, M.C.; Nilsson, P.; Turesson, C.; Englund, M.; Dalbeth, N.; Jacobsson, L. The risk of clinically diagnosed gout by serum urate levels: Results from 30 years follow-up of the Malmö Preventive Project cohort in southern Sweden. Arthritis Res. Ther. 2018, 20, 190. [Google Scholar] [CrossRef] [PubMed]
- Dalbeth, N.; Phipps-Green, A.; Frampton, C.; Neogi, T.; Taylor, W.J.; Merriman, T.R. Relationship between serum urate concentration and clinically evident incident gout: An individual participant data analysis. Ann. Rheum. Dis. 2018, 77, 1048–1052. [Google Scholar] [CrossRef] [PubMed]
- Forman, J.P.; Choi, H.; Curhan, G.C. Uric acid and insulin sensitivity and risk of incident hypertension. Arch. Intern. Med. 2009, 169, 155–162. [Google Scholar] [CrossRef] [PubMed]
- Shani, M.; Vinker, S.; Dinour, D.; Leiba, M.; Twig, G.; Holtzman, E.J.; Leiba, A. High Normal Uric Acid Levels Are Associated with an Increased Risk of Diabetes in Lean, Normoglycemic Healthy Women. J. Clin. Endocrinol. Metab. 2016, 101, 3772–3778. [Google Scholar] [CrossRef] [PubMed]
- Shepertycky, M.R.; Banno, K.; Kryger, M.H. Differences between men and women in the clinical presentation of patients diagnosed with obstructive sleep apnea syndrome. Sleep 2005, 28, 309–314. [Google Scholar]
- Valipour, A.; Lothaller, H.; Rauscher, H.; Zwick, H.; Burghuber, O.C.; Lavie, P. Gender-related differences in symptoms of patients with suspected breathing disorders in sleep: A clinical population study using the sleep disorders questionnaire. Sleep 2007, 30, 312–319. [Google Scholar] [CrossRef]
- Young, T.; Palta, M.; Dempsey, J.; Skatrud, J.; Weber, S.; Badr, S. The occurrence of sleep-disordered breathing among middle-aged adults. N. Engl. J. Med. 1993, 328, 1230–1235. [Google Scholar] [CrossRef]
- Young, T.; Finn, L. Epidemiological insights into the public health burden of sleep disordered breathing: Sex differences in survival among sleep clinic patients. Thorax 1998, 53 (Suppl. S3), S16–S19. [Google Scholar] [CrossRef] [PubMed]
- Yoo, T.W.; Sung, K.C.; Shin, H.S.; Kim, B.J.; Kim, B.S.; Kang, J.H.; Lee, M.H.; Park, J.R.; Kim, H.; Rhee, E.J.; et al. Relationship between serum uric acid concentration and insulin resistance and metabolic syndrome. Circ. J. 2005, 69, 928–933. [Google Scholar] [CrossRef] [PubMed]
- Cai, W.; Duan, X.-M.; Liu, Y.; Yu, J.; Tang, Y.-L.; Liu, Z.-L.; Jiang, S.; Zhang, C.P.; Liu, J.Y.; Xu, J.X.; et al. Uric Acid Induces Endothelial Dysfunction by Activating the HMGB1/RAGE Signaling Pathway. BioMed Res. Int. 2017, 2017, 4391920. [Google Scholar] [CrossRef] [PubMed]
- Gaubert, M.; Marlinge, M.; Alessandrini, M.; Laine, M.; Bonello, L.; Fromonot, J.; Paganelli, F. Uric acid levels are associated with endothelial dysfunction and severity of coronary atherosclerosis during a first episode of acute coronary syndrome. Purinergic Signal. 2018, 14, 191–199. [Google Scholar] [CrossRef] [PubMed]
- Yu, W.; Cheng, J.-D. Uric Acid and Cardiovascular Disease: An Update From Molecular Mechanism to Clinical Perspective. Front. Pharmacol. 2020, 11, 582680. [Google Scholar] [CrossRef] [PubMed]
- Faulx, M.D.; Larkin, E.K.; Hoit, B.D.; Aylor, J.E.; Wright, A.T.; Redline, S. Sex influences endothelial function in sleep-disordered breathing. Sleep 2004, 27, 1113–1120. [Google Scholar] [CrossRef] [PubMed]
- Yukawa, K.; Inoue, Y.; Yagyu, H.; Hasegawa, T.; Komada, Y.; Namba, K.; Nagai, N.; Nemoto, S.; Sano, E.; Shibusawa, M.; et al. Gender differences in the clinical characteristics among Japanese patients with obstructive sleep apnea syndrome. Chest 2009, 135, 337–343. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Cheng, J.; Yang, W.; Zou, H.; Su, C.; Miao, J. Gender differences in clinical manifestations and polysomnographic findings in Chinese patients with obstructive sleep apnea. Sleep Breath. 2020, 24, 1019–1026. [Google Scholar] [CrossRef]
- Kent, B.D.; Grote, L.; Ryan, S.; Pépin, J.-L.; Bonsignore, M.R.; Tkacova, R.; Saaresranta, T.; Verbraecken, J.; Lévy, P.; Hedner, J.; et al. Diabetes mellitus prevalence and control in sleep-disordered breathing: The European Sleep Apnea Cohort (ESADA) study. Chest 2014, 146, 982–990. [Google Scholar] [CrossRef]
- Matsumoto, T.; Murase, K.; Tachikawa, R.; Minami, T.; Hamada, S.; Tanizawa, K.; Inouchi, M.; Handa, T.; Oga, T.; Yanagita, M.; et al. Microalbuminuria in Patients with Obstructive Sleep Apnea–Chronic Obstructive Pulmonary Disease Overlap Syndrome. Ann. ATS 2016, 13, 917–925. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Males (n = 2456) | Females (n = 5439) | p Value | |
|---|---|---|---|
| Age, years old | 59 ± 13 | 56 ± 12 | <0.0001 |
| BMI, kg/m2 | 23.2 ± 3.1 | 21.8 ± 3.3 | <0.0001 |
| BMI ≥ 25 kg/m2, n (%) | 592 (24.1) | 807 (14.8) | <0.0001 |
| Postmenopausal, n (%) * | ― | 3508 (64.8) | ― |
| Currently smoking, n (%) | 550 (22.4) | 201 (3.7) | <0.0001 |
| Drinking ≥ 4 day/week, n (%) | 1229 (50.0) | 672 (12.4) | <0.0001 |
| Serum uric acid, mg/dL | 5.8 ± 1.2 | 4.3 ± 1.0 | <0.0001 |
| Acti-ODI3%, events/h | 11.5 ± 9.0 | 6.5 ± 5.4 | <0.0001 |
| The severity of SDB *, Normal/mild/moderate/severe, n (%) | 486/1403/453/114 (19.8/57.1/18.4/4.6) | 2803/2273/321/42 (51.5/41.8/5.9/0.8) | <0.0001 |
| Hypertension, n (%) | 1081 (44.9) | 1549 (29.1) | <0.0001 |
| Diabetes mellitus, n (%) | 269 (11.0) | 228 (4.2) | <0.0001 |
| Dyslipidemia, n (%) | 1020 (50.7) | 2111 (46.9) | 0.0049 |
| Metabolic syndrome, n (%) | 747 (30.6) | 477 (8.8) | <0.0001 |
| Menopausal status, pre/post, n (%) | 1909/3508 (35.2/64.8) | ― | ― |
| Serum Uric Acid < 5 mg/dL (n = 203) | Serum Uric Acid ≥ 5 mg/dL (n = 160) | p Value | |
|---|---|---|---|
| Age, years old | 66 ± 10 | 66 ± 9 | 0.45 |
| Age ≥ 60 years old, n (%) | 160 (79) | 129 (81) | 0.67 |
| BMI, kg/m2 | 24.1 ± 3.9 | 26.1 ± 4.4 | <0.0001 |
| BMI ≥ 25 mg/m2, n (%) | 69 (43) | 91 (57) | 0.0002 |
| Menopausal status, post, n (%) | 178 (88) | 151 (94) | 0.0299 |
| Current smoking, n (%) | 2 (2) | 3 (2) | 0.9477 |
| Drinking habit ≥ 4 day/week, n (%) | 19 (9) | 18 (11) | 0.5545 |
| 3% ODI, events/h | 21.6 ± 7.3 | 21.6 ± 7.8 | 0.9520 |
| CT90, % | 3.4 ± 3.9 | 4.2 ± 7.4 | 0.1308 |
| Creatinine clearance, mL/min | 86.2 ± 31.1 | 82.5 ± 29.0 | 0.2505 |
| Creatinine clearance < 70 mL/min, n (%) | 61 (30) | 54 (34) | 0.4518 |
| Hypertension, n (%) | 123 (61) | 100 (64) | 0.5342 |
| Diabetes mellitus, n (%) | 24 (12) | 36 (23) | 0.0067 |
| Dyslipidemia, n (%) | 118 (68) | 94 (68) | 0.9550 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sunadome, H.; Murase, K.; Tabara, Y.; Matsumoto, T.; Minami, T.; Kanai, O.; Nagasaki, T.; Takahashi, N.; Hamada, S.; Tanizawa, K.; et al. Associations between Sleep-Disordered Breathing and Serum Uric Acid and Their Sex Differences: The Nagahama Study. Nutrients 2023, 15, 4237. https://doi.org/10.3390/nu15194237
Sunadome H, Murase K, Tabara Y, Matsumoto T, Minami T, Kanai O, Nagasaki T, Takahashi N, Hamada S, Tanizawa K, et al. Associations between Sleep-Disordered Breathing and Serum Uric Acid and Their Sex Differences: The Nagahama Study. Nutrients. 2023; 15(19):4237. https://doi.org/10.3390/nu15194237
Chicago/Turabian StyleSunadome, Hironobu, Kimihiko Murase, Yasuharu Tabara, Takeshi Matsumoto, Takuma Minami, Osamu Kanai, Tadao Nagasaki, Naomi Takahashi, Satoshi Hamada, Kiminobu Tanizawa, and et al. 2023. "Associations between Sleep-Disordered Breathing and Serum Uric Acid and Their Sex Differences: The Nagahama Study" Nutrients 15, no. 19: 4237. https://doi.org/10.3390/nu15194237
APA StyleSunadome, H., Murase, K., Tabara, Y., Matsumoto, T., Minami, T., Kanai, O., Nagasaki, T., Takahashi, N., Hamada, S., Tanizawa, K., Togawa, J., Uiji, S., Wakamura, T., Komenami, N., Setoh, K., Kawaguchi, T., Morita, S., Takahashi, Y., Nakayama, T., ... Chin, K. (2023). Associations between Sleep-Disordered Breathing and Serum Uric Acid and Their Sex Differences: The Nagahama Study. Nutrients, 15(19), 4237. https://doi.org/10.3390/nu15194237