
Are Twin Pregnancies at Higher Risk for Iron and Calcium Deficiency than Singleton Pregnancies?

 , , , , ,
, , , , ,  and
and
Abstract
:1. Introduction
2. Material and Methods
2.1. Study Population
2.2. Blood Collection
2.3. Serum Analysis
2.4. Statistical Analysis
3. Results
3.1. Group Characteristics
3.2. Perinatal Outcomes in Singleton and Twin Pregnancies
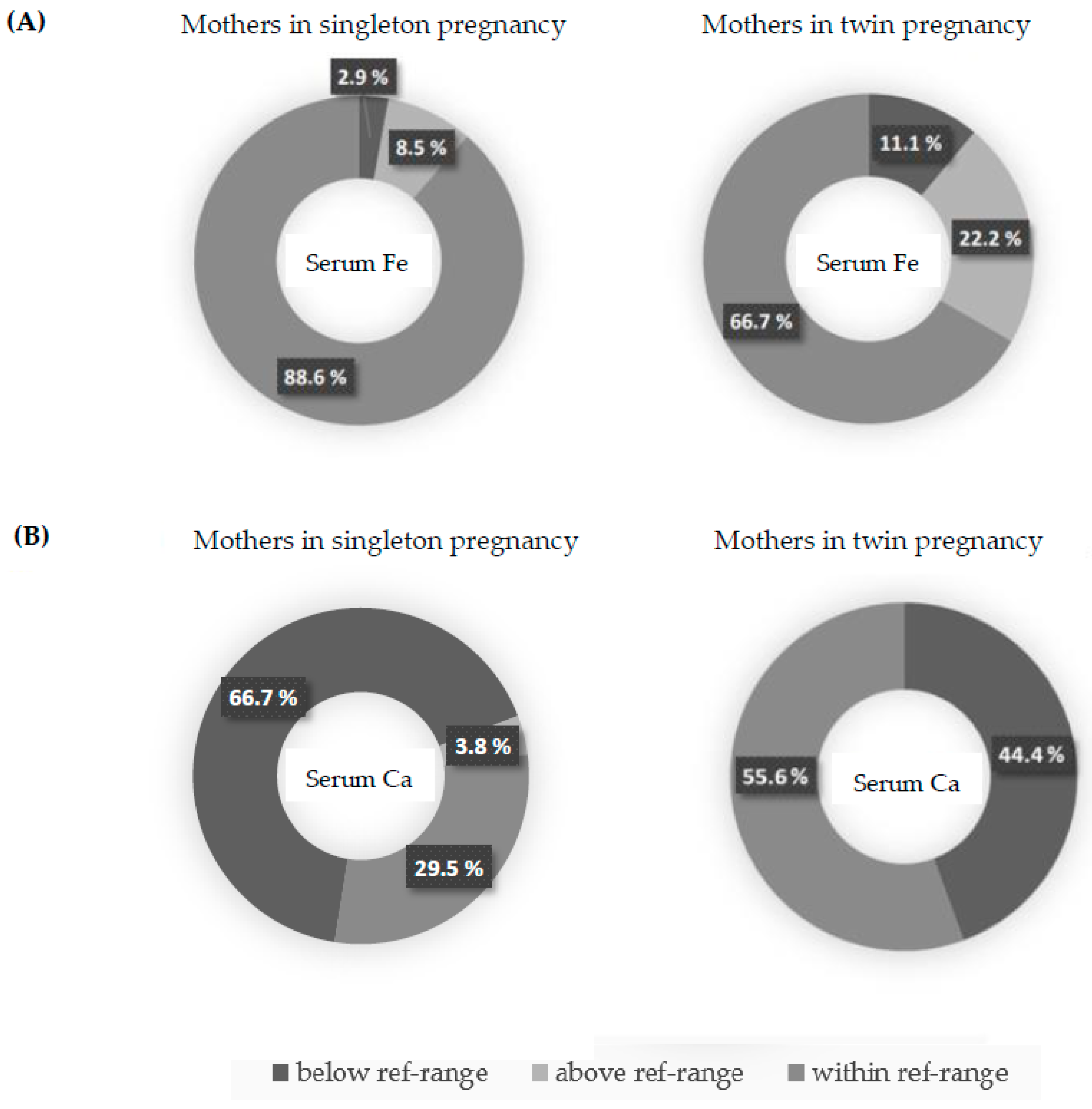
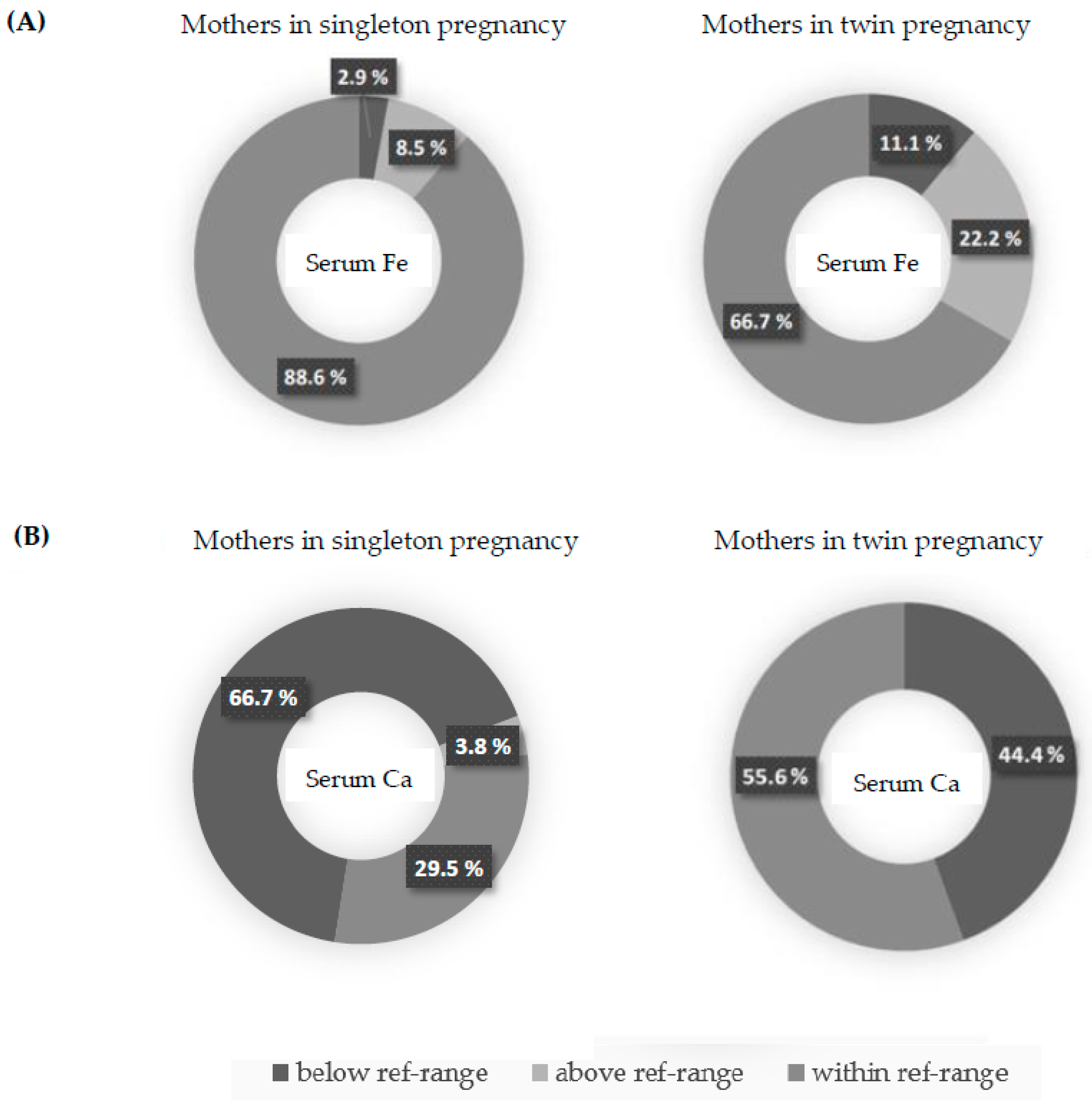
3.3. Iron and Calcium Status in Singleton and Twin Pregnancies
3.4. Iron and Calcium Status in Relation to Prenatal Supplementation
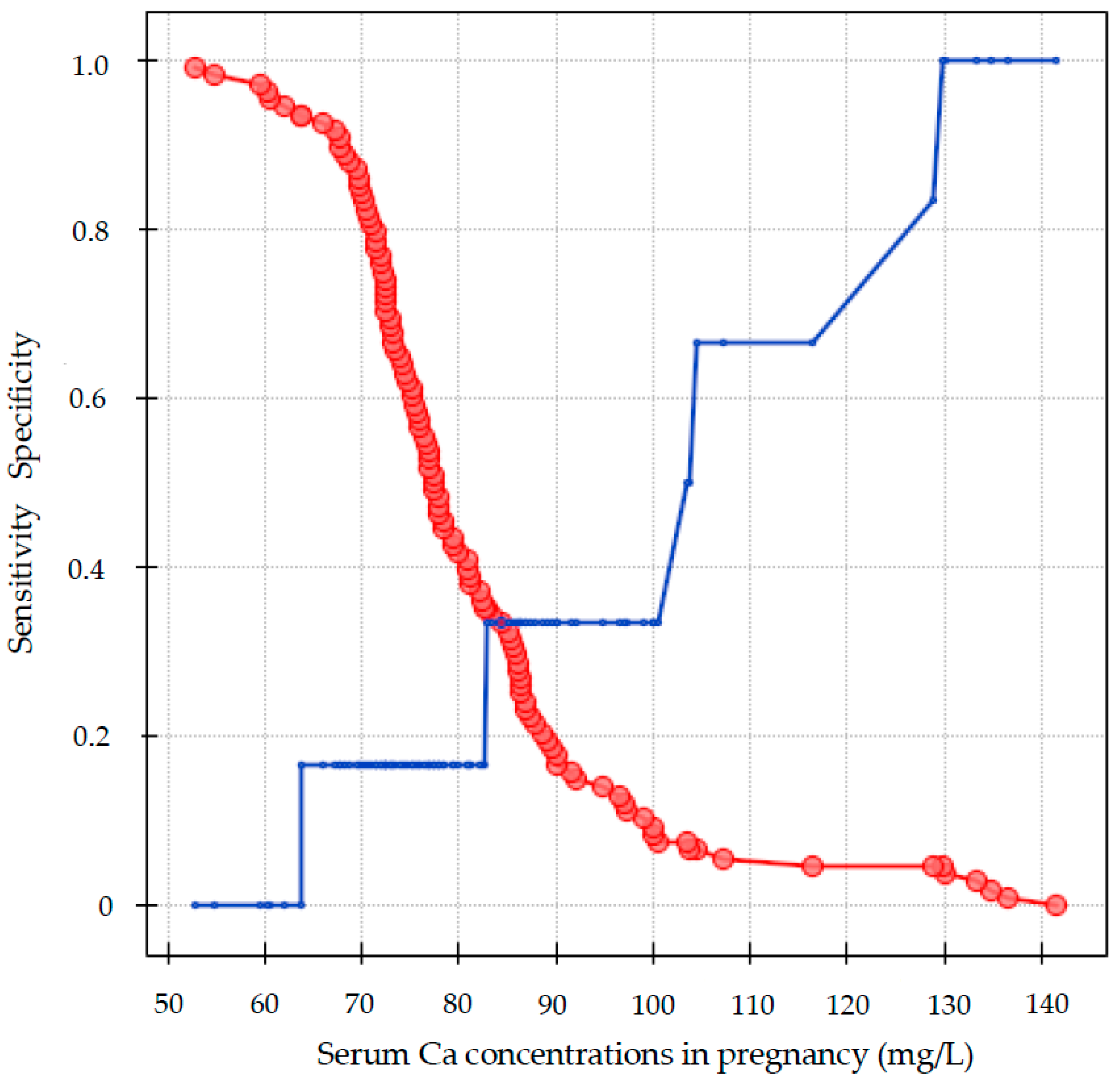
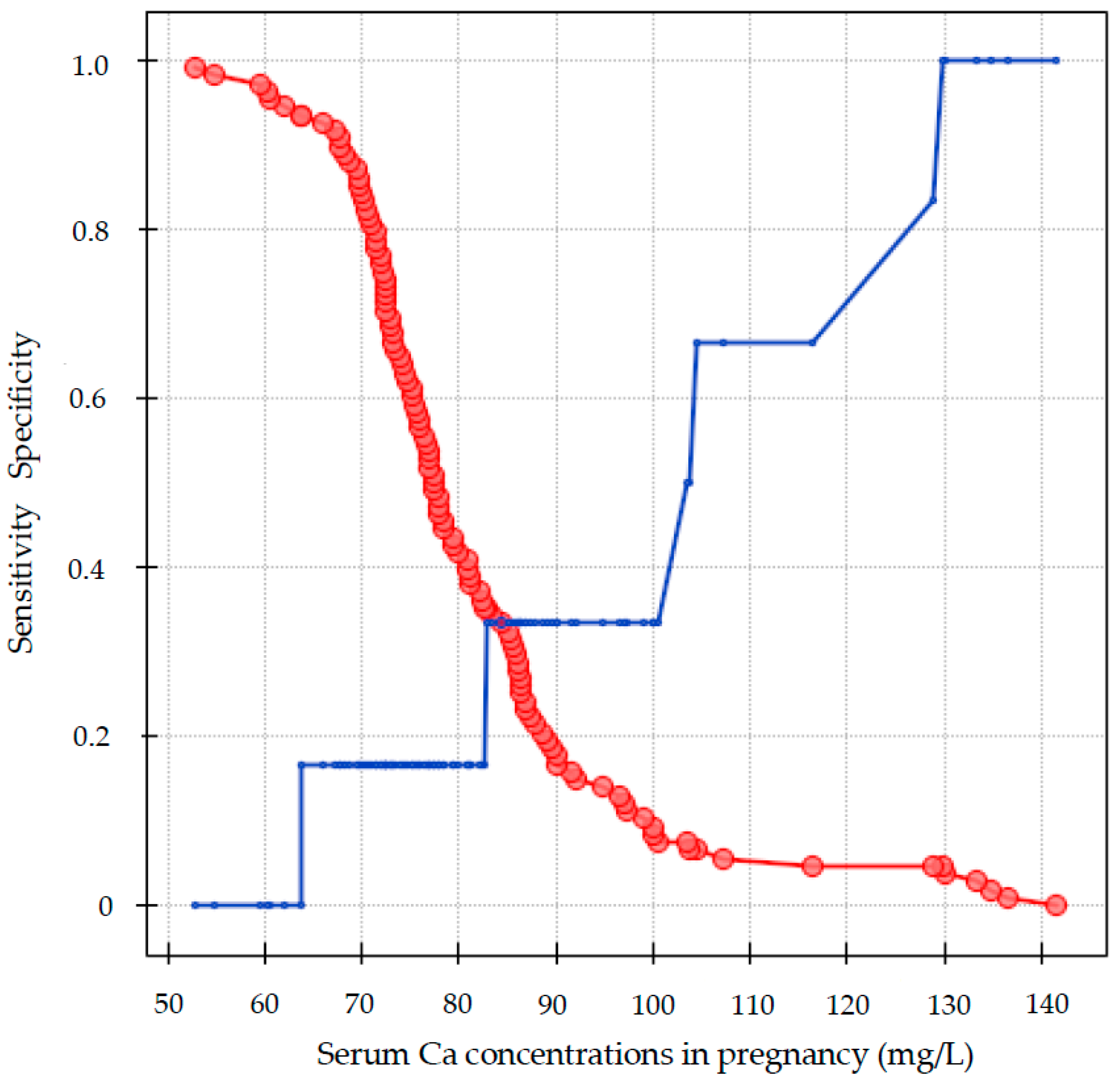
3.5. Maternal Serum Iron and Calcium for the Prediction of Adverse Outcomes
4. Discussion
4.1. The Iron Status in Singleton and Twin Pregnancy
4.2. The Calcium Status in Singleton and Twin Pregnancy
4.3. The Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mei, Z.; Cogswell, M.E.; Looker, A.C.; Pfeiffer, C.M.; Cusick, S.E.; Lacher, D.A.; Grummer-Strawn, L.M. Assessment of iron status in US pregnant women from the National Health and Nutrition Examination Survey (NHANES), 1999. Am. J. Clin. Nutr. 2011, 93, 1312–1320. [Google Scholar] [CrossRef]
- Mikulska, A.A.; Karaźniewicz-Łada, M.; Filipowicz, D.; Ruchała, M.; Główka, F.K. Metabolic Characteristics of Hashimoto’s Thyroiditis Patients and the Role of Microelements and Diet in the Disease Management—An Overview. Int. J. Mol. Sci. 2022, 23, 6580. [Google Scholar] [CrossRef]
- Rasmussen, K. Is there a causal relationship between iron deficiency or iron-deficiency anemia and weight at birth, length of gestation and perinatal mortality? J. Nutr. 2001, 131, 590S–601S. [Google Scholar] [CrossRef] [PubMed]
- Scholl, T.O.; Hediger, M.L.; Fischer, R.L.; Shearer, J.W. Anemia vs iron deficiency—Increased risk of preterm delivery in a prospective study. Am. J. Clin. Nutr. 1992, 55, 985–988. [Google Scholar] [CrossRef] [PubMed]
- Geltman, P.L.; Meyers, A.F.; Mehta, S.D.; Brugnara, C.; Villon, I.; Wu, Y.A.; Bauchner, H. Daily multivitamins with iron to prevent anemia in highrisk infants: A randomized clinical trial. Pediatrics 2004, 114, 86–93. [Google Scholar] [CrossRef] [PubMed]
- Lozoff, B.; Beard, J.; Connor, J. Long-lasting neural and behavioral effects of iron deficiency in infancy. Nutr. Rev. 2006, 64, S34–S43. [Google Scholar] [CrossRef]
- Algarín, C.; Peirano, P.; Garrido, M.; Pizarro, F.; Lozoff, B. Iron deficiency anemia in infancy: Long-lasting effects on auditory and visual system functioning. Pediatr. Res. 2003, 53, 217–223. [Google Scholar] [CrossRef]
- Beard, J.L. Why iron deficiency is important in infant development. J. Nutr. 2008, 138, 2534–2538. [Google Scholar] [CrossRef]
- Walker, S.P.; Wachs, T.D.; Gardner, J.M.; Lozoff, B.; Wasserman, G.A.; Pollitt, E.; Carter, J.A. Child development: Risk factors for adverse outcomes in developing countries. Lancet 2007, 369, 145–157. [Google Scholar] [CrossRef]
- Stanisławska-Kubiak, M.; Majewska, K.A.; Kędzia, A.; Samborski, W.; Ruchala, M.; Mojs, E.H. Changes in cognitive functions in a girl with severe acquired hypothyroidism in comparison to the healthy twin sister. Endokrynol. Pol. 2020, 71, 365–366. [Google Scholar] [CrossRef]
- Blickstein, I.; Goldschmit, R.; Lurie, S. Hemoglobin levels during twin vs. singleton pregnancies. Parity makes the difference. J. Reprod. Med. 1995, 40, 47–50. [Google Scholar]
- Kosto, A.; Okby, R.; Levy, M.; Sergienko, R.; Sheiner, E. The effect of maternal anemia on maternal and neonatal outcomes in twin prengnacies. J. Matern. Fetal Neonatal Med. 2016, 29, 2297–2300. [Google Scholar] [CrossRef]
- Bajoria, R.; Lazda, E.J.; Ward, S.; Sooranna, S.R. Iron metabolism in monochorionic twin pregnancies in relation to twin-twin transfusion syndrome. Hum. Reprod. 2001, 16, 567–573. [Google Scholar] [CrossRef]
- Caglar, M.K.; Kollee, L.A. Determination of serum ferritin in the evaluation of iron depletion and iron overload in chronic twin-to-twin transfusion syndrome. J. Perinat. Med. 1989, 17, 357–359. [Google Scholar]
- Ru, Y.; Pressman, E.K.; Cooper, E.M.; Guillet, R.; Katzman, P.J.; Kent, T.R.; Bacak, S.J.; O’Brien, K.O. Iron deficiency and anemia are prevalent in women with multiple gestations. Am. J. Clin. Nutr. 2016, 104, 1052–1060. [Google Scholar] [CrossRef]
- Goodnight, W.; Newman, R.; Society of Maternal–Fetal Medicine. Optimal nutrition for improved twin pregnancy outcome. Obstet. Gynecol. 2009, 114, 1121–1134. [Google Scholar] [CrossRef]
- World Health Organization (WHO). WHO Recommendations on Antenatal Care for a Positive Pregnancy Experience; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- American College of Obstetricians and Gynecologists. ACOG Practice Bulletin No. 95, Anemia in pregnancy. Obstet. Gynecol. 2008, 112, 201–207. [Google Scholar] [CrossRef]
- Pavord, S.; Daru, J.; Prasannan, N.; Robinson, S.; Stanworth, S.; Girling, J.; BSH Committee. UK guidelines on the management of iron deficiency in pregnancy. Br. J. Haematol. 2020, 188, 819–830. [Google Scholar] [CrossRef]
- Milman, N. Iron prophylaxis in pregnancy--general or individual and in which dose? Ann. Hematol. 2006, 85, 821–828. [Google Scholar] [CrossRef]
- FIGO Working Group on Good Clinical Practice in Maternal-Fetal Medicine. Good Clinical Practice Advice: Iron Deficiency Anemia in Pregnancy. Int. J. Gynaecol. Obstet. 2019, 144, 322–324. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence (NICE). Antenatal care for uncomplicated pregnancies. In Clinical Guidelines; National Institute for Health and Care Excellence (NICE): London, UK, 2019. [Google Scholar]
- Abbas, A.M.; Elhalwagy, M.M.; Afifi, K.; Ibrahim, K.; Sweed, M.S. Single vs. Double Dose Iron Supplementation for Prevention of Iron Deficiency Anemia in Twin Pregnancy: A Randomized Controlled Clinical Trial. Open J. Obstet. Gynecol. 2020, 10, 1788–1802. [Google Scholar] [CrossRef]
- Kant, S.; Haldar, P.; Gupta, A.; Lohiya, A. Serum calcium level among pregnant women and its association with pre-eclampsia and delivery outcomes: A cross-sectional study from North India. Nepal J. Epidemiol. 2019, 9, 795–803. [Google Scholar] [CrossRef]
- CMR (Indian Council of Medical Research). National Institute of Nutrition/Indian Council of Medical Research. Dietary Guidelines for Indians; National Institute of Nutrition: Hyderabad, India, 2011. [Google Scholar]
- Pitkin, R.M.; Gebhardt, M.P. Serum calcium concentrations in human pregnancy. Am. J. Obstet. Gynecol. 1977, 127, 775–778. [Google Scholar] [CrossRef]
- Sabour, H.; Hossein-Nezhad, A.; Maghbooli, Z.; Madani, F.; Mir, E.; Larijani, B. Relationship between pregnancy outcomes and maternal vitamin D and calcium intake: A cross-sectional study. Gynecol. Endocrinol. 2006, 22, 585–589. [Google Scholar] [CrossRef]
- Hofmeyr, G.J.; Lawrie, T.A.; Atallah, A.N.; Duley, L.; Torloni, M.R. Calcium supplementation during pregnancy for preventing hypertensive disorders and related problems. Cochrane Database Syst. Rev. 2014, 10, CD001059. [Google Scholar] [CrossRef]
- Pitkin, R.M. Calcium metabolism in pregnancy and the perinatal period: A review. Am. J. Obstet. Gynecol. 1985, 151, 99–109. [Google Scholar] [CrossRef]
- Kumar, A.; Kaur, S. Calcium: A Nutrient in Pregnancy. J. Obstet. Gynaecol. India 2017, 67, 313–318. [Google Scholar] [CrossRef]
- Hadlock, F.P.; Harrist, R.B.; Martinez-Poyer, J. In utero analysis of fetal growth: A sonographic weight standard. Radiology 1991, 181, 129–133. [Google Scholar] [CrossRef]
- Hadlock, F.P.; Deter, R.L.; Harrist, R.B.; Park, S.K. Estimating fetal age: Computer-assisted analysis of multiple fetal growth parameters. Radiology 1984, 152, 497–5011. [Google Scholar] [CrossRef]
- Hoeflich, J.; Hollenbach, B.; Behrends, T.; Hoeg, A.; Stosnach, H.; Schomburg, L. The choice of biomarkers determines the selenium status in young German vegans and vegetarians. Br. J. Nutr. 2010, 104, 1601–1604. [Google Scholar] [CrossRef]
- Hughes, D.J.; Fedirko, V.; Jenab, M.; Schomburg, L.; Méplan, C.; Freisling, H.; Bueno-De-Mesquita, H.; Hybsier, S.; Becker, N.P.; Czuban, M.; et al. Selenium status is associated with colorectal cancer risk in the European prospective investigation of cancer and nutrition cohort. Int. J. Cancer 2014, 136, 1149–1161. [Google Scholar] [CrossRef]
- Karavasiloglou, N.; Hughes, D.J.; Murphy, N.; Schomburg, L.; Sun, Q.; Seher, V.; Rohrmann, S.; Weiderpass, E.; Tjønneland, A.; Olsen, A.; et al. Prediagnostic serum calcium concentrations and risk of colorectal cancer development in 2 large European prospective cohorts. Am. J. Clin. Nutr. 2023, 117, 33–45. [Google Scholar] [CrossRef]
- Cikim, G.; Gunal, M.Y.; Tok, A.; Kilinc, M.; Hansu, K.; Susam, S. In Twin Pregnancies, Zinc and Iron Decreased, While Copper Increased Minimally. Middle Black Sea J. Health Sci. 2022, 8, 450–457. [Google Scholar] [CrossRef]
- Campbell, R.K.; Buhimschi, C.S.; Zhao, G.; Dela Rosa, C.; Stetson, B.T.; Backes, C.H.; Buhimschi, I.A. Prevalence of and Risk Factors for Iron Deficiency in Twin and Singleton Newborns. Nutrients 2022, 14, 3854. [Google Scholar] [CrossRef]
- Shinar, S.; Skornick-Rapaport, A.; Maslovitz, S. Iron Supplementation in Twin Pregnancy—The Benefit of Doubling the Iron Dose in Iron Deficient Pregnant Women: A Randomized Controlled Trial. Twin Res. Hum. Genet. 2017, 20, 419–424. [Google Scholar] [CrossRef]
- Shinar, S.; Skornick-Rapaport, A.; Maslovitz, S. Iron supplementation in singleton pregnancy: Is there a benefit to doubling the dose of elemental iron in iron-deficient pregnant women? a randomized controlled trial. J. Perinatol. 2017, 37, 782–786. [Google Scholar] [CrossRef]
- Adaji, J.A.; Isah, A.Y.; Agida, E.T.; Otu, T.; Abdullahi, H.I. Daily versus twice daily dose of ferrous sulphate supplementation in pregnant women: A randomized clinical trial. Niger. J. Clin. Pract. 2019, 22, 1132–1139. [Google Scholar]
- Ru, Y.; Pressman, E.K.; Guillet, R.; Katzman, P.J.; Bacak, S.J.; O’Brien, K.O. Predictors of anemia and iron status at birth in neonates born to women carrying multiple fetuses. Pediatr. Res. 2018, 84, 199–204. [Google Scholar] [CrossRef]
- Ali, M.K.; Abbas, A.M.; Abdelmagied, A.M.; Mohammed, G.E.; Abdalmageed, O.S. A randomized clinical trial of the efficacy of single versus double-daily dose of oral iron for prevention of iron deficiency anemia in women with twin gestations. J. Matern. Fetal. Neonatal Med. 2017, 30, 2884–2889. [Google Scholar] [CrossRef]
- Sukonpan, K.; Phupong, V. Serum calcium and serum magnesium in normal and preeclamptic pregnancy. Arch. Gynecol. Obstet. 2005, 273, 12–16. [Google Scholar] [CrossRef]
- Kim, J.; Kim, Y.J.; Lee, R.; Moon, J.H.; Jo, I. Serum levels of zinc, calcium, and iron are associated with the risk of preeclampsia in pregnant women. Nutr. Res. 2012, 32, 764–769. [Google Scholar] [CrossRef] [PubMed]
- Jain, S.; Sharma, P.; Kulshreshtha, S.; Mohan, G.; Singh, S. The role of calcium, magnesium, and zinc in pre-eclampsia. Biol. Trace Elem. Res. 2010, 133, 162–170. [Google Scholar] [CrossRef] [PubMed]
- An, L.; Li, W.; Xie, T.; Peng, X.; Li, B.; Xie, S.; Xu, J.; Zhou, X.; Guo, S. Calcium supplementation reducing the risk of hypertensive disorders of pregnancy and related problems: A meta-analysis of multicentre randomized controlled trials. Int. J. Nurs. Pract. 2015, 21 (Suppl. S2), 19–31. [Google Scholar] [CrossRef] [PubMed]
- Grzeszczak, K.; Kapczuk, P.; Kupnicka, P.; Cecerska-Heryć, E.; Kwiatkowski, S.; Chlubek, D.; Kosik-Bogacka, D. Calcium, Potassium, Sodium, and Magnesium Concentrations in the Placenta, Umbilical Cord, and Fetal Membrane from Women with Multiple Pregnancies. Life 2023, 13, 153. [Google Scholar] [CrossRef]
- Nakayama, S.; Yasui, T.; Suto, M.; Sato, M.; Kaji, T.; Uemura, H.; Maeda, K.; Irahara, M. Differences in bone metabolism between singleton pregnancy and twin pregnancy. Bone 2011, 49, 513–519. [Google Scholar] [CrossRef]
- Goswami, D.; Rani, R.; Saxena, A.; Arora, M.S.; Batra, S.; Sreenivas, V. Maternal and neonatal vitamin-D status in twin versus singleton pregnancies. J. Obstet. Gynaecol. Res. 2016, 42, 1250–1257. [Google Scholar] [CrossRef]
- Haliloglu, B.; Ilter, E.; Aksungar, F.B.; Celik, A.; Coksuer, H.; Gunduz, T.; Yucel, E.; Ozekici, U. Bone turnover and maternal 25(OH) vitamin D3 levels during pregnancy and the postpartum period: Should routine vitamin D supplementation be increased in pregnant women? Eur. J. Obstet. Gynecol. Reprod. Biol. 2011, 158, 24–27. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mothers in Singleton Pregnancy (n = 105) | Mothers in Twin Pregnancy (n = 9) | p-Value | |
|---|---|---|---|
| Me (Q1–Q3) | Me (Q1–Q3) | ||
| Age (years) | 34 (32–36) | 34 (32–36) | 0.9297 |
| SBP (mm Hg) | 110 (100–120) | 118 (111–120) | 1.0000 |
| DBP (mm Hg) | 70 (60–73) | 65 (60–73) | 1.0000 |
| Gravidity (n) | 2 (1–2) | 2 (2–2) | 0.4053 |
| Parity (n) | 0 (0–1) | 1 (0–1) | 0.2729 |
| RBC (T/L) | 4.19 (3.9–4.4) | 4.4 (4.12–4.59) | 0.2269 |
| Hb (mmol/L) | 7.6 (6.9–8.0) | 7.2 (7.0–7.7) | 0.7093 |
| Ht (L/L) | 0.363 (0.334–0.381) | 0.355 (0.345–0.375) | 0.9382 |
| MCV (fL) | 87.6 (84.6–90.0) | 85.2 (85.0–86.2) | 0.1029 |
| MCH (fmol) | 1.84 (1.74–1.91) | 1.75 (1.7–1.79) | 0.0771 |
| MCHC (mmol/L) | 20.9 (20.5–21.2) | 20.3 (19.9–20.5) | 0.0814 |
| RDW (%) | 13.2 (12.7–13.6) | 13.1 (12.9–13.7) | 0.8970 |
| Prevalence of anemia (%) * | 17.1 | 22.2 | 0.6565 |
| Singleton Pregnancy (n = 105) | Twin Pregnancy (n = 9) | p-Value | |
|---|---|---|---|
| Me (Q1–Q3) | Me (Q1–Q3) | ||
| The week of delivery | 39 (38–40) | 36 (36–37) | 0.0001 |
| Birth weight (g) | 3475 (3180–3760) | 2740 (2380–3020) | 0.0001 |
| The newborn weight at the day of hospital discharge (g) | 62 (56–70) | 66 (62–79) | 0.1136 |
| 1 min Apgar score (points) | 10 (10–10) | 10 (9–10) | 0.4603 |
| 3 min Apgar score (points) | 10 (10–10) | 10 (10–10) | 0.2542 |
| Umbilical venous pH | 7.28 (7.22–7.33) | 7.31 (7.26–7.33) | 0.5037 |
| Umbilical venous BE | −2.57 (−5.38–−0.52) | −2.31 (−4.31–−1.68) | 0.9958 |
| Body length (cm) | 54 (53–56) | 50 (49–52) | 0.0001 |
| Head circumference (cm) | 34.5 (33.5–35.5) | 33 (32–35) | 0.0268 |
| Thoracic circumference (cm) | 34 (33–35) | 31 (30–32) | 0.0001 |
| The length of hospitalization (days) | 5 (4–6) | 6 (6–9) | 0.0186 |
| Mothers in Singleton Pregnancy (n = 105) | Mothers in Twin Pregnancy (n = 9) | p-Value | OR | p-Value | RR | p-Value | |
|---|---|---|---|---|---|---|---|
| Me (Q1–Q3) | Me (Q1–Q3) | ||||||
| Serum Fe concentration (µg/L) | 1729.5 (1204.7–2346.0) | 2048.0 (1175.6–3098.0) | 0.6273 | - | - | - | - |
| below ref-range (%) | 2.9 | 11.1 | 0.2836 | 4.25 (0.39–45.68) | 0.2324 | 3.88 (0.44–33.66) | 0.2174 |
| within ref-range (%) | 88.6 | 66.7 | 0.0955 | 0.25 (0.05–1.16) | 0.0788 | 0.75 (0.47–1.20) | 0.2331 |
| above ref-range (%) | 8.5 | 22.2 | 0.2093 | 3.04 (0.54–16.91) | 0.2024 | 2.59 (0.65–10.22) | 0.1737 |
| Serum Ca concentration (mg/L) | 77.5 (72.4–86.4) | 103.5 (70.2–107.2) | 0.1491 | - | - | - | - |
| below ref-range (%) | 66.7 | 44.4 | 0.2739 | 0.40 (0.10–1.58) | 0.1918 | 0.66 (0.31–1.40) | 0.2847 |
| within ref-range (%) | 29.5 | 55.6 | 0.1382 | 2.98 (0.75–11.86) | 0.1205 | 1.88 (0.97–3.62) | 0.0584 |
| above ref-range (%) | 3.8 | 0.0 | 1.0000 | 1.18 (0.05–23.76) | 0.9106 | 1.17 (0.06–20.33) | 0.9103 |
| Newborns from Singleton Pregnancy (n = 61) | Newborns from Twin Pregnancy (n = 12) | p-Value | |
|---|---|---|---|
| Me (Q1–Q3) | Me (Q1–Q3) | ||
| Umbilical cord serum Fe concentration (µg/L) | 2514.0 (2021.5–3283.0) | 2938 (2283.0–3451.0) | 0.2431 |
| Umbilical cord serum Ca concentration (mg/L) | 90.4 (82.4–97.8) | 93.5 (84.4–100.5) | 0.4717 |
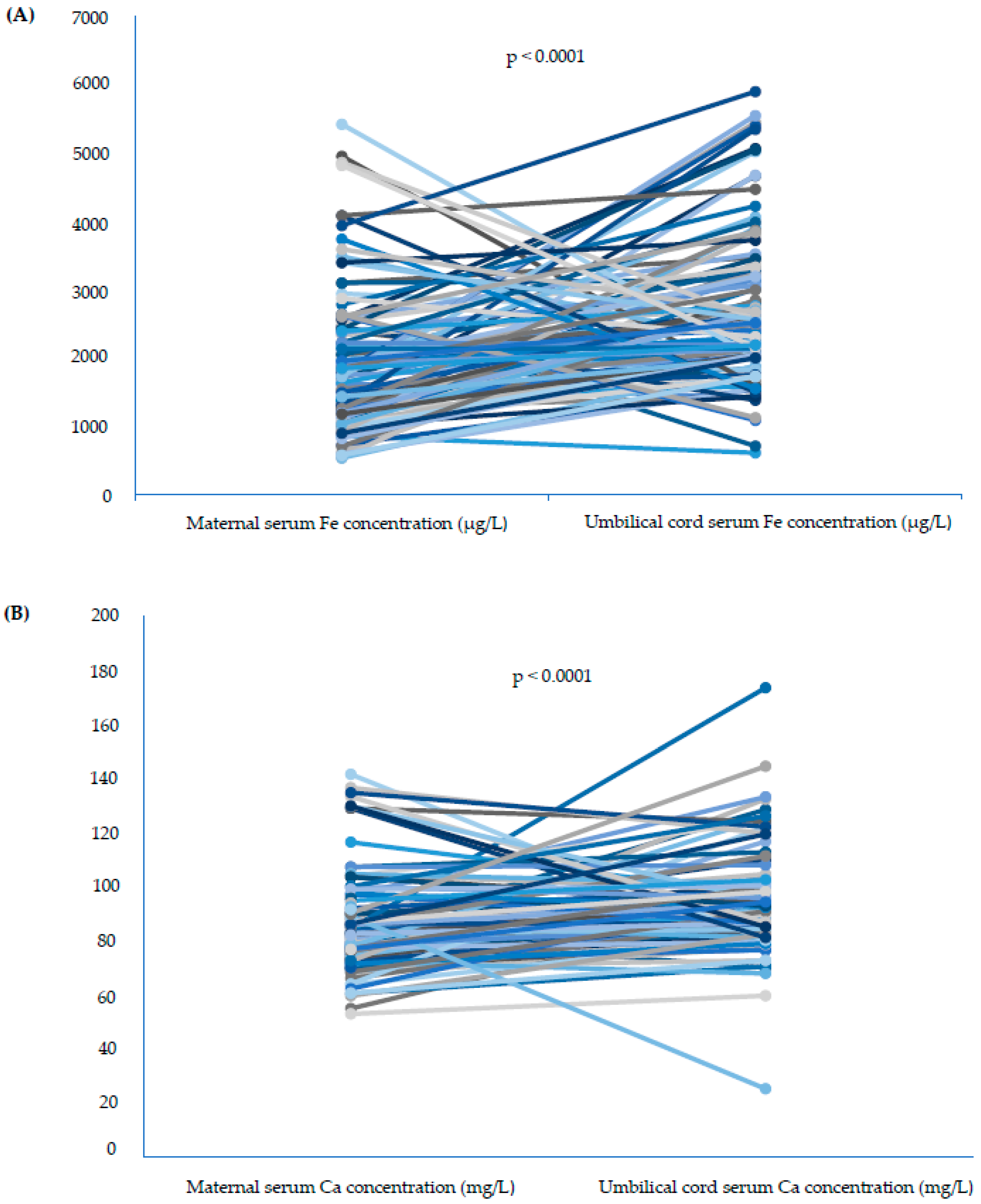
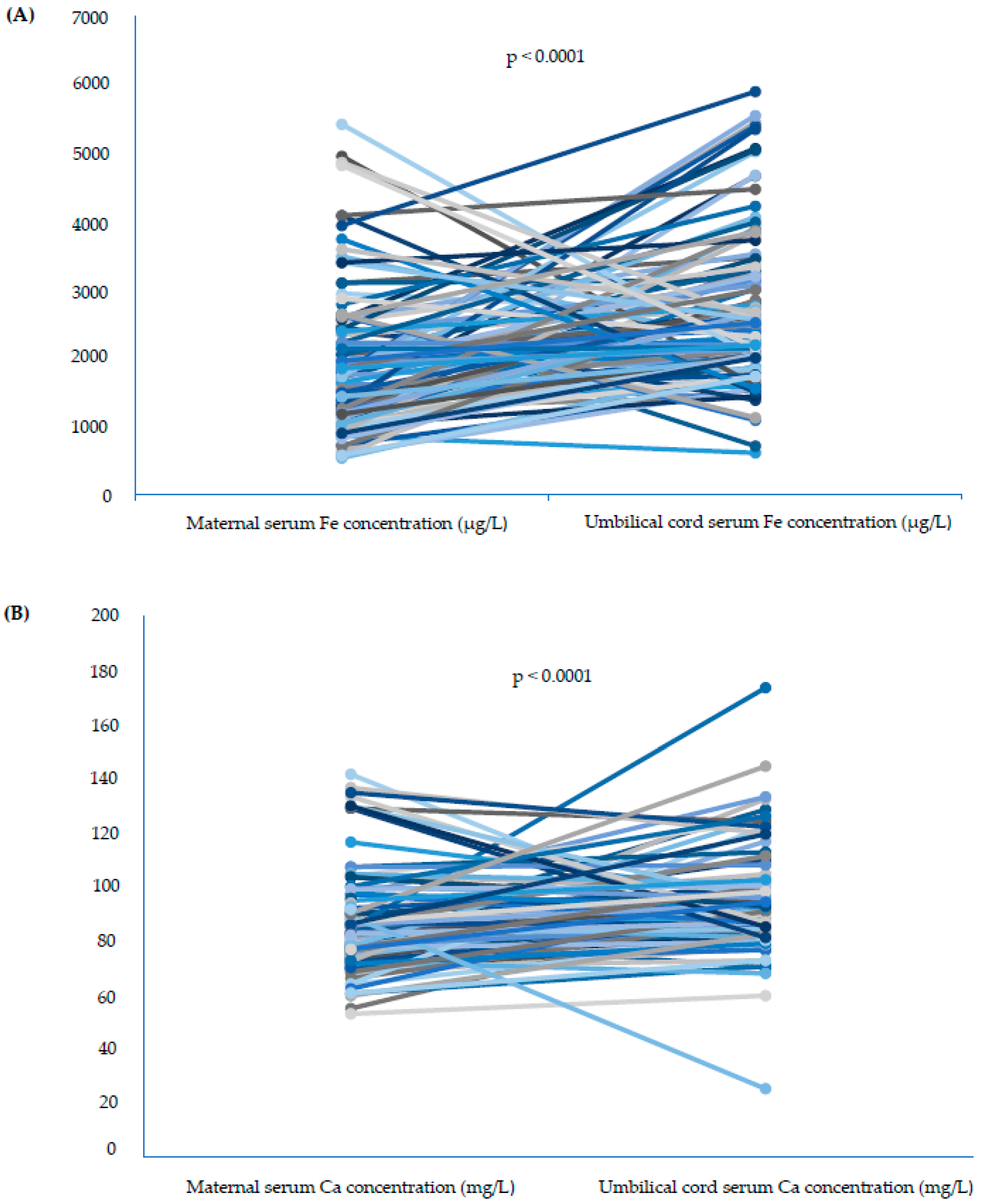
| Mothers (n = 114) | Newborns (n = 73) | p-Value for Mann–Whitney U Test | p-Value for Wilcoxon Test | |
|---|---|---|---|---|
| Me (Q1–Q3) | Me (Q1–Q3) | |||
| Serum Fe concentration (µg/L) | 1745.6 (1222.5–2398.0) | 2562.0 (2031.0–3231.0) | 0.0001 | <0.0001 |
| Serum Ca concentration (mg/L) | 78.1 (72.1–89.1) | 90.8 (83.3–98.4) | 0.0001 | <0.0001 |
| Singleton Pregnancies (n = 103) | Twin Pregnancies (n = 9) | |||||
|---|---|---|---|---|---|---|
| Prenatal Supplementation (+) (n = 67) | Prenatal Supplementation (−) (n = 36) | p-Value | Prenatal Supplementation (+) (n = 5) | Prenatal Supplementation (−) (n = 4) | p-Value | |
| Me (Q1–Q3) | Me (Q1–Q3) | Me (Q1–Q3) | Me (Q1–Q3) | |||
| Maternal serum Fe concentration (µg/L) | 1817.6 (1257.2–2386.5) | 1518.7 (944.0–1901.7) | 0.0464 | 2048.0 (1030.8–2222.0) | 2352.0 (1274.9–3568.5) | 1.0000 |
| Maternal serum Ca concentration (mg/L) | 79.3 (73.1–86.9) | 76.2 (71.6–84.6) | 0.2403 | 82.8 (70.2–104.6) | 116.2 (95.1–129.1) | 1.0000 |
| Umbilical cord blood serum Fe concentration (µg/L) | 2512.0 (2058.0–3220.0) | 2382.0 (1731.0–2826.0) | 0.2057 | 2938.0 (2611.0–3372.5) | 2562.0 (1952.4–3483.0) | 0.5361 |
| Umbilical cord blood serum Ca concentration (mg/L) | 91.1 (82.4–99.9) | 87.7 (82.8–95.2) | 0.3569 | 97.2 (83.7–106.2) | 91.3 (85.7–94.4) | 0.6330 |
| AUC | Cut-Off | Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) | p-Value | |
|---|---|---|---|---|---|---|---|
| Maternal serum Fe concentrations (μg/L) | |||||||
| Preterm birth | 0.490 | <1175.6 | 50 | 79 | 12 | 97 | 0.9082 |
| Birth weight < 2500 g | 0.685 | <965.2 | 67 | 88 | 24 | 98 | 0.1275 |
| Maternal serum Ca concentrations (mg/L) | |||||||
| Preterm birth | 0.253 | <63.9 | 17 | 94 | 13 | 95 | 0.0423 |
| Small birth weight | 0.469 | <71.3 | 50 | 81 | 13 | 97 | 0.7996 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dera-Szymanowska, A.; Filipowicz, D.; Misan, N.; Szymanowski, K.; Chillon, T.S.; Asaad, S.; Sun, Q.; Szczepanek-Parulska, E.; Schomburg, L.; Ruchała, M. Are Twin Pregnancies at Higher Risk for Iron and Calcium Deficiency than Singleton Pregnancies? Nutrients 2023, 15, 4047. https://doi.org/10.3390/nu15184047
Dera-Szymanowska A, Filipowicz D, Misan N, Szymanowski K, Chillon TS, Asaad S, Sun Q, Szczepanek-Parulska E, Schomburg L, Ruchała M. Are Twin Pregnancies at Higher Risk for Iron and Calcium Deficiency than Singleton Pregnancies? Nutrients. 2023; 15(18):4047. https://doi.org/10.3390/nu15184047
Chicago/Turabian StyleDera-Szymanowska, Anna, Dorota Filipowicz, Natalia Misan, Krzysztof Szymanowski, Thilo Samson Chillon, Sabrina Asaad, Qian Sun, Ewelina Szczepanek-Parulska, Lutz Schomburg, and Marek Ruchała. 2023. "Are Twin Pregnancies at Higher Risk for Iron and Calcium Deficiency than Singleton Pregnancies?" Nutrients 15, no. 18: 4047. https://doi.org/10.3390/nu15184047
APA StyleDera-Szymanowska, A., Filipowicz, D., Misan, N., Szymanowski, K., Chillon, T. S., Asaad, S., Sun, Q., Szczepanek-Parulska, E., Schomburg, L., & Ruchała, M. (2023). Are Twin Pregnancies at Higher Risk for Iron and Calcium Deficiency than Singleton Pregnancies? Nutrients, 15(18), 4047. https://doi.org/10.3390/nu15184047