
Do People Want the ‘New Normal’? A Mixed Method Investigation of Young Person, Parent, and Clinician Experience and Preferences for Eating Disorder Treatment Delivery in the Post-COVID-19 World

 , ,
, ,
Abstract
:1. Background
2. Materials and Methods
2.1. Study Design
2.2. Sample
2.3. Treatment Setting
2.4. Ethical Approval and Consent
2.5. Procedure
2.6. Analysis Plan
2.7. Reflexivity Statement
3. Results
3.1. Sample
3.2. Treatment Characteristics
3.3. Quantitative Findings
3.3.1. Young Person and Parent/Caregiver Experience of Online Treatment
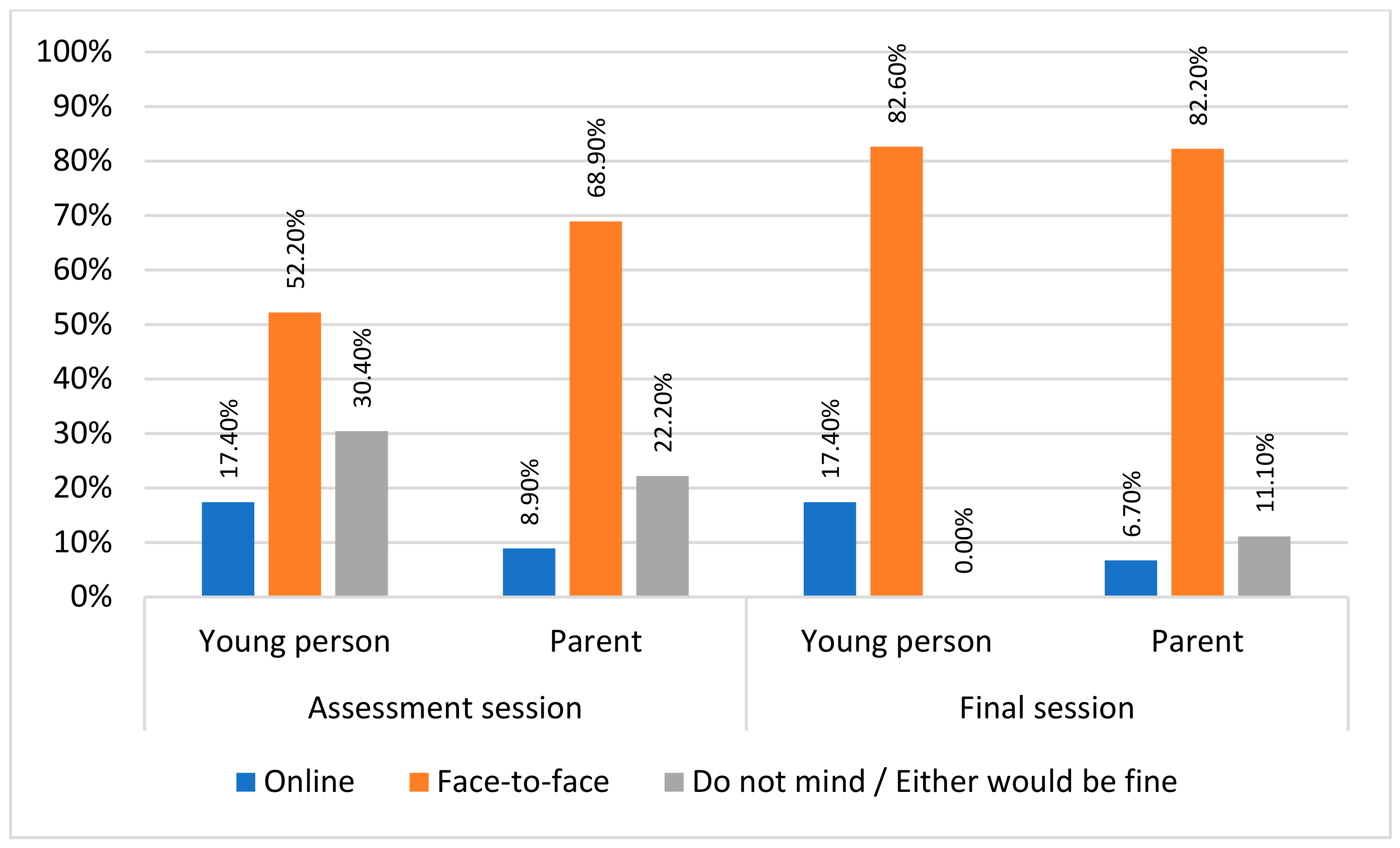
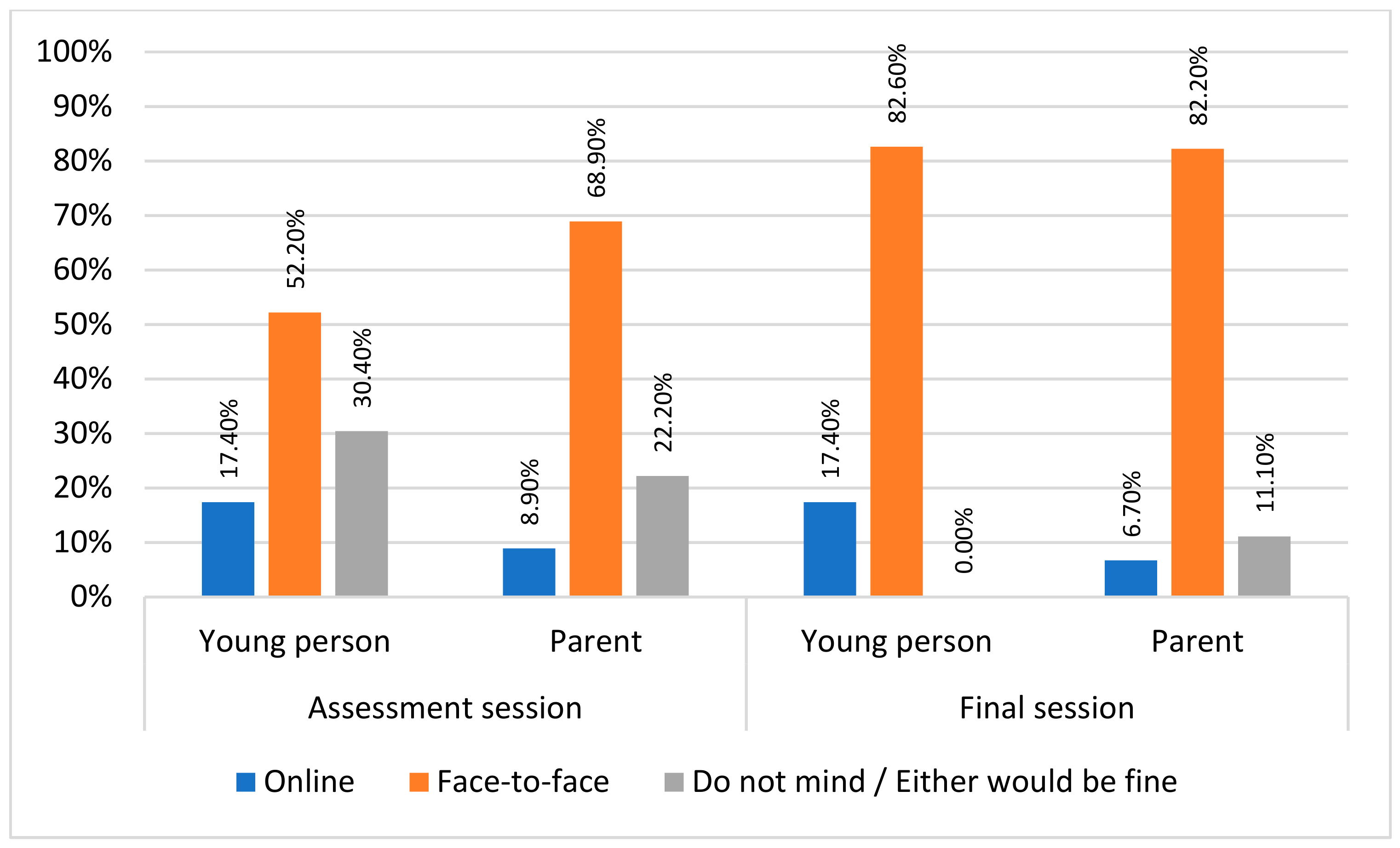
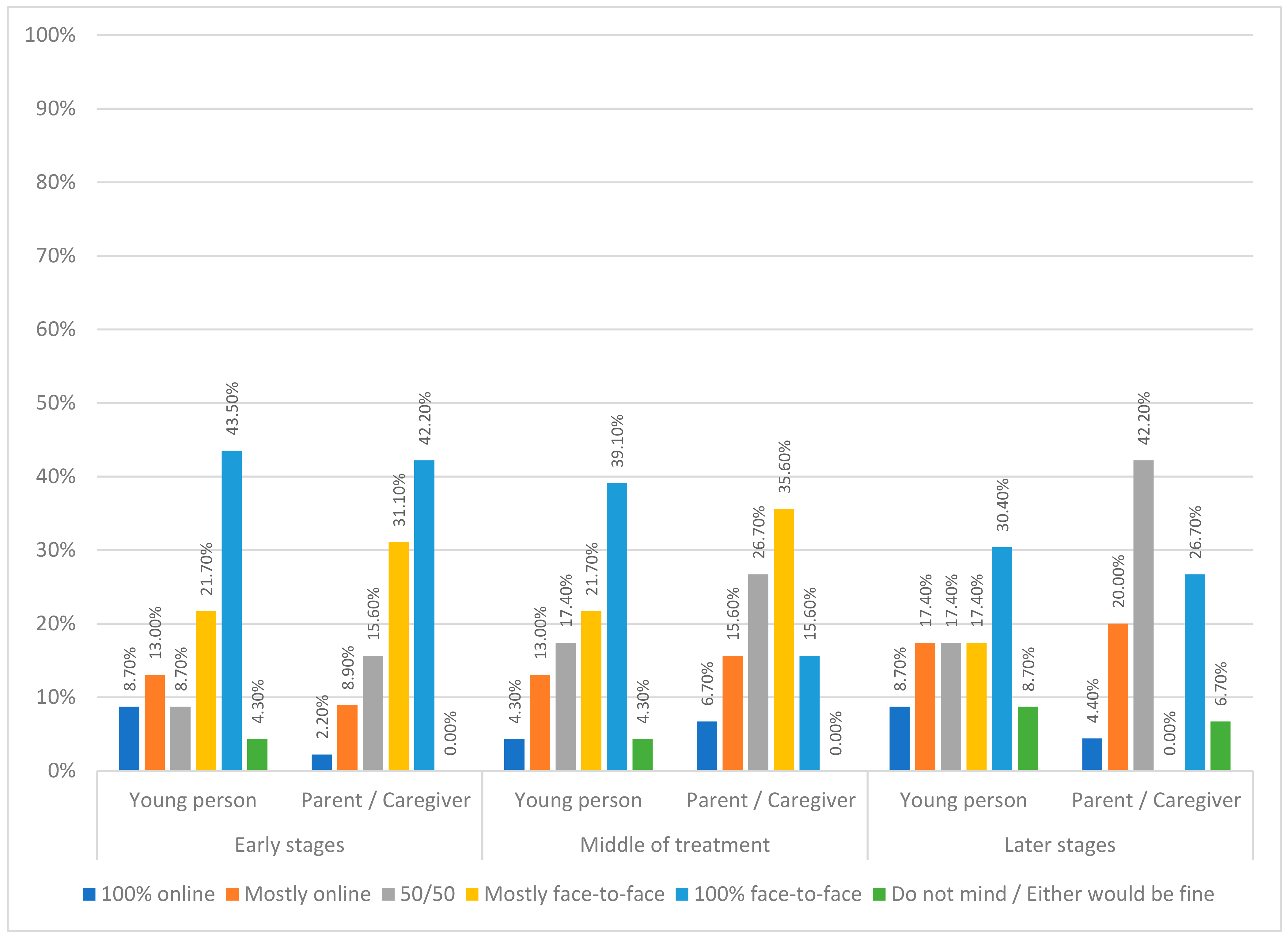
3.3.2. Treatment Mode Preferences
3.3.3. Perceived Impact of Treatment Mode on Different Aspects of Treatment
3.3.4. Comparison of Current Experiences of Online Therapy to Those at the Beginning of the COVID-19 Pandemic
3.4. Qualitative Findings
3.4.1. Theme 1: Something Gained
Care Continuity and Increased Access
‘We had to travel over the summer holidays so it was fantastic to be able to continue therapy’(parent/caregiver)
‘… online [meant we had] continuity of therapy when not able to attend clinic’(young person)
‘I have found that for some families and young people, especially those with neuro diverse conditions or who live far and are less able to attend in person, conducting online therapy has been more beneficial or enabled the process better.’(clinician)
Convenience and Comfort
‘Face-to-face is preferred, however, sometimes online is good to discuss simple practical issues that does not require a meeting’(parent/caregiver)
‘Also, there are times when travel is difficult and online is a good compromise.’(parent/caregiver)
‘My own home…my dogs are there…having them sit with me whilst I have the meeting makes me feel calmer’(young person)
‘Flexibility for staff and patients. Some patients more comfortable in own home’(clinician)
‘[online is] more comfortable … easier to tell her [therapist] how I feel’(young person)
‘Towards the end online can work better in terms of returning to normal life and not missing school’(clinician)
New Opportunities
‘I was sceptical about the effectiveness at first but after two years I feel it can have the same intensity and effectiveness as face-to-face.’(clinician)
‘I was always opposed to this idea thinking it would really impact the therapeutic relationship. However, I have worked really effectively with many patients and families since with good outcomes with some patients I had never seen in person.’(clinician)
‘I think that I started to use different strategies to engage people on-line—more playful, use of humour—which is easier when families are in their own space and not behaving a certain way because they are in a clinic.’(clinician)
‘I have had more attendance from wider family members than for face-to-face treatment. I think there is also an advantage for some people in that they can more directly translate conversations to home (e.g., meal strategies, self-soothe boxes, etc.)’(clinician)
‘I think the therapist can get a real insight into the patients home life through what goes on around the sessions—ours were chaos with dogs and siblings coming through which often broke the ice when we were at an impasse.’(parent/caregiver)
‘Easier for family therapy as you can organise the whole family to be in one place’(young person)
3.4.2. Theme 2: Something Lost
Depth of Treatment Experience
‘[I] don’t feel that I can open up as much when just looking at someone one a screen.’(young person)
‘I strongly believe nuances of communication are lost online leading to a lower level of understanding of what is going on for my daughter.’(parent/caregiver)
‘I cannot always easily sense the family’s emotional experience and dynamics during a virtual session especially if a family member is not as engaged.’(clinician)
‘Face-to-face contribute [s to a] speedier recovery—more connected.’(parent/caregiver)
‘Online therapy may result in slower recovery … less connection.’(young person)
‘…it has felt like, the treatment was longer.’(clinician)
Therapy Flow
‘I sometimes was a bit anxious to tell her [the therapist] how I felt because I was worried someone in my family would be listening as it was online meaning I was in my home.’(young person)
‘Confidentiality is tough—we live in a small flat. My child can’t speak freely without fearing being overheard.’(parent/caregiver)
‘Confidentiality worries due to sharing an environment with others might have an impact on individual sessions if there are restrictions on availability of a separate room’(clinician)
‘It’s easier for me to talk face-to-face. Online I get distracted and lose interest’(young person)
‘It can be more difficult to fully open up as it’s a less intimate setting. Also, quite easy to get distracted or impatient for the session to end when at home.’(young person)
‘My child tends to look away and shut down online—she does not do this as much in a room and if she does you can bring her around easier’(parent/caregiver)
Lack of Insight into Progress
‘It was a bit more distressing to be weighed at home than in the clinic’(young person)
‘It was easier for my eating disorder to convince me to lie’(young person)
‘Lack of ability to read body language and gauge mood as accurately. Inability to weigh people, physically examine them, take bloods, do ECGs, etc. leading to lack of accurate knowledge about actual state of someone’s health’(parent/caregiver)
‘It might not be very easy to visually see the changes in patient’s physical state. It might make it easier to falsify weight by patients with eating disorders’(clinician)
Is this Real? Devaluation vs. Realness
‘Not feeling my issues were being taken seriously and not taking the advice given as seriously when online’(young person)
‘… doesn’t feel as ‘real’ as face-to-face’(parent/caregiver)
‘One of the strangest things has been saying goodbye to people online. Sometimes it makes it seem like they weren’t even real.’(clinician)
3.4.3. Theme 3: One Size Does Not Fit All
Dynamic Flexibility
‘I feel it can be effective for some patients but not all. I am less confident drawing out formulations and other diagrams online’(clinician)
‘Online would not work for my child, she needed 100% face-to-face (I suppose it depends on the child).’(parent/caregiver)
‘I think groups for young people would probably work better in person- it’s easier to be a spectator rather than a participant in an online group. For family and individual work I find both types of treatment fairly equitable’(clinician)
‘I am more likely to offer an individual, skills-based treatment (e.g., CBT) online rather than face-to-face’(clinician)
Timing
‘I think it is important to meet your therapist face-to-face occasionally (especially at the beginning of treatment when needing to monitor weight and physical health)…’(young person)
‘…to promote engagement and early behaviour change then face-to-face can be preferable for some young people and families. Towards the end online can work better in terms of returning to normal life and not missing school etc’(clinician)
‘Initial stages of treatment where there could be prominent physical or psychological risk or any stage when risk is increasing, can change the appropriate format for a given patient and requires flexibility.’(clinician)
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Carlbring, P.; Andersson, G.; Cuijpers, P.; Riper, H.; Hedman-Lagerlöf, E. Internet-based vs. face-to-face cognitive behavior therapy for psychiatric and somatic disorders: An updated systematic review and meta-analysis. Cogn. Behav. Ther. 2018, 47, 1–18. [Google Scholar] [PubMed]
- Wootton, B.M. Remote cognitive–behavior therapy for obsessive–Compulsive symptoms: A meta-analysis. Clin. Psychol. Rev. 2016, 43, 103–113. [Google Scholar] [PubMed]
- Aardoom, J.J.; Dingemans, A.E.; Spinhoven, P.; Van Furth, E.F. Treating eating disorders over the internet: A systematic review and future research directions: Treating Eating Disorders Over the Internet. Int. J. Eat. Disord. 2013, 46, 539–552. [Google Scholar] [PubMed]
- Anderson, K.E.; Byrne, C.E.; Crosby, R.D.; Le Grange, D. Utilizing Telehealth to deliver family-based treatment for adolescent anorexia nervosa. Int. J. Eat. Disord. 2017, 50, 1235–1238. [Google Scholar] [CrossRef] [PubMed]
- Sproch, L.E.; Anderson, K.P. Clinician-Delivered Teletherapy for Eating Disorders. Psychiatr. Clin. N. Am. 2019, 42, 243–252. [Google Scholar]
- Davis, C.; Ng, K.C.; Oh, J.Y.; Baeg, A.; Rajasegaran, K.; Chew, C.S.E. Caring for Children and Adolescents with Eating Disorders in the Current Coronavirus 19 Pandemic: A Singapore Perspective. J. Adolesc. Health 2020, 67, 131–134. [Google Scholar]
- Simon, P.D. A quick review of recommendations and evidences on telepsychotherapy and digital psychiatry for researchers and mental health professionals in the time of COVID-19. Int. J. Soc. Psychiatry 2020, 67, 604–605. [Google Scholar]
- Smith, K.; Ostinelli, E.; Macdonald, O.; Cipriani, A. COVID-19 and Telepsychiatry: Development of Evidence-Based Guidance for Clinicians. JMIR Ment. Health 2020, 7, e21108. [Google Scholar]
- Waller, G.; Pugh, M.; Mulkens, S.; Moore, E.; Mountford, V.A.; Carter, J.; Wicksteed, A.; Maharaj, A.; Wade, T.D.; Wisniewski, L.; et al. Cognitive-behavioral therapy in the time of coronavirus: Clinician tips for working with eating disorders via telehealth when face-to-face meetings are not possible. Int. J. Eat. Disord. 2020, 53, 1132–1141. [Google Scholar]
- Weissman, R.S.; Bauer, S.; Thomas, J.J. Access to evidence-based care for eating disorders during the COVID-19 crisis. Int. J. Eat. Disord. 2020, 53, 639–646. [Google Scholar]
- Linardon, J.; Messer, M.; Rodgers, R.F.; Fuller-Tyszkiewicz, M. A systematic scoping review of research on COVID-19 impacts on eating disorders: A critical appraisal of the evidence and recommendations for the field. Int. J. Eat. Disord. 2021, 55, 3–38. [Google Scholar] [CrossRef] [PubMed]
- Shaw, H.; Robertson, S.; Ranceva, N. What was the impact of a global pandemic (COVID-19) lockdown period on experiences within an eating disorder service? A service evaluation of the views of patients, parents/carers and staff. J. Eat. Disord. 2021, 9, 14. [Google Scholar] [CrossRef] [PubMed]
- Lewis, Y.D.; Elran-Barak, R.; Grundman-Shem Tov, R.; Zubery, E. The abrupt transition from face-to-face to online treatment for eating disorders: A pilot examination of patients’ perspectives during the COVID-19 lockdown. J. Eat. Disord. 2021, 9, 31. [Google Scholar] [CrossRef]
- Linardon, J.; Shatte, A.; Tepper, H.; Fuller-Tyszkiewicz, M. A survey study of attitudes toward, and preferences for, e-therapy interventions for eating disorder psychopathology. Int. J. Eat. Disord. 2020, 53, 907–916. [Google Scholar] [CrossRef] [PubMed]
- Brothwood, P.L.; Baudinet, J.; Stewart, C.S.; Simic, M. Moving online: Young people and parents’ experiences of adolescent eating disorder day programme treatment during the COVID-19 pandemic. J. Eat. Disord. 2021, 9, 62. [Google Scholar] [CrossRef]
- Stewart, C.; Konstantellou, A.; Kassamali, F.; McLaughlin, N.; Cutinha, D.; Bryant-Waugh, R.; Simic, M.; Eisler, I.; Baudinet, J. Is this the ‘new normal’? A mixed method investigation of young person, parent and clinician experience of online eating disorder treatment during the COVID-19 pandemic. J. Eat. Disord. 2021, 9, 78. [Google Scholar] [CrossRef]
- Wood, S.M.; White, K.; Peebles, R.; Pickel, J.; Alausa, M.; Mehringer, J.; Dowshen, N. Outcomes of a Rapid Adolescent Telehealth Scale-Up During the COVID-19 Pandemic. J. Adolesc. Health 2020, 67, 172–178. [Google Scholar] [CrossRef]
- Tan, Y.; Lattie, E.G.; Qiu, Y.; Teng, Z.; Wu, C.; Tang, H.; Chen, J. Accessibility of mental health support in China and preferences on web-based services for mood disorders: A qualitative study. Internet Interv. 2021, 26, 100475. [Google Scholar] [CrossRef]
- Nesher Shoshan, H.; Wehrt, W. Understanding “Zoom fatigue”: A mixed-method approach. Appl. Psychol. 2022, 71, 827–852. [Google Scholar] [CrossRef]
- Li, B.B.J.; Yee, A.Z. Understanding videoconference fatigue: A systematic review of dimensions, antecedents and theories. Internet Res. 2023, 33, 796–819. [Google Scholar] [CrossRef]
- Nagata, J.M. Rapid Scale-Up of Telehealth During the COVID-19 Pandemic and Implications for Subspecialty Care in Rural Areas. J. Rural Health 2021, 37, 144–145. [Google Scholar] [CrossRef] [PubMed]
- Braun, V.; Clarke, V.; Boulton, E.; Davey, L.; McEvoy, C. The online survey as a qualitative research tool. Int. J. Soc. Res. Methodol. 2021, 24, 641–654. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013; 947p. [Google Scholar]
- Simic, M.; Stewart, C.S.; Konstantellou, A.; Eisler, I.; Baudinet, J. From efficacy to effectiveness: Child and adolescent eating disorder treatments in the real world (part 1)—Treatment course and outcomes. J. Eat. Disord. 2022, 10, 27. [Google Scholar] [CrossRef] [PubMed]
- Stewart, C.S.; Baudinet, J.; Munuve, A.; Bell, A.; Konstantellou, A.; Eisler, I.; Simic, M. From efficacy to effectiveness: Child and adolescent eating disorder treatments in the real world (Part 2): 7-year follow-up. J. Eat. Disord. 2022, 10, 14. [Google Scholar] [CrossRef] [PubMed]
- Baudinet, J.; Simic, M.; Griffiths, H.; Donnelly, C.; Stewart, C.; Goddard, E. Targeting maladaptive overcontrol with radically open dialectical behaviour therapy in a day programme for adolescents with restrictive eating disorders: An uncontrolled case series. J. Eat. Disord. 2020, 8, 68. [Google Scholar] [CrossRef]
- Simic, M.; Stewart, C.S.; Eisler, I.; Baudinet, J.; Hunt, K.; O’Brien, J.; McDermott, B. Intensive treatment program (ITP): A case series service evaluation of the effectiveness of day patient treatment for adolescents with a restrictive eating disorder. Int. J. Eat. Disord. 2018, 51, 1261–1269. [Google Scholar] [CrossRef]
- Baudinet, J.; Simic, M.; Eisler, I. From Treatment Models to Manuals: Maudsley Single- and Multi-Family Therapy for Adolescent Eating Disorders. In Systemic Approaches to Manuals, 1st ed.; Mariotti, M., Saba, G., Stratton, P., Eds.; European Family Therapy Association Series; Springer: Cham, Switzerland, 2021; pp. 349–372. [Google Scholar]
- Eisler, I.; Simic, M.; Blessitt, E.; Dodge, L.; MCCAED Team. Maudsley Service Manual for Child and Adolescent Eating Disorders. 2016. Available online: https://mccaed.slam.nhs.uk/wp-content/uploads/2019/11/Maudsley-Service-Manual-for-Child-and-Adolescent-Eating-Disorders-July-2016.pdf (accessed on 5 July 2021).
- Baudinet, J.; Eisler, I.; Dawson, L.; Simic, M.; Schmidt, U. Multi-Family Therapy for Eating Disorders: A Systematic Scoping Review of the Quantitative and Qualitative Findings. Int. J. Eat. Disord. 2021, 54, 2095–2120. [Google Scholar] [CrossRef]
- Simic, M.; Baudinet, J.; Blessitt, E.; Wallis, A.; Eisler, I. Multi-Family Therapy for Anorexia Nervosa: A Treatment Manual, 1st ed.; Routledge: London, UK, 2021. [Google Scholar]
- Baudinet, J.; Stewart, C.; Bennett, E.; Konstantellou, A.; Parham, R.; Smith, K.; Hunt, K.; Eisler, I.; Simic, M. Radically open dialectical behaviour therapy adapted for adolescents: A case series. BMC Psychiatry 2021, 21, 462. [Google Scholar] [CrossRef]
- Baudinet, J.; Watson, C.; Brothwood, P.L.; Parham, R.; Smith, L.; Snowden, N.; Konstantellou, A.; Hunt, K.; Simic, M. Adolescent experience of radically open dialectical behaviour therapy: A qualitative study. BMC Psychiatry 2022, 22, 466. [Google Scholar] [CrossRef]
- Qualtrics XM. Qualtrics: Provo, UT, USA. 2005. Available online: https://www.qualtrics.com (accessed on 21 March 2023).
- Braun, V.; Clarke, V. One size fits all? What counts as quality practice in (reflexive) thematic analysis? Qual. Res. Psychol. 2021, 18, 328–352. [Google Scholar] [CrossRef]
- IBM. Statistical Package for Social Sciences (SPSS); IBM Corporation: Armonk, NY, USA, 2019. [Google Scholar]
- Microsoft Corporation. Microsoft Excel. 2018. Available online: https://office.microsoft.com/excel (accessed on 25 July 2023).
- Hamadi, L.; Holliday, J. Moderators and mediators of outcome in treatments for anorexia nervosa and bulimia nervosa in adolescents: A systematic review of randomized controlled trials. Int. J. Eat. Disord. 2020, 53, 3–19. [Google Scholar] [CrossRef] [PubMed]
- Jewell, T.; Blessitt, E.; Stewart, C.; Simic, M.; Eisler, I. Family Therapy for Child and Adolescent Eating Disorders: A Critical Review. Fam. Process 2016, 55, 577–594. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Treatment Mode | Young People % (n) | Parents/Caregivers % (n) |
|---|---|---|
| 100% online | 16.00% (4) | 12.20% (6) |
| Mostly online | 28.00% (7) | 26.50% (13) |
| 50/50 | 8.00% (2) | 12.20% (6) |
| Mostly face-to-face | 36.00% (9) | 40.80% (20) |
| 100% face-to-face | 12.00% (3) | 8.20% (4) |
| Missing | 0 | 0 |
| Young People (N = 25) | Parents/Caregivers (N = 49) | Test Statistics | |||
|---|---|---|---|---|---|
| Mdn. (IQR) | n | Mdn. (IQR) | n | ||
| Overall experience | 5 (4–6) | 22 | 6 (5–7) | 45 | U = 330.00, p = 0.24 |
| Difficulties understood by therapist | 6 (5–6) | 23 | 7 (6–7) | 45 | U = 295.50, p = 0.002 * |
| Address important issues | 6 (5–7) | 23 | 7 (6–7) | 45 | U = 394.00, p = 0.83 |
| Impact of technology on treatment experience | 2 (1–4) | 18 | 3.5 (1–4) | 42 | U = 334.50, p = 0.47 |
| Benefit from online therapy | 6 (4–7) | 15 | 6 (5–7) | 36 | U = 262.00, p = 0.86 |
| Overall experience | 5 (4–6) | 22 | 6 (5–7) | 45 | U = 330.00, p = 0.24 |
| Young People % (n) | Parents/Caregivers % (n) | Clinicians % (n) | |
|---|---|---|---|
| 100% online | 4.30% (1) | 0.00% (0) | 0.00% (0) |
| Mostly online | 13.00% (3) | 15.60% (7) | 6.30% (1) |
| 50/50 | 21.70% (5) | 24.40% (11) | 37.50% (6) |
| Mostly face-to-face | 26.10% (6) | 35.60% (16) | 31.30% (5) |
| 100% face-to-face | 34.80% (8) | 24.40% (11) | 0.00% (0) |
| Missing | 2 | 4 | 4 |
| Online Better % (n) | Both Equally Good % (n) | Face-to-Face Better % (n) | ||||
|---|---|---|---|---|---|---|
| Young Person | Parent/ Caregiver | Young Person | Parent/ Caregiver | Young Person | Parent/ Caregiver | |
| Engagement with therapist | 0.00% (0) | 5.00% (2) | 29.40% (5) | 42.5% (17) | 70.60% (12) | 52.50% (21) |
| Confidentiality | 17.60% (3) | 5.00% (2) | 58.80% (10) | 67.5% (27) | 23.50% (4) | 27.50% (11) |
| Ability to discuss emotional difficulties | 11.80% (2) | 5.00% (2) | 41.20% (7) | 35.0% (14) | 47.10% (8) | 60.00% (24) |
| Ability to discuss practical difficulties | 17.60% (3) | 5.00% (2) | 47.10% (8) | 35.0% (14) | 35.30% (6) | 60.00% (24) |
| Speed of recovery | 11.80% (2) | 5.00% (2) | 47.10% (8) | 52.50% (21) | 41.20% (7) | 42.50% (17) |
| Involvement of family | 25.00% (4) | 17.50% (7) | 43.80% (7) | 50.00% (20) | 31.30% (5) | 32.50% (13) |
| 2020 Sample ^ | 2022 Sample | Test Statistic | |||
|---|---|---|---|---|---|
| Mdn. (IQR) | N | Mdn. (IQR) | N | ||
| Clinicians | N = 23 | N = 16 | |||
| Self-efficacy | 7 (6–8) | 23 | 8 (7.25–8) | 16 | U = 130.50, p = 0.13 |
| Self-efficacy compared to face-to-face | 4 (3–6) | 23 | 4.5 (3–6) | 16 | U = 175.00, p = 0.81 |
| Level of comfort | 4 (3–6) | 23 | 9 (8.25–10) | 16 | U = 18.00, p < 0.001 ** |
| Comfort compared to face-to-face | 4 (3–6) | 23 | 5 (5–7) | 16 | U = 119.50, p = 0.07 |
| Impact of technology on treatment experience | 4 (2–6) | 23 | 5 (2–7.75) | 16 | U = 174.00, p = 0.79 |
| Young People | N = 53 | N = 25 | |||
| Overall experience | 5 (4–6) | 53 | 5 (4–6) | 22 | U = 491.00, p = 0.27 |
| Difficulties understood by therapist | 6 (4.25–7) | 52 | 6 (5–6) | 23 | U = 572.50, p = 0.76 |
| Address important issues | 5 (4–6) | 52 | 6 (5–7) | 23 | U = 446.50, p = 0.07 |
| Impact of technology on treatment experience | 3 (2–4) | 53 | 2 (1–4) | 18 | U = 348.00, p = 0.08 |
| Benefit from online therapy | 5 (3.75–7) | 46 | 6 (4–7) | 15 | U = 305.50, p = 0.50 |
| Parents/Caregivers | N = 75 | N = 49 | |||
| Overall experience | 6 (4.75–7) | 70 | 6 (5–7) | 45 | U = 1565.00, p = 0.95 |
| Difficulties understood by therapist | 7 (6–7) | 70 | 7 (6–7) | 45 | U = 1501.00, p = 0.64 |
| Address important issues | 6 (5–7) | 71 | 7 (6–7) | 45 | U = 1160.50, p = 0.01 * |
| Impact of technology on treatment experience | 7 (5–7) | 58 | 3.5 (1–4) | 42 | U = 420.50, p < 0.001 ** |
| Benefit from online therapy | 7 (5–7) | 58 | 6 (5–7) | 36 | U = 951.50, p = 0.45 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baudinet, J.; Konstantellou, A.; Hambleton, A.; Bialluch, K.; Hurford, G.; Stewart, C.S. Do People Want the ‘New Normal’? A Mixed Method Investigation of Young Person, Parent, and Clinician Experience and Preferences for Eating Disorder Treatment Delivery in the Post-COVID-19 World. Nutrients 2023, 15, 3732. https://doi.org/10.3390/nu15173732
Baudinet J, Konstantellou A, Hambleton A, Bialluch K, Hurford G, Stewart CS. Do People Want the ‘New Normal’? A Mixed Method Investigation of Young Person, Parent, and Clinician Experience and Preferences for Eating Disorder Treatment Delivery in the Post-COVID-19 World. Nutrients. 2023; 15(17):3732. https://doi.org/10.3390/nu15173732
Chicago/Turabian StyleBaudinet, Julian, Anna Konstantellou, Ashlea Hambleton, Katrin Bialluch, Georgina Hurford, and Catherine S. Stewart. 2023. "Do People Want the ‘New Normal’? A Mixed Method Investigation of Young Person, Parent, and Clinician Experience and Preferences for Eating Disorder Treatment Delivery in the Post-COVID-19 World" Nutrients 15, no. 17: 3732. https://doi.org/10.3390/nu15173732
APA StyleBaudinet, J., Konstantellou, A., Hambleton, A., Bialluch, K., Hurford, G., & Stewart, C. S. (2023). Do People Want the ‘New Normal’? A Mixed Method Investigation of Young Person, Parent, and Clinician Experience and Preferences for Eating Disorder Treatment Delivery in the Post-COVID-19 World. Nutrients, 15(17), 3732. https://doi.org/10.3390/nu15173732