
The Effects of Creatine Monohydrate Loading on Exercise Recovery in Active Women throughout the Menstrual Cycle

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
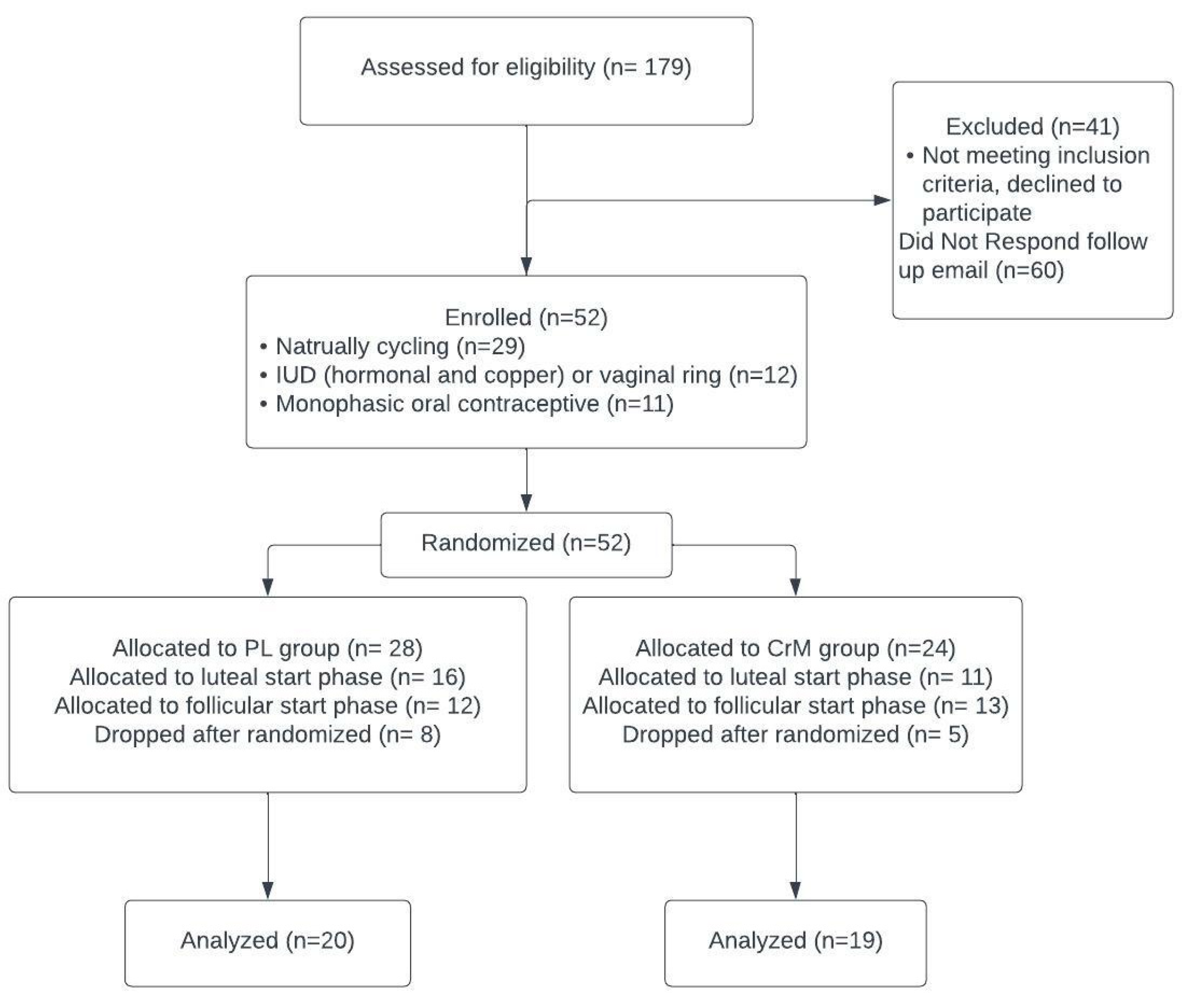
2.1. Subjects
2.2. Experimental Design
2.3. Phase Tracking
2.4. Heart Rate Variability
2.5. Repeated Sprint Ability
2.6. Supplementation
2.7. Dietary Intake
2.8. Statistical Analysis
3. Results
3.1. Estrogen
3.2. Heart Rate Variability (HRV)
3.2.1. Standard Deviation of Normal-to-Normal RR Intervals (SDNN)
3.2.2. Root Mean Square of Successive Differences (RMSSD)
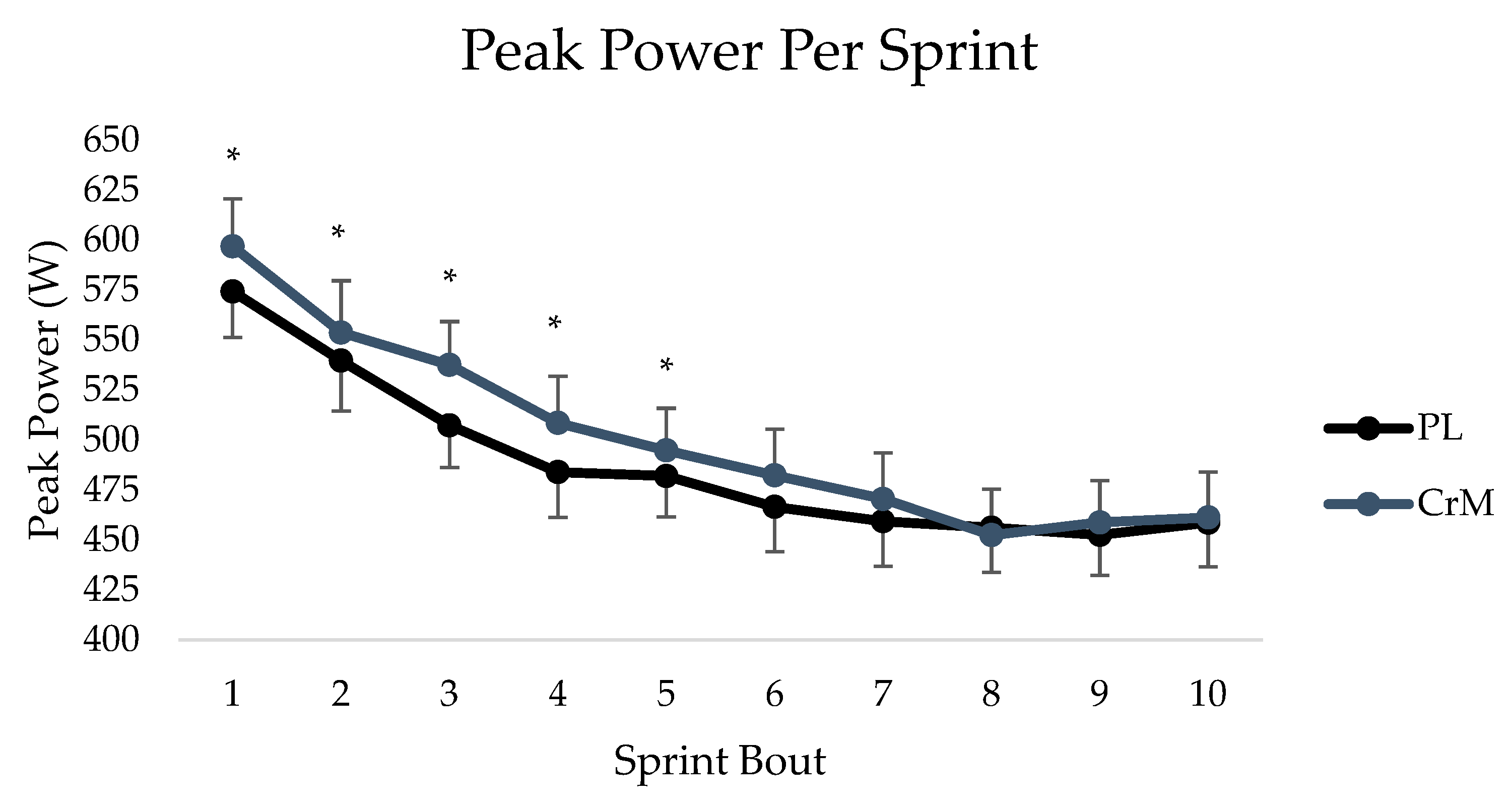
3.3. Exercise Performance
4. Discussion
4.1. Recovery from Exercise
4.2. Resting HRV
4.3. Exercise Performance
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kreider, R.B.; Kalman, D.S.; Antonio, J.; Ziegenfuss, T.N.; Wildman, R.; Collins, R.; Candow, D.G.; Kleiner, S.M.; Almada, A.L.; Lopez, H.L. International Society of Sports Nutrition position stand: Safety and efficacy of creatine supplementation in exercise, sport, and medicine. J. Int. Soc. Sports Nutr. 2017, 14, 18. [Google Scholar] [CrossRef]
- Smith-Ryan, A.E.; Cabre, H.E.; Eckerson, J.M.; Candow, D.G. Creatine supplementation in women’s health: A lifespan perspective. Nutrients 2021, 13, 877. [Google Scholar] [CrossRef] [PubMed]
- Kantor, E.D.; Rehm, C.D.; Du, M.; White, E.; Giovannucci, E.L. Trends in dietary supplement use among US adults from 1999–2012. JAMA J. Am. Med. Assoc. 2016, 316, 1464–1474. [Google Scholar] [CrossRef]
- Bird, S.P. Creatine supplementation and exercise performance: A brief review. J. Sport Sci. Med. 2003, 2, 123–132. [Google Scholar]
- Cooke, W.H.; Grandjean, P.W.; Barnes, W.S. Effect of oral creatine supplementation on power output and fatigue during bicycle ergometry. J. Appl. Physiol. 1995, 78, 670–673. [Google Scholar] [CrossRef] [PubMed]
- Rawson, E.S.; Gunn, B.; Clarkson, P.M. The Effects of Creatine Supplementation on Exercise-Induced Muscle Damage. J. Strength Cond. Res. 2001, 15, 178–184. [Google Scholar] [PubMed]
- Ellery, S.J.; Walker, D.W.; Dickinson, H. Creatine for women: A review of the relationship between creatine and the reproductive cycle and female-specific benefits of creatine therapy. Amino Acids 2016, 48, 1807–1817. [Google Scholar] [CrossRef]
- Deminice, R.; Rosa, F.T.; Franco, G.S.; Jordao, A.A.; de Freitas, E.C. Effects of creatine supplementation on oxidative stress and inflammatory markers after repeated-sprint exercise in humans. Nutrition 2013, 29, 1127–1132. [Google Scholar] [CrossRef]
- Bongiovanni, T.; Genovesi, F.; Nemmer, M.; Carling, C.; Alberti, G.; Howatson, G. Nutritional Interventions for Reducing the Signs and Symptoms of Exercise-Induced Muscle Damage and Accelerate Recovery in Athletes: Current Knowledge, Practical Application and Future Perspectives. Eur. J. Appl. Physiol. 2020, 120, 1965–1996. [Google Scholar] [CrossRef]
- Greenhaff, P.L.; Bodin, K.; Soderlund, K.; Hultman, E. Effect of oral creatine supplementation on skeletal muscle phosphocreatine resynthesis. Am. J. Physiol. Endocrinol. Metab. 1994, 266, E725–E730. [Google Scholar] [CrossRef]
- Kerksick, C.M.; Wilborn, C.D.; Roberts, M.D.; Smith-Ryan, A.; Kleiner, S.M.; Jäger, R.; Kreider, R.B. ISSN exercise & sports nutrition review update: Research & recommend. J. Int. Soc. Sports Nutr. 2018, 15, 38. [Google Scholar] [PubMed]
- Cottrell, G.T.; Coast, J.R.; Herb, R.A. Effect of recovery interval on multiple-bout sprint cycling performance after acute creatine supplementation. J. Strength Cond. Res. 2002, 16, 109–116. [Google Scholar] [PubMed]
- Atakan, M.M.; Karavelioğlu, M.B.; Harmancı, H.; Cook, M.; Bulut, S. Short term creatine loading without weight gain improves sprint, agility and leg strength performance in female futsal players. Sci. Sport 2019, 34, 321–327. [Google Scholar] [CrossRef]
- Javorka, M.; Žila, I.; Balhárek, T.; Javorka, K. Heart rate recovery after exercise: Relations to heart rate variability and complexity. Braz. J. Med. Biol Res. 2002, 35, 991–1000. [Google Scholar] [CrossRef]
- Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Heart rate variability. Standards of measurement, physiological interpretation, and clinical use. Eur. Heart J. 1996, 17, 354–381. [Google Scholar] [CrossRef]
- Cornelissen, V.A.; Verheyden, B.; Aubert, A.E.; Fagard, R.H. Effects of aerobic training intensity on resting, exercise and post-exercise blood pressure, heart rate and heart-rate variability. J. Hum. Hypertens. 2010, 24, 175–182. [Google Scholar] [CrossRef]
- Tenan, M.S.; Brothers, R.M.; Tweedell, A.J.; Hackney, A.C.; Griffin, L. Changes in resting heart rate variability across the menstrual cycle. Psychophysiology 2014, 51, 996–1004. [Google Scholar] [CrossRef]
- Bai, X.; Li, J.; Zhou, L.; Li, X. Influence of the menstrual cycle on nonlinear properties of heart rate variability in young women. Am. J. Physiol. Hearth Circ. Physiol. 2009, 297, H765–H774. [Google Scholar] [CrossRef]
- Brar, T.K.; Singh, K.D.; Kumar, A. Effect of different phases of menstrual cycle on heart rate variability (HRV). J. Clin. Diagn. Res. 2015, 9, CC01–CC04. [Google Scholar] [CrossRef]
- Bergström, R.M. Physiology of the Autonomic Nervous System. Acta Anaesthesiol. Scand. 1964, 8, 17–20. [Google Scholar] [CrossRef]
- Gualano, B.; Roschel, H.; Lancha, A.H.; Brightbill, C.E.; Rawson, E.S. In sickness and in health: The widespread application of creatine supplementation. Amino Acids 2012, 43, 519–529. [Google Scholar] [CrossRef]
- Stout, J.; Eckerson, J.; Ebersole, K.; Moore, G.; Perry, S.; Housh, T.; Batheja, A. Effect of creatine loading on neuromuscular fatigue threshold. J. Appl. Physiol. 2000, 88, 109–112. [Google Scholar] [CrossRef]
- Olsen, S.; Aagaard, P.; Kadi, F.; Tufekovic, G.; Verney, J.; Olesen, J.L.; Kjær, M. Creatine supplementation augments the increase in satellite cell and myonuclei number in human skeletal muscle induced by strength training. J. Physiol. 2006, 573, 525–534. [Google Scholar] [CrossRef]
- Antonio, J.; Candow, D.G.; Forbes, S.C.; Gualano, B.; Jagim, A.R.; Kreider, R.B.; Ziegenfuss, T.N. Common questions and misconceptions about creatine supplementation: What does the scientific evidence really show? J. Int. Soc. Sports Nutr. 2021, 18, 13. [Google Scholar] [CrossRef] [PubMed]
- Vernillo, G.; Agnello, L.; Barbuti, A.; Di Meco, S.; Lombardi, G.; Merati, G.; La Torre, A. Postexercise autonomic function after repeated-sprints training. Eur. J. Appl. Physiol. 2015, 115, 2445–2455. [Google Scholar] [CrossRef] [PubMed]
- Weberruss, H.; Maucher, J.; Oberhoffer, R.; Müller, J. Recovery of the cardiac autonomic nervous and vascular system after maximal cardiopulmonary exercise testing in recreational athletes. Eur. J. Appl. Physiol. 2018, 118, 205–211. [Google Scholar] [CrossRef]
- Hung, C.H.; Clemente, F.M.; Bezerra, P.; Chiu, Y.W.; Chien, C.H.; Crowley-McHattan, Z.; Chen, Y.S. Post-exercise recovery of ultra-short-term heart rate variability after yo-yo intermittent recovery test and repeated sprint ability test. Int. J. Environ. Res. Public Health 2020, 17, 4070. [Google Scholar] [CrossRef] [PubMed]
- Mert, K.U.; Ilgüy, S.; Dural, M.; Mert, G.Ö.; Özakin, E. Effects of creatine supplementation on cardiac autonomic functions in bodybuilders. PACE Pacing Clin. Electrophysiol. 2017, 40, 721–727. [Google Scholar] [CrossRef] [PubMed]
- Sato, N.; Miyake, S.; Akatsu, J.; Kumashiro, M. Power spectral analysis of heart rate variability in healthy young women during the normal menstrual cycle. Psychosom. Med. 1995, 57, 331–335. [Google Scholar] [CrossRef]
- Eckerson, J.M. Creatine as an Ergogenic Aid for Female Athletes. Strength Cond. J. 2016, 38, 14–23. [Google Scholar] [CrossRef]
- Rawson, E.S.; Stec, M.J.; Frederickson, S.J.; Miles, M.P. Low-dose creatine supplementation enhances fatigue resistance in the absence of weight gain. Nutrition 2011, 27, 451–455. [Google Scholar] [CrossRef] [PubMed]
- Gotshalk, L.A.; Kraemer, W.J.; Mendonca, M.A.G.; Vingren, J.L.; Kenny, A.M.; Spiering, B.A.; Hatfield, D.L.; Fragala, M.S.; Volek, J.S. Creatine supplementation improves muscular performance in older women. Eur. J. Appl. Physiol. 2007, 102, 223–231. [Google Scholar] [CrossRef] [PubMed]
- Eckerson, J.M.; Stout, J.R.; Moore, G.A.; Stone, N.J.; Nishimura, K.; Tamura, K. Effect of Two and Five Days of Creatine Loading on Anaerobic Working Capacity in Women. Strength Cond. 2004, 18, 618–624. [Google Scholar]
- Moore, S.R.; Gordon, A.N.; Cabre, H.E.; Hackney, A.C.; Smith-Ryan, A.E. A randomized controlled trial of changes in fluid distribution across menstrual phases with creatine supplementation. Nutrients 2023, 15, 429. [Google Scholar] [CrossRef]
- Giacomoni, M.; Bernard, T.; Gavarry, O.; Altare, S.; Falgairette, G. Influence of the menstrual cycle phase and menstrual symptoms on maximal anaerobic performance. Med. Sci. Sports Exerc. 2000, 32, 486–492. [Google Scholar] [CrossRef] [PubMed]
- Tsampoukos, A.; Peckham, E.A.; James, R.; Nevill, M.E. Effect of menstrual cycle phase on sprinting performance. Eur. J. Appl. Physiol. 2010, 109, 659–667. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Supplement Group | Age (y) | Height (cm) | Weight (kg) | BMI (kg/m2) | Percent Body Fat (%) | Estimated VO2 Max (mL/kg/min) | Average Cycle Length (days) |
|---|---|---|---|---|---|---|---|
| CrM (n = 19) | 25.5 ± 7.2 | 164.6 ± 6.1 | 66.2 ± 9.2 | 23.0 ± 5.0 | 26.9 ± 6.1 | 38.3 ± 7.3 | 28.9 ± 4.6 |
| PL (n = 20) | 23.8 ± 4.3 | 167.0 ± 4.8 | 64.1 ± 7.0 | 24.4 ± 2.9 | 27.9 ± 5.7 | 39.7 ± 4.6 | 28.1 ± 5.8 |
| Creatine (n = 19) | Placebo (n = 20) | |||||||
|---|---|---|---|---|---|---|---|---|
| Follicular Pre | Follicular Post | Luteal Pre | Luteal Post | Follicular Pre | Follicular Post | Luteal Pre | Luteal Post | |
| SDNN | ||||||||
| Resting (ms) | 120.6 ± 7.4 | 120.1 ± 7.4 | 112.6 ± 7.4 | 103.3 ± 7.8 | 114.6 ± 7.2 | 110.3 ± 7.2 | 113.7 ± 7.2 | 103.3 ± 7.8 |
| Average Recovery (ms) | 41.4 ± 3.0 | 39.4 ± 2.6 | 37.0 ± 0.0 | 33.7 ± 2.4 | 47.0 ± 2.9 | 48.0 ± 2.5 | 41.6 ± 2.9 | 44.4 ± 2.3 |
| 5 min Post-Exercise (ms) | 78.0 ± 6.0 | 73.6 ± 5.2 | 65.1 ± 5.1 | 60.1 ± 4.8 | 77.9 ± 5.8 | 80.4 ± 5.1 | 70.0 ± 5.0 | 74.0 ± 4.7 |
| RMSSD | ||||||||
| Resting (ms) | 98.9 ± 7.3 | 93.1 ± 8.1 | 87.9 ± 8.1 | 75.5 ± 8.1 | 87.3 ± 7.1 | 84.6 ± 7.9 | 81.2 ± 7.9 | 80.5 ± 7.9 |
| Average Recovery (ms) | 12.2 ± 3.0 | 12.6 ± 2.7 | 12.0 ± 3.4 | 8.4 ± 2.1 | 16.1 ± 2.9 | 15.8 ± 2.6 | 15.6 ± 3.3 | 15.0 ± 2.0 |
| 5 min Post-Exercise (ms) | 17.2 ± 4.0 | 16.3 ± 3.9 | 11.8 ± 3.2 | 9.4 ± 2.4 | 16.2 ± 3.8 | 15.6 ± 3.8 | 16.0 ± 3.1 | 14.9 ± 2.3 |
| Creatine (n = 19) | Placebo (n = 20) | |||||||
|---|---|---|---|---|---|---|---|---|
| Follicular Pre | Follicular Post | Luteal Pre | Luteal Post | Follicular Pre | Follicular Post | Luteal Pre | Luteal Post | |
| Total Average Power (W) | 3160.5 ± 246.5 | 5116.5 ± 5 | 2372.5 ± 319.0 | 2553.3 ± 336.8 | 2874.2 ± 241.2 | 2835 ± 1190.7 | 2845.4 ± 310.9 | 3017.2 ± 328.3 |
| Fatigue Index(%) | 29.2 ± 2.6 | 30.3 ± 2.6 | 37.9 ± 4.7 | 30.3 ± 3.5 * | 27.5 ± 2.4 | 23.8 ± 2.6 | 27.6 ± 4.4 | 27.3 ± 3.3 |
| Peak Power (W) | 492.9 ± 21.9 | 508.1 ± 21.7 | 484.8 ± 25.0 | 520.6 ± 22.1 | 484.0 ± 21.2 | 488.8 ± 20.4 | 484.5 ± 24.1 | 494.6 ± 21.4 |
| Time to Peak Power (ms) | 1663.5 ± 181.6 | 2265.6 ± 207.3 | 1937.1 ± 159.7 | 2141.2 ± 239.0 | 1782.5 ± 175.5 | 2269.7 ± 200.2 | 2001.7 ± 154.3 | 2310.9 ± 230.9 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gordon, A.N.; Moore, S.R.; Patterson, N.D.; Hostetter, M.E.; Cabre, H.E.; Hirsch, K.R.; Hackney, A.C.; Smith-Ryan, A.E. The Effects of Creatine Monohydrate Loading on Exercise Recovery in Active Women throughout the Menstrual Cycle. Nutrients 2023, 15, 3567. https://doi.org/10.3390/nu15163567
Gordon AN, Moore SR, Patterson ND, Hostetter ME, Cabre HE, Hirsch KR, Hackney AC, Smith-Ryan AE. The Effects of Creatine Monohydrate Loading on Exercise Recovery in Active Women throughout the Menstrual Cycle. Nutrients. 2023; 15(16):3567. https://doi.org/10.3390/nu15163567
Chicago/Turabian StyleGordon, Amanda N., Sam R. Moore, Noah D. Patterson, Maggie E. Hostetter, Hannah E. Cabre, Katie R. Hirsch, Anthony C. Hackney, and Abbie E. Smith-Ryan. 2023. "The Effects of Creatine Monohydrate Loading on Exercise Recovery in Active Women throughout the Menstrual Cycle" Nutrients 15, no. 16: 3567. https://doi.org/10.3390/nu15163567
APA StyleGordon, A. N., Moore, S. R., Patterson, N. D., Hostetter, M. E., Cabre, H. E., Hirsch, K. R., Hackney, A. C., & Smith-Ryan, A. E. (2023). The Effects of Creatine Monohydrate Loading on Exercise Recovery in Active Women throughout the Menstrual Cycle. Nutrients, 15(16), 3567. https://doi.org/10.3390/nu15163567