
Interaction of Passive Smoking and Diet Habits on Vitamin D Deficiency among Women of Reproductive Age in Rural Central China

Abstract
1. Introduction
2. Methods
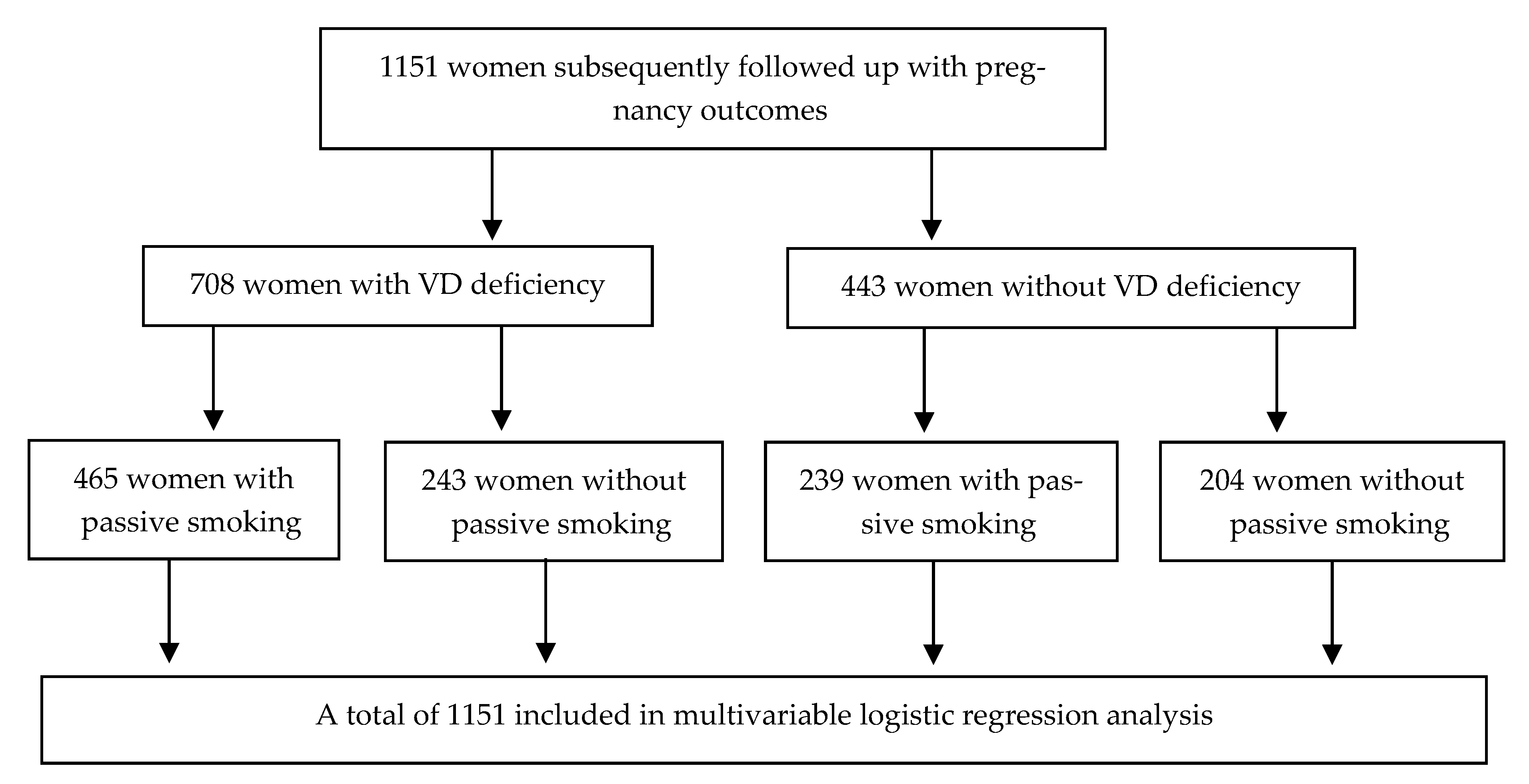
2.1. Study Design and Population
2.2. Collection of Data and Blood Sample
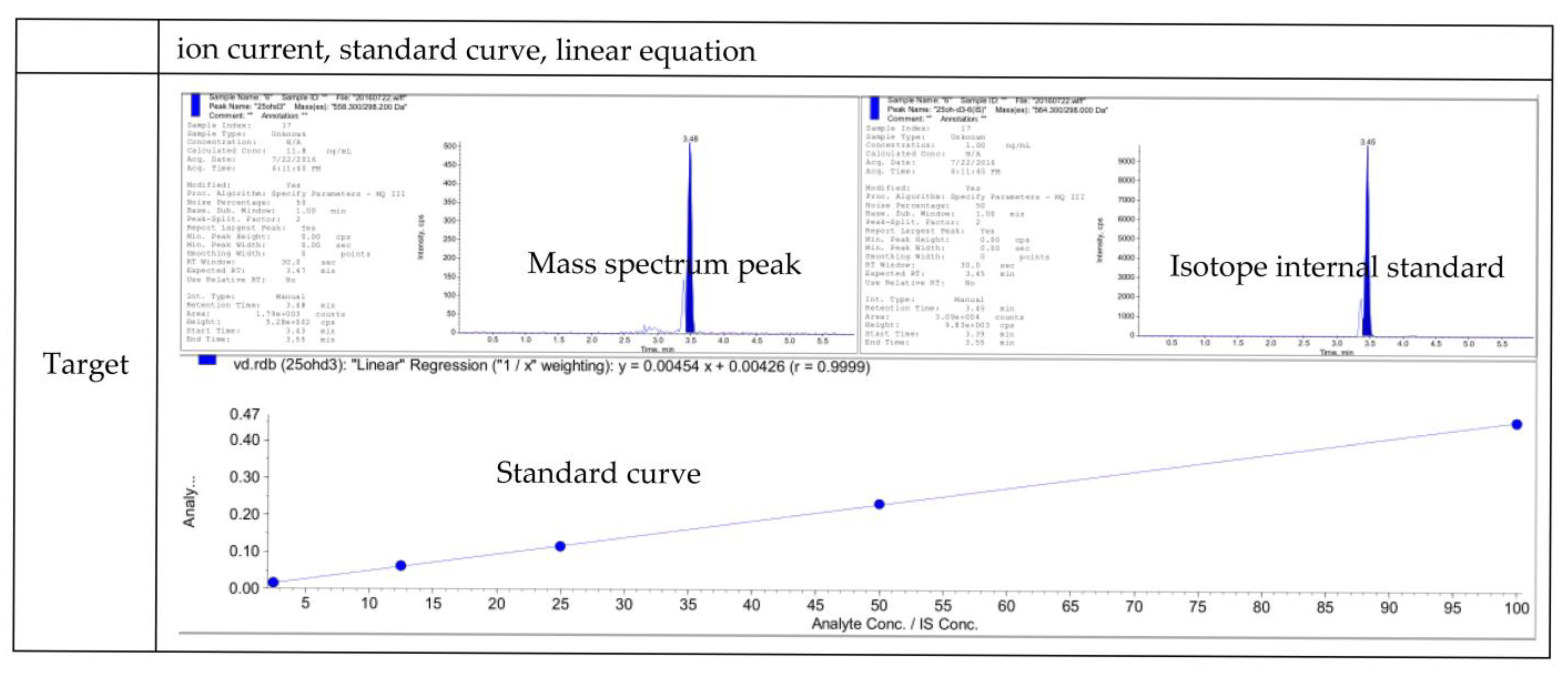
2.3. Measurement of Vitamin D
2.4. Definitions of Nutritional Supplementation and Passive Smoking
2.5. Statistical Analysis
3. Results
3.1. Distribution of Vitamin D Deficiency among Women of Reproductive Age in Rural Central China
3.2. The Risk of Vitamin D Deficiency by Multivariable Logistic Regression Analysis
3.3. Interaction between Passive Smoking and Inadequate Nutrition on the Risk of Vitamin D Deficiency
4. Discussion
4.1. Factors Influencing Vitamin D and Their Interaction
4.2. Strengths and Limitations
4.3. Suggestions Based on Research Findings
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hossein, A. Vitamin D for Health: A Global Perspective—Mayo Clinic Proceedings. Mayo Clin. Proc. 2013, 88, 720–755. [Google Scholar] [CrossRef] [PubMed]
- Bischoff-Ferrari, H.A. Vitamin D—Role in Pregnancy and Early Childhood. Ann. Nutr. Metab. 2011, 59, 17–21. [Google Scholar] [CrossRef] [PubMed]
- Ginde, A.A.; Sullivan, A.F.; Mansbach, J.M.; Camargo, C.A., Jr. Vitamin D insufficiency in pregnant and nonpregnant women of reproductive age in the United States. Am. J. Obstet. Gynecol. 2010, 202, 431–436. [Google Scholar] [CrossRef] [PubMed]
- Lips, P. Worldwide status of vitamin D nutrition. J. Steroid Biochem. Mol. Biol. 2010, 121, 297–300. [Google Scholar] [CrossRef] [PubMed]
- Lamberg-Allardt, C.J.; Outila, T.A.; Karkkainen, M.U.; Rita, H.J.; Valsta, L.M. Vitamin D deficiency and bone health in healthy adults in Finland: Could this be a concern in other parts of Europe? J. Bone Miner. Res. 2010, 16, 2066–2073. [Google Scholar] [CrossRef]
- Lopes, V.M.; Lopes, J.R.; Brasileiro, J.P.; Oliveira, I.; Lacerda, R.P.; Andrade, M.R.; Tierno, N.I.; Souza, R.C.; Motta, L.A. Highly prevalence of vitamin D deficiency among Brazilian women of reproductive age. Arch. Endocrinol. Metab. 2017, 61, 21–27. [Google Scholar] [CrossRef]
- Md Zahirul, I.; Mohammed, A.; Christel, L.A. Hypovitaminosis D is common in both veiled and nonveiled Bangladeshi women. Asia Pac. J. Clin. Nutr. 2006, 15, 81. [Google Scholar]
- Sachan, A.; Gupta, R.; Das, V.; Agarwal, A.; Awasthi, P.K.; Bhatia, V. High prevalence of vitamin D deficiency among pregnant women and their newborns in northern India. Am. J. Clin. Nutr. 2005, 81, 1060–1064. [Google Scholar] [CrossRef]
- Zhao, Y.; Zhao, W.; Hao, Q.; Ge, M.; Zhang, Y.; Hu, F.; Lu, Y.; Zhou, L.; Liu, X.; Dong, B. Vitamin D status and obesity markers in older adults: Results from West China Health and Aging Trends study. BMC Geriatr. 2021, 21, 528. [Google Scholar] [CrossRef]
- Yan, X.; Zhang, N.; Cheng, S.; Wang, Z.; Qin, Y. Gender Differences in Vitamin D Status in China. Med. Sci. Monit. 2019, 25, 7094–7099. [Google Scholar] [CrossRef]
- Yang, C.; Jing, W.; Ge, S.; Sun, W. Vitamin D status and vitamin D deficiency risk factors among pregnancy of Shanghai in China. BMC Pregnancy Childbirth 2021, 21, 431. [Google Scholar] [CrossRef]
- Palacios, C.; Gonzalez, L. Is vitamin D deficiency a major global public health problem? J. Steroid Biochem. Mol. Biol. 2014, 144 (Pt A), 138–145. [Google Scholar] [CrossRef]
- Thandrayen, K.; Pettifor, J.M. Maternal vitamin D status: Implications for the development of infantile nutritional rickets. Rheum Dis. Clin. N. Am. 2012, 38, 61–79. [Google Scholar] [CrossRef]
- Le Goaziou, M.F.; Contardo, G.; Dupraz, C.; Martin, A.; Laville, M.; Schott-Pethelaz, A.M. Risk factors for vitamin D deficiency in women aged 20–50 years consulting in general practice: A cross-sectional study. Eur. J. Gen. Pract. 2011, 17, 146–152. [Google Scholar] [CrossRef]
- Visser, J.; Knight, K.; Philips, L.; Visser, W.; Wallace, M.; Blaauw, R. Determinants of serum 25-hydroxyvitamin D levels in healthy young adults living in the western cape, South Africa. Clin. Nutr. 2018, 37, S284. [Google Scholar] [CrossRef]
- Serrao Cabral, M.M.; Bos, A.J.G.; Amano, H.; Seino, S.; Shinkai, S. Relationship between skin color, sun exposure, UV protection, fish intake and serum levels of vitamin D in Japanese older adults. Nutr. Food Sci. 2017, 47, 409–422. [Google Scholar] [CrossRef]
- Jungert, A.; Spinneker, A.; Nagel, A.; Neuhauser-Berthold, M. Dietary intake and main food sources of vitamin D as a function of age, sex, vitamin D status, body composition, and income in an elderly German cohort. Food Nutr. Res. 2014, 58, 23632. [Google Scholar] [CrossRef]
- Kühn, T.; Kaaks, R.; Teucher, B.; Hirche, F.; Dierkes, J.; Weikert, C.; Katzke, V.; Boeing, H.; Stangl, G.I.; Buijsse, B. Dietary, lifestyle, and genetic determinants of vitamin D status: A cross-sectional analysis from the European Prospective Investigation into Cancer and Nutrition (EPIC)-Germany study. Eur. J. Nutr. 2014, 53, 731–741. [Google Scholar] [CrossRef]
- Iolanda, C.; Michele, P.; Marco, S.; Giulia, P.; Giovanna, T.; Boner, A.L. Correlation between Vitamin D serum levels and passive smoking exposure in children with asthma. Allergy Asthma Proc. 2018, 39, 8–14. [Google Scholar]
- Alsharairi, N.A. Diet and Food Allergy as Risk Factors for Asthma in the Arabian Gulf Region: Current Evidence and Future Research Needs. Int. J. Environ. Res. Public Health 2019, 16, 3852. [Google Scholar] [CrossRef]
- Dwarkanath, P.; Vinotha, P.; Thomas, T.; Joseph, S.; Thomas, A.; Shirley, G.; Sheela, C.N.; Mehta, S.; Kurpad, A.V. Relationship of Early Vitamin D Concentrations and Gestational Diabetes Mellitus in Indian Pregnant Women. Front. Nutr. 2019, 6, 116. [Google Scholar] [CrossRef] [PubMed]
- Hyppönen, E.; Cavadino, A.; Williams, D.; Fraser, A.; Vereczkey, A.; Fraser, W.D.; Bánhidy, F.; Lawlor, D.; Czeizel, A.E. Vitamin D and Pre-Eclampsia: Original Data, Systematic Review and Meta-Analysis. Ann. Nutr. Metab. 2014, 63, 331–340. [Google Scholar] [CrossRef] [PubMed]
- Maysa, A.; Wood, R.J. Vitamin D and gestational diabetes mellitus. Nutr. Rev. 2013, 71, 158–167. [Google Scholar]
- Agarwal, R.; Virmani, D.; Jaipal, M.L.; Gupta, S.; Gupta, N.; Sankar, M.J.; Bhatia, S.; Agarwal, A.; Devgan, V.; Deorari, A.; et al. Vitamin D Status of Low Birth Weight Infants in Delhi: A Comparative Study. J. Trop. Pediatr. 2012, 58, 446–450. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Liu, M.; Yu, P.; Jian, L.; Li, C. Low levels of serum 25-hydroxyvitamin D and risk of metabolic syndrome in China. Int. J. Clin. Exp. Med. 2015, 8, 13790–13796. [Google Scholar]
- Xiao, Y.; Wei, L.; Xiong, X.; Yang, M.; Sun, L. Association Between Vitamin D Status and Diabetic Complications in Patients With Type 2 Diabetes Mellitus: A Cross-Sectional Study in Hunan China. Front. Endocrinol. 2020, 11, 564738. [Google Scholar] [CrossRef]
- Zhang, Y.Y.; Qiu, H.B.; Tian, J.W. Association Between Vitamin D and Hyperuricemia Among Adults in the United States. Front. Nutr. 2020, 7, 592777. [Google Scholar] [CrossRef]
- Jiang, X.; Peng, M.; Chen, S.; Wu, S.; Zhang, W. Vitamin D deficiency is associated with dyslipidemia: A cross-sectional study in 3788 subjects. Curr. Med. Res. Opin. 2019, 35, 1059–1063. [Google Scholar] [CrossRef]
- Lin, S.; Jiang, L.; Zhang, Y.; Chai, J.; Pei, L. Socioeconomic status and vitamin D deficiency among women of reproductive age: A population-based, case–control study in rural northern China. BMJ Open 2021, 11, e42227. [Google Scholar] [CrossRef]
- Lin, S.; Zhang, Y.; Jiang, L.; Li, J.; Chai, J.; Pei, L.; Shang, X. Interactive Effects of Maternal Vitamin D Status and Socio-Economic Status on the Risk of Spontaneous Abortion: Evidence from Henan Province, China. Nutrients 2022, 14, 291. [Google Scholar] [CrossRef]
- Liao, X.; Zhang, Z.; Zhang, H.; Zhu, H.; Zhou, J.; Huang, Q.; Wang, Z.; Wang, L.; Liu, Z. Application guideline for vitamin D and bone health in adult Chinese (2014 Starter Edition). Chin. J. Osteoporos. 2014, 20, 1011–1030. [Google Scholar]
- WHO. Guidelines for the Conduct of Tobacco Smoking Surveys of the General Population; WHO: Geneva, Switzerland, 1983. [Google Scholar]
- Wang, M.; Luo, X.; Xu, S.; Liu, W.; Ding, F.; Zhang, X.; Wang, L.; Liu, J.; Hu, J.; Wang, W. Trends in smoking prevalence and implication for chronic diseases in China: Serial national cross-sectional surveys from 2003 to 2013. Lancet Respir Med. 2019, 7, 35–45. [Google Scholar] [CrossRef]
- Morabia, A.; Bernstein, M.S.; Antonini, S. Smoking, dietary calcium and vitamin D deficiency in women: A population-based study. Eur. J. Clin. Nutr. 2000, 54, 684–689. [Google Scholar] [CrossRef]
- Zia, S.; Ndoye, A.; Nguyen, V.T.; Grando, S.A. Nicotine enhances expression of the alpha 3, alpha 4, alpha 5, and alpha 7 nicotinic receptors modulating calcium metabolism and regulating adhesion and motility of respiratory epithelial cells. Res. Commun. Mol. Pathol. Pharmacol. 1997, 97, 243–262. [Google Scholar]
- Thieden, E.; Philipsen, P.A.; Heydenreich, J.; Wulf, H.C. Vitamin D level in summer and winter related to measured UVR exposure and behavior. Photochem. Photobiol. 2009, 85, 1480–1484. [Google Scholar] [CrossRef]
- Aghajafari, F.; Nagulesapillai, T.; Ronksley, P.E.; Tough, S.C.; O’Beirne, M.; Rabi, D.M. Association between maternal serum 25-hydroxyvitamin D level and pregnancy and neonatal outcomes: Systematic review and meta-analysis of observational studies. BMJ 2013, 346, f1169. [Google Scholar] [CrossRef]
- Karras, S.N.; Fakhoury, H.; Muscogiuri, G.; Grant, W.B.; van den Ouweland, J.M.; Colao, A.M.; Kotsa, K. Maternal vitamin D levels during pregnancy and neonatal health: Evidence to date and clinical implications. Ther. Adv. Musculoskelet. Dis. 2016, 8, 124–135. [Google Scholar] [CrossRef]
- Chen, Y.H.; Fu, L.; Hao, J.H.; Yu, Z.; Zhu, P.; Wang, H.; Xu, Y.Y.; Zhang, C.; Tao, F.B.; Xu, D.X. Maternal vitamin D deficiency during pregnancy elevates the risks of small for gestational age and low birth weight infants in Chinese population. J. Clin. Endocrinol. Metab. 2015, 100, 1912–1919. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Demographic Characteristics and Socioeconomic Status | VD Deficiency (n = 708) | VD Sufficiency (n = 443) | χ2 | p | ||
|---|---|---|---|---|---|---|
| n | % | n | % | |||
| Age | ||||||
| <25 | 214 | 30.23 | 145 | 32.73 | 2.641 | 0.267 |
| 25– | 279 | 39.41 | 183 | 41.31 | ||
| 30– | 215 | 30.37 | 115 | 25.96 | ||
| Ethnicity | ||||||
| Han | 693 | 97.88 | 434 | 97.97 | 0.010 | 0.920 |
| Minority | 15 | 2.12 | 9 | 2.03 | ||
| Education | ||||||
| Primary school or below | 58 | 8.19 | 22 | 4.97 | 12.268 | 0.002 |
| Junior middle school | 482 | 68.08 | 278 | 62.75 | ||
| High school or above | 168 | 23.73 | 142 | 32.13 | ||
| Occupation | ||||||
| Enterprises | 32 | 4.52 | 30 | 6.77 | 3.091 | 0.378 |
| Business or service | 64 | 9.04 | 39 | 8.80 | ||
| Agriculture or industry | 99 | 13.98 | 55 | 12.42 | ||
| Housework | 513 | 72.46 | 319 | 72.01 | ||
| Family annual income(Yuan) 1 | ||||||
| <5000 | 51 | 7.20 | 9 | 2.03 | 31.694 | <0.001 |
| 5000– | 260 | 36.72 | 120 | 27.09 | ||
| 10,000– | 395 | 55.95 | 314 | 70.88 | ||
| Exposure Factor | VD Deficiency | VD Sufficiency | χ2 | p | ||
|---|---|---|---|---|---|---|
| (n = 708) | (n = 443) | |||||
| n | % | n | % | |||
| BMI | ||||||
| <18.5 | 42 | 5.93 | 34 | 7.67 | 2.629 | 0.453 |
| 18.5– | 425 | 60.03 | 272 | 61.4 | ||
| 24– | 171 | 24.15 | 102 | 23.02 | ||
| 28– | 68 | 9.6 | 34 | 7.67 | ||
| Gravidity | ||||||
| 0 | 165 | 23.37 | 136 | 31.41 | 23.733 | <0.001 |
| 1 | 258 | 36.54 | 191 | 44.11 | ||
| ≥2 | 283 | 40.08 | 116 | 26.79 | ||
| History of chronic diseases 1 | ||||||
| Yes | 33 | 4.66 | 18 | 4.06 | 0.235 | 0.628 |
| No | 674 | 95.2 | 425 | 95.94 | ||
| Passive smoking | ||||||
| Yes | 465 | 65.68 | 239 | 53.95 | 15.778 | <0.001 |
| No | 243 | 34.32 | 204 | 46.05 | ||
| Alcohol consumption | ||||||
| Yes | 12 | 1.69 | 6 | 1.35 | 0.205 | 0.651 |
| No | 696 | 98.31 | 437 | 98.65 | ||
| Nutritional supplement | ||||||
| Yes | 149 | 21.05 | 155 | 34.99 | 27.258 | <0.001 |
| No | 559 | 78.95 | 288 | 65.01 | ||
| Fresh meat intake | ||||||
| ≥4 times per week | 77 | 10.89 | 59 | 13.32 | 3.370 | 0.185 |
| 1–3 times per week | 307 | 43.42 | 204 | 46.05 | ||
| ≤3 times per month | 323 | 45.68 | 180 | 40.63 | ||
| Fish and shrimp intake | ||||||
| ≥1 time per week | 48 | 6.79 | 31 | 7 | 4.572 | 0.102 |
| 1–3 times per month | 84 | 11.88 | 72 | 16.25 | ||
| Rarely | 575 | 81.33 | 340 | 76.75 | ||
| Egg intake | ||||||
| Everyday | 191 | 27.02 | 163 | 36.79 | 25.776 | <0.001 |
| 4–6 times per week | 158 | 22.35 | 123 | 27.77 | ||
| ≤3 times per week | 358 | 35.44 | 157 | 50.61 | ||
| Milk or dairy products intake | ||||||
| ≥4 times per week | 113 | 15.98 | 94 | 21.22 | 6.309 | 0.043 |
| ≥1 time per month | 226 | 32 | 120 | 21.09 | ||
| Almost never | 368 | 52.05 | 229 | 51.69 | ||
| Beans and soy products intake | ||||||
| Everyday | 171 | 24.19 | 119 | 26.86 | 6.677 | 0.083 |
| 4–6 times per week | 130 | 18.39 | 100 | 22.57 | ||
| 1–3 times per week | 188 | 26.59 | 114 | 25.73 | ||
| ≤3 times per month | 218 | 30.83 | 110 | 24.83 | ||
| Vegetables and fruits intake | ||||||
| Everyday | 548 | 77.51 | 346 | 78.1 | 1.063 | 0.588 |
| 4–6 times per week | 100 | 14.14 | 67 | 15.12 | ||
| ≤3 times per week | 59 | 8.35 | 30 | 6.77 | ||
| Factor | β | S.E. | Wald | Sig | OR (95% CI) |
|---|---|---|---|---|---|
| Education | |||||
| High school or above | 2.816 | 0.245 | 1.00 | ||
| Junior middle school | 0.444 | 0.291 | 2.327 | 0.127 | 1.60 (0.88–2.76) |
| Primary school or below | 0.175 | 0.145 | 1.443 | 0.230 | 1.19 (0.90–1.58) |
| Family annual income (Yuan) | |||||
| <5000 | 1.406 | 0.382 | 13.567 | <0.001 | 4.08 (1.93–8.62) |
| 5000– | 0.454 | 0.143 | 10.144 | 0.001 | 1.58 (1.19–2.08) |
| ≥10,000 | 20.825 | <0.001 | 1.00 | ||
| Gravidity | |||||
| 0 | 16.967 | <0.001 | 1.00 | ||
| 1 | 0.070 | 0.158 | 0.200 | 0.655 | 1.07 (0.79–1.46) |
| ≥2 | 0.613 | 0.168 | 13.261 | <0.001 | 1.85 (1.33–2.57) |
| Passive smoking | |||||
| No | 1.00 | ||||
| Yes | 0.505 | 0.130 | 14.982 | <0.001 | 1.66 (1.28–2.14) |
| Nutritional supplementation | |||||
| No | 1.00 | ||||
| Yes | −0.670 | 0.145 | 21.234 | <0.001 | 0.51 (0.39–0.68) |
| Egg intake | |||||
| Everyday | 12.731 | 0.002 | 1.00 | ||
| 4–6 times per week | 0.101 | 0.172 | 0.345 | 0.557 | 1.11 (0.79–1.55) |
| <3 times per week | 0.522 | 0.156 | 11.171 | 0.001 | 1.69 (1.24–2.29) |
| Milk or dairy products intake | |||||
| ≥4 times per week | 3.298 | 0.192 | 1.00 | ||
| ≥1 time per month | 0.140 | 0.197 | 0.505 | 0.477 | 1.15 (0.78–1.69) |
| Almost never | −0.138 | 0.180 | 0.581 | 0.446 | 0.87 (0.61–1.24) |
| VD Deficiency | VD Sufficiency | OR (95% CI) | Regression Coefficient | Interactive Coefficient | ||
|---|---|---|---|---|---|---|
| (n = 708) | (n = 443) | |||||
| Model 1 | ||||||
| Passive smoking | Nutritional supplementation | |||||
| No | Yes | 52 | 77 | 1.00 | ||
| No | No | 191 | 127 | 2.20 (1.43–3.39) * | 0.788 | - |
| Yes | Yes | 97 | 78 | 1.94 (1.20–3.12) * | 0.661 | - |
| Yes | No | 368 | 161 | 3.40 (2.26–5.13) * | 1.224 | 2.35 |
| Model 2 | ||||||
| Passive smoking | Egg intake(≥4 times per week) | |||||
| No | Yes | 115 | 134 | 1.00 | ||
| No | No | 127 | 70 | 1.89 (1.28–2.81) * | 0.638 | - |
| Yes | Yes | 234 | 152 | 1.81 (1.30–2.51) * | 0.592 | - |
| Yes | No | 231 | 87 | 2.87 (2.00–4.10) * | 1.052 | 2.79 |
| Model 3 | ||||||
| Passive smoking | Milk or dairy products intake (≥4 times per week) | |||||
| No | Yes | 34 | 42 | 1.00 | ||
| No | No | 208 | 162 | 1.32(0.79–2.20) | 0.278 | - |
| Yes | Yes | 79 | 52 | 1.83 (1.02–3.28) * | 0.606 | - |
| Yes | No | 386 | 187 | 2.18 (1.33–3.58) * | 0.781 | 1.70 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, Y.; Lin, S.; Li, J.; Song, X.; Chen, G.; Pei, L. Interaction of Passive Smoking and Diet Habits on Vitamin D Deficiency among Women of Reproductive Age in Rural Central China. Nutrients 2023, 15, 126. https://doi.org/10.3390/nu15010126
Zhang Y, Lin S, Li J, Song X, Chen G, Pei L. Interaction of Passive Smoking and Diet Habits on Vitamin D Deficiency among Women of Reproductive Age in Rural Central China. Nutrients. 2023; 15(1):126. https://doi.org/10.3390/nu15010126
Chicago/Turabian StyleZhang, Yuan, Shiqi Lin, Jiajia Li, Xinming Song, Gong Chen, and Lijun Pei. 2023. "Interaction of Passive Smoking and Diet Habits on Vitamin D Deficiency among Women of Reproductive Age in Rural Central China" Nutrients 15, no. 1: 126. https://doi.org/10.3390/nu15010126
APA StyleZhang, Y., Lin, S., Li, J., Song, X., Chen, G., & Pei, L. (2023). Interaction of Passive Smoking and Diet Habits on Vitamin D Deficiency among Women of Reproductive Age in Rural Central China. Nutrients, 15(1), 126. https://doi.org/10.3390/nu15010126