
The Association of Soft Drink Consumption and the 24-Hour Movement Guidelines with Suicidality among Adolescents of the United States



Abstract
:1. Introduction
2. Methods
2.1. Design and Participants
2.2. Independent Variables
2.2.1. Soft Drink Consumption
2.2.2. The Recommendations of the 24 h Movement Guidelines
2.3. Dependent Variables
2.4. Covariates
2.4.1. Demographic Factors
2.4.2. Weight Status
2.4.3. Dietary Behaviors
2.4.4. Depressive Symptoms
2.5. Statistical Analysis
3. Results
3.1. Characteristics of Included Participants
3.2. The Weighted Prevalence of Suicidality by the Recommendations of the 24 h Movement Guidelines and Levels of Soft Drink Consumption
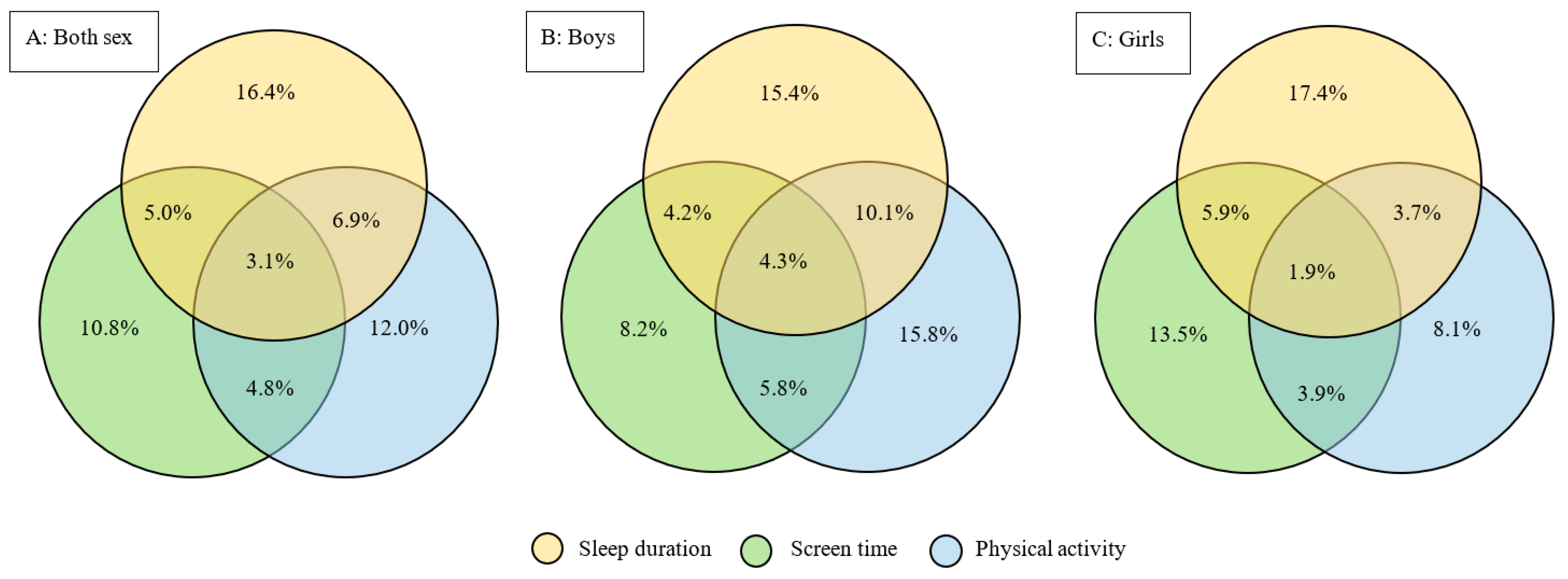
3.3. The Weighted Prevalence of Meeting the Recommendations of the 24 h Movement Guidelines
3.4. The Association of the 24 h Movement Guidelines and Soft Drink Consumption with Suicidality
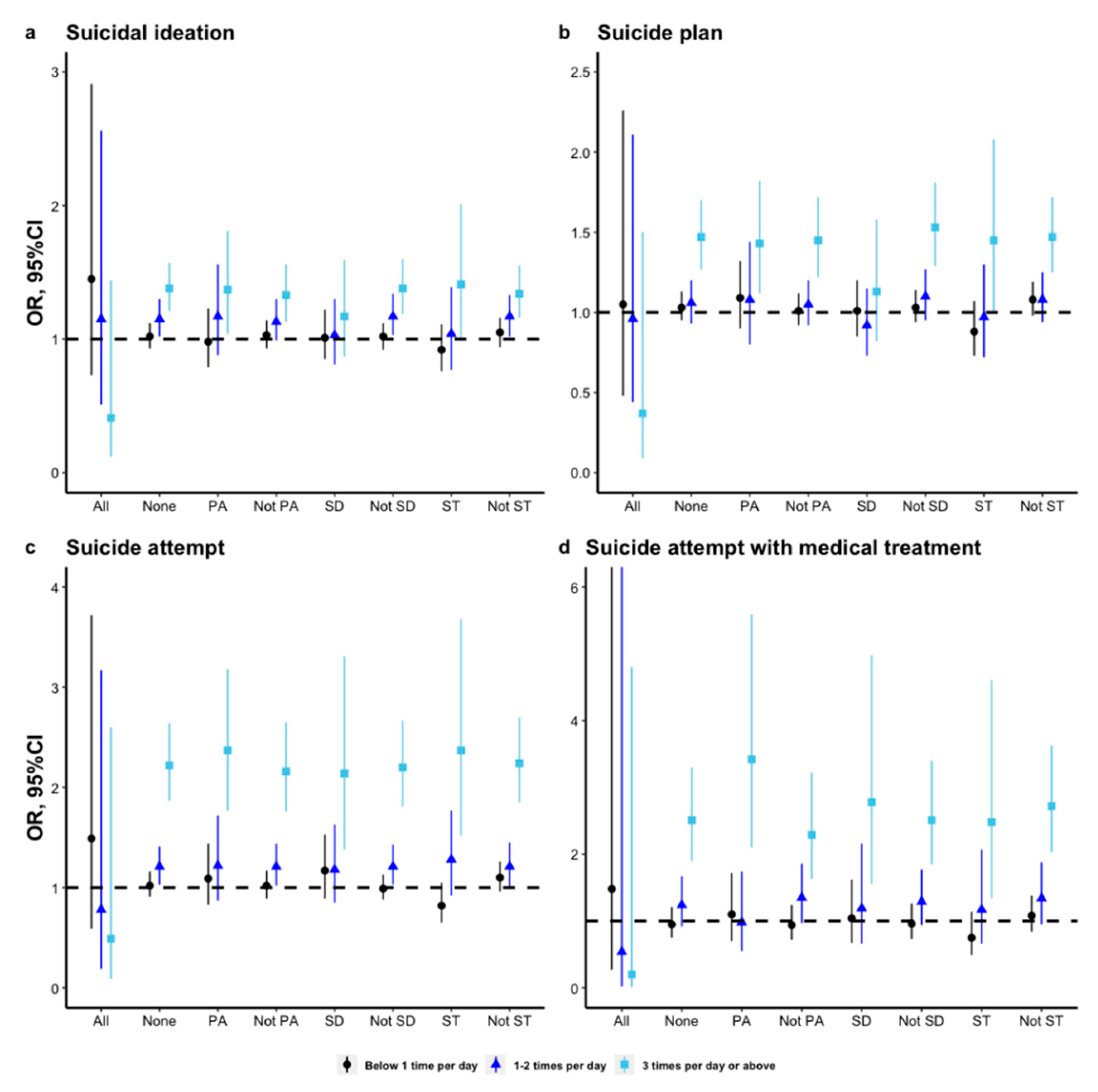
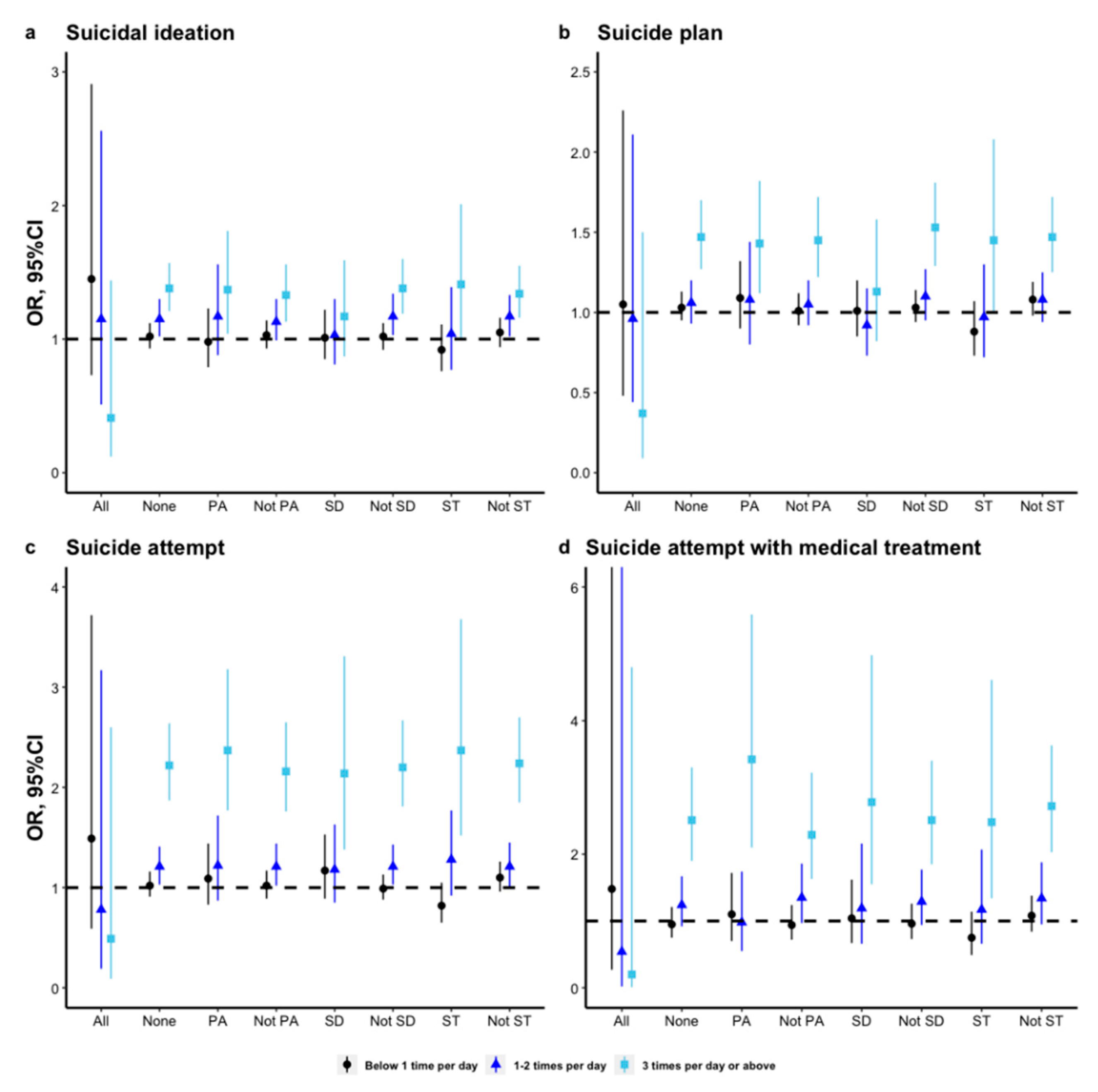
3.5. Subgroup Analyses of the Association between Soft Drink Consumption and Suicidality by Different Recommendations of the 24 h Movement Guidelines
3.6. Sensitivity Analysis
4. Discussions
4.1. Recommendations of the 24 h Movement Guidelines and Suicidality
4.2. Soft Drink Consumption and Suicidality
4.3. Interactive Association of the 24 h Movement Guidelines and Soft Drink Consumption with Suicidality
4.4. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Suicide Worldwide in 2019. Available online: https://www.who.int/publications/i/item/9789240026643 (accessed on 1 October 2021).
- Turecki, G.; Brent, D.A. Suicide and suicidal behaviour. Lancet 2016, 387, 1227–1239. [Google Scholar] [CrossRef]
- National Center for Injury Prevention and Control. 10 Leading Causes of Death by Age Group, United States. Available online: https://www.cdc.gov/injury/images/lc-charts/leading_causes_of_death_by_age_group_2018_1100w850h.jpg (accessed on 1 October 2021).
- May, A.M.; Czyz, E.K.; West, B.T. Differentiating Adolescent Suicide Attempters and Ideators: A Classification Tree Analysis of Risk Behaviors. J. Adolesc. Health 2020, 67, 837–850. [Google Scholar] [CrossRef] [PubMed]
- Thapar, A.; Collishaw, S.; Pine, D.S.; Thapar, A.K. Depression in adolescence. Lancet 2012, 379, 1056–1067. [Google Scholar] [CrossRef] [Green Version]
- Hawton, K.; Saunders, K.E.; O’Connor, R.C. Self-harm and suicide in adolescents. Lancet 2012, 379, 2373–2382. [Google Scholar] [CrossRef]
- Khalid, S.; Williams, C.M.; Reynolds, S.A. Is there an association between diet and depression in children and adolescents? A systematic review. Br. J. Nutr. 2016, 116, 2097–2108. [Google Scholar] [CrossRef] [PubMed]
- Cunha, C.M.; Costa, P.R.F.; de Oliveira, L.P.M.; Queiroz, V.A.O.; Pitangueira, J.C.D.; Oliveira, A.M. Dietary patterns and cardiometabolic risk factors among adolescents: Systematic review and meta-analysis. Br. J. Nutr. 2018, 119, 859–879. [Google Scholar] [CrossRef] [PubMed]
- Sampasa-Kanyinga, H.; Chaput, J.P.; Goldfield, G.S.; Janssen, I.; Wang, J.; Hamilton, H.A.; Colman, I. 24-hour movement guidelines and suicidality among adolescents. J. Affect. Disord. 2020, 274, 372–380. [Google Scholar] [CrossRef]
- Sampasa-Kanyinga, H.; Colman, I.; Goldfield, G.S.; Janssen, I.; Wang, J.; Tremblay, M.S.; Barnes, J.D.; Walsh, J.J.; Chaput, J.P. 24-Hour Movement Behaviors and Internalizing and Externalizing Behaviors Among Youth. J. Adolesc. Health 2021, 68, 969–977. [Google Scholar] [CrossRef]
- World Health Organization. Global Action Plan on Physical Activity 2018–2030: More Active People for a Healthier World: At-a-Glance. Available online: https://apps.who.int/iris/handle/10665/272721 (accessed on 1 October 2021).
- World Health Organization. WHO Guidelines on Physical Activity and Sedentary Behaviour. Available online: https://apps.who.int/iris/handle/10665/336656 (accessed on 1 October 2021).
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef]
- Chaput, J.P.; Willumsen, J.; Bull, F.; Chou, R.; Ekelund, U.; Firth, J.; Jago, R.; Ortega, F.B.; Katzmarzyk, P.T. 2020 WHO guidelines on physical activity and sedentary behaviour for children and adolescents aged 5-17 years: Summary of the evidence. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 141. [Google Scholar] [CrossRef]
- Tremblay, M.S.; Carson, V.; Chaput, J.P.; Connor Gorber, S.; Dinh, T.; Duggan, M.; Faulkner, G.; Gray, C.E.; Gruber, R.; Janson, K.; et al. Canadian 24-Hour Movement Guidelines for Children and Youth: An Integration of Physical Activity, Sedentary Behaviour, and Sleep. Appl. Physiol. Nutr. Metab. 2016, 41, S311–S327. [Google Scholar] [CrossRef] [PubMed]
- Hirshkowitz, M.; Whiton, K.; Albert, S.M.; Alessi, C.; Bruni, O.; DonCarlos, L.; Hazen, N.; Herman, J.; Katz, E.S.; Kheirandish-Gozal, L.; et al. National Sleep Foundation’s sleep time duration recommendations: Methodology and results summary. Sleep Health 2015, 1, 40–43. [Google Scholar] [CrossRef]
- Janssen, I.; Roberts, K.C.; Thompson, W. Adherence to the 24-Hour Movement Guidelines among 10- to 17-year-old Canadians. Health Promot. Chronic Dis. Prev. Can. 2017, 37, 369–375. [Google Scholar] [CrossRef] [PubMed]
- Roberts, K.C.; Yao, X.; Carson, V.; Chaput, J.P.; Janssen, I.; Tremblay, M.S. Meeting the Canadian 24-Hour Movement Guidelines for Children and Youth. Health Rep. 2017, 28, 3–7. [Google Scholar]
- Shi, Y.; Huang, W.Y.; Sit, C.H.; Wong, S.H. Compliance With 24-Hour Movement Guidelines in Hong Kong Adolescents: Associations With Weight Status. J. Phys. Act. Health 2020, 17, 287–292. [Google Scholar] [CrossRef] [PubMed]
- Zhu, X.; Healy, S.; Haegele, J.A.; Patterson, F. Twenty-Four-Hour Movement Guidelines and Body Weight in Youth. J. Pediatr. 2020, 218, 204–209. [Google Scholar] [CrossRef] [PubMed]
- Guerrero, M.D.; Barnes, J.D.; Walsh, J.J.; Chaput, J.P.; Tremblay, M.S.; Goldfield, G.S. 24-Hour Movement Behaviors and Impulsivity. Pediatrics 2019, 144, e20190187. [Google Scholar] [CrossRef]
- Walsh, J.J.; Barnes, J.D.; Cameron, J.D.; Goldfield, G.S.; Chaput, J.P.; Gunnell, K.E.; Ledoux, A.A.; Zemek, R.L.; Tremblay, M.S. Associations between 24 hour movement behaviours and global cognition in US children: A cross-sectional observational study. Lancet Child Adolesc. Health 2018, 2, 783–791. [Google Scholar] [CrossRef]
- Sampasa-Kanyinga, H.; Colman, I.; Goldfield, G.S.; Janssen, I.; Wang, J.; Hamilton, H.A.; Chaput, J.P. Associations between the Canadian 24 h movement guidelines and different types of bullying involvement among adolescents. Child Abuse Negl. 2020, 108, 104638. [Google Scholar] [CrossRef]
- Sampasa-Kanyinga, H.; Chaput, J.P.; Goldfield, G.S.; Janssen, I.; Wang, J.; Hamilton, H.A.; Ferro, M.A.; Colman, I. The Canadian 24-Hour Movement Guidelines and Psychological Distress among Adolescents: Les Directives canadiennes en matière de mouvement sur 24 heures et la détresse psychologique chez les adolescents. Can. J. Psychiatry 2021, 66, 624–633. [Google Scholar] [CrossRef]
- Lu, S.; Cheval, B.; Yu, Q.; Hossain, M.M.; Chen, S.T.; Taylor, A.; Bao, R.; Doig, S.; Li, J.; Wang, T.; et al. Associations of 24-Hour Movement Behavior with Depressive Symptoms and Anxiety in Children: Cross-Sectional Findings from a Chinese Sample. Healthcare 2021, 9, 1532. [Google Scholar] [CrossRef] [PubMed]
- Sampasa-Kanyinga, H.; Colman, I.; Goldfield, G.S.; Janssen, I.; Wang, J.; Podinic, I.; Tremblay, M.S.; Saunders, T.J.; Sampson, M.; Chaput, J.P. Combinations of physical activity, sedentary time, and sleep duration and their associations with depressive symptoms and other mental health problems in children and adolescents: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 72. [Google Scholar] [CrossRef] [PubMed]
- Pengpid, S.; Peltzer, K. Loneliness is associated with poor mental health, social-environmental factors, and health risk behaviours among national samples of in-school adolescents in four Caribbean countries. Psychol. Health Med. 2022, 27, 559–570. [Google Scholar] [CrossRef] [PubMed]
- Ashdown-Franks, G.; Vancampfort, D.; Firth, J.; Smith, L.; Sabiston, C.M.; Stubbs, B.; Koyanagi, A. Association of leisure-time sedentary behavior with fast food and carbonated soft drink consumption among 133,555 adolescents aged 12-15 years in 44 low- and middle-income countries. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 35. [Google Scholar] [CrossRef]
- Chaves, O.C.; Velasquez-Melendez, G.; Costa, D.; Caiaffa, W.T. Soft drink consumption and body mass index in Brazilian adolescents: National Adolescent Student Health Survey. Rev. Bras. Epidemiol. 2018, 21, e180010. [Google Scholar] [CrossRef]
- Iannotti, R.J.; Wang, J. Patterns of physical activity, sedentary behavior, and diet in U.S. adolescents. J. Adolesc. Health 2013, 53, 280–286. [Google Scholar] [CrossRef] [Green Version]
- Mueller, N.T.; Jacobs, D.R., Jr.; MacLehose, R.F.; Demerath, E.W.; Kelly, S.P.; Dreyfus, J.G.; Pereira, M.A. Consumption of caffeinated and artificially sweetened soft drinks is associated with risk of early menarche. Am. J. Clin. Nutr. 2015, 102, 648–654. [Google Scholar] [CrossRef] [Green Version]
- Solnick, S.J.; Hemenway, D. Soft drinks, aggression and suicidal behaviour in US high school students. Int. J. Inj. Contr. Saf. Promot. 2014, 21, 266–273. [Google Scholar] [CrossRef]
- Holubcikova, J.; Kolarcik, P.; Madarasova Geckova, A.; Reijneveld, S.A.; van Dijk, J.P. The mediating effect of daily nervousness and irritability on the relationship between soft drink consumption and aggressive behaviour among adolescents. Int. J. Public Health 2015, 60, 699–706. [Google Scholar] [CrossRef]
- Shi, Z.; Malki, A.; Abdel-Salam, A.G.; Liu, J.; Zayed, H. Association between Soft Drink Consumption and Aggressive Behaviour among a Quarter Million Adolescents from 64 Countries Based on the Global School-Based Student Health Survey (GSHS). Nutrients 2020, 12, 694. [Google Scholar] [CrossRef] [Green Version]
- Mrug, S.; Jones, L.C.; Elliott, M.N.; Tortolero, S.R.; Peskin, M.F.; Schuster, M.A. Soft Drink Consumption and Mental Health in Adolescents: A Longitudinal Examination. J. Adolesc. Health 2021, 68, 155–160. [Google Scholar] [CrossRef]
- Park, S.; Rim, S.J.; Lee, J.H. Associations between dietary behaviours and perceived physical and mental health status among Korean adolescents. Nutr. Diet 2018, 75, 488–493. [Google Scholar] [CrossRef] [PubMed]
- Sim, E.; Sohn, W.; Choi, E.S.; Noh, H. Sugar-sweetened beverage consumption frequency in Korean adolescents: Based on the 2015 Youth Risk Behavior Web-Based Survey. Int. Dent. J. 2019, 69, 376–382. [Google Scholar] [CrossRef] [PubMed]
- Pabayo, R.; Dias, J.; Hemenway, D.; Molnar, B.E. Sweetened beverage consumption is a risk factor for depressive symptoms among adolescents living in Boston, Massachusetts, USA. Public Health Nutr. 2016, 19, 3062–3069. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hong, S.A.; Peltzer, K. Dietary behaviour, psychological well-being and mental distress among adolescents in Korea. Child Adolesc. Psychiatry Ment. Health 2017, 11, 56. [Google Scholar] [CrossRef] [Green Version]
- Pengpid, S.; Peltzer, K. High Carbonated Soft Drink Intake is Associated with Health Risk Behavior and Poor Mental Health among School-Going Adolescents in Six Southeast Asian Countries. Int. J. Environ. Res. Public Health 2019, 17, 132. [Google Scholar] [CrossRef] [Green Version]
- Pan, X.; Zhang, C.; Shi, Z. Soft drink and sweet food consumption and suicidal behaviours among Chinese adolescents. Acta Paediatr. 2011, 100, e215–e222. [Google Scholar] [CrossRef]
- Jacob, L.; Stubbs, B.; Koyanagi, A. Consumption of carbonated soft drinks and suicide attempts among 105,061 adolescents aged 12-15 years from 6 high-income, 22 middle-income, and 4 low-income countries. Clin. Nutr. 2020, 39, 886–892. [Google Scholar] [CrossRef]
- Li, X.; Chi, G.; Taylor, A.; Chen, S.T.; Memon, A.R.; Zhang, Y.; Song, Y.; Li, J.; Luo, X.; Zou, L. Lifestyle Behaviors and Suicide-Related Behaviors in Adolescents: Cross-Sectional Study Using the 2019 YRBS Data. Front. Public Health 2021, 9, 766972. [Google Scholar] [CrossRef]
- Xiao, Y.; Romanelli, M.; Lindsey, M.A. A latent class analysis of health lifestyles and suicidal behaviors among US adolescents. J. Affect. Disord. 2019, 255, 116–126. [Google Scholar] [CrossRef]
- Centers for disease control and prevention of United States. Youth Risk Behavior Surveillance System Data & Document. Available online: https://www.cdc.gov/healthyyouth/data/yrbs/data.htm, (accessed on 1 October 2021).
- Baiden, P.; LaBrenz, C.A.; Asiedua-Baiden, G.; Muehlenkamp, J.J. Examining the intersection of race/ethnicity and sexual orientation on suicidal ideation and suicide attempt among adolescents: Findings from the 2017 Youth Risk Behavior Survey. J. Psychiatr. Res. 2020, 125, 13–20. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, W.; Nabors, L.; Mahabee-Gittens, M.E.; Merianos, A.L. E-cigarette and marijuana use and the attainment of obesity prevention guidelines among U.S. adolescents. Prev. Med. Rep. 2021, 23, 101445. [Google Scholar] [CrossRef]
- Ross, R.; Chaput, J.P.; Giangregorio, L.M.; Janssen, I.; Saunders, T.J.; Kho, M.E.; Poitras, V.J.; Tomasone, J.R.; El-Kotob, R.; McLaughlin, E.C.; et al. Canadian 24-Hour Movement Guidelines for Adults aged 18–64 years and Adults aged 65 years or older: An integration of physical activity, sedentary behaviour, and sleep. Appl. Physiol. Nutr. Metab. 2020, 45, S57–S102. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention of United States. Growth Chart Training. Available online: https://www.cdc.gov/nccdphp/dnpao/growthcharts/resources/sas.htm (accessed on 1 October 2021).
- Fleary, S.A. Combined Patterns of Risk for Problem and Obesogenic Behaviors in Adolescents: A Latent Class Analysis Approach. J. Sch. Health 2017, 87, 182–193. [Google Scholar] [CrossRef] [PubMed]
- Rao, J.; Scott, A. On Chi-squared Tests For Multiway Contigency Tables with Proportions Estimated From Survey Data. Ann. Stat. 1984, 12, 46–60. [Google Scholar] [CrossRef]
- Thomas, D.; Rao, J. Small-sample comparison of level and power for simple goodness-of-fit statistics under cluster sampling. JASA 1987, 82, 630–636. [Google Scholar] [CrossRef]
- Korn, E.; Graubard, B. Confidence Intervals For Proportions With Small Expected Number of Positive Counts Estimated From Survey Data. Surv. Methodol. 1998, 23, 193–201. [Google Scholar]
- van Buuren, S.; Groothuis-Oudshoorn, K. mice: Multivariate Imputation by Chained Equations in R. J. Stat. Softw. 2011, 45, 1–67. [Google Scholar] [CrossRef] [Green Version]
- VanderWeele, T.J.; Ding, P. Sensitivity Analysis in Observational Research: Introducing the E-Value. Ann. Intern. Med. 2017, 167, 268–274. [Google Scholar] [CrossRef]
- Mathur, M.B.; Ding, P.; Riddell, C.A.; VanderWeele, T.J. Web Site and R Package for Computing E-values. Epidemiology 2018, 29, e45–e47. [Google Scholar] [CrossRef]
- Ma, C.; Li, Z.; Tong, Y.; Zhao, M.; Magnussen, C.G.; Xi, B. Leisure sedentary time and suicide risk among young adolescents: Data from 54 low- and middle-income countries. J. Affect. Disord. 2022, 298, 457–463. [Google Scholar] [CrossRef] [PubMed]
- Vancampfort, D.; Stubbs, B.; Mugisha, J.; Firth, J.; Van Damme, T.; Smith, L.; Koyanagi, A. Leisure-time sedentary behavior and suicide attempt among 126,392 adolescents in 43 countries. J. Affect. Disord. 2019, 250, 346–353. [Google Scholar] [CrossRef] [PubMed]
- Coyne, S.M.; Hurst, J.L.; Dyer, W.J.; Hunt, Q.; Schvanaveldt, E.; Brown, S.; Jones, G. Suicide Risk in Emerging Adulthood: Associations with Screen Time over 10 years. J. Youth Adolesc. 2021, 50, 2324–2338. [Google Scholar] [CrossRef] [PubMed]
- Chiu, H.Y.; Lee, H.C.; Chen, P.Y.; Lai, Y.F.; Tu, Y.K. Associations between sleep duration and suicidality in adolescents: A systematic review and dose-response meta-analysis. Sleep Med. Rev. 2018, 42, 119–126. [Google Scholar] [CrossRef]
- Felez-Nobrega, M.; Haro, J.M.; Vancampfort, D.; Koyanagi, A. Sex difference in the association between physical activity and suicide attempts among adolescents from 48 countries: A global perspective. J. Affect. Disord. 2020, 266, 311–318. [Google Scholar] [CrossRef]
- Kivimäki, P.; Kekkonen, V.; Valtonen, H.; Tolmunen, T.; Honkalampi, K.; Tacke, U.; Hintikka, J.; Lehto, S.M.; Laukkanen, E. Alcohol use among adolescents, aggressive behaviour, and internalizing problems. J. Adolesc. 2014, 37, 945–951. [Google Scholar] [CrossRef]
- Borges, G.; Bagge, C.L.; Cherpitel, C.J.; Conner, K.R.; Orozco, R.; Rossow, I. A meta-analysis of acute use of alcohol and the risk of suicide attempt. Psychol. Med. 2017, 47, 949–957. [Google Scholar] [CrossRef] [Green Version]
- Harrell, C.S.; Zainaldin, C.; McFarlane, D.; Hyer, M.M.; Stein, D.; Sayeed, I.; Neigh, G.N. High-fructose diet during adolescent development increases neuroinflammation and depressive-like behavior without exacerbating outcomes after stroke. Brain Behav. Immun. 2018, 73, 340–351. [Google Scholar] [CrossRef]
- Jacques, A.; Chaaya, N.; Beecher, K.; Ali, S.A.; Belmer, A.; Bartlett, S. The impact of sugar consumption on stress driven, emotional and addictive behaviors. Neurosci. Biobehav. Rev. 2019, 103, 178–199. [Google Scholar] [CrossRef]
- Shelton, R.C.; Miller, A.H. Inflammation in depression: Is adiposity a cause? Dialogues Clin. Neurosci. 2011, 13, 41–53. [Google Scholar] [CrossRef]
- Brundin, L.; Bryleva, E.Y.; Thirtamara Rajamani, K. Role of Inflammation in Suicide: From Mechanisms to Treatment. Neuropsychopharmacology 2017, 42, 271–283. [Google Scholar] [CrossRef] [PubMed]
- Liu, B.-P.; Fang, H.-J.; Jia, C.-X. The Serial Mediation of the Association between Breakfast Skipping and Suicidality by Weight Status and Depressive Symptoms: Findings from the National Youth Risk Behavior Surveys of the United States. Nutrients 2022, 14, 956. [Google Scholar] [CrossRef] [PubMed]
- Harrell, C.S.; Burgado, J.; Kelly, S.D.; Johnson, Z.P.; Neigh, G.N. High-fructose diet during periadolescent development increases depressive-like behavior and remodels the hypothalamic transcriptome in male rats. Psychoneuroendocrinology 2015, 62, 252–264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chakraborti, A.; Graham, C.; Chehade, S.; Vashi, B.; Umfress, A.; Kurup, P.; Vickers, B.; Chen, H.A.; Telange, R.; Berryhill, T.; et al. High Fructose Corn Syrup-Moderate Fat Diet Potentiates Anxio-Depressive Behavior and Alters Ventral Striatal Neuronal Signaling. Front. Neurosci. 2021, 15, 669410. [Google Scholar] [CrossRef]
- Cisternas, P.; Salazar, P.; Serrano, F.G.; Montecinos-Oliva, C.; Arredondo, S.B.; Varela-Nallar, L.; Barja, S.; Vio, C.P.; Gomez-Pinilla, F.; Inestrosa, N.C. Fructose consumption reduces hippocampal synaptic plasticity underlying cognitive performance. Biochim. Biophys. Acta 2015, 1852, 2379–2390. [Google Scholar] [CrossRef] [Green Version]
- de Sousa Rodrigues, M.E.; Bekhbat, M.; Houser, M.C.; Chang, J.; Walker, D.I.; Jones, D.P.; Oller do Nascimento, C.M.P.; Barnum, C.J.; Tansey, M.G. Chronic psychological stress and high-fat high-fructose diet disrupt metabolic and inflammatory gene networks in the brain, liver, and gut and promote behavioral deficits in mice. Brain Behav. Immun. 2017, 59, 158–172. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
| Variables | Suicidality, % (95% CI) | |||
|---|---|---|---|---|
| Suicidal Ideation | Suicide Plan | Suicide Attempt | Suicide Attempt with Medical Treatment | |
| Total | 17.3 (16.8–17.8) | 14.0 (13.5–14.5) | 8.1 (7.7–8.5) | 2.6 (2.4–2.8) |
| The recommendations of the 24 h movement guidelines | ||||
| Appropriate sleep duration a | 11.4 (10.8–12.0) | 9.5 (9.0–10.1) | 5.2 (4.7–5.7) | 1.5 (1.3–1.8) |
| Inappropriate sleep duration a | 20.2 (19.6–20.8) | 16.3 (15.6–16.9) | 9.2 (8.7–9.7) | 2.9 (2.6–3.2) |
| p for difference | <0.001 | <0.001 | <0.001 | <0.001 |
| Screen time ≤2 h/day | 14.7 (13.8–15.6) | 11.9 (11.0–12.8) | 7.1 (6.3–7.9) | 2.4 (2.0–2.8) |
| Screen time >2 h/day | 18.1 (17.5–18.6) | 14.7 (14.2–15.3) | 8.3 (7.9–8.6) | 2.5 (2.3–2.7) |
| p for difference | <0.001 | <0.001 | 0.005 | 0.496 |
| Physical activity ≥1 h/day | 13.0 (12.3–13.8) | 10.9 (10.2–11.6) | 6.3 (5.8–6.8) | 2.1 (1.8–2.3) |
| Physical activity <1 h/day | 18.8 (18.2–19.4) | 15.2 (14.6–15.8) | 8.7 (8.2–9.2) | 2.7 (2.4–3.0) |
| p for difference | <0.001 | <0.001 | <0.001 | <0.001 |
| Meeting all the recommendations | 6.8 (5.4–8.2) | 4.7 (3.6–5.9) | 3.5 (2.3–4.7) | 1.2 (0.3–2.0) |
| Not meeting all the recommendations | 17.8 (17.2–18.3) | 14.4 (13.9–15.0) | 8.0 (7.6–8.5) | 2.5 (2.3–2.7) |
| p for difference | <0.001 | <0.001 | <0.001 | 0.036 |
| Soft drink consumption | ||||
| None | 15.3 (14.5–16.2) | 12.5 (11.7–13.3) | 6.6 (6.0–7.2) | 2.1 (1.7–2.4) |
| <1 time/day | 16.8 (16.1–17.4) | 13.5 (12.9–14.2) | 7.3 (6.8–7.7) | 2.1 (1.8–2.3) |
| 1–2 times/day | 18.5 (17.3–19.7) | 14.4 (13.3–15.5) | 8.5 (7.7–9.4) | 2.8 (2.3–3.3) |
| 3 time/day | 24.5 (22.9–26.2) | 20.9 (19.2–22.7) | 16.0 (14.5–17.5) | 6.4 (5.3–7.5) |
| p for difference | <0.001 | <0.001 | <0.001 | <0.001 |
| Variables | Suicidal Ideation, OR (95% CI) a | Suicide Plan, OR (95% CI) a | Suicide Attempt, OR (95% CI) a | Suicide attempt with medical treatment, OR (95% CI) a |
|---|---|---|---|---|
| Total | ||||
| 24 h movement guidelines | ||||
| Meeting all the recommendations | Reference | Reference | Reference | Reference |
| Not meeting all the recommendations | 1.69 (1.30–2.19) *** | 1.76 (1.34–2.32) *** | 1.12 (0.74–1.68) | 1.04 (0.49–2.23) |
| Soft drink consumption | ||||
| None | Reference | Reference | Reference | Reference |
| <1 time/day | 1.03 (0.94–1.12) | 1.03 (0.95–1.13) | 1.03 (0.92–1.16) | 0.96 (0.77–1.21) |
| 1–2 times/day | 1.15 (1.02–1.30) * | 1.06 (0.93–1.20) | 1.21 (1.04–1.41) * | 1.25 (0.93–1.67) |
| 3 times/day | 1.37 (1.20–1.55) *** | 1.45 (1.26–1.68) *** | 2.20 (1.86–2.61) *** | 2.49 (1.90–3.27) *** |
| p for trend | <0.001 | <0.001 | <0.001 | <0.001 |
| Boy | ||||
| 24 h movement guidelines | ||||
| Meeting all the recommendations | Reference | Reference | Reference | Reference |
| Not meeting all the recommendations | 2.18 (1.51–3.13) *** | 2.28 (1.56–3.34) *** | 1.68 (0.87–3.23) | 0.80 (0.27–2.37) |
| Soft drink consumption | ||||
| None | Reference | Reference | Reference | Reference |
| <1 time/day | 0.97 (0.83–1.13) | 1.01 (0.87–1.18) | 0.79 (0.61–1.02) | 0.58 (0.38–0.89) * |
| 1–2 times/day | 1.11 (0.91–1.36) | 1.01 (0.83–1.24) | 0.99 (0.75–1.32) | 0.87 (0.53–1.43) |
| 3 times/day | 1.40 (1.15–1.71) *** | 1.52 (1.22–1.90) *** | 2.09 (1.59–2.76) *** | 2.58 (1.60–4.16) *** |
| p for trend | <0.001 | 0.001 | <0.001 | <0.001 |
| Girl | ||||
| 24 h movement guidelines | ||||
| Meeting all the recommendations | Reference | Reference | Reference | Reference |
| Not meeting all the recommendations | 1.30 (0.89–1.90) | 1.36 (0.90–2.07) | 0.78 (0.44–1.35) | 1.53 (0.71–3.30) |
| Soft drink consumption | ||||
| None | Reference | Reference | Reference | Reference |
| <1 time/day | 1.04 (0.94–1.17) | 1.03 (0.93–1.15) | 1.15 (0.99–1.33) | 1.17 (0.92–1.49) |
| 1–2 times/day | 1.16 (0.99–1.36) | 1.09 (0.91–1.29) | 1.32 (1.09–1.59) ** | 1.47 (1.05–2.05) * |
| 3 times/day | 1.29 (1.08–1.55) ** | 1.36 (1.13–1.63) ** | 2.13 (1.73–2.62) *** | 2.19 (1.64–2.94) *** |
| p for trend | 0.003 | 0.004 | <0.001 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, B.-P.; Jia, C.-X.; Li, S.-X. The Association of Soft Drink Consumption and the 24-Hour Movement Guidelines with Suicidality among Adolescents of the United States. Nutrients 2022, 14, 1870. https://doi.org/10.3390/nu14091870
Liu B-P, Jia C-X, Li S-X. The Association of Soft Drink Consumption and the 24-Hour Movement Guidelines with Suicidality among Adolescents of the United States. Nutrients. 2022; 14(9):1870. https://doi.org/10.3390/nu14091870
Chicago/Turabian StyleLiu, Bao-Peng, Cun-Xian Jia, and Shi-Xue Li. 2022. "The Association of Soft Drink Consumption and the 24-Hour Movement Guidelines with Suicidality among Adolescents of the United States" Nutrients 14, no. 9: 1870. https://doi.org/10.3390/nu14091870
APA StyleLiu, B.-P., Jia, C.-X., & Li, S.-X. (2022). The Association of Soft Drink Consumption and the 24-Hour Movement Guidelines with Suicidality among Adolescents of the United States. Nutrients, 14(9), 1870. https://doi.org/10.3390/nu14091870