
The Effectiveness of Web-Based Interventions to Promote Health Behaviour Change in Adolescents: A Systematic Review


Abstract
:1. Introduction
2. Methods
2.1. Data Sources
2.2. Inclusion and Exclusion Criteria
2.2.1. Participants/Population
Inclusion Criteria
Exclusion Criteria
2.2.2. Intervention/Exposure
Inclusion Criteria
Exclusion Criteria
2.2.3. Comparator(s)/Control
Inclusion Criteria
Exclusion Criteria
2.2.4. Outcome(s)
Inclusion Criteria
Exclusion Criteria
2.2.5. Study Design
Inclusion Criteria
Exclusion Criteria
2.3. Data Extraction
2.4. Data Synthesis
3. Results
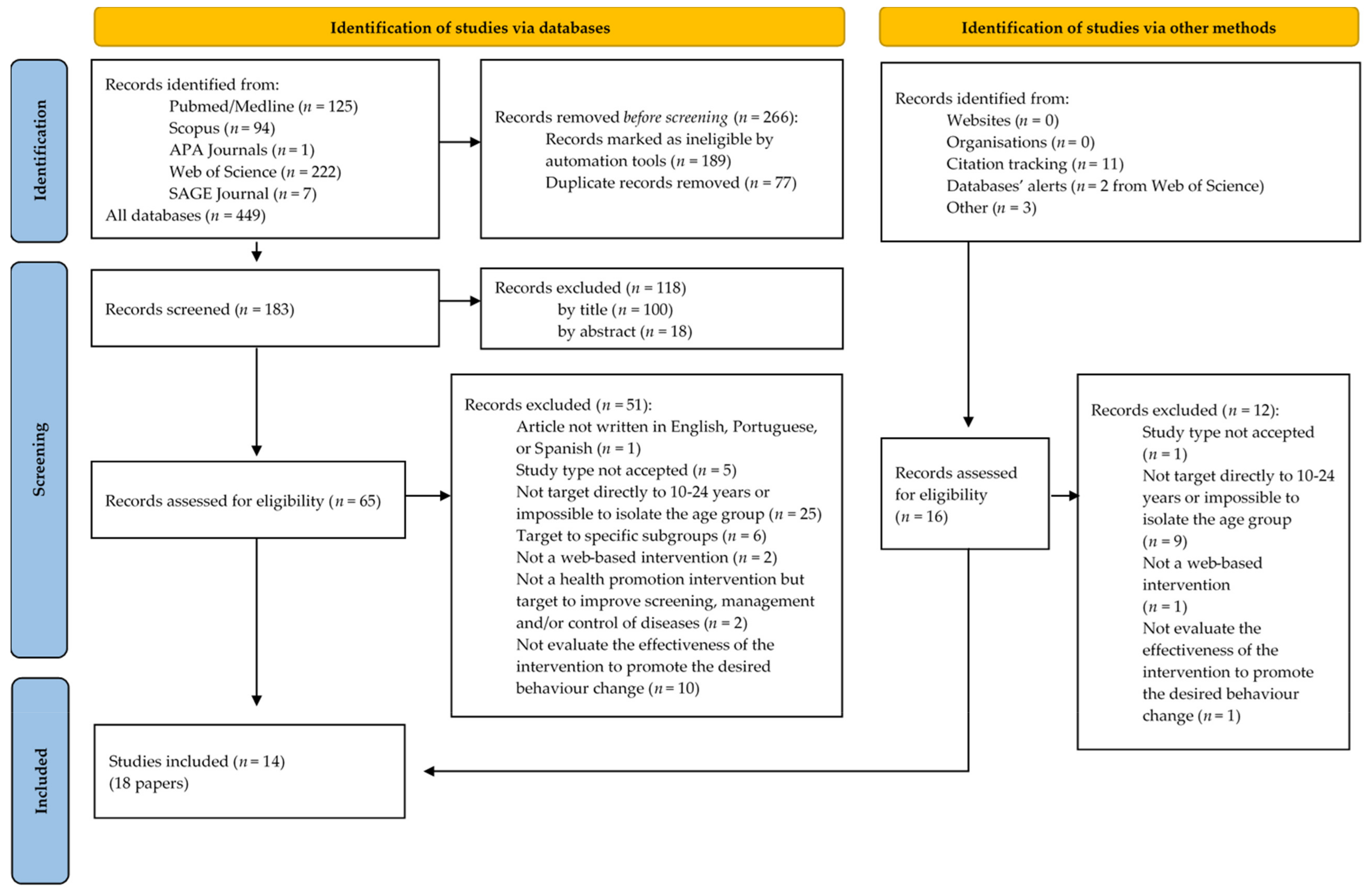
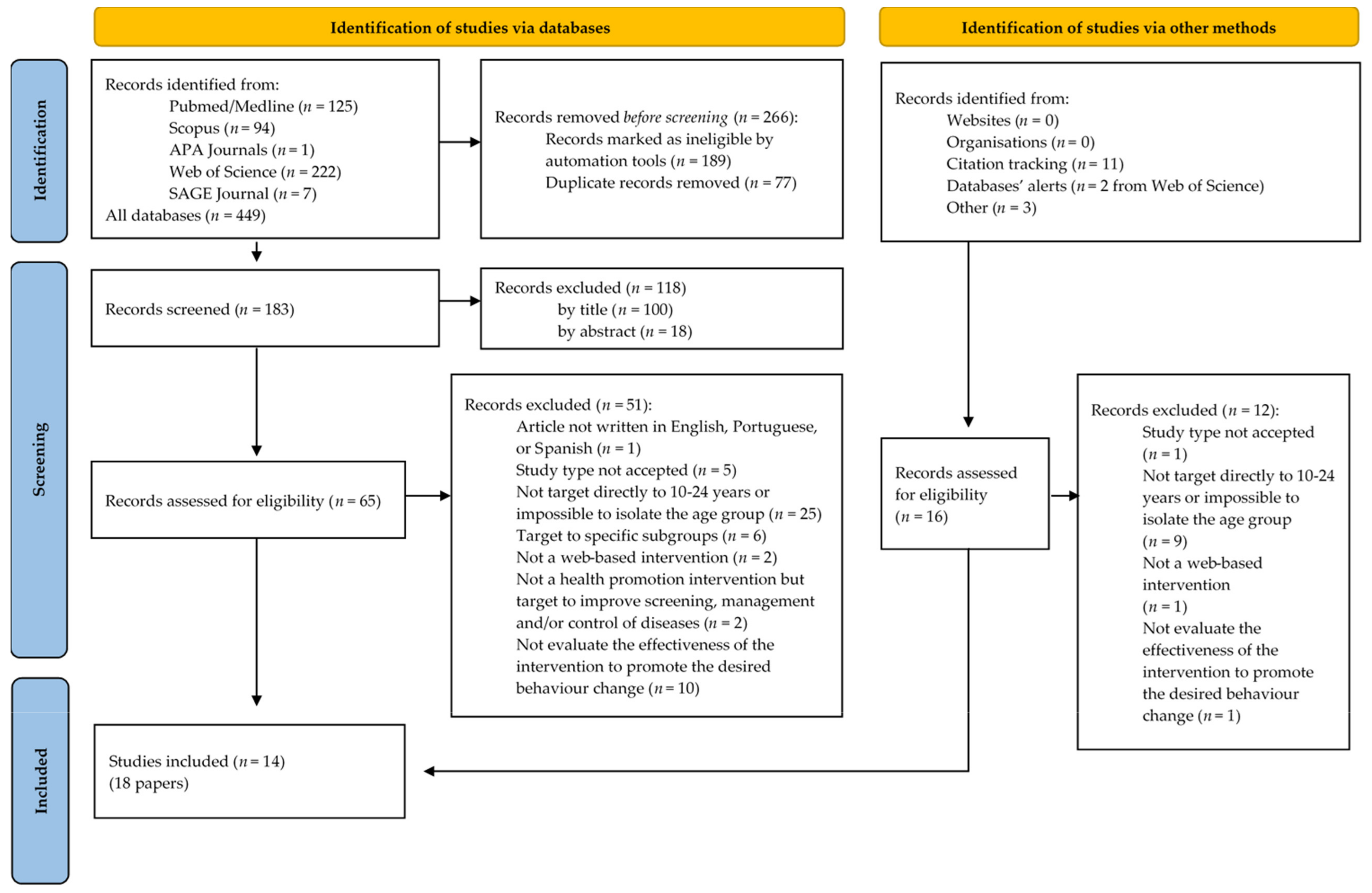
3.1. Study Selection
3.2. Description of the Studies

{kind=link}
{kind=link}
| Author, Year, Country | Setting | Study Design | Participants | Web-Based Intervention | Health Outcomes of Interest | Main Findings |
|---|---|---|---|---|---|---|
| Wilson, M. et al., (2017) [30] USA, North-western United States | School | One-group pre-/post-test design (pre-experimental) | N = 20 students (convenience sample) Mean age of 16.8 years. | Multicomponent Intervention: wearable digital tracking device using an Internet-based platform + group physical activities + nutrition group education/individual counselling session on healthy eating + weekly goal-setting sessions. | Measured at baseline and post-intervention: BMI calculation. Blood glucose level. Blood pressure and pulse measurements. Fitness and cardiovascular fitness. Cognitive and affective variables related to health behaviours. Adolescents’ physical activity (PA) and healthy eating. Self-efficacy for PA and healthy eating. Self-determination. Screen time. | Participants showed improvements from pre-test to post-test in health and fitness markers (positive changes in weight, fitness, and cardiovascular measurements) and improved motivation toward PA and reduced screen time. |
| Larsen, B. et al., (2018) [31] USA (San Diego, CA) | Hispanic community | Pre/post-test design (Single-arm pilot trial) | N = 21 Latina adolescents Mean age of 14.7 years. | Website mobile phone friendly (tailored Internet-delivered activity manuals, computer-expert system tailored reports, activity tip sheets, and a guide of local activity resources) | Measured at baseline and follow-up (12 weeks): PA by 7-day physical activity recall (PAR) interview and ActiGraph GT3X+ accelerometers. | Results from the 7-day PAR showed that positive changes in PA at 12 weeks were seen not just in quantity but also in type. The usage of validated self-report measures showed to be better than accelerometers among this population since there are some activities in which the accelerometer may not be worn or that were not well measured by the accelerometer. |
| Huang, S. J. et al., (2019) [39] Taiwan, Taipei City | School | Quasi-experimental (Three-armed) | N initial = 617 students Mean age of 11.4 years. | Two experimental groups: One using a web-based exercise program applying a self-management strategy combined with geographical information system (GIS) mapping function and using a narrative animated cartoon. The other was knowledge-only using only the animated story. | Measured at baseline, immediately post and 3-month follow-up: PA by the Chinese version of the Child/Adolescent Activity Log. Exercise-related self-efficacy using a 5-item Exercise-Related-Self-Efficacy Scale. Perceived benefit of PA using a self-developed 7-item Perceived-Benefit-of-Exercise Scale. | This intervention using self-management strategy + GIS mapping function was effective in producing small but significant increases in school children’s self-efficacy and PA. The perceived benefit and self-efficacy of regular PA might have partly affected the participants’ PA levels because the self-efficacy factor was always higher for both experimental groups than for the control at the post-test and follow-up; it was also higher for the self-management group than for the knowledge-only group. The intervention was more effective for male students than females. |
| Pirzadeh, A. et al., (2020) [38] Iran, Isfahan | University | Quasi-experimental | N = 278 high school students Mean age is not described. | Two web-based intervention groups. One group received education through a website with tailored education strategies based on TTM. The second group only received general education by the same website but without tailored materials. | Measured before intervention and 6 months after: Stage of exercise behaviour change questionnaire. Processes of change questionnaire. Decision-making balance questionnaire. Exercise self-efficacy scale. International PA questionnaire short form. | Education on PA based on the website can be effective. The percentage of students with low, moderate, and severe levels of physical activity in the two intervention groups has increased significantly after the intervention. Participants showed significant progress during stages of change post-intervention and changes were greater in the group who was trained by the TTM. |
| Duan, Y. P. et al., (2017) [40] China, Central Region | University | Randomized controlled trial | N initial = 493 undergraduate students N post-intervention = 337 N 1-month follow-up = 142 Mean age of 19.2 years. | Web-based intervention modules target social–cognitive indicators for health behaviour change for Physical Activity and Fruit and Vegetable Intake (FVI) (information about risks and benefits, motivating intentions to change, identification of barriers, goal setting, development of action plans, coping plans and social support, providing tailored normative feedback). | PA by Chinese short version of the International Physical Activity Questionnaire (IPAQ-C). FVI in the past 7 days. Stages of behavioural change for PA and FVI. Social-cognitive indicators of behaviour change: positive and negative outcome expectancies for PA and FVI; self-efficacy for PA and FVI; action planning; coping planning; social support; intentions for PA and FVI; habit scale. | Students in the intervention group reported more FVI over time. Average FVI for the intervention group were all greater than the recommended amounts at the end of the 8-week intervention and the 1-month follow-up. In terms of PA behaviour, there was no significant interaction effect. Positive results on stage progression for the PA and FVI. All 6 tests revealed significant treatment effects on motivational, volitional, and distal indicators of PA and FVI over time. |
| Khalil, G. E. et al., (2017) [32] USA, Texas, Houston | School | Randomized controlled trial (2-arm single-blinded) | N = 101 adolescents Mean age of 13.4 years. | Two web-based intervention groups: One features interactivity and entertainment to engage adolescent users (text, animations, videos, task-oriented activities, two-dimensional environment to explore health information and make a virtual character). The second included the same health information but without any features of interactivity or entertainment. | Measured at baseline and follow-up: Intention to smoke using items adapted from the susceptibility to smoke scale. | The more participants considered intervention interactive and entertaining, the more they were probably going to show a reduction in their intention to smoke. Perceived interactivity had a more grounded relationship with the reduction in intention to smoke than perceived entertainment. |
| Castillo-Arcos Ldel, C. et al., (2016) [42] Mexico, Urban Mexico | School | Quasi-experimental (single-stage cluster sampling) | N = 193 participants Mean age of 15.8 years. | Multicomponent intervention: 6 online sessions + 2 face-to-face activities aimed at increasing levels of social competence and resilience about sexual behaviours. | Measured pre-and post-intervention: Self-reported risky sexual behaviours (defined as self-reporting unprotected sex, multiple concurrent sexual partners, and alcohol or drug use during sex). Resilience to risky sexual behaviour (defined as the ability to identify and practice strategies to avoid risky sexual behaviour). | The intervention was independently associated with improved self-reported resilience to risky sexual behaviours though not with a significant reduction in those behaviours in multivariate analyses. Participant age mediated the effect of the intervention on resilience, influencing the effectiveness of the intervention. |
| Doubova, S. V. et al., (2017) [41] Mexico, Mexico City | School | Quasi-experimental (field trial) | N = 833 adolescents Mean age is not described. | Multicomponent intervention: Educational sessions through a website displayed by two central characters + class discussions Main topics: dating, courtship, sexual relationships, misconceptions and myths about gender roles and sexual relationships, partner abuse, STIs, early pregnancy, self-esteem, safe sex, use of condoms and condom negotiation. | Measured at baseline, at the end of the four educational sessions (first month), and the end of the follow-up period (fourth month): Knowledge of STIs. Multidimensional Condom Attitudes Scale measuring attitudes regarding condom use. Self-efficacy toward consistent condom use. | The intervention had a positive effect on improving adolescents’ knowledge of STIs, attitudes and self-efficacy toward consistent condom use. In the intervention group, the average knowledge of STIs increased by 30 points compared to the control group. An increase in positive attitudes and self-efficacy toward consistent condom use was also observed more often in the intervention group. |
| Brown, K. E. et al., (2018) [36] United Kingdom (UK), Midlands | Clinical (sexual health service) | Pilot randomized controlled trial (two-armed parallel-group) | N initial = 88 integrated sexual health service attendees N follow-up = 67 Mean age of 20.0 years. | Multicomponent intervention: brief tailored web-based programme + paper-based action planning card. Content about contraceptive pills and/or condoms use using characters with audio to take the user through the process of identifying environmental cues to key target behaviours and planning to perform those behaviours when the environmental cue is present. | Measured at baseline and 3-month follow-up: Self-reported contraceptive pill or condom “mishaps” in the past 3 months. Contraceptive pill or condom use intention. Attitude toward contraceptive pill or condom use. Perceived behavioural control over pill or condom use. Subjective norm relating to pill or condom use. Trait self-control. | The intervention supported pill and condom users to produce quality plans since potential improvements were identified. Bivariate correlations suggest that perceived behavioural control may have a role over method use within intervention content. Additionally, having greater levels of trait self-control may negatively affect plan quality. The study suggests early indications that the intervention could reduce the number of mishaps of intervention participants. |
| Widman, L. et al., (2018) [33] USA, South-eastern | School | Randomized Controlled Trial | N = 222 tenth-grade girls Mean age of 15.2 years. | Interactive, skills-focused web-based intervention. The intervention includes 5 modules about safer sex motivation, HIV and other STDs, sexual norms and attitudes, safer sex self-efficacy, sexual communication skills that can be completed on a computer, tablet, or smartphone device. Each module used audio and video clips, tips from other adolescents, interactive games and quizzes, infographics, and skill-building exercises with self-feedback given in real-time). | Measured at pre-test, post-test and 4-month follow-up: Behavioural assessment of sexual assertiveness skills (at refusing unwanted sexual activity and negotiating condom use). Self-reported sexual assertiveness by Multidimensional Sexual Self Concept Scale. Knowledge regarding HIV and other STDs. Intentions to use condoms and to communicate about sex with items from the AIDS Risk Behaviour Assessment. Sexual Self-Efficacy from self-efficacy for HIV prevention scale. | Immediately post-test, the intervention group showed better sexual assertiveness skills measured with a behavioural task, higher self-reported assertiveness, intentions to communicate about sexual health, knowledge regarding HIV and other STDs, safer sex norms and attitudes, and condom self-efficacy compared with the control condition. At a 4-month follow-up, group differences remained in knowledge regarding HIV and other STDs, condom attitudes, and condom self-efficacy. |
| Arnaud, N. et al., (2016) [35] European countries (Sweden, Germany, Belgium, and the Czech Republic) | Online | Randomized controlled trial (Two-armed multisite) | N initial = 1449 adolescents (Convenience sample) N follow-up = 211 Mean age of 16.8 years. | Interactive web-based system to generate individually tailored content. Generated information in small units using text and graphics and referred to previous participants’ statements. | Measured at baseline and 3-month follow-up: Self-reported drinking index (drinking frequency, frequency of binge drinking, and typical quantity of drinks) using AUDIT-C screening tool. | Self-reported risky drinking as measured by a drinking index was significantly reduced for participants in the intervention group. Statistically significant mean differences at follow-up in favour of the intervention were found for drinking frequency and binge drinking frequency but not for quantity when missing follow-up data were not imputed. In contrast, analyses using an EM-imputed dataset revealed drinking quantity as the only significant secondary effect. |
| Norman, P. et al., (2018) [37] UK, large city | University | Randomized controlled trial (full-factorial design) | N initial = 2,951 students before starting university N post-intervention = 2681 Mean age of 18.8 years. | Brief online intervention combining self-affirmation x TPB-based messages x implementation intentions in a factorial design. | Measured at baseline, 1-week, 1-month and 6-month follow-up: Self-reported alcohol intake (total number of units consumed and number of binge drinking sessions/week). Hazardous and harmful patterns of alcohol use from 10-item AUDIT (only at 6-month follow-up). Cognitions about binge drinking (intention, affective attitude, cognitive attitude, subjective norms, descriptive norms, and perceived control) and extent of endorsement for the beliefs (Engaging in binge drinking at university would be fun; engaging in binge drinking at university would have a negative impact on my studies; my friends engaging in binge drinking would make my binge drinking at university more likely). | TPB-based messages had significant effects on reducing the quantity of alcohol consumed, frequency of binge drinking and harmful patterns of alcohol use over the first 6 months at university. Its effects did not diminish over time. The messages also had significant positive effects on intentions to binge drink, cognitive attitudes, subjective norms, descriptive norms, and self-efficacy, although some effects weakened over time. The effects on the quantity of alcohol and frequency of binge drinking were mediated by TPB variables with significant indirect effects through intention and self-efficacy. The effect sizes for the TPB-based messages on the quantity of alcohol consumed (d = 0.20) and the frequency of binge drinking (d = 0.17) were small. Messages were sufficiently relevant and persuasive to produce changes in behaviour without the need to form if-then plans. Non-significant effects were found for self-affirmation and forming implementation intentions. |
| Coughlin, L. N. et al., (2021) [34] USA, Michigan | Online | Pre/post-test design (Pilot study) | N = 39 participants Mean age of 20.7 years. | Mobile intervention with tailored messages and tips, inspirational images to reinforce content, web links to articles, or other web-based resources, based on users’ responses to daily and weekly surveys. The intervention included gamification through a virtual aquarium environment. | Measured at baseline and 1-month follow up: Concerning alcohol use (quantity and frequency of use, consequences of use, intention, importance confidence of change, perceived risk, reasons for use, and past month driving under influence of use). | Participants’ substance use declined over time, and those reporting using the app more often reported less substance use (including fewer days drinking alcohol, binge drinking, fewer consequences of use and episodes of driving after drinking) at the 1-month follow-up than those who reported using the app less often. |
| Doumas, D. M. et al., (2021) [28] USA, Northwest region | School | Randomized controlled trial | N = 311 high school seniors Mean age of 17.1 years old. | Online personalized normative feedback intervention via text, graphs, and video recordings. The program is intended to reduce risk factors for alcohol use and increase protective behaviours. | Measured at baseline, 30-day and 6-month follow-up: Weekly drinking quantity. Estimated peak blood alcohol concentration (eBAC). Self-reported peak alcohol volume. Classification of High-Risk vs. Low-Risk drinkers by participants’ report on the frequency of binge drinking in the past month. | The intervention effects were moderated by risk status, such that high-risk students in the intervention condition reported a greater reduction in alcohol use relative to students in the control condition. For weekly drinking quantity, intervention effects were limited to the baseline to 30-day follow-up period. Among high-risk students was found a significant decrease in weekly drinking in the intervention condition. However, intervention effects from baseline to the 6-month follow-up were not significant since the control condition also reported significant decreases in weekly drinking. For eBAC, intervention effects were evident at the 30-day follow-up and were sustained at the 6-month follow-up. Specifically, among high-risk students, we found a significant decrease in eBAC relative at the 30-day and 6-month follow-up. It is unclear why sustained intervention effects were found for eBAC but not for weekly drinking. Non-significant intervention effects for low-risk drinkers. |
3.3. Recruitment and Participants
3.4. Web-Based Interventions
3.5. Behaviour Change Theories and Techniques
3.6. Effectiveness of the Web-Based Interventions
3.7. Other Outcomes
3.8. Risk of Bias Assessment
4. Discussion
4.1. Summary of Findings
4.2. Limitations of This Review
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Davis, R.; Campbell, R.; Hildon, Z.; Hobbs, L.; Michie, S. Theories of behaviour and behaviour change across the social and behavioural sciences: A scoping review. Health Psychol. Rev. 2015, 9, 323–344. [Google Scholar] [CrossRef]
- Every Woman Every Child. The Global Strategy for Women’s, Children’s and Adolescents’ Health (2016–2030); United Nations: New York, NY, USA, 2015.
- National Research Council (US) and Institute of Medicine (US) Committee on Adolescent Health Care Services and Models of Care for Treatment Prevention, and Healthy Development. Adolescents Health Status. In Adolescent Health Services-Missing Opportunities; Robert, S., Lawrence, J.A.G., Leslie, J.S., Eds.; National Academies Press: Washington, DC, USA, 2009; pp. 52–133. [Google Scholar]
- Kathryn, L.; Santoro, C.S.; Schoenman, J.; Myers, C.; Chockley, N. The Case for Investing in Youth Health Literacy: One Step on the Path to Achieving Health Equity for Adolescents; National Institute for Health Care Management Research and Educational Foundation: Washington, DC, USA, 2011. [Google Scholar]
- World Health Organization. Global Accelerated Action for the Health of Adolescents (AA-HA!): Guidance to Support Country Implementation; Licence: CC BY-NC-SA 3.0 IGO.; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Lehtimaki, S.S.N.; Solis, L. Adolescent Health: The Missing Population in Universal Health Coverage; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Steinberg, L. How to Improve the Health of American Adolescents. Perspect Psychol. Sci. 2015, 10, 711–715. [Google Scholar] [CrossRef] [PubMed]
- Kann, L.; McManus, T.; Harris, W.A.; Shanklin, S.L.; Flint, K.H.; Queen, B.; Lowry, R.; Chyen, D.; Whittle, L.; Thornton, J.; et al. Youth Risk Behaviour Surveillance-United States, 2017. MMWR Surveill. Summ. 2018, 67, 1–114. [Google Scholar] [CrossRef] [PubMed]
- Tylee, A.; Haller, D.M.; Graham, T.; Churchill, R.; Sanci, L.A. Youth-friendly primary-care services: How are we doing and what more needs to be done? Lancet 2007, 369, 1565–1573. [Google Scholar] [CrossRef]
- Petrescu, D.G.; Tribus, L.C.; Raducu, R.; Purcarea, V.L. Social marketing and behavioural change. Rom. J. Ophthalmol. 2021, 65, 101–103. [Google Scholar] [CrossRef]
- Chichirez, C.M.; Purcărea, V.L. Health marketing and behavioural change: A review of the literature. J. Med. Life 2018, 11, 15–19. [Google Scholar]
- Michie, S.; Richardson, M.; Johnston, M.; Abraham, C.; Francis, J.; Hardeman, W.; Eccles, M.P.; Cane, J.; Wood, C.E. The behaviour change technique taxonomy (v1) of 93 hierarchically clustered techniques: Building an international consensus for the reporting of behaviour change interventions. Ann. Behav. Med. 2013, 46, 81–95. [Google Scholar] [CrossRef]
- Milne-Ives, M.; Lam, C.; De Cock, C.; Van Velthoven, M.H.; Meinert, E. Mobile Apps for Health Behaviour Change in Physical Activity, Diet, Drug and Alcohol Use, and Mental Health: Systematic Review. JMIR Mhealth Uhealth 2020, 8, e17046. [Google Scholar] [CrossRef]
- Meskó, B.; Drobni, Z.; Bényei, É.; Gergely, B.; Gyorffy, Z. Digital health is a cultural transformation of traditional healthcare. mHealth 2017, 3, 38. [Google Scholar] [CrossRef] [Green Version]
- Horvath, K.J.; Ecklund, A.M.; Hunt, S.L.; Nelson, T.F.; Toomey, T.L. Developing Internet-based health interventions: A guide for public health researchers and practitioners. J. Med. Internet Res. 2015, 17, e28. [Google Scholar] [CrossRef]
- Teixeira, P.J.; Marques, M.M. Health Behaviour Change for Obesity Management. Obes. Facts 2017, 10, 666–673. [Google Scholar] [CrossRef]
- Ronquillo, Y.; Meyers, A.; Korvek, S.J. Digital Health. In StatPearls; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2021. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Schwab, K. The Fourth Industrial Revolution: What It Means, How to Respond; World Economic Forum (Cologny, Geneva): Geneva, Switzerland, 2016; Available online: https://www.weforum.org/agenda/2016/01/the-fourth-industrial-revolution-what-it-means-and-how-to-respond/ (accessed on 27 June 2021).
- Sawyer, S.M.; Azzopardi, P.S.; Wickremarathne, D.; Patton, G.C. The age of adolescence. Lancet Child. Adolesc. Health 2018, 2, 223–228. [Google Scholar] [CrossRef]
- Barak, A.; Klein, B.; Proudfoot, J.G. Defining Internet-Supported Therapeutic Interventions. Ann. Behav. Med. 2009, 38, 4–17. [Google Scholar] [CrossRef]
- Armijo-Olivo, S.; Stiles, C.R.; Hagen, N.A.; Biondo, P.D.; Cummings, G.G. Assessment of study quality for systematic reviews: A comparison of the Cochrane Collaboration Risk of Bias Tool and the Effective Public Health Practice Project Quality As-sessment Tool: Methodological research. J. Eval. Clin. Pract. 2012, 18, 12–18. [Google Scholar] [CrossRef]
- Thomas, B.H.; Ciliska, D.; Dobbins, M.; Micucci, S. A process for systematically reviewing the literature: Providing the research evidence for public health nursing interventions. Worldviews Evid. Based Nurs. 2004, 1, 176–184. [Google Scholar] [CrossRef]
- Doumas, D.M.; Esp, S. Reducing Alcohol-Related Consequences Among High School Seniors: Efficacy of a Brief, Web-Based Intervention. J. Couns. Dev. 2019, 97, 53–61. [Google Scholar] [CrossRef]
- Doumas, D.M.; Esp, S.; Flay, B.; Bond, L. A Randomized Controlled Trial Testing the Efficacy of a Brief Online Alcohol Inter-vention for High School Seniors. J. Stud. Alcohol Drugs 2017, 78, 706–715. [Google Scholar] [CrossRef]
- Doumas, D.M.; Esp, S.; Johnson, J.; Trull, R.; Shearer, K. The eCHECKUP TO GO for High School: Impact on risk factors and protective behavioural strategies for alcohol use. Addict. Behav. 2017, 64, 93–100. [Google Scholar] [CrossRef]
- Doumas, D.M.; Hausheer, R.; Esp, S. Age of Drinking Initiation as a Moderator of the Efficacy of a Brief, Web-Based Personalized Feedback Alcohol Intervention. J. Child Adolesc. Subst. Abus. 2016, 25, 591–597. [Google Scholar] [CrossRef]
- Doumas, D.M.; Esp, S.; Turrisi, R.; Bond, L. A Randomized Controlled Trial of the eCHECKUP to GO for High School Seniors across the Academic Year. Subst. Use Misuse 2021, 56, 1932. [Google Scholar] [CrossRef]
- Donato, H.; Donato, M. Stages for Undertaking a Systematic Review. Acta Med. Port. 2019, 32, 227–235. [Google Scholar] [CrossRef] [Green Version]
- Wilson, M.; Ramsay, S.; Young, K.J. Engaging Overweight Adolescents in a Health and Fitness Program Using Wearable Activity Trackers. J. Pediatr. Health Care 2017, 31, e25–e34. [Google Scholar] [CrossRef]
- Larsen, B.; Benitez, T.; Cano, M.; Dunsiger, S.S.; Marcus, B.H.; Mendoza-Vasconez, A.; Sallis, J.F.; Zive, M. Web-Based Physical Activity Intervention for Latina Adolescents: Feasibility, Accept-ability, and Potential Efficacy of the Niñas Saludables Study. J. Med. Internet Res. 2018, 20, e170. [Google Scholar] [CrossRef]
- Khalil, G.E.; Wang, H.; Calabro, K.S.; Mitra, N.; Shegog, R.; Prokhorov, A.V. From the Experience of Interactivity and Enter-tainment to Lower Intention to Smoke: A Randomized Controlled Trial and Path Analysis of a Web-Based Smoking Prevention Program for Adolescents. J. Med. Internet Res. 2017, 19, e44. [Google Scholar] [CrossRef] [Green Version]
- Widman, L.; Golin, C.E.; Kamke, K.; Burnette, J.L.; Prinstein, M.J. Sexual Assertiveness Skills and Sexual Decision-Making in Adolescent Girls: Randomized Controlled Trial of an Online Program. Am. J. Public Health 2018, 108, 96–102. [Google Scholar] [CrossRef]
- Coughlin, L.N.; Nahum-Shani, I.; Philyaw-Kotov, M.L.; Bonar, E.E.; Rabbi, M.; Klasnja, P.; Murphy, S.; Walton, M.A. Developing an Adaptive Mobile Intervention to Address Risky Substance Use Among Adolescents and Emerging Adults: Usability Study. JMIR Mhealth Uhealth 2021, 9, e24424. [Google Scholar] [CrossRef] [PubMed]
- Arnaud, N.; Baldus, C.; Elgán, T.H.; De Paepe, N.; Tønnesen, H.; Csémy, L.; Thomasius, R.; Blankers, M.; Haug, S. Effectiveness of a Web-Based Screening and Fully Automated Brief Motivational Intervention for Adolescent Substance Use: A Randomized Controlled Trial. J. Med. Internet Res. 2016, 18, e103. [Google Scholar] [CrossRef] [Green Version]
- Brown, K.E.; Beasley, K.; Das, S. Self-Control, Plan Quality, and Digital Delivery of Action Planning for Condom and Con-traceptive Pill Use of 14–24-Year-Olds: Findings from a Clinic-Based Online Pilot Randomised Controlled Trial. Appl. Psychol. Health Well Being 2018, 10, 391–413. [Google Scholar] [CrossRef] [Green Version]
- Norman, P.; Cameron, D.; Epton, T.; Webb, T.L.; Harris, P.R.; Millings, A.; Sheeran, P. A randomized controlled trial of a brief online intervention to reduce alcohol consumption in new university students: Combining self-affirmation, theory of planned behaviour messages, and im-plementation intentions. Br. J. Health Psychol. 2018, 23, 108–127. [Google Scholar] [CrossRef]
- Pirzadeh, A.; Zamani, F.; Khoshali, M.; Kelishadi, R. Web-based intervention on the promotion of physical activity among Iranian youth using the transtheoretical model. J. Educ. Health Promot. 2020, 9, 118. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.J.; Hung, W.C.; Shyu, M.L.; Chang, K.C.; Chen, C.K. Web-based intervention to promote physical activity in Taiwanese children. J. Pediatr. Nurs. 2019, 45, e35–e43. [Google Scholar] [CrossRef] [PubMed]
- Duan, Y.P.; Wienert, J.; Hu, C.; Si, G.Y.; Lippke, S. Web-Based Intervention for Physical Activity and Fruit and Vegetable Intake among Chinese University Students: A Randomized Controlled Trial. J. Med. Internet Res. 2017, 19, e106. [Google Scholar] [CrossRef] [PubMed]
- Doubova, S.V.; Martinez-Vega, I.P.; Infante-Castañeda, C.; Pérez-Cuevas, R. Effects of an internet-based educational inter-vention to prevent high-risk sexual behaviour in Mexican adolescents. Health Educ. Res. 2017, 32, 487–498. [Google Scholar] [CrossRef]
- Castillo-Arcos, L.C.; Benavides-Torres, R.A.; López-Rosales, F.; Onofre-Rodríguez, D.J.; Valdez-Montero, C.; Maas-Góngora, L. The effect of an Internet-based intervention designed to reduce HIV/AIDS sexual risk among Mexican adolescents. AIDS Care 2016, 28, 191–196. [Google Scholar] [CrossRef]
- Nicholl, B.I.; Sandal, L.F.; Stochkendahl, M.J.; McCallum, M.; Suresh, N.; Vasseljen, O.; Hartvigsen, J.; Mork, P.J.; Kjaer, P.; Søgaard, K.; et al. Digital Support Interventions for the Self-Management of Low Back Pain: A Systematic Review. J. Med. Internet Res. 2017, 19, e179. [Google Scholar] [CrossRef]
- Sin, J.; Galeazzi, G.; McGregor, E.; Collom, J.; Taylor, A.; Barrett, B.; Lawrence, V.; Henderson, C. Digital Interventions for Screening and Treating Common Mental Disorders or Symptoms of Common Mental Illness in Adults: Systematic Review and Meta-analysis. J. Med. Internet Res. 2020, 22, e20581. [Google Scholar] [CrossRef]
- Brigden, A.; Anderson, E.; Linney, C.; Morris, R.; Parslow, R.; Serafimova, T.; Smith, L.; Briggs, E.; Loades, M.; Crawley, E. Digital Behaviour Change Interventions for Younger Children with Chronic Health Conditions: Systematic Review. J. Med. Internet Res. 2020, 22, e16924. [Google Scholar] [CrossRef]
- Manby, L.; Aicken, C.; Delgrange, M.; Bailey, J.V. Effectiveness of eHealth Interventions for HIV Prevention and Management in Sub-Saharan Africa: Systematic Review and Meta-analyses. AIDS Behav. 2021, 26, 457–469. [Google Scholar] [CrossRef]
- Pfaeffli Dale, L.; Dobson, R.; Whittaker, R.; Maddison, R. The effectiveness of mobile-health behaviour change interventions for cardiovascular disease self-management: A systematic review. Eur. J. Prev. Cardiol. 2016, 23, 801–817. [Google Scholar] [CrossRef]
- Brown, V.; Tran, H.; Downing, K.L.; Hesketh, K.D.; Moodie, M. A systematic review of economic evaluations of web-based or telephone-delivered interventions for preventing overweight and obesity and/or improving obesity-related behaviours. Obes. Rev. 2021, 22, e13227. [Google Scholar] [CrossRef]
- Ryan, K.; Dockray, S.; Linehan, C. A systematic review of tailored eHealth interventions for weight loss. Digit. Health 2019, 5, 1–29. [Google Scholar] [CrossRef]
- Chen, Y.; Perez-Cueto, F.J.A.; Giboreau, A.; Mavridis, I.; Hartwell, H. The Promotion of Eating Behaviour Change through Digital Interventions. Int. J. Environ. Res. Public Health 2020, 17, 7488. [Google Scholar] [CrossRef]
- Villinger, K.; Wahl, D.R.; Boeing, H.; Schupp, H.T.; Renner, B. The effectiveness of app-based mobile interventions on nutrition behaviours and nutrition-related health outcomes: A systematic review and meta-analysis. Obes. Rev. 2019, 20, 1465–1484. [Google Scholar] [CrossRef] [Green Version]
- Stephenson, A.; McDonough, S.M.; Murphy, M.H.; Nugent, C.D.; Mair, J.L. Using computer, mobile and wearable technolo-gy-enhanced interventions to reduce sedentary behaviour: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 105. [Google Scholar] [CrossRef]
- Wibowo, R.A.; Kelly, P.; Baker, G. The effect of smartphone application interventions on physical activity level among uni-versity/college students: A systematic review protocol. Phys. Ther. Rev. 2020, 25, 135–142. [Google Scholar] [CrossRef]
- Young, C.L.; Trapani, K.; Dawson, S.; O’Neil, A.; Kay-Lambkin, F.; Berk, M.; Jacka, F.N. Efficacy of online lifestyle interventions targeting lifestyle behaviour change in depressed populations: A systematic review. Aust. N. Z. J. Psychiatry 2018, 52, 834–846. [Google Scholar] [CrossRef] [Green Version]
- Kaner, E.F.; Beyer, F.R.; Garnett, C.; Crane, D.; Brown, J.; Muirhead, C.; Redmore, J.; O’Donnell, A.; Newham, J.J.; de Vocht, F.; et al. Personalised digital interventions for reducing hazardous and harmful alcohol consumption in community-dwelling populations. Cochrane Database Syst. Rev. 2017, 9, Cd011479. [Google Scholar] [CrossRef] [Green Version]
- Newby, K.; Teah, G.; Cooke, R.; Li, X.; Brown, K.; Salisbury-Finch, B.; Kwah, K.; Bartle, N.; Curtis, K.; Fulton, E.; et al. Do automated digital health behaviour change interventions have a positive effect on self-efficacy? A systematic review and meta-analysis. Health Psychol. Rev. 2021, 15, 140–158. [Google Scholar] [CrossRef] [PubMed]
- Sanyal, C.; Stolee, P.; Juzwishin, D.; Husereau, D. Economic evaluations of eHealth technologies: A systematic review. PLoS ONE 2018, 13, e0198112. [Google Scholar] [CrossRef] [Green Version]
- Wantland, D.J.; Portillo, C.J.; Holzemer, W.L.; Slaughter, R.; McGhee, E.M. The effectiveness of Web-based vs. non-Web-based interventions: A meta-analysis of behavioural change outcomes. J. Med. Internet Res. 2004, 6, e40. [Google Scholar] [CrossRef] [PubMed]
- Enam, A.; Torres-Bonilla, J.; Eriksson, H. Evidence-Based Evaluation of eHealth Interventions: Systematic Literature Review. J. Med. Internet Res. 2018, 20, e10971. [Google Scholar] [CrossRef] [PubMed]
- Aarts, S.; Akker, M.V.D.; Winkens, B. The importance of effect sizes. Eur. J. Gen. Pract. 2014, 20, 61–64. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.J.; Choi, S.; Kim, S.-A.; Song, M. Intervention Strategies Based on Information-Motivation-Behavioural Skills Model for Health Behaviour Change: A Systematic Review. Asian Nurs. Res. 2014, 8, 172–181. [Google Scholar] [CrossRef] [Green Version]
- Michie, S.; Johnston, M. Behaviour Change Techniques. In Encyclopedia of Behavioural Medicine; Gellman, M.D., Turner, J.R., Eds.; Springer: New York, NY, USA, 2013; pp. 182–187. [Google Scholar]
- Murray, E. Web-Based Interventions for Behavior Change and Self-Management: Potential, Pitfalls, and Progress. Medicina 2012, 1, e3. [Google Scholar] [CrossRef]
| Components | Strong | Moderate | Weak |
|---|---|---|---|
| Selection bias | Very likely to be representative of the target population and greater than 80% participation rate | Somewhat likely to be representative of the target population and 60–79% participation rate | All other responses or not stated |
| Study design | RCT and CCT | Cohort analytic, case–control, cohort. Or an interrupted time series | All other designs or not stated |
| Confounders | Controlled for at least 80% of confounders | Controlled for 60–79% of confounders | Confounders not controlled for or not stated |
| Blinding | Blinding of outcome assessor and study participants to intervention status and/or research question | Blinding of either outcome assessor or study participants | Outcome assessor and study participants are aware of intervention status and/or research question |
| Data collection methods | Tools are valid and reliable | Tools are valid but reliability is not described | No evidence of validity or reliability |
| Withdrawals and drop-outs | Follow up rate >80% of participants | Follow-up rate of 60–79% of participants | Follow-up rate of <60% of participants or withdrawals and drop-outs not described |
| Author, Year | Section Rating | Global Rating | |||||
|---|---|---|---|---|---|---|---|
| Selection Bias | Study Design | Confounders | Blinding | Data Collection Methods | Withdrawals and Drop-Outs | ||
| Doumas, D. M. et al., (2021) [28] | WEAK | STRONG | STRONG | WEAK | STRONG | MODERATE | WEAK |
| Wilson, M. et al., (2017) [30] | WEAK | MODERATE | STRONG | WEAK | STRONG | MODERATE | WEAK |
| Larsen, B. et al., (2018) [31] | WEAK | MODERATE | STRONG | WEAK | STRONG | STRONG | WEAK |
| Khalil, G. E. et al., (2017) [32] | WEAK | STRONG | STRONG | WEAK | WEAK | NOT APPLICABLE | WEAK |
| Widman, L. et al., (2018) [33] | MODERATE | STRONG | STRONG | WEAK | WEAK | STRONG | WEAK |
| Coughlin, L. N. et al., (2021) [34] | WEAK | MODERATE | STRONG | WEAK | STRONG | STRONG | WEAK |
| Arnaud, N. et al., (2016) [35] | WEAK | STRONG | STRONG | WEAK | STRONG | WEAK | WEAK |
| Brown, K. E. et al., (2018) [36] | MODERATE | STRONG | STRONG | WEAK | STRONG | STRONG | MODERATE |
| Norman, P. et al., (2018) [37] | WEAK | STRONG | STRONG | WEAK | STRONG | WEAK | WEAK |
| Pirzadeh, A. et al., (2020) [38] | WEAK | STRONG | WEAK | WEAK | STRONG | STRONG | WEAK |
| Huang, S. J. et al., (2019) [39] | MODERATE | STRONG | STRONG | WEAK | MODERATE | WEAK | WEAK |
| Duan, Y. P. et al., (2017) [40] | MODERATE | STRONG | WEAK | WEAK | STRONG | WEAK | WEAK |
| Doubova, S. V. et al., (2017) [41] | WEAK | STRONG | STRONG | MODERATE | STRONG | STRONG | MODERATE |
| Castillo-Arcos Ldel, C. et al., (2016) [42] | WEAK | STRONG | STRONG | WEAK | WEAK | MODERATE | WEAK |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Sousa, D.; Fogel, A.; Azevedo, J.; Padrão, P. The Effectiveness of Web-Based Interventions to Promote Health Behaviour Change in Adolescents: A Systematic Review. Nutrients 2022, 14, 1258. https://doi.org/10.3390/nu14061258
de Sousa D, Fogel A, Azevedo J, Padrão P. The Effectiveness of Web-Based Interventions to Promote Health Behaviour Change in Adolescents: A Systematic Review. Nutrients. 2022; 14(6):1258. https://doi.org/10.3390/nu14061258
Chicago/Turabian Stylede Sousa, Daniela, Adriana Fogel, José Azevedo, and Patrícia Padrão. 2022. "The Effectiveness of Web-Based Interventions to Promote Health Behaviour Change in Adolescents: A Systematic Review" Nutrients 14, no. 6: 1258. https://doi.org/10.3390/nu14061258
APA Stylede Sousa, D., Fogel, A., Azevedo, J., & Padrão, P. (2022). The Effectiveness of Web-Based Interventions to Promote Health Behaviour Change in Adolescents: A Systematic Review. Nutrients, 14(6), 1258. https://doi.org/10.3390/nu14061258