
Health Behaviors of Austrian Secondary School Teachers and Principals at a Glance: First Results of the From Science 2 School Study Focusing on Sports Linked to Mixed, Vegetarian, and Vegan Diets †

 ,
,  ,
,  ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
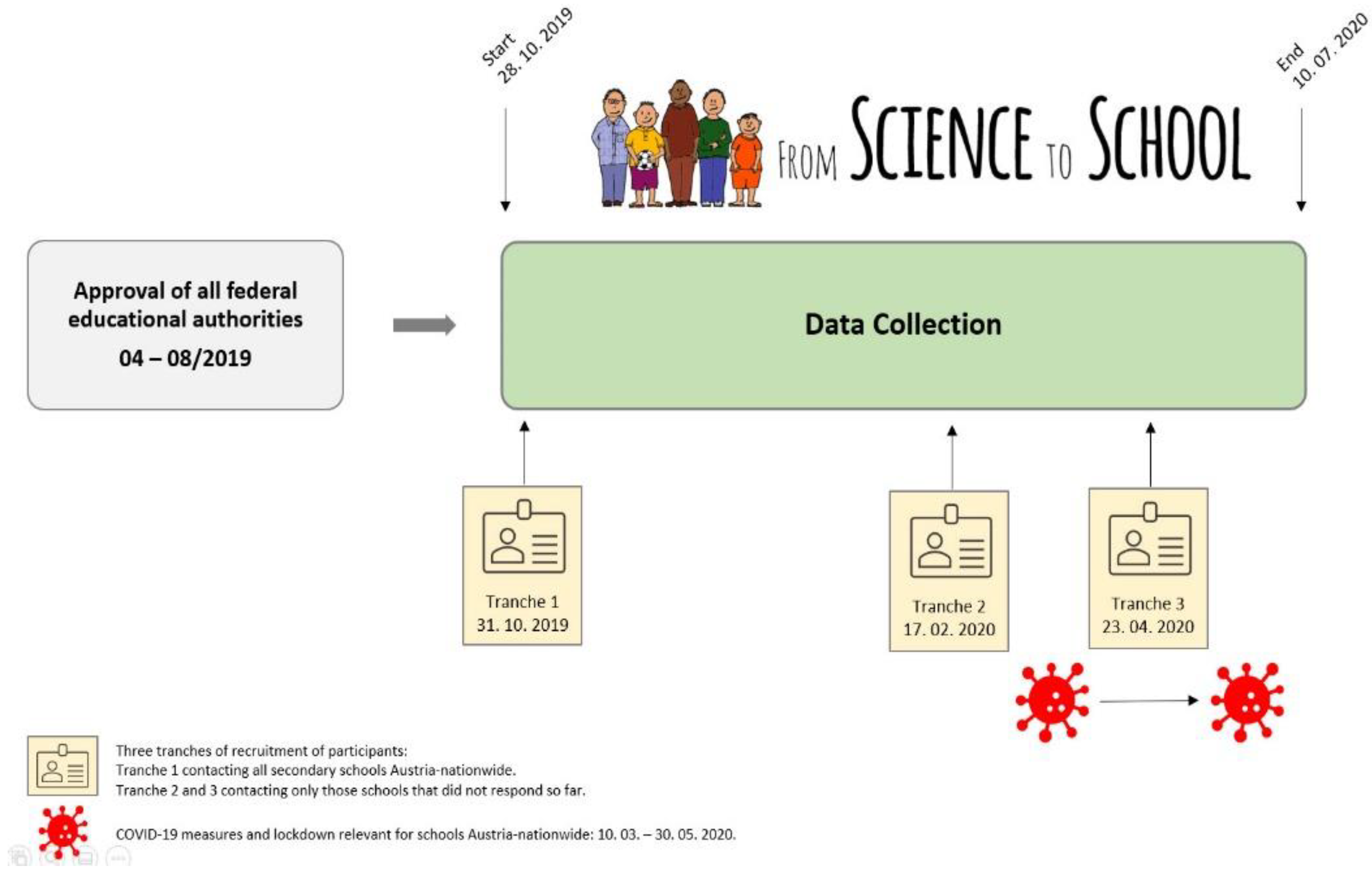
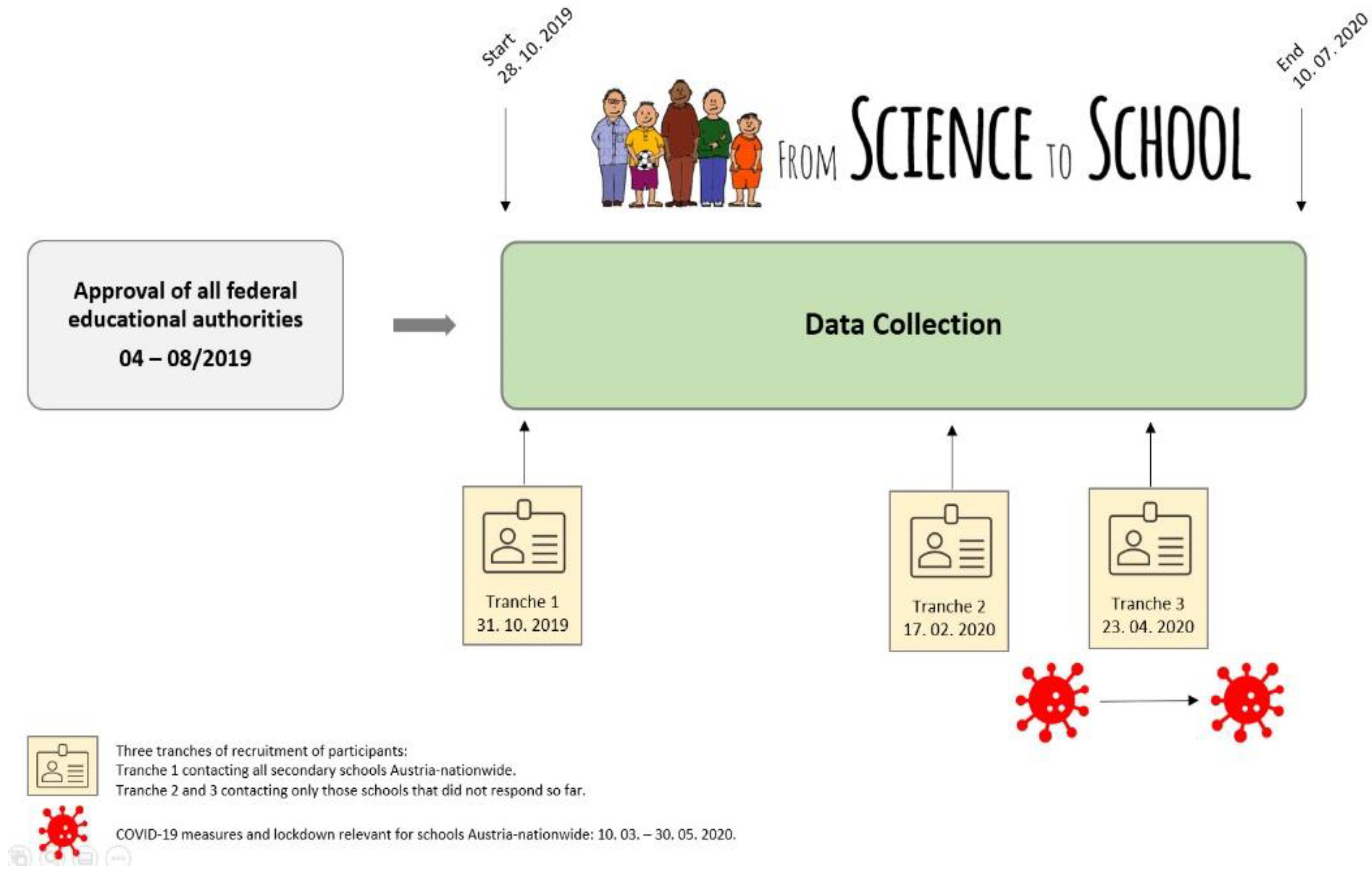
2.1. Study Protocol and Ethical Approval
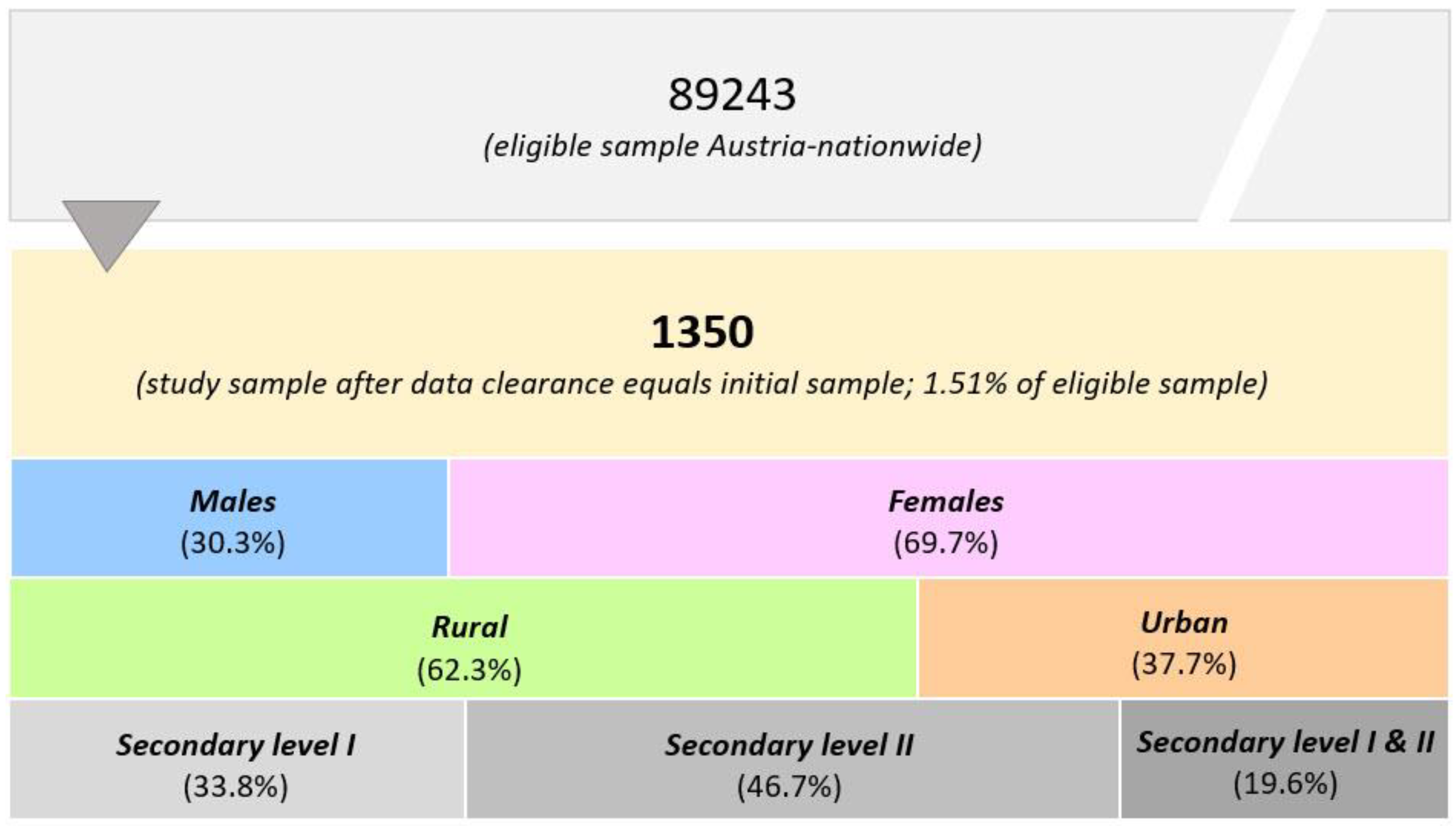
2.2. Participants
2.3. Procedures
2.4. Measures
2.5. Data Clearance
2.6. Statistical Analysis
3. Results
3.1. Anthropometric Characteristics
3.2. Sports Participation
3.3. Diet
3.4. Physical Activity and Health Behaviors
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| N | Age (Years) | Height (cm) | Body Weight (kg) | BMI (kg/m2) | Overweight/ Obesity (%) | |
|---|---|---|---|---|---|---|
| Burgenland | 151 | 44.4 ± 11.4 | 170.8 + 8.1 | 69.8 ± 14.0 | 23.8 ± 3.5 | 29.8 |
| Urban | 16 | 46.5 ± 9.5 | 169.5 + 6.1 | 68.9 ± 12.7 | 23.9 ± 3.7 | 31.3 |
| Rural | 135 | 44.1 ± 11.6 | 171.0 ± 8.3 | 69.9 ± 14.1 | 23.8 ± 3.5 | 29.6 |
| Carinthia | 52 | 47.5 ± 10.7 | 170.7 ± 7.7 | 69.4 ± 12.8 | 23.7 + 3.1 | 30.8 |
| Urban | 21 | 47.0 ± 10.9 | 171.1 ± 9.0 | 70.5 ± 14.3 | 23.9 ± 3.4 | 38.1 |
| Rural | 31 | 47.8 ± 10.7 | 170.3 ± 6.9 | 68.8 ± 11.9 | 23.6 ± 2.9 | 25.8 |
| Lower Austria | 231 | 46.4 ± 11.1 | 170.1 ± 8.6 | 73.3 ± 15.6 | 25.2 ± 4.5 | 43.7 |
| Urban | 51 | 48.6 ± 11.6 | 169.4 ± 9.0 | 71.3 ± 15.4 | 24.7 ± 3.8 | 39.2 |
| Rural | 180 | 45.8 ± 10.9 | 170.3 ± 8.4 | 73.8 + 15.6 | 25.4 ± 4.7 | 45.0 |
| Salzburg | 89 | 44.3 ± 11.8 | 172.2 ± 8.6 | 71.5 ± 13.4 | 24.0 ± 3.6 | 31.5 |
| Urban | 28 | 42.1 ± 12.5 | 169.8 ± 8.0 | 66.5 ± 11.9 | 23.0 ± 3.4 | 17.9 |
| Rural | 61 | 45.4 ± 11.4 | 173.3 ± 8.7 | 73.9 ± 13.5 | 24.5 ± 3.6 | 37.7 |
| Styria | 180 | 47.3 ± 12.2 | 171.5 ± 13.6 | 71.7 ± 13.6 | 24.3 ± 3.9 | 36.7 |
| Urban | 71 | 46.8 ± 12.4 | 171.3 ± 8.1 | 71.6 ± 13.7 | 24.3 ± 4.0 | 40.8 |
| Rural | 109 | 47.6 ±12.1 | 171.6 ± 8.6 | 71.8 ± 13.6 | 24.3 ± 3.9 | 33.9 |
| Tyrol | 190 | 46.0 ± 11.6 | 171.0 + 8.5 | 70.8 ± 14.3 | 24.1 ± 3.6 | 36.8 |
| Urban | 59 | 46.5 ± 12.0 | 171.1 ± 8.9 | 70.2 ± 13.6 | 23.8 ± 3.5 | 32.2 |
| Rural | 131 | 45.8 ± 11.5 | 170.9 ± 8.4 | 71.2 ± 14.6 | 24.2 ± 3.7 | 38.9 |
| Upper Austria | 176 | 46.1 ± 10.5 | 172.1 ± 8.0 | 72.3 ± 14.6 | 24.3 ± 3.9 | 35.8 |
| Urban | 50 | 45.4 + 11.4 | 172.8 ± 7.8 | 72.2 ± 11.8 | 24.1 ± 3.1 | 38.0 |
| Rural | 126 | 46.4 ± 10.2 | 171.8 ± 8.1 | 72.3 ± 15.6 | 24.3 ± 4.2 | 34.9 |
| Vienna | 138 | 45.2 ± 12.0 | 171.2 ± 7.6 | 70.3 ± 15.6 | 23.9 ± 4.5 | 27.7 |
| Urban | 138 | 45.2 ± 12.0 | 171.2 ± 7.6 | 70.3 ± 15.6 | 23.9 ± 4.5 | 27.7 |
| Rural | None | |||||
| Vorarlberg | 143 | 44.7 ± 11.0 | 171.7 ± 8.9 | 70.0 ± 15.2 | 23.6 ± 3.9 | 25.9 |
| Urban | 75 | 45.5 ± 10.5 | 171.2 ± 7.9 | 69.9 ± 13.2 | 23.8 ± 3.9 | 25.3 |
| Rural | 68 | 43.9 + 11.6 | 172.3 ± 10.0 | 70.1 ± 17.3 | 23.4 + 4.0 | 26.5 |
| N | Leisure-Time Sports (%) | Club Sports (%) | Days/Week with Sport (Mean ± SD) * | Daily Fruits (%) | Daily Veggies (%) | Fluid Intake >2 L/Day (%) | Water Most Common Fluid (%) | Vegetarian /Vegan (%) | Alcohol (%) | Smoking (%) | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Burgenland | 151 | 86.1 | 27.8 | 3.0 ± 1.3 | 58.9 | 62.9 | 25.8 | 79.5 | 12.6 | 78.1 | 6.6 |
| Urban | 16 | 87.5 | 31.3 | 2.1 ± 0.9 | 37.5 | 68.8 | 18.8 | 81.3 | 18.8 | 93.8 | 0.0 |
| Rural | 135 | 85.9 | 27.4 | 3.1 ± 1.4 | 61.5 | 62.2 | 26.7 | 79.3 | 11.9 | 76.3 | 7.4 |
| Carinthia | 52 | 88.5 | 25.0 | 3.3 ± 1.6 | 65.4 | 63.5 | 23.1 | 75.0 | 5.8 | 73.1 | 17.3 |
| Urban | 21 | 85.7 | 19.0 | 3.1 ± 1.4 | 61.9 | 47.6 | 28.6 | 90.5 | 4.8 | 71.4 | 23.8 |
| Rural | 31 | 90.3 | 29.0 | 3.4 ± 1.7 | 67.7 | 74.2 | 19.4 | 64.5 | 6.5 | 74.2 | 12.9 |
| Lower Austria | 231 | 86.6 | 24.2 | 2.8 ± 1.4 | 63.6 | 70.1 | 31.2 | 71.0 | 12.1 | 80.5 | 10.8 |
| Urban | 51 | 92.2 | 27.5 | 2.9 ± 1.3 | 64.7 | 72.5 | 27.5 | 74.5 | 15.7 | 88.2 | 3.9 |
| Rural | 180 | 85.0 | 23.3 | 2.8 ± 1.5 | 63.3 | 69.4 | 32.2 | 70.0 | 11.1 | 78.3 | 12.7 |
| Salzburg | 89 | 96.6 | 44.9 | 3.2 ± 1.6 | 68.5 | 80.7 | 34.8 | 76.4 | 13.5 | 86.5 | 9.0 |
| Urban | 28 | 96.4 | 39.3 | 3.5 ± 1.7 | 75.0 | 85.7 | 35.7 | 89.3 | 32.1 | 85.7 | 10.7 |
| Rural | 61 | 96.7 | 47.5 | 3.1 ± 1.6 | 65.6 | 78.3 | 34.4 | 70.5 | 4.9 | 86.9 | 8.2 |
| Styria | 180 | 87.2 | 26.1 | 2.8 ± 1.4 | 60.6 | 73.3 | 25.0 | 76.7 | 10.6 | 78.3 | 11.7 |
| Urban | 71 | 90.1 | 21.1 | 2.7 ± 1.3 | 50.7 | 74.6 | 29.6 | 73.2 | 14.1 | 90.1 | 9.9 |
| Rural | 109 | 85.3 | 29.4 | 2.9 ± 1.4 | 67.0 | 72.5 | 22.0 | 78.9 | 8.3 | 70.6 | 12.8 |
| Tyrol | 190 | 90.0 | 26.8 | 3.2 ± 1.5 | 68.9 | 70.0 | 28.4 | 77.9 | 7.4 | 84.7 | 7.4 |
| Urban | 59 | 86.4 | 18.6 | 3.1 ± 1.3 | 71.2 | 74.6 | 25.4 | 74.6 | 11.9 | 86.4 | 8.5 |
| Rural | 131 | 91.6 | 30.5 | 3.3 ± 1.6 | 67.9 | 67.9 | 29.8 | 79.4 | 5.3 | 84.0 | 6.9 |
| Upper Austria | 176 | 91.5 | 40.3 | 2.7 ± 1.4 | 55.1 | 74.4 | 22.7 | 75.6 | 11.9 | 85.2 | 12.5 |
| Urban | 50 | 88.0 | 36.0 | 2.5 ± 1.1 | 58.0 | 76.0 | 16.0 | 70.0 | 14.0 | 88.0 | 14.0 |
| Rural | 126 | 92.9 | 42.1 | 2.8 ± 1.4 | 54.0 | 73.8 | 25.4 | 76.6 | 11.1 | 84.1 | 11.9 |
| Vienna | 138 | 86.2 | 21.7 | 2.8 ± 1.4 | 63.8 | 78.3 | 27.5 | 76.8 | 10.1 | 76.1 | 15.9 |
| Urban | 138 | 86.2 | 21.7 | 2.8 ± 1.4 | 63.8 | 78.3 | 27.5 | 76.8 | 10.1 | 76.1 | 15.9 |
| Rural | None | ||||||||||
| Vorarlberg | 143 | 89.5 | 30.8 | 3.1 ± 1.5 | 60.1 | 76.2 | 23.1 | 78.3 | 11.2 | 86.7 | 11.9 |
| Urban | 75 | 90.7 | 29.3 | 3.0 ± 1.5 | 60.0 | 80.0 | 24.0 | 78.7 | 13.3 | 85.3 | 10.7 |
| Rural | 68 | 88.2 | 32.4 | 3.3 ± 1.5 | 60.3 | 72.1 | 22.1 | 77.9 | 8.8 | 88.2 | 13.2 |
References
- Organization for Economic Cooperation and Development. State of Health in the EU—Austria. Available online: https://ec.europa.eu/health/sites/default/files/state/docs/2019_chp_at_english.pdf (accessed on 14 December 2021).
- Perez-Lasierra, J.L.; Casajus, J.A.; González-Agüero, A.; Moreno-Franco, B. Association of physical activity levels and prevalence of major degenerative diseases: Evidence from the national health and nutrition examination survey (NHANES) 1999–2018. Exp. Gerontol. 2021, 158, 111656. [Google Scholar] [CrossRef] [PubMed]
- Duan, Y.; Shang, B.; Liang, W.; Du, G.; Yang, M.; Rhodes, R.E. Effects of eHealth-based multiple health behavior change interventions on physical activity, healthy diet, and weight in people with noncommunicable diseases: Systematic review and meta-analysis. J. Med. Internet Res. 2021, 23, e23786. [Google Scholar] [CrossRef] [PubMed]
- Myers, J.; McAuley, P.; Lavie, C.J.; Despres, J.P.; Arena, R.; Kokkinos, P. Physical activity and cardiorespiratory fitness as major markers of cardiovascular risk: Their independent and interwoven importance to health status. Prog. Cardiovasc. Dis. 2015, 57, 306–314. [Google Scholar] [CrossRef] [PubMed]
- Umegaki, H.; Sakurai, T.; Arai, H. Active life for brain health: A narrative review of the mechanism underlying the protective effects of physical activity on the brain. Front. Aging Neurosci. 2021, 13, 761674. [Google Scholar] [CrossRef]
- Jensen, C.T.; Heinze, C.; Andersen, P.K.; Bauman, A.; Klinker, C.D. Mental health and physical activity in vocational education and training schools students: A population-based survey. Eur. J. Public Health 2021, ckab202. [Google Scholar] [CrossRef]
- Skurvydas, A.; Lisinskiene, A.; Lochbaum, M.; Majauskiene, D.; Valanciene, D.; Dadeliene, R.; Fatkulina, N.; Sarkauskiene, A. Physical activity, stress, depression, emotional intelligence, logical thinking, and overall health in a large Lithuanian from October 2019 to June 2020: Age and gender differences adult sample. Int. J. Environ. Res. Public Health 2021, 18, 12809. [Google Scholar] [CrossRef]
- Casali, N.; Cerea, S.; Moro, T.; Paoli, A.; Ghisi, M. Just do it: High intensity physical activity preserves mental and physical health in elite and non-elite athletes during COVID-19. Front. Psychol. 2021, 12, 757150. [Google Scholar] [CrossRef]
- Jain, R.; Verma, V.; Rana, K.B.; Meena, M.L. Effect of physical activity intervention on the musculoskeletal health of university student computer users during homestay. Int. J. Occup. Saf. Ergon. 2021, 3, 1–19. [Google Scholar] [CrossRef]
- Parker, H.M.; Gallagher, R.; Duffield, C.; Ding, D.; Sibbritt, D.; Perry, L. Occupational and leisure-time physical activity have different relationships with health: A cross-sectional survey study of working nurses. J. Phys. Act. Health 2021, 1, 1–8. [Google Scholar] [CrossRef]
- Prince, S.A.; Rasmussen, C.L.; Biswas, A.; Holtermann, A.; Aulakh, T.; Merucci, K.; Coenen, P. The effect of leisure time physical activity and sedentary behaviour on the health of workers with different occupational physical activity demands: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2021, 18, 100. [Google Scholar] [CrossRef]
- Rusch, L.M.; Swede, H.; Dugan, A.G.; Cherniack, M.G.; Barnes-Farrell, J.; Cavallari, J.M. Leisure-time physical activity and general health mitigate effects of job demands on nonrestorative sleep: CDC National Healthy Worksite Project. J. Occup. Environ. Med. 2021, 63, 665–672. [Google Scholar] [CrossRef] [PubMed]
- Larsen, M.N.; Madsen, M.; Cyril, R.; Madsen, E.E.; Lind, R.R.; Ryom, K.; Christiansen, S.R.; Elbe, A.M.; Krustrup, P. Well-being, physical fitness and health profile of 10–12 years old boys in relation to leisure-time sports club activities: A cross-sectional study. BMJ Open 2021, 11, e050194. [Google Scholar] [CrossRef] [PubMed]
- Madsen, M.; Larsen, M.N.; Cyril, R.; Møller, T.K.; Madsen, E.E.; Ørntoft, C.; Lind, R.R.; Ryom, K.; Christiansen, S.R.; Wikman, J.; et al. Well-Being, physical fitness, and health profile of 2203 Danish girls aged 10–12 in relation to leisure-time sports club activity-with special emphasis on the five most popular sports. J. Strength Cond. Res. 2020. [Google Scholar] [CrossRef] [PubMed]
- Schroeder, E.C.; Welk, G.J.; Franke, W.D.; Lee, D.C. Associations of health club membership with physical activity and cardiovascular health. PLoS ONE 2017, 12, e0170471. [Google Scholar] [CrossRef]
- GBD-Diet-Collaborators. Health effects of dietary risks in 195 countries, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2019, 393, 1958–1972. [Google Scholar] [CrossRef] [Green Version]
- Cacau, L.T.; Benseñor, I.M.; Goulart, A.C.; Cardoso, L.O.; Lotufo, P.A.; Moreno, L.A.; Marchioni, D.M. Adherence to the planetary health diet index and obesity indicators in the Brazilian longitudinal study of adult health (ELSA-Brasil). Nutrients 2021, 13, 3691. [Google Scholar] [CrossRef] [PubMed]
- Cai, H.; Sobue, T.; Kitamura, T.; Ishihara, J.; Nanri, A.; Mizoue, T.; Iwasaki, M.; Yamaji, T.; Inoue, M.; Tsugane, S.; et al. Low-carbohydrate diet and risk of cancer incidence: The Japan Public Health Center-based prospective study. Cancer Sci. 2021, 113, 744. [Google Scholar] [CrossRef]
- Hlaing-Hlaing, H.; Dolja-Gore, X.; Tavener, M.; James, E.L.; Hodge, A.M.; Hure, A.J. Diet quality and incident non-communicable disease in the 1946–1951 cohort of the Australian longitudinal study on women‘s health. Int. J. Environ. Res. Public Health 2021, 18, 11375. [Google Scholar] [CrossRef]
- Danko, A.; Naughton, M.; Spees, C.; Bittoni, A.M.; Krok-Schoen, J.L. Diet quality and the number of comorbidities are associated with general health among older female cancer survivors. J. Aging Health 2021, 33, 908–918. [Google Scholar] [CrossRef]
- Melina, V.; Craig, W.; Levin, S. Position of the Academy of Nutrition and Dietetics: Vegetarian diets. J. Acad. Nutr. Diet 2016, 116, 1970–1980. [Google Scholar] [CrossRef]
- Leitzmann, C.; Keller, M. Vegetarische und Vegane Ernährung, 4th ed.; UTB: Stuttgart, Germany, 2020; pp. 95–117, 284–308, 309–399. [Google Scholar]
- Bloomer, R.J.; Gunnels, T.A.; Schriefer, J.M. Comparison of a restricted and unrestricted vegan diet plan with a restricted omnivorous diet plan on health-specific measures. Healthcare 2015, 3, 544–555. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larpin, C.; Wozniak, H.; Genton, L.; Serratrice, J. Alimentations végétariennes et véganes: Quelles conséquences sur la santé? [Vegetarian and vegan diets and their impact on health]. Rev. Med. Suisse. 2019, 15, 1849–1853. [Google Scholar] [PubMed]
- Motamed-Gorji, N.; Heshmat, R.; Qorbani, M.; Motlagh, M.E.; Soltani, A.; Shafiee, G.; Asayesh, H.; Ardalan, G.; Matin, N.; Mahdavi Gorabi, A.; et al. Is the association of weight disorders with perceived health status and life satisfaction independent of physical activity in children and adolescents? The CASPIAN-IV Study. J. Trop. Pediatr. 2019, 65, 249–263. [Google Scholar] [CrossRef] [PubMed]
- McCrorie, P.; Mitchell, R.; Macdonald, L.; Jones, A.; Coombes, E.; Schipperijn, J.; Ellaway, A. The relationship between living in urban and rural areas of Scotland and children‘s physical activity and sedentary levels: A country-wide cross-sectional analysis. BMC Public Health 2020, 20, 304. [Google Scholar] [CrossRef]
- Ramuth, H.; Schutz, Y.; Joonas, N.; Dulloo, A.G. Total energy expenditure assessed by doubly labeled water technique and estimates of physical activity in Mauritanian children: Analysis by gender and ethnicity. Eur. J. Clin. Nutr. 2020, 74, 445–453. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheung, P. Teachers as role models for physical activity: Are preschool children more active when their teachers are active? Eur. Phy. Educ. Rev. 2020, 26, 101–110. [Google Scholar] [CrossRef]
- Wong, L.S.; Gibson, A.-M.; Farooq, A.; Reilly, J.J. Interventions to increase moderate-to-vigorous physical activity in elementary school physical education lessons: Systematic review. J. Sch. Health 2021, 91, 836–845. [Google Scholar] [CrossRef]
- Eather, N.; Morgan, P.J.; Lubans, D.R. Social support from teachers mediates physical activity behavior change in children participating in the Fit-4-Fun intervention. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 68. [Google Scholar] [CrossRef] [Green Version]
- Karnik, S.; Kanekar, A. Childhood obesity: A global public health crisis. Int. J. Prev. Med. 2012, 3, 1–7. [Google Scholar]
- Salmon, J.; Koorts, H.; Timperio, A. Specific Interventions Targeting Sedentary Behaviour in Children and Adolescents. In Sedentary Behaviour Epidemiology, 1st ed.; Leitzmann, M., Jochem, C., Schmid, D., Eds.; Springer Nature: Cham, Switzerland, 2018; pp. 431–443. [Google Scholar]
- Hawkins, M.; Belson, S.I.; McClave, R.; Kohls, L.; Little, S.; Snelling, A. Healthy schoolhouse 2.0 health promotion intervention to reduce childhood obesity in Washington, DC: A feasibility study. Nutrients 2021, 13, 2935. [Google Scholar] [CrossRef]
- Lehrplan AHS Unterstufe (Sekundarstufe I) 2018. Inkraftretungsdatum: 9. Jänner 2018. Anlage A: Erster Teil. Allgemeines Bildungsziel, Punkt 5. Bildungsbereiche. Gesundheit und Bewegung. Available online: https://www.ris.bka.gv.at/GeltendeFassung/Bundesnormen/10008568/Lehrpl%c3%a4ne%20%e2%80%93%20allgemeinbildende%20h%c3%b6here%20Schulen%2c%20Fassung%20vom%2031.08.2017.pdf?FassungVom=2017-08-31 (accessed on 31 December 2021).
- Lehrplan AHS Oberstufe (Sekundarstufe II) 2018. Inkraftretungsdatum: 1. September 2018. Anlage D: Erster Teil. Allgemeines Bildungsziel, Punkt 5. Bildungsbereiche. Gesundheit und Bewegung. Available online: https://www.ris.bka.gv.at/GeltendeFassung.wxe?Abfrage=Bundesnormen&Gesetzesnummer=10008568&FassungVom=2018-09-01 (accessed on 31 December 2021).
- Lehrplan der Mittelschule. 2021. Available online: https://www.bmbwf.gv.at/Themen/schule/schulpraxis/lp/lp_ms.html (accessed on 31 December 2021).
- Lehrplan Primarstufe/Volksschule. 2012. Sechster Teil, Bildungs- & Lehraufgaben, Lehrstoff & Didaktische Grundsätze der Verbindlichen Übungen der Vorschulstufe. Allgemeine Bestimmungen; Bewegung und Sport, Gesundheitserziehung. Available online: https://www.bmbwf.gv.at/Themen/schule/schulpraxis/lp/lp_vs.html#heading_Allgemeine_Bestimmungen (accessed on 28 February 2022).
- Lehrplan Primarstufe/Volksschule. 2012. Siebenter Teil, Bildungs- und Lehraufgaben Sowie Lehrstoff und Didaktische Grundsätze der Pflichtgegenstände der Grundschule und der Volksschuloberstufe: Bewegung und Sport. Available online: https://www.bmbwf.gv.at/Themen/schule/schulpraxis/lp/lp_vs.html#heading_Gesamtstundenzahl_und_Stundenausmass (accessed on 28 February 2022).
- Felder-Puig, R.; Ramelow, D.; Maier, G.; Teutsch, F. Ergebnisse der WieNGS Lehrer/Innen-Befragung 2017; Institut für Gesundheitsförderung und Prävention: Wien, Austria, 2017. [Google Scholar]
- Hofmann, F.; Griebler, R.; Ramelow, D.; Unterweger, K.; Griebler, U.; Felder-Puig, R.; Dür, W. Gesundheit und Gesundheitsverhalten von Österreichs Lehrer/Innen: Ergebnisse der Lehrer/Innenbefragung 2010; LBIHPR Forschungsbericht; Bundesministerium für Gesundheit (BMG): Wien, Austria, 2012. [Google Scholar]
- Hofmann, F.; Felder-Puig, R. HBSC Factsheet Nr. 05/2013. In Gesundheitszustand und—Verhalten Österreichischer Lehrkräfte: Ergebnisse der Lehrer/Innen-Gesundheitsbefragung 2010; LBIHPR Forschungsbericht; Bundesministerium für Gesundheit (BMG): Wien, Austria, 2013. [Google Scholar]
- Steen, R. Lehrer/innen stark machen!—Nachdenken über Gesundheit in der Schule. Ein Beitrag aus Sicht der Gesundheitsförderung. Make Teachers Stronger!—Considerations on Health in Schools. A Contribution from the Viewpoint of Health Promotion. Gesundheitswesen 2011, 73, 112–116. [Google Scholar] [CrossRef] [PubMed]
- Teutsch, F.; Hofmann, F.; Felder-Puig, R. Kontext und Praxis schulischer Gesundheitsförderung. In Ergebnisse der Österreichischen Schulleiter/Innenbefragung 2014; LBIHPR Forschungsbericht; Bundesministerium für Gesundheit (BMG): Wien, Austria, 2015. [Google Scholar]
- Nieskens, B.; Rupprecht, S.; Erbring, S. Was hält Lehrkräfte gesund? Ergebnisse der Gesundheitsforschung für Lehrkräfte und Schulen. In Handbuch Lehrergesundheit Impulse für die Entwicklung Guter Gesunder Schulen; Eine Veröffentlichung der DAK-Gesundheit und der Unfallkasse Nordrhein-Westfalen; Carl Link (Wolters Kuiwer): Köln, Germany, 2012; pp. 31–96, 217. [Google Scholar]
- Wirnitzer, K.C.; Drenowatz, C.; Cocca, A.; Tanous, D.R.; Motevalli, M.; Wirnitzer, G.; Schätzer, M.; Ruedl, G.; Kirschner, W. Health behaviors of Austrian secondary level pupils at a glance: First results of the from science 2 school study focusing on sports linked to mixed, vegetarian, and vegan diets. Int. J. Environ. Res. Public Health 2021, 18, 12782. [Google Scholar] [CrossRef] [PubMed]
- Wirnitzer, K.; Tanous, D.R.; Motevalli, M.; Göbel, G.; Wirnitzer, G.; Ruedl, G.; Kirschner, W. Health behavior with a special focus on the prevalence of omnivorous, vegetarian and vegan diets linked to sports and physical exercise among Austrian pupils, teachers and principals of secondary level I and II—From Science 2 School Study Protocol. Front. Public Health, 2021; under review. [Google Scholar]
- Rothland, M.; Klusmann, U. Belastung und Beanspruchung im Lehrerberuf. In Enzyklopädie Erziehungswissenschaft Online (EEO); Rahm, S., Nerowski, C., Eds.; Fachgebiet Schulpädagogik; Juventa: Weinheim, Germany, 2012. [Google Scholar]
- McKinsey & Company. Available online: https://www.mckinsey.com/industries/education/our-insights/how-the-worlds-best-performing-school-systems-come-out-on-top (accessed on 28 December 2021).
- Wirnitzer, K.C.; Drenowatz, C. Improving Child & Adolescent Health for better Public Health—Fiction or within the scope of possibility? The perspective of a lifestyle-centered approach for Addressing Today’s Global Health Paradox. In International Research & Knowledge Exchange for Addressing Today’s Global Health Paradox, 1st ed.; Wirnitzer, K., Drenowatz, C., Kirschner, W., Tanous, D., Rosemann, T., Eds.; Editorial Meeting 2; Frontiers in Public Health: Lausanne, Switzerland, 2020; pp. 45–47. [Google Scholar]
- Nanakorn, S.; Osaka, R.; Chusilp, K.; Tsuda, A.; Maskasame, S.; Ratanasiri, A. Gender differences in health-related practices among university students in northeast Thailand. Asia Pac. J. Public Health 1999, 11, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Bärebring, L.; Palmqvist, M.; Winkvist, A.; Augustin, H. Gender differences in perceived food healthiness and food avoidance in a Swedish population-based survey: A cross sectional study. Nutr. J. 2020, 19, 140. [Google Scholar] [CrossRef]
- Ek, S. Gender differences in health information behaviour: A Finnish population-based survey. Health Promot. Int. 2015, 30, 736–745. [Google Scholar] [CrossRef] [Green Version]
- Kanter, R.; Caballero, B. Global gender disparities in obesity: A review. Adv. Nutr. 2012, 3, 491–498. [Google Scholar] [CrossRef]
- Ameye, H.; Swinnen, J. Obesity, Income and Gender: The Changing Global Relationship; LICOS Discussion Paper, No. 415; Katholieke Universiteit Leuven, LICOS Centre for Institutions and Economic Performance: Leuven, Belgium, 2019. [Google Scholar]
- Center of Disease Control and Prevention. Body Mass Index: Considerations for Practitioners. Available online: https://www.cdc.gov/obesity/downloads/bmiforpactitioners.pdf (accessed on 12 November 2021).
- NCD Risk Factor Collaboration (NCD-RisC). Trends in adult body-mass index in 200 countries from 1975 to 2014: A pooled analysis of 1698 population-based measurement studies with 19·2 million participants. Lancet 2016, 387, 1377–1396. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Xu, L.; Li, J.; Sun, L.; Qin, W.; Ding, G.; Wang, Q.; Zhu, J.; Yu, Z.; Xie, S.; et al. Gender differences in the association between body mass index and health-related quality of life among adults: A cross-sectional study in Shandong, China. BMC Public Health 2019, 19, 1021. [Google Scholar] [CrossRef] [Green Version]
- Subhaluksuksakorn, P.; Sinjariyanon, W.; Pimsaran, R. Gender difference in underweight, overweight and obesity among first-year students of Suranaree University of Technology in 2015. J. Med. Assoc. Thai. 2016, 99, S24–S29. [Google Scholar]
- Averett, S.L.; Stacey, N.; Wang, Y. Decomposing race and gender differences in underweight and obesity in South Africa. Econ. Hum. Biol. 2014, 15, 23–40. [Google Scholar] [CrossRef]
- Jenkins, P.E.; Morgan, C.; Houlihan, C. Outpatient CBT for underweight patients with eating disorders: Effectiveness within a National Health Service (NHS) eating disorders service. Behav. Cogn. Psychother. 2019, 47, 217–229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Commission—Austria Physical Activity Fact Sheet. Available online: https://fgoe.org/sites/fgoe.org/files/inline-files/AUSTRIA-Physical-Activity-Factsheet.pdf (accessed on 17 December 2021).
- World Health Organization (WHO). Austria Physical Activity Factsheet 2018. Available online: https://www.euro.who.int/__data/assets/pdf_file/0009/382338/austria-eng.pdf (accessed on 17 December 2021).
- Center for Disease Control and Prevention. Ho Much Physical Activity Do Adults Need? Available online: https://www.cdc.gov/physicalactivity/basics/adults/index.htm (accessed on 15 December 2021).
- National Health Service. Physical Activity Guidelines for Adults Aged 19 to 64. Available online: https://www.nhs.uk/live-well/exercise/ (accessed on 15 December 2021).
- American Heart Association. Available online: https://www.heart.org/en/healthy-living/fitness/fitness-basics/aha-recs-for-physical-activity-in-adults (accessed on 15 December 2021).
- World Health Organization (WHO). Global Recommendations on Physical Activity for Health. Available online: https://www.who.int/publications/i/item/9789241599979 (accessed on 30 December 2021).
- Su, C.; Jia, X.F.; Wang, Z.H.; Wang, H.J.; Ouyang, Y.F.; Zhang, B. Longitudinal association of leisure time physical activity and sedentary behaviors with body weight among Chinese adults from China Health and Nutrition Survey 2004–2011. Eur. J. Clin. Nutr. 2017, 71, 383–388. [Google Scholar] [CrossRef]
- Quist, J.S.; Rosenkilde, M.; Petersen, M.B.; Gram, A.S.; Sjödin, A.; Stallknecht, B. Effects of active commuting and leisure-time exercise on fat loss in women and men with overweight and obesity: A randomized controlled trial. Int. J. Obes. 2018, 42, 469–478. [Google Scholar] [CrossRef] [PubMed]
- Schäfer, C.; Mayr, B.; Fernandez La Puente de Battre, M.D.; Reich, B.; Schmied, C.; Loidl, M.; Niederseer, D.; Niebauer, J. Health effects of active commuting to work: The available evidence before GISMO. Scand. J. Med. Sci. Sports 2020, 30, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Sattler, M.C.; Färber, T.; Traußnig, K.; Köberl, G.; Paier, C.; Dietz, D.; van Poppel, M.N.M. Cross-sectional association between active commuting and perceived commuting stress in Austrian adults: Results from the HOTway study. Ment. Health Phys. Act. 2020, 19, 100356. [Google Scholar] [CrossRef]
- Wirnitzer, K.; Boldt, P.; Lechleitner, C.; Wirnitzer, G.; Leitzmann, C.; Rosemann, T.; Knechtle, B. Health status of female and male vegetarian and vegan endurance runners compared to omnivores—results from the NURMI Study (Step 2). Nutrients 2018, 11, 29. [Google Scholar] [CrossRef] [Green Version]
- Cardoso, L.S.M.; Gomes, C.S.; Moreira, A.D.; Bernal, R.T.I.; Ribeiro, A.L.P.; Malta, D.C. Fruit and vegetable consumption, leisure-time physical activity and binge drinking in Belo Horizonte, Brazil, according to the Health Vulnerability Index. Rev. Bras. Epidemiol. 2021, 24, e210013. [Google Scholar] [CrossRef]
- van der Avoort, C.M.T.; Ten Haaf, D.S.M.; de Vries, J.H.M.; Verdijk, L.B.; van Loon, L.J.C.; Eijsvogels, T.M.H.; Hopman, M.T.E. Higher levels of physical activity are associated with greater fruit and vegetable intake in older adults. J. Nutr. Health Aging 2021, 25, 230–241. [Google Scholar] [CrossRef] [PubMed]
- de Visser, R.O.; Conroy, D.; Davies, E.; Cooke, R. Understanding motivation to adhere to guidelines for alcohol intake, physical activity, and fruit and vegetable intake among U.K. university students. Health Educ. Behav. 2021, 48, 480–487. [Google Scholar] [CrossRef]
- Turner-McGrievy, G.M.; Davidson, C.R.; Wingard, E.E.; Wilcox, S.; Frongillo, E.A. Comparative effectiveness of plant-based diets for weight loss: A randomized controlled trial of five different diets. Nutrition 2015, 31, 350–358. [Google Scholar] [CrossRef]
- Medawar, E.; Huhn, S.; Villringer, A.; Witte, V. The effects of plant-based diets on the body and the brain: A systematic review. Transl. Psychiatry 2019, 9, 226. [Google Scholar] [CrossRef] [PubMed]
- Wirnitzer, K.C. Vegan diet in sports and exercise. health benefits and advantages to athletes and physically active people. A narrative review. Int. J. Sports Exerc. Med. 2020, 6, 165. [Google Scholar]
- Leitzmann, C. Veganimus. Grundlagen, Vorteile, Risiken, 1st ed.; CH Beck: München, Germany, 2018; pp. 105–106. [Google Scholar]
- Halkjær, J.; Olsen, A.; Overvad, K.; Jakobsen, M.U.; Boeing, H.; Buijsse, B.; Palli, D.; Tognon, G.; Du, H.; van der A, D.L.; et al. Intake of total, animal and plant protein and subsequent changes in weight or waist circumference in European men and women: The Diogenes project. Int. J. Obes. 2011, 35, 1104–1113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tucker, L.A.; Tucker, J.M.; Bailey, B.; LeCheminant, J.D. Meat intake increases risk of weight gain in women: A prospective cohort investigation. Am. J. Health Promot. 2014, 29, e43–e52. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.H.; Kang, J.G.; Lee, S.J.; Han, K.D.; Ihm, S.H.; Cho, K.H.; Park, Y.G. Underweight increases the risk of end-stage renal diseases for type 2 diabetes in Korean population: Data from the National Health Insurance Service Health Checkups 2009–2017. Diabetes Care 2020, 43, 1118–1125. [Google Scholar] [CrossRef]
- NHS. Underweight Adults. Available online: https://www.nhs.uk/live-well/healthy-weight/managing-your-weight/advice-for-underweight-adults/ (accessed on 19 December 2021).
- Mengesha Kassie, A.; Beletew Abate, B.; Wudu Kassaw, M.; Gebremeskel Aragie, T. Prevalence of underweight and its associated factors among reproductive age group women in Ethiopia: Analysis of the 2016 Ethiopian demographic and health survey data. J. Environ. Public Health 2020, 2020, 9718714. [Google Scholar] [CrossRef]
- Gutin, I. In BMI we trust: Reframing the body mass index as a measure of health. Soc. Theory Health 2018, 16, 256–271. [Google Scholar] [CrossRef] [PubMed]
- Freigang, R.; Geier, A.K.; Schmid, G.L.; Frese, T.; Klement, A.; Unverzagt, S. Misclassification of self-reported Body Mass Index categories. Dtsch. Ärzteblatt Int. 2020, 117, 253–260. [Google Scholar] [CrossRef]
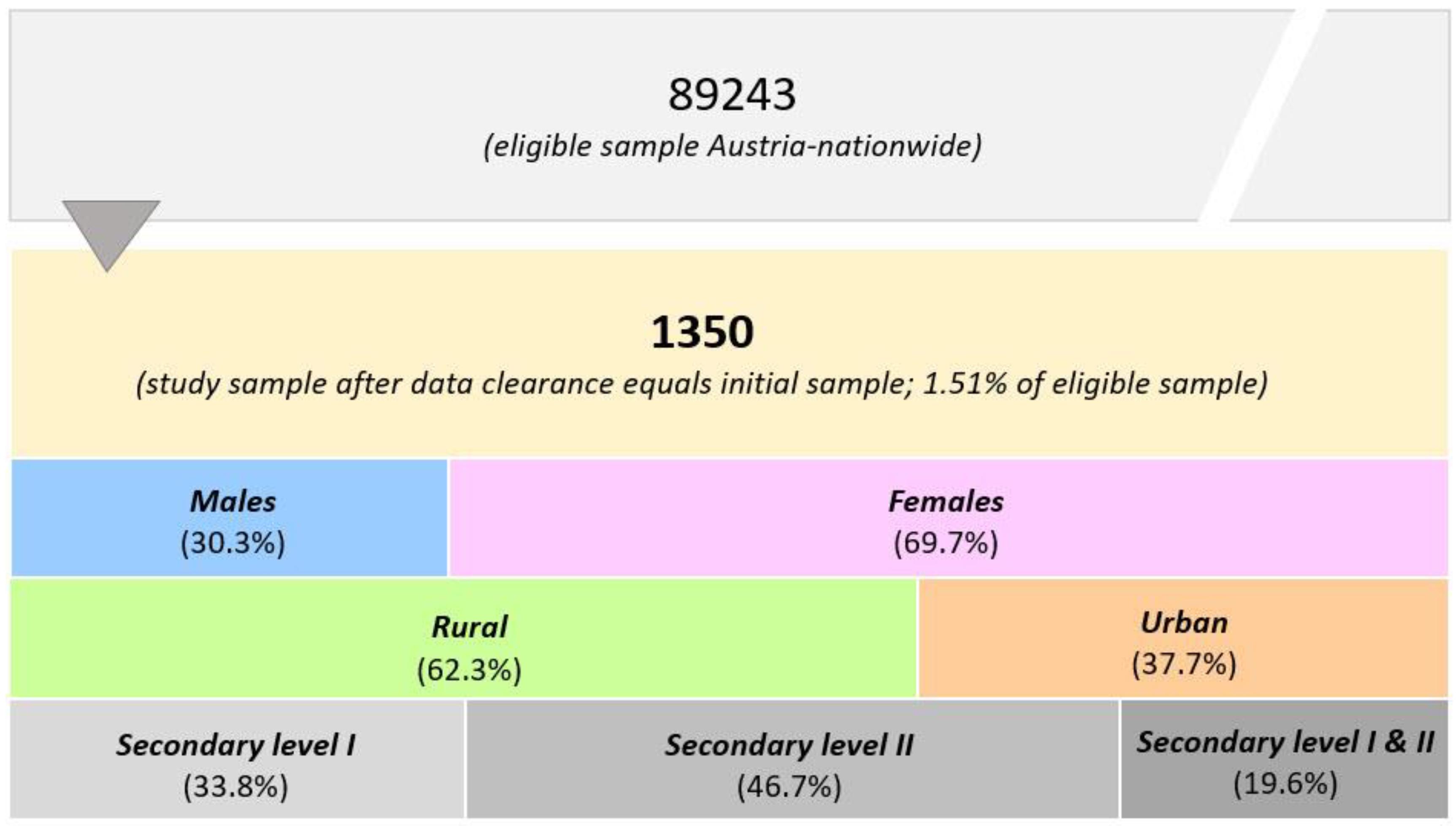
| Total (N) | Male N (%) | Female N (%) | Secondary Level I N (%) | Secondary Level II N (%) | Secondary Level I & II N (%) | |
|---|---|---|---|---|---|---|
| 1350 | 409 (30.3) | 941 (69.7) | 456 (33.8) | 630 (46.7) | 264 (19.6) | |
| Living Environment | ||||||
| Urban | 509 | 150 (29.5) | 359 (70.5) | 126 (24.8) | 247 (48.5) | 136 (26.7) |
| Rural | 841 | 259 (30.8) | 582 (69.2) | 330 (39.2) | 383 (45.5) | 128 (15.2) |
| Nationality | ||||||
| Austrian | 1318 | 398 (30.2) | 920 (69.8) | 446 (33.8) | 619 (47.0) | 253 (19.2) |
| Other | 32 | 11 (34.4) | 21 (65.5) | 10 (31.3) | 11 (34.4) | 11 (34.4) |
| School Type | ||||||
| Middle School | 485 | 133 (27.4) | 352 (72.6) | X | ||
| AHS | 216 | 80 (37.0) | 136 (63.0) | X | X | X |
| Middle School and AHS | 6 | 3 (50.0) | 3 (50.0) | X | X | |
| Prevocational School | 44 | 23 (52.3) | 21 (47.7) | X | ||
| AHS and BMS | 117 | 37 (31.6) | 80 (68.4) | X | ||
| AHS and BHS | 22 | 4 (18.2) | 18 (81.8) | X | X | |
| Sec. Tech. and Voc. School (BMS, 4 years) | 86 | 33 (38.4) | 53 (61.6) | X | ||
| Sec. Tech. and Voc. School (BHS, 5 years) | 313 | 91 (29.1) | 222 (70.9) | X | ||
| Other | 61 | 5 (8.2) | 56 (91.8) | X | X | X |
| Total | Male | Female | Secondary Level I | Secondary Level II | Secondary Level I and II | |
|---|---|---|---|---|---|---|
| Age (years) | 45.8 ± 11.4 | 47.3 ± 11.4 | 45.2 ± 11.4 | 45.6 ± 12.0 | 46.7 ± 11.0 | 43.9 ± 11.3 |
| Urban | 45.9 ± 11.6 | 46.2 ± 11.7 | 45.8 ± 11.6 | 46.2 ± 12.5 | 47.0 ± 11.3 | 43.7 ± 11.2 |
| Rural | 45.7 ± 11.3 | 48.0 ± 11.1 | 44.7 ± 11.2 | 45.4 ± 11.8 | 46.6 ± 10.7 | 44.2 ± 11.5 |
| Body Weight (kg) 1,2 | 71.3 ± 14.6 | 82.6 ± 12.6 | 66.4 ± 12.5 | 70.4 ± 14.3 | 71.9 ± 15.0 | 71.4 ± 14.0 |
| Urban | 70.5 ± 14.0 | 80.8 ± 12.5 | 66.1 ± 12.3 | 70.5 ± 13.7 | 70.4 ± 14.4 | 70.6 ± 13.8 |
| Rural | 71.8 ± 14.9 | 83.6 ± 12.5 | 66.5 ± 12.6 | 70.4 ± 14.5 | 72.8 ± 15.3 | 72.3 ± 14.3 |
| Height (cm) 2 | 171.2 ± 8.3 | 179.8 ± 6.7 | 167.4 ± 5.8 | 170.4 ± 7.8 | 171.6 ± 8.7 | 171.6 ± 8.2 |
| Urban | 171.0 ± 8.1 | 179.5 ± 6.9 | 167.5 ± 5.5 | 170.8 ± 8.0 | 170.7 ± 8.2 | 171.9 ± 7.9 |
| Rural | 171.3 ± 8.5 | 180.0 ± 6.6 | 167.4 ± 5.9 | 170.2 ± 7.7 | 172.2 ± 9.0 | 171.3 ± 8.4 |
| BMI (kg/m2) 1 | 24.2 ± 4.0 | 25.5 ± 3.4 | 23.6 ± 4.1 | 24.2 ± 4.1 | 24.3 ± 3.9 | 24.2 ± 3.9 |
| Urban | 24.0 ± 3.9 | 25.0 ± 3.3 | 23.5 ± 4.1 | 24.1 ± 3.9 | 24.0 ± 3.9 | 23.8 ± 3.9 |
| Rural | 24.3 ± 4.0 | 25.8 ± 3.4 | 23.7 ± 4.1 | 24.2 ± 4.2 | 24.4 ± 3.9 | 24.5 ± 3.9 |
| Underweight (%) | 2.6 | 0.0 | 3.7 | 3.1 | 2.5 | 1.9 |
| Urban | 3.0 | 0.0 | 4.1 | 2.4 | 3.2 | 3.0 |
| Rural | 2.4 | 0.0 | 3.4 | 3.3 | 2.1 | 0.8 |
| Normal Weight (%) | 63.0 | 53.5 | 67.1 | 61.6 | 62.1 | 67.7 |
| Urban | 65.2 | 59.3 | 67.6 | 61.1 | 64.8 | 69.6 |
| Rural | 61.7 | 50.2 | 66.8 | 61.8 | 60.3 | 65.6 |
| Overweight (%) | 25.6 | 36.2 | 21.0 | 26.5 | 27.3 | 19.8 |
| Urban | 22.6 | 31.3 | 19.8 | 29.4 | 23.5 | 17.0 |
| Rural | 27.0 | 39.0 | 21.6 | 25.5 | 29.8 | 22.6 |
| Obese (%) | 8.8 | 10.3 | 8.2 | 8.8 | 8.1 | 10.6 |
| Urban | 8.7 | 9.3 | 8.4 | 7.1 | 8.5 | 10.4 |
| Rural | 8.9 | 10.8 | 8.1 | 9.4 | 7.8 | 10.9 |
| Leisure-Time Sports N (%) | Club Sports N (%) | Sport Days/Week Mean ± SD | |
|---|---|---|---|
| Total Sample | 1198 (88.7) | 384 (29.2) | 2.9 ± 1.5 |
| Male | 372 (91.0) | 160 (39.1) | 3.1 ± 1.5 |
| Female | 826 (87.8) | 234 (24.9) | 2.9 ± 1.4 |
| Teaching Levels | |||
| Secondary Level I | 408 (89.5) | 139 (30.5) | 2.9 ± 1.4 |
| Secondary Level II | 556 (88.3) | 167 (26.5) | 2.9 ± 1.5 |
| Both (Level I and II) | 234 (88.6) | 88 (33.3) | 3.1 ± 1.5 |
| Living Environment | |||
| Urban | 452 (88.8) | 130 (25.5) | 2.9 ± 1.4 |
| Rural | 746 (88.7) | 264 (31.4) | 3.0 ± 1.5 |
| Nationality | |||
| Austria | 1170 (88.8) | 387 (29.4) | 2.9 ± 1.4 |
| Other | 28 (87.5) | 7 (21.9) | 3.1 ± 1.6 |
| Leisure-Time Sports | Club Sports | |||
|---|---|---|---|---|
| Yes | No | Yes | No | |
| Age (years) | 45.8 ± 11.5 | 45.8 ± 10.9 | 45.7 ± 11.4 | 45.9 ± 11.4 |
| Height (cm) 2 | 171.2 ± 8.2 | 171.1 ± 9.1 | 172.7 ± 8.3 | 170.6 ± 8.2 |
| Body Weight (kg) 1 | 70.7 ± 13.9 | 76.1 ± 18.2 | 71.8 ± 14.0 | 71.1 ± 14.8 |
| BMI (kg/m2) 1 | 24.0 ± 3.7 | 25.9 ± 5.4 | 24.0 ± 3.6 | 24.3 ± 4.1 |
| BMI Subgroups (%) | ||||
| Underweight (%) 1 | 2.3 | 4.6 | 1.5 | 3.0 |
| Normal weight (%) 1,2 | 65.7 | 41.7 | 68.8 | 60.6 |
| Overweight (%) 1 | 24.5 | 34.4 | 23.1 | 26.6 |
| Obese (%) 1,2 | 7.5 | 19.2 | 6.6 | 9.7 |
| Mixed Diet N (%) | Vegetarian N (%) | Vegan N (%) | |
|---|---|---|---|
| Total Sample | 1205 (89.3) | 106 (7.9) | 39 (2.9) |
| Male | 384 (93.9) | 14 (3.4) | 11 (2.7) |
| Female | 821 (87.2) | 92 (9.8) | 28 (3.0) |
| Teaching Levels | |||
| Secondary Level I | 399 (87.5) | 44 (9.6) | 13 (2.9) |
| Secondary Level II | 568 (90.2) | 45 (7.1) | 17 (2.7) |
| Both (Level I and II) | 238 (90.2) | 17 (6.4) | 9 (3.4) |
| Living Environment | |||
| Urban | 442 (86.8) | 46 (9.0) | 21 (4.1) |
| Rural | 763 (90.7) | 60 (7.1) | 18 (2.1) |
| Nationality | |||
| Austria | 1177 (89.3) | 103 (7.8) | 38 (2.9) |
| Other | 28 (87.5) | 3 (9.4) | 1 (3.1) |
| Mixed Diet | Vegetarian | Vegan | |
|---|---|---|---|
| Age (years) 2 | 45.9 ± 11.4 | 45.0 ± 10.7 | 44.2 ± 12.3 |
| Height (cm) 1 | 171.3 ± 8.3 | 169.2 ± 6.9 | 172.2 ± 10.9 |
| Body Weight (kg) 1 | 71.8 ± 14.5 | 66.4 ± 11.1 | 71.3 ± 14.6 |
| BMI (kg/m2) 1,2 | 24.4 ± 4.0 | 23.1 ± 3.2 | 22.7 ± 4.3 |
| BMI Subgroups (%) | |||
| Underweight (%) 1,2 | 2.2 | 2.8 | 15.4 |
| Normal Weight (%) 2,3 | 62.6 | 69.8 | 56.4 |
| Overweight (%) | 25.9 | 23.6 | 20.5 |
| Obese (%) 1,3 | 9.3 | 3.8 | 7.7 |
| Leisure-Time Sports | Club Sports | Sport Days/Week | |||||
|---|---|---|---|---|---|---|---|
| Yes | No | Yes | No | None | 1–3 Days | 4–7 Days | |
| Daily Fruit 1,3 | 63.9 | 50.7 | 61.4 | 62.8 | 50.3 | 60.5 | 72.4 |
| Daily vegetable 1,3 | 74.2 | 56.6 | 72.1 | 72.3 | 56.9 | 72.3 | 78.9 |
| Fluid Intake (>2 L/day) 1,2,3 | 28.5 | 15.1 | 34.8 | 23.7 | 15.0 | 23.1 | 41.9 |
| Water as most common drink | 76.5 | 73.0 | 76.4 | 76.0 | 73.2 | 75.2 | 79.8 |
| Alcohol 1 | 82.3 | 75.0 | 82.0 | 81.3 | 75.2 | 83.5 | 79.2 |
| Smoking 1,3 | 10.1 | 17.8 | 9.6 | 11.5 | 18.3 | 10.5 | 8.5 |
| Mixed Diet | Vegetarian | Vegan | |
|---|---|---|---|
| Leisure-time sports participation | 88.9 | 88.7 | 83.9 |
| Club sports participation | 29.8 | 22.6 | 29.0 |
| Fluid Intake (>2 L/day) | 26.4 | 32.2 | 29.0 |
| Water as most common drink 1,2,3 | 76.2 | 80.9 | 58.1 |
| Alcohol 2 | 82.0 | 74.8 | 87.1 |
| Smoking | 11.3 | 7.8 | 9.7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wirnitzer, K.C.; Drenowatz, C.; Cocca, A.; Tanous, D.R.; Motevalli, M.; Wirnitzer, G.; Schätzer, M.; Ruedl, G.; Kirschner, W. Health Behaviors of Austrian Secondary School Teachers and Principals at a Glance: First Results of the From Science 2 School Study Focusing on Sports Linked to Mixed, Vegetarian, and Vegan Diets. Nutrients 2022, 14, 1065. https://doi.org/10.3390/nu14051065
Wirnitzer KC, Drenowatz C, Cocca A, Tanous DR, Motevalli M, Wirnitzer G, Schätzer M, Ruedl G, Kirschner W. Health Behaviors of Austrian Secondary School Teachers and Principals at a Glance: First Results of the From Science 2 School Study Focusing on Sports Linked to Mixed, Vegetarian, and Vegan Diets. Nutrients. 2022; 14(5):1065. https://doi.org/10.3390/nu14051065
Chicago/Turabian StyleWirnitzer, Katharina C., Clemens Drenowatz, Armando Cocca, Derrick R. Tanous, Mohamad Motevalli, Gerold Wirnitzer, Manuel Schätzer, Gerhard Ruedl, and Werner Kirschner. 2022. "Health Behaviors of Austrian Secondary School Teachers and Principals at a Glance: First Results of the From Science 2 School Study Focusing on Sports Linked to Mixed, Vegetarian, and Vegan Diets" Nutrients 14, no. 5: 1065. https://doi.org/10.3390/nu14051065
APA StyleWirnitzer, K. C., Drenowatz, C., Cocca, A., Tanous, D. R., Motevalli, M., Wirnitzer, G., Schätzer, M., Ruedl, G., & Kirschner, W. (2022). Health Behaviors of Austrian Secondary School Teachers and Principals at a Glance: First Results of the From Science 2 School Study Focusing on Sports Linked to Mixed, Vegetarian, and Vegan Diets. Nutrients, 14(5), 1065. https://doi.org/10.3390/nu14051065