
Reducing Metabolic Syndrome through a Group Educational Intervention Program in Adults with Obesity: IGOBE Program

 , ,
, ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participant Selection and Recruitment
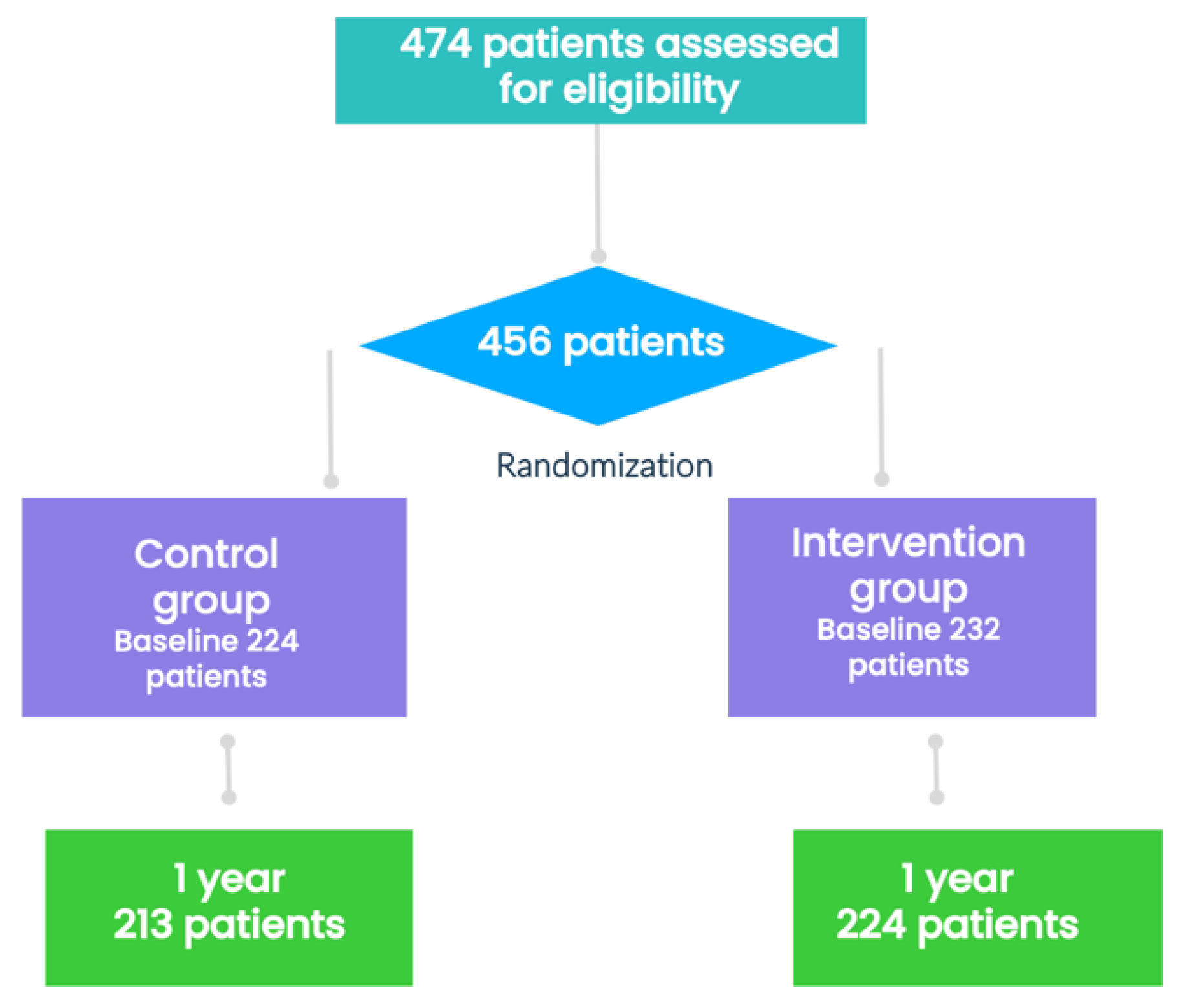
2.3. Randomization and Study Protocol
2.3.1. Control Group
2.3.2. Intervention Group
2.4. Measurements
2.5. Statistical Analyses
3. Results
3.1. Baseline Characteristics
3.2. Changes in Body Weight, Body Composition, Waist Circumference, and Blood Pressure
3.3. Metabolic Syndrome
3.4. Metabolic Syndrome Components
3.5. Medications
3.6. Laboratory Test
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Obesity and Overweight. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 29 December 2021).
- Aranceta-Bartrina, J.; Pérez-Rodrigo, C.; Alberdi-Aresti, G.; Ramos-Carrera, N.; Lázaro-Masedo, S. Prevalence of General Obesity and Abdominal Obesity in the Spanish Adult Population (Aged 25–64 Years) 2014–2015: The ENPE Study. Rev. Esp. Cardiol. Engl. Ed. 2016, 69, 579–587. [Google Scholar] [CrossRef] [PubMed]
- CDC Defining Adult Overweight and Obesity. Available online: https://www.cdc.gov/obesity/adult/defining.html (accessed on 23 January 2022).
- Eckel, R.H.; Alberti, K.G.M.M.; Grundy, S.M.; Zimmet, P.Z. The Metabolic Syndrome. Lancet Lond. Engl. 2010, 375, 181–183. [Google Scholar] [CrossRef]
- Phillips, C.; Lopez-Miranda, J.; Perez-Jimenez, F.; McManus, R.; Roche, H.M. Genetic and Nutrient Determinants of the Metabolic Syndrome. Curr. Opin. Cardiol. 2006, 21, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Mili, N.; Paschou, S.A.; Goulis, D.G.; Dimopoulos, M.-A.; Lambrinoudaki, I.; Psaltopoulou, T. Obesity, Metabolic Syndrome, and Cancer: Pathophysiological and Therapeutic Associations. Endocrine 2021, 74, 478–497. [Google Scholar] [CrossRef]
- Milovanovic, T.; Pantic, I.; Dragasevic, S.; Lugonja, S.; Dumic, I.; Rajilic-Stojanovic, M. The Interrelationship Among Non-Alcoholic Fatty Liver Disease, Colonic Diverticulosis and Metabolic Syndrome. J. Gastrointest. Liver Dis. JGLD 2021, 30, 274–282. [Google Scholar] [CrossRef]
- Zuin, M.; Rigatelli, G.; Bilato, C.; Cervellati, C.; Zuliani, G.; Roncon, L. Prognostic Role of Metabolic Syndrome in COVID-19 Patients: A Systematic Review Meta-Analysis. Viruses 2021, 13, 1938. [Google Scholar] [CrossRef]
- Alberti, K.G.M.M.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.-C.; James, W.P.T.; Loria, C.M.; Smith, S.C.; et al. Harmonizing the Metabolic Syndrome: A Joint Interim Statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009, 120, 1640–1645. [Google Scholar] [CrossRef] [Green Version]
- Cornier, M.-A.; Dabelea, D.; Hernandez, T.L.; Lindstrom, R.C.; Steig, A.J.; Stob, N.R.; Van Pelt, R.E.; Wang, H.; Eckel, R.H. The Metabolic Syndrome. Endocr. Rev. 2008, 29, 777–822. [Google Scholar] [CrossRef]
- Orchard, T.J.; Temprosa, M.; Goldberg, R.; Haffner, S.; Ratner, R.; Marcovina, S.; Fowler, S. Diabetes Prevention Program Research Group The Effect of Metformin and Intensive Lifestyle Intervention on the Metabolic Syndrome: The Diabetes Prevention Program Randomized Trial. Ann. Intern. Med. 2005, 142, 611–619. [Google Scholar] [CrossRef]
- Salas-Salvadó, J.; Fernández-Ballart, J.; Ros, E.; Martínez-González, M.-A.; Fitó, M.; Estruch, R.; Corella, D.; Fiol, M.; Gómez-Gracia, E.; Arós, F.; et al. Effect of a Mediterranean Diet Supplemented with Nuts on Metabolic Syndrome Status: One-Year Results of the PREDIMED Randomized Trial. Arch. Intern. Med. 2008, 168, 2449–2458. [Google Scholar] [CrossRef] [Green Version]
- Look AHEAD Research Group; Pi-Sunyer, X.; Blackburn, G.; Brancati, F.L.; Bray, G.A.; Bright, R.; Clark, J.M.; Curtis, J.M.; Espeland, M.A.; Foreyt, J.P.; et al. Reduction in Weight and Cardiovascular Disease Risk Factors in Individuals with Type 2 Diabetes: One-Year Results of the Look AHEAD Trial. Diabetes Care 2007, 30, 1374–1383. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paul-Ebhohimhen, V.; Avenell, A. A Systematic Review of the Effectiveness of Group versus Individual Treatments for Adult Obesity. Obes. Facts 2009, 2, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Renjilian, D.A.; Perri, M.G.; Nezu, A.M.; McKelvey, W.F.; Shermer, R.L.; Anton, S.D. Individual versus Group Therapy for Obesity: Effects of Matching Participants to Their Treatment Preferences. J. Consult. Clin. Psychol. 2001, 69, 717–721. [Google Scholar] [CrossRef] [PubMed]
- Borek, A.J.; Abraham, C.; Greaves, C.J.; Tarrant, M. Group-Based Diet and Physical Activity Weight-Loss Interventions: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. Appl. Psychol. Health Well-Being 2018, 10, 62–86. [Google Scholar] [CrossRef]
- Porca, C.; Rodriguez-Carnero, G.; Tejera, C.; Andujar, P.; Casanueva, F.F.; Crujeiras, A.B.; Bellido, D. Effectiveness to Promote Weight Loss Maintenance and Healthy Lifestyle Habits of a Group Educational Intervention Program in Adults with Obesity: IGOBE Program. Obes. Res. Clin. Pract. 2021, 15, 570–578. [Google Scholar] [CrossRef]
- Salas-Salvadó, J.; Rubio, M.A.; Barbany, M.; Moreno, B.; Grupo Colaborativo de la SEEDO. SEEDO 2007 Consensus for the evaluation of overweight and obesity and the establishment of therapeutic intervention criteria. Med. Clin. 2007, 128, 184–196. [Google Scholar] [CrossRef]
- Gargallo Fernández, M.; Marset, J.B.; Lesmes, I.B.; Izquierdo, J.Q.; Sala, X.F.; Salas-Salvadó, J.; Grupo de Consenso FESNAD-SEEDO. FESNAD-SEEDO consensus summary: Evidence-based nutritional recommendations for the prevention and treatment of overweight and obesity in adults. Endocrinol. Nutr. Organo Soc. Esp. Endocrinol. Nutr. 2012, 59, 429–437. [Google Scholar] [CrossRef]
- Jensen, M.D.; Ryan, D.H.; Donato, K.A.; Apovian, C.M.; Ard, J.D.; Comuzzie, A.G.; Hu, F.B.; Hubbard, V.S.; Jakicic, J.M.; Kushner, R.F.; et al. Executive Summary: Guidelines (2013) for the Management of Overweight and Obesity in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Obesity Society Published by the Obesity Society and American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Based on a Systematic Review from the The Obesity Expert Panel, 2013. Obes. Silver Spring 2014, 22 (Suppl. 2), S5–S39. [Google Scholar] [CrossRef] [Green Version]
- de la Torre, M.L.; Bellido, D.; Soto, A.; Carreira, J.; Hernández Mijares, A. Standardisation of the Waist Circumference (WC) for Each Range of Body Mass Index (BMI) in Adult Outpatients Attended to in Endocrinology and Nutrition Departments. Nutr. Hosp. 2010, 25, 262–269. [Google Scholar]
- Cleeman, J.I.; Grundy, S.M.; Becker, D.; Clark, L. Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel III). JAMA 2001, 285, 2486–2497. [Google Scholar] [CrossRef]
- Crujeiras, A.B.; Diaz-Lagares, A.; Moreno-Navarrete, J.M.; Sandoval, J.; Hervas, D.; Gomez, A.; Ricart, W.; Casanueva, F.F.; Esteller, M.; Fernandez-Real, J.M. Genome-Wide DNA Methylation Pattern in Visceral Adipose Tissue Differentiates Insulin-Resistant from Insulin-Sensitive Obese Subjects. Transl. Res. J. Lab. Clin. Med. 2016, 178, 13–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crujeiras, A.B.; Cabia, B.; Carreira, M.C.; Amil, M.; Cueva, J.; Andrade, S.; Seoane, L.M.; Pardo, M.; Sueiro, A.; Baltar, J.; et al. Secreted Factors Derived from Obese Visceral Adipose Tissue Regulate the Expression of Breast Malignant Transformation Genes. Int. J. Obes. 2016, 40, 514–523. [Google Scholar] [CrossRef] [PubMed]
- Mechanick, J.I.; Hurley, D.L.; Garvey, W.T. Adiposity-based chronic disease as a new diagnostic term: The american association of clinical endocrinologists and american college of endocrinology position statement. Endocr. Pract. Off. J. Am. Coll. Endocrinol. Am. Assoc. Clin. Endocrinol. 2017, 23, 372–378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elam, M.; Lovato, L.; Ginsberg, H. The ACCORD-Lipid study: Implications for treatment of dyslipidemia in Type 2 diabetes mellitus. Clin. Lipidol. 2011, 6, 9–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keech, A.; Simes, R.J.; Barter, P.; Best, J.; Scott, R.; Taskinen, M.R.; Forder, P.; Pillai, A.; Davis, T.; Glasziou, P.; et al. FIELD study investigators. Effects of long-term fenofibrate therapy on cardiovascular events in 9795 people with type 2 diabetes mellitus (the FIELD study): Randomised controlled trial. Lancet 2005, 366, 1849–1861. [Google Scholar] [CrossRef]
- Bhatt, D.L.; Steg, P.G.; Miller, M.; Brinton, E.A.; Jacobson, T.A.; Ketchum, S.B.; Doyle, R.T., Jr.; Juliano, R.A.; Jiao, L.; Granowitz, C.; et al. REDUCE-IT Investigators. Cardiovascular Risk Reduction with Icosapent Ethyl for Hypertriglyceridemia. N. Engl. J. Med. 2019, 380, 11–22. [Google Scholar] [CrossRef]
- Gaede, P.; Vedel, P.; Larsen, N.; Jensen, G.V.H.; Parving, H.-H.; Pedersen, O. Multifactorial Intervention and Cardiovascular Disease in Patients with Type 2 Diabetes. N. Engl. J. Med. 2003, 348, 383–393. [Google Scholar] [CrossRef] [Green Version]
- European Health Interview Survey—Access to Microdata—Eurostat. Available online: https://ec.europa.eu/eurostat/web/microdata/european-health-interview-survey (accessed on 2 January 2022).


{kind=link}
{kind=link}
| Variable | Global (n = 437) | Control Group (n = 213) | Intervention Group (n = 224) | p-Value |
|---|---|---|---|---|
| General characteristics | ||||
| Age, y, mean (SD) | 12.8 | 13.4 | 12.1 | 0.021 |
| Men, n (%) | 81 (18.5) | 37 (17.4) | 44 (19.6) | 0.541 |
| Current smokers, n (%) | 82 (18.7) | 44 (20.6) | 38 (16.9) | 0.744 |
| Body weight, kg, mean (SD) | 221.5 | 18.3 | 23.9 | 0.772 |
| BMI, kg/m2, mean (SD) | 7.0 | 5.6 | 7.9 | 0.716 |
| Waist circumference, cm, mean (SD) | 15.2 | 16.0 | 0.863 | |
| Fat mass, kg, mean (SD) | 11.7 | 13.1 | 0.898 | |
| Fat mass, %, mean (SD) | 5.8 | 5.1 | 0.923 | |
| Visceral fat, cm2, mean (SD) | 50.6 | 48.8 | 51.6 | 0.914 |
| Hypertension a, n (%) | 197 (45.1) | 88 (41.3) | 109 (48.6) | 0.123 |
| Hypercholesterolemia b, n (%) | 180 (41.1) | 98 (46.2) | 82 (36.9) | 0.028 |
| Hypertriglyceridemia c, n (%) | 134 (30.6) | 68 (32.7) | 66 (30.0) | 0.132 |
| Type 2 diabetes mellitus, n (%) | 102 (23.3) | 49 (23.0) | 53 (23.7) | 0.402 |
| Metabolic syndrome d, n (%) | 267 (61.1) | 122 (57.3) | 145 (64.7) | 0.542 |
| Metabolic syndrome components d | ||||
| Abdominal obesity n (%) | 387 (88.5) | 180 (84.5) | 207 (92.4) | 0.596 |
| Low HDL level, n (%) | 158 (36.1) | 75 (35.2) | 83 (37.0) | 0.323 |
| High triglycerides level, n (%) | 428 (97.9) | 208 (97.6) | 220 (98.2) | 0.746 |
| High fasting serum glucose level, n (%) | 207 (47.3) | 99 (46.5) | 108 (48.2) | 0.311 |
| High blood pressure, n (%) | 316 (72.3) | 159 (74.6) | 157 (70.0) | 0.336 |
| Medications, n (%) | ||||
| Antihypertensive drugs | 197 (546) | 88 (41.3) | 109 (48.7) | 0.123 |
| Statins | 137 (31.3) | 61 (28.6) | 76 (33.9) | 0.233 |
| Fibrates | 21 (4.8) | 11 (5.2) | 10 (4.5) | 0.732 |
| Hypoglycemic agents | 105 (24.0) | 51 (24.0) | 54 (24.1) | 0.365 |
| Insulin | 31 (7.1) | 13 (6.1) | 18 (8.0) | 0.214 |
| Variable | Global | Control Group | Intervention Group | p-Value |
|---|---|---|---|---|
| Body weight, kg, mean (SD) | ||||
| Basal | 221.5 | 18.3 | 23.9 | 0.772 |
| 1 year | 102.6 ± 20.5 | 19.4 | 21.3 | 0.002 |
| Change 1-year respect basal (%) | 6.13 | 7.26 | <0.001 | |
| BMI, kg/m2, mean (SD) | ||||
| Basal | 7.0 | 5.6 | 7.9 | 0.716 |
| 1 year | 6.6 | 6.1 | 6.8 | <0.001 |
| Change 1-year respect basal (%) | 6.25 | 7.70 | <0.001 | |
| Waist circumference, cm, mean (SD) | ||||
| Basal | 15.2 | 16.0 | 0.863 | |
| 1 year | 14.9 | 14.4 | <0.001 | |
| Change 1-year respect basal (%) | 6.43 | 6.9 | <0.001 | |
| Fat mass, kg, mean (SD) | ||||
| Basal | 11.7 | 13.1 | 0.898 | |
| 1 year | 12.1 | 11.9 | <0.001 | |
| Change 1-year respect basal (%) | 13.77 | 14.8 | <0.001 | |
| Fat mass, %, mean (SD) | 5.8 | 5.1 | 0.923 | |
| Basal | 5.8 | 5.1 | 0.923 | |
| 1 year | 5.9 | 6.2 | 0.001 | |
| Change 1-year respect basal (%) | 10.67 | 11.01 | <0.001 | |
| Visceral fat, cm2, mean (SD) | ||||
| Basal | 48.8 | 51.6 | 0.914 | |
| 1 year | 49.8 | 46.5 | <0.001 | |
| Change 1-year respect basal (%) | 13.77 | 14.8 | <0.001 |
| Variable | Control Group (n = 213) | Intervention Group (n = 224) | p-Value * |
|---|---|---|---|
| MetS n (%) | |||
| Baseline prevalence | 122 (57.3) | 145 (64.7) | 0.542 |
| 1-year prevalence | 117 (55.2) | 115 (51.3) | 0.004 |
| Change 1-year respect basal (%) | −2.1 | −13.4 | <0.001 |
| Abdominal obesity n (%) | |||
| Baseline prevalence | 180 (84.5) | 207 (92.4) | 0.596 |
| 1-year prevalence | 108 (50.7) | 114 (50.9) | 0.007 |
| Change 1-year respect basal (%) | −33.8 | −41.5 | <0.001 |
| Low HDL level n (%) | |||
| Baseline prevalence | 75 (35.2) | 83 (37.0) | 0.323 |
| 1-year prevalence | 67 (31.5) | 73 (32.6) | 0.478 |
| Change 1-year respect basal (%) | −3.7% | −4.4% | <0.001 |
| High triglycerides level n (%) | |||
| Baseline prevalence | 208 (97.6) | 220 (98.2) | 0.746 |
| 1-year prevalence | 196 (92.0) | 216 (96.4) | 0.063 |
| Change 1-year respect basal (%) | −5.6 | −1.8 | <0.001 |
| High fasting serum glucose level or use of antidiabetic drugs, n (%) | |||
| Baseline prevalence | 99 (46.5) | 108 (48.2) | 0.311 |
| 1-year prevalence | 88 (41.3) | 79 (35.2) | 0.163 |
| Change 1-year respect basal (%) | −5.2 | −13.0 | <0.001 |
| High blood pressure or use of antihypertensive drugs, n (%) | |||
| Baseline prevalence | 159 (74.6) | 157 (70.0) | 0.336 |
| 1-year prevalence | 145 (68.1) | 139 (62.1) | 0.010 |
| Change 1-year respect basal (%) | −6.5 | −7.9 | <0.001 |
| Medications, n (%) | Control Group (n = 213) | Intervention Group (n = 224) | p-Value |
|---|---|---|---|
| Antihypertensive drugs | |||
| Basal | 88 (41.3) | 109 (48.7) | 0.501 |
| 12 months | 88 (41.3) | 116 (51.7) | 0.256 |
| Statins | |||
| Basal | 61 (28.6) | 76 (33.9) | 0.233 |
| 12 months | 67 (31.4) | 78 (34.8) | 0.555 |
| Fibrates | |||
| Basal | 11 (5.2) | 10 (4.5) | 0.732 |
| 12 months | 13 (6.1) | 9 (4.0) | 0.739 |
| Hypoglycemic agents | |||
| Basal | 51 (24.0) | 54 (24.1) | 0.365 |
| 12 months | 56 (26.3) | 54 (24.1) | 0.475 |
| Insulin | |||
| Basal | 13 (6.1) | 18 (8.0) | 0.214 |
| 12 months | 14 (6.5) | 19 (8.5) | 0.271 |
| Variable | Control Group | Intervention Group | p-Value | |||
|---|---|---|---|---|---|---|
| Basal | 1 Year | Basal | 1 Year | Basal | 1 Year | |
| Fasting blood glucose mg/dL | 105 ± 29 | 106 ± 31 | 107 ± 28 | 104 ± 30 | 0.851 | 0.494 |
| HbA1c % | 6.5 ± 1.3 | 6.3 ± 1.1 | 6.5 ± 1.3 | 6.1 ± 0.9 | 0.869 | 0.227 |
| Total cholesterol, mg/dL | 195 ± 38 | 192 ± 36 | 190 ± 33 | 191 ± 37 | 0.129 | 0.754 |
| HDL levels, mg/dL | 52 ± 14 | 50 ± 10 | 52 ± 13 | 52 ± 13 | 0.955 | 0.087 |
| LDL levels, mg/dL | 117 ± 32 | 114 ± 32 | 111 ± 30 | 112 ± 31 | 0.067 | 0.599 |
| Triglyceride levels, mg/dL | 140 ± 76 | 144 ± 75 | 133 ± 58 | 135 ± 62 | 0.304 | 0.177 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tejera, C.; Porca, C.; Rodriguez-Carnero, G.; Andújar, P.; Casanueva, F.F.; Bellido, D.; Crujeiras, A.B. Reducing Metabolic Syndrome through a Group Educational Intervention Program in Adults with Obesity: IGOBE Program. Nutrients 2022, 14, 1066. https://doi.org/10.3390/nu14051066
Tejera C, Porca C, Rodriguez-Carnero G, Andújar P, Casanueva FF, Bellido D, Crujeiras AB. Reducing Metabolic Syndrome through a Group Educational Intervention Program in Adults with Obesity: IGOBE Program. Nutrients. 2022; 14(5):1066. https://doi.org/10.3390/nu14051066
Chicago/Turabian StyleTejera, Cristina, Cristina Porca, Gemma Rodriguez-Carnero, Paula Andújar, Felipe F. Casanueva, Diego Bellido, and Ana B. Crujeiras. 2022. "Reducing Metabolic Syndrome through a Group Educational Intervention Program in Adults with Obesity: IGOBE Program" Nutrients 14, no. 5: 1066. https://doi.org/10.3390/nu14051066
APA StyleTejera, C., Porca, C., Rodriguez-Carnero, G., Andújar, P., Casanueva, F. F., Bellido, D., & Crujeiras, A. B. (2022). Reducing Metabolic Syndrome through a Group Educational Intervention Program in Adults with Obesity: IGOBE Program. Nutrients, 14(5), 1066. https://doi.org/10.3390/nu14051066