
Potential Benefits of the Mediterranean Diet and Physical Activity in Patients with Hidradenitis Suppurativa: A Cross-Sectional Study in a Spanish Population


 ,
,  and
and 
Abstract
:1. Introduction
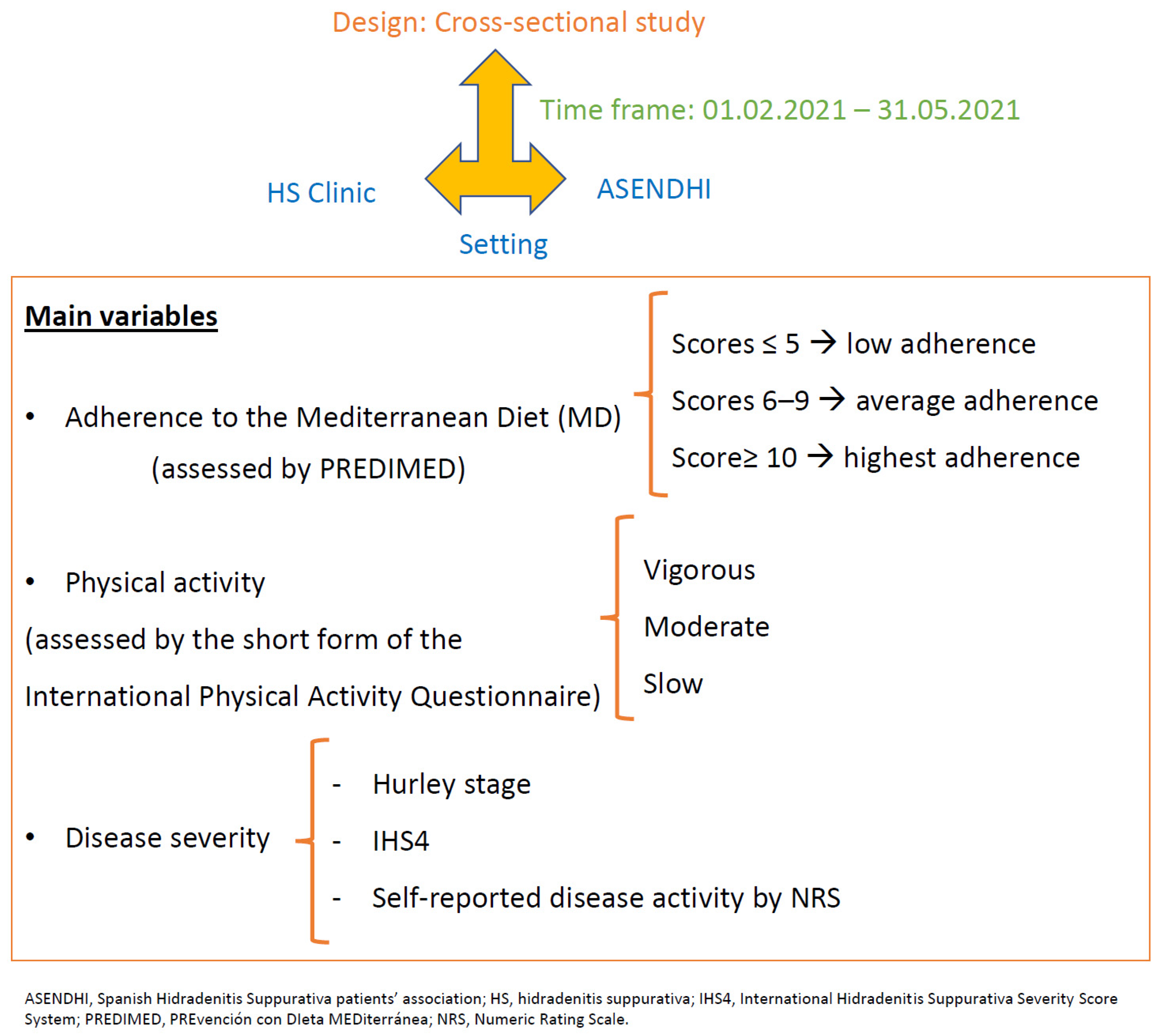
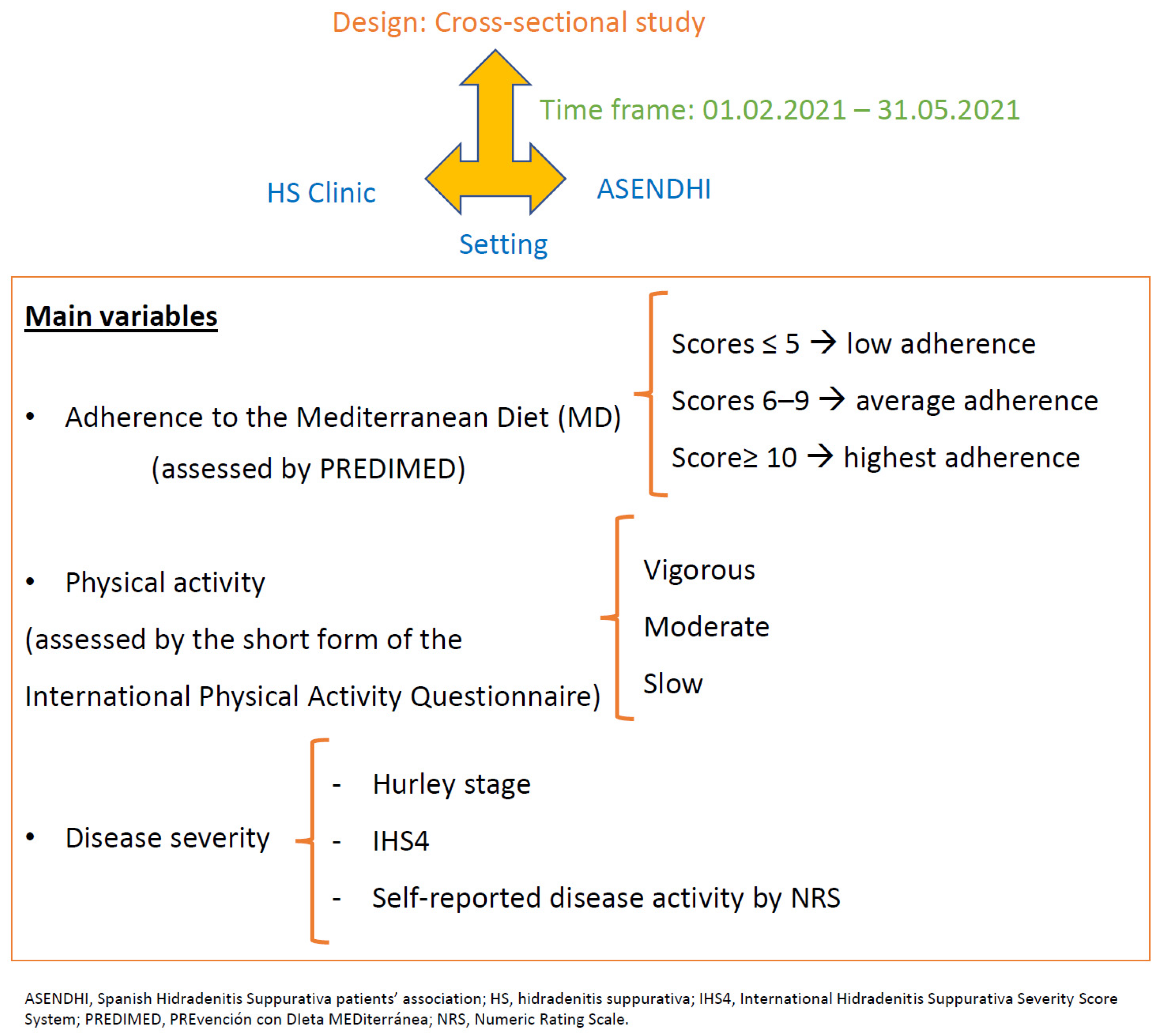
2. Materials and Methods
3. Results
3.1. Sociodemographic and Clinical Features of the Sample
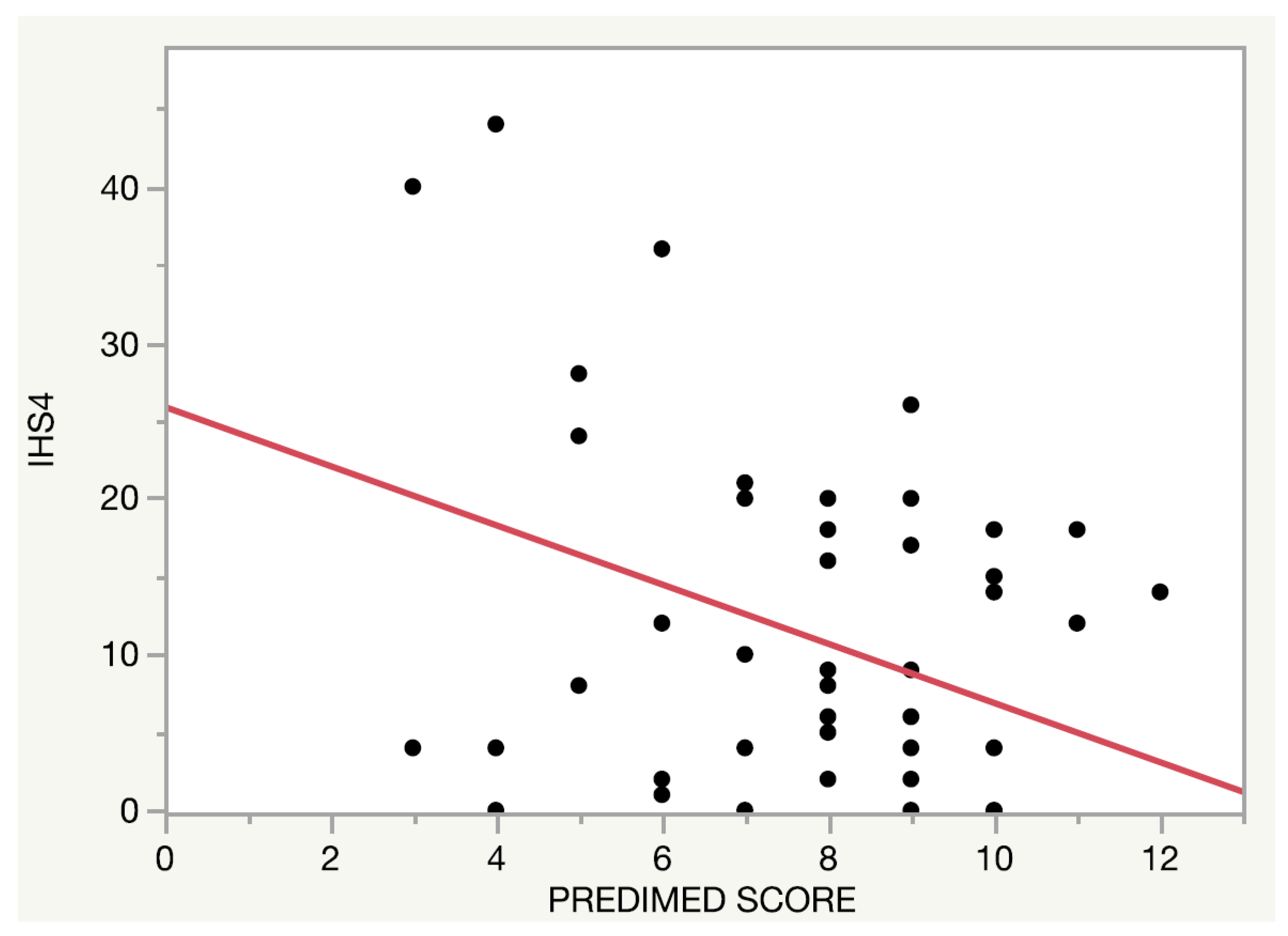
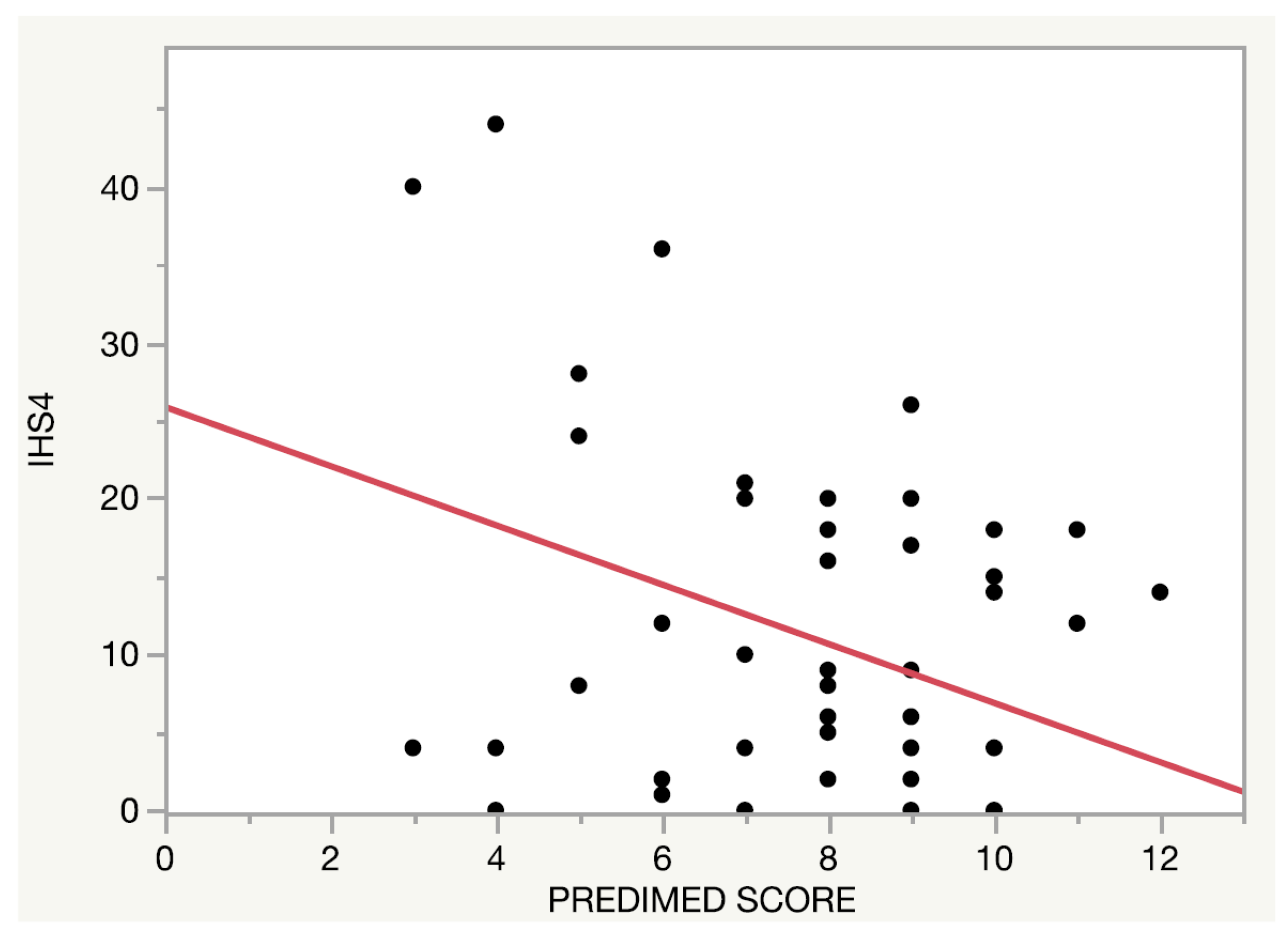
3.2. Adherence to the Mediterranean Diet
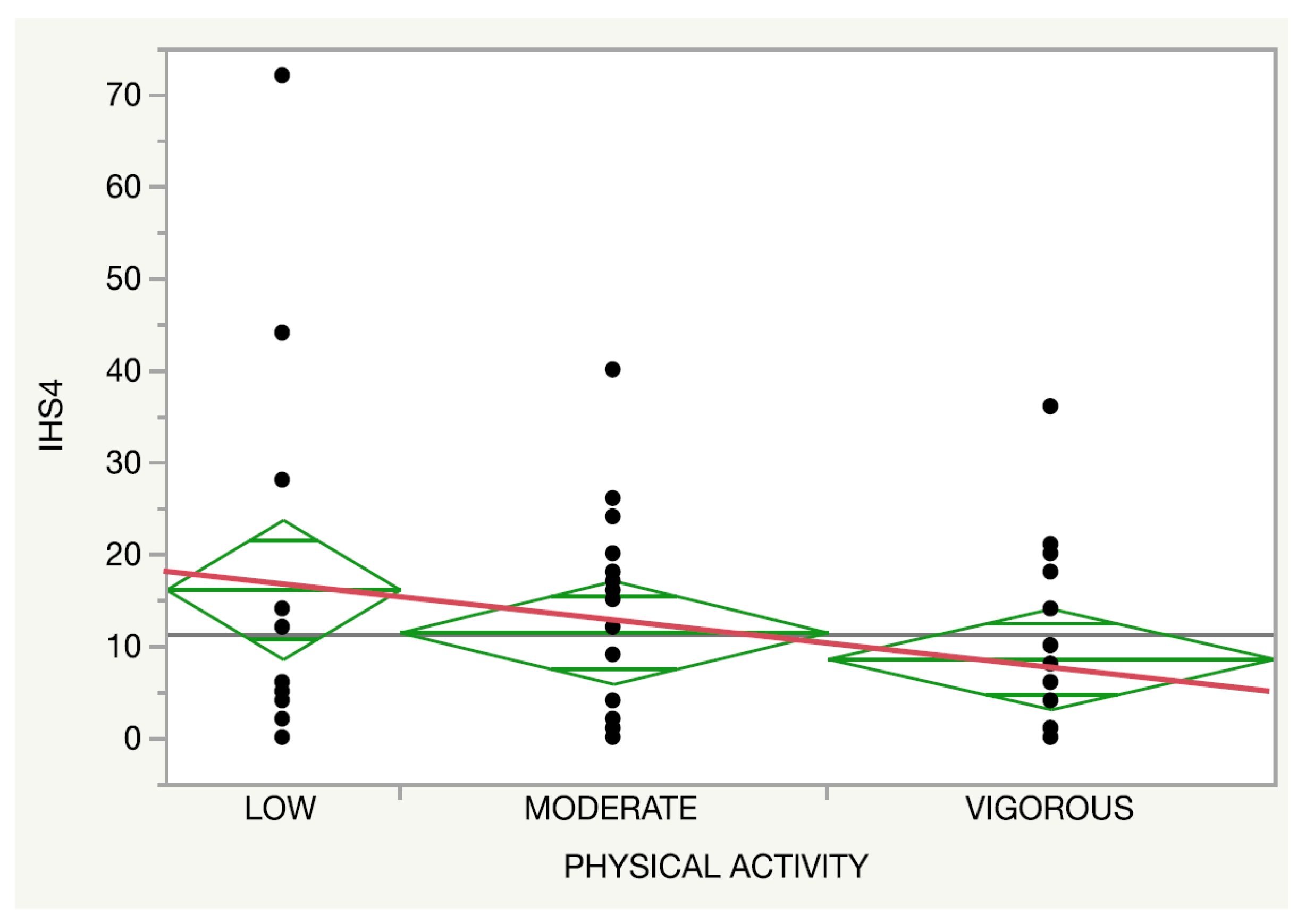
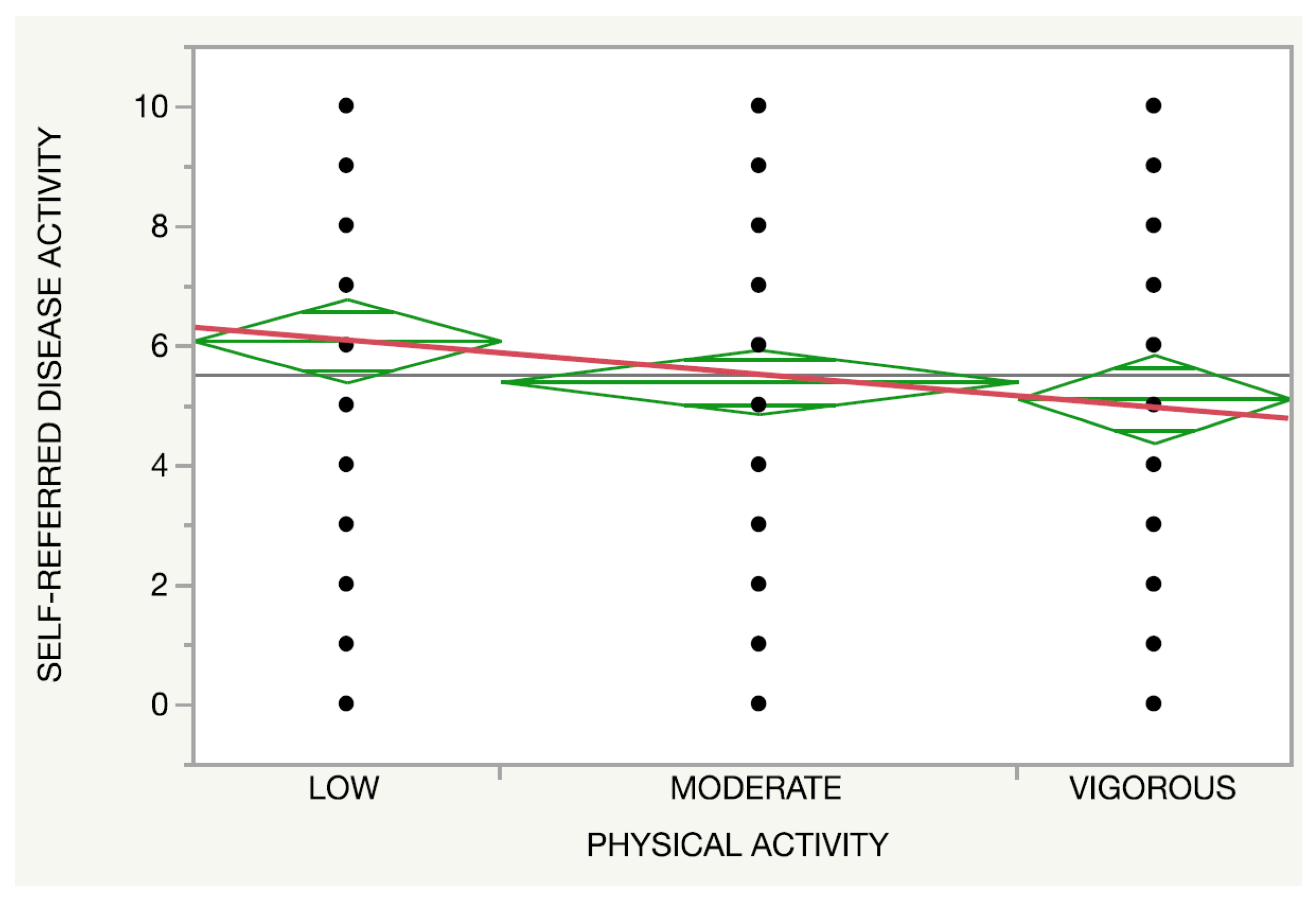
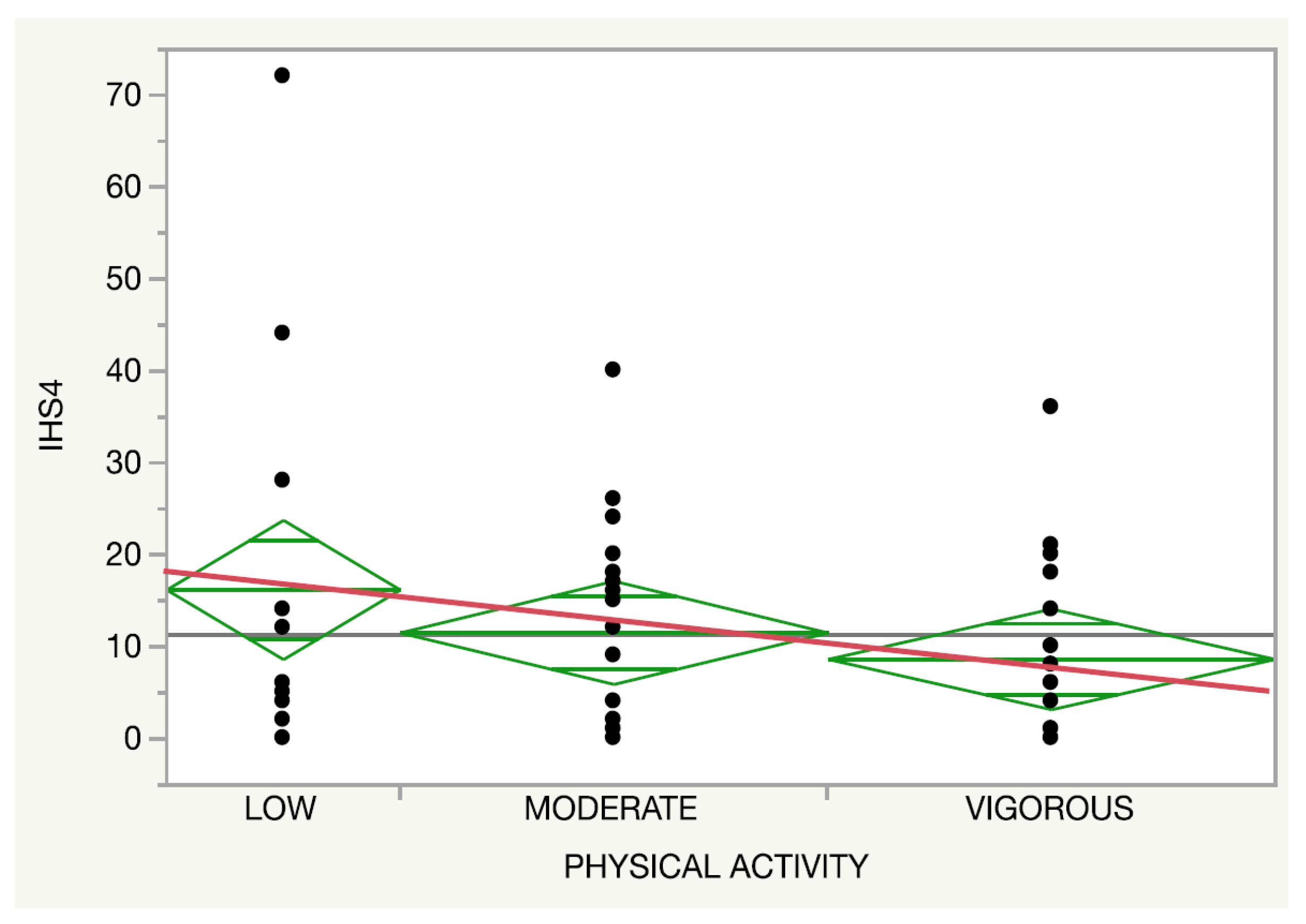
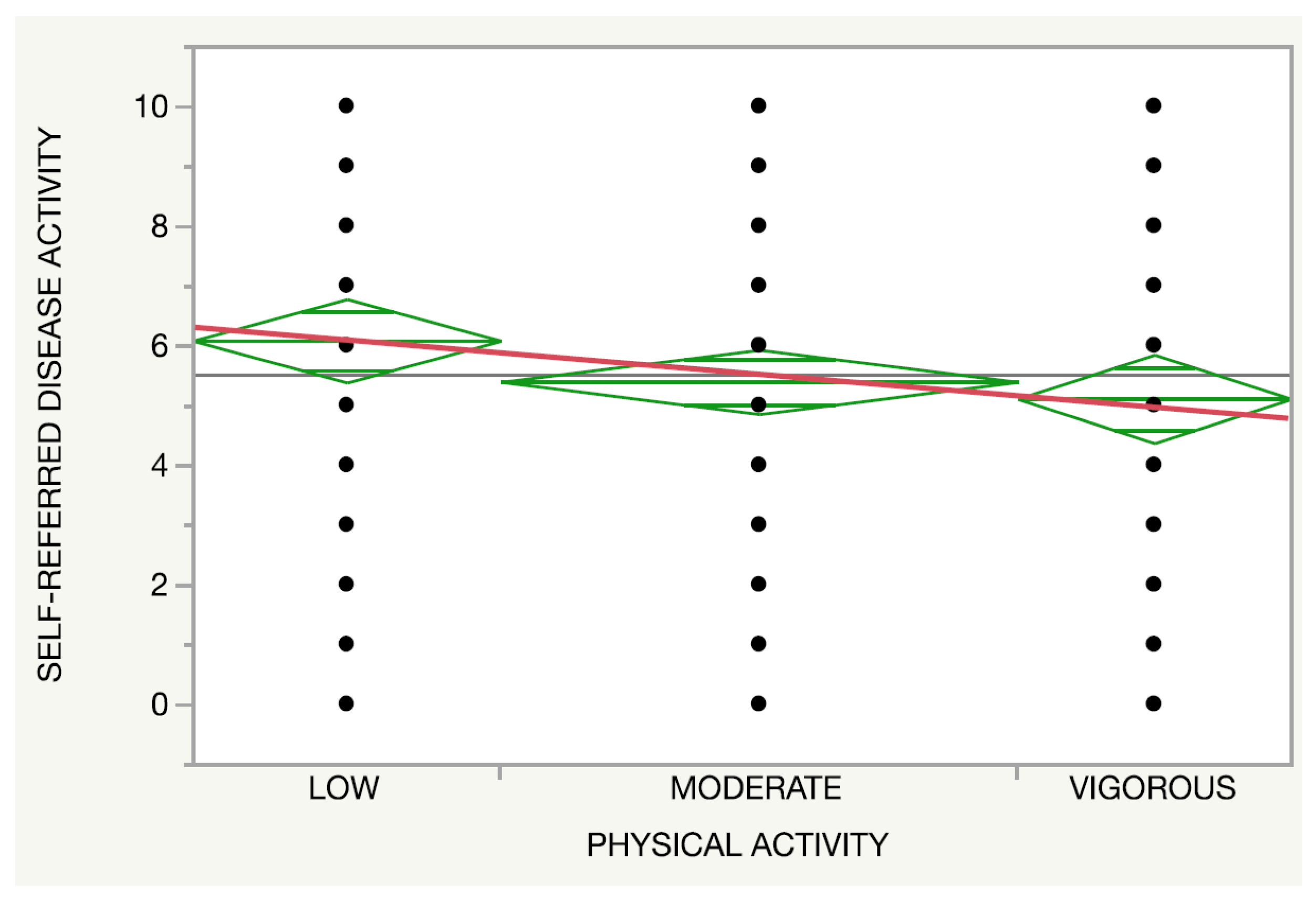
3.3. Physical Activity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nguyen, T.V.; Damiani, G.; Orenstein, L.A.; Hamzavi, I.; Jemec, G. Hidradenitis suppurativa: An update on epidemiology, phenotypes, diagnosis, pathogenesis, comorbidities and quality of life. J. Eur. Acad. Dermatol. Venereol. 2021, 35, 50–61. [Google Scholar] [CrossRef] [PubMed]
- Goldburg, S.R.; Strober, B.E.; Payette, M.J. Hidradenitis suppurativa: Epidemiology, clinical presentation, and pathogenesis. J. Am. Acad. Dermatol. 2020, 82, 1045–1058. [Google Scholar] [CrossRef] [PubMed]
- Montero-Vilchez, T.; Diaz-Calvillo, P.; Rodriguez-Pozo, J.-A.; Cuenca-Barrales, C.; Martinez-Lopez, A.; Arias-Santiago, S.; Molina-Leyva, A. The Burden of Hidradenitis Suppurativa Signs and Symptoms in Quality of Life: Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 6709. [Google Scholar] [CrossRef] [PubMed]
- Molina-Leyva, A.; Cuenca-Barrales, C. Pruritus and Malodour in Patients with Hidradenitis Suppurativa: Impact on Quality of Life and Clinical Features Associated with Symptom Severity. Dermatology 2019, 236, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Del Duca, E.; Morelli, P.; Bennardo, L.; Di Raimondo, C.; Nistico, S.P. Cytokine Pathways and Investigational Target Therapies in Hidradenitis Suppurativa. Int. J. Mol. Sci. 2020, 21, 8436. [Google Scholar] [CrossRef] [PubMed]
- Nomura, T. Hidradenitis Suppurativa as a Potential Subtype of Autoinflammatory Keratinization Disease. Front. Immunol. 2020, 11, 847. [Google Scholar] [CrossRef]
- Theut Riis, P.; Saunte, D.; Benhadou, F.; del Marmol, V.; Guillem, P.; El-Domyati, M.; Abdel-Wahab, H.; Antoniou, C.; Dessinioti, C.; Gürer, M.; et al. Low and high body mass index in hidradenitis suppurativa patients-different subtypes? J. Eur. Acad. Dermatol. Venereol. 2018, 32, 307–312. [Google Scholar] [CrossRef]
- Choi, F.; Lehmer, L.; Ekelem, C.; Mesinkovska, N.A. Dietary and metabolic factors in the pathogenesis of hidradenitis suppurativa: A systematic review. Int. J. Dermatol. 2019, 59, 143–153. [Google Scholar] [CrossRef]
- Macklis, P.C.; Tyler, K.; Kaffenberger, J.; Kwatra, S.; Kaffenberger, B.H. Lifestyle modifications associated with symptom im-provement in hidradenitis suppurativa patients. Arch. Dermatol. Res. 2021. [Google Scholar] [CrossRef]
- Fernandez, J.M.; Marr, K.D.; Hendricks, A.J.; Price, K.N.; Ludwig, C.M.; Maarouf, M.; Hsiao, J.L.; Shi, V.Y. Alleviating and exacerbating foods in hidradenitis suppurativa. Dermatol. Ther. 2020, 33, 14246. [Google Scholar] [CrossRef]
- Sivanand, A.; Gulliver, W.P.; Josan, C.K.; Alhusayen, R.; Fleming, P.J. Weight Loss and Dietary Interventions for Hidradenitis Suppurativa: A Systematic Review. J. Cutan. Med. Surg. 2019, 24, 64–72. [Google Scholar] [CrossRef] [PubMed]
- Dempsey, A.; Butt, M.; Kirby, J.S. Prevalence and Impact of Dietary Avoidance among Individuals with Hidradenitis Suppurativa. Dermatology 2020, 236, 289–295. [Google Scholar] [CrossRef] [PubMed]
- Bach-Faig, A.; Berry, E.M.; Lairon, D.; Reguant, J.; Trichopoulou, A.; Dernini, S.; Medina, F.X.; Battino, M.; Belahsen, R.; Miranda, G.; et al. Mediterranean diet pyramid today. Science and cultural updates. Public Health Nutr. 2011, 14, 2274–2284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zheng, Q.; Sun, X.Y.; Miao, X.; Xu, R.; Ma, T.; Zhang, Y.N.; Li, H.J.; Li, B.; Li, X. Association between physical activity and risk of prevalent psoriasis: A MOOSE-compliant meta-analysis. Medicine 2018, 97, e11394. [Google Scholar] [CrossRef]
- Estruch, R.; Ros, E.; Martinez-Gonzalez, M.A. Mediterranean diet for primary prevention of cardiovascular disease. N. Engl. J. Med. 2013, 369, 676–677. [Google Scholar] [CrossRef] [Green Version]
- Amati, F.; Hassounah, S.; Swaka, A. The Impact of Mediterranean Dietary Patterns During Pregnancy on Maternal and Offspring Health. Nutrients 2019, 11, 1098. [Google Scholar] [CrossRef] [Green Version]
- Barrea, L.; Fabbrocini, G.; Annunziata, G.; Muscogiuri, G.; Donnarumma, M.; Marasca, C.; Colao, A.; Savastano, S. Role of Nutrition and Adherence to the Mediterranean Diet in the Multidisciplinary Approach of Hidradenitis Suppurativa: Evaluation of Nutritional Status and Its Association with Severity of Disease. Nutrients 2018, 11, 57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silfvast-Kaiser, A.; Youssef, R.; Paek, S.Y. Diet in hidradenitis suppurativa: A review of published and lay literature. Int. J. Dermatol. 2019, 58, 1225–1230. [Google Scholar] [CrossRef] [PubMed]
- Tresserra-Rimbau, A.; Rimm, E.B.; Medina-Remón, A.; Martínez-González, M.A.; López-Sabater, M.C.; Covas, M.I.; Corella, D.; Salas-Salvadó, J.; Gómez-Gracia, E.; Lapetra, J.; et al. Polyphenol intake and mortality risk: A re-analysis of the PREDIMED trial. BMC Med. 2014, 12, 77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phan, C.; Touvier, M.; Kesse-Guyot, E.; Adjibade, M.; Hercberg, S.; Wolkenstein, P.; Chosidow, O.; Ezzedine, K.; Sbidian, E. Association Between Mediterranean Anti-inflammatory Dietary Profile and Severity of Psoriasis: Results from the NutriNet-Sante Cohort. JAMA Dermatol. 2018, 154, 1017–1024. [Google Scholar] [CrossRef]
- Wilson, P.; Bohjanen, K.; Ingraham, S.; Leon, A. Psoriasis and physical activity: A review. J. Eur. Acad. Dermatol. Venereol. 2012, 26, 1345–1353. [Google Scholar] [CrossRef] [PubMed]
- Eiken, H.C.; Holm, J.G.; Thomsen, S.F. Studies on the role of diet in the management of hidradenitis suppurativa are needed. J. Am. Acad. Dermatol. 2020, 82, e137–e138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martinez-Gonzalez, M.A.; Garcia-Arellano, A.; Toledo, E.; Salas-Salvado, J.; Buil-Cosiales, P.; Corella, D. A 14-item Mediter-ranean diet assessment tool and obesity indexes among high-risk subjects: The PREDIMED trial. PLoS ONE 2012, 7, e43134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International Physical Activity Questionnaire: 12-Country Reliability and Validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vinas, B.R.; Ribas Barba, L.; Ngo, J.; Serra Majem, L. Validity of the international physical activity questionnaire in the Catalan population (Spain). Gac. Sanit. 2013, 27, 254–257. [Google Scholar]
- Ovadja, Z.N.; Schuit, M.M.; van der Horst, C.; Lapid, O. Inter- and intrarater reliability of Hurley staging for hidradenitis sup-purativa. Br. J. Dermatol. 2019, 181, 344–349. [Google Scholar] [CrossRef] [Green Version]
- Cuenca-Barrales, C.; Ruiz-Villaverde, R.; Molina-Leyva, A. Sexual Distress in Patients with Hidradenitis Suppurativa: A Cross-Sectional Study. J. Clin. Med. 2019, 8, 532. [Google Scholar] [CrossRef] [Green Version]
- Kirby, J.; Hereford, B.; Thorlacius, L.; Villumsen, B.; Ingram, J.; Garg, A.; Butt, M.; Esmann, S.; King, T.; Tan, J.; et al. Validation of global item for assessing impact on quality of life of patients with hidradenitis suppurativa. Br. J. Dermatol. 2021, 184, 681–687. [Google Scholar] [CrossRef]
- Zouboulis, C.C.; Tzellos, T.; Kyrgidis, A.; Jemec, G.B.E.; Bechara, F.G.; Giamarellos-Bourboulis, E.J.; Ingram, J.R.; Kanni, T.; Karagiannidis, I.; Martorell, A.; et al. Development and validation of the International Hidradenitis Suppurativa Severity Score System (IHS 4), a novel dynamic scoring system to assess HS severity. Br. J. Dermatol. 2017, 177, 1401–1409. [Google Scholar] [CrossRef] [Green Version]
- Lubrano, E.; Perrotta, F.M.; Parsons, W.J.; Marchesoni, A. Patient’s Global Assessment as an Outcome Measure for Psoriatic Arthritis in Clinical Practice: A Surrogate for Measuring Low Disease Activity? J. Rheumatol. 2015, 42, 2332–2338. [Google Scholar] [CrossRef]
- Zouboulis, C.C.; Desai, N.; Emtestam, L.; Hunger, R.E.; Ioannides, D.; Juhász, I.; Lapins, J.; Matusiak, L.; Prens, E.P.; Revuz, J.; et al. European S1 guideline for the treatment of hidradenitis suppurativa/acne inversa. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 619–644. [Google Scholar] [CrossRef] [PubMed]
- Schutte-Rodin, S.; Broch, L.; Buysse, D.; Dorsey, C.; Sateia, M. Clinical Guideline for the Evaluation and Management of Chronic Insomnia in Adults. J. Clin. Sleep Med. 2008, 4, 487–504. [Google Scholar] [CrossRef] [PubMed]
- Savard, J.; Ganz, P.A. Subjective or Objective Measures of Cognitive Functioning-What’s More Important? JAMA Oncol. 2016, 2, 1263–1264. [Google Scholar] [CrossRef] [PubMed]
- Cobo-Cuenca, A.I.; Garrido-Miguel, M.; Soriano-Cano, A.; Ferri-Morales, A.; Martinez-Vizcaino, V.; Martin-Espinosa, N.M. Adherence to the Mediterranean Diet and Its Association with Body Composition and Physical Fitness in Spanish University Students. Nutrients 2019, 11, 2830. [Google Scholar] [CrossRef] [Green Version]
- Molina-Leyva, A.; Cuenca-Barrales, C.; Vega-Castillo, J.; Ruiz-Carrascosa, J.; Ruiz-Villaverde, R. Adherence to Mediterranean diet in Spanish patients with psoriasis: Cardiovascular benefits? Dermatol. Ther. 2019, 32, e12810. [Google Scholar] [CrossRef]
- Montero-Vilchez, T.; Salvador-Rodriguez, L.; Sanchez-Diaz, M.; Cuenca-Barrales, C.; Martinez-Lopez, A.; Arias-Santiago, S.; Molina-Leyva, A. Clinical selection criteria in new clinical trials of hidradenitis suppurativa: External validity and implications on the daily clinical practice. Dermatol. Ther. 2020, 33, 14254. [Google Scholar] [CrossRef]
- David, L.A.; Maurice, C.F.; Carmody, R.N.; Gootenberg, D.B.; Button, J.E.; Wolfe, B.E.; Ling, A.V.; Devlin, A.S.; Varma, Y.; Fischbach, M.A.; et al. Diet rapidly and reproducibly alters the human gut microbiome. Nature 2014, 505, 559–563. [Google Scholar] [CrossRef] [Green Version]
- Zhao, X.; Gan, L.; Pan, H.; Kan, D.; Majeski, M.; Adam, S.; Unterman, T.G. Multiple elements regulate nuclear/cytoplasmic shuttling of FOXO1: Characterization of phosphorylation- and 14-3-3-dependent and -independent mechanisms. Biochem. J. 2004, 378, 839–849. [Google Scholar] [CrossRef] [Green Version]
- Agamia, N.; Abdallah, D.; Sorour, O.S.; Mourad, B.; Younan, D.Y. Skin expression of mammalian target of rapamycin and forkhead box transcription factor O1, and serum insulin-like growth factor-1 in patients with acne vulgaris and their relationship with diet. Br. J. Dermatol. 2016, 174, 1299–1307. [Google Scholar] [CrossRef]
- De Rosa, V.; Galgani, M.; Santopaolo, M.; Colamatteo, A.; Laccetti, R.; Matarese, G. Nutritional control of immunity: Balancing the metabolic requirements with an appropriate immune function. Semin. Immunol. 2015, 27, 300–309. [Google Scholar] [CrossRef]
- Ferrari, F.; Bock, P.M.; Motta, M.T.; Helal, L. Biochemical and Molecular Mechanisms of Glucose Uptake Stimulated by Physical Exercise in Insulin Resistance State: Role of Inflammation. Arq. Bras. Cardiol. 2019, 113, 1139–1148. [Google Scholar] [CrossRef] [PubMed]
- Boer, J. Should Hidradenitis Suppurativa Be Included in Dermatoses Showing Koebnerization? Is It Friction or Fiction? Dermatology 2017, 233, 47–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boer, J. Resolution of hidradenitis suppurativa after weight loss by dietary measures, especially on frictional locations. J. Eur. Acad. Dermatol. Venereol. 2015, 30, 895–896. [Google Scholar] [CrossRef] [PubMed]
- Andersen, V.; Holmskov, U.; Sørensen, S.B.; Jawhara, M.; Andersen, K.W.; Bygum, A.; Hvid, L.; Grauslund, J.; Wied, J.; Glerup, H.; et al. A Proposal for a Study on Treatment Selection and Lifestyle Recommendations in Chronic Inflammatory Diseases: A Danish Multidisciplinary Collaboration on Prognostic Factors and Personalised Medicine. Nutrients 2017, 9, 499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.-I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. Primary Prevention of Cardiovascular Disease with a Mediterranean Diet Supplemented with Extra-Virgin Olive Oil or Nuts. N. Engl. J. Med. 2018, 378, e34. [Google Scholar] [CrossRef] [PubMed]
- Bulger, D.A.; Minhas, S.; Asbeutah, A.A.; Kayali, S.; Shirwany, H.A.; Patel, J.R.; Seitz, M.P.; Clark, K.; Patel, T.; Khouzam, R.N. Chronic Systemic Inflammatory Skin Disease as a Risk Factor for Cardiovascular Disease. Curr. Probl. Cardiol. 2021, 46, 100799. [Google Scholar] [CrossRef]
- Garg, A.; Malviya, N.; Strunk, A.; Wright, S.; Alavi, A.; Alhusayen, R.; Alikhan, A.; Daveluy, S.D.; Delorme, I.; Goldfarb, N.; et al. Comorbidity screening in hidradenitis suppurativa: Evidence-based recommendations from the US and Canadian Hidradenitis Suppurativa Foundations. J. Am. Acad. Dermatol. 2021; in press. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N = 221 | |
|---|---|
| ASENDHI | 74.20% (164/221) |
| Age (years) | 38.36 (10.74) |
| Sex | |
| Female | 73.30% (162/221) |
| Male | 26.29% (59/221) |
| BMI (kg/m2) | 29.65 (6.26) |
| Smoking habit (yes) | 57.46% (127/221) |
| Number of cigarettes per day | 7.60 (8.29) |
| Blood pressure medication (yes) | 15.38% (34/221) |
| Cholesterol or triglyceride medication (yes) | 9.95% (22/221) |
| Diabetes medication (yes) | 8.1% (18/221) |
| Disease duration (years) | 16.77 (9.96) |
| Self-reported Hurley | |
| I | 29.41% (65/221) |
| II | 38.91% (86/221) |
| III | 31.67% (70/221) |
| Self-referred disease activity | 5.51 (2.80) |
| Actual HS treatment | |
| Oral antibiotics | 17.19 (38/221) |
| Topical antibiotics | 19.00% (42/221) |
| Biologics | 30.31% (67/221) |
| None | 21.71% (48/221) |
| Systemic treatment different form antibiotics | 11.68% (26/221) |
| IHS4 (only patients from our HS Clinic, n = 57) | 11.31 (13.17) |
| Predimed | % |
|---|---|
| Use of extra virgin olive oil as main culinary lipid | 86.87% (192/221) |
| Extra virgin olive oil > 4 tablespoons | 44.79% (99/221) |
| Vegetables ≥ 2 servings/day | 52.48% (116/221) |
| Fruits ≥ 3 servings/day | 30.76% (68/221) |
| Red/processed meats < 1/day | 68.32% (151/221) |
| Butter, cream, margarine < 1/day | 72.39% (160/221) |
| Soda drinks < 1/day | 62.44% (138/221) |
| Wine glasses ≥ 7/week | 7.69% (17/221) |
| Legumes ≥ 3/week | 44.79% (99/221) |
| Fish/seafood ≥ 3/week | 28.95% (64/221 |
| Commercial sweets and confectionery ≥ 2/week | 48.86% (108/221) |
| Tree nuts ≥ 3/week | 40.27% (89/221) |
| Poultry rather than red meats | 79.63% (176/221) |
| Use of sofrito sauce ≥ 2/week | 73.75% (163/221) |
| Total Predimed punctuation | 7.41 (2.16) |
| Variables | Univariant (Beta) | p * | Multivariant (Beta) | p ** | |
|---|---|---|---|---|---|
| Age | 0.03 (0.01) | 0.02 * | 0.01 (0.01) | 0.32 | |
| Sex | Male | 7.40 (0.28) | 0.96 | - | - |
| Female | 7.41 (0.17) | - | - | ||
| BMI (kg/m2) | −0.005 (0.02) | 0.82 | - | - | |
| Cigarettes/day | −0.01 (0.017) | 0.44 | - | - | |
| Number of cigarettes per day | 7.73 (0.37) | 0.35 | - | - | |
| Blood pressure medication (yes) | 7.31 (0.46) | 0.82 | - | - | |
| Cholesterol or triglyceride medication (yes) | 7.55 (0.51) | 0.77 | - | - | |
| Diabetes medication (yes) | 0.02 (0.01) | 0.07 | - | - | |
| Actual treatment | Oral antibiotics | 7.23 (0.35) | 0.66 | - | - |
| Topical antibiotics | 7.04 (0.33) | - | - | ||
| Biologics | 7.53 (0.26) | - | - | ||
| None | 7.54 (0.31) | - | - | ||
| Systemic treatment different form antibiotics | 7.73 (0.42) | - | - | ||
| Age of onset | 0.20 (0.26) | 0.43 | - | - | |
| Disease duration | 0.54 (0.30) | 0.07 | 0.01 (0.01) | 0.54 | |
| Self-referred disease activity | −0.17 (0.08) | 0.04 | −0.11 (0.05) | 0.02 ** | |
| Self-reported Hurley | I | 7.86 (2.01) | 0.02 * | −0.36 (0.14) | 0.01 ** |
| II–III | 7.23 (2.20) | ||||
| Physical activity level | Low–Moderate | 7.09 (0.27) | 0.06 | 0.31 (0.14) | 0.02 ** |
| Vigorous | 7.77 (0.21) | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lorite-Fuentes, I.; Montero-Vilchez, T.; Arias-Santiago, S.; Molina-Leyva, A. Potential Benefits of the Mediterranean Diet and Physical Activity in Patients with Hidradenitis Suppurativa: A Cross-Sectional Study in a Spanish Population. Nutrients 2022, 14, 551. https://doi.org/10.3390/nu14030551
Lorite-Fuentes I, Montero-Vilchez T, Arias-Santiago S, Molina-Leyva A. Potential Benefits of the Mediterranean Diet and Physical Activity in Patients with Hidradenitis Suppurativa: A Cross-Sectional Study in a Spanish Population. Nutrients. 2022; 14(3):551. https://doi.org/10.3390/nu14030551
Chicago/Turabian StyleLorite-Fuentes, Irene, Trinidad Montero-Vilchez, Salvador Arias-Santiago, and Alejandro Molina-Leyva. 2022. "Potential Benefits of the Mediterranean Diet and Physical Activity in Patients with Hidradenitis Suppurativa: A Cross-Sectional Study in a Spanish Population" Nutrients 14, no. 3: 551. https://doi.org/10.3390/nu14030551
APA StyleLorite-Fuentes, I., Montero-Vilchez, T., Arias-Santiago, S., & Molina-Leyva, A. (2022). Potential Benefits of the Mediterranean Diet and Physical Activity in Patients with Hidradenitis Suppurativa: A Cross-Sectional Study in a Spanish Population. Nutrients, 14(3), 551. https://doi.org/10.3390/nu14030551