
Chair-Stand Exercise Improves Sarcopenia in Rehabilitation Patients after Stroke
 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
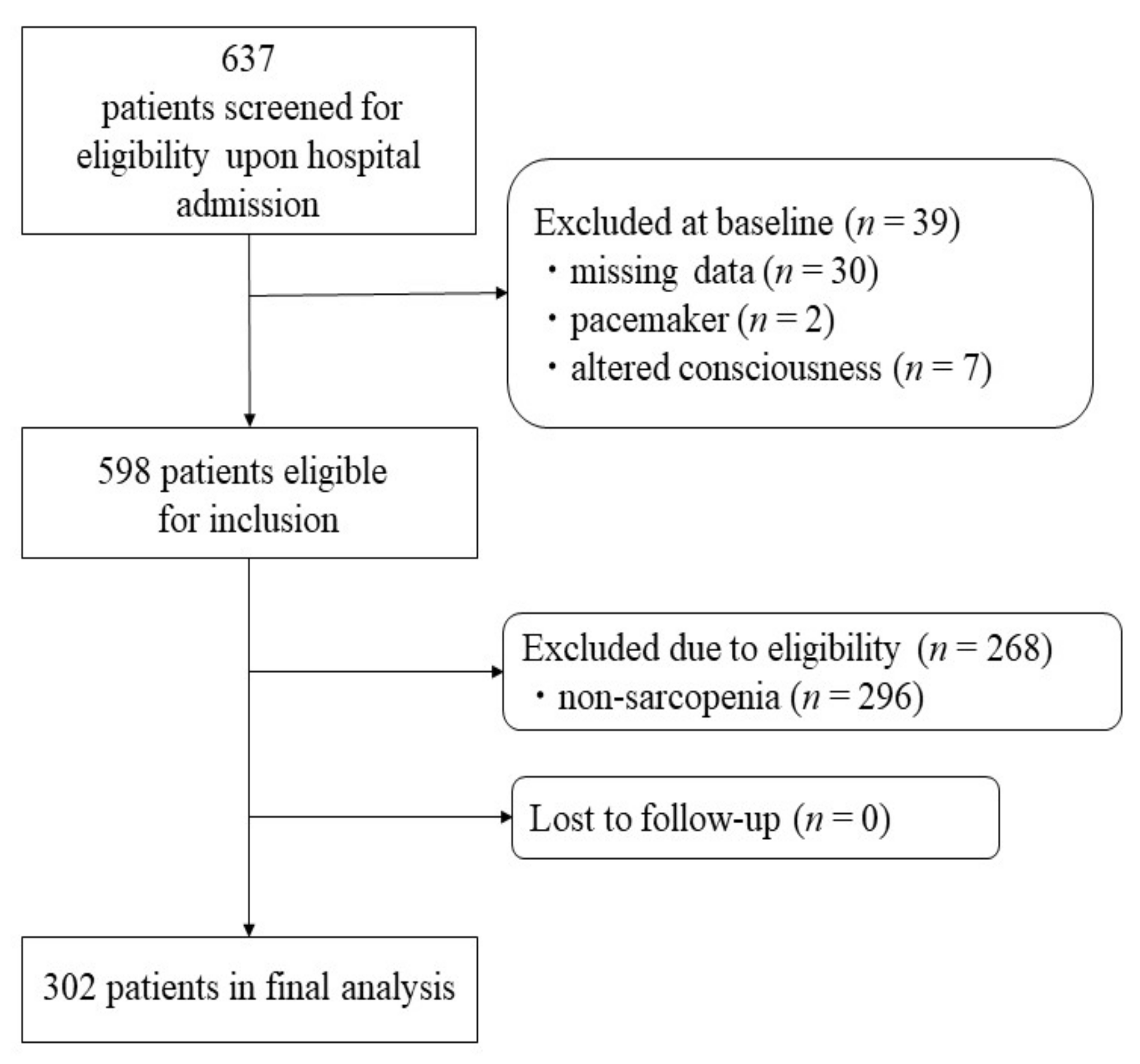
2.1. Participants and Setting
2.2. Convalescent Rehabilitation Program
2.3. “Chair-Stand Exercise” as Whole-Body Resistance Training
2.4. Data Collection
2.5. Sarcopenia Definition
2.6. Outcome Measures
2.7. Sample Size Calculation
2.8. Ethics Approval
2.9. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Shiraishi, A.; Yoshimura, Y.; Wakabayashi, H.; Tsuji, Y. Prevalence of stroke-related sarcopenia and its association with poor oral status in post-acute stroke patients: Implications for oral sarcopenia. Clin. Nutr. 2018, 37, 204–207. [Google Scholar] [CrossRef] [PubMed]
- Rondanelli, M.; Cereda, E.; Klersy, C.; Faliva, M.A.; Peroni, G.; Nichetti, M.; Gasparri, C.; Iannello, G.; Spadaccini, D.; Infantino, V.; et al. Improving rehabilitation in sarcopenia: A randomized-controlled trial utilizing a muscle-targeted food for special medical purposes. J. Cachexia Sarcopenia Muscle 2020, 11, 1535–1547. [Google Scholar] [CrossRef] [PubMed]
- Mayhew, A.J.; Amog, K.; Phillips, S.; Parise, G.; McNicholas, P.D.; De Souza, R.J.; Thabane, L.; Raina, P. The prevalence of sarcopenia in community-dwelling older adults, an exploration of differences between studies and within definitions: A systematic review and meta-analyses. Age Ageing 2019, 48, 48–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papadopoulou, S.K.; Tsintavis, P.; Potsaki, G.; Papandreou, D. Differences in the Prevalence of Sarcopenia in Community-Dwelling, Nursing Home and Hospitalized Individuals. A Systematic Review and Meta-Analysis. J. Nutr. Health Aging 2020, 24, 83–90. [Google Scholar] [CrossRef]
- Shafiee, G.; Keshtkar, A.; Soltani, A.; Ahadi, Z.; Larijani, B.; Heshmat, R. Prevalence of sarcopenia in the world: A systematic review and meta- analysis of general population studies. J. Diabetes Metab. Disord. 2017, 16, 21. [Google Scholar] [CrossRef] [Green Version]
- Petermann-Rocha, F.; Balntzi, V.; Gray, S.R.; Lara, J.; Ho, F.K.; Pell, J.P.; Celis-Morales, C. Global prevalence of sarcopenia and severe sarcopenia: A systematic review and meta-analysis. J. Cachexia Sarcopenia Muscle 2021. [Google Scholar] [CrossRef]
- Tu, D.Y.; Kao, F.M.; Tsai, S.T.; Tung, T.H. Sarcopenia among the Elderly Population: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Healthcare 2021, 9, 650. [Google Scholar] [CrossRef]
- Yoshimura, Y.; Wakabayashi, H.; Bise, T.; Nagano, F.; Shimazu, S.; Shiraishi, A.; Yamaga, M.; Koga, H. Sarcopenia is associated with worse recovery of physical function and dysphagia and a lower rate of home discharge in Japanese hospitalized adults undergoing convalescent rehabilitation. Nutrition 2019, 61, 111–118. [Google Scholar] [CrossRef]
- Yoshimura, Y.; Wakabayashi, H.; Nagano, F.; Bise, T.; Shimazu, S.; Kudo, M.; Shiraishi, A. Sarcopenic Obesity Is Associated with Activities of Daily Living and Home Discharge in Post-Acute Rehabilitation. J. Am. Med. Dir. Assoc. 2020, 21, 1475–1480. [Google Scholar] [CrossRef]
- Kido, Y.; Yoshimura, Y.; Wakabayashi, H.; Momosaki, R.; Nagano, F.; Bise, T.; Shimazu, S.; Shiraishi, A. Sarcopenia is associated with incontinence and recovery of independence in urination and defecation in post-acute rehabilitation patients. Nutrition 2021, 91–92, 111397. [Google Scholar] [CrossRef]
- Churilov, I.; Churilov, L.; Brock, K.; Murphy, D.; MacIsaac, R.J.; Ekinci, E.I. Sarcopenia Is Associated with Reduced Function on Admission to Rehabilitation in Patients with Diabetes. J. Clin. Endocrinol. Metab. 2021, 106, E687–E695. [Google Scholar] [CrossRef]
- Goates, S.; Du, K.; Arensberg, M.B.; Gaillard, T.; Guralnik, J.; Pereira, S.L. Economic Impact of Hospitalizations in US Adults with Sarcopenia. J. Frailty Aging 2019, 8, 93–99. [Google Scholar] [CrossRef]
- Arai, H.; Wakabayashi, H.; Yoshimura, Y.; Yamada, M.; Kim, H. Chapter 4 Treatment of sarcopenia. Geriatr. Gerontol. Int. 2018, 18, 28–44. [Google Scholar] [CrossRef]
- Dent, E.; Morley, J.E.; Cruz-Jentoft, A.J.; Arai, H.; Kritchevsky, S.B.; Guralnik, J.; Bauer, J.M.; Pahor, M.; Clark, B.C.; Cesari, M.; et al. International Clinical Practice Guidelines for Sarcopenia (ICFSR): Screening, Diagnosis and Management. J. Nutr. Health Aging 2018, 22, 1148–1161. [Google Scholar] [CrossRef]
- Cruz-Jentoft, J.; Landi, F.; Schneider, S.M.; Zuniga, C.; Arai, H.; Boirie, Y.; Chen, L.-K.; Fielding, R.A.; Martin, F.C.; Michel, J.-P.; et al. Prevalence of and interventions for sarcopenia in ageing adults: A systematic review. Report of the International Sarcopenia Initiative (EWGSOP and IWGS). Age Ageing 2014, 43, 748–759. [Google Scholar] [CrossRef]
- Yoshimura, Y.; Bise, T.; Shimazu, S.; Tanoue, M.; Tomioka, Y.; Araki, M.; Nishino, T.; Kuzuhara, A.; Takatsuki, F. Effects of a leucine-enriched amino acid supplement on muscle mass, muscle strength, and physical function in post-stroke patients with sarcopenia: A randomized controlled trial. Nutrition 2019, 58, 1–6. [Google Scholar] [CrossRef]
- Winstein, C.J.; Stein, J.; Arena, R.; Bates, B.; Cherney, L.R.; Cramer, S.C.; Deruyter, F.; Eng, J.J.; Fisher, B.; Harvey, R.L.; et al. Guidelines for Adult Stroke Rehabilitation and Recovery: A Guideline for Healthcare Professionals from the American Heart Association/American Stroke Association. Stroke 2016, 47, e98–e169. [Google Scholar] [CrossRef]
- Buntin, M.B.; Colla, C.H.; Deb, P.; Sood, N.; Escarce, J.J. Medicare spending and outcomes after postacute care for stroke and hip fracture. Med. Care 2010, 48, 776–784. [Google Scholar] [CrossRef] [Green Version]
- Scherbakov, N.; Sandek, A.; Doehner, W. Stroke-Related Sarcopenia: Specific Characteristics. J. Am. Med. Dir. Assoc. 2015, 16, 272–276. [Google Scholar] [CrossRef]
- Su, Y.; Yuki, M.; Otsuki, M. Prevalence of stroke-related sarcopenia: A systematic review and meta-analysis. J. Stroke Cerebrovasc. Dis. 2020, 29, 105092. [Google Scholar] [CrossRef]
- Li, W.; Yue, T.; Liu, Y. New understanding of the pathogenesis and treatment of stroke-related sarcopenia. Biomed. Pharmacother. 2020, 131, 110721. [Google Scholar] [CrossRef]
- Dennis, M. Poor nutritional status on admission predicts poor outcomes after stroke observational data from the food trial. Stroke 2003, 34, 1450–1455. [Google Scholar]
- Moore, S.A.; Hrisos, N.; Errington, L.; Rochester, L.; Rodgers, H.; Witham, M.; Sayer, A.A. Exercise as a treatment for sarcopenia: An umbrella review of systematic review evidence. Physiotherapy 2019, 107, 189–201. [Google Scholar] [CrossRef]
- Oyanagi, K.; Kitai, T.; Yoshimura, Y.; Yokoi, Y.; Ohara, N.; Kohara, N.; Sakai, N.; Honda, A.; Onishi, H.; Iwata, K. Effect of early intensive rehabilitation on the clinical outcomes of patients with acute stroke. Geriatr. Gerontol. Int. 2021, 21, 623–628. [Google Scholar] [CrossRef]
- Yoshimura, Y.; Wakabayashi, H.; Nagano, F.; Bise, T.; Shimazu, S.; Shiraishi, A. Chair-stand exercise improves post-stroke dysphagia. Geriatr. Gerontol. Int. 2020, 20, 885–891. [Google Scholar] [CrossRef]
- Matsufuji, S.; Shoji, T.; Yano, Y.; Tsujimoto, Y.; Kishimoto, H.; Tabata, T.; Emoto, M.; Inaba, M. Effect of chair stand exercise on activity of daily living: A randomized controlled trial in hemodialysis patients. J. Ren. Nutr. 2015, 25, 17–24. [Google Scholar] [CrossRef]
- Miyai, I.; Sonoda, S.; Nagai, S.; Takayama, Y.; Inoue, Y.; Kakehi, A.; Kurihara, M.; Ishikawa, M. Results of new policies for inpatient rehabilitation coverage in Japan. Neurorehabil. Neural Repair 2011, 25, 540–547. [Google Scholar] [CrossRef]
- Shimazu, S.; Yoshimura, Y.; Kudo, M.; Nagano, F.; Bise, T.; Shiraishi, A.; Sunahara, T. Frequent and personalized nutritional support leads to improved nutritional status, activities of daily living, and dysphagia after stroke. Nutrition 2021, 83, 111091. [Google Scholar] [CrossRef]
- Shiraishi, A.; Yoshimura, Y.; Wakabayashi, H.; Tsuji, Y.; Yamaga, M.; Koga, H. Hospital dental hygienist intervention improves activities of daily living, home discharge and mortality in post-acute rehabilitation. Geriatr. Gerontol. Int. 2019, 19, 189–196. [Google Scholar] [CrossRef]
- Kose, E.; Wakabayashi, H. Rehabilitation pharmacotherapy: A scoping review. Geriatr. Gerontol. Int. 2020, 20, 655–663. [Google Scholar] [CrossRef]
- Rubenstein, L.Z.; Harker, J.O.; Salvà, A.; Guigoz, Y.; Vellas, B. Screening for undernutrition in geriatric practice: Developing the short-form mini-nutritional assessment (MNA-SF). J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, M366–M372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kunieda, K.; Ohno, T.; Fujishima, I.; Hojo, K.; Morita, T. Reliability and validity of a tool to measure the severity of dysphagia: The Food Intake LEVEL Scale. J. Pain Symptom Manag. 2013, 46, 201–206. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Banks, J.L.; Marotta, C.A. Outcomes validity and reliability of the modified Rankin scale: Implications for stroke clinical trials: A literature review and synthesis. Stroke 2007, 38, 1091–1096. [Google Scholar] [CrossRef] [Green Version]
- Huang, C.Y.; Lin, G.H.; Huang, Y.J.; Song, C.Y.; Lee, Y.C.; How, M.J.; Chen, Y.-M.; Hsueh, I.-P.; Chen, M.-H.; Hsieh, C.-L. Improving the utility of the Brunnstrom recovery stages in patients with stroke: Validation and quantification. Medicine 2016, 95, e4508. [Google Scholar] [CrossRef]
- Ottenbacher, K.J.; Hsu, Y.; Granger, C.V.; Fiedler, R.C. The reliability of the functional independence measure: A quantitative review. Arch. Phys. Med. Rehabil. 1996, 77, 1226–1232. [Google Scholar] [CrossRef]
- Da Rocha, A.Q.; Lobo, P.C.B.; Pimentel, G.D. Muscle Function Loss and Gain of Body Weight during the COVID-19 Pandemic in Elderly Women: Effects of One Year of Lockdown. J. Nutr. Health Aging 2021, 25, 1028–1029. [Google Scholar] [CrossRef]
- Chen, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Chou, M.Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Asian Working Group for Sarcopenia: 2019 Consensus Update on Sarcopenia Diagnosis and Treatment. J. Am. Med. Dir. Assoc. 2020, 21, 300–307.e2. [Google Scholar] [CrossRef]
- Beckwée, D.; Delaere, A.; Aelbrecht, S.; Baert, V.; Beaudart, C.; Bruyere, O.; de Saint-Hubert, M.; Bautmans, I.; Sarcopenia Guidelines Development Group of the Belgian Society of Gerontology and Geriatrics (BSGG). Exercise Interventions for the Prevention and Treatment of Sarcopenia. A Systematic Umbrella Review. J. Nutr. Health Aging 2019, 23, 494–502. [Google Scholar] [CrossRef]
- Phu, S.; Boersma, D.; Duque, G. Exercise and Sarcopenia. J. Clin. Densitom. 2015, 18, 488–492. [Google Scholar] [CrossRef]
- Yoshimura, Y.; Bise, T.; Nagano, F.; Shimazu, S.; Shiraishi, A.; Yamaga, M.; Koga, H. Systemic Inflammation in the Recovery Stage of Stroke: Its Association with Sarcopenia and Poor Functional Rehabilitation Outcomes. Prog. Rehabil. Med. 2018, 3, 20180011. [Google Scholar] [CrossRef] [Green Version]
- Yoshimura, Y.; Wakabayashi, H.; Bise, T.; Tanoue, M. Prevalence of sarcopenia and its association with activities of daily living and dysphagia in convalescent rehabilitation ward inpatients. Clin. Nutr. 2018, 37, 2022–2028. [Google Scholar] [CrossRef]
- Fujita, E.; Taaffe, D.R.; Yoshitake, Y.; Kanehisa, H. Repeated sit-to-stand exercise enhances muscle strength and reduces lower body muscular demands in physically frail elders. Exp. Gerontol. 2019, 116, 86–92. [Google Scholar] [CrossRef]
- Wakabayashi, H.; Sakuma, K. Rehabilitation nutrition for sarcopenia with disability: A combination of both rehabilitation and nutrition care management. J. Cachexia Sarcopenia Muscle 2014, 5, 269–277. [Google Scholar] [CrossRef]
- Yoshimura, Y.; Wakabayashi, H.; Momosaki, R.; Nagano, F.; Bise, T.; Shimazu, S.; Shiraishi, A. Stored Energy Increases Body Weight and Skeletal Muscle Mass in Older, Underweight Patients after Stroke. Nutrients 2021, 13, 3274. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Total (N = 302) | Low Freq. Chair-Stand ex. (N = 154) | High Freq. Chair-Stand ex. (N = 148) | p Value | |
|---|---|---|---|---|
| Age, years | 78.6 (10.5) | 78.5 (11.6) | 78.6 (9.2) | 0.916 |
| Sex, male, n (%) | 140 (46.4) | 64 (41.6) | 76 (51.4) | 0.106 |
| Stroke type, n (%) | ||||
| Cerebral infarction | 196 (64.9) | 97 (63.0) | 99 (66.9) | 0.547 |
| Cerebral hemorrhage | 94 (31.1) | 52 (33.8) | 42 (28.4) | 0.323 |
| Subarachnoid hemorrhage | 12 (4.0) | 5 (3.2) | 7 (4.7) | 0.567 |
| Stroke history, n (%) | 96 (31.8) | 43 (27.9) | 53 (35.8) | 0.174 |
| Premorbid mRS, score | 1 (0–2) | 1 (0–3) | 1 (0–2) | 0.165 |
| Onset-admission days | 14 (10–22) | 14 (10–21) | 15 (10–26) | 0.065 |
| Paralysis, n (%) | ||||
| Right/Left/Both | 148 (49.0)/98 (32.5)/22 (7.3) | 77 (50.0)/48 (31.2)/11 (7.1) | 71 (48.0)/50 (33.8)/11 (7.4) | 0.731 |
| BRS, score | ||||
| Upper limb/Hand-finger/Lower limb | 5 (2–6)/5 (2–6)/5 (2–6) | 4 (2–5)/5 (2–6)/5 (2–6) | 4 (2–6)/5 (2–6)/5 (2–6) | 0.312 |
| FIM, score | ||||
| -Total | 44 (26–78) | 42 (25–78) | 49 (26–80) | 0.245 |
| -Motor | 26 (14–57) | 26 (13–56) | 27 (14–56) | 0.609 |
| -Cognitive | 16 (9–23) | 15 (8–23) | 17 (10–26) | 0.098 |
| FILS, score | 7 (2–9) | 7 (2–8) | 7 (2–9) | 0.111 |
| CCI, score | 3 (2–4) | 3 (2–4) | 3 (2–4) | 0.143 |
| Nutritional status | ||||
| MNA-SF, score | 5 (3–8) | 5 (3–8) | 6 (3–8) | 0.694 |
| BMI, kg/m2 | 21.2 (18.7–22.7) | 21.2 (18.7–22.9) | 21.0 (18.9–22.7) | 0.656 |
| Energy intake, kcal/kg/day | 27.9 (24.1–32.5) | 27.6 (23.8–32.6) | 28.1 (24.2–32.4) | 0.609 |
| Protein intake, g/kg/day | 1.1 (0.9–1.3) | 1.1 (0.9–1.3) | 1.1 (0.9–1.3) | 0.915 |
| Muscle-related variables | ||||
| HGS, kg | 12.6 (5.5–17.7) | 10.30 (1.0–15.2) | 14.0 (6.7–18.9) | 0.001 |
| SMI, kg/m2 | 5.1 (4.6–6.0) | 5.0 (4.7–5.9) | 5.4 (4.6–6.2) | 0.072 |
| Laboratory data | ||||
| Alb, g/dL | 3.4 (0.5) | 3.42 (0.49) | 3.49 (0.51) | 0.237 |
| CRP, g/dL | 1.2 (2.2) | 1.44 (2.64) | 1.17 (1.72) | 0.092 |
| Hb, mg/dL | 12.9 (1.5) | 12.65 (1.58) | 12.96 (1.53) | 0.124 |
| Number of drugs | 5 (3–8) | 5 (3–8) | 5 (3–8) | 0.593 |
| Rehabilitation therapy, units/day | 8.2 (7.2–8.5) | 8.2 (7.5–8.4) | 8.1 (6.9–8.5) | 0.400 |
| Chair-stand exercise, frequency/day | 77 (64–97) | 65 (52–76) | 98 (88–111) | - |
| Total (N = 302) | Low Freq. Chair-Stand ex. (N = 154) | High Freq. Chair-Stand ex. (N = 148) | p Value | |
|---|---|---|---|---|
| SMI, kg/m2 | ||||
| change (pre-post exercise) | 0.2 (0.1–0.5) | 0.1 (−0.1–0.3) | 0.4 (0.1–0.8) | <0.001 |
| at discharge | 5.4 (4.8–6.3) | 5.09 (4.71–5.90) | 5.83 (5.00–6.70) | <0.001 |
| HGS, kg | ||||
| change (pre-post exercise) | 2.4 (0.0–6.8) | 1.1 (0.0–4.5) | 3.2 (0.1–7.5) | <0.001 |
| at discharge | 15.5 (11.0–22.4) | 13.80 (9.72–18.95) | 18.40 (12.95–24.05) | <0.001 |
| Sarcopenia at discharge, number | 236 (78.1) | 136 (88.3) | 100 (67.6) | <0.001 |
| FIM-motor at discharge, score | 61 (37–83) | 55 (36–79) | 72 (40–83) | 0.052 |
| Length of hospital stay, days | 117 (73–142) | 118 (79–131) | 107 (71–128) | 0.141 |
| Home discharge, number | 154 (51.0) | 70 (45.5) | 84 (56.8) | 0.051 |
| SMI at Discharge | HGS at Discharge | Sarcopenia at Discharge | ||||||
|---|---|---|---|---|---|---|---|---|
| β | B (95% CI) | p Value | Β | B (95% CI) | p Value | OR (95% CI) | p Value | |
| Age | −0.060 | −0.005 (−0.014, 0.005) | 0.315 | −0.130 | −0.099 (−0.200, 0.002) | 0.054 | 1.091 (1.021, 1.165) | 0.010 |
| LOS | 0.110 | 0.002 (−0.001, 0.005) | 0.118 | 0.085 | 0.018 (−0.015, 0.050) | 0.278 | 0.961 (0.934, 0.989) | 0.007 |
| FIM-motor | −0.057 | −0.002 (−0.011, 0.006) | 0.579 | −0.052 | −0.022 (−0.114, 0.071) | 0.646 | 0.906 (0.842, 0.976) | 0.009 |
| FIM-cognitive | −0.036 | −0.004 (−0.021, 0.013) | 0.652 | 0.114 | 0.117 (−0.066, 0.300) | 0.207 | 0.957 (0.863, 1.061) | 0.402 |
| CCI | −0.005 | −0.003 (−0.063, 0.058) | 0.930 | −0.045 | −0.207 (−0.846, 0.431) | 0.521 | 0.638 (0.404, 1.010) | 0.055 |
| Rehabilitation | 0.026 | 0.009 (−0.028, 0.046) | 0.617 | 0.055 | 0.182 (−0.207, 0.572) | 0.355 | 1.073 (0.857, 1.343) | 0.540 |
| BRS-lower limb | 0.153 | 0.071 (0.002, 0.141) | 0.045 | −0.084 | −0.368 (−1.103, 0.366) | 0.323 | 0.734 (0.419, 1.283) | 0.278 |
| Protein intake | −0.091 | −0.358 (−0.785, 0.070) | 0.101 | 0.053 | 1.966 (−2.555, 6.486) | 0.391 | 0.573 (0.014, 2.191) | 0.771 |
| HGS at admission | 0.006 | 0.001 (−0.014, 0.015) | 0.927 | 0.520 | 0.517 (0.361, 0.672) | <0.001 | 1.045 (0.948, 1.152) | 0.374 |
| SMI at admission | 0.770 | 0.933 (0.792, 1.074) | <0.001 | 0.338 | 3.860 (2.368, 5.353) | <0.001 | 0.012 (0.001, 0.116) | <0.001 |
| Chair-stand exercise, freq./day | 0.270 | 0.008 (0.005, 0.012) | <0.001 | 0.131 | 0.039 (0.002, 0.075) | 0.039 | 0.968 (0.945, 0.992) | 0.010 |
| R2 | 0.772 | 0.751 | 0.431 | |||||
| SMI at Discharge | HGS at Discharge | Sarcopenia at Discharge | ||||||
|---|---|---|---|---|---|---|---|---|
| β | B (95% CI) | p Value | Β | B (95% CI) | p Value | OR (95% CI) | p Value | |
| Age | −0.174 | −0.016 (−0.026, −0.007) | 0.001 | −0.131 | −0.125 (−0.270, 0.020) | 0.089 | 1.035 (0.979, 1.094) | 0.229 |
| LOS | 0.044 | 0.001 (−0.002, 0.003) | 0.500 | 0.078 | 0.015 (−0.021, 0.051) | 0.417 | 0.993 (0.978, 1.009) | 0.379 |
| FIM-motor | −0.084 | −0.003 (−0.012, 0.005) | 0.412 | −0.296 | −0.122 (0.243, −0.001) | 0.048 | 1.030 (0.987, 1.075) | 0.178 |
| FIM-cognitive | 0.027 | 0.003 (−0.013, 0.018) | 0.722 | 0.087 | 0.095 (−0.138, 0.327) | 0.423 | 0.960 (0.878, 1.051) | 0.377 |
| CCI | 0.075 | 0.047 (−0.014, 0.108) | 0.131 | −0.054 | −0.343 (−1.253, 0.566) | 0.457 | 1.149 (0.788, 1.674) | 0.470 |
| Rehabilitation | −0.033 | −0.023 (−0.102, 0.057) | 0.574 | 0.102 | 0.718 (−0.464, 1.900) | 0.232 | 0.725 (0.413, 1.272) | 0.262 |
| BRS-lower limb | 0.028 | 0.012 (−0.048, 0.072) | 0.689 | 0.039 | 0.172 (−0.716, 1.061) | 0.702 | 0.931 (0.671, 1.291) | 0.666 |
| Protein intake | −0.097 | −0.252 (−0.529, 0.025) | 0.074 | −0.083 | −2.196 (−6.305, 1.913) | 0.293 | 1.472 (0.642, 2.783) | 0.148 |
| HGS at admission | 0.098 | 0.014 (−0.007, 0.036) | 0.188 | 0.629 | 0.940 (0.620, 1.259) | <0.001 | 0.873 (0.779, 0.978) | 0.019 |
| SMI at admission | 0.750 | 0.956 (0.825, 1.086) | <0.001 | −0.014 | −0.188 (−2.127, 1.752) | 0.849 | 0.180 (0.066, 0.490) | 0.001 |
| Chair-stand exercise, freq./day | 0.206 | 0.004 (0.002, 0.006) | <0.001 | 0.067 | 0.028 (0.016, 0.045) | 0.037 | 0.992 (0.979, 0.998) | 0.012 |
| R2 | 0.712 | 0.689 | 0.398 | |||||
| FIM-Motor at Discharge | Length of Hospital Stay | Home Discharge | ||||||
|---|---|---|---|---|---|---|---|---|
| β | B (95% CI) | p Value | Β | B (95% CI) | p Value | OR (95% CI) | p Value | |
| Age | −0.051 | −0.125 (−0.314, 0.063) | 0.192 | −0.195 | −0.831 (−1.228, −0.433) | <0.001 | 0.996 (0.963, 1.031) | 0.834 |
| Sex (male) | −0.308 | −15.955 (−21.167, −10.743) | <0.001 | 0.098 | 8.832 (−2.421, 20.084) | 0.124 | 0.890 (0.769, 0.1522) | 0.101 |
| Los | 0.097 | 0.056 (0.003, 0.109) | 0.040 | - | - | - | 1.008 (0.998, 1.017) | 0.129 |
| FIM-motor | 0.370 | 0.443 (0.280, 0.605) | <0.001 | −0.424 | −0.878 (−1.214, −0.541) | <0.001 | 1.075 (1.042, 1.109) | <0.001 |
| FIM-cognitive | 0.097 | 0.297 (−0.021, 0.614) | 0.067 | 0.066 | 0.350 (−0.338, 1.038) | 0.317 | 1.020 (0.969, 1.075) | 0.446 |
| CCI | −0.050 | −0.778 (−1.959, 0.403) | 0.196 | 0.109 | 2.957 (0.420, 5.494) | 0.023 | 0.894 (0.730, 1.093) | 0.274 |
| Rehabilitation | 0.069 | 0.870 (−0.056, 1.797) | 0.066 | −0.063 | −1.395 (−3.398, 0.608) | 0.172 | 1.411 (1.065, 1.870) | 0.017 |
| BRS-lower limb | 0.199 | 2.548 (1.219, 3.877) | <0.001 | −0.169 | −3.748 (−6.597, −0.900) | 0.010 | 1.094 (0.878, 1.362) | 0.424 |
| Protein intake | −0.061 | −5.257 (−11.947, 1.434) | 0.123 | 0.031 | 4.608 (−9.887, 19.102) | 0.532 | 1.019 (0.982, 1.121) | 0.122 |
| HGS at admission | 0.251 | 0.802 (0.469, 1.134) | <0.001 | −0.074 | −0.412 (−1.132, 0.308) | 0.261 | 1.065 (1.007, 1.125) | 0.027 |
| SMI at admission | 0.269 | 6.951 (4.234, 9.667) | <0.001 | −0.104 | −4.664 (−10.528, 1.200) | 0.119 | 2.046 (1.246, 3.361) | 0.005 |
| Chair-stand exercise, freq./day | 0.158 | 0.041 (0.010, 0.098) | 0.047 | −0.065 | −0.080 (−0.191, 0.031) | 0.159 | 1.005 (0.995, 1.016) | 0.288 |
| R2 | 0.617 | 0.598 | 0.554 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoshimura, Y.; Wakabayashi, H.; Nagano, F.; Bise, T.; Shimazu, S.; Shiraishi, A.; Kido, Y.; Matsumoto, A. Chair-Stand Exercise Improves Sarcopenia in Rehabilitation Patients after Stroke. Nutrients 2022, 14, 461. https://doi.org/10.3390/nu14030461
Yoshimura Y, Wakabayashi H, Nagano F, Bise T, Shimazu S, Shiraishi A, Kido Y, Matsumoto A. Chair-Stand Exercise Improves Sarcopenia in Rehabilitation Patients after Stroke. Nutrients. 2022; 14(3):461. https://doi.org/10.3390/nu14030461
Chicago/Turabian StyleYoshimura, Yoshihiro, Hidetaka Wakabayashi, Fumihiko Nagano, Takahiro Bise, Sayuri Shimazu, Ai Shiraishi, Yoshifumi Kido, and Ayaka Matsumoto. 2022. "Chair-Stand Exercise Improves Sarcopenia in Rehabilitation Patients after Stroke" Nutrients 14, no. 3: 461. https://doi.org/10.3390/nu14030461
APA StyleYoshimura, Y., Wakabayashi, H., Nagano, F., Bise, T., Shimazu, S., Shiraishi, A., Kido, Y., & Matsumoto, A. (2022). Chair-Stand Exercise Improves Sarcopenia in Rehabilitation Patients after Stroke. Nutrients, 14(3), 461. https://doi.org/10.3390/nu14030461