
Interventions on Microbiota: Where Do We Stand on a Gut–Brain Link in Autism? A Systematic Review

 , ,
, ,
Abstract
:1. Introduction
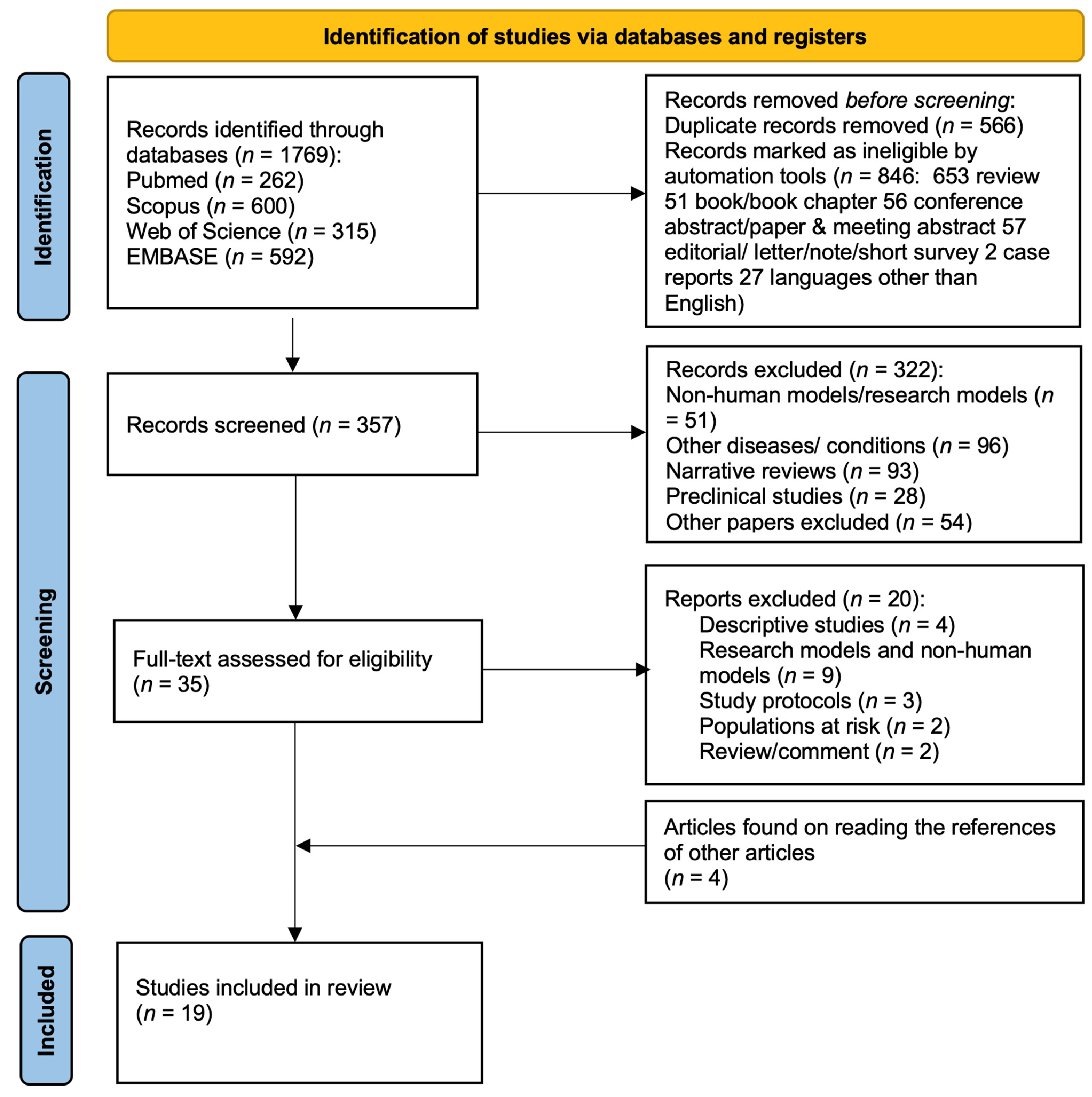
2. Materials and Methods
3. Results
4. Study Characteristics
5. Study Quality
6. Relevant Data Emerging from Studies on Treatments Acting on the Gut–Brain Axis in ASD
6.1. Clinical Studies on Probiotics
6.2. Clinical Studies on Prebiotics
6.3. Clinical Studies on Fecal Microbiota Transplantation
7. Discussion
8. Conclusions and Future Perspectives
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Narzisi, A.; Posada, M.; Barbieri, F.; Chericoni, N.; Ciuffolini, D.; Pinzino, M.; Romano, R.; Scattoni, M.L.; Tancredi, R.; Calderoni, S.; et al. Prevalence of Autism Spectrum Disorder in a large Italian catchment area: A school-based population study within the ASDEU project. Epidemiol. Psychiatr. Sci. 2018, 29, e5. [Google Scholar] [CrossRef] [PubMed]
- Dinan, T.G.; Cryan, J.F. Gut microbiota: A missing link in psychiatry. World Psychiatry 2020, 19, 111–112. [Google Scholar] [CrossRef] [PubMed]
- Collins, S.M.; Surette, M.; Bercik, P. The interplay between the intestinal microbiota and the brain. Nat. Rev. Microbiol. 2012, 10, 735–742. [Google Scholar] [CrossRef] [PubMed]
- Finegold, S.M.; Dowd, S.E.; Gontcharova, V.; Liu, C.; Henley, K.E.; Wolcott, R.D.; Youn, E.; Summanen, P.H.; Granpeesheh, D.; Dixon, D.; et al. Pyrosequencing study of fecal microflora of autistic and control children. Anaerobe 2010, 16, 444–453. [Google Scholar] [CrossRef] [PubMed]
- Adams, J.B.; Johansen, L.J.; Powell, L.D.; Quig, D.; Rubin, R.A. Gastrointestinal flora and gastrointestinal status in children with autism-comparisons to typical children and correlation with autism severity. BMC Gastroenterol. 2011, 11, 22. [Google Scholar] [CrossRef] [Green Version]
- de Theije, C.G.; Wu, J.; da Silva, S.L.; Kamphuis, P.J.; Garssen, J.; Korte, S.M.; Kraneveld, A.D. Pathways underlying the gut-to-brain connection in autism spectrum disorders as future targets for disease management. Eur. J. Pharmacol. 2011, 668 (Suppl. 1), S70–S80. [Google Scholar] [CrossRef]
- Mayer, E.A.; Padua, D.; Tillisch, K. Altered brain-gut axis in autism: Comorbidity or causative mechanisms? BioEssays 2014, 36, 933–939. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Yang, J.; Zhang, H.; Yu, J.; Yao, Z. Oral probiotic administration during pregnancy prevents autism-related behaviors in offspring induced by maternal immune activation via anti-inflammation in mice. Autism Res. 2019, 12, 576–588. [Google Scholar] [CrossRef]
- Hsiao, E.Y.; McBride, S.W.; Hsien, S.; Sharon, G.; Hyde, E.R.; McCue, T.; Codelli, J.A.; Chow, J.; Reisman, S.E.; Petrosino, J.F.; et al. Microbiota Modulate Behavioral and Physiological Abnormalities Associated with Neurodevelopmental Disorders. Cell 2013, 155, 1451–1463. [Google Scholar] [CrossRef] [Green Version]
- Sandler, R.H.; Finegold, S.M.; Bolte, E.R.; Buchanan, C.P.; Maxwell, A.P.; Väisänen, M.-L.; Nelson, M.N.; Wexler, H.M. Short-Term Benefit From Oral Vancomycin Treatment of Regressive-Onset Autism. J. Child Neurol. 2000, 15, 429–435. [Google Scholar] [CrossRef]
- Ristori, M.V.; Quagliariello, A.; Reddel, S.; Ianiro, G.; Vicari, S.; Gasbarrini, A.; Putignani, L. Autism, Gastrointestinal Symptoms and Modulation of Gut Microbiota by Nutritional Interventions. Nutrients 2019, 11, 2812. [Google Scholar] [CrossRef] [Green Version]
- Dinan, T.G.; Stanton, C.; Cryan, J.F. Psychobiotics: A Novel Class of Psychotropic. Biol. Psychiatry 2013, 74, 720–726. [Google Scholar] [CrossRef] [PubMed]
- Saulnier, D.M.; Ringel, Y.; Heyman, M.B.; Foster, J.A.; Bercik, P.; Shulman, R.J.; Versalovic, J.; Verdu, E.F.; Dinan, T.G.; Hecht, G.; et al. The intestinal microbiome, probiotics and prebiotics in neurogastroenterology. Gut Microbes 2013, 4, 17–27. [Google Scholar] [CrossRef] [PubMed]
- Petschow, B.; Doré, J.; Hibberd, P.; Dinan, T.; Reid, G.; Blaser, M.; Cani, P.; Degnan, F.H.; Foster, J.; Gibson, G.; et al. Probiotics, prebiotics, and the host microbiome: The science of translation. Ann. N. Y. Acad. Sci. 2013, 1306, 1–17. [Google Scholar] [CrossRef]
- Duque, A.L.R.F.; Demarqui, F.M.; Santoni, M.M.; Zanelli, C.F.; Adorno, M.A.T.; Milenkovic, D.; Mesa, V.; Sivieri, K. Effect of probiotic, prebiotic, and synbiotic on the gut microbiota of autistic children using an in vitro gut microbiome model. Food Res. Int. 2021, 149, 110657. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.H.; Cho, Y.-S. Fecal Microbiota Transplantation: Current Applications, Effectiveness, and Future Perspectives. Clin. Endosc. 2016, 49, 257–265. [Google Scholar] [CrossRef] [PubMed]
- Grehan, M.J.; Borody, T.J.; Leis, S.M.; Campbell, J.; Mitchell, H.; Wettstein, A. Durable Alteration of the Colonic Microbiota by the Administration of Donor Fecal Flora. J. Clin. Gastroenterol. 2010, 44, 551–561. [Google Scholar] [CrossRef] [PubMed]
- Kang, D.-W.; Adams, J.B.; Gregory, A.C.; Borody, T.; Chittick, L.; Fasano, A.; Khoruts, A.; Geis, E.; Maldonado, J.; McDonough-Means, S.; et al. Microbiota Transfer Therapy alters gut ecosystem and improves gastrointestinal and autism symptoms: An open-label study. Microbiome 2017, 5, 10. [Google Scholar] [CrossRef]
- Kang, D.-W.; Adams, J.B.; Coleman, D.M.; Pollard, E.L.; Maldonado, J.; McDonough-Means, S.; Caporaso, J.G.; Krajmalnik-Brown, R. Long-term benefit of Microbiota Transfer Therapy on autism symptoms and gut microbiota. Sci. Rep. 2019, 9, 5821. [Google Scholar] [CrossRef]
- Li, N.; Chen, H.; Cheng, Y.; Xu, F.; Ruan, G.; Ying, S.; Tang, W.; Chen, L.; Chen, M.; Lv, L.; et al. Fecal Microbiota Transplantation Relieves Gastrointestinal and Autism Symptoms by Improving the Gut Microbiota in an Open-Label Study. Front. Cell. Infect. Microbiol. 2021, 11, 759435. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 2021, 372, 89. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.C.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parracho, H.M.R.T.; Gibson, G.R.; Knott, F.; Bosscher, D.; Kleerebezem, M.; McCartney, A.L. A double-blind, placebo-controlled, crossover-designed probiotic feeding study in children diagnosed with autistic spectrum disorders. Int. J. Probiotics Prebiotics 2010, 5, 69–74. [Google Scholar]
- Kałużna-Czaplińska, J.; Błaszczyk, S. The level of arabinitol in autistic children after probiotic therapy. Nutrition 2012, 28, 124–126. [Google Scholar] [CrossRef]
- West, R.; Roberts, E.; Sichel, L.S.; Sichel, J. Improvements in Gastrointestinal Symptoms among Children with Autism Spectrum Disorder Receiving the Delpro® Probiotic and Immunomodulator Formulation. Probiotics Health 2013, 1, 1–6. [Google Scholar]
- Arnold, L.E.; Luna, R.A.; Williams, K.; Chan, J.; Parker, R.A.; Wu, Q.; Hollway, J.A.; Jeffs, A.; Lu, F.; Coury, D.L.; et al. Probiotics for Gastrointestinal Symptoms and Quality of Life in Autism: A Placebo-Controlled Pilot Trial. J. Child Adolesc. Psychopharmacol. 2019, 29, 659–669. [Google Scholar] [CrossRef]
- Liu, Y.-W.; Liong, M.T.; Chung, Y.-C.E.; Huang, H.-Y.; Peng, W.-S.; Cheng, Y.-F.; Lin, Y.-S.; Wu, Y.-Y.; Tsai, Y.-C. Effects of Lactobacillus plantarum PS128 on Children with Autism Spectrum Disorder in Taiwan: A Randomized, Double-Blind, Placebo-Controlled Trial. Nutrients 2019, 11, 820. [Google Scholar] [CrossRef] [Green Version]
- Niu, M.; Li, Q.; Zhang, J.; Wen, F.; Dang, W.; Duan, G.; Li, H.; Ruan, W.; Yang, P.; Guan, C.; et al. Characterization of Intestinal Microbiota and Probiotics Treatment in Children With Autism Spectrum Disorders in China. Front. Neurol. 2019, 10, 1084. [Google Scholar] [CrossRef] [Green Version]
- Santocchi, E.; Guiducci, L.; Prosperi, M.; Calderoni, S.; Gaggini, M.; Apicella, F.; Tancredi, R.; Billeci, L.; Mastromarino, P.; Grossi, E.; et al. Effects of Probiotic Supplementation on Gastrointestinal, Sensory and Core Symptoms in Autism Spectrum Disorders: A Randomized Controlled Trial. Front. Psychiatry 2020, 11, 944. [Google Scholar] [CrossRef]
- Mensi, M.; Rogantini, C.; Marchesi, M.; Borgatti, R.; Chiappedi, M. Lactobacillus plantarum PS128 and Other Probiotics in Children and Adolescents with Autism Spectrum Disorder: A Real-World Experience. Nutrients 2021, 13, 2036. [Google Scholar] [CrossRef]
- Grimaldi, R.; Gibson, G.R.; Vulevic, J.; Giallourou, N.; Castro-Mejía, J.L.; Hansen, L.H.; Gibson, E.L.; Nielsen, D.S.; Costabile, A. A prebiotic intervention study in children with autism spectrum disorders (ASDs). Microbiome 2018, 6, 133. [Google Scholar] [CrossRef]
- Guo, M.; Zhu, J.; Yang, T.; Lai, X.; Liu, X.; Liu, J.; Chen, J.; Li, T. Vitamin A improves the symptoms of autism spectrum disorders and decreases 5-hydroxytryptamine (5-HT): A pilot study. Brain Res. Bull. 2018, 137, 35–40. [Google Scholar] [CrossRef]
- Inoue, R.; Sakaue, Y.; Kawada, Y.; Tamaki, R.; Yasukawa, Z.; Ozeki, M.; Ueba, S.; Sawai, C.; Nonomura, K.; Tsukahara, T.; et al. Dietary supplementation with partially hydrolyzed guar gum helps improve constipation and gut dysbiosis symptoms and behavioral irritability in children with autism spectrum disorder. J. Clin. Biochem. Nutr. 2019, 64, 217–223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, J.; Liu, X.; Xiong, X.-Q.; Yang, T.; Cui, T.; Hou, N.-L.; Lai, X.; Liu, S.; Guo, M.; Liang, X.-H.; et al. Effect of vitamin A supplementation on gut microbiota in children with autism spectrum disorders—A pilot study. BMC Microbiol. 2017, 17, 204. [Google Scholar] [CrossRef]
- Shaaban, S.Y.; El Gendy, Y.G.; Mehanna, N.S.; El-Senousy, W.M.; El-Feki, H.S.A.; Saad, K.; El-Asheer, O.M. The role of probiotics in children with autism spectrum disorder: A prospective, open-label study. Nutr. Neurosci. 2018, 21, 676–681. [Google Scholar] [CrossRef]
- Sanctuary, M.R.; Kain, J.N.; Chen, S.Y.; Kalanetra, K.; Lemay, D.; Rose, D.R.; Yang, H.T.; Tancredi, D.J.; German, J.B.; Slupsky, C.M.; et al. Pilot study of probiotic/colostrum supplementation on gut function in children with autism and gastrointestinal symptoms. PLoS ONE 2019, 14, e0210064. [Google Scholar] [CrossRef]
- Wang, Y.; Li, N.; Yang, J.-J.; Zhao, D.-M.; Chen, B.; Zhang, G.-Q.; Chen, S.; Cao, R.-F.; Yu, H.; Zhao, C.-Y.; et al. Probiotics and fructo-oligosaccharide intervention modulate the microbiota-gut brain axis to improve autism spectrum reducing also the hyper-serotonergic state and the dopamine metabolism disorder. Pharmacol. Res. 2020, 157, 104784. [Google Scholar] [CrossRef] [PubMed]
- Magiati, I.; Moss, J.; Yates, R.; Charman, T.; Howlin, P. Is the Autism Treatment Evaluation Checklist a useful tool for monitoring progress in children with autism spectrum disorders? J. Intellect. Disabil. Res. 2011, 55, 302–312. [Google Scholar] [CrossRef]
- Davenport, T.L. Autism Behavior Checklist, in Encyclopedia of Child Behavior and Development; Goldstein, S., Naglieri, J.A., Eds.; Springer: Boston, MA, USA, 2011; pp. 182–183. [Google Scholar]
- Rasquin, A.; Di Lorenzo, C.; Forbes, D.; Guiraldes, E.; Hyams, J.S.; Staiano, A.; Walker, L.S. Childhood Functional Gastrointestinal Disorders: Child/Adolescent. Gastroenterology 2006, 130, 1527–1537. [Google Scholar] [CrossRef] [PubMed]
- Hansen, R.L.; Ozonoff, S.; Krakowiak, P.; Angkustsiri, K.; Jones, C.; Deprey, L.J.; Le, D.-N.; Croen, L.A.; Hertz-Picciotto, I. Regression in Autism: Prevalence and Associated Factors in the CHARGE Study. Ambul. Pediatr. 2008, 8, 25–31. [Google Scholar] [CrossRef]
- Svedlund, J.; Sjodin, I.; Dotevall, G. GSRS?A clinical rating scale for gastrointestinal symptoms in patients with irritable bowel syndrome and peptic ulcer disease. Dig. Dis. Sci. 1988, 33, 129–134. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Fu, X.; Liao, X.; Li, Y. Effects of gut microbial-based treatments on gut microbiota, behavioral symptoms, and gastrointestinal symptoms in children with autism spectrum disorder: A systematic review. Psychiatry Res. 2020, 293, 113471. [Google Scholar] [CrossRef] [PubMed]
- Martínez-González, A.E.; Andreo-Martínez, P. Prebióticos, probióticos y trasplante de microbiota fecal en el autismo: Una revisión sistemática. Revista de Psiquiatría y Salud Mental 2020, 13, 150–164. [Google Scholar] [CrossRef] [PubMed]
- Davies, C.; Mishra, D.; Eshraghi, R.S.; Mittal, J.; Sinha, R.; Bulut, E.; Mittal, R.; Eshraghi, A.A. Altering the gut microbiome to potentially modulate behavioral manifestations in autism spectrum disorders: A systematic review. Neurosci. Biobehav. Rev. 2021, 128, 549–557. [Google Scholar] [CrossRef]
- Farrah, K.; Young, K.; Tunis, M.C.; Zhao, L. Risk of bias tools in systematic reviews of health interventions: An analysis of PROSPERO-registered protocols. Syst. Rev. 2019, 8, 280. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Wan, G.-B.; Huang, M.-S.; Agyapong, G.; Zou, T.-L.; Zhang, X.-Y.; Liu, Y.-W.; Song, Y.-Q.; Tsai, Y.-C.; Kong, X.-J. Probiotic Therapy for Treating Behavioral and Gastrointestinal Symptoms in Autism Spectrum Disorder: A Systematic Review of Clinical Trials. Curr. Med Sci. 2019, 39, 173–184. [Google Scholar] [CrossRef] [PubMed]
- Slim, K.; Nini, E.; Forestier, D.; Kwiatkowski, F.; Panis, Y.; Chipponi, J. Methodological index for non-randomized studies (MINORS ): Development and validation of a new instrument. ANZ J. Surg. 2003, 73, 712–716. [Google Scholar] [CrossRef]
- Ng, Q.X.; Loke, W.; Venkatanarayanan, N.; Lim, D.Y.; Soh, A.Y.S.; Yeo, W.S. A Systematic Review of the Role of Prebiotics and Probiotics in Autism Spectrum Disorders. Medicina 2019, 55, 129. [Google Scholar] [CrossRef] [Green Version]
- Ma, L.-L.; Wang, X.; Yang, Z.-H.; Huang, D.; Weng, H.; Zeng, X.-T. Methodological quality (risk of bias) assessment tools for primary and secondary medical studies: What are they and which is better? Mil. Med Res. 2020, 7, 7. [Google Scholar] [CrossRef] [Green Version]
- Blades, M. Autism: An interesting dietary case history. Nutr. Food Sci. 2000, 30, 137–140. [Google Scholar] [CrossRef] [Green Version]
- Grossi, E.; Melli, S.; Dunca, D.; Terruzzi, V. Unexpected improvement in core autism spectrum disorder symptoms after long-term treatment with probiotics. SAGE Open Med Case Rep. 2016, 4, 2050313X16666231. [Google Scholar] [CrossRef]
- Kobliner, V.; Mumper, E.; Baker, S.M. Reduction in Obsessive Compulsive Disorder and Self-Injurious Behavior With Saccharomyces boulardii in a Child with Autism: A Case Report. Integr. Med. 2018, 17, 38–41. [Google Scholar]
- Cheng, L.-H.; Liu, Y.-W.; Wu, C.-C.; Wang, S.; Tsai, Y.-C. Psychobiotics in mental health, neurodegenerative and neurodevelopmental disorders. J. Food Drug Anal. 2019, 27, 632–648. [Google Scholar] [CrossRef] [Green Version]
- Lord, C.; Rutter, M.; DiLavore, P.C.; Risi, S.; Gotham, K.; Bishop, S.L. Autism Diagnostic Observation Schedule, (ADOS-2) Modules, 2nd ed.; Western Psychological Services: Torrance, CA, USA, 2012. [Google Scholar]
- Tomova, A.; Husarova, V.; Lakatosova, S.; Bakos, J.; Vlkova, B.; Babinska, K.; Ostatnikova, D. Gastrointestinal microbiota in children with autism in Slovakia. Physiol. Behav. 2015, 138, 179–187. [Google Scholar] [CrossRef] [PubMed]
- Pierce, K.; Gazestani, V.H.; Bacon, E.; Barnes, C.C.; Cha, D.; Nalabolu, S.; Lopez, L.; Moore, A.; Pence-Stophaeros, S.; Courchesne, E. Evaluation of the Diagnostic Stability of the Early Autism Spectrum Disorder Phenotype in the General Population Starting at 12 Months. JAMA Pediatr. 2019, 173, 578–587. [Google Scholar] [CrossRef]
- Horlin, C.; Falkmer, M.; Parsons, R.; Albrecht, M.; Falkmer, T. The Cost of Autism Spectrum Disorders. PLoS ONE 2014, 9, e106552. [Google Scholar] [CrossRef] [Green Version]
- Lord, C.; Charman, T.; Havdahl, A.; Carbone, P.; Anagnostou, E.; Boyd, B.; Carr, T.; de Vries, P.J.; Dissanayake, C.; Divan, G.; et al. The Lancet Commission on the future of care and clinical research in autism. Lancet 2021, 399, 271–334. [Google Scholar] [CrossRef]
- Patusco, R.; Ziegler, J. Role of Probiotics in Managing Gastrointestinal Dysfunction in Children with Autism Spectrum Disorder: An Update for Practitioners. Adv. Nutr. Int. Rev. J. 2018, 9, 637–650. [Google Scholar] [CrossRef]
- Glascoe, F.P. Parents’ Evaluation of Developmental Status: How Well Do Parents’ Concerns Identify Children With Behavioral and Emotional Problems? Clin. Pediatr. 2003, 42, 133–138. [Google Scholar] [CrossRef]
- Jones, R.M.; Carberry, C.; Hamo, A.; Lord, C. Placebo-like response in absence of treatment in children with Autism. Autism Res. 2017, 10, 1567–1572. [Google Scholar] [CrossRef]
- Whalley, B.; Hyland, M. Placebo by proxy: The effect of parents’ beliefs on therapy for children’s temper tantrums. J. Behav. Med. 2012, 36, 341–346. [Google Scholar] [CrossRef]
- Clooney, A.G.; Fouhy, F.; Sleator, R.D.; O’Driscoll, A.; Stanton, C.; Cotter, P.D.; Claesson, M.J. Comparing Apples and Oranges?: Next Generation Sequencing and Its Impact on Microbiome Analysis. PLoS ONE 2016, 11, e0148028. [Google Scholar] [CrossRef]
- Veenstra-VanderWeele, J.; Cook, E.H.; King, B.H.; Zarevics, P.; Cherubini, M.; Walton-Bowen, K.; Bear, M.F.; Wang, P.P.; Carpenter, R.L. Arbaclofen in Children and Adolescents with Autism Spectrum Disorder: A Randomized, Controlled, Phase 2 Trial. Neuropsychopharmacology 2017, 42, 1390–1398. [Google Scholar] [CrossRef] [PubMed]
- Hollander, E.; Uzunova, G. Are there new advances in the pharmacotherapy of autism spectrum disorders? World Psychiatry 2017, 16, 101–102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vrieze, A.; Out, C.; Fuentes, S.; Jonker, L.; Reuling, I.; Kootte, R.S.; van Nood, E.; Holleman, F.; Knaapen, M.; Romijn, J.A.; et al. Impact of oral vancomycin on gut microbiota, bile acid metabolism, and insulin sensitivity. J. Hepatol. 2014, 60, 824–831. [Google Scholar] [CrossRef]
- Freedberg, D.E.; Toussaint, N.; Chen, S.; Ratner, A.; Whittier, S.; Wang, T.C.; Wang, H.H.; Abrams, J.A. Proton Pump Inhibitors Alter Specific Taxa in the Human Gastrointestinal Microbiome: A Crossover Trial. Gastroenterology 2015, 149, 883–885. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Reference | Country | Population | Intervention | Dose | Study Design | Microbiota Analysis (Sequencing Methods) | Main Results | Limits | |
|---|---|---|---|---|---|---|---|---|---|
| Sandler et al. (2000) | U.S. | 11 ASD (regressive onset) 10 ♂ 1 ♀ Age 3.5–7 yrs | PRO | Vancomycin + PRO (Lact acidophilus, Lact bulgaricus, Bifid bifidum) | Vancomycin (500 mg/d) 3/day × 8 wks, PRO (40 × 109 CFU/mL) × 4 wks | Open-label trial | NO | Short-term improvement in ASD symptoms (CARS) during vancomycin treatment | Reduced compliance during PRO treatment No control group (microbiota compared with microbiota of adults) Small sample, unblinded study |
| Parracho et al. (2010) | England | 62 ASD 59 ♂ 3 ♀ age 4–16 yrs | PRO | Lact plantarum WCFS1 | 4.5 × 1010 CFU/cp, 1 cp/day 3 wks per arm (PRO-wash out-PLA-wash out) | Randomized double blind placebo-controlled trial, cross-over | YES (FISH) | More aggressive and antisocial behaviors, anxiety problems and communication difficulties in the PLA group Improvement of the anti-social behaviors, anxiety, and communication problems No major differences in GI symptoms ↑ Lact/Enterococci and ↓ Clostridium coccoides found in the stools of ASD children as compared with PLA | Very high dropout rates (17/62 completed the study, 9 PRO and 8 PLA) No TD control group |
| Kaluzna-Czaplinska e Blaszczyk (2012) | Poland | 22 ASD 20 ♂ 2 ♀ age 4–10 yrs Severe GI symptoms | PRO | Lact acidophilus (Rosell-11 species) | 5 × 109 CFU/g2/day × 2 mths | Open-label trial with self-control study | NO | Improvement in ability of concentration and carrying out orders; no difference in reacting to other people’s emotions or using eye contact | High risk of selection bias Unblinded study Microbiota not analyzed No TD control group No PLA group |
| West et al. (2013) | U.S. | 33 ASD ♂♀missing age 3–16 yrs | PRO | DelPRO (Lact acidophilus, casei, delbrueckii + Bifid longum, bifidum + 8 mg Lact rhamnosus V lysate) | 1 × 108 billion CFU 3 times/day × 21 days | Open-label trial | NO | 88% subjects ↓ ATEC total score, 48% ↓ diarrhea, 52% ↓ constipation | Risk of selection bias 25/33 reported ATEC scores, 21/33 returned stool frequency diaries Unblinded study Microbiota not analyzed No TD control group No PLA group |
| Kang et al. (2017) | U.S. | 18 ASD with GI symptoms (moderate/severe) 16 ♂ 2 ♀ age 7–16 yrs | FMT | SHGM orally or rectally | Initial dose 2.5 × 1012 cells/day and maintenance dose 2.5 × 109 cells/day for 7 or 8 weeks (+vancomycin + MoviPrep + Prilosec) Duration: 4 mths and 2 wks | Open-label trial | YES (NGS) | ↓ 80% reduction of GI symptoms at the end of treatment lasting 8 wks after treatment. Behavioural symptoms of ASD significantly improved and continued improving 8 wks after treatment. ↑ diversity and abundance of Bifid, Prevotella and Desulfovibrio, increased after MTT, lasting for 8 wks | ASD symptoms changes not reported Small sample, unblinded study No TD control group No PLA group |
| Liu et al. (2017) | China | 64 ASD 55 ♂ 9 ♀ age 1–8 yrs | PRE | 20 study participants (17 ♂ 3 ♀) with plasma retinol deficiency (<1.05 μmol/L) treated with VA | 200,000 UI once × 6 mths | Single-blind, nonrandomized, interventional pilot study | YES (NGS) | Significant ↑ Bacteroidetes/Firmicutes and ↓ Bifid; no change in the ASD severity or behavioral problems | No PLA group No TD control group |
| Grimaldi et al. (2018) | England | 41 ASD 31 ♂ 10 ♀ age 4–11 yrs | PRE | Bimuno galacto-oligosaccharide (B-GOS®: 80% galacto-oligosaccharides) | 1.8 g in powder (unknown frequency) × 6 mths. At the end of intervention, patients were followed-up for 2 additional weeks. | Randomized double blind placebo-controlled trial | YES (FISH) | Improvements in anti-social behaviour After treatment: ↑ Lachnospiraceae, significant changes in faecal and urinary metabolites | High dropout rates (26/41 completed the study) No TD control group |
| Guo et al. (2018) | China | 33 ASD (28 ♂ 5 ♀) age 5.14 ± 1.33 yrs 32 TD; age 5.18 ± 0.87 yrs | PRE | VA in the 33 ASD | Single administration 200,000 UI | Open-label, interventional pilot study | NO | 6 mths after administration: reduction of ASD severity and 5-hydroxytryptamine (positively correlated with ASD symptoms) | Unblinded study Microbiota not analyzed No PLA group |
| Shaaban et al. (2018) | Egypt | 30 ASD 19 ♂ 11 ♀ age 5–9 yrs 30 HC children (relatives) age 5–9 yrs | PRE + PRO | Lact acidophilus + Lact rhamnosus +Bifid longum and dried carrot | 1 g = 100 × 106 CFU for each species 5 g/day × 3 mths | Open-label, prospective study | Unclear | ↑ fecal levels of Bifid and Lact, significant improvements in ASD severity (↓ ATEC) and GI symptoms (6-GSI) | Unblinded study No TD control group |
| Arnold et al. (2019) | U.S. | 13 ASD-GI-anxiety 6 ♂ 4 ♀ 6 ASD with PRO 4 ASD with PLA age 2–11 yrs | PRO | VISBIOME: 4 Lact strains (casei, plantarum, acidophilus, delbrueckii subsp Bulgaricus) + 3 Bifid strains (longum, infantis, breve)+ 1 Strept thermophilus strain and starch | 9 × 105 bacteria in half packet Half packet/2 times per day in the first 4 wks 1 packet/ 2 times per day if no effects are observed at 4 wks and 15 wks Duration: 4 mths and 3 wks | Randomized double blind placebo-controlled trial, crossover | YES (NGS) | PRO: ↑ LactImprovement of GI symptoms and anxiety compared to baseline, but without statistical significance | High dropout rates (10/13 completed the study) Small sample No TD control group |
| Inoue et al. (2019) | Japan | 13 ASD 12 ♂ 1 ♀ age 4–9 yrs | PRE | Partially hydrolyzed guar gum (Taiyo Kagaku Co.Ltd., Mie, Japan) β-endogalactomannase produced by a strain of Asp. Niger | 6 g/day Duration: 2–15 mths (median = 2) | Open-label, interventional study | YES (NGS) | Significant ↓ irritability after supplementation with partially hydrolyzed guar gum | Unblinded study No TD control group No PLA group Small sample |
| Kang et al. (2019) | U.S. | 18 ASD with GI symptoms (moderate/severe) 16 ♂ 2 ♀ age 7–17 yrs | FMT | SHGM orally or rectally | Initial dose 2.5 × 1012 cells/day and maintenance dose 2.5 × 109 cells/day for 7 or 8 weeks (+vancomycin + MoviPrep + Prilosec) Duration: 2-year follow-up | Open-label trial | YES (NGS) | Changes in gut microbiota lasted for 2 yrs, including significant ↑ in bacterial diversity and relative abundance of Bifid | ASD symptoms changes not reported Small sample, unblinded study No TD control group No PLA group |
| Liu et al. (2019) | China | 39 ASD with PRO 41 ASD with PLA 80 ♂ 0 ♀ age 7–15 yrs | PRO | Lact plantarum PS128, 3 × 1010 CFU cp | 1 cp/day × 1 mth | Randomized double blind placebo-controlled trial | YES (NGS) | ↓ anxiety, hyperactivity and opposition/defiance behaviors; no change in the ASD symptoms | High dropout rates (9 out 80 subjects) Microbiota not analyzed No TD control group |
| Niu et al. (2019) | China | 114 ASD (22 GI with PRO + ABA; 15 NGI with PRO + ABA; 28 ABA) ♂ ♀missing 40 TD age 3–8 yrs | PRO | 3 Lact strains (bulgaricus, acidophilus, casei) + 3 Bifid strains (infantis, longum, bifidum) | 6 g/day (36 billion CFU in total) + ABA training Duration: 1 mth | Open-label, two-arm, randomized trial | YES (NGS) | PRO + ABA vs only ABA: ↓ Total and subdomain ATEC scores; ↓ GI in 86.4% of 22 ASD GI with PRO + ABA | Small sample, unblinded study |
| Sanctuary et al. (2019) | U.S. | (20 ASD initially screened) 8 ASD with GI symptoms 7♂ 1 ♀age 2–11 yrs | PRE + PRO | Bifidobacterium infantis in combination with a bovine colostrum product (BCP) as a source of oligosaccharides | PRO 20 billion CFU/day, BCP 5.1–10.8 g/day 4 ASD with PRO + BCP 4 ASD with BCP 5 wks + 2 wks wash out + 5 wks | Randomized double blind trial, crossover | YES (NGS) | Combined treatment: some participants ↓ frequency of GI symptoms (++pain, diarrhea, stool consistency) and some atypical behaviors (++irritability, stereotypies, hypo/ hyperactivity) ↓ IL-13 and TNFα production in some participants | High dropout rates (8/20 completed the study) Lack of a control group with PLA and a PRO-only group No TD control group |
| Santocchi et al. (2020) | Italy | 85 ASD (30 GI and 55 NGI) 71♂ 14 ♀ Average age 4.2 yrs | PRO | De Simone formulation-Vivomixx® (1 Strept strain + 3 Bifid strains + 4 Lact strains) | 2 packets/day (900 billions of bacteria) in the first mth and 1 packet/day (450 billions of bacteria) for the next 5 months | Randomized double blind placebo-controlled trial | NO | NGI PRO vs NGI PLA groups: ↓ ADOS GI PRO vs GI PLA groups: ↑ improvements in some GI symptoms, adaptive functioning and sensory profiles | High dropout rates (>GI group), 63/85 completed the study No information about microbiota No TD control group |
| Wang et al. (2020) | China | 26 ASD (16 ASD with PRE + PRO; 10 ASD with PLA) 24♂ 2 ♀ age 3–9 yrs | PRE + PRO | 4 PRO strains (Bifid infantis and lactis, Lact rhamnosus and paracasei) + fructooligosaccharide (FOS) | 1010 CFU/pack/day 1, 2 or 3.6 mths | Randomized double blind placebo-controlled trial | YES (NGS) | ↓ Total and subdomain ATEC scores compared to baseline ↓ Total 6-GSI score | Lack of a PRO-only group No TD control group |
| Mensi et al. (2021) | Italy | 131 ASD 112 ♂ 19 ♀ Average age 86.1 ± 41.1 mths | PRO | Lact plantarum (105 ASD), OP (26 ASD) | Lact plantarum group: 3 × 1010 CFU if weight < 30 kg, 6 × 1010 CFU if weight > 30 kg OP group: prescribed PRO based on age, weight, and specific product Duration: 6 mths | Open-label trial | NO | ↑ level of shared attention (54 ASD), ↓ stereotyped movements (43 ASD), ↑ communication skills (32 ASD) and ↑ personal autonomies (23 ASD) Higher improvements in Lact plantarum group No different improvements between GI and NGI subjects | Unblinded study Unbalanced number of subjects between Lact plantarum and OP groups Heterogeneous treatment in OP group Microbiota not analyzed No TD control group No PLA group |
| Li et al. (2021) | China | 40 ASD (37 ♂ 3 ♀) age 8.03 ± 3.73 yrs 16 TD; age 7.13 ± 3.20 yrs | FMT | SHGM orally or rectally | Rectal route: dose of 2 × 1014 CFU, 50–100 mL per child, once a week. Oral route: dose of 2 × 1014 CFU, 8–16 capsules per child, once a week (+polyethylene glycol) Duration: 1 mth of FMT and 2 mths FU after the end of treatment | Open-label trial | YES (NGS) | ↓ 35% reduction of GI symptoms at the end of treatment, lasting 8 wks after treatment, improvement of stool properties at the end of treatment compared to baseline, persisting 8 wks after FMT in ASD children. Mood, behavior, emotion, language and core ASD symptoms improved after FMT ↓ parents’ anxiety levels | Unblinded study No PLA group |
| First Author, Year | Randomization Process | Deviations from Intended Interventions | Missing Outcome Data | Measurement of the Outcome | Selection of the Reported Result | Overall Risk-of-Bias |
|---|---|---|---|---|---|---|
| Parracho, 2010 | Low | High | High | Low | Low | High |
| Grimaldi, 2018 | Low | Low | High | Low | Unclear | High |
| Arnold, 2019 | Low | Low | Low | High | Low | High |
| Liu, 2019 | Low | Low | Low | Low | Low | Low |
| Sanctuary, 2019 | Low | Low | High | Low | Low | High |
| Santocchi, 2020 | Low | Low | Low | Low | Low | Low |
| Wang, 2020 | Low | High | High | Low | High | High |
| Pre-Intervention | At Intervention | Postintervention | ||||||
|---|---|---|---|---|---|---|---|---|
| First Author, Year | Bias Due to Confounding | Bias in Selection of Participants into the Study | Bias in Classification of Interventions | Bias Due to Deviations from Intended Interventions | Bias Due to Missing Data | Bias in Measurement of Outcomes | Bias in Selection of the Reported Result | Overall Risk-of-Bias |
| Sandler, 2000 | High | High | Low | High | High | Low | Low | High |
| Kaluzna-Czaplinska, 2012 | Low | High | High | Low | Low | High | Low | High |
| West, 2013 | High | High | Low | High | High | High | High | High |
| Kang, 2017 and 2019 | High | High | Low | High | High | Low | High | High |
| Liu, 2017 | Unclear | Low | Low | Low | High | Low | High | High |
| Guo, 2018 | High | High | Low | High | Low | High | High | High |
| Shaaban, 2018 | Low | Low | Low | High | Unclear | Low | High | High |
| Inoue, 2019 | Low | Unclear | Unclear | High | Low | Low | High | High |
| Niu, 2019 | Low | Unclear | High | High | High | Low | High | High |
| Mensi, 2021 | High | Low | High | High | Low | High | High | High |
| Li, 2021 | High | High | Low | Low | Low | Low | High | High |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Prosperi, M.; Santocchi, E.; Guiducci, L.; Frinzi, J.; Morales, M.A.; Tancredi, R.; Muratori, F.; Calderoni, S. Interventions on Microbiota: Where Do We Stand on a Gut–Brain Link in Autism? A Systematic Review. Nutrients 2022, 14, 462. https://doi.org/10.3390/nu14030462
Prosperi M, Santocchi E, Guiducci L, Frinzi J, Morales MA, Tancredi R, Muratori F, Calderoni S. Interventions on Microbiota: Where Do We Stand on a Gut–Brain Link in Autism? A Systematic Review. Nutrients. 2022; 14(3):462. https://doi.org/10.3390/nu14030462
Chicago/Turabian StyleProsperi, Margherita, Elisa Santocchi, Letizia Guiducci, Jacopo Frinzi, Maria Aurora Morales, Raffaella Tancredi, Filippo Muratori, and Sara Calderoni. 2022. "Interventions on Microbiota: Where Do We Stand on a Gut–Brain Link in Autism? A Systematic Review" Nutrients 14, no. 3: 462. https://doi.org/10.3390/nu14030462
APA StyleProsperi, M., Santocchi, E., Guiducci, L., Frinzi, J., Morales, M. A., Tancredi, R., Muratori, F., & Calderoni, S. (2022). Interventions on Microbiota: Where Do We Stand on a Gut–Brain Link in Autism? A Systematic Review. Nutrients, 14(3), 462. https://doi.org/10.3390/nu14030462