
The Impact of a High-Carbohydrate/Low Fat vs. Low-Carbohydrate Diet on Performance and Body Composition in Physically Active Adults: A Cross-Over Controlled Trial


Abstract
:
1. Introduction
2. Materials and Methods
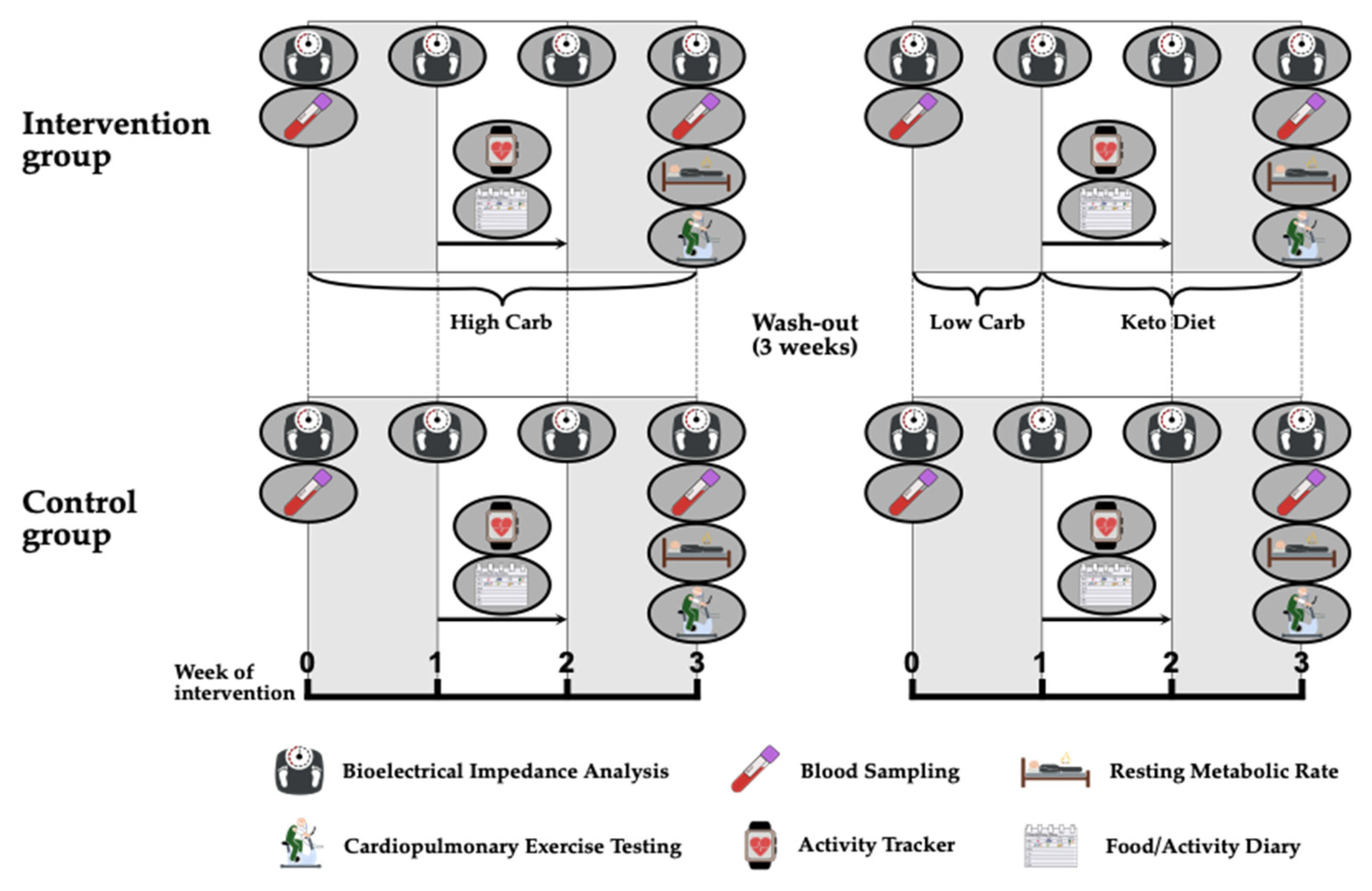
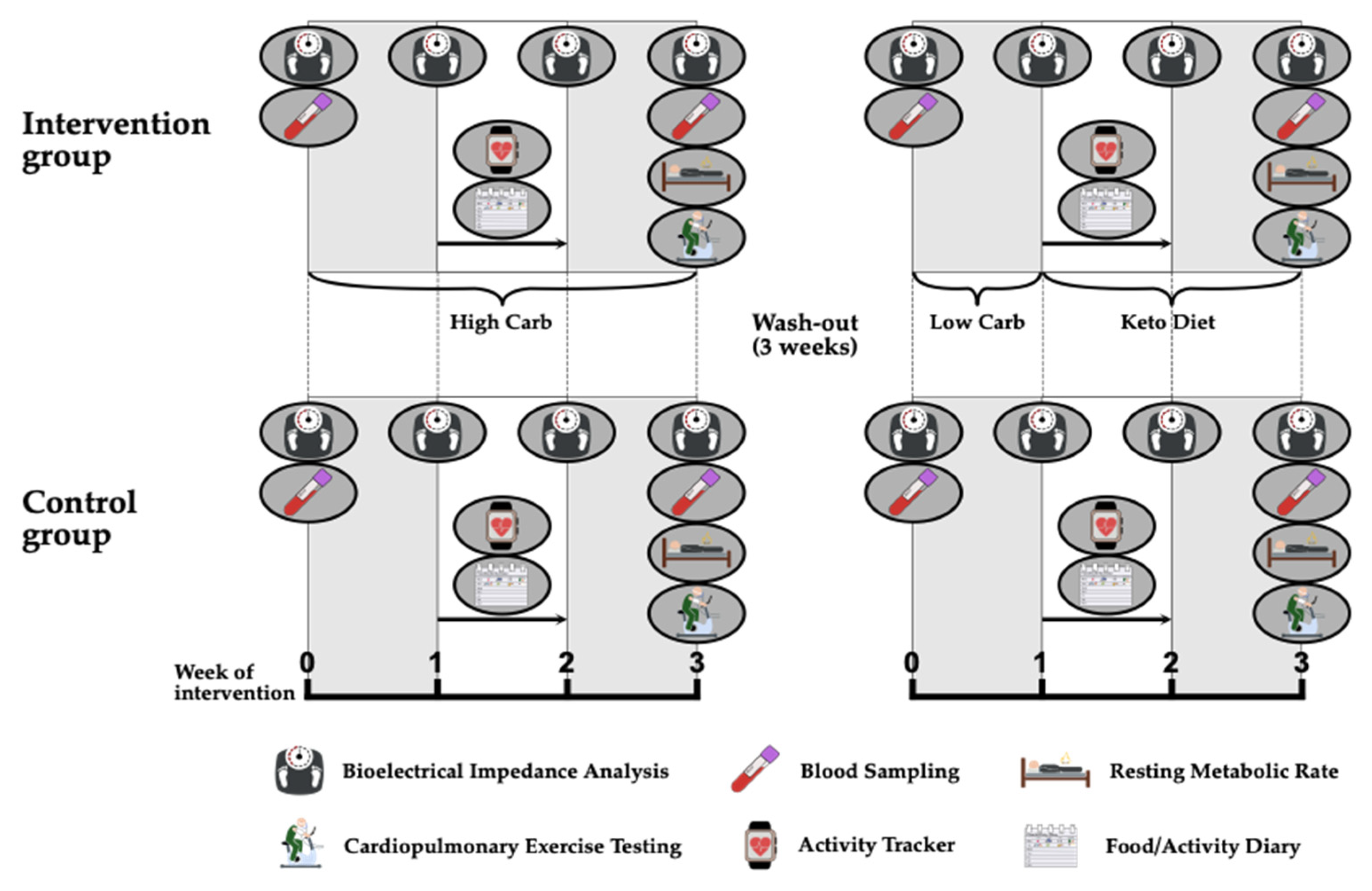
2.1. Design and Participants
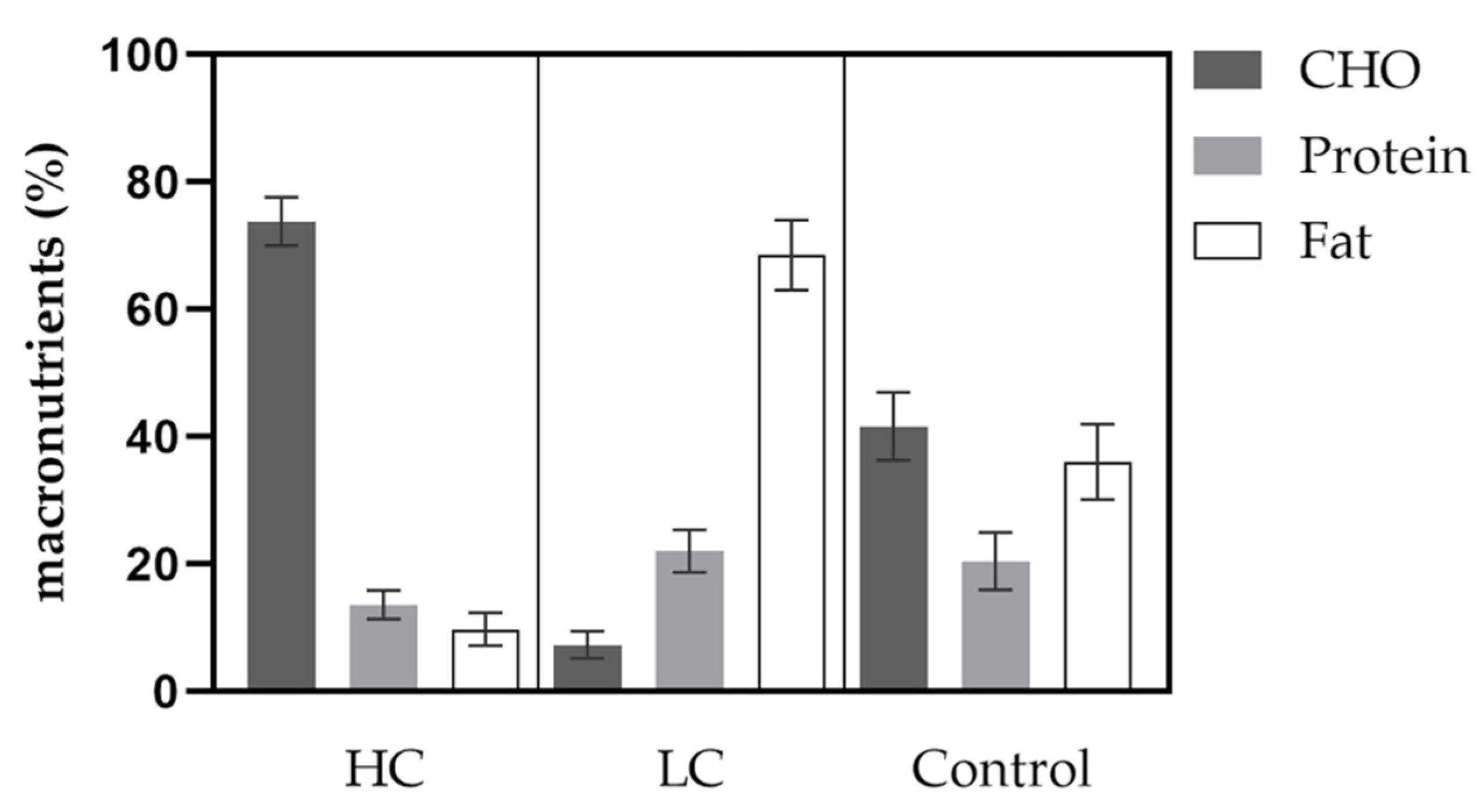
2.2. Diet Intervention
2.3. Aerobic Performance
2.4. Resting Metabolic Rate
2.5. Body Composition
2.6. Daily Activity and Nutrition
2.7. Venous Blood Samples
2.8. Statistical Analysis
3. Results
3.1. Performance Parameters
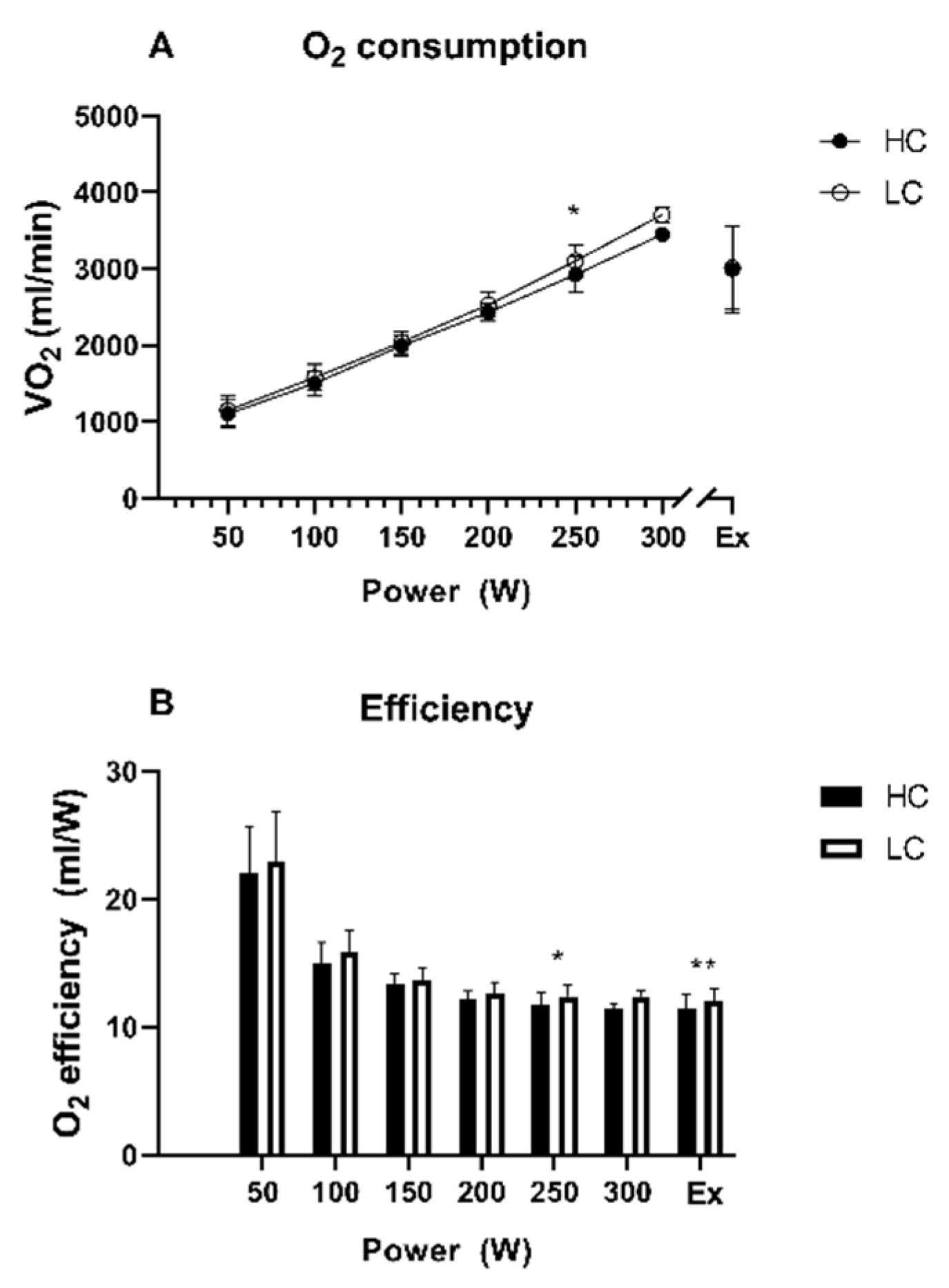
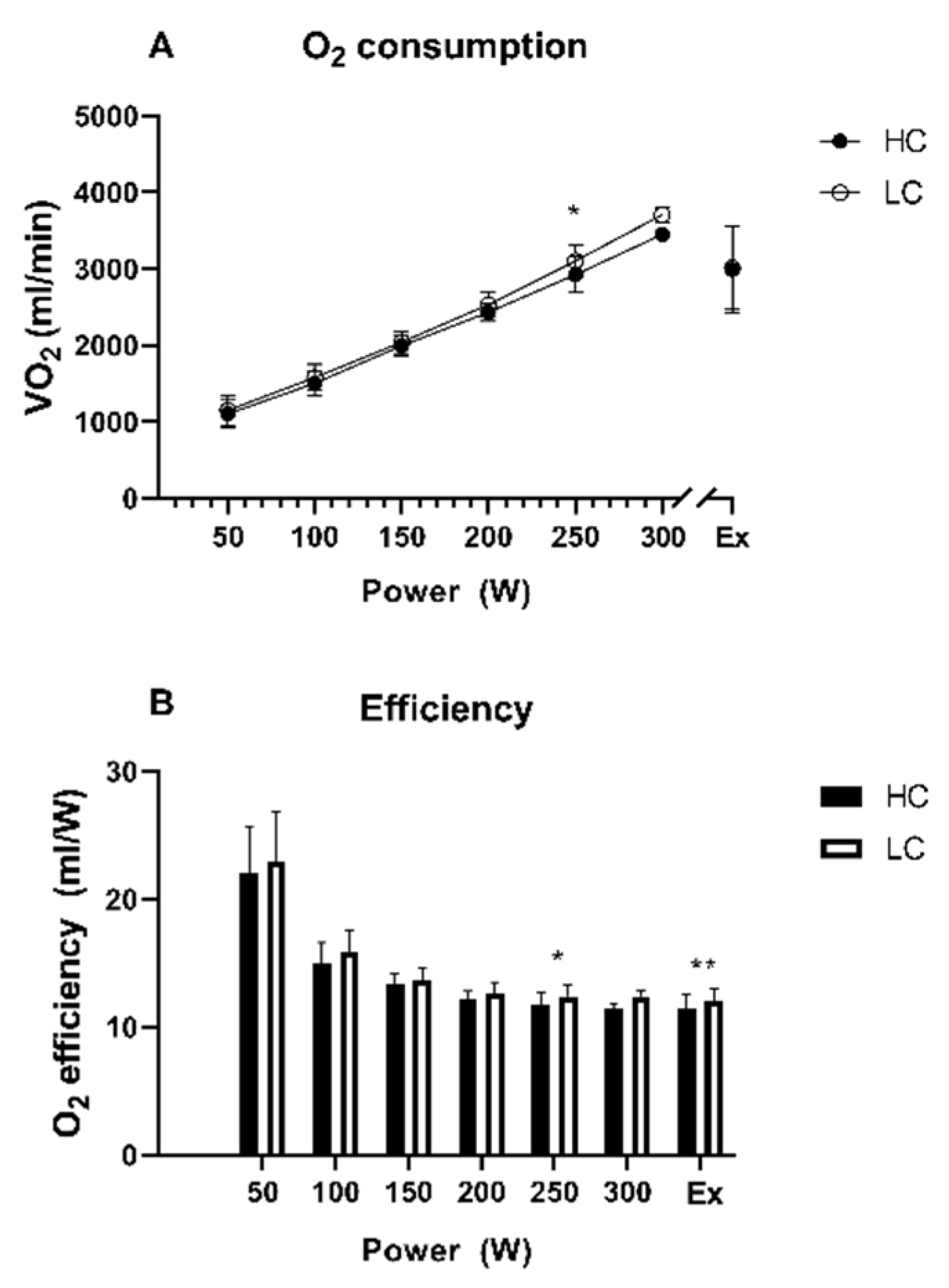
3.1.1. Peak Oxygen Uptake (VO2peak)
3.1.2. Peak Performance (Ppeak)
3.1.3. Oxygen Efficiency (O2 Efficiency)
3.1.4. Time to Exhaustion (TTE)
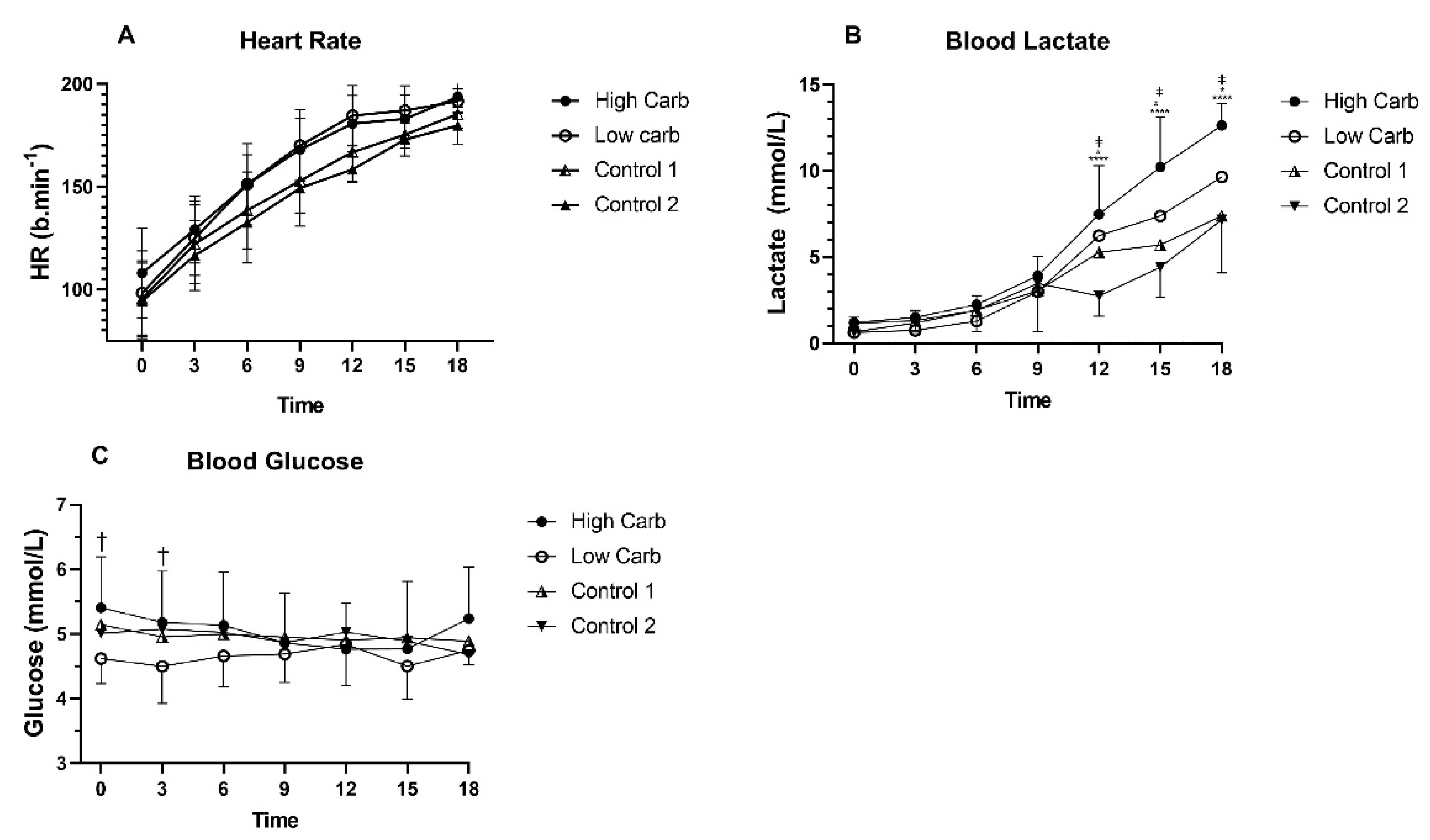
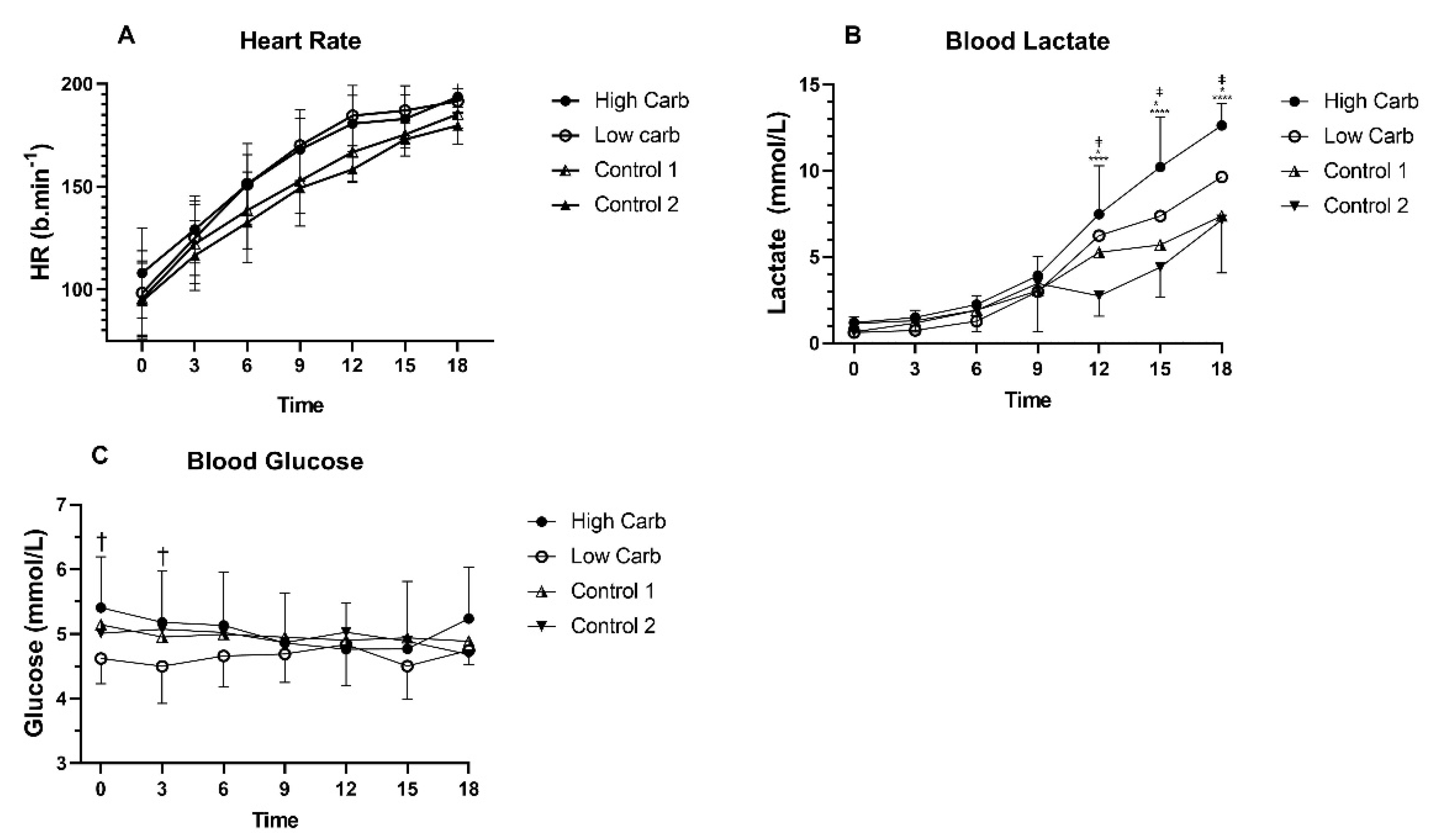
3.1.5. Heart Rate during CPX Test
3.1.6. Blood Lactate during CPX Testing
3.1.7. Blood Glucose during CPX Testing
3.1.8. Correlations of Respiratory and Functional Capacity Data
3.2. Body Composition, Physical Activity and Nutrition
3.2.1. Body Mass
3.2.2. Lean Body Mass and Skeletal Muscle Mass
3.2.3. Body Fat and Visceral Fat
3.2.4. Physical Activity
3.2.5. Resting Metabolic Rate (RMR)
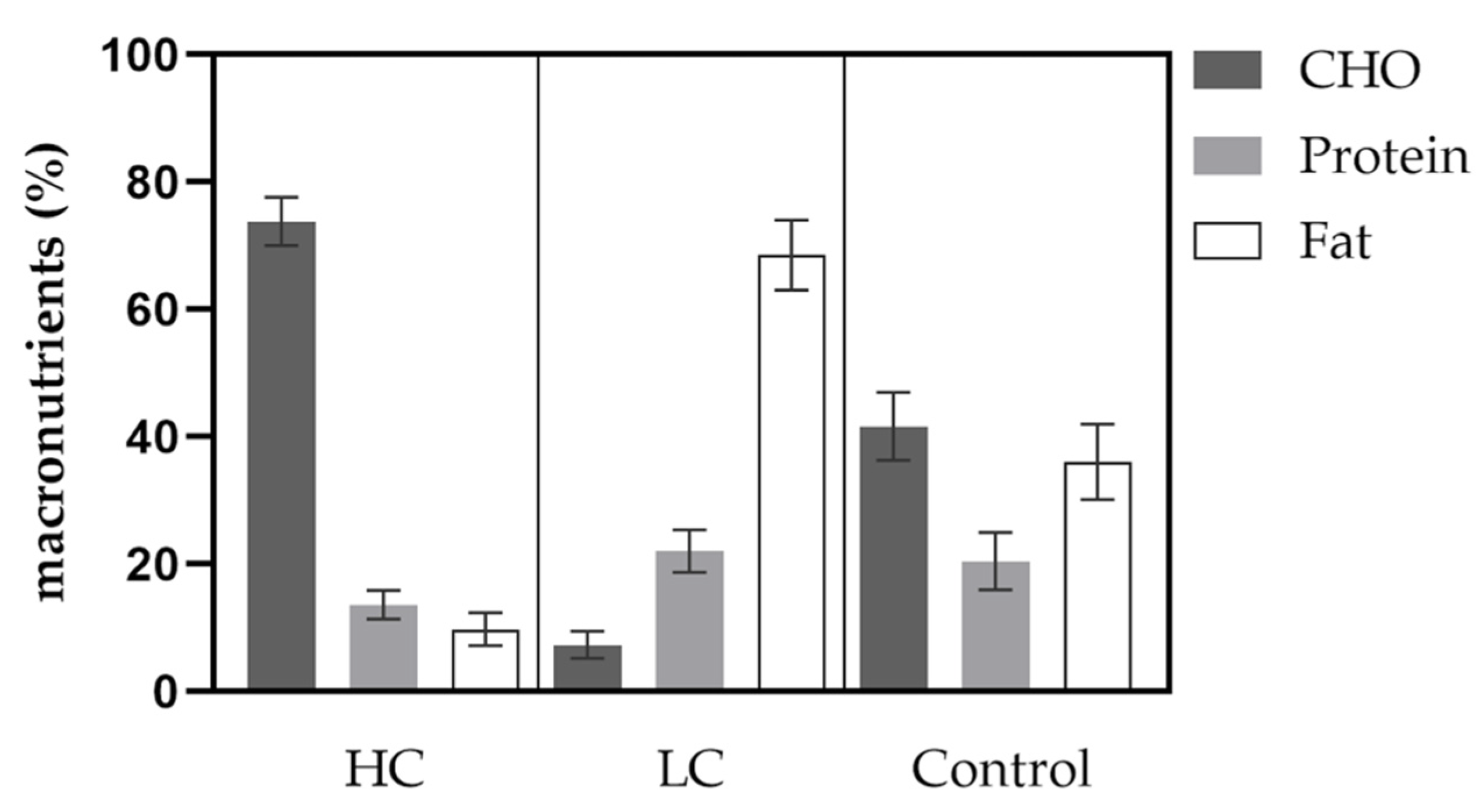
3.2.6. Nutrition
3.3. Biochemical Parameters
3.3.1. Beta-Hydroxybutyrate
3.3.2. Total Cholesterol
3.3.3. Low-Density-Lipoprotein (LDL-C)
3.3.4. High-Density-Lipoprotein (HDL-C)
3.3.5. Triglycerides (TG)
3.3.6. C-Reactive Protein (CRP) and Interleukin 6 (IL-6)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Phillips, J.A. Dietary Guidelines for Americans, 2020–2025. Workplace Health Saf. 2021, 69, 395. [Google Scholar] [CrossRef]
- Spriet, L.L. Performance Nutrition for Athletes. Sports Med. 2019, 49, 1–2. [Google Scholar] [CrossRef] [Green Version]
- Huntriss, R.; Campbell, M.; Bedwell, C. The interpretation and effect of a low-carbohydrate diet in the management of type 2 diabetes: A systematic review and meta-analysis of randomised controlled trials. Eur. J. Clin. Nutr. 2018, 72, 311–325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- VanItallie, T.B.; Nufert, T.H. Ketones: Metabolism’s ugly duckling. Nutr. Rev. 2003, 61, 327–341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adam-Perrot, A.; Clifton, P.; Brouns, F. Low-carbohydrate diets: Nutritional and physiological aspects. Obes. Rev. 2006, 7, 49–58. [Google Scholar] [CrossRef]
- Paoli, A.; Rubini, A.; Volek, J.S.; Grimaldi, K.A. Beyond weight loss: A review of the therapeutic uses of very-low-carbohydrate (ketogenic) diets. Eur. J. Clin. Nutr. 2013, 67, 789–796. [Google Scholar] [CrossRef] [Green Version]
- Margolis, L.M.; O’Fallon, K.S. Utility of Ketone Supplementation to Enhance Physical Performance: A Systematic Review. Adv. Nutr. 2020, 11, 412–419. [Google Scholar] [CrossRef] [Green Version]
- Harvey, C.; Schofield, G.M.; Williden, M. The use of nutritional supplements to induce ketosis and reduce symptoms associated with keto-induction: A narrative review. PeerJ 2018, 6, e4488. [Google Scholar] [CrossRef]
- Aronica, L.; Volek, J.; Poff, A.; D’Agostino, D.P. Genetic variants for personalised management of very low carbohydrate ketogenic diets. BMJ Nutr. Prev. Health 2020, 3, 363–373. [Google Scholar] [CrossRef]
- Helge, J.W. A high carbohydrate diet remains the evidence based choice for elite athletes to optimise performance. J. Physiol. 2017, 595, 2775. [Google Scholar] [CrossRef] [Green Version]
- Valenzuela, P.L.; Castillo-Garcia, A.; Lucia, A.; Naclerio, F. Effects of Combining a Ketogenic Diet with Resistance Training on Body Composition, Strength, and Mechanical Power in Trained Individuals: A Narrative Review. Nutrients 2021, 13, 83. [Google Scholar] [CrossRef]
- Lambert, E.V.; Speechly, D.P.; Dennis, S.C.; Noakes, T.D. Enhanced endurance in trained cyclists during moderate intensity exercise following 2 weeks adaptation to a high fat diet. Eur. J. Appl. Physiol. Occup. Physiol. 1994, 69, 287–293. [Google Scholar] [CrossRef]
- Walberg, J.L.; Ruiz, V.K.; Tarlton, S.L.; Hinkle, D.E.; Thye, F.W. Exercise capacity and nitrogen loss during a high or low carbohydrate diet. Med. Sci. Sports Exerc. 1988, 20, 34–43. [Google Scholar] [CrossRef]
- Phinney, S.D.; Horton, E.S.; Sims, E.A.; Hanson, J.S.; Danforth, E., Jr.; LaGrange, B.M. Capacity for moderate exercise in obese subjects after adaptation to a hypocaloric, ketogenic diet. J. Clin. Investig. 1980, 66, 1152–1161. [Google Scholar] [CrossRef] [PubMed]
- Brinkworth, G.D.; Noakes, M.; Clifton, P.M.; Buckley, J.D. Effects of a low carbohydrate weight loss diet on exercise capacity and tolerance in obese subjects. Obesity 2009, 17, 1916–1923. [Google Scholar] [CrossRef] [PubMed]
- Volek, J.S.; Noakes, T.; Phinney, S.D. Rethinking fat as a fuel for endurance exercise. Eur. J. Sport Sci. 2015, 15, 13–20. [Google Scholar] [CrossRef] [PubMed]
- Bogardus, C.; LaGrange, B.M.; Horton, E.S.; Sims, E.A. Comparison of carbohydrate-containing and carbohydrate-restricted hypocaloric diets in the treatment of obesity. Endurance and metabolic fuel homeostasis during strenuous exercise. J. Clin. Investig. 1981, 68, 399–404. [Google Scholar] [CrossRef] [Green Version]
- Cordain, L.; Eaton, S.B.; Sebastian, A.; Mann, N.; Lindeberg, S.; Watkins, B.A.; O’Keefe, J.H.; Brand-Miller, J. Origins and evolution of the Western diet: Health implications for the 21st century. Am. J. Clin. Nutr. 2005, 81, 341–354. [Google Scholar] [CrossRef]
- Kanter, M. High-Quality Carbohydrates and Physical Performance: Expert Panel Report. Nutr. Today 2018, 53, 35–39. [Google Scholar] [CrossRef] [Green Version]
- Kerksick, C.M.; Arent, S.; Schoenfeld, B.J.; Stout, J.R.; Campbell, B.; Wilborn, C.D.; Taylor, L.; Kalman, D.; Smith-Ryan, A.E.; Kreider, R.B.; et al. International society of sports nutrition position stand: Nutrient timing. J. Int. Soc. Sports Nutr. 2017, 14, 33. [Google Scholar] [CrossRef]
- Marquet, L.A.; Hausswirth, C.; Molle, O.; Hawley, J.A.; Burke, L.M.; Tiollier, E.; Brisswalter, J. Periodization of Carbohydrate Intake: Short-Term Effect on Performance. Nutrients 2016, 8, 755. [Google Scholar] [CrossRef] [Green Version]
- Hofmann, P.; Tschakert, G. Special Needs to Prescribe Exercise Intensity for Scientific Studies. Cardiol. Res. Pract. 2011, 2011, 209302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burke, L.M.; Kiens, B.; Ivy, J.L. Carbohydrates and fat for training and recovery. J. Sports Sci. 2004, 22, 15–30. [Google Scholar] [CrossRef] [Green Version]
- Pitsiladis, Y.P.; Maughan, R.J. The effects of alterations in dietary carbohydrate intake on the performance of high-intensity exercise in trained individuals. Eur. J. Appl. Physiol. Occup. Physiol. 1999, 79, 433–442. [Google Scholar] [CrossRef] [PubMed]
- Burke, L.M. Ketogenic low-CHO, high-fat diet: The future of elite endurance sport? J. Physiol. 2021, 599, 819–843. [Google Scholar] [CrossRef]
- Hu, J.R.; Wu, Y.; Sacks, F.M.; Appel, L.J.; Miller Iii, E.R.; Young, J.H.; Juraschek, S.P. Effects of carbohydrate quality and amount on plasma lactate: Results from the OmniCarb trial. BMJ Open Diabetes Res. Care 2020, 8, e001457. [Google Scholar] [CrossRef] [PubMed]
- Ullmann, D.; Connor, W.E.; Hatcher, L.F.; Connor, S.L.; Flavell, D.P. Will a high-carbohydrate, low-fat diet lower plasma lipids and lipoproteins without producing hypertriglyceridemia? Arterioscler. Thromb. 1991, 11, 1059–1067. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Retterstol, K.; Svendsen, M.; Narverud, I.; Holven, K.B. Effect of low carbohydrate high fat diet on LDL cholesterol and gene expression in normal-weight, young adults: A randomized controlled study. Atherosclerosis 2018, 279, 52–61. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Xu, D. Effects of aerobic exercise on lipids and lipoproteins. Lipids Health Dis. 2017, 16, 132. [Google Scholar] [CrossRef] [Green Version]
- Shai, I.; Schwarzfuchs, D.; Henkin, Y.; Shahar, D.R.; Witkow, S.; Greenberg, I.; Golan, R.; Fraser, D.; Bolotin, A.; Vardi, H.; et al. Weight loss with a low-carbohydrate, Mediterranean, or low-fat diet. N. Engl. J. Med. 2008, 359, 229–241. [Google Scholar] [CrossRef] [Green Version]
- Parks, E.J. Effect of dietary carbohydrate on triglyceride metabolism in humans. J. Nutr. 2001, 131, 2772S–2774S. [Google Scholar] [CrossRef] [PubMed]
- Mansoor, N.; Vinknes, K.J.; Veierod, M.B.; Retterstol, K. Effects of low-carbohydrate diets v. low-fat diets on body weight and cardiovascular risk factors: A meta-analysis of randomised controlled trials. Br. J. Nutr. 2016, 115, 466–479. [Google Scholar] [CrossRef] [PubMed]
- Bueno, N.B.; de Melo, I.S.; de Oliveira, S.L.; da Rocha Ataide, T. Very-low-carbohydrate ketogenic diet v. low-fat diet for long-term weight loss: A meta-analysis of randomised controlled trials. Br. J. Nutr. 2013, 110, 1178–1187. [Google Scholar] [CrossRef] [Green Version]
- Masood, W.; Annamaraju, P.; Uppaluri, K.R. Ketogenic Diet; StatPearls: Treasure Island, FL, USA, 2021. [Google Scholar]
- Ma, S.; Huang, Q.; Tominaga, T.; Liu, C.; Suzuki, K. An 8-Week Ketogenic Diet Alternated Interleukin-6, Ketolytic and Lipolytic Gene Expression, and Enhanced Exercise Capacity in Mice. Nutrients 2018, 10, 1696. [Google Scholar] [CrossRef] [Green Version]
- Kammerer, U.; Klement, R.J.; Joos, F.T.; Sutterlin, M.; Reuss-Borst, M. Low Carb and Ketogenic Diets Increase Quality of Life, Physical Performance, Body Composition, and Metabolic Health of Women with Breast Cancer. Nutrients 2021, 13, 1029. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Intervention Group (n = 18) | Control Group (n = 6) | p-Value | |
|---|---|---|---|
| Females | 13 | 1 | |
| Age (years) | 24.9 ± 1.3 | 28.5 ± 6.9 | 0.03 |
| BMI (kg/m2) | 21.8 ± 1.8 | 23.1 ± 2.9 | 0.22 |
| CRP (mg/dL) | 1.2 ± 0.7 | 1.4 ± 1.0 | 0.09 |
| HDL-C (mg/dL) | 76.7 ± 9.7 | 58.7 ± 11.2 | <0.0001 |
| LDL-C (mg/dL) | 95.8 ± 30.7 | 87.1 ± 13.7 | 0.54 |
| Cholesterol (mg/dL) | 188 ± 34 | 163 ± 26 | 0.09 |
| Triglycerides (mg/dL) | 78 ± 32 | 84 ± 37 | 0.30 |
| BHB (mmol/L) | 0.04 ± 0.04 | 0.09 ± 0.01 | 0.44 |
| Parameter | After HC | After LC | After Control 1 | After Control 2 | p-Value HC vs. LC | p-Value HC vs. Control 1 | p-Value HC vs. Control 2 | p-Value LC vs. Control 1 | p-Value LC vs. Control 2 |
|---|---|---|---|---|---|---|---|---|---|
| VO2peak (mL/min/kg) | 47 ± 7 | 47 ± 7 | 49 ± 7 | 47 ± 9 | ns | ns | ns | ns | |
| PPeak (Watt) | 251 ± 43 | 240 ± 45 | 311 ± 61 | 308 ± 69 | 0.0001 | 0.02 | 0.03 | 0.009 | 0.02 |
| TTE (Minutes) | 14.47 ± 2.36 | 14.08 ± 2.36 | 18.20 ± 3.42 | 18.1 ± 4.1 | 0.002 | 0.02 | 0.04 | 0.01 | 0.009 |
| HC | LC | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Parameter | Baseline | Week 1 | Week 2 | Week 3 | Δ Week 3 | Baseline | Week 1 | Week 2 | Week 3 | Δ Week 3 |
| Body mass (kg) | 65.2 ± 11.1 | 64.6 ± 11.0 ** | 63.8 ± 10.9 *** | 63.8 ±11.1 *** | −1.4 ± 0.9 | 64.8 ± 11.6 | 63.9 ± 11.2 *** | 63.5 ± 11.1 *** | 63.5 ±11.3 *** | −1.3 ± 0.9 |
| Lean body mass (kg) | 50.5 ± 11.7 | 50.5 ± 11.7 | 50.2 ± 11.7 | 50.4 ±11.5 | −0.2 ± 0.9 | 50.5 ± 11.7 | 50.4 ± 11.7 | 50.3 ± 11.5 | 50.6 ± 11.7 | 0.2 ± 1.1 |
| Skeletal muscle mass (kg) | 28.3 ± 7.3 | 28.3 ± 7.3 | 28.1 ± 7.2 | 28.2 ± 7.0 | −0.1 ± 0.6 | 28.3 ± 7.2 | 28.3 ± 7.2 | 28.2 ± 7.1 | 28.4 ± 7.2 | 0.1 ± 0.7 |
| Body fat (%) | 22.7 ± 6.5 | 22.1 ± 6.5 | 21.6 ± 6.6 ** | 21.2 ± 6.2 ** | −1.4 ± 1.4 | 22.3 ± 5.7 | 21.3 ± 6.0 *** | 21.0 ± 6.1 *** | 20.6 ± 6.0 *** | −1.7 ± 1.4 |
| Visceral fat (cm2) | 58.6 ± 17.8 | 56.3 ± 16.8 * | 54.1 ± 16.8 *** | 53.9 ± 16.2 *** | −4.7 ± 3.8 | 57.6 ± 15.9 | 53.3 ± 16.3 *** | 51.9 ± 16.5 *** | 50.6 ± 16.6 *** | −7.0 ± 4.6 |
| Total body water (L) | 37.2 ± 8.6 | 37.1 ± 8.6 | 37.0 ± 8.6 | 37.1 ± 8.5 | −0.1 ± 0.7 | 37.1 ± 8.6 | 37.1 ± 8.6 | 37.0 ± 8.5 | 37.2 ± 8.7 | 0.1 ± 0.8 |
| Parameter | HC Baseline | after HC | p-Value Baseline vs. after HC | LC Baseline | after LC | p-Value Baseline vs. after LC | Control 1 Baseline | after Control 1 | p-Value Baseline vs. Control 1 | Control 2 Baseline | after Control 2 | p-Value Baseline vs. Control 2 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| BHB (mmol/L) | 0.06 ± 0.05 | 0.05 ± 0.07 | ns | 0.04 ± 0.02 | 0.42 ± 0.27 | <0.0001 | 0.09 ± 0.1 | 0.05 ± 0.02 | ns | 0.07 ± 0.07 | 0.05 ± 0.02 | ns |
| Total cholesterol (mg/dL) | 189 ± 34 | 158 ± 27 | 0.02 | 187 ± 35 | 203 ± 60 | ns | 163 ± 26 | 154 ± 35 | ns | 159 ± 41 | 187 ± 43 | ns |
| LDL-C (mg/dL) | 98 ± 34 | 78 ± 23 | 0.02 | 94 ± 28 | 105 ± 51 | ns | 87 ± 27 | 77 ± 30 | ns | 85 ± 37 | 110 ± 41 | ns |
| HDL-C (mg/dL) | 77 ± 9 | 58 ± 9 | <0.0001 | 77 ± 11 | 82 ± 16 | ns | 59 ± 11 | 56 ± 11 | ns | 58 ± 17 | 59 ± 11 | ns |
| TG (mg/dL) | 76 ± 38 | 104 ± 44 | 0.005 | 81 ± 26 | 80 ± 24 | ns | 86 ± 45 | 104 ± 45 | ns | 83 ± 31 | 96 ± 33 | ns |
| CRP mg/dL) | 1.3 ± 1.4 | 0.9 ± 0.4 | ns | 0.9 ± 0.8 | 0.8 ± 0.4 | ns | 1.4 ± 1.0 | 1.1 ± 0.7 | ns | 2.0 ± 1.7 | 1.9 ± 2.3 | ns |
| IL-6 (mg/dL) | 1.6 ± 0.2 | 1.7 ± 0.9 | ns | 1.7 ± 0.4 | 1.6 ± 0.2 | ns | 1.8 ± 0.4 | 1.9 ± 0.4 | ns | 1.9 ± 0.7 | 1.5 ± 0.1 | ns |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wachsmuth, N.B.; Aberer, F.; Haupt, S.; Schierbauer, J.R.; Zimmer, R.T.; Eckstein, M.L.; Zunner, B.; Schmidt, W.; Niedrist, T.; Sourij, H.; et al. The Impact of a High-Carbohydrate/Low Fat vs. Low-Carbohydrate Diet on Performance and Body Composition in Physically Active Adults: A Cross-Over Controlled Trial. Nutrients 2022, 14, 423. https://doi.org/10.3390/nu14030423
Wachsmuth NB, Aberer F, Haupt S, Schierbauer JR, Zimmer RT, Eckstein ML, Zunner B, Schmidt W, Niedrist T, Sourij H, et al. The Impact of a High-Carbohydrate/Low Fat vs. Low-Carbohydrate Diet on Performance and Body Composition in Physically Active Adults: A Cross-Over Controlled Trial. Nutrients. 2022; 14(3):423. https://doi.org/10.3390/nu14030423
Chicago/Turabian StyleWachsmuth, Nadine B., Felix Aberer, Sandra Haupt, Janis R. Schierbauer, Rebecca T. Zimmer, Max L. Eckstein, Beate Zunner, Walter Schmidt, Tobias Niedrist, Harald Sourij, and et al. 2022. "The Impact of a High-Carbohydrate/Low Fat vs. Low-Carbohydrate Diet on Performance and Body Composition in Physically Active Adults: A Cross-Over Controlled Trial" Nutrients 14, no. 3: 423. https://doi.org/10.3390/nu14030423
APA StyleWachsmuth, N. B., Aberer, F., Haupt, S., Schierbauer, J. R., Zimmer, R. T., Eckstein, M. L., Zunner, B., Schmidt, W., Niedrist, T., Sourij, H., & Moser, O. (2022). The Impact of a High-Carbohydrate/Low Fat vs. Low-Carbohydrate Diet on Performance and Body Composition in Physically Active Adults: A Cross-Over Controlled Trial. Nutrients, 14(3), 423. https://doi.org/10.3390/nu14030423