
The Impact of Dietary Flavonols on Central Obesity Parameters in Polish Adults


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Group
2.2. Methods
2.2.1. Flavonol Intake Assessment
2.2.2. Anthropometrical and Body Composition Measurements
2.2.3. Statistical Analysis
2.2.4. Ethics
3. Results
3.1. General Characteristics of the Study Population
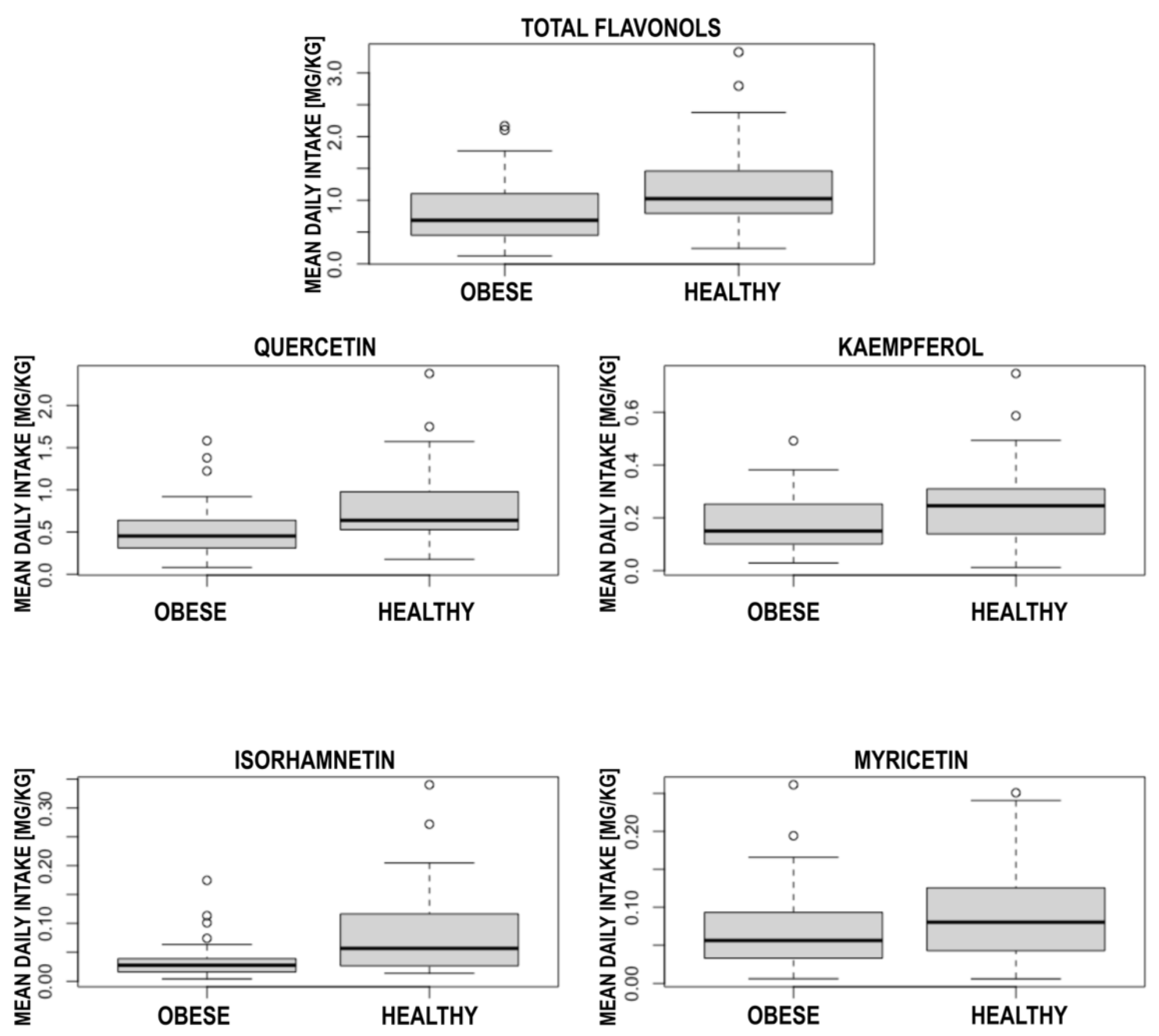
3.2. Central Obesity and Healthy Participants Comparison
3.3. Body Composition in Central Obese Participants
3.4. Anthropometrical Parameters in Central Obese Participants
3.5. Flavonols’ Sources in Central Obese Participants
4. Discussion
Limitations of the Study
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. The Top 10 Causes of Death—Factsheet. Available online: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death (accessed on 14 October 2022).
- Wormser, D.; Kaptoge, S.; Di Angelantonio, E.; Wood, A.M.; Pennells, L.; Thompson, A.; Sarwar, N.; Kizer, J.R.; Lawlor, D.A.; Nordestgaard, B.G.; et al. Separate and combined associations of body-mass index and abdominal adiposity with cardiovascular disease: Collaborative analysis of 58 prospective studies. Lancet 2011, 377, 1085–1095. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.-Q.; Burgess, S.; Staley, J.R.; Wood, A.M.; Bell, S.; Kaptoge, S.K.; Guo, Q.; Bolton, T.R.; Mason, A.M.; Butterworth, A.S.; et al. Body mass index and all cause mortality in HUNT and UK Biobank studies: Linear and non-linear mendelian randomisation analyses. BMJ 2019, 364, l1042. [Google Scholar] [CrossRef] [PubMed]
- Bentham, J.; Di Cesare, M.; Bilano, V.; Bixby, H.; Zhou, B.; Stevens, G.A.; Riley, L.M.; Taddei, C.; Hajifathalian, K.; Lu, Y.; et al. Worldwide Trends in Body-Mass Index, Underweight, Overweight, and Obesity from 1975 to 2016: A Pooled Analysis of 2416 Population-Based Measurement Studies in 128.9 Million Children, Adolescents, and Adults. Lancet 2017, 390, 2627–2642. [Google Scholar] [CrossRef]
- Liu, B.; Du, Y.; Wu, Y.; Snetselaar, L.G.; Wallace, R.B.; Bao, W. Trends in obesity and adiposity measures by race or ethnicity among adults in the United States 2011-18: Population based study. BMJ 2021, 372, n365. [Google Scholar] [CrossRef]
- Visseren, F.L.J.; Mach, F.; Smulders, Y.M.; Carballo, D.; Koskinas, K.C.; Bäck, M.; Benetos, A.; Biffi, A.; Boavida, J.-M.; Capodanno, D.; et al. 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice: Developed by the Task Force for cardio-vascular disease prevention in clinical practice with representatives of the European Society of Cardiology and 12 medical societies with the special contribution of the European Association of Preventive Cardiology (EAPC). Eur. Heart J. 2021, 42, 3227–3337. [Google Scholar] [CrossRef]
- Garvey, W.T.; Mechanick, J.I.; Brett, E.M.; Garber, A.J.; Hurley, D.L.; Jastreboff, A.M.; Nadolsky, K.; Pessah-Pollack, R.; Plodkowski, R.; Reviewers of the AACE/ACE Obesity Clinical Practice Guidelines. American association of clinical endocrinologists and american college of endocrinology comprehensive clinical practice guidelines for medical care of patients with obesity. Endocr. Pract. 2016, 22, 1–203. [Google Scholar] [CrossRef] [PubMed]
- Romero-Corral, A.; Somers, V.K.; Sierra-Johnson, J.; Thomas, R.; Collazo-Clavell, M.L.; Korinek, J.; Allison, T.G.; A Batsis, J.; Kuniyoshi, F.S.; Lopez-Jimenez, F. Accuracy of body mass index in diagnosing obesity in the adult general population. Int. J. Obes. 2008, 32, 959–966. [Google Scholar] [CrossRef] [PubMed]
- Yumuk, V.; Tsigos, C.; Fried, M.; Schindler, K.; Busetto, L.; Micic, D.; Toplak, H. European Guidelines for Obesity Management in Adults. Obes. Facts 2015, 8, 402–424. [Google Scholar] [CrossRef] [PubMed]
- Popiołek, J.; Teter, M.; Kozak, G.; Powrózek, T.; Mlak, R.; Karakuła-Juchnowicz, H.; Małecka-Massalska, T. Anthropometrical and Bioelectrical Impedance Analysis Parameters in Anorexia Nervosa Patients’ Nutritional Status Assessment. Medicina 2019, 55, 671. [Google Scholar] [CrossRef]
- Wannamethee, S.G.; Atkins, J.L. Muscle loss and obesity: The health implications of sarcopenia and sarcopenic obesity. Proc. Nutr. Soc. 2015, 74, 405–412. [Google Scholar] [CrossRef]
- Kawai, T.; Autieri, M.V.; Scalia, R. Adipose tissue inflammation and metabolic dysfunction in obesity. Am. J. Physiol. Cell Physiol. 2021, 320, C375–C391. [Google Scholar] [CrossRef]
- Jiang, N.; Li, Y.; Shu, T.; Wang, J. Cytokines and inflammation in adipogenesis: An updated review. Front. Med. 2019, 13, 314–329. [Google Scholar] [CrossRef] [PubMed]
- Coppack, S.W. Pro-inflammatory cytokines and adipose tissue. Proc. Nutr. Soc. 2001, 60, 349–356. [Google Scholar] [CrossRef] [PubMed]
- Okamoto, Y.; Higashiyama, H.; Rong, J.X.; McVey, M.J.; Kinoshita, M.; Asano, S.; Hansen, M.K. Comparison of mitochondrial and macrophage content between subcutaneous and visceral fat in db/db mice. Exp. Mol. Pathol. 2007, 83, 73–83. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Torres, I.; Castrejón-Téllez, V.; Soto, M.E.; Rubio-Ruiz, M.E.; Manzano-Pech, L.; Guarner-Lans, V. Oxidative Stress, Plant Natural Antioxidants, and Obesity. Int. J. Mol. Sci. 2021, 22, 1786. [Google Scholar] [CrossRef]
- Zamora-Ros, R.; Andres-Lacueva, C.; Lamuela-Raventós, R.M.; Berenguer, T.; Jakszyn, P.; Barricarte, A.; Ardanaz, E.; Amiano, P.; Dorronsoro, M.; Larrañaga, N.; et al. Estimation of Dietary Sources and Flavonoid Intake in a Spanish Adult Population (EPIC-Spain). J. Am. Diet. Assoc. 2010, 110, 390–398. [Google Scholar] [CrossRef]
- Sampson, L.; Rimm, E.; Hollman, P.C.; de Vries, J.H.; Katan, M.B. Flavonol and Flavone Intakes in US Health Professionals. J. Am. Diet. Assoc. 2002, 102, 1414–1420. [Google Scholar] [CrossRef]
- Zamora-Ros, R.; Knaze, V.; Luján-Barroso, L.; Slimani, N.; Romieu, I.; Fedirko, V.; de Magistris, M.S.; Ericson, U.; Amiano, P.; Trichopoulou, A.; et al. Estimated dietary intakes of flavonols, flavanones and flavones in the European Prospective Investigation into Cancer and Nutrition (EPIC) 24 hour dietary recall cohort. Br. J. Nutr. 2011, 106, 1915–1925. [Google Scholar] [CrossRef]
- Panche, A.N.; Diwan, A.D.; Chandra, S.R. Flavonoids: An overview. J. Nutr. Sci. 2016, 5, e47. [Google Scholar] [CrossRef]
- Sagar, N.A.; Pareek, S.; Benkeblia, N.; Xiao, J. Onion (Allium cepa L.) bioactives: Chemistry, pharmacotherapeutic functions, and industrial applications. Food Front. 2022, 3, 380–412. [Google Scholar] [CrossRef]
- Dwyer, J.T.; Peterson, J. Tea and flavonoids: Where we are, where to go next. Am. J. Clin. Nutr. 2013, 98, 1611S–1618S. [Google Scholar] [CrossRef] [PubMed]
- Awad, M.A.; de Jager, A.; van Westing, L.M. Flavonoid and chlorogenic acid levels in apple fruit: Characterisation of variation. Sci. Hortic. 2000, 83, 249–263. [Google Scholar] [CrossRef]
- Olsen, H.; Aaby, K.; Borge, G.I.A. Characterization and Quantification of Flavonoids and Hydroxycinnamic Acids in Curly Kale (Brassica oleracea L. Convar. acephala Var. sabellica) by HPLC-DAD-ESI-MSn. J. Agric. Food Chem. 2009, 57, 2816–2825. [Google Scholar] [CrossRef] [PubMed]
- Zivcak, M.; Brückova, K.; Sytar, O.; Brestic, M.; Olsovska, K.; Allakhverdiev, S.I. Lettuce flavonoids screening and phenotyping by chlorophyll fluorescence excitation ratio. Planta 2017, 245, 1215–1229. [Google Scholar] [CrossRef] [PubMed]
- Slimestad, R.; Fossen, T.; Verheul, M.J. The Flavonoids of Tomatoes. J. Agric. Food Chem. 2008, 56, 2436–2441. [Google Scholar] [CrossRef]
- Wu, X.; Zhao, Y.; Haytowitz, D.B.; Chen, P.; Pehrsson, P.R. Effects of domestic cooking on flavonoids in broccoli and calculation of retention factors. Heliyon 2019, 5, e01310. [Google Scholar] [CrossRef] [PubMed]
- Giuffrè, A.M. HPLC-DAD detection of changes in phenol content of red berry skins during grape ripening. Eur. Food Res. Technol. 2013, 237, 555–564. [Google Scholar] [CrossRef]
- Zhu, L.; Zhang, Y.; Lu, J. Phenolic Contents and Compositions in Skins of Red Wine Grape Cultivars among Various Genetic Backgrounds and Originations. Int. J. Mol. Sci. 2012, 13, 3492–3510. [Google Scholar] [CrossRef]
- Maria, G.A.; Riccardo, N. Citrus bergamia, Risso: The peel, the juice and the seed oil of the bergamot fruit of Reggio Calabria (South Italy). Emir. J. Food Agric. 2020, 32, 522–523. [Google Scholar] [CrossRef]
- Costanzo, G.; Vitale, E.; Iesce, M.R.; Naviglio, D.; Amoresano, A.; Fontanarosa, C.; Spinelli, M.; Ciaravolo, M.; Arena, C. Antioxidant Properties of Pulp, Peel and Seeds of Phlegrean Mandarin (Citrus reticulata Blanco) at Different Stages of Fruit Ripening. Antioxidants 2022, 11, 187. [Google Scholar] [CrossRef]
- Häkkinen, S.H.; Kärenlampi, S.O.; Heinonen, I.M.; Mykkänen, H.M.; Törrönen, A.R. Content of the Flavonols Quercetin, Myricetin, and Kaempferol in 25 Edible Berries. J. Agric. Food Chem. 1999, 47, 2274–2279. [Google Scholar] [CrossRef] [PubMed]
- Cassidy, A.; O’Reilly, É.J.; Kay, C.; Sampson, L.; Franz, M.; Forman, J.P.; Curhan, G.; Rimm, E.B. Habitual intake of flavonoid subclasses and incident hypertension in adults. Am. J. Clin. Nutr. 2011, 93, 338–347. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.-A.; Kim, J.; Jun, S.; Wie, G.-A.; Shin, S.; Joung, H. Association between dietary flavonoid intake and obesity among adults in Korea. Appl. Physiol. Nutr. Metab. 2020, 45, 203–212. [Google Scholar] [CrossRef] [PubMed]
- Nishimura, M.; Muro, T.; Kobori, M.; Nishihira, J. Effect of Daily Ingestion of Quercetin-Rich Onion Powder for 12 Weeks on Visceral Fat: A Randomised, Double-Blind, Placebo-Controlled, Parallel-Group Study. Nutrients 2020, 12, 91. [Google Scholar] [CrossRef] [PubMed]
- Popiolek-Kalisz, J.; Fornal, E. Dietary Isorhamnetin Intake Is Inversely Associated with Coronary Artery Disease Occurrence in Polish Adults. Int. J. Environ. Res. Public Health 2022, 19, 12546. [Google Scholar] [CrossRef]
- Bhagwat, S.; Haytowitz, D.B.; Holden, J.M. USDA Database for the Flavonoid Content of Selected Foods Release 3; U.S. Department of Agriculture: Beltsville, MD, USA, 2011. Available online: https://www.ars.usda.gov/arsuserfiles/80400525/data/flav/flav_r03.pdf (accessed on 14 October 2022).
- Després, J.-P.; Lemieux, I. Abdominal obesity and metabolic syndrome. Nature 2006, 444, 881–887. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Obesity: Preventing and Managing the Global Epidemic. Report of a WHO Consultation; WHO Technical Report Series 894; World Health Organization: Geneva, Switzerland, 2000. [Google Scholar]
- Cederholm, T.; Barazzoni, R.; Austin, P.; Ballmer, P.; Biolo, G.; Bischoff, S.C.; Compher, C.; Correia, I.; Higashiguchi, T.; Holst, M.; et al. ESPEN guidelines on definitions and terminology of clinical nutrition. Clin. Nutr. 2017, 36, 49–64. [Google Scholar] [CrossRef]
- Stepaniak, U.; Micek, A.; Waśkiewicz, A.; Bielecki, W.; Drygas, W.; Janion, M.; Kozakiewicz, K.; Niklas, A.; Puch-Walczak, A.; Pająk, A. Prevalence of general and abdominal obesity and overweight among adults in Poland. Results of the WOBASZ II study (2013–2014) and comparison with the WOBASZ study (2003–2005). Pol. Arch. Med. Wewn. 2016, 126, 662–671. [Google Scholar] [CrossRef]
- Zhang, C.; Rexrode, K.; van Dam, R.; Li, T.Y.; Hu, F.B. Abdominal Obesity and the Risk of All-Cause, Cardiovascular, and Cancer Mortality: Sixteen Years of Follow-up in US Women. Circulation 2008, 117, 1658–1667. [Google Scholar] [CrossRef]
- Furukawa, S.; Fujita, T.; Shimabukuro, M.; Iwaki, M.; Yamada, Y.; Nakajima, Y.; Nakayama, O.; Makishima, M.; Matsuda, M.; Shimomura, I. Increased oxidative stress in obesity and its impact on metabolic syndrome. J. Clin. Investig. 2004, 114, 1752–1761. [Google Scholar] [CrossRef]
- Keaney, J.F.; Larson, M.; Vasan, R.S.; Wilson, P.W.; Lipinska, I.; Corey, D.; Massaro, J.; Sutherland, P.; Vita, J.; Benjamin, E. Obesity and Systemic Oxidative Stress: Clinical Correlates of Oxidative Stress in the Framingham Study. Arter. Thromb. Vasc. Biol. 2003, 23, 434–439. [Google Scholar] [CrossRef]
- Popiolek-Kalisz, J.; Fornal, E. The Effects of Quercetin Supplementation on Blood Pressure—Meta-Analysis. Curr. Probl. Cardiol. 2022, 47, 101350. [Google Scholar] [CrossRef] [PubMed]
- Popiolek-Kalisz, J.; Fornal, E. The Impact of Flavonols on Cardiovascular Risk. Nutrients 2022, 14, 1973. [Google Scholar] [CrossRef] [PubMed]
- Popiolek-Kalisz, J.; Blaszczak, P.; Fornal, E. Dietary Isorhamnetin Intake Is Associated with Lower Blood Pressure in Coronary Artery Disease Patients. Nutrients 2022, 14, 4586. [Google Scholar] [CrossRef]
- Sharma, A.; Sharma, P.; Singh Tuli, H.; Sharma, A.K. Phytochemical and Pharmacological Properties of Flavonols. In eLS; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2018. [Google Scholar]
- Kuti, J.O.; Konuru, H.B. Antioxidant Capacity and Phenolic Content in Leaf Extracts of Tree Spinach (Cnidoscolus spp.). J. Agric. Food Chem. 2004, 52, 117–121. [Google Scholar] [CrossRef] [PubMed]
- Häkkinen, S.H.; Kärenlampi, S.O.; Mykkänen, H.M.; Törrönen, A.R. Influence of Domestic Processing and Storage on Flavonol Contents in Berries. J. Agric. Food Chem. 2000, 48, 2960–2965. [Google Scholar] [CrossRef]
- Rodriguez-Mateos, A.; Cifuentes-Gomez, T.; George, T.W.; Spencer, J.P.E. Impact of Cooking, Proving, and Baking on the (Poly)phenol Content of Wild Blueberry. J. Agric. Food Chem. 2014, 62, 3979–3986. [Google Scholar] [CrossRef] [PubMed]
- Huber, K.; Brigide, P.; Bretas, E.B.; Canniatti-Brazaca, S.G. Effect of Thermal Processing and Maceration on the Antioxidant Activity of White Beans. PLoS ONE 2014, 9, e99325. [Google Scholar] [CrossRef]
- Del Pino-García, R.; González-SanJosé, M.L.; Rivero-Pérez, M.D.; García-Lomillo, J.; Muñiz, P. The effects of heat treatment on the phenolic composition and antioxidant capacity of red wine pomace seasonings. Food Chem. 2017, 221, 1723–1732. [Google Scholar] [CrossRef]
- García-Macías, P.; Ordidge, M.; Vysini, E.; Waroonphan, S.; Battey, N.H.; Gordon, M.H.; Hadley, P.; John, P.; Lovegrove, J.A.; Wagstaffe, A. Changes in the Flavonoid and Phenolic Acid Contents and Antioxidant Activity of Red Leaf Lettuce (Lollo Rosso) Due to Cultivation under Plastic Films Varying in Ultraviolet Transparency. J. Agric. Food Chem. 2007, 55, 10168–10172. [Google Scholar] [CrossRef]
- Ma, X.; Laaksonen, O.; Zheng, J.; Yang, W.; Trépanier, M.; Kallio, H.; Yang, B. Flavonol glycosides in berries of two major subspecies of sea buckthorn (Hippophaë rhamnoides L.) and influence of growth sites. Food Chem. 2016, 200, 189–198. [Google Scholar] [CrossRef] [PubMed]
- Liaudanskas, M.; Okulevičiūtė, R.; Lanauskas, J.; Kviklys, D.; Zymonė, K.; Rendyuk, T.; Žvikas, V.; Uselis, N.; Janulis, V. Variability in the Content of Phenolic Compounds in Plum Fruit. Plants 2020, 9, 1611. [Google Scholar] [CrossRef] [PubMed]
- Knab, A.M.; Shanely, R.A.; Jin, F.; Austin, M.D.; Sha, W.; Nieman, D.C. Quercetin with vitamin C and niacin does not affect body mass or composition. Appl. Physiol. Nutr. Metab. 2011, 36, 331–338. [Google Scholar] [CrossRef] [PubMed]
- Khorshidi, M.; Moini, A.; Alipoor, E.; Rezvan, N.; Gorgani-Firuzjaee, S.; Yaseri, M.; Hosseinzadeh-Attar, M.J. The effects of quercetin supplementation on metabolic and hormonal parameters as well as plasma concentration and gene expression of resistin in overweight or obese women with polycystic ovary syndrome. Phytother. Res. 2018, 32, 2282–2289. [Google Scholar] [CrossRef] [PubMed]
- Egert, S.; Bosy-Westphal, A.; Seiberl, J.; Kürbitz, C.; Settler, U.; Plachta-Danielzik, S.; Wagner, A.E.; Frank, J.; Schrezenmeir, J.; Rimbach, G.; et al. Quercetin reduces systolic blood pressure and plasma oxidised low-density lipoprotein concentrations in overweight subjects with a high-cardiovascular disease risk phenotype: A double-blinded, placebo-controlled cross-over study. Br. J. Nutr. 2009, 102, 1065–1074. [Google Scholar] [CrossRef]
- Egert, S.; Boesch-Saadatmandi, C.; Wolffram, S.; Rimbach, G.; Muller, M.J. Serum Lipid and Blood Pressure Responses to Quercetin Vary in Overweight Patients by Apolipoprotein E Genotype. J. Nutr. 2010, 140, 278–284. [Google Scholar] [CrossRef]
- Kaur, D.; Shri, R.; Kamboj, A. Bioactivity-directed isolation, characterization, and quantification of an anxiolytic flavonoid from Brassica oleracea L. J. Food Biochem. 2021, 45, e13608. [Google Scholar] [CrossRef]
- Wang, T.; Wu, Q.; Zhao, T. Preventive Effects of Kaempferol on High-Fat Diet-Induced Obesity Complications in C57BL/6 Mice. BioMed Res. Int. 2020, 2020, 4532482. [Google Scholar] [CrossRef]
- Bian, Y.; Lei, J.; Zhong, J.; Wang, B.; Wan, Y.; Li, J.; Liao, C.; He, Y.; Liu, Z.; Ito, K.; et al. Kaempferol reduces obesity, prevents intestinal inflammation, and modulates gut microbiota in high-fat diet mice. J. Nutr. Biochem. 2022, 99, 108840. [Google Scholar] [CrossRef]
- Somerset, S.M.; Johannot, L. Dietary Flavonoid Sources in Australian Adults. Nutr. Cancer 2008, 60, 442–449. [Google Scholar] [CrossRef]
- Rodríguez-Rodríguez, C.; Torres, N.; Gutiérrez-Uribe, J.A.; Noriega, L.G.; Torre-Villalvazo, I.; Leal-Díaz, A.M.; Antunes-Ricardo, M.; Márquez-Mota, C.; Ordaz, G.; Chavez-Santoscoy, R.A.; et al. The effect of isorhamnetin glycosides extracted from Opuntia ficus-indica in a mouse model of diet induced obesity. Food Funct. 2015, 6, 805–815. [Google Scholar] [CrossRef] [PubMed]
- Akindehin, S.; Jung, Y.-S.; Kim, S.-N.; Son, Y.-H.; Lee, I.; Seong, J.K.; Jeong, H.W.; Lee, Y.-H. Myricetin Exerts Anti-Obesity Effects through Upregulation of SIRT3 in Adipose Tissue. Nutrients 2018, 10, 1962. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Li, M.; Zhang, Y.; Chu, S.; Huo, Y.; Zhao, J.; Wan, C. Huangjinya Black Tea Alleviates Obesity and Insulin Resistance via Modulating Fecal Metabolome in High-Fat Diet-Fed Mice. Mol. Nutr. Food Res. 2020, 64, e2000353. [Google Scholar] [CrossRef] [PubMed]
- Ben Lagha, A.; Grenier, D. Black tea theaflavins attenuate Porphyromonas gingivalis virulence properties, modulate gingival keratinocyte tight junction integrity and exert anti-inflammatory activity. J. Periodontal Res. 2017, 52, 458–470. [Google Scholar] [CrossRef]
- Ramadan, G.; El-Beih, N.M.; Talaat, R.M.; El-Ghffar, E.A.A. Anti-inflammatory activity of green versus black tea aqueous extract in a rat model of human rheumatoid arthritis. Int. J. Rheum. Dis. 2017, 20, 203–213. [Google Scholar] [CrossRef]
- Liu, L.; Wu, X.; Zhang, B.; Yang, W.; Li, D.; Dong, Y.; Yin, Y.; Chen, Q. Protective effects of tea polyphenols on exhaustive exercise-induced fatigue, inflammation and tissue damage. Food Nutr. Res. 2017, 61, 1333390. [Google Scholar] [CrossRef]
- Pan, S.; Deng, X.; Sun, S.; Lai, X.; Sun, L.; Li, Q.; Xiang, L.; Zhang, L.; Huang, Y. Black tea affects obesity by reducing nutrient intake and activating AMP-activated protein kinase in mice. Mol. Biol. Rep. 2018, 45, 689–697. [Google Scholar] [CrossRef]
- Pan, M.-H.; Gao, Y.; Tu, Y. Mechanisms of Body Weight Reduction by Black Tea Polyphenols. Molecules 2016, 21, 1659. [Google Scholar] [CrossRef]
- Shishikura, Y.; Khokhar, A.S.; Murray, B.S. Effects of Tea Polyphenols on Emulsification of Olive Oil in a Small Intestine Model System. J. Agric. Food Chem. 2006, 54, 1906–1913. [Google Scholar] [CrossRef]
- Kudo, N.; Arai, Y.; Suhara, Y.; Ishii, T.; Nakayama, T.; Osakabe, N. A Single Oral Administration of Theaflavins Increases Energy Expenditure and the Expression of Metabolic Genes. PLoS ONE 2015, 10, e0137809. [Google Scholar] [CrossRef]
- Ohishi, T.; Fukutomi, R.; Shoji, Y.; Goto, S.; Isemura, M. The Beneficial Effects of Principal Polyphenols from Green Tea, Coffee, Wine, and Curry on Obesity. Molecules 2021, 26, 453. [Google Scholar] [CrossRef] [PubMed]
- Tang, G.-Y.; Meng, X.; Gan, R.-Y.; Zhao, C.-N.; Liu, Q.; Feng, Y.-B.; Li, S.; Wei, X.-L.; Atanasov, A.G.; Corke, H.; et al. Health Functions and Related Molecular Mechanisms of Tea Components: An Update Review. Int. J. Mol. Sci. 2019, 20, 6196. [Google Scholar] [CrossRef] [PubMed]
- Khan, N.; Mukhtar, H. Tea Polyphenols in Promotion of Human Health. Nutrients 2019, 11, 39. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, T.; Matsuo, Y. Production Mechanisms of Black Tea Polyphenols. Chem. Pharm. Bull. 2020, 68, 1131–1142. [Google Scholar] [CrossRef] [PubMed]
- Hibi, M.; Takase, H.; Iwasaki, M.; Osaki, N.; Katsuragi, Y. Efficacy of tea catechin-rich beverages to reduce abdominal adiposity and metabolic syndrome risks in obese and overweight subjects: A pooled analysis of 6 human trials. Nutr. Res. 2018, 55, 1–10. [Google Scholar] [CrossRef]
- Lee, A.; Lim, W.; Kim, S.; Khil, H.; Cheon, E.; An, S.; Hong, S.; Lee, D.H.; Kang, S.-S.; Oh, H.; et al. Coffee Intake and Obesity: A Meta-Analysis. Nutrients 2019, 11, 1274. [Google Scholar] [CrossRef]
- Higdon, J.V.; Frei, B. Coffee and Health: A Review of Recent Human Research. Crit. Rev. Food Sci. Nutr. 2006, 46, 101–123. [Google Scholar] [CrossRef]


{kind=link}
| Anthropometrical Parameter [Unit] | Mean Value | SD |
|---|---|---|
| Body mass [kg] | 80.18 | ±10.35 |
| BMI [kg/m2] | 29.18 | ±3.75 |
| Waist circumference [cm] | 102.72 | ±11.09 |
| TBW [kg] | 41.67 | ±6.00 |
| TBW% [%] | 52.26 | ±5.70 |
| ECF [kg] | 18.48 | ±2.95 |
| ECF% [%] | 44.39 | ±3.26 |
| ICF [kg] | 23.19 | ±3.71 |
| ICF% [%] | 55.63 | ±3.23 |
| FFM [kg] | 56.94 | ±8.17 |
| FFM% [%] | 71.36 | ±7.80 |
| FM [kg] | 23.12 | ±7.46 |
| FM% [%] | 28.61 | ±7.79 |
| Anthropometrical Parameter [Unit] | Central Obesity (n = 39) | SD | Healthy Control (n = 40) | SD | p |
|---|---|---|---|---|---|
| Body mass [kg] | 80.18 | ±10.35 | 59.48 | ±10.43 | <0.001 |
| BMI [kg/m2] | 29.18 | ±3.75 | 20.94 | ±1.65 | <0.001 |
| Waist circumference [cm] | 102.72 | ±11.09 | 65.6 | ±6.55 | <0.001 |
| Mean Daily Intake [mg/kg] | Central Obesity (n = 39) | SD | Healthy Control (n = 40) | SD | p |
|---|---|---|---|---|---|
| Total flavonols | 0.82 | ±0.44 | 1.18 | ±0.66 | 0.005 |
| Quercetin | 0.52 | ±0.29 | 0.77 | ±0.45 | 0.003 |
| Kaempferol | 0.19 | ±0.11 | 0.25 | ±0.15 | 0.04 |
| Isorhamnetin | 0.03 | ±0.02 | 0.08 | ±0.07 | <0.001 |
| Myricetin | 0.07 | ±0.05 | 0.09 | ±0.06 | 0.19 |
| Quercetin | |||
|---|---|---|---|
| R | 95% CI | p | |
| TBW | −0.127 | −0.425; 0.197 | 0.44 |
| TBW% | 0.225 | −0.097; 0.505 | 0.17 |
| ECF | −0.131 | −0.428; 0.193 | 0.43 |
| ECF% | −0.011 | −0.326; 0.305 | 0.95 |
| ICF | −0.099 | −0.402; 0.223 | 0.55 |
| ICF% | 0.004 | −0.312; 0.319 | 0.98 |
| FFM | −0.126 | −0.424; 0.198 | 0.45 |
| FFM% | 0.215 | −0.108; 0.497 | 0.19 |
| FM | −0.352 | −0.601; −0.041 | 0.03 |
| FM% | −0.225 | −0.505; 0.097 | 0.17 |
| BMI | −0.336 | −0.589; −0.023 | 0.04 |
| Waist circumference | −0.322 | −0.582; −0.002 | 0.05 |
| Kaempferol | |||
| R | 95% CI | p | |
| TBW | −0.062 | −0.371; 0.258 | 0.71 |
| TBW% | 0.330 | 0.016; 0.585 | 0.04 |
| ECF | −0.083 | −0.388; 0.239 | 0.62 |
| ECF% | −0.024 | −0.337; 0.294 | 0.89 |
| ICF | −0.034 | −0.345; 0.285 | 0.84 |
| ICF% | 0.021 | −0.297; 0.334 | 0.90 |
| FFM | −0.062 | −0.370; 0.259 | 0.71 |
| FFM% | 0.321 | 0.006; 0.578 | 0.05 |
| FM | −0.425 | −0.653; −0.127 | 0.01 |
| FM% | −0.330 | −0.585; −0.016 | 0.04 |
| BMI | −0.285 | −0.551; 0.03 | 0.08 |
| Waist circumference | −0.293 | −0.560; 0.03 | 0.07 |
| Isorhamnetin | |||
| R | 95% CI | p | |
| TBW | −0.034 | −0.345; 0.285 | 0.84 |
| TBW% | −0.029 | −0.342; 0.289 | 0.86 |
| ECF | 0.013 | −0.304; 0.327 | 0.94 |
| ECF% | 0.094 | −0.229; 0.397 | 0.57 |
| ICF | −0.064 | −0.372; 0.257 | 0.70 |
| ICF% | −0.102 | −0.405; 0.220 | 0.54 |
| FFM | −0.034 | −0.346; 0.284 | 0.84 |
| FFM% | −0.039 | −0.350; 0.280 | 0.81 |
| FM | 0.003 | −0.313; 0.318 | 0.99 |
| FM% | 0.029 | −0.289; 0.342 | 0.86 |
| BMI | −0.110 | −0.411; 0.213 | 0.51 |
| Waist circumference | −0.033 | −0.349; 0.290 | 0.84 |
| Myricetin | |||
| R | 95% CI | p | |
| TBW | −0.079 | −0.385; 0.243 | 0.63 |
| TBW% | 0.254 | −0.067; 0.527 | 0.12 |
| ECF | −0.079 | −0.385; 0.243 | 0.63 |
| ECF% | 0.011 | −0.305; 0.325 | 0.95 |
| ICF | −0.063 | −0.371; 0.258 | 0.70 |
| ICF% | −0.016 | −0.330; 0.301 | 0.92 |
| FFM | −0.078 | −0.384; 0.244 | 0.64 |
| FFM% | 0.246 | −0.076; 0.521 | 0.13 |
| FM | −0.352 | −0.601; −0.041 | 0.03 |
| FM% | −0.254 | −0.527; 0.067 | 0.12 |
| BMI | −0.279 | −0.546; 0.040 | 0.09 |
| Waist circumference | −0.367 | −0.615; −0.054 | 0.02 |
| Total flavonols | |||
| R | 95% CI | p | |
| TBW | −0.109 | −0.410; 0.214 | 0.51 |
| TBW% | 0.259 | −0.062; 0.531 | 0.11 |
| ECF | −0.114 | −0.415; 0.209 | 0.49 |
| ECF% | −0.007 | −0.322; 0.309 | 0.97 |
| ICF | −0.084 | −0.389; 0.238 | 0.61 |
| ICF% | 0.0003 | −0.315; 0.316 | 0.99 |
| FFM | −0.108 | −0.410; 0.215 | 0.51 |
| FFM% | 0.249 | −0.073; 0.523 | 0.13 |
| FM | −0.378 | −0.620; −0.071 | 0.02 |
| FM% | −0.259 | −0.531; 0.061 | 0.11 |
| BMI | −0.330 | −0.584; −0.016 | 0.04 |
| Waist circumference | −0.328 | −0.586; −0.009 | 0.04 |
| Fat Mass | |||
|---|---|---|---|
| Product | R | 95% CI | p |
| White onion | 0.178 | −0.146; 0.467 | 0.28 |
| Red onion | −0.074 | −0.381; 0.247 | 0.65 |
| Tomatoes | 0.283 | −0.036; 0.549 | 0.08 |
| Blueberry | 0.043 | −0.276; 0.354 | 0.79 |
| Apple | −0.088 | −0.393; 0.234 | 0.59 |
| Black tea | −0.511 | −0.712; −0.233 | <0.001 |
| Green tea | 0.007 | −0.310; 0.321 | 0.97 |
| Coffee | −0.003 | −0.318; 0.313 | 0.98 |
| Wine | −0.100 | −0.403; 0.223 | 0.55 |
| Fat mass % | |||
| Product | R | 95% CI | p |
| White onion | 0.145 | −0.178; 0.441 | 0.38 |
| Red onion | −0.120 | −0.419; 0.204 | 0.47 |
| Tomatoes | 0.166 | −0.158; 0.457 | 0.31 |
| Blueberry | 0.235 | −0.087; 0.512 | 0.15 |
| Apple | 0.012 | −0.305; 0.326 | 0.94 |
| Black tea | −0.522 | −0.719; −0.247 | <0.001 |
| Green tea | 0.057 | −0.263; 0.366 | 0.73 |
| Coffee | 0.183 | −0.141; 0.471 | 0.26 |
| Wine | −0.092 | −0.396; 0.230 | 0.58 |
| Waist circumference | |||
| Product | R | 95% CI | p |
| White onion | 0.169 | −0.159; 0.464 | 0.31 |
| Red onion | 0.031 | −0.291; 0.347 | 0.86 |
| Tomatoes | 0.370 | 0.057; 0.617 | 0.02 |
| Blueberry | −0.277 | −0.548; 0.047 | 0.09 |
| Apple | −0.018 | −0.336; 0.303 | 0.91 |
| Black tea | −0.201 | −0.489; 0.127 | 0.23 |
| Green tea | −0.141 | −0.441; 0.187 | 0.40 |
| Coffee | −0.352 | −0.604; −0.036 | 0.03 |
| Wine | −0.025 | −0.342; 0.297 | 0.88 |
| BMI | |||
| Product | R | 95% CI | p |
| White onion | −0.069 | −0.377; 0.252 | 0.67 |
| Red onion | −0.050 | −0.360; 0.270 | 0.76 |
| Tomatoes | 0.283 | −0.035; 0.550 | 0.08 |
| Blueberry | −0.062 | −0.370; 0.259 | 0.71 |
| Apple | −0.052 | −0.361; 0.268 | 0.76 |
| Black tea | −0.311 | −0.570; 0.005 | 0.05 |
| Green tea | −0.010 | −0.325 0.306 | 0.95 |
| Coffee | −0.137 | −0.434; 0.187 | 0.41 |
| Wine | 0.045 | −0.275; 0.355 | 0.79 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Popiolek-Kalisz, J. The Impact of Dietary Flavonols on Central Obesity Parameters in Polish Adults. Nutrients 2022, 14, 5051. https://doi.org/10.3390/nu14235051
Popiolek-Kalisz J. The Impact of Dietary Flavonols on Central Obesity Parameters in Polish Adults. Nutrients. 2022; 14(23):5051. https://doi.org/10.3390/nu14235051
Chicago/Turabian StylePopiolek-Kalisz, Joanna. 2022. "The Impact of Dietary Flavonols on Central Obesity Parameters in Polish Adults" Nutrients 14, no. 23: 5051. https://doi.org/10.3390/nu14235051
APA StylePopiolek-Kalisz, J. (2022). The Impact of Dietary Flavonols on Central Obesity Parameters in Polish Adults. Nutrients, 14(23), 5051. https://doi.org/10.3390/nu14235051