
A Smartphone Healthcare Application, CALO mama Plus, to Promote Weight Loss: A Randomized Controlled Trial

 ,
,  , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
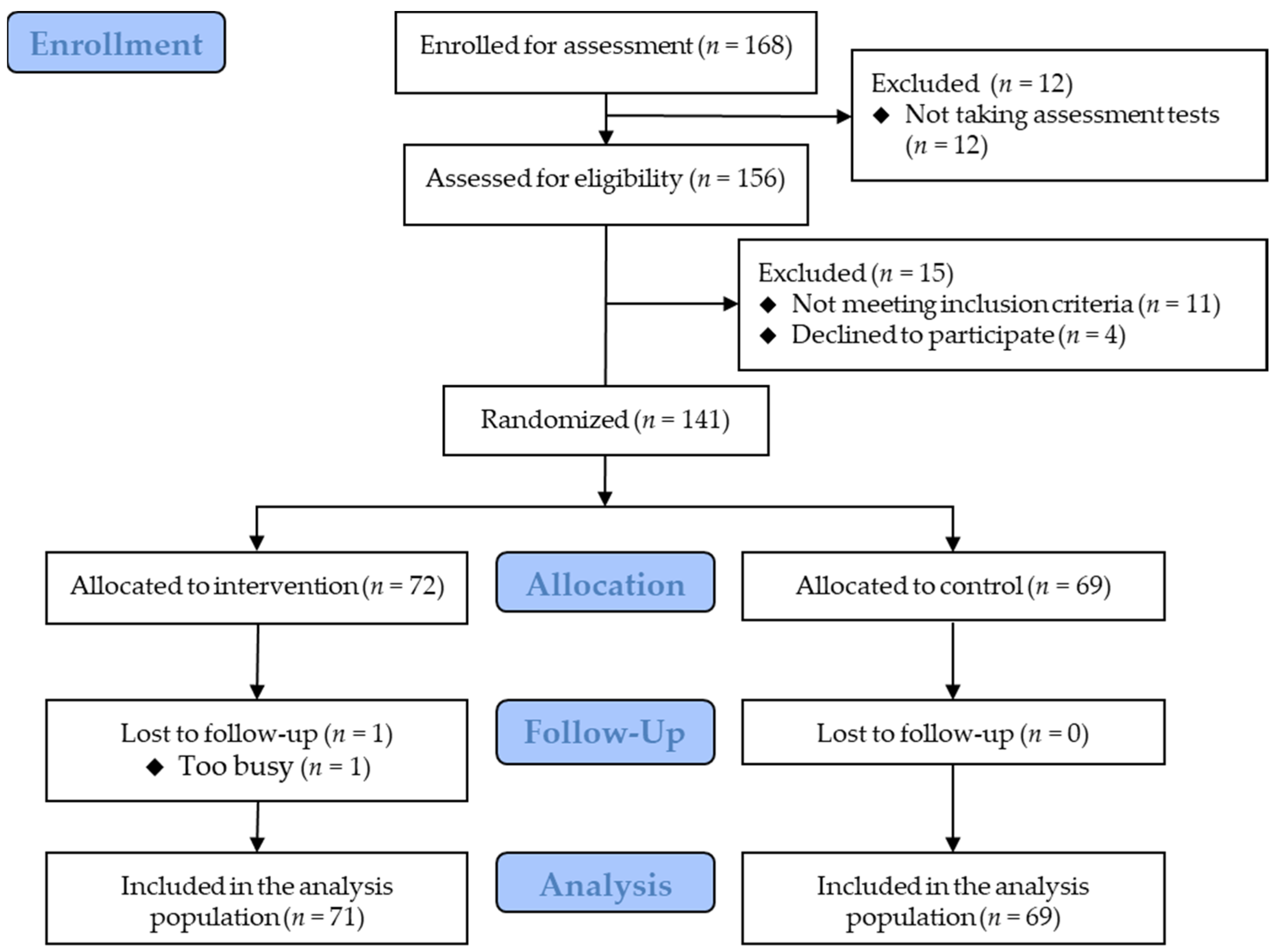
2.1. Study Design
2.2. Participants
2.3. Randomization
2.4. Interventions
2.4.1. Setting
2.4.2. Conversion of Users’ Input Data
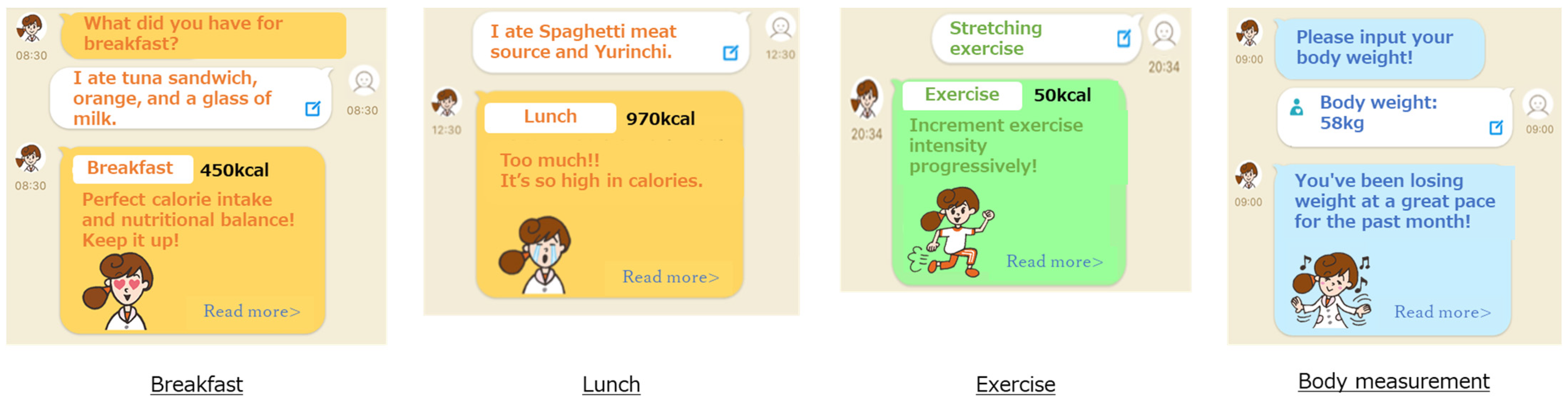
2.4.3. Feedback to Users
2.5. Measurements
2.5.1. Basic Characteristics
2.5.2. Body Weight
2.5.3. Blood Biochemistry Measures
2.5.4. Dietary Intake
2.5.5. Physical Activity
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Veronese, N.; Li, Y.; Manson, J.E.; Willett, W.C.; Fontana, L.; Hu, F.B. Combined associations of body weight and lifestyle factors with all cause and cause specific mortality in men and women: Prospective cohort study. BMJ 2016, 355, i5855. [Google Scholar] [CrossRef] [PubMed]
- WHO. Obesity and Overweight. 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 7 October 2022).
- Jensen, M.D.; Ryan, D.H.; Apovian, C.M.; Ard, J.D.; Comuzzie, A.G.; Donato, K.A.; Hu, F.B.; Hubbard, V.S.; Jakicic, J.M.; Kushner, R.F.; et al. 2013 AHA/ACC/TOS guideline for the management of overweight and obesity in adults. Circulation 2014, 129 (Suppl. 2), S102–S138. [Google Scholar] [CrossRef] [PubMed]
- Diabetes Prevention Program Research Group. The Diabetes Prevention Program (DPP): Description of lifestyle intervention. Diabetes Care 2002, 25, 2165–2171. [Google Scholar] [CrossRef] [PubMed]
- Mosa, A.S.; Yoo, I.; Sheets, L. A systematic review of healthcare applications for smartphones. BMC Med. Inf. Decis. Mak. 2012, 12, 67. [Google Scholar] [CrossRef]
- Schoeppe, S.; Alley, S.; Van Lippevelde, W.; Bray, N.A.; Williams, S.L.; Duncan, M.J.; Vandelanotte, C. Efficacy of interventions that use apps to improve diet, physical activity and sedentary behaviour: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 127. [Google Scholar] [CrossRef]
- Stephens, J.; Allen, J. Mobile phone interventions to increase physical activity and reduce weight: A systematic review. J. Cardiovasc. Nurs. 2013, 28, 320–329. [Google Scholar] [CrossRef]
- Chen, Y.; Perez-Cueto, F.J.A.; Giboreau, A.; Mavridis, I.; Hartwell, H. The promotion of eating behaviour change through digital interventions. Int. J. Environ. Res. Public Health 2020, 17, 7488. [Google Scholar] [CrossRef]
- Lee, D.; Yoon, S.N. Application of artificial intelligence-based technologies in the healthcare industry: Opportunities and challenges. Int. J. Environ. Res. Public Health 2021, 18, 271. [Google Scholar] [CrossRef]
- Yu, K.H.; Beam, A.L.; Kohane, I.S. Artificial intelligence in healthcare. Nat. Biomed. Eng. 2018, 2, 719–731. [Google Scholar] [CrossRef]
- Sasaki, Y.; Sato, K.; Kobayashi, S.; Asakura, K. Nutrient and food group prediction as orchestrated by an automated image recognition system in a smartphone app (CALO mama): Validation study. JMIR Res. 2022, 6, e31875. [Google Scholar] [CrossRef]
- Tanaka, K.; Sasai, H.; Wakaba, K.; Murakami, S.; Ueda, M.; Yamagata, F.; Sawada, M.; Takekoshi, K. Professional dietary coaching within a group chat using a smartphone application for weight loss: A randomized controlled trial. J. Multidiscip. Healthc. 2018, 11, 339–347. [Google Scholar] [CrossRef] [PubMed]
- Alencar, M.K.; Johnson, K.; Mullur, R.; Gray, V.; Gutierrez, E.; Korosteleva, O. The efficacy of a telemedicine-based weight loss program with video conference health coaching support. J. Telemed. Telecare 2019, 25, 151–157. [Google Scholar] [CrossRef] [PubMed]
- Beleigoli, A.M.; Andrade, A.Q.; Cancado, A.G.; Paulo, M.N.; Diniz, M.F.H.; Ribeiro, A.L. Web-based digital health interventions for weight loss and lifestyle habit changes in overweight and obese adults: Systematic review and meta-analysis. J. Med. Internet Res. 2019, 21, e298. [Google Scholar] [CrossRef] [PubMed]
- Sato, K.; Kobayashi, S.; Yamaguchi, M.; Sakata, R.; Sasaki, Y.; Murayama, C.; Kondo, N. Working from home and dietary changes during the COVID-19 pandemic: A longitudinal study of health app (CALO mama) users. Appetite 2021, 165, 105323. [Google Scholar] [CrossRef] [PubMed]
- Schulz, K.F.; Altman, D.G.; Moher, D.; Group, C. CONSORT 2010 statement: Updated guidelines for reporting parallel group randomised trials. BMJ 2010, 340, c332. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health, Labor and Welfare. The Dietary Reference Intakes for Japanese, 2020. 2019. Available online: https://www.mhlw.go.jp/stf/shingi/other-kenkou_539644.html (accessed on 7 October 2022).
- Shinya, S.; Masaru, A.; Akira, H.; Eisaku, H.; Susumu, O. Development of an assay of seven biochemical items, HbA1c, and hematocrit using a small amount of blood collected from the fingertip. Clin. Chim. Acta 2012, 413, 192–197. [Google Scholar] [CrossRef]
- Kobayashi, S.; Honda, S.; Murakami, K.; Sasaki, S.; Okubo, H.; Hirota, N.; Notsu, A.; Fukui, M.; Date, C. Both comprehensive and brief self-administered diet history questionnaires satisfactorily rank nutrient intakes in Japanese adults. J. Epidemiol. 2012, 22, 151–159. [Google Scholar] [CrossRef]
- Kobayashi, S.; Murakami, K.; Sasaki, S.; Okubo, H.; Hirota, N.; Notsu, A.; Fukui, M.; Date, C. Comparison of relative validity of food group intakes estimated by comprehensive and brief-type self-administered diet history questionnaires against 16 d dietary records in Japanese adults. Public Health Nutr. 2011, 14, 1200–1211. [Google Scholar] [CrossRef]
- Ohkawara, K.; Oshima, Y.; Hikihara, Y.; Ishikawa-Takata, K.; Tabata, I.; Tanaka, S. Real-time estimation of daily physical activity intensity by a triaxial accelerometer and a gravity-removal classification algorithm. Br. J. Nutr. 2011, 105, 1681–1691. [Google Scholar] [CrossRef]
- Oshima, Y.; Kawaguchi, K.; Tanaka, S.; Ohkawara, K.; Hikihara, Y.; Ishikawa-Takata, K.; Tabata, I. Classifying household and locomotive activities using a triaxial accelerometer. Gait Posture 2010, 31, 370–374. [Google Scholar] [CrossRef]
- Masse, L.C.; Fuemmeler, B.F.; Anderson, C.B.; Matthews, C.E.; Trost, S.G.; Catellier, D.J.; Treuth, M. Accelerometer data reduction: A comparison of four reduction algorithms on select outcome variables. Med. Sci. Sport. Exerc. 2005, 37 (Suppl. 11), S544–S554. [Google Scholar] [CrossRef] [PubMed]
- Troiano, R.P.; Berrigan, D.; Dodd, K.W.; Masse, L.C.; Tilert, T.; McDowell, M. Physical activity in the United States measured by accelerometer. Med. Sci. Sport. Exerc. 2008, 40, 181–188. [Google Scholar] [CrossRef] [PubMed]
- Tsushita, K.; Hosler, A.S.; Miura, K.; Ito, Y.; Fukuda, T.; Kitamura, A.; Tatara, K. Rationale and descriptive analysis of specific health guidance: The nationwide lifestyle intervention program targeting metabolic syndrome in Japan. J. Atheroscler. Thromb. 2018, 25, 308–322. [Google Scholar] [CrossRef] [PubMed]
- Muramoto, A.; Matsushita, M.; Kato, A.; Yamamoto, N.; Koike, G.; Nakamura, M.; Numata, T.; Tamakoshi, A.; Tsushita, K. Three percent weight reduction is the minimum requirement to improve health hazards in obese and overweight people in Japan. Obes. Res. Clin. Pract. 2014, 8, e466–e475. [Google Scholar] [CrossRef]
- Okubo, H.; Sasaki, S.; Rafamantanantsoa, H.H.; Ishikawa-Takata, K.; Okazaki, H.; Tabata, I. Validation of self-reported energy intake by a self-administered diet history questionnaire using the doubly labeled water method in 140 Japanese adults. Eur. J. Clin. Nutr. 2008, 62, 1343–1350. [Google Scholar] [CrossRef]
- Goethals, L.; Barth, N.; Guyot, J.; Hupin, D.; Celarier, T.; Bongue, B. Impact of home quarantine on physical activity among older adults living at home during the COVID-19 pandemic: Qualitative interview study. JMIR Aging 2020, 3, e19007. [Google Scholar] [CrossRef]
- Mattioli, A.V.; Puviani, M.B.; Nasi, M.; Farinetti, A. COVID-19 pandemic: The effects of quarantine on cardiovascular risk. Eur. J. Clin. Nutr. 2020, 74, 852–855. [Google Scholar] [CrossRef]
- Tison, G.H.; Avram, R.; Kuhar, P.; Abreau, S.; Marcus, G.M.; Pletcher, M.J.; Olgin, J.E. Worldwide effect of COVID-19 on physical activity: A descriptive study. Ann. Intern. Med. 2020, 173, 767–770. [Google Scholar] [CrossRef]
- Examination Committee of Criteria for ‘Obesity Disease’ in Japan; Japan Society for the Study of Obesity. New criteria for ‘obesity disease’ in Japan. Circ. J. 2002, 66, 987–992. [Google Scholar] [CrossRef]
- Ministry of Health, Labor and Welfare. The National Health and Nutrition Survey (NHNS) Japan, 2019. 2019. Available online: https://www.nibiohn.go.jp/eiken/kenkounippon21/download_files/eiyouchousa/2019.pdf (accessed on 7 October 2022).
- NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: A pooled analysis of 2416 population-based measurement studies in 128·9 million children, adolescents, and adults. Lancet 2017, 390, 2627–2642. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence. Obesity in Adults: Prevention and Lifestyle Weight Management Programmes. 2016. Available online: https://www.nice.org.uk/guidance/qs111 (accessed on 7 October 2022).



{kind=link}
{kind=link}
| Intervention (n = 72) | Control (n = 69) | |
|---|---|---|
| Age, years | 42.3 ± 9.4 | 44.0 ± 9.1 |
| Sex (men), n (%) | 53 (74) | 51 (74) |
| Height, cm | 167.6 ± 7.5 | 168.6 ± 8.4 |
| Body mass index, kg/m2 | 27.3 ± 3.3 | 27.8 ± 3.7 |
| Waist circumference, cm | 90.7 ± 8.7 | 92.2 ± 8.6 |
| Systolic blood pressure, mm Hg | 120.3 ± 12.5 | 126.6 ± 13.9 |
| Diastolic blood pressure, mm Hg | 77.2 ± 9.5 | 80.4 ± 11.6 |
| Medical history, n (%) | ||
| Any | 27 (38) | 28 (41) |
| Fatty liver | 10 (14) | 15 (22) |
| Hypertension | 10 (14) | 13 (19) |
| Dyslipidemia | 17 (24) | 21 (30) |
| Diabetes | 3 (4) | 4 (6) |
| Gout | 7 (10) | 7 (10) |
| Medication use, n (%) | ||
| Any | 20 (28) | 8 (12) |
| Antihypertensive | 6 (8) | 3 (4) |
| Lipid-lowering | 7 (10) | 4 (6) |
| Hypoglycemic | 2 (3) | 2 (3) |
| Antigout | 4 (6) | 1 (1) |
| Family medical history, n (%) | ||
| Stroke | 17 (24) | 16 (23) |
| Heart disease | 15 (21) | 8 (12) |
| Hypertension | 36 (50) | 33 (48) |
| Dyslipidemia | 22 (31) | 15 (22) |
| Diabetes | 24 (33) | 20 (29) |
| Weight control history | ||
| Lifetime maximum weight, kg | 79.7 ± 10.2 | 82.8 ± 12.9 |
| Age at maximum weight, years | 39.2 ± 10.5 | 38.7 ± 10.2 |
| Weight at the age of 20 years, kg | 63.6 ± 8.8 | 65.1 ± 11.7 |
| ≥3 kg of weight loss in the past, n (%) | 37 (51) | 44 (64) |
| Current smoking, n (%) | 7 (10) | 10 (14) |
| Current exercise habit, n (%) | 22 (31) | 21 (30) |
| Premenopausal women, n (% of women) | 11 (58) | 11 (61) |
| Working status | ||
| Employed full-time, n (%) | 64 (89) | 60 (87) |
| Shift or late-night work, n (%) | 2 (3) | 1 (1) |
| Four-year college graduate or higher, n (%) | 52 (72) | 52 (75) |
| Household income, n (%) | ||
| <3,000,000 JPY | 8 (11) | 4 (6) |
| 3,000,000 JPY to 5,000,000 JPY | 10 (14) | 8 (12) |
| 5,000,000 JPY to 7,000,000 JPY | 14 (19) | 17 (25) |
| 7,000,000 JPY to 10,000,000 JPY | 21 (29) | 24 (35) |
| ≥10,000,000 JPY | 19 (26) | 16 (23) |
| Living alone, n (%) | 14 (19) | 11 (16) |
| Married, n (%) | 50 (69) | 54 (78) |
| Intervention | Control | Adjusted Mean Difference 1 (p-Value) | |||
|---|---|---|---|---|---|
| n | Mean ± SD | n | Mean ± SD | ||
| Weight, kg | |||||
| Baseline | 72 | 76.5 ± 9.6 | 69 | 79.1 ± 11.3 | |
| Month 3 | 71 | 73.8 ± 9.5 | 69 | 78.4 ± 12.0 | |
| Change | 71 | −2.4 ± 4.0 | 69 | −0.7 ± 3.3 | −1.60 [−2.83, −0.38] (p = 0.011) |
| Change 2 Median [Q1, Q3] | 71 | −1.3 [−3.2, −0.5] | 69 | −0.4 [−1.6, 0.9] | (p < 0.001) |
| Triglyceride, mg/dL | |||||
| Baseline | 72 | 140.6 ± 99.8 | 69 | 161.5 ± 127.4 | |
| Month 3 | 71 | 129.7 ± 139.3 | 67 | 171.1 ± 142.5 | |
| Change | 71 | −9.9 ± 87.7 | 67 | 8.6 ± 144.8 | −23.73 [−61.94, 14.47] (p = 0.22) |
| HDL cholesterol, mg/dL | |||||
| Baseline | 72 | 60.9 ± 12.0 | 69 | 57.9 ± 12.8 | |
| Month 3 | 71 | 63.6 ± 12.8 | 67 | 58.4 ± 12.0 | |
| Change | 71 | 2.4 ± 6.1 | 67 | 1.4 ± 7.6 | 1.42 [−0.84, 3.68] (p = 0.22) |
| LDL cholesterol, mg/dL | |||||
| Baseline | 72 | 122.3 ± 30.1 | 69 | 119.0 ± 30.5 | |
| Month 3 | 71 | 118.8 ± 28.3 | 67 | 117.9 ± 28.4 | |
| Change | 71 | −3.2 ± 15.5 | 67 | 0.0 ± 17.2 | −2.45 [−7.50, 2.61] (p = 0.34) |
| Hemoglobin A1c, % | |||||
| Baseline | 72 | 5.6 ± 0.4 | 69 | 5.5 ± 0.4 | |
| Month 3 | 71 | 5.6 ± 0.4 | 67 | 5.6 ± 0.5 | |
| Change | 71 | 0.0 ± 0.1 | 67 | 0.1 ± 0.2 | −0.04 [−0.08, 0.01] (p = 0.15) |
| Glucose, mg/dL | |||||
| Baseline | 72 | 108.2 ± 14.3 | 69 | 107.4 ± 15.3 | |
| Month 3 | 71 | 106.8 ± 16.0 | 67 | 107.7 ± 13.6 | |
| Change | 71 | −1.5 ± 11.6 | 67 | 1.2 ± 11.8 | −2.43 [−6.08, 1.23] (p = 0.19) |
| Intervention | Control | Adjusted Mean Difference 1 (p-Value) | |||
|---|---|---|---|---|---|
| n | Mean ± SD | n | Mean ± SD | ||
| Energy intake, kcal/day | |||||
| Baseline | 72 | 1866.2 ± 539.9 | 69 | 1847.1 ± 655.0 | |
| Month 3 | 71 | 1764.2 ± 579.6 | 69 | 1715.2 ± 562.4 | |
| Change | 71 | −85.5 ± 465.4 | 69 | −132.0 ± 513.2 | 58.7 [−82.5, 199.8] (p = 0.41) |
| Protein intake, % | |||||
| Baseline | 72 | 15.3 ± 2.8 | 69 | 14.6 ± 2.7 | |
| Month 3 | 71 | 15.5 ± 2.4 | 69 | 15.2 ± 2.9 | |
| Change | 71 | 0.1 ± 2.9 | 69 | 0.7 ± 2.4 | −0.18 [−0.94, 0.58] (p = 0.63) |
| Fat intake, % | |||||
| Baseline | 72 | 29.1 ± 5.8 | 69 | 27.6 ± 7.0 | |
| Month 3 | 71 | 29.1 ± 4.8 | 69 | 28.1 ± 6.3 | |
| Change | 71 | −0.1 ± 5.8 | 69 | 0.6 ± 6.3 | 0.18 [−1.45, 1.82] (p = 0.82) |
| Carbohydrate intake, % | |||||
| Baseline | 72 | 48.3 ± 9.2 | 69 | 47.5 ± 9.6 | |
| Month 3 | 71 | 49.0 ± 8.4 | 69 | 46.7 ± 10.3 | |
| Change | 71 | 0.8 ± 8.9 | 69 | −0.7 ± 8.0 | 1.85 [−0.67, 4.36] (p = 0.15) |
| Step count, steps/day | |||||
| Baseline | 70 | 8087 ± 3567 | 69 | 7751 ± 3145 | |
| Month 3 | 68 | 7783 ± 4030 | 64 | 6688 ± 3018 | |
| Change | 68 | −401 ± 3613 | 64 | −1271 ± 2391 | 922 [−21, 1865] (p = 0.055) |
| MVPA, min/day | |||||
| Baseline | 70 | 65.2 ± 39.8 | 69 | 60.4 ± 25.8 | |
| Month 3 | 68 | 62.7 ± 41.0 | 64 | 54.3 ± 23.1 | |
| Change | 68 | −2.0 ± 33.3 | 64 | −7.5 ± 20.2 | 6.78 [−1.60, 15.15] (p = 0.11) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nakata, Y.; Sasai, H.; Gosho, M.; Kobayashi, H.; Shi, Y.; Ohigashi, T.; Mizuno, S.; Murayama, C.; Kobayashi, S.; Sasaki, Y. A Smartphone Healthcare Application, CALO mama Plus, to Promote Weight Loss: A Randomized Controlled Trial. Nutrients 2022, 14, 4608. https://doi.org/10.3390/nu14214608
Nakata Y, Sasai H, Gosho M, Kobayashi H, Shi Y, Ohigashi T, Mizuno S, Murayama C, Kobayashi S, Sasaki Y. A Smartphone Healthcare Application, CALO mama Plus, to Promote Weight Loss: A Randomized Controlled Trial. Nutrients. 2022; 14(21):4608. https://doi.org/10.3390/nu14214608
Chicago/Turabian StyleNakata, Yoshio, Hiroyuki Sasai, Masahiko Gosho, Hiroyuki Kobayashi, Yutong Shi, Tomohiro Ohigashi, Shinichiro Mizuno, Chiaki Murayama, Satomi Kobayashi, and Yuki Sasaki. 2022. "A Smartphone Healthcare Application, CALO mama Plus, to Promote Weight Loss: A Randomized Controlled Trial" Nutrients 14, no. 21: 4608. https://doi.org/10.3390/nu14214608
APA StyleNakata, Y., Sasai, H., Gosho, M., Kobayashi, H., Shi, Y., Ohigashi, T., Mizuno, S., Murayama, C., Kobayashi, S., & Sasaki, Y. (2022). A Smartphone Healthcare Application, CALO mama Plus, to Promote Weight Loss: A Randomized Controlled Trial. Nutrients, 14(21), 4608. https://doi.org/10.3390/nu14214608