
Efficacy and Safety of Fig (Ficus carica L.) Leaf Tea in Adults with Mild Atopic Dermatitis: A Double-Blind, Randomized, Placebo-Controlled Preliminary Trial


Abstract
1. Introduction
2. Materials and Methods
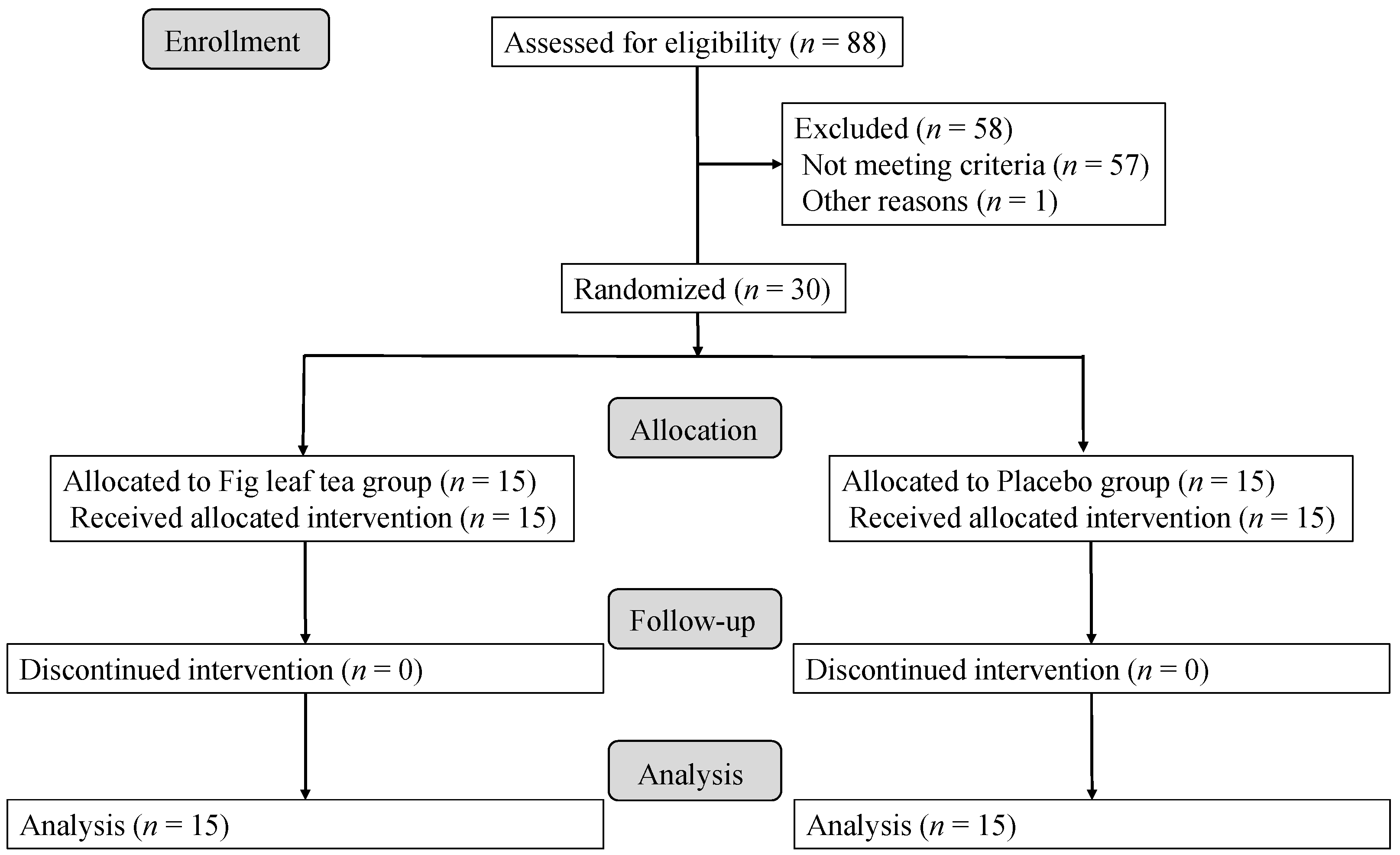
2.1. Participants and Ethics Approval
2.2. Study Design
2.3. Preparation of Fig Leaf Tea
2.4. Study Outcomes
2.5. Safety Assessments
2.6. Nutrient Analysis of Fig Leaf Tea
2.7. Statistical Analysis
3. Results
3.1. Background of Participants
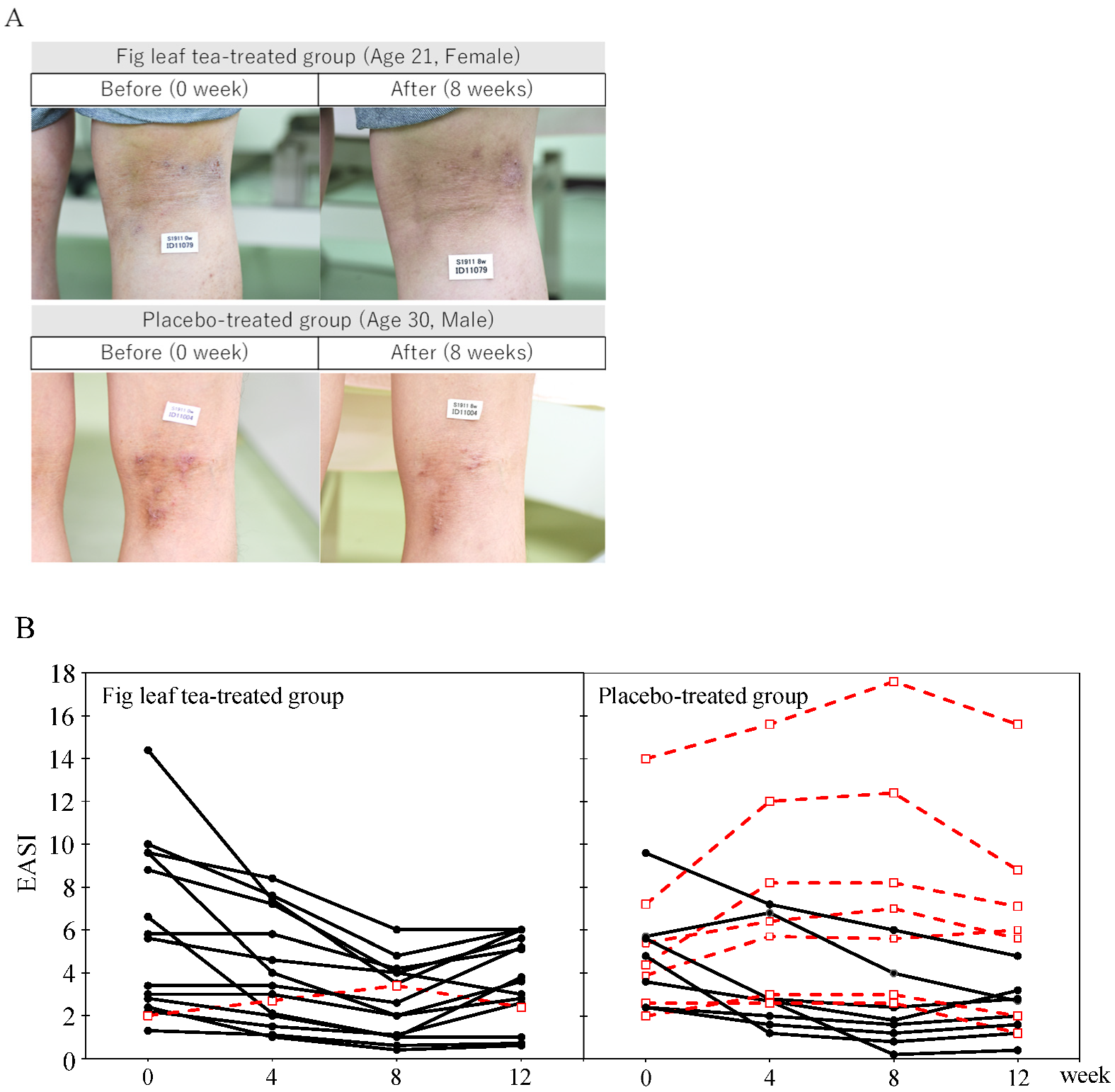
3.2. Comparison of Skin Symptoms
3.3. Comparison of Subjective Symptoms
3.4. Comparison of Blood Components
3.5. Comparison of Safety Assessments
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Harris, J.; Cullinan, P.; Williams, H.; Mills, P.; Moffat, S.; White, C.; Taylor, A.N. Environmental associations with eczema in early life. Br. J. Dermatol. 2001, 144, 795–802. [Google Scholar] [CrossRef] [PubMed]
- Kalliomäki, M.; Salminen, S.; Arvilommi, H.; Kero, P.; Koskinen, P.; Isolauri, E. Probiotics in primary prevention of atopic disease: A randomised placebo-controlled trial. Lancet 2001, 357, 1076–1079. [Google Scholar] [CrossRef]
- Rautava, S.; Kalliomäki, M.; Isolauri, E. Probiotics during pregnancy and breast-feeding might confer immunomodulatory protection against atopic disease in the infant. J. Allergy Clin. Immunol. 2002, 109, 119–121. [Google Scholar] [CrossRef] [PubMed]
- Pelucchi, C.; Chatenoud, L.; Turati, F.; Galeone, C.; Moja, L.; Bach, J.F.; La Vecchia, C. Probiotics supplementation during pregnancy or infancy for the prevention of atopic dermatitis: A meta-analysis. Epidemiology 2012, 23, 402–414. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, K.; Yokoyama, K.; Matsukawa, T.; Kato, S.; Kato, S.; Yamada, K.; Hirota, T. Efficacy of prolonged ingestion of Lactobacillus acidophilus L-92 in adult patients with atopic dermatitis. J. Dairy Sci. 2016, 99, 5039–5046. [Google Scholar] [CrossRef]
- 5 Things to Know about Probiotics. Available online: https://www.nccih.nih.gov/health/tips/things-to-know-about-probiotics (accessed on 16 May 2022).
- Doron, S.; Snydman, D.R. Risk and safety of probiotics. Clin. Infect. Dis. 2015, 60 (Suppl. S2), S129–S134. [Google Scholar] [CrossRef]
- Palmer, C.N.; Irvine, A.D.; Terron-Kwiatkowski, A.; Zhao, Y.; Liao, H.; Lee, S.P.; Goudie, D.R.; Sandilands, A.; Campbell, L.E.; Smith, F.J.; et al. Common loss-of-function variants of the epidermal barrier protein filaggrin are a major predisposing factor for atopic dermatitis. Nat. Genet. 2006, 38, 441–446. [Google Scholar] [CrossRef]
- Tokura, Y. Extrinsic and intrinsic types of atopic dermatitis. J. Dermatol. Sci. 2010, 58, 1–7. [Google Scholar] [CrossRef]
- Saeki, H.; Tamaki, K. Thymus and activation regulated chemokine (TARC)/CCL17 and skin diseases. J. Dermatol. Sci. 2006, 43, 75–84. [Google Scholar] [CrossRef]
- Leung, D.Y.; Guttman-Yassky, E. Deciphering the complexities of atopic dermatitis: Shifting paradigms in treatment approaches. J. Allergy Clin. Immunol. 2014, 134, 769–779. [Google Scholar] [CrossRef]
- Pastore, S.; Mascia, F.; Giustizieri, M.L.; Giannetti, A.; Girolomoni, G. Pathogenetic mechanisms of atopic dermatitis. Arch. Immunol. Ther. Exp. 2000, 48, 497–504. [Google Scholar]
- Mack, M.R.; Kim, B.S. The itch-scratch cycle: A neuroimmune perspective. Trends Immunol. 2018, 39, 980–991. [Google Scholar] [CrossRef]
- Hepburn, D.J.; Aeling, J.L.; Weston, W.L. A reappraisal of topical steroid potency. Pediatr. Dermatol. 1996, 13, 239–245. [Google Scholar] [CrossRef]
- Li, M.; Tan, W.; Du, J.; Wang, Q.; Wang, L.; Lei, M.; Hao, P.S. Tacrolimus ointment in the treatment of hormone-dependent dermatitis: A protocol of systematic review. Medicine 2020, 99, e22159. [Google Scholar] [CrossRef]
- Nakagawa, H.; Nemoto, O.; Igarashi, A.; Saeki, H.; Kaino, H.; Nagata, T. Delgocitinib ointment, a topical Janus kinase inhibitor, in adult patients with moderate to severe atopic dermatitis: A phase 3, randomized, double-blind, vehicle-controlled study and an open-label, long-term extension study. J. Am. Acad. Dermatol. 2020, 82, 823–831. [Google Scholar] [CrossRef]
- Coondoo, A.; Phiske, M.; Verma, S.; Lahiri, K. Side-effects of topical steroids: A long overdue revisit. Indian Dermatol. Online J. 2014, 5, 416–425. [Google Scholar] [CrossRef]
- Hengge, U.R.; Ruzicka, T.; Schwartz, R.A.; Cork, M.J. Adverse effects of topical glucocorticosteroids. J. Am. Acad. Dermatol. 2006, 54, 1–15. [Google Scholar] [CrossRef]
- Ohtsuki, M.; Morimoto, H.; Nakagawa, H. Tacrolimus ointment for the treatment of adult and pediatric atopic dermatitis: Review on safety and benefits. J. Dermatol. 2018, 45, 936–942. [Google Scholar] [CrossRef]
- Katoh, N.; Ohya, Y.; Ikeda, M.; Ebihara, T.; Katayama, I.; Saeki, H.; Shimojo, N.; Tanaka, A.; Nakahara, T.; Nagao, M.; et al. Clinical practice guidelines for the management of atopic dermatitis 2018. J. Dermatol. 2019, 46, 1053–1101. [Google Scholar] [CrossRef]
- Zou, Q.; Zhang, X.; Liu, X.; Li, Y.; Tan, Q.; Dan, Q.; Yuan, T.; Liu, X.; Liu, R.H.; Liu, Z. Ficus carica polysaccharide attenuates DSS-induced ulcerative colitis in C57BL/6 mice. Food Funct. 2020, 11, 6666–6679. [Google Scholar] [CrossRef]
- Baek, H.I.; Ha, K.C.; Kim, H.M.; Choi, E.K.; Park, E.O.; Park, B.H.; Yang, H.J.; Kim, M.J.; Kang, H.J.; Chae, S.W. Randomized, double-blind, placebo-controlled trial of Ficus carica paste for the management of functional constipation. Asia Pac. J. Clin. Nutr. 2016, 25, 487–496. [Google Scholar] [PubMed]
- Mazhin, S.A.; Zaker, M.A.; Shahbazian, H.B.; Azemi, M.E.; Madanchi, N. Ficus carica leaves decoction on glycemic factors of patients with type 2 diabetes mellitus: A double-blind clinical trial. Jundishapur. J. Nat. Pharm. Prod. 2016, 11, e25814. [Google Scholar]
- Irudayaraj, S.S.; Christudas, S.; Antony, S.; Duraipandiyan, V.; Abdullah, A.D.N.; Ignacimuthu, S. Protective effects of Ficus carica leaves on glucose and lipids levels, carbohydrate metabolism enzymes and β-cells in type 2 diabetic rats. Pharm. Biol. 2017, 55, 1074–1081. [Google Scholar] [CrossRef] [PubMed]
- Patil, V.V.; Patil, V.R. Evaluation of anti-inflammatory activity of Ficus carica Linn. leaves. Indian J. Nat. Prod. Resour. 2011, 2, 151–155. [Google Scholar]
- Zhang, Y.; Wan, Y.; Huo, B.; Li, B.; Jin, Y.; Hu, X. Extracts and components of Ficus carica leaves suppress survival, cell cycle, and migration of triple-negative breast cancer MDA-MB-231 cells. Onco Targets Ther. 2018, 11, 4377–4386. [Google Scholar] [CrossRef] [PubMed]
- Joerin, L.; Kauschka, M.; Bonnländer, B.; Pischel, I.; Benedek, B.; Butterweck, V. Ficus carica leaf extract modulates the lipid profile of rats fed with a high-fat diet through an increase of HDL-C. Phytother. Res. 2014, 28, 261–267. [Google Scholar] [CrossRef]
- Purnamasari, R.; Winarni, D.; Permanasari, A.A.; Agustina, E.; Hayaza, S.; Darmanto, W. Anticancer activity of methanol extract of Ficus carica leaves and fruits against proliferation, apoptosis, and necrosis in Huh7it cells. Cancer Inform. 2019, 18, 1176935119842576. [Google Scholar] [CrossRef]
- Khodarahmi, G.A.; Ghasemi, N.; Hassanzadeh, F.; Safaie, M. Cytotoxic effects of different extracts and latex of Ficus carica L. on HeLa cell line. Iran. J. Pharm. Res. 2011, 10, 273–277. [Google Scholar]
- AlGhalban, F.M.; Khan, A.A.; Khattak, M.N.K. Comparative anticancer activities of Ficus carica and Ficus salicifolia latex in MDA-MB-231 cells. Saudi J. Biol. Sci. 2021, 28, 3225–3234. [Google Scholar]
- Takahashi, T.; Okiura, A.; Saito, K.; Kohno, M. Identification of phenylpropanoids in fig (Ficus carica L.) leaves. J. Agric Food Chem. 2014, 62, 10076–10083. [Google Scholar]
- Abe, T. Fig (Ficus carica L.) leaf tea suppresses allergy by acceleration disassembly of IgE-receptor complexes. Biosci. Biotechnol. Biochem. 2020, 84, 1013–1022. [Google Scholar] [CrossRef]
- Holm, J.G.; Agner, T.; Sand, C.; Thomsen, S.F. Omalizumab for atopic dermatitis: Case series and a systematic review of the literature. Int. J. Dermatol. 2017, 56, 18–26. [Google Scholar] [CrossRef]
- Holm, J.G.; Thomsen, S.F. Omalizumab for atopic dermatitis: Evidence for and against its use. G. Ital. Dermatol. Venereol. 2019, 154, 480–487. [Google Scholar] [CrossRef]
- Chan, S.; Cornelius, V.; Cro, S.; Harper, J.I.; Lack, G. Treatment effect of omalizumab on severe pediatric atopic dermatitis: The ADAPT randomized clinical trial. JAMA Pediatr. 2020, 174, 29–37. [Google Scholar] [CrossRef]
- Condit, I. Fig varieties: A monograph. Hilgardia 1955, 23, 323–538. [Google Scholar] [CrossRef]
- Takahashi, T.; Okiura, A.; Kohno, M. Phenylpropanoid composition in fig (Ficus carica L.) leaves. J. Nat. Med. 2017, 71, 770–775. [Google Scholar] [CrossRef]
- Charman, C.R.; Venn, A.J.; Ravenscroft, J.C.; Williams, H.C. Translating Patient-Oriented Eczema Measure (POEM) scores into clinical practice by suggesting severity strata derived using anchor-based methods. Br. J. Dermatol. 2013, 169, 1326–1332. [Google Scholar] [CrossRef]
- Ministry of Education, Culture, Sports, Science and Technology (Japan). Standard Tables of Food Composition in Japan, 2020. 2020. Available online: https://www.mext.go.jp/a_menu/syokuhinseibun/mext_01110.html (accessed on 21 June 2022). (In Japanese).
- Kanda, Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant. 2013, 48, 452–458. [Google Scholar] [CrossRef]
- Leshem, Y.A.; Hajar, T.; Hanifin, J.M.; Simpson, E.L. What the Eczema Area and Severity Index score tells us about the severity of atopic dermatitis: An interpretability study. Br. J. Dermatol. 2015, 172, 1353–1357. [Google Scholar] [CrossRef]
- Schram, M.E.; Spuls, P.I.; Leeflang, M.M.; Lindeboom, R.; Bos, J.D.; Schmitt, J. EASI, (objective) SCORAD and POEM for atopic eczema: Responsiveness and minimal clinically important difference. Allergy 2012, 67, 99–106. [Google Scholar] [CrossRef]
- Thijs, J.; Krastev, T.; Weidinger, S.; Buckens, C.F.; de Bruin-Weller, M.; Bruijnzeel-Koomen, C.; Flohr, C.; Hijnen, D. Biomarkers for atopic dermatitis: A systematic review and meta-analysis. Curr. Opin. Allergy Clin. Immunol. 2015, 15, 453–460. [Google Scholar] [CrossRef] [PubMed]
- Kataoka, Y. Thymus and activation-regulated chemokine as a clinical biomarker in atopic dermatitis. J. Dermatol. 2014, 41, 221–229. [Google Scholar] [CrossRef] [PubMed]
- Ito, K.; Inoue, Y.; Ikezawa, Y.; Takeshita, Y.; Aihara, M.; Ikezawa, Y. Relationship among fluctuations of serum TARC levels, peripheral eosinophil counts and serum IgE levels in atopic dermatitis patients. J. Environ. Dermatol. Cutan. Allergol. 2012, 6, 351–358. (In Japanese) [Google Scholar]
- Matsuo, K.; Nagakubo, D.; Komori, Y.; Fujisato, S.; Takeda, N.; Kitamatsu, M.; Nishiwaki, K.; Quan, Y.-S.; Kamiyama, F.; Oiso, N.; et al. CCR4 is critically involved in skin allergic inflammation of BALB/c mice. J. Investig. Dermatol. 2018, 138, 1764–1773. [Google Scholar] [CrossRef] [PubMed]
- Kakinuma, T.; Nakamura, K.; Wakugawa, M.; Mitsui, H.; Tada, Y.; Saeki, H.; Torii, H.; Asahina, A.; Onai, N.; Matsushima, K.; et al. Thymus and activation-regulated chemokine in atopic dermatitis: Serum thymus and activation-regulated chemokine level is closely related with disease activity. J. Allergy Clin. Immunol. 2001, 107, 535–541. [Google Scholar] [CrossRef]
- Lim, J.Y.; Lee, J.H.; Lee, D.H.; Lee, J.H.; Kim, D.K. Umbelliferone reduces the expression of inflammatory chemokines in HaCaT cells and DNCB/DFE-induced atopic dermatitis symptoms in mice. Int. Immunopharmacol. 2019, 75, 105830. [Google Scholar] [CrossRef]
- Gond, N.Y.; Khadabadi, S.S. Hepatoprotective activity of Ficus carica leaf extract on rifampicin-induced hepatic damage in rats. Indian J. Pharm. Sci. 2008, 70, 364–366. [Google Scholar] [CrossRef]
- Aghel, N.; Kalantari, H.; Rezazadeh, S. Hepatoprotective effect of Ficus carica leaf extract on mice intoxicated with carbon tetrachloride. Iran. J. Pharm. Res. 2011, 10, 63–68. [Google Scholar]
- Mohan, G.K.; Pallavi, E.; Ravi, K.B.; Ramesh, M.; Venkatesh, S. Hepatoprotective activity of Ficus carica Linn leaf extract against carbon tetrachloride-induced hepatotoxicity in rats. DARU J. Pharm. Sci 2007, 15, 162–166. [Google Scholar]
- Kimata, H. Prevalence of fatty liver in non-obese Japanese children with atopic dermatitis. Indian Pediatr. 2005, 42, 587–593. [Google Scholar]
- Iwasaki, A.; Yamashita, Y.; Tsubaki, T.; Matsuda, S.; Sugihara, Y.; Akimoto, K.; Akasawa, A.; Obata, T.; Iikura, Y. Study of liver function in babies with atopic dermatitis by using 13C-methacetin breath test. Arerugi 1992, 41, 645–653. (In Japanese) [Google Scholar]
- Silverberg, J.I.; Silverberg, N.B. Atopic dermatitis: Update on pathogenesis and comorbidities. Curr. Dermatol. Rep. 2012, 1, 168–178. [Google Scholar] [CrossRef]
- Gittlen, S.D.; Schulman, E.S.; Maddrey, W.C. Raised histamine concentrations in chronic cholestatic liver disease. Gut 1990, 31, 96–99. [Google Scholar] [CrossRef]
- Thornton, J.R.; Losowsky, M.S. Opioid peptides and primary biliary cirrhosis. BMJ 1988, 297, 1501–1504. [Google Scholar] [CrossRef]
- Kwashima, Y. A study on pruritogens of pruritus in primary biliary cirrhosis: Relations with peripheral concentration of opioid peptides. Teikyo Igaku. Zasshi. 2005, 28, 89–97. [Google Scholar]
- Moniaga, C.S.; Iwamoto, S.; Kitamura, T.; Fujishiro, M.; Takahashi, N.; Kina, K.; Ogawa, H.; Tominaga, M.; Takamori, K. Plasma dynorphin A concentration reflects the degree of pruritus in chronic liver disease: A preliminary report. Acta Derm. Venereol. 2019, 99, 442–443. [Google Scholar] [CrossRef]
- Tominaga, M.; Ogawa, H.; Takamori, K. Possible roles of epidermal opioid systems in pruritus of atopic dermatitis. J. Investig. Dermatol. 2007, 127, 2228–2235. [Google Scholar] [CrossRef]
- Bigliardi, P.L.; Stammer, H.; Jost, G.; Rufli, T.; Büchner, S.; Bigliardi-Qi, M. Treatment of pruritus with topically applied opiate receptor antagonist. J. Am. Acad. Dermatol. 2007, 56, 979–988. [Google Scholar] [CrossRef]
- Hussein, A.; Shugaev, I. Phototoxic response to Ficus carica leaf and shoot saps. Isr. Med. Assoc. J. 2012, 14, 399–400. [Google Scholar]
- Ameer, B.; Weintraub, R.A. Drug interactions with grapefruit juice. Clin. Pharmacokinet. 1997, 33, 103–121. [Google Scholar] [CrossRef]
- Bailey, D.G.; Malcolm, J.; Arnold, O.; Spence, J.D. Grapefruit juice-drug interactions. Br. J. Clin. Pharmacol. 1998, 46, 101–110. [Google Scholar] [CrossRef] [PubMed]
- Hanley, M.J.; Cancalon, P.; Widmer, W.W.; Greenblatt, D.J. The effect of grapefruit juice on drug disposition. Expert Opin. Drug Metab. Toxicol. 2011, 7, 267–286. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Nutritional Compositions | Contents |
|---|---|
| Calories (Kcal/100 mL) | 2 |
| Carbohydrate (g/100 mL) | 0.5 |
| Crude fat (g/100 mL) | <0.1 |
| Crude protein (g/100 mL) | <0.1 |
| Water (%) | 99.8 |
| Ash (g/100 mL) | <0.1 |
| Fiber (g/100 mL) | <0.1 |
| Total phenolic compounds (g/100 mL) | 0.02 |
| Rutin (mg/100 mL) | 3.7 |
| Quercetin malonyl glucoside (mg/100 mL) | 0.6 |
| Isoschaftoside (mg/100 mL) | 2.3 |
| 8-Hydoroxy coumalin (mg/100 mL) | 1 |
| Sodium ascorbate (mg/100 mL) | 250 |
| Fig Leaf Tea Group (n = 15) | Placebo Group (n = 15) | p-Value | |
|---|---|---|---|
| Age (years) | 41.0 ± 10.8 | 40.7 ± 11.2 | 0.934 |
| Sex (M/F) | 8/7 | 9/6 | 1.000 |
| Height (cm) | 167.2 ± 7.7 | 166.3 ± 11.6 | 0.815 |
| Weight (kg) | 64.3 ± 11.7 | 65.4 ± 13.9 | 0.824 |
| BMI (kg/m2) | 23.0 ± 3.5 | 23.4 ± 3.0 | 0.696 |
| EASI | 5.83 ± 3.89 | 5.15 ± 3.18 | 0.803 |
| Group | Measurement | Variation | ||||||
|---|---|---|---|---|---|---|---|---|
| 0 Week | 4 Week | 8 Week | 12 Week | 4 Week | 8 Week | 12 Week | ||
| EASI | Fig leaf tea | 5.83 ± 3.89 | 4.12 ± 2.56 † | 2.71 ± 1.71 † | 3.63 ± 1.96 | −1.71 ± 2.25 | −3.13 ± 3.18 | −2.21 ± 2.92 |
| Placebo | 5.15 ± 3.18 | 5.37 ± 4.14 | 4.96 ± 4.81 | 4.33 ± 3.95 | 0.22 ± 2.31 | −0.19 ± 2.92 | −0.81 ± 2.28 | |
| p-value | 0.803 | 0.633 | 0.280 | 0.983 | 0.044 * | 0.036 * | 0.245 | |
| Group | Measurement | Variation | ||||||
|---|---|---|---|---|---|---|---|---|
| 0 Week | 4 Week | 8 Week | 12 Week | 4 Week | 8 Week | 12 Week | ||
| POEM | Fig leaf tea | 9.8 ± 5.9 | 8.5 ± 4.9 | 8.5 ± 6.7 | 7.5 ± 7.1 | −1.3 ± 5.8 | −1.3 ± 7.4 | −2.3 ± 7.1 |
| Placebo | 13.1 ± 5.7 | 10.7 ± 4.7 | 8.3 ± 5.8 † | 8.3 ± 4.0 † | −2.4 ± 3.9 | −4.8 ± 5.2 | −4.9 ± 4.9 | |
| p-value | 0.058 | 0.220 | 0.900 | 0.453 | 0.544 | 0.109 | 0.176 | |
| VAS | Group | Measurement | Variation | |||||
|---|---|---|---|---|---|---|---|---|
| 0 Week | 4 Week | 8 Week | 12 Week | 4 Week | 8 Week | 12 Week | ||
| Skin condition | Fig leaf tea | 29.1 ± 13.4 | 25.0 ± 13.5 | 22.3 ± 13.1 | 22.1 ± 16.2 | −4.1 ± 10.5 | −6.7 ± 12.2 | −6.9 ± 14.8 |
| Placebo | 32.1 ± 14.2 | 28.1 ± 14.1 | 23.9 ± 13.9 | 24.3 ± 14.3 | −4.0 ± 11.3 | −8.2 ± 11.6 | −7.8 ± 11.3 | |
| p-value | 0.663 | 0.520 | 0.917 | 0.683 | 0.724 | 0.806 | 0.806 | |
| Impact on QOL | Fig leaf tea | 15.6 ± 8.2 | 16.2 ± 11.7 | 15.7 ± 11.4 | 16.9 ± 12.4 | 0.6 ± 7.8 | 0.1 ± 8.6 | 1.4 ± 8.2 |
| Placebo | 18.2 ± 10.5 | 17.8 ± 10.0 | 17.0 ± 10.8 | 19.3 ± 11.7 | −0.4 ± 9.4 | −1.1 ± 8.8 | 1.2 ± 8.4 | |
| p-value | 0.481 | 0.653 | 0.618 | 0.595 | 0.838 | 0.820 | 0.868 | |
| Group | Measurement | Variation | ||||||
|---|---|---|---|---|---|---|---|---|
| 0 Week | 4 Week | 8 Week | 12 Week | 4 Week | 8 Week | 12 Week | ||
| TARC | Fig leaf tea | 323 ± 146 | 399 ± 202 | 365 ± 169 | 406 ± 255 | 76 ± 94 | 42 ± 79 | 82 ± 175 |
| Placebo | 983 ± 2770 | 1191 ± 2856 †† | 808 ± 1620 | 671 ± 1240 | 208 ± 360 | −175 ± 1217 | −312 ± 1541 | |
| p-value | 0.624 | 0.775 | 0.983 | 0.967 | 0.534 | 0.772 | 0.494 | |
| Th1/Th2 | Fig leaf tea | 8.2 ± 3.8 | 7.7 ± 3.6 | 7.5 ± 3.6 | 8.3 ± 3.4 | −0.4 ± 3.3 | −0.7 ± 1.6 | 0.2 ± 1.6 |
| Placebo | 6.4 ± 2.6 | 6.4 ± 3.5 | 5.6 ± 2.4 | 6.4 ± 2.6 | 0.0 ± 2.4 | −0.7 ± 1.6 | 0.0 ± 1.6 | |
| p-value | 0.142 | 0.308 | 0.109 | 0.090 | 0.667 | 0.919 | 0.777 | |
| IgE | Fig leaf tea | 314 ± 788 | 282 ± 647 | 294 ± 670 | 303 ± 706 | −32 ± 145 | −20 ± 124 | −11 ± 96 |
| Placebo | 297 ± 438 | 337 ± 606 | 406 ± 716 | 456 ± 924 | 41 ± 179 | 109 ± 287 | 160 ± 497 | |
| p-value | 0.267 | 0.461 | 0.187 | 0.217 | 0.507 | 0.089 | 0.217 | |
| Normal Range | Group | Measurement | Variation | ||||
|---|---|---|---|---|---|---|---|
| −2 Week | 8 Week | 12 Week | 8 Week | 12 Week | |||
| AST | 10–40 | Fig leaf tea | 19.2 ± 4.7 | 17.5 ± 2.5 | 17.8 ± 3.5 | −1.7 ± 3.3 | −1.4 ± 2.2 |
| Placebo | 19.7 ± 6.4 | 20.8 ± 6.6 | 20.2 ± 7.1 | 1.1 ± 3.2 | 0.5 ± 3.1 | ||
| p-value | 0.820 | 0.078 | 0.250 | 0.022 * | 0.061 | ||
| ALT | 5–40 | Fig leaf tea | 17.5 ± 10.1 | 15.5 ± 6.8 | 16.1 ± 9.7 | −2.0 ± 5.6 | −1.5 ± 4.1 |
| Placebo | 19.6 ± 13.1 | 20.7 ± 10.5 | 19.9 ± 11.6 | 1.1 ± 6.6 | 0.3 ± 5.0 | ||
| p-value | 0.631 | 0.125 | 0.330 | 0.181 | 0.291 | ||
| LDH | 115–245 | Fig leaf tea | 169.7 ± 21.6 | 159.3 ± 19.2 | 166.4 ± 22.6 | −10.4 ± 16.6 | −3.3 ± 16.1 |
| Placebo | 168.9 ± 40.4 | 173.3 ± 46.8 | 169.0 ± 41.2 | 4.3 ± 19.9 | 0.1 ± 11.9 | ||
| p-value | 0.951 | 0.293 | 0.832 | 0.037 * | 0.525 | ||
| ALP | 115–359 | Fig leaf tea | 166.2 ± 35.4 | 157.7 ± 35.4 † | 156.9 ± 31.3 | −8.5 ± 9.8 | −9.3 ± 15.1 |
| Placebo | 178.2 ± 43.8 | 180.0 ± 45.7 | 182.4 ± 39.6 | 1.8 ± 21.3 | 4.2 ± 24.7 | ||
| p-value | 0.417 | 0.148 | 0.060 | 0.105 | 0.083 | ||
| Normal Range | Group | Measurement | Variation | ||||
|---|---|---|---|---|---|---|---|
| −2 Week | 8 Week | 12 Week | 8 Week | 12 Week | |||
| uric acid | M: 3.7–7.0 F: 2.5–7.0 | Fig leaf tea | 5.03 ± 1.38 | 5.15 ± 1.37 | 5.15 ± 1.21 | 0.12 ± 0.57 | 0.12 ± 0.67 |
| Placebo | 5.25 ± 1.47 | 5.60 ± 1.48 | 5.72 ± 1.68 | 0.35 ± 0.70 | 0.47 ± 0.74 | ||
| p-value | 0.667 | 0.391 | 0.293 | 0.338 | 0.188 | ||
| urea nitrogen | 8.0–22.0 | Fig leaf tea | 13.76 ± 3.84 | 14.26 ± 2.99 | 13.71 ± 2.07 | 0.50 ± 2.30 | −0.05 ± 3.73 |
| Placebo | 12.64 ± 2.95 | 12.11 ± 3.73 | 12.70 ± 3.41 | −0.53 ± 3.74 | 0.06 ± 2.85 | ||
| p-value | 0.379 | 0.094 | 0.336 | 0.375 | 0.931 | ||
| γ-GTP | M: ≤70 F: ≤30 | Fig leaf tea | 21.67 ± 12.53 | 24.40 ± 17.89 | 22.33 ± 14.82 | 2.73 ± 14.58 | 0.67 ± 3.87 |
| Placebo | 21.33 ± 17.17 | 21.67 ± 16.24 | 21.93 ± 18.42 | 0.33 ± 4.10 | 0.60 ± 3.50 | ||
| p-value | 0.952 | 0.665 | 0.948 | 0.548 | 0.961 | ||
| total bilirubin | 0.3–1.2 | Fig leaf tea | 0.69 ± 0.27 | 0.73 ± 0.35 | 0.77 ± 0.31 | 0.03 ± 0.33 | 0.08 ± 0.44 |
| Placebo | 0.63 ± 0.30 | 0.73 ± 0.33 | 0.66 ± 0.28 | 0.10 ± 0.23 | 0.03 ± 0.23 | ||
| p-value | 0.527 | 1.000 | 0.299 | 0.531 | 0.717 | ||
| total protein | 6.7–8.3 | Fig leaf tea | 7.39 ± 0.26 | 7.27 ± 0.34 | 7.29 ± 0.30 | −0.12 ± 0.33 | −0.11 ± 0.23 |
| Placebo | 7.37 ± 0.29 | 7.43 ± 0.43 | 7.36 ± 0.34 | 0.06 ± 0.33 | −0.01 ± 0.24 | ||
| p-value | 0.844 | 0.267 | 0.537 | 0.151 | 0.280 | ||
| albumin | 3.8–5.2 | Fig leaf tea | 4.54 ± 0.26 | 4.54 ± 0.32 | 4.56 ± 0.28 | 0.00 ± 0.23 | 0.02 ± 0.22 |
| Placebo | 4.63 ± 0.22 | 4.69 ± 0.29 | 4.65 ± 0.20 | 0.05 ± 0.27 | 0.01 ± 0.20 | ||
| p-value | 0.324 | 0.199 | 0.344 | 0.565 | 0.932 | ||
| creatinine | M: 0.61–1.04 F: 0.47–0.79 | Fig leaf tea | 0.73 ± 0.14 | 0.76 ± 0.14 | 0.75 ± 0.13 | 0.03 ± 0.08 | 0.02 ± 0.09 |
| Placebo | 0.71 ± 0.18 | 0.72 ± 0.17 | 0.71 ± 0.16 | 0.01 ± 0.05 | 0.00 ± 0.05 | ||
| p-value | 0.685 | 0.453 | 0.465 | 0.453 | 0.549 | ||
| amylase | 37–125 | Fig leaf tea | 82.13 ± 15.56 | 79.47 ± 18.49 | 78.80 ± 18.00 | −2.67 ± 11.63 | −3.53 ± 8.80 |
| Placebo | 76.33 ± 25.92 | 68.73 ± 23.86 | 70.73 ± 26.68 | −7.60 ± 6.83 | −5.60 ± 10.52 | ||
| p-value | 0.465 | 0.180 | 0.353 | 0.170 | 0.567 | ||
| total-Cho | 150–219 | Fig leaf tea | 197.13 ± 29.81 | 193.53 ± 31.71 | 191.27 ± 36.58 | −3.60 ± 14.82 | −5.87 ± 14.34 |
| Placebo | 195.67 ± 35.35 | 193.80 ± 38.63 | 190.93 ± 36.72 | −1.87 ± 15.56 | −4.73 ± 13.91 | ||
| p-value | 0.903 | 0.984 | 0.980 | 0.757 | 0.828 | ||
| LDL-Cho | 70–139 | Fig leaf tea | 115.67 ± 21.97 | 115.20 ± 25.01 | 111.07 ± 27.54 | −0.47 ± 19.96 | −4.60 ± 15.57 |
| Placebo | 117.40 ± 33.36 | 116.47 ± 32.44 | 115.00 ± 30.10 | −0.93 ± 14.38 | −2.40 ± 13.78 | ||
| p-value | 0.868 | 0.906 | 0.712 | 0.936 | 0.685 | ||
| TG | 50–149 | Fig leaf tea | 97.33 ± 53.10 | 77.33 ± 38.51 | 91.47 ± 67.02 | −20.00 ± 27.72 | −5.87 ± 56.67 |
| Placebo | 102.07 ± 71.83 | 98.33 ± 61.22 | 90.33 ± 58.73 | −3.73 ± 42.02 | −11.73 ± 39.44 | ||
| p-value | 0.839 | 0.272 | 0.961 | 0.223 | 0.745 | ||
| glucose | 70–109 | Fig leaf tea | 86.33 ± 9.22 | 87.80 ± 9.45 | 89.00 ± 7.50 | 1.47 ± 4.91 | 2.67 ± 8.05 |
| Placebo | 90.53 ± 10.00 | 88.73 ± 7.37 | 94.73 ± 12.54 | −1.80 ± 6.05 | 4.20 ± 9.01 | ||
| p-value | 0.242 | 0.765 | 0.142 | 0.116 | 0.627 | ||
| Na | 136–147 | Fig leaf tea | 140.80 ± 1.01 | 140.07 ± 1.33 | 140.27 ± 1.87 | −0.73 ± 1.16 | −0.53 ± 1.46 |
| Placebo | 140.27 ± 1.10 | 139.20 ± 1.93 | 139.47 ± 2.03 | −1.07 ± 1.22 | −0.80 ± 2.04 | ||
| p-value | 0.178 | 0.166 | 0.271 | 0.451 | 0.684 | ||
| Cl | 98–109 | Fig leaf tea | 103.93 ± 1.53 | 104.87 ± 1.13 | 104.33 ± 1.23 | 0.93 ± 1.28 | 0.40 ± 1.45 |
| Placebo | 103.60 ± 1.72 | 103.27 ± 1.79 | 104.07 ± 2.55 | −0.33 ± 2.26 | 0.47 ± 3.09 | ||
| p-value | 0.580 | 0.007 ** | 0.719 | 0.072 | 0.940 | ||
| K | 3.6–5.0 | Fig leaf tea | 4.05 ± 0.22 | 3.98 ± 0.13 | 3.94 ± 0.16 | −0.07 ± 0.18 | −0.11 ± 0.23 |
| Placebo | 4.15 ± 0.18 | 3.91 ± 0.23 | 4.02 ± 0.30 | −0.24 ± 0.28 | −0.13 ± 0.31 | ||
| p-value | 0.158 | 0.340 | 0.370 | 0.055 | 0.789 | ||
| Mg | 1.8–2.6 | Fig leaf tea | 2.29 ± 0.12 | 2.29 ± 0.14 | 2.27 ± 0.13 | −0.01 ± 0.21 | −0.03 ± 0.14 |
| Placebo | 2.25 ± 0.17 | 2.22 ± 0.18 | 2.17 ± 0.17 | −0.03 ± 0.09 | −0.03 ± 0.20 | ||
| p-value | 0.471 | 0.265 | 0.412 | 0.650 | 0.915 | ||
| Ca | 8.5–10.2 | Fig leaf tea | 9.45 ± 0.23 | 9.37 ± 0.35 | 9.36 ± 0.33 | −0.07 ± 0.30 | −0.09 ± 0.31 |
| Placebo | 9.46 ± 0.23 | 9.55 ± 0.33 | 9.35 ± 0.24 | 0.09 ± 0.32 | −0.11 ± 0.25 | ||
| p-value | 0.876 | 0.176 | 0.949 | 0.170 | 0.849 | ||
| Fe | F: 54–200 M: 48–154 | Fig leaf tea | 108.87 ± 45.17 | 94.73 ± 52.37 | 108.73 ± 50.86 | −14.13 ± 57.02 | −0.13 ± 70.60 |
| Placebo | 99.73 ± 33.67 | 99.93 ± 40.33 | 93.67 ± 42.32 | 0.20 ± 47.90 | −6.07 ± 46.56 | ||
| p-value | 0.536 | 0.763 | 0.386 | 0.462 | 0.788 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abe, T.; Koyama, Y.; Nishimura, K.; Okiura, A.; Takahashi, T. Efficacy and Safety of Fig (Ficus carica L.) Leaf Tea in Adults with Mild Atopic Dermatitis: A Double-Blind, Randomized, Placebo-Controlled Preliminary Trial. Nutrients 2022, 14, 4470. https://doi.org/10.3390/nu14214470
Abe T, Koyama Y, Nishimura K, Okiura A, Takahashi T. Efficacy and Safety of Fig (Ficus carica L.) Leaf Tea in Adults with Mild Atopic Dermatitis: A Double-Blind, Randomized, Placebo-Controlled Preliminary Trial. Nutrients. 2022; 14(21):4470. https://doi.org/10.3390/nu14214470
Chicago/Turabian StyleAbe, Tatsuya, Yukari Koyama, Kosaku Nishimura, Aya Okiura, and Toru Takahashi. 2022. "Efficacy and Safety of Fig (Ficus carica L.) Leaf Tea in Adults with Mild Atopic Dermatitis: A Double-Blind, Randomized, Placebo-Controlled Preliminary Trial" Nutrients 14, no. 21: 4470. https://doi.org/10.3390/nu14214470
APA StyleAbe, T., Koyama, Y., Nishimura, K., Okiura, A., & Takahashi, T. (2022). Efficacy and Safety of Fig (Ficus carica L.) Leaf Tea in Adults with Mild Atopic Dermatitis: A Double-Blind, Randomized, Placebo-Controlled Preliminary Trial. Nutrients, 14(21), 4470. https://doi.org/10.3390/nu14214470