

Association between Ultra-Processed Food Consumption and Diabetes in Chinese Adults—Results from the China Health and Nutrition Survey



Abstract
1. Introduction
2. Materials and Methods
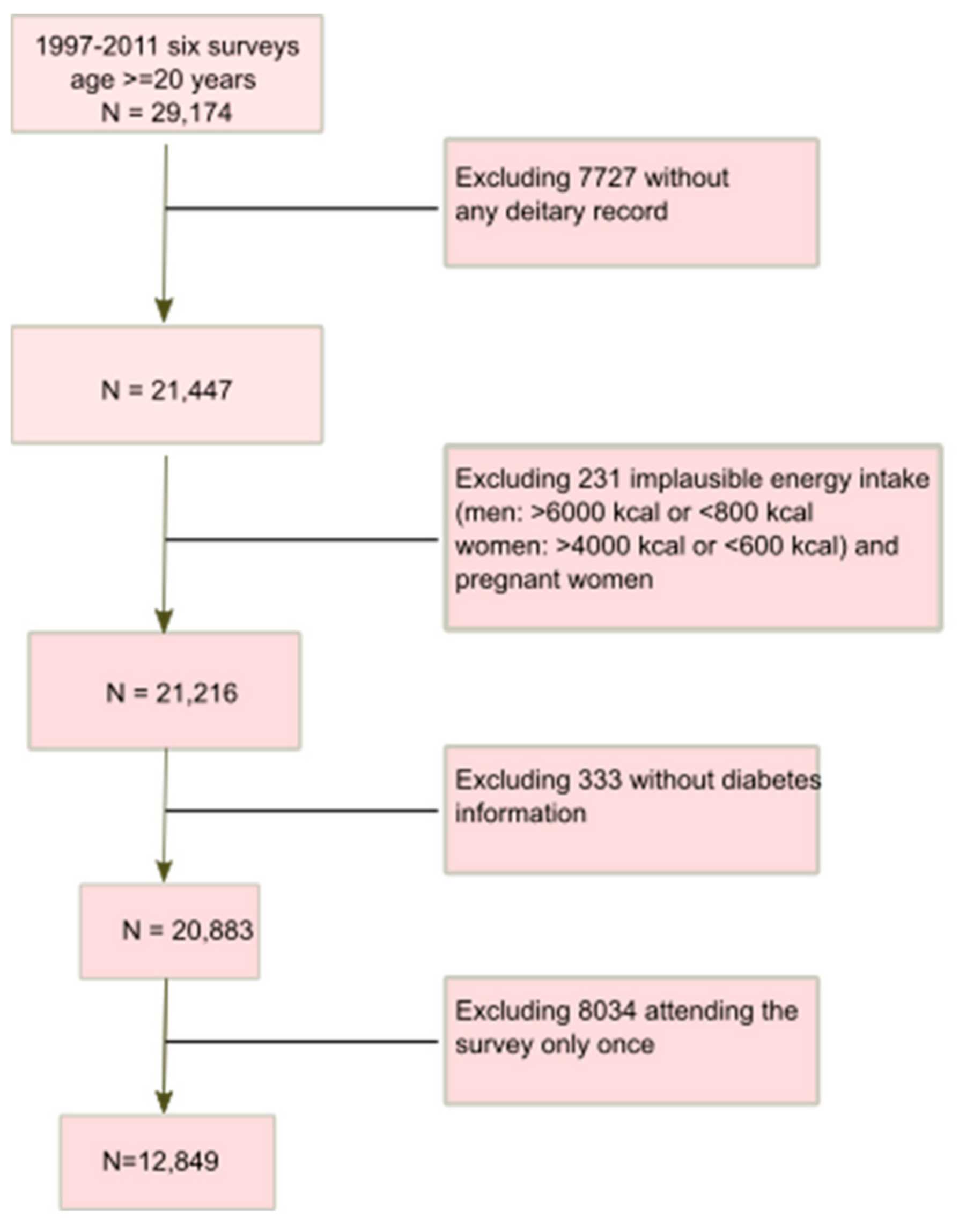
2.1. Study Design and Sample
2.2. Outcome Variable
2.3. UPF Assessment
2.4. Covariates
2.5. Statistical Analysis
3. Results
3.1. Population Profile
3.2. Consumption of UPF during 1997–2011
3.3. Diabetes and UPF Consumption Level
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Harding, J.L.; Pavkov, M.E.; Magliano, D.J.; Shaw, J.E.; Gregg, E.W. Global trends in diabetes complications: A review of current evidence. Diabetologia 2019, 62, 3–16. [Google Scholar] [CrossRef] [PubMed]
- International Diabetes Federation. IDF Diabetes Atlas. 2019. Available online: www.diabetesatlas.org/en/ (accessed on 27 April 2020).
- Dicker, D.; Nguyen, G.; Abate, D.; Abate, K.H.; Abay, S.M.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdela, J.; et al. Global, regional, and national age-sex-specific mortality and life expectancy, 1950–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1684–1735. [Google Scholar] [CrossRef]
- Jannasch, F.; Kroger, J.; Schulze, M.B. Dietary Patterns and Type 2 Diabetes: A Systematic Literature Review and Meta-Analysis of Prospective Studies. J. Nutr. 2017, 147, 1174–1182. [Google Scholar] [CrossRef] [PubMed]
- Monteiro, C.; Cannon, G.; Levy, R.B.; Claro, R.; Moubarac, J.; Martins, A.P.B.; Louzada, M.L.; Baraldi, L.G.; Canella, D. The Food System. Ultra-processing: The big issue for nutrition, disease, health, well-being. World Nutr. 2012, 3, 527–569. [Google Scholar]
- Monteiro, C.A.; Cannon, G.; Moubarac, J.C.; Levy, R.B.; Louzada, M.L.C.; Jaime, P.C. The UN Decade of Nutrition, the NOVA food classification and the trouble with ultra-processing. Public Health Nutr. 2018, 21, 5–17. [Google Scholar] [CrossRef]
- Euromonitor International. Passport Global Market Information Database. 2015. Available online: http://go.euromonitor.com/Passport-Home (accessed on 9 April 2022).
- Matos, R.A.; Adams, M.; Sabate, J. Review: The Consumption of Ultra-Processed Foods and Non-communicable Diseases in Latin America. Front. Nutr. 2021, 8, 622714. [Google Scholar] [CrossRef]
- Costa de Miranda, R.; Rauber, F.; Levy, R.B. Impact of ultra-processed food consumption on metabolic health. Curr. Opin. Lipidol. 2021, 32, 24–37. [Google Scholar] [CrossRef]
- Gomez-Smith, M.; Karthikeyan, S.; Jeffers, M.S.; Janik, R.; Thomason, L.A.; Stefanovic, B.; Corbett, D. A physiological characterization of the Cafeteria diet model of metabolic syndrome in the rat. Physiol. Behav. 2016, 167, 382–391. [Google Scholar] [CrossRef]
- Jensen, P.N.; Howard, B.V.; Best, L.G.; O’Leary, M.; Devereux, R.B.; Cole, S.A.; Maccluer, J.W.; Ali, T.; Lee, E.T.; Yeh, F.L.; et al. Associations of diet soda and non-caloric artificial sweetener use with markers of glucose and insulin homeostasis and incident diabetes: The Strong Heart Family Study. Eur. J. Clin. Nutr. 2020, 74, 322–327. [Google Scholar] [CrossRef]
- Micha, R.; Michas, G.; Mozaffarian, D. Unprocessed red and processed meats and risk of coronary artery disease and type 2 diabetes—An updated review of the evidence. Curr. Atheroscler. Rep. 2012, 14, 515–524. [Google Scholar] [CrossRef]
- Moradi, S.; Hojjati Kermani, M.a.; Bagheri, R.; Mohammadi, H.; Jayedi, A.; Lane, M.M.; Asbaghi, O.; Mehrabani, S.; Suzuki, K. Ultra-Processed Food Consumption and Adult Diabetes Risk: A Systematic Review and Dose-Response Meta-Analysis. Nutrients 2021, 13, 4410. [Google Scholar] [CrossRef] [PubMed]
- Sartorelli, D.S.; Crivellenti, L.C.; Zuccolotto, D.C.C.; Franco, L.J. Relationship between minimally and ultra-processed food intake during pregnancy with obesity and gestational diabetes mellitus. Cad. Saude Publica 2019, 35, e00049318. [Google Scholar] [CrossRef] [PubMed]
- Popkin, B.M. Nutrition Transition and the Global Diabetes Epidemic. Curr. Diab. Rep. 2015, 15, 64. [Google Scholar] [CrossRef] [PubMed]
- Drewnowski, A. The carbohydrate-fat problem: Can we construct a healthy diet based on dietary guidelines? Adv. Nutr. 2015, 6, 318s–325s. [Google Scholar] [CrossRef] [PubMed]
- Zhai, F.; Wang, H.; Du, S.; He, Y.; Wang, Z.; Ge, K.; Popkin, B.M. Prospective study on nutrition transition in China. Nutr. Rev. 2009, 67, S56–S61. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Shi, Z. Dietary Pattern during 1991–2011 and Its Association with Cardio Metabolic Risks in Chinese Adults: The China Health and Nutrition Survey. Nutrients 2017, 9, 1218. [Google Scholar] [CrossRef]
- Li, M.; Shi, Z. Ultra-Processed Food Consumption Associated with Overweight/Obesity among Chinese Adults-Results from China Health and Nutrition Survey 1997–2011. Nutrients 2021, 13, 2796. [Google Scholar] [CrossRef]
- Chinese Center for Disease Control and Prevention. China Health and Nutrition Survey. 2011. Available online: www.cpc.unc.edu/projects/china (accessed on 6 April 2022).
- Popkin, B.M.; Du, S.; Zhai, F.; Zhang, B. Cohort Profile: The China Health and Nutrition Survey--monitoring and understanding socio-economic and health change in China, 1989–2011. Int. J. Epidemiol. 2010, 39, 1435–1440. [Google Scholar] [CrossRef]
- Zhai, F.Y.; Du, S.F.; Wang, Z.H.; Zhang, J.G.; Du, W.W.; Popkin, B.M. Dynamics of the Chinese diet and the role of urbanicity, 1991–2011. Obes. Rev. 2014, 15, 16–26. [Google Scholar] [CrossRef]
- Wang, G. Chinese Food Composition Table 1991; People’s Medical Publishing House: Beijing, China, 1991. [Google Scholar]
- Wolfson, J.A.; Bleich, S.N. Is cooking at home associated with better diet quality or weight-loss intention? Public Health Nutr. 2015, 18, 1397–1406. [Google Scholar] [CrossRef]
- Andrade, G.C.; Gombi-Vaca, M.F.; Louzada, M.; Azeredo, C.M.; Levy, R.B. The consumption of ultra-processed foods according to eating out occasions. Public Health Nutr. 2020, 23, 1041–1048. [Google Scholar] [CrossRef] [PubMed]
- Monteiro, C.A.; Moubarac, J.C.; Cannon, G.; Ng, S.W.; Popkin, B. Ultra-processed products are becoming dominant in the global food system. Obes. Rev. 2013, 14, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Duan, M.J.; Vinke, P.C.; Navis, G.; Corpeleijn, E.; Dekker, L.H. Ultra-processed food and incident type 2 diabetes: Studying the underlying consumption patterns to unravel the health effects of this heterogeneous food category in the prospective Lifelines cohort. BMC Med. 2022, 20, 7. [Google Scholar] [CrossRef] [PubMed]
- Srour, B.; Fezeu, L.K.; Kesse-Guyot, E.; Allès, B.; Debras, C.; Druesne-Pecollo, N.; Chazelas, E.; Deschasaux, M.; Hercberg, S.; Galan, P.; et al. Ultraprocessed Food Consumption and Risk of Type 2 Diabetes Among Participants of the NutriNet-Sante Prospective Cohort. JAMA Intern. Med. 2020, 180, 283–291. [Google Scholar] [CrossRef] [PubMed]
- Llavero-Valero, M.; Escalada-San Martin, J.; Martinez-Gonzalez, M.A.; Basterra-Gortari, F.J.; de la Fuente-Arrillaga, C.; Bes-Rastrollo, M. Ultra-processed foods and type-2 diabetes risk in the SUN project: A prospective cohort study. Clin. Nutr. 2021, 40, 2817–2824. [Google Scholar] [CrossRef] [PubMed]
- Levy, R.B.; Rauber, F.; Chang, K.; da Costa Louzada, M.L.; Monteiro, C.A.; Millett, C.; Vamos, E.P. Ultra-processed food consumption and type 2 diabetes incidence: A prospective cohort study. Clin. Nutr. 2021, 40, 3608–3614. [Google Scholar] [CrossRef]
- Nardocci, M.; Polsky, J.Y.; Moubarac, J.C. Consumption of ultra-processed foods is associated with obesity, diabetes and hypertension in Canadian adults. Can. J. Public Health 2021, 112, 421–429. [Google Scholar] [CrossRef] [PubMed]
- Tappuni, A.R.; Al-Kaabi, R.; Joury, E. Effect of Free Sugars on Diabetes, Obesity, and Dental Caries. J. Dent. Res. 2017, 96, 116. [Google Scholar] [CrossRef] [PubMed]
- Popov, D.; Simionescu, M.; Shepherd, P.R. Saturated-fat diet induces moderate diabetes and severe glomerulosclerosis in hamsters. Diabetologia 2003, 46, 1408–1418. [Google Scholar] [CrossRef] [PubMed]
- Fardet, A. Minimally processed foods are more satiating and less hyperglycemic than ultra-processed foods: A preliminary study with 98 ready-to-eat foods. Food Funct. 2016, 7, 2338–2346. [Google Scholar] [CrossRef] [PubMed]
- Rolls, B.J. The relationship between dietary energy density and energy intake. Physiol. Behav. 2009, 97, 609–615. [Google Scholar] [CrossRef] [PubMed]
- Malone, J.I.; Hansen, B.C. Does obesity cause type 2 diabetes mellitus (T2DM)? Or is it the opposite? Pediatr. Diabetes 2019, 20, 5–9. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Zhang, X.-P.; Yuan, J.; Cai, B.; Wang, X.-L.; Wu, X.-L.; Zhang, Y.-H.; Yin, T.; Zhu, X.-H.; Gu, Y.-J.; et al. Association of body mass index and age with incident diabetes in Chinese adults: A population-based cohort study. BMJ Open 2018, 8, e021768. [Google Scholar] [CrossRef]
- Zhong, Y.; Wu, L.; Chen, X.; Huang, Z.; Hu, W. Effects of Food-Additive-Information on Consumers’ Willingness to Accept Food with Additives. Int. J. Environ. Res. Public Health 2018, 15, 2394. [Google Scholar] [CrossRef]
- Partridge, D.; Lloyd, K.A.; Rhodes, J.M.; Walker, A.W.; Johnstone, A.M.; Campbell, B.J. Food additives: Assessing the impact of exposure to permitted emulsifiers on bowel and metabolic health-introducing the FADiets study. Nutr. Bull. 2019, 44, 329–349. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharyya, S.; Feferman, L.; Unterman, T.; Tobacman, J.K. Exposure to common food additive carrageenan alone leads to fasting hyperglycemia and in combination with high fat diet exacerbates glucose intolerance and hyperlipidemia without effect on weight. J. Diabetes Res. 2015, 2015, 513429. [Google Scholar] [CrossRef] [PubMed]
- Pepino, M.Y.; Tiemann, C.D.; Patterson, B.W.; Wice, B.M.; Klein, S. Sucralose affects glycemic and hormonal responses to an oral glucose load. Diabetes Care 2013, 36, 2530–2535. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.Y.; Lin, Y.C.; Kuo, H.K.; Hwang, J.J.; Lin, J.L.; Chen, P.C.; Lin, L.Y. Association among acrylamide, blood insulin, and insulin resistance in adults. Diabetes Care 2009, 32, 2206–2211. [Google Scholar] [CrossRef]
- Gramec Skledar, D.; Peterlin Mašič, L. Bisphenol A and its analogs: Do their metabolites have endocrine activity? Environ. Toxicol. Pharmacol. 2016, 47, 182–199. [Google Scholar] [CrossRef] [PubMed]
- Gibney, M.J.; Forde, C.G.; Mullally, D.; Gibney, E.R. Ultra-processed foods in human health: A critical appraisal. Am. J. Clin. Nutr. 2017, 106, 717–724. [Google Scholar] [CrossRef]
- Yang, W.; Lu, J.; Weng, J.; Jia, W.; Ji, L.; Xiao, J.; Shan, Z.; Liu, J.; Tian, H.; Ji, Q.; et al. Prevalence of diabetes among men and women in China. N. Engl. J. Med. 2010, 362, 1090–1101. [Google Scholar] [CrossRef]
- Zuo, H.; Shi, Z.; Hussain, A. Prevalence, trends and risk factors for the diabetes epidemic in China: A systematic review and meta-analysis. Diabetes Res. Clin. Pract. 2014, 104, 63–72. [Google Scholar] [CrossRef]
- Shen, X.; Vaidya, A.; Wu, S.; Gao, X. The Diabetes Epidemic in China: An Integrated Review of National Surveys. Endocr. Pract. 2016, 22, 1119–1129. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Yuan, Y.C.; Guo, M.N.; Xin, Z.; Chen, G.J.; Bentley, A.R.; Hua, L.; Zheng, J.P.; Ekoru, K.; Yang, J.K. Incidence of Type 1 Diabetes May Be Underestimated in the Chinese Population: Evidence From 21.7 Million People Between 2007 and 2017. Diabetes Care 2021, 44, 2503–2509. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| None | 1–19 g/d | 20–49 g/d | ≥50 g/d | p-Value | |
|---|---|---|---|---|---|
| N | n = 10,129 | n = 616 | n = 708 | n = 1396 | |
| Survey year at entry | <0.001 | ||||
| 1997 | 58.7% | 63.6% | 48.2% | 39.9% | |
| 2000 | 16.4% | 13.3% | 15.3% | 15.9% | |
| 2004 | 12.4% | 11.5% | 12.9% | 12.0% | |
| 2006 | 5.0% | 3.4% | 9.9% | 9.7% | |
| 2009 | 7.5% | 8.1% | 13.8% | 22.6% | |
| Age, mean (years) | 43.2 (14.7) | 43.7 (15.9) | 43.2 (15.2) | 44.2 (14.7) | 0.091 |
| Sex | <0.001 | ||||
| Men | 46.8% | 44.2% | 50.8% | 66.0% | |
| Women | 53.2% | 55.8% | 49.2% | 34.0% | |
| Income | <0.001 | ||||
| Low | 31.7% | 24.2% | 20.3% | 21.8% | |
| Medium | 33.2% | 34.5% | 32.2% | 31.6% | |
| High | 35.0% | 41.3% | 47.5% | 46.7% | |
| Education | <0.001 | ||||
| Low | 47.5% | 42.6% | 30.9% | 33.5% | |
| Medium | 32.0% | 33.0% | 32.7% | 30.8% | |
| High | 20.4% | 24.4% | 36.4% | 35.7% | |
| Urbanization | <0.001 | ||||
| Low | 36.4% | 28.2% | 19.8% | 20.5% | |
| Medium | 30.1% | 26.9% | 25.3% | 28.2% | |
| High | 33.5% | 44.8% | 54.9% | 51.4% | |
| Energy intake, mean (kcal/d) | 2242.9 (633.1) | 2153.6 (595.6) | 2214.7 (600.3) | 2480.9 (702.5) | <0.001 |
| Percent (%) of UPF over total energy intake/d | 0.0 (0.0) | 1.6 (1.5) | 4.9 (2.8) | 14.3 (11.1) | <0.001 |
| Percent (%) of UPF over total food intake/d | 0.0 (0.0) | 1.2 (0.7) | 3.2 (1.2) | 10.4 (6.8) | <0.001 |
| Fat intake, mean (g/d) | 65.3 (35.7) | 65.3 (33.7) | 75.6 (35.7) | 82.1 (39.9) | <0.001 |
| Protein intake, mean (g/d) | 67.5 (22.1) | 67.5 (21.7) | 71.1 (22.9) | 76.6 (25.0) | <0.001 |
| Carbohydrate intake, mean (g/d) | 345.7 (120.6) | 322.2 (114.2) | 308.7 (112.0) | 323.1 (113.6) | <0.001 |
| Traditional dietary pattern score, mean | −0.0 (1.0) | 0.1 (0.9) | 0.1 (1.0) | 0.1 (1.0) | <0.001 |
| Modern dietary pattern score, mean | −0.3 (0.7) | −0.2 (0.8) | 0.2 (1.0) | 0.7 (1.2) | <0.001 |
| Smoking | <0.001 | ||||
| Non smoker | 69.1% | 69.8% | 66.1% | 53.5% | |
| Ex-smokers | 1.3% | 1.0% | 2.1% | 3.0% | |
| Current smokers | 29.6% | 29.3% | 31.8% | 43.5% | |
| Alcohol drinking | 32.1% | 34.5% | 39.8% | 57.8% | <0.001 |
| Physical activity, mean (MET-hrs/week) | 141.0 (117.0) | 135.6 (117.2) | 132.2 (112.5) | 143.1 (118.9) | 0.15 |
| BMI (kg/m2), mean (SD) | 22.6 (3.2) | 22.8 (3.3) | 23.1 (3.3) | 23.0 (3.3) | <0.001 |
| Diabetes | 2.0% | 1.3% | 2.5% | 2.8% | 0.087 |
| Hypertension | 15.1% | 19.4% | 16.5% | 19.5% | <0.001 |
| Cumulative UPF Intake (g/day) | |||||
|---|---|---|---|---|---|
| None | 1–19 | 20–49 | ≥50 | p for Trend | |
| Unadjusted | 1.00 | 2.13 (1.76–2.56) | 2.79 (2.29–3.40) | 2.60 (2.10–3.23) | <0.001 |
| Model 1 | 1.00 | 1.53 (1.27–1.85) | 2.15 (1.76–2.64) | 2.21 (1.76–2.77) | <0.001 |
| Model 2 | 1.00 | 1.34 (1.09–1.65) | 1.87 (1.50–2.34) | 1.96 (1.53–2.51) | <0.001 |
| Model 3 | 1.00 | 1.29 (1.05–1.58) | 1.79 (1.43–2.23) | 1.85 (1.45–2.36) | <0.001 |
| Model 4 | 1.00 | 1.29 (1.05–1.58) | 1.74 (1.40–2.17) | 1.79 (1.40–2.29) | <0.001 |
| Model 5 | 1.00 | 1.21 (0.98–1.48) | 1.49 (1.19–1.86) | 1.40 (1.08–1.80) | <0.001 |
| Model 6 | 1.00 | 1.22 (0.97–1.53) | 1.55 (1.20–2.00) | 1.37 (1.00–1.88) | 0.003 |
| None | 1–19 g/d | 20–49 g/d | ≥50 g/d | p for Trend | |
|---|---|---|---|---|---|
| n = 3764 | n = 1947 | n = 1323 | n = 1348 | ||
| Diabetes cases | 364 | 227 | 169 | 180 | <0.001 |
| Unadjusted | 1.00 | 1.23 (1.03–1.66) | 1.37 (1.13–1.66) | 1.44 (1.19–1.74) | 0.003 |
| Model 1 | 1.00 | 1.10 (0.92–1.31) | 1.27 (1.04–1.55) | 1.46 (1.19–1.77) | <0.001 |
| Model 2 | 1.00 | 1.05 (0.86–1.28) | 1.21 (0.96–1.51) | 1.31 (1.04–1.65) | 0.015 |
| Model 3 | 1.00 | 1.07 (0.87–1.31) | 1.16 (0.92–1.46) | 1.24 (0.97–1.57) | 0.060 |
| Sensitivity analysis | 1.00 | 1.16 (0.79–1.68) | 0.85 (0.62–1.15) | 1.23 (1.01–1.50) | 0.037 |
| Cumulative UPF Intake (g/day) | ||||||
|---|---|---|---|---|---|---|
| None | 1–19 | 20–49 | ≥50 | p Value | p Interaction | |
| Sex | 0.637 | |||||
| Men | 1.00 | 1.51 (1.10–2.09) | 2.00 (1.45–2.76) | 2.22 (1.60–3.09) | <0.001 | |
| Women | 1.00 | 1.23 (0.94–1.61) | 1.82 (1.34–2.49) | 1.78 (1.21–2.61) | <0.001 | |
| Education | 0.146 | |||||
| Low | 1.00 | 1.59 (1.21–2.10) | 2.62 (1.90–3.61) | 2.22 (1.50–3.30) | <0.001 | |
| Medium | 1.00 | 0.95 (0.63–1.45) | 1.51 (0.98–2.32) | 1.77 (1.11–2.80) | 0.008 | |
| High | 1.00 | 1.03 (0.65–1.63) | 1.12 (0.70–1.79) | 1.39 (0.86–2.25) | 0.195 | |
| Income | 0.475 | |||||
| Low | 1.00 | 1.14 (0.80–1.64) | 2.25 (1.50–3.37) | 2.11 (1.32–3.38) | <0.001 | |
| Medium | 1.00 | 1.25 (0.89–1.76) | 1.40 (0.94–2.10) | 1.56 (1.00–2.45) | 0.020 | |
| High | 1.00 | 1.34 (0.94–1.91) | 1.99 (1.38–2.85) | 2.02 (1.37–2.98) | <0.001 | |
| Urbanization | 0.469 | |||||
| Low | 1.00 | 1.12 (0.71–1.77) | 1.34 (0.73–2.45) | 1.36 (0.69–2.68) | 0.223 | |
| Medium | 1.00 | 1.45 (1.00–2.11) | 1.88 (1.24–2.83) | 2.49 (1.61–3.85) | <0.001 | |
| High | 1.00 | 1.24 (0.93–1.67) | 1.99 (1.45–2.71) | 1.81 (1.27–2.57) | <0.001 | |
| Smoking | 0.987 | |||||
| Non smoker | 1.00 | 1.37 (1.08–1.73) | 1.99 (1.52–2.61) | 2.18 (1.61–2.97) | <0.001 | |
| Current smokers | 1.00 | 1.29 (0.86–1.93) | 1.56 (1.04–2.35) | 1.68 (1.11–2.52) | 0.006 | |
| Overweight/obesity | 0.366 | |||||
| No | 1.00 | 1.14 (0.85–1.53) | 1.77 (1.29–2.43) | 1.70 (1.19–2.41) | <0.001 | |
| Yes | 1.00 | 1.43 (1.06–1.92) | 1.72 (1.24–2.38) | 1.91 (1.35–2.71) | <0.001 | |
| Hypertension | 0.684 | |||||
| No | 1.00 | 1.19 (0.90–1.56) | 1.61 (1.19–2.16) | 1.77 (1.28–2.43) | <0.001 | |
| Yes | 1.00 | 1.34 (1.00–1.79) | 1.94 (1.41–2.66) | 1.87 (1.32–2.66) | <0.001 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, M.; Shi, Z. Association between Ultra-Processed Food Consumption and Diabetes in Chinese Adults—Results from the China Health and Nutrition Survey. Nutrients 2022, 14, 4241. https://doi.org/10.3390/nu14204241
Li M, Shi Z. Association between Ultra-Processed Food Consumption and Diabetes in Chinese Adults—Results from the China Health and Nutrition Survey. Nutrients. 2022; 14(20):4241. https://doi.org/10.3390/nu14204241
Chicago/Turabian StyleLi, Ming, and Zumin Shi. 2022. "Association between Ultra-Processed Food Consumption and Diabetes in Chinese Adults—Results from the China Health and Nutrition Survey" Nutrients 14, no. 20: 4241. https://doi.org/10.3390/nu14204241
APA StyleLi, M., & Shi, Z. (2022). Association between Ultra-Processed Food Consumption and Diabetes in Chinese Adults—Results from the China Health and Nutrition Survey. Nutrients, 14(20), 4241. https://doi.org/10.3390/nu14204241