
Low-Glycemic Index Diets as an Intervention in Metabolic Diseases: A Systematic Review and Meta-Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. PRISMA Guidelines
2.2. Data Sources and Search Strategy
2.3. Eligibility Criteria
2.4. Study Selection
2.5. Study Quality
2.6. Data Extraction
2.7. Statistical Synthesis and Analysis
3. Results
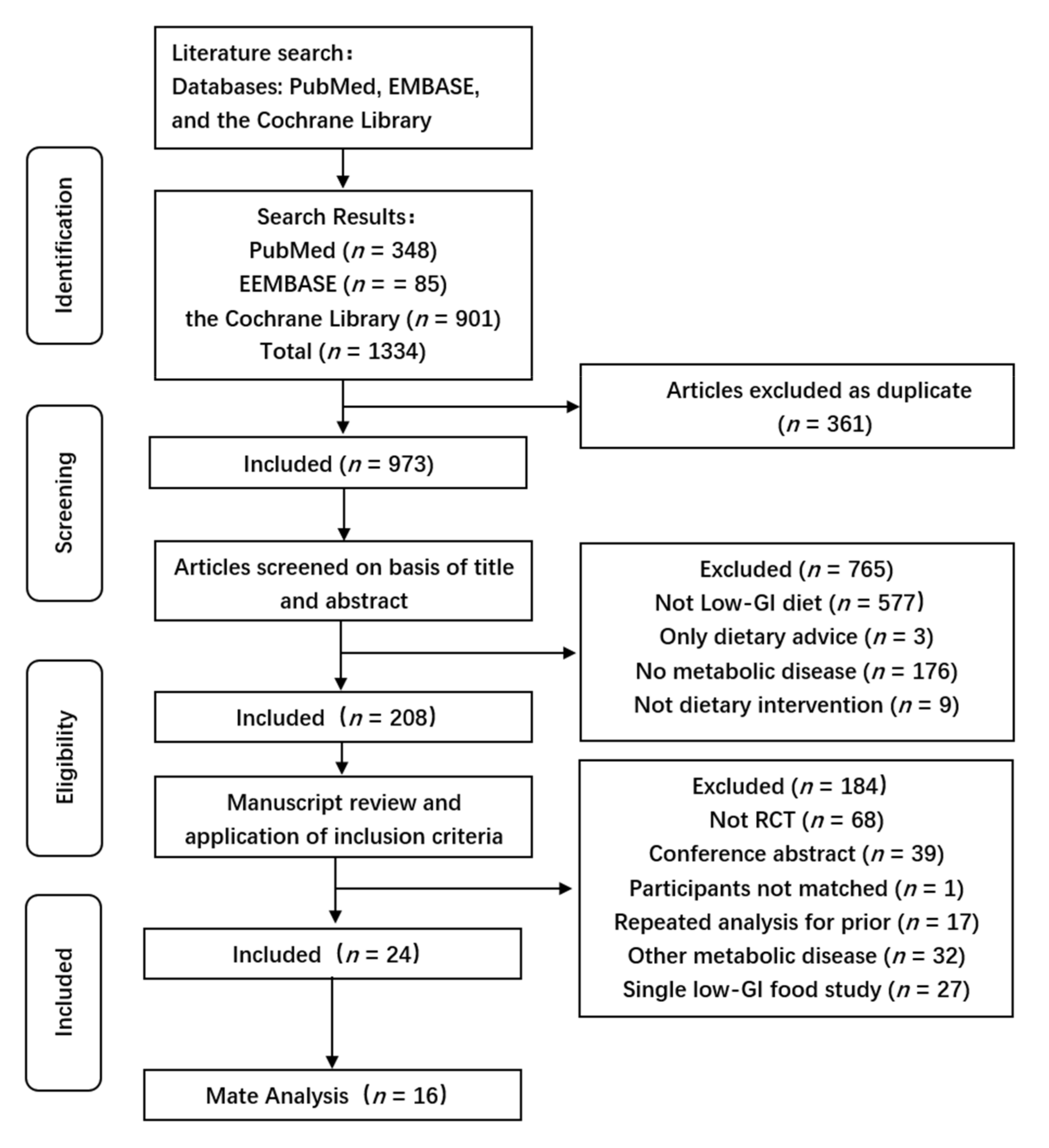
3.1. Results of the Literature Searches
3.2. Characteristics of the Included Studies
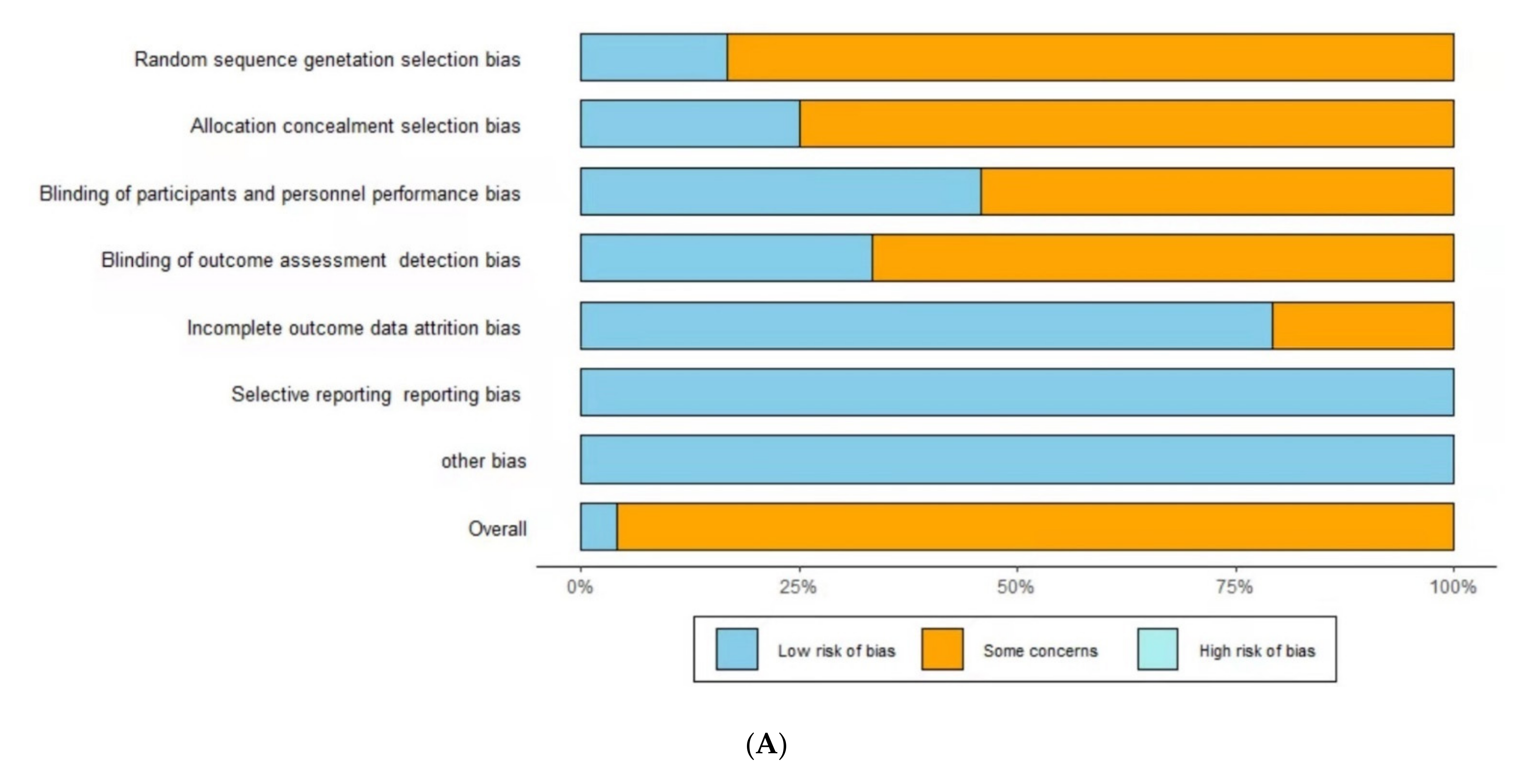
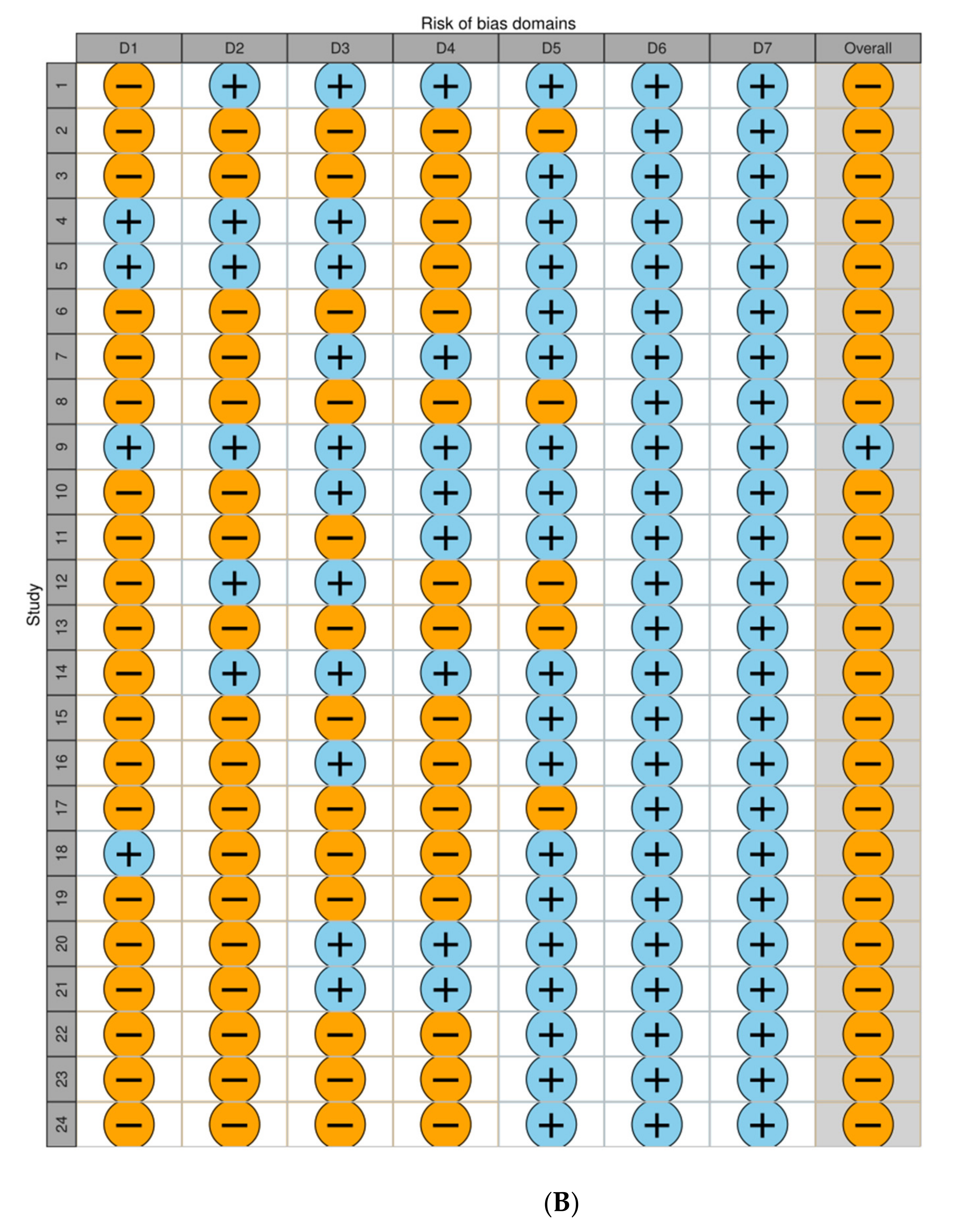
3.3. Quality of the Included Studies
3.4. Body Mass
3.5. BMI
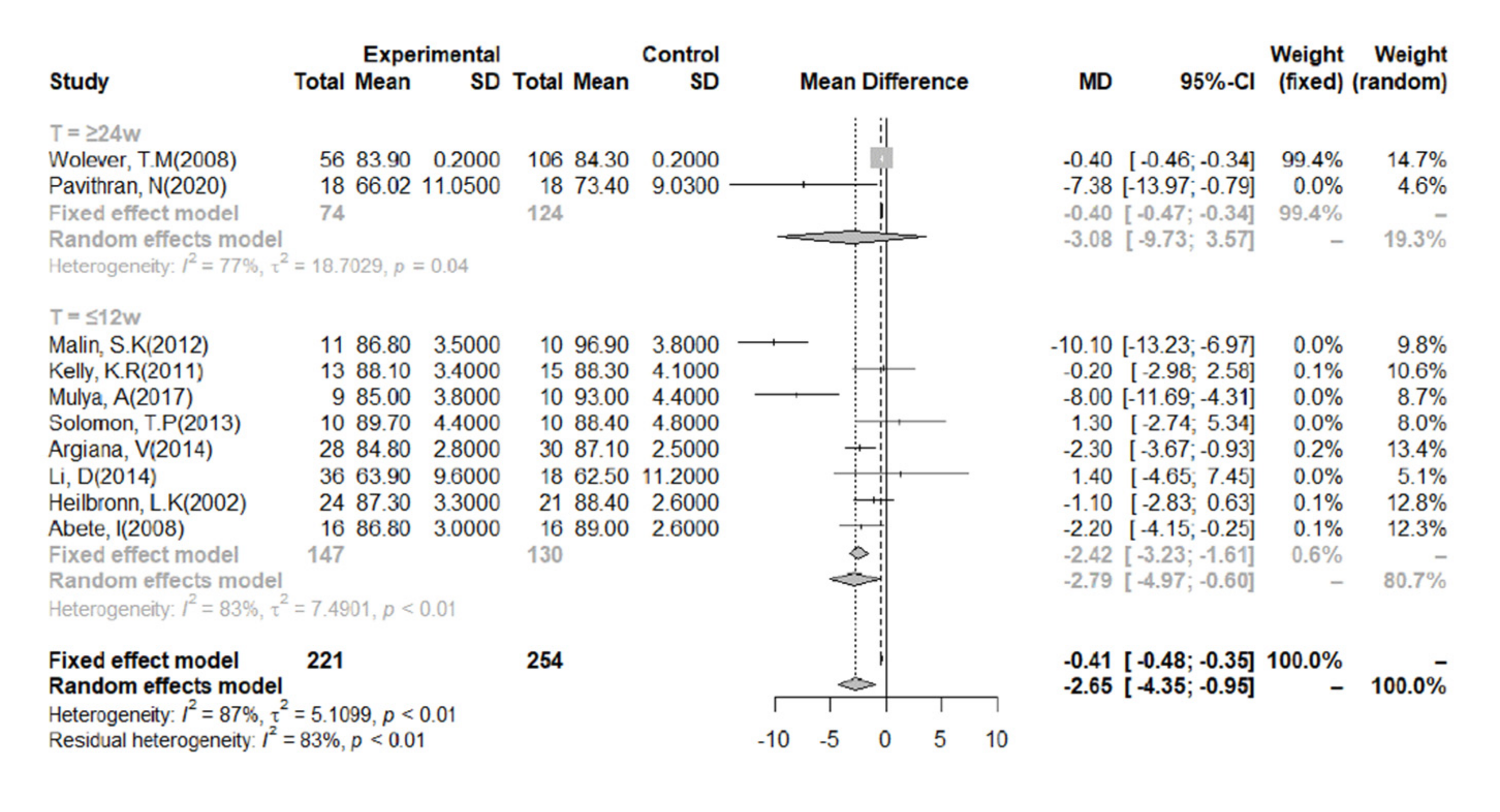
3.6. FBG
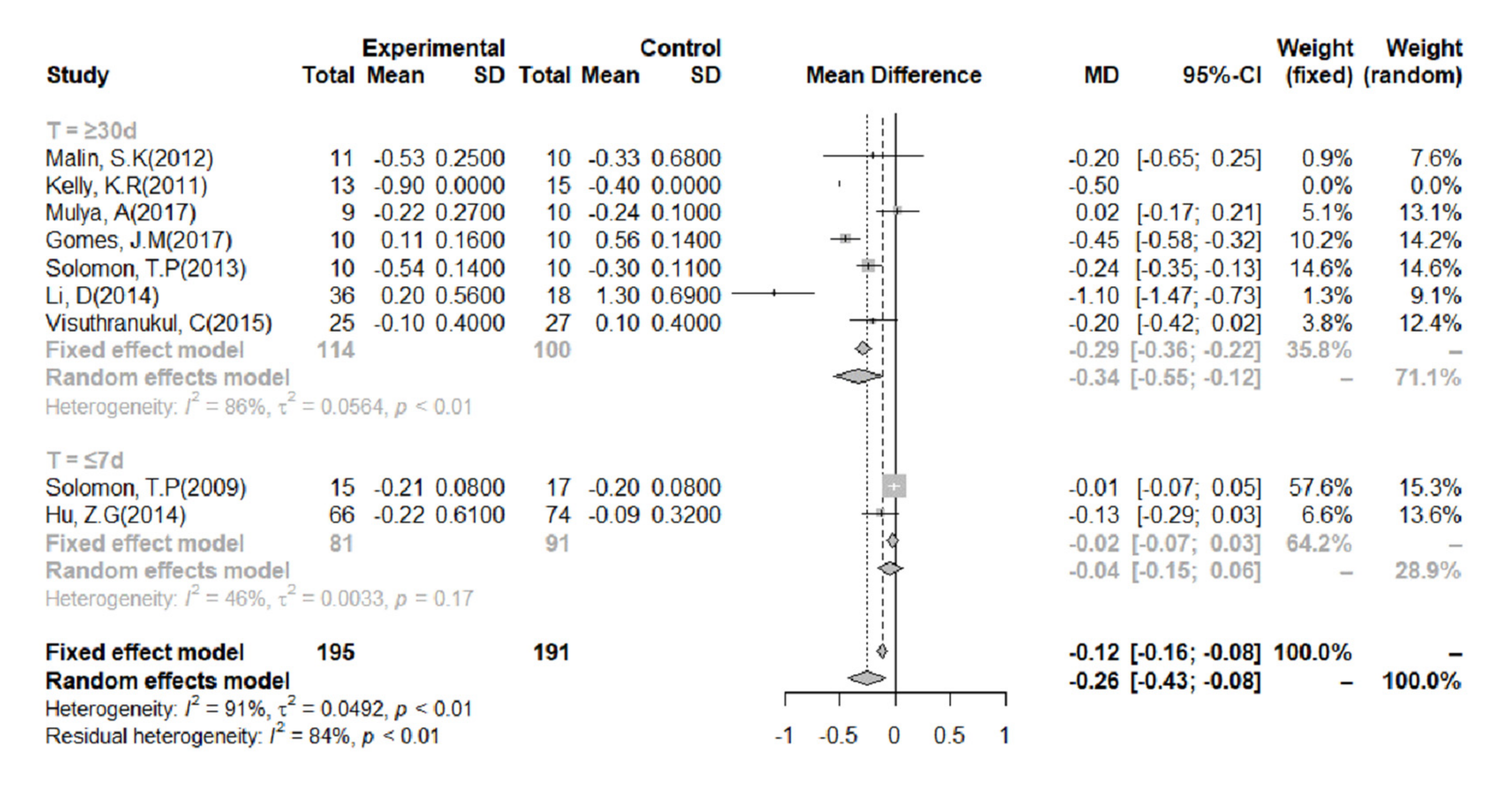
3.7. HbA1c%
4. Discussion
Strengths and Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Roth, G.A.; Mensah, G.A.; Johnson, C.O.; Addolorato, G.; Ammirati, E.; Baddour, L.M.; Barengo, N.C.; Beaton, A.Z.; Benjamin, E.J.; Benziger, C.P.; et al. Global Burden of Cardiovascular Diseases and Risk Factors, 1990–2019: Update From the GBD 2019 Study. J. Am. Coll. Cardiol. 2020, 76, 2982–3021. [Google Scholar] [CrossRef] [PubMed]
- GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef]
- Bommer, C.; Sagalova, V.; Heesemann, E.; Manne-Goehler, J.; Atun, R.; Bärnighausen, T.; Davies, J.; Vollmer, S. Global Economic Burden of Diabetes in Adults: Projections From 2015 to 2030. Diabetes Care 2018, 41, 963–970. [Google Scholar] [CrossRef] [Green Version]
- Saklayen, M.G. The Global Epidemic of the Metabolic Syndrome. Curr. Hypertens. Rep. 2018, 20, 12. [Google Scholar] [CrossRef] [Green Version]
- Kelly, T.; Yang, W.; Chen, C.S.; Reynolds, K.; He, J. Global burden of obesity in 2005 and projections to 2030. Int. J. Obes. 2008, 32, 1431–1437. [Google Scholar] [CrossRef] [Green Version]
- Kim, K.H.; Lee, M.S. Autophagy—A key player in cellular and body metabolism. Nat. Rev. Endocrinol. 2014, 10, 322–337. [Google Scholar] [CrossRef]
- Wilson, P.W.; D’Agostino, R.B.; Sullivan, L.; Parise, H.; Kannel, W.B. Overweight and obesity as determinants of cardiovascular risk: The Framingham experience. Arch. Intern. Med. 2002, 162, 1867–1872. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jenkins, D.J.; Wolever, T.M.; Taylor, R.H.; Barker, H.; Fielden, H.; Baldwin, J.M.; Bowling, A.C.; Newman, H.C.; Jenkins, A.L.; Goff, D.V. Glycemic index of foods: A physiological basis for carbohydrate exchange. Am. J. Clin. Nutr. 1981, 34, 362–366. [Google Scholar] [CrossRef] [Green Version]
- Eleazu, C.O. The concept of low glycemic index and glycemic load foods as panacea for type 2 diabetes mellitus; prospects, challenges and solutions. Afr. Health Sci. 2016, 16, 468–479. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vega-López, S.; Venn, B.J.; Slavin, J.L. Relevance of the Glycemic Index and Glycemic Load for Body Weight, Diabetes, and Cardiovascular Disease. Nutrients 2018, 10, 1361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiu, C.J.; Taylor, A. Dietary hyperglycemia, glycemic index and metabolic retinal diseases. Prog. Retin. Eye Res. 2011, 30, 18–53. [Google Scholar] [CrossRef] [Green Version]
- Jenkins, D.J.; Kendall, C.W.; Augustin, L.S.; Franceschi, S.; Hamidi, M.; Marchie, A.; Jenkins, A.L.; Axelsen, M. Glycemic index: Overview of implications in health and disease. Am. J. Clin. Nutr. 2002, 76, 266S–273S. [Google Scholar] [CrossRef]
- Devlin, B.L.; Parr, E.B.; Radford, B.E.; Hawley, J.A. Lower nocturnal blood glucose response to a potato-based mixed evening meal compared to rice in individuals with type 2 diabetes. Clin. Nutr. 2021, 40, 2200–2209. [Google Scholar] [CrossRef] [PubMed]
- Abete, I.; Parra, D.; Martinez, J.A. Energy-restricted diets based on a distinct food selection affecting the glycemic index induce different weight loss and oxidative response. Clin. Nutr. 2008, 27, 545–551. [Google Scholar] [CrossRef] [Green Version]
- Mulya, A.; Haus, J.M.; Solomon, T.P.J.; Kelly, K.R.; Malin, S.K.; Rocco, M.; Barkoukis, H.; Kirwan, J.P. Exercise training-induced improvement in skeletal muscle PGC-1alpha-mediated fat metabolism is independent of dietary glycemic index. Obesity 2017, 25, 721–729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, Z.G.; Tan, R.S.; Jin, D.; Li, W.; Zhou, X.Y. A low glycemic index staple diet reduces postprandial glucose values in Asian women with gestational diabetes mellitus. J. Investig. Med. 2014, 62, 975–979. [Google Scholar] [CrossRef]
- Heilbronn, L.K.; Noakes, M.; Clifton, P.M. The effect of high- and low-glycemic index energy restricted diets on plasma lipid and glucose profiles in type 2 diabetic subjects with varying glycemic control. J. Am. Coll. Nutr. 2002, 21, 120–127. [Google Scholar] [CrossRef]
- Livesey, G.; Taylor, R.; Livesey, H.F.; Buyken, A.E.; Jenkins, D.J.A.; Augustin, L.S.A.; Sievenpiper, J.L.; Barclay, A.W.; Liu, S.; Wolever, T.M.S.; et al. Dietary Glycemic Index and Load and the Risk of Type 2 Diabetes: A Systematic Review and Updated Meta-Analyses of Prospective Cohort Studies. Nutrients 2019, 11, 1280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ojo, O.; Ojo, O.O.; Adebowale, F.; Wang, X.H. The Effect of Dietary Glycaemic Index on Glycaemia in Patients with Type 2 Diabetes: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrients 2018, 10, 373. [Google Scholar] [CrossRef] [Green Version]
- Thomas, D.; Elliott, E.J. Low glycaemic index, or low glycaemic load, diets for diabetes mellitus. Cochrane Database Syst. Rev. 2009, 2009, Cd006296. [Google Scholar] [CrossRef]
- Schwingshackl, L.; Hoffmann, G. Long-term effects of low glycemic index/load vs. high glycemic index/load diets on parameters of obesity and obesity-associated risks: A systematic review and meta-analysis. Nutr. Metab. Cardiovasc. Dis. NMCD 2013, 23, 699–706. [Google Scholar] [CrossRef]
- Askari, M.; Dehghani, A.; Abshirini, M.; Raeisi, T.; Alizadeh, S. Glycemic index, but not glycemic load, is associated with an increased risk of metabolic syndrome: Meta-analysis of observational studies. Int. J. Clin. Pract. 2021, 75, e14295. [Google Scholar] [CrossRef]
- Mirrahimi, A.; de Souza, R.J.; Chiavaroli, L.; Sievenpiper, J.L.; Beyene, J.; Hanley, A.J.; Augustin, L.S.; Kendall, C.W.; Jenkins, D.J. Associations of glycemic index and load with coronary heart disease events: A systematic review and meta-analysis of prospective cohorts. J. Am. Heart Assoc. 2012, 1, e000752. [Google Scholar] [CrossRef] [Green Version]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jenkins, D.J.; Kendall, C.W.; McKeown-Eyssen, G.; Josse, R.G.; Silverberg, J.; Booth, G.L.; Vidgen, E.; Josse, A.R.; Nguyen, T.H.; Corrigan, S.; et al. Effect of a low-glycemic index or a high-cereal fiber diet on type 2 diabetes: A randomized trial. JAMA 2008, 300, 2742–2753. [Google Scholar] [CrossRef] [Green Version]
- Turner-McGrievy, G.M.; Jenkins, D.J.; Barnard, N.D.; Cohen, J.; Gloede, L.; Green, A.A. Decreases in dietary glycemic index are related to weight loss among individuals following therapeutic diets for type 2 diabetes. J. Nutr. 2011, 141, 1469–1474. [Google Scholar] [CrossRef] [PubMed]
- Ebbeling, C.B.; Leidig, M.M.; Sinclair, K.B.; Hangen, J.P.; Ludwig, D.S. A reduced-glycemic load diet in the treatment of adolescent obesity. Arch. Pediatrics Adolesc. Med. 2003, 157, 773–779. [Google Scholar] [CrossRef]
- Wolever, T.M.; Gibbs, A.L.; Mehling, C.; Chiasson, J.L.; Connelly, P.W.; Josse, R.G.; Leiter, L.A.; Maheux, P.; Rabasa-Lhoret, R.; Rodger, N.W.; et al. The Canadian Trial of Carbohydrates in Diabetes (CCD), a 1-y controlled trial of low-glycemic-index dietary carbohydrate in type 2 diabetes: No effect on glycated hemoglobin but reduction in C-reactive protein. Am. J. Clin. Nutr. 2008, 87, 114–125. [Google Scholar] [CrossRef] [Green Version]
- Wolever, T.M.; Mehling, C.; Chiasson, J.L.; Josse, R.G.; Leiter, L.A.; Maheux, P.; Rabasa-Lhoret, R.; Rodger, N.W.; Ryan, E.A. Low glycaemic index diet and disposition index in type 2 diabetes (the Canadian trial of carbohydrates in diabetes): A randomised controlled trial. Diabetologia 2008, 51, 1607–1615. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malin, S.K.; Niemi, N.; Solomon, T.P.; Haus, J.M.; Kelly, K.R.; Filion, J.; Rocco, M.; Kashyap, S.R.; Barkoukis, H.; Kirwan, J.P. Exercise training with weight loss and either a high- or low-glycemic index diet reduces metabolic syndrome severity in older adults. Ann. Nutr. Metab. 2012, 61, 135–141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kelly, K.R.; Haus, J.M.; Solomon, T.P.; Patrick-Melin, A.J.; Cook, M.; Rocco, M.; Barkoukis, H.; Kirwan, J.P. A low-glycemic index diet and exercise intervention reduces TNF(alpha) in isolated mononuclear cells of older, obese adults. J. Nutr. 2011, 141, 1089–1094. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Osella, A.R.; Colaianni, G.; Correale, M.; Pesole, P.L.; Bruno, I.; Buongiorno, C.; Deflorio, V.; Leone, C.M.; Colucci, S.C.; Grano, M.; et al. Irisin Serum Levels in Metabolic Syndrome Patients Treated with Three Different Diets: A Post-Hoc Analysis from a Randomized Controlled Clinical Trial. Nutrients 2018, 10, 844. [Google Scholar] [CrossRef] [Green Version]
- Gomes, J.M.G.; Fabrini, S.P.; Alfenas, R.C.G. Low glycemic index diet reduces body fat and attenuates inflammatory and metabolic responses in patients with type 2 diabetes. Arch. Endocrinol. Metab. 2017, 61, 137–144. [Google Scholar] [CrossRef] [Green Version]
- Solomon, T.P.; Haus, J.M.; Kelly, K.R.; Cook, M.D.; Riccardi, M.; Rocco, M.; Kashyap, S.R.; Barkoukis, H.; Kirwan, J.P. Randomized trial on the effects of a 7-d low-glycemic diet and exercise intervention on insulin resistance in older obese humans. Am. J. Clin. Nutr. 2009, 90, 1222–1229. [Google Scholar] [CrossRef]
- Fraser, A.; Abel, R.; Lawlor, D.A.; Fraser, D.; Elhayany, A. A modified Mediterranean diet is associated with the greatest reduction in alanine aminotransferase levels in obese type 2 diabetes patients: Results of a quasi-randomised controlled trial. Diabetologia 2008, 51, 1616–1622. [Google Scholar] [CrossRef] [Green Version]
- Visuthranukul, C.; Sirimongkol, P.; Prachansuwan, A.; Pruksananonda, C.; Chomtho, S. Low-glycemic index diet may improve insulin sensitivity in obese children. Pediatric Res. 2015, 78, 567–573. [Google Scholar] [CrossRef] [Green Version]
- Jenkins, D.J.; Srichaikul, K.; Kendall, C.W.; Sievenpiper, J.L.; Abdulnour, S.; Mirrahimi, A.; Meneses, C.; Nishi, S.; He, X.; Lee, S.; et al. The relation of low glycaemic index fruit consumption to glycaemic control and risk factors for coronary heart disease in type 2 diabetes. Diabetologia 2011, 54, 271–279. [Google Scholar] [CrossRef] [Green Version]
- Pavithran, N.; Kumar, H.; Menon, A.S.; Pillai, G.K.; Sundaram, K.R.; Ojo, O. The Effect of a Low GI Diet on Truncal Fat Mass and Glycated Hemoglobin in South Indians with Type 2 Diabetes-A Single Centre Randomized Prospective Study. Nutrients 2020, 12, 179. [Google Scholar] [CrossRef] [Green Version]
- Solomon, T.P.; Haus, J.M.; Cook, M.A.; Flask, C.A.; Kirwan, J.P. A low-glycemic diet lifestyle intervention improves fat utilization during exercise in older obese humans. Obesity 2013, 21, 2272–2278. [Google Scholar] [CrossRef]
- Fabricatore, A.N.; Wadden, T.A.; Ebbeling, C.B.; Thomas, J.G.; Stallings, V.A.; Schwartz, S.; Ludwig, D.S. Targeting dietary fat or glycemic load in the treatment of obesity and type 2 diabetes: A randomized controlled trial. Diabetes Res. Clin. Pract. 2011, 92, 37–45. [Google Scholar] [CrossRef] [Green Version]
- Argiana, V.; Kanellos, P.; Makrilakis, K.; Eleftheriadou, I.; Tsitsinakis, G.; Kokkinos, A.; Perrea, D.; Tentolouris, N. The effect of consumption of low-glycemic-index and low-glycemic-load desserts on anthropometric parameters and inflammatory markers in patients with type 2 diabetes mellitus. Eur. J. Nutr. 2015, 54, 1173–1180. [Google Scholar] [CrossRef]
- Li, D.; Zhang, P.; Guo, H.; Ling, W. Taking a low glycemic index multi-nutrient supplement as breakfast improves glycemic control in patients with type 2 diabetes mellitus: A randomized controlled trial. Nutrients 2014, 6, 5740–5755. [Google Scholar] [CrossRef] [Green Version]
- Mirza, N.M.; Klein, C.J.; Palmer, M.G.; McCarter, R.; He, J.; Ebbeling, C.B.; Ludwig, D.S.; Yanovski, J.A. Effects of high and low glycemic load meals on energy intake, satiety and hunger in obese Hispanic-American youth. Int. J. Pediatric Obes. IJPO 2011, 6, e523–e531. [Google Scholar] [CrossRef] [Green Version]
- Basharat, S.; Gilani, S.A.; Burq, A.I.; Bashir, S. Low glycaemic index diet is effective in managing weight among obese postpartum women. JPMA J. Pak. Med. Assoc. 2018, 68, 548–553. [Google Scholar] [PubMed]
- Chiavaroli, L.; Kendall, C.W.C.; Braunstein, C.R.; Blanco Mejia, S.; Leiter, L.A.; Jenkins, D.J.A.; Sievenpiper, J.L. Effect of pasta in the context of low-glycaemic index dietary patterns on body weight and markers of adiposity: A systematic review and meta-analysis of randomised controlled trials in adults. BMJ Open 2018, 8, e019438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zafar, M.I.; Mills, K.E.; Zheng, J.; Peng, M.M.; Ye, X.; Chen, L.L. Low glycaemic index diets as an intervention for obesity: A systematic review and meta-analysis. Obes. Rev. Off. J. Int. Assoc. Study Obes. 2019, 20, 290–315. [Google Scholar] [CrossRef]
- Maki, K.C.; Rains, T.M.; Kaden, V.N.; Raneri, K.R.; Davidson, M.H. Effects of a reduced-glycemic-load diet on body weight, body composition, and cardiovascular disease risk markers in overweight and obese adults. Am. J. Clin. Nutr. 2007, 85, 724–734. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Livesey, G.; Taylor, R.; Livesey, H.F.; Buyken, A.E.; Jenkins, D.J.A.; Augustin, L.S.A.; Sievenpiper, J.L.; Barclay, A.W.; Liu, S.; Wolever, T.M.S.; et al. Dietary Glycemic Index and Load and the Risk of Type 2 Diabetes: Assessment of Causal Relations. Nutrients 2019, 11, 1436. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wan, C.S.; Nankervis, A.; Teede, H.; Aroni, R. Dietary intervention strategies for ethnic Chinese women with gestational diabetes mellitus: A systematic review and meta-analysis. Nutr. Diet. J. Dietit. Assoc. Aust. 2019, 76, 211–232. [Google Scholar] [CrossRef]
- Gilbertson, H.R.; Brand-Miller, J.C.; Thorburn, A.W.; Evans, S.; Chondros, P.; Werther, G.A. The effect of flexible low glycemic index dietary advice versus measured carbohydrate exchange diets on glycemic control in children with type 1 diabetes. Diabetes Care 2001, 24, 1137–1143. [Google Scholar] [CrossRef] [Green Version]
- Esfahani, A.; Wong, J.M.; Mirrahimi, A.; Villa, C.R.; Kendall, C.W. The application of the glycemic index and glycemic load in weight loss: A review of the clinical evidence. IUBMB Life 2011, 63, 7–13. [Google Scholar] [CrossRef]
- Zafar, M.I.; Mills, K.E.; Zheng, J.; Regmi, A.; Hu, S.Q.; Gou, L.; Chen, L.L. Low-glycemic index diets as an intervention for diabetes: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2019, 110, 891–902. [Google Scholar] [CrossRef] [PubMed]
- Miller, C.K.; Headings, A.; Peyrot, M.; Nagaraja, H. A behavioural intervention incorporating specific glycaemic index goals improves dietary quality, weight control and glycaemic control in adults with type 2 diabetes. Public Health Nutr. 2011, 14, 1303–1311. [Google Scholar] [CrossRef] [PubMed]
- Nutrition and Metabolic Management Branch of China Association for the Promotion of International Exchanges in Healthcare; Clinical Nutrition Branch of Chinese Nutrition Society; Diabetes Branch of Chinese Medical Association; Parenteral and Enteral Nutrition Branch of Chinese Medical Association; Nutrition Physician Professional Committee of Chinese Medical Doctor Association. Guidelines for Medical Nutritional Treatment of Overweight/Obesity in China (2021). Chin. J. Front. Med. 2021, 13, 1–55. [Google Scholar] [CrossRef]
- Thomas, D.E.; Elliott, E.J. The use of low-glycaemic index diets in diabetes control. Br. J. Nutr. 2010, 104, 797–802. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ebbeling, C.B.; Swain, J.F.; Feldman, H.A.; Wong, W.W.; Hachey, D.L.; Garcia-Lago, E.; Ludwig, D.S. Effects of dietary composition on energy expenditure during weight-loss maintenance. JAMA 2012, 307, 2627–2634. [Google Scholar] [CrossRef] [Green Version]
- Hare-Bruun, H.; Nielsen, B.M.; Grau, K.; Oxlund, A.L.; Heitmann, B.L. Should glycemic index and glycemic load be considered in dietary recommendations? Nutr. Rev. 2008, 66, 569–590. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author (Year) | Country | Diabetes Type | N | N Int. | N Con. | Gender Ratio (F:M) | BMI | Average Age (Year) | FBG (mmol/L) |
|---|---|---|---|---|---|---|---|---|---|
| Jenkins, D.J (2008) [27] | Canada | T2DM | 210 | 106 | 104 | 0.6 | 30.9 | 60.5 | NS |
| Turner-McGrievy (2011) [28] | USA | T2DM | 99 | 49 | 50 | 1.5 | 34.8 | 55.2 | NS |
| Ebbeling, C.B (2003) [29] | USA | adiposity | 14 | 7 | 7 | 2.2 | 36.0 | 16.1 | NS |
| Wolever, T.M (2008) [30] | Canada | T2DM | 162 | 56 | 106 | 1.2 | 31.0 | 59.9 | 7.4 |
| Wolever, T.M (2008) [31] | Canada | T2DM | 135 | 46 | 89 | 1.2 | 31.0 | 59.7 | 7.3 |
| Malin, S.K (2012) [32] | USA | MetS | 21 | 11 | 10 | 0.9 | 35.5 | 66.2 | 8.0 |
| Kelly, K.R (2011) [33] | USA | adiposity | 28 | 13 | 15 | 1.2 | 34.2 | 66.0 | 5.9 |
| Mulya, A (2017) [15] | USA | adiposity | 19 | 9 | 10 | 0.9 | 34.0 | 64.0 | 5.5 |
| Osella, A.R (2018) [34] | USA | MetS | 231 | 55 | 176 | 0.7 | NS | 57.6 | NS |
| Gomes, J.M (2017) [35] | Brazil | T2DM | 20 | 10 | 10 | 1.0 | 29.2 | 42.4 | 8.2 |
| Solomon, T.P (2009) [36] | USA | adiposity | 32 | 15 | 17 | 1.1 | 33.8 | 66.0 | 5.6 |
| Fraser, A (2008) [37] | Israel | T2DM | 201 | 73 | 128 | 1.5 | 31.4 | 56.0 | 10.3 |
| Visuthranukul, C (2015) [38] | Thailand | adiposity | 52 | 25 | 27 | 0.5 | 33.6 | 12.0 | 5.0 |
| Jenkins, D.J (2011) [39] | Canada | T2DM | 152 | 79 | 73 | 0.6 | 30.5 | 61.5 | NS |
| Pavithran, N (2020) [40] | India | T2DM | 36 | 18 | 18 | 0.7 | 27.0 | 52.0 | NS |
| Solomon, T.P (2013) [41] | USA | adiposity | 20 | 10 | 10 | 1.2 | 35.0 | 65.0 | 5.9 |
| Fabricatore, A.N (2011) [42] | USA | T2DM | 79 | 40 | 39 | 3.9 | 36.3 | 52.7 | NS |
| Argiana, V (2014) [43] | Greece | T2DM | 58 | 28 | 30 | 1.1 | 32.5 | 62.2 | NS |
| Li, D (2014) [44] | China | T2DM | 54 | 36 | 18 | 0.6 | 24.3 | 56.0 | 6.8 |
| Mirza, N.M (2011) [45] | USA | adiposity | 88 | 45 | 43 | 0.9 | 29.5 | 12.2 | NS |
| Hu, Z.G (2014) [16] | China | GDM | 140 | 66 | 74 | All famale | NS | 30.0 | 5.0 |
| Heilbronn, L.K (2002) [17] | Australia | T2DM | 45 | 24 | 21 | 1.0 | 33.8 | 56.7 | 7.0 |
| Basharat, S (2018) [46] | Pakistan | adiposity | 74 | 38 | 36 | All famale | 31.4 | 27.0 | NS |
| Abete, I (2008) [14] | Spain | adiposity | 32 | 16 | 16 | 0.8 | 32.5 | 36.0 | NS |
| First Author (Year) | Time Duration | Study Length | Randomization Method | Blinding | Energy Restriction | Int. Type | Con.Type | GI Int. | GI Con. | CHO(%) Int. | CHO(%) Con. |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Jenkins, D.J (2008) | 8 July 2004–22 May 2007 | 6 months | ID | Yes | No | LGID | HCFD | 69.6 | 83.5 | 44.0 | 47.5 |
| Turner-McGrievy (2011) | 2003–2004 | 22 weeks | NS | No | No | LGID | ADAD | NS | NS | NS | NS |
| Ebbeling, C.B (2003) | 1 December 2000–30 September 2001 | 6 months | NS | No | No | LGID | LFD | 58.0 | 59.0 | 58.0 | 52.0 |
| Wolever, T.M (2008) | NS | 1 year | Opaque envelope | No | No | LGID | HGID/LCHOD | 55.1 | 61.3 | 51.9 | 43.1 |
| Wolever, T.M (2008) | January 2002–October 2003 | 1 year | Opaque envelope | No | No | LGID | HGID/LCHOD | 55.0 | 61.4 | 52.0 | 42.7 |
| Malin, S.K (2012) | NS | 12 weeks | NS | No | No | LGID | HGID | 40.3 | 80.3 | 56.2 | 57.8 |
| Kelly, K.R (2011) | NS | 12 weeks | NS | No | No | LGID | HGID | 40.3 | 80.2 | 55.8 | 57.7 |
| Mulya, A (2017) | NS | 12 weeks | NS | No | No | LGID | HGID | 40.0 | 80.0 | NS | NS |
| Osella, A.R (2018) | December 2007–April 2008 | 24 weeks | Nonce | Yes | No | LGID | Med-D/LGIMD/RD | NS | NS | 46.5 | NS |
| Gomes, J.M (2017) | April 2007–September 2007 | 30 days | NS | Yes | No | LGID | HGID | 35.8 | 74.1 | 59.8 | 53.5 |
| Solomon, T.P (2009) | NS | 7 days | NS | No | No | LGID | HGID | 41.1 | 80.9 | 56.2 | 57.2 |
| Fraser, A (2008) | March 2003–April 2004 | 12 months | Nonce | Yes | Yes | LGID | MMD/ADA | NS | NS | NS | NS |
| Visuthranukul, C (2015) | January 2010–January 2013 | 6 months | NS | No | No | LGID | LFD | NS | NS | NS | NS |
| Jenkins, D.J (2011) | May 2004–May 2007 | 6 months | ID | Yes | No | LGID | HCFD | 69.6 | 83.5 | 44.0 | 47.5 |
| Pavithran, N (2020) | October 2018–April 2019 | 24 weeks | NS | No | No | LGID | RD | NS | NS | NS | NS |
| Solomon, T.P (2013) | NS | 3 months | NS | No | No | LGID | HGID | 39.8 | 80.0 | 54.7 | 55.6 |
| Fabricatore, A.N (2011) | September 2006–July 2009 | 40 weeks | Nonce | No | Yes | LGID | LFD | 63.6 | 63.4 | 44.0 | 46.0 |
| Argiana, V (2014) | NS | 12 weeks | Nonce | No | Yes | LGID | RD | 19.0–49.0 | 60.0–65.0 | NS | NS |
| Li, D (2014) | June 2013–October 2013 | 12 weeks | NS | No | No | LGID | RD | NS | NS | 54.6 | 52.1 |
| Mirza, N.M (2011) | NS | 12 weeks | NS | No | No | LGLD | HGLD | 36.1 | 59.5 | NS | NS |
| Hu, Z.G (2014) | October 2011–April 2013 | 5 days | NS | No | Yes | LGID | RD | NS | NS | NS | NS |
| Heilbronn, L.K (2002) | NS | 12 weeks | NS | No | Yes | LGID | HGID | 43.0 | 75.0 | 58.9 | 60.8 |
| Basharat, S (2018) | April 2005–2005 June | 12 weeks | NS | No | No | LGID | RD | 44.6 | 66.0 | 45.0 | 52.7 |
| Abete, I (2008) | NS | 8 weeks | NS | No | Yes | LGID | HGID | 40.0–45.0 | 60.0–65.0 | NS | NS |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ni, C.; Jia, Q.; Ding, G.; Wu, X.; Yang, M. Low-Glycemic Index Diets as an Intervention in Metabolic Diseases: A Systematic Review and Meta-Analysis. Nutrients 2022, 14, 307. https://doi.org/10.3390/nu14020307
Ni C, Jia Q, Ding G, Wu X, Yang M. Low-Glycemic Index Diets as an Intervention in Metabolic Diseases: A Systematic Review and Meta-Analysis. Nutrients. 2022; 14(2):307. https://doi.org/10.3390/nu14020307
Chicago/Turabian StyleNi, Chunxiao, Qingqing Jia, Gangqiang Ding, Xifeng Wu, and Min Yang. 2022. "Low-Glycemic Index Diets as an Intervention in Metabolic Diseases: A Systematic Review and Meta-Analysis" Nutrients 14, no. 2: 307. https://doi.org/10.3390/nu14020307
APA StyleNi, C., Jia, Q., Ding, G., Wu, X., & Yang, M. (2022). Low-Glycemic Index Diets as an Intervention in Metabolic Diseases: A Systematic Review and Meta-Analysis. Nutrients, 14(2), 307. https://doi.org/10.3390/nu14020307