
Adherence to the Mediterranean Diet among Children and Youth in the Mediterranean Region in Croatia: A Comparative Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Questionnaire
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Marques, G.F.S.; Pinto, S.M.O.; Reis, A.; Martins, T.D.B.; Conceicao, A.P.D.; Pinheiro, A.R.V. Adherence to the Mediterranean Diet in Elementary School Children (1st Cycle). Rev. Paul. Pediatr. 2021, 39, e2019259. [Google Scholar] [CrossRef]
- Grosso, G.; Buscemi, S.; Galvano, F.; Mistretta, A.; Marventano, S.; La Vela, V.; Drago, F.; Gangi, S.; Basile, F.; Biondi, A. Mediterranean diet and cancer: Epidemiological evidence and mechanism of selected aspects. BMC Surg. 2013, 13 (Suppl. 2), S14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Esposito, K.; Maiorino, M.I.; Bellastella, G.; Chiodini, P.; Panagiotakos, D.; Giugliano, D. A journey into a Mediterranean diet and type 2 diabetes: A systematic review with meta-analyses. BMJ Open 2015, 5, e008222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mattioli, A.V.; Palmiero, P.; Manfrini, O.; Puddu, P.E.; Nodari, S.; Dei Cas, A.; Mercuro, G.; Scrutinio, D.; Palermo, P.; Sciomer, S.; et al. Mediterranean diet impact on cardiovascular diseases: A narrative review. J. Cardiovasc. Med. 2017, 18, 925–935. [Google Scholar] [CrossRef] [PubMed]
- Schwingshackl, L.; Schwedhelm, C.; Galbete, C.; Hoffmann, G. Adherence to Mediterranean Diet and Risk of Cancer: An Updated Systematic Review and Meta-Analysis. Nutrients 2017, 9, 1063. [Google Scholar] [CrossRef]
- Grosso, G.; Marventano, S.; Yang, J.; Micek, A.; Pajak, A.; Scalfi, L.; Galvano, F.; Kales, S.N. A comprehensive meta-analysis on evidence of Mediterranean diet and cardiovascular disease: Are individual components equal? Crit. Rev. Food Sci. Nutr. 2017, 57, 3218–3232. [Google Scholar] [CrossRef]
- Vidal-Peracho, C.; Tricas-Moreno, J.M.; Lucha-Lopez, A.C.; Lucha-Lopez, M.O.; Camunas-Pescador, A.C.; Caverni-Munoz, A.; Fanlo-Mazas, P. Adherence to Mediterranean Diet Pattern among Spanish Adults Attending a Medical Centre: Nondiabetic Subjects and Type 1 and 2 Diabetic Patients. J. Diabetes Res. 2017, 2017, 5957821. [Google Scholar] [CrossRef] [Green Version]
- Liyanage, T.; Ninomiya, T.; Wang, A.; Neal, B.; Jun, M.; Wong, M.G.; Jardine, M.; Hillis, G.S.; Perkovic, V. Effects of the Mediterranean Diet on Cardiovascular Outcomes-A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0159252. [Google Scholar] [CrossRef] [Green Version]
- Tsakiraki, M.; Grammatikopoulou, M.G.; Stylianou, C.; Tsigga, M. Nutrition transition and health status of Cretan women: Evidence from two generations. Public Health Nutr. 2011, 14, 793–800. [Google Scholar] [CrossRef] [Green Version]
- Belahsen, R. Nutrition transition and food sustainability. Proc. Nutr. Soc. 2014, 73, 385–388. [Google Scholar] [CrossRef] [Green Version]
- Karnik, S.; Kanekar, A. Childhood obesity: A global public health crisis. Int. J. Prev. Med. 2012, 3, 1–7. [Google Scholar] [PubMed] [Green Version]
- Musić Milanović, S.; Lang Morović, M.; Križan, H. WHO European Childhood Obesity Surveillance Initiative (COSI), Croatia 2018/2019 (CroCOSI); Croatian Institute of Public Health: Zagreb, Croatia, 2021. [Google Scholar]
- OECD. Heavy Burden of Obesity: The Economics of Prevention—A Quick Guide for Policy Makers; OECD: Paris, France, 2019. [Google Scholar]
- De Santi, M.; Callari, F.; Brandi, G.; Toscano, R.V.; Scarlata, L.; Amagliani, G.; Schiavano, G.F. Mediterranean diet adherence and weight status among Sicilian Middle school adolescents. Int. J. Food Sci. Nutr. 2020, 71, 1010–1018. [Google Scholar] [CrossRef]
- Stefan, L.; Prosoli, R.; Juranko, D.; Cule, M.; Milinovic, I.; Novak, D.; Sporis, G. The Reliability of the Mediterranean Diet Quality Index (KIDMED) Questionnaire. Nutrients 2017, 9, 419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salcin, L.O.; Karin, Z.; Miljanovic Damjanovic, V.; Ostojic, M.; Vrdoljak, A.; Gilic, B.; Sekulic, D.; Lang-Morovic, M.; Markic, J.; Sajber, D. Physical Activity, Body Mass, and Adherence to the Mediterranean Diet in Preschool Children: A Cross-Sectional Analysis in the Split-Dalmatia County (Croatia). Int. J. Environ. Res. Public Health 2019, 16, 3237. [Google Scholar]
- Nenadić, D.B.; Kolak, E.; Selak, M.; Smoljo, M.; Radić, J.; Vučković, M.; Dropuljić, B.; Pijerov, T.; Cikoš, D.B. Anthropometric Parameters and Mediterranean Diet Adherence in Preschool Children in Split-Dalmatia County, Croatia—Are They Related? Nutrients 2021, 13, 4252. [Google Scholar]
- Serra-Majem, L.; Ribas, L.; Ngo, J.; Ortega, R.M.; García, A.; Pérez-Rodrigo, C.; Aranceta, J. Food, youth and the Mediterranean diet in Spain. Development of KIDMED, Mediterranean Diet Quality Index in children and adolescents. Public Health Nutr. 2004, 7, 931–935. [Google Scholar] [CrossRef]
- World Health Organization. Obesity: Preventing and Managing the Global Epidemic. Report of a WHO Consultation; WHO Technical Report Series 894; World Health Organization: Geneva, Switzerland, 2000; pp. 1–253. [Google Scholar]
- Kolcic, I.; Relja, A.; Gelemanovic, A.; Miljkovic, A.; Boban, K.; Hayward, C.; Rudan, I.; Polasek, O. Mediterranean diet in the southern Croatia—does it still exist? Croat. Med. J. 2016, 57, 415–424. [Google Scholar] [CrossRef] [Green Version]
- Shier, V.; Nicosia, N.; Datar, A. Neighborhood and home food environment and children’s diet and obesity: Evidence from military personnel’s installation assignment. Soc. Sci. Med. 2016, 158, 122–131. [Google Scholar] [CrossRef] [Green Version]
- Neumark-Sztainer, D.; Hannan, P.J.; Story, M.; Croll, J.; Perry, C. Family meal patterns: Associations with sociodemographic characteristics and improved dietary intake among adolescents. J. Am. Diet. Assoc. 2003, 103, 317–322. [Google Scholar] [CrossRef]
- Larson, N.I.; Neumark-Sztainer, D.; Hannan, P.J.; Story, M. Family meals during adolescence are associated with higher diet quality and healthful meal patterns during young adulthood. J. Am. Diet. Assoc. 2007, 107, 1502–1510. [Google Scholar] [CrossRef]
- Arcila-Agudelo, A.M.; Ferrer-Svoboda, C.; Torres-Fernandez, T.; Farran-Codina, A. Determinants of Adherence to Healthy Eating Patterns in a Population of Children and Adolescents: Evidence on the Mediterranean Diet in the City of Mataro (Catalonia, Spain). Nutrients 2019, 11, 854. [Google Scholar] [CrossRef] [Green Version]
- Deliens, T.; Clarys, P.; De Bourdeaudhuij, I.; Deforche, B. Determinants of eating behaviour in university students: A qualitative study using focus group discussions. BMC Public Health 2014, 14, 53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marquis, M. Exploring convenience orientation as a food motivation for college students living in residence halls. Int. J. Consum. Stud. 2005, 29, 55–63. [Google Scholar] [CrossRef]
- Grosso, G.; Marventano, S.; Buscemi, S.; Scuderi, A.; Matalone, M.; Platania, A.; Giorgianni, G.; Rametta, S.; Nolfo, F.; Galvano, F.; et al. Factors Associated with Adherence to the Mediterranean Diet among Adolescents Living in Sicily, Southern Italy. Nutrients 2013, 5, 4908–4923. [Google Scholar] [CrossRef] [Green Version]
- Mariscal-Arcas, M.; Rivas, A.; Velasco, J.; Ortega, M.; Caballero, A.M.; Olea-Serrano, F. Evaluation of the Mediterranean Diet Quality Index (KIDMED) in children and adolescents in Southern Spain. Public Health Nutr. 2009, 12, 1408–1412. [Google Scholar] [CrossRef] [Green Version]
- Sahingoz, S.A.; Sanlier, N. Compliance with Mediterranean Diet Quality Index (KIDMED) and nutrition knowledge levels in adolescents. A case study from Turkey. Appetite 2011, 57, 272–277. [Google Scholar] [CrossRef] [PubMed]
- Cabrera, S.G.; Fernandez, N.H.; Hernandez, C.R.; Nissensohn, M.; Roman-Vinas, B.; Serra-Majem, L. KIDMED test; prevalence of low adherence to the Mediterranean Diet in children and young; a systematic review. Nutr. Hosp. 2015, 32, 2390–2399. [Google Scholar]
- Iaccarino Idelson, P.; Scalfi, L.; Valerio, G. Adherence to the Mediterranean Diet in children and adolescents: A systematic review. Nutr. Metab. Cardiovasc. Dis. 2017, 27, 283–299. [Google Scholar] [CrossRef]
- Agostinis-Sobrinho, C.; Santos, R.; Rosario, R.; Moreira, C.; Lopes, L.; Mota, J.; Martinkenas, A.; Garcia-Hermoso, A.; Correa-Bautista, J.E.; Ramirez-Velez, R. Optimal Adherence to a Mediterranean Diet May Not Overcome the Deleterious Effects of Low Physical Fitness on Cardiovascular Disease Risk in Adolescents: A Cross-Sectional Pooled Analysis. Nutrients 2018, 10, 815. [Google Scholar] [CrossRef] [Green Version]
- Rollins, B.Y.; Belue, R.Z.; Francis, L.A. The beneficial effect of family meals on obesity differs by race, sex, and household education: The national survey of children’s health, 2003–2004. J. Am. Diet. Assoc. 2010, 110, 1335–1339. [Google Scholar] [CrossRef] [Green Version]
- Roccaldo, R.; Censi, L.; D’Addezio, L.; Toti, E.; Martone, D.; D’Addesa, D.; Cernigliaro, A.; ZOOM8 Study group. Adherence to the Mediterranean diet in Italian school children (The ZOOM8 Study). Int. J. Food Sci. Nutr. 2014, 65, 621–628. [Google Scholar] [CrossRef] [PubMed]
- Shalá, A.; López-Guimera, G.; Fauquet, J.; Puntí, J.; Leiva, D.; Sánchez-Carracedo, D. Association between Family Meals and the Adherence to the Mediterranean Diet in Spanish Adolescents. J. Child Adolesc. Behav. 2017, 5, 272–366. [Google Scholar] [CrossRef] [Green Version]
- Svensson, A.; Larsson, C.; Eiben, G.; Lanfer, A.; Pala, V.; Hebestreit, A.; Huybrechts, I.; Fernandez-Alvira, J.M.; Russo, P.; Koni, A.C.; et al. European children’s sugar intake on weekdays versus weekends: The IDEFICS study. Eur. J. Clin. Nutr. 2014, 68, 822–828. [Google Scholar] [CrossRef] [PubMed]
- Lehtisalo, J.; Erkkola, M.; Tapanainen, H.; Kronberg-Kippila, C.; Veijola, R.; Knip, M.; Virtanen, S.M. Food consumption and nutrient intake in day care and at home in 3-year-old Finnish children. Public Health Nutr. 2010, 13, 957–964. [Google Scholar] [CrossRef] [Green Version]
- Garemo, M.; Lenner, R.A.; Strandvik, B. Swedish pre-school children eat too much junk food and sucrose. Acta Paediatr. 2007, 96, 266–272. [Google Scholar] [CrossRef] [PubMed]
- Haines, P.S.; Hama, M.Y.; Guilkey, D.K.; Popkin, B.M. Weekend eating in the United States is linked with greater energy, fat, and alcohol intake. Obes. Res. 2003, 11, 945–949. [Google Scholar] [CrossRef] [PubMed]
- Sepp, H.; Lennernas, M.; Pettersson, R.; Abrahamsson, L. Children’s nutrient intake at preschool and at home. Acta Paediatr. 2001, 90, 483–491. [Google Scholar] [CrossRef]
- Hart, C.N.; Raynor, H.A.; Osterholt, K.M.; Jelalian, E.; Wing, R.R. Eating and activity habits of overweight children on weekdays and weekends. Int. J. Pediatr. Obes. 2011, 6, 467–472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jago, R.; Thompson, J.L.; Sebire, S.J.; Wood, L.; Pool, L.; Zahra, J.; Lawlor, D.A. Cross-sectional associations between the screen-time of parents and young children: Differences by parent and child gender and day of the week. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feeley, A.; Musenge, E.; Pettifor, J.M.; Norris, S.A. Changes in dietary habits and eating practices in adolescents living in urban South Africa: The birth to twenty cohort. Nutrition 2012, 28, e1–e6. [Google Scholar] [CrossRef] [PubMed]
- Warnberg, J.; Perez-Farinos, N.; Benavente-Marin, J.C.; Gomez, S.F.; Labayen, I.; AGZ; Gusi, N.; Aznar, S.; Alcaraz, P.E.; Gonzalez-Valeiro, M.; et al. Screen Time and Parents’ Education Level Are Associated with Poor Adherence to the Mediterranean Diet in Spanish Children and Adolescents: The PASOS Study. J. Clin. Med. 2021, 10, 795. [Google Scholar] [CrossRef]
- Llargues, E.; Franco, R.; Recasens, A.; Nadal, A.; Vila, M.; Perez, M.J.; Manresa, J.M.; Recasens, I.; Salvador, G.; Serra, J.; et al. Assessment of a school-based intervention in eating habits and physical activity in school children: The AVall study. J. Epidemiol. Community Health 2011, 65, 896–901. [Google Scholar] [CrossRef] [PubMed]
- Bibiloni, M.d.M.; Pich, J.; Cordova, A.; Pons, A.; Tur, J.A. Association between sedentary behaviour and socioeconomic factors, diet and lifestyle among the Balearic Islands adolescents. BMC Public Health 2012, 12, 718. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martinez-Gomez, D.; Veiga, O.L.; Gomez-Martinez, S.; Zapatera, B.; Calle, M.E.; Marcos, A.; AFINOS Study Group. Behavioural correlates of active commuting to school in Spanish adolescents: The AFINOS (Physical Activity as a Preventive Measure Against Overweight, Obesity, Infections, Allergies, and Cardiovascular Disease Risk Factors in Adolescents) study. Public Health Nutr. 2011, 14, 1779–1786. [Google Scholar] [CrossRef] [Green Version]
- Moliner-Urdiales, D.; Ruiz, J.R.; Ortega, F.B.; Rey-Lopez, J.P.; Vicente-Rodriguez, G.; Espana-Romero, V.; Munguia-Izquierdo, D.; Castillo, M.J.; Sjostrom, M.; Moreno, L.A.; et al. Association of objectively assessed physical activity with total and central body fat in Spanish adolescents; The HELENA Study. Int. J. Obes. 2009, 33, 1126–1135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wittmeier, K.D.M.; Mollard, R.C.; Kriellaars, D.J. Physical activity intensity and risk of overweight and adiposity in children. Obesity 2008, 16, 415–420. [Google Scholar] [CrossRef] [PubMed]
- Beets, M.W.; Cardinal, B.J.; Alderman, B.L. Parental social support and the physical activity-related behaviors of youth: A review. Health Educ. Behav. 2010, 37, 621–644. [Google Scholar] [CrossRef]
- Yao, C.A.; Rhodes, R.E. Parental correlates in child and adolescent physical activity: A meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 10. [Google Scholar] [CrossRef] [Green Version]
- Edwardson, C.L.; Gorely, T. Parental influences on different types and intensities of physical activity in youth: A systematic review. Psychol. Sport Exerc. 2010, 11, 522–535. [Google Scholar] [CrossRef]
- Martikainen, P.; Aromaa, A.; Heliovaara, M.; Klaukka, T.; Knekt, P.; Maatela, J.; Lahelma, E. Reliability of perceived health by sex and age. Soc. Sci.Med. 1999, 48, 1117–1122. [Google Scholar] [CrossRef]
- Theunissen, N.C.; Vogels, T.G.; Koopman, H.M.; Verrips, G.H.; Zwinderman, K.A.; Verloove-Vanhorick, S.P.; Wit, J.M. The proxy problem: Child report versus parent report in health-related quality of life research. Qual. Life Res. 1998, 7, 387–397. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Variable | Descriptive Statistics |
|---|---|
| Gender, n (%) | |
| Females | 1340 (49.2%) |
| Males | 1382 (50.8%) |
| Age, median (interquartile range) | 10.0 (6.0) |
| BMI classification, n (%) | |
| Underweight | 199 (7.3%) |
| Normal weight | 1884 (69.2%) |
| Overweight | 351 (12.9%) |
| Obese | 163 (6%) |
| Educational stage, n (%) | |
| Kindergarten | 485 (17.8%) |
| Primary school (1st–4th grade) | 941 (34.5%) |
| Primary school (5th–8th grade) | 780 (28.6%) |
| Secondary school | 343 (12.6%) |
| Faculty (college students) | 173 (6.3%) |
| Total Sample | Kindergarten | Primary School (1st–4th Grade) | Primary School (5th–8th Grade) | Secondary School | Faculty | p Value | |
|---|---|---|---|---|---|---|---|
| KIDMED index score, n (%) 1 | |||||||
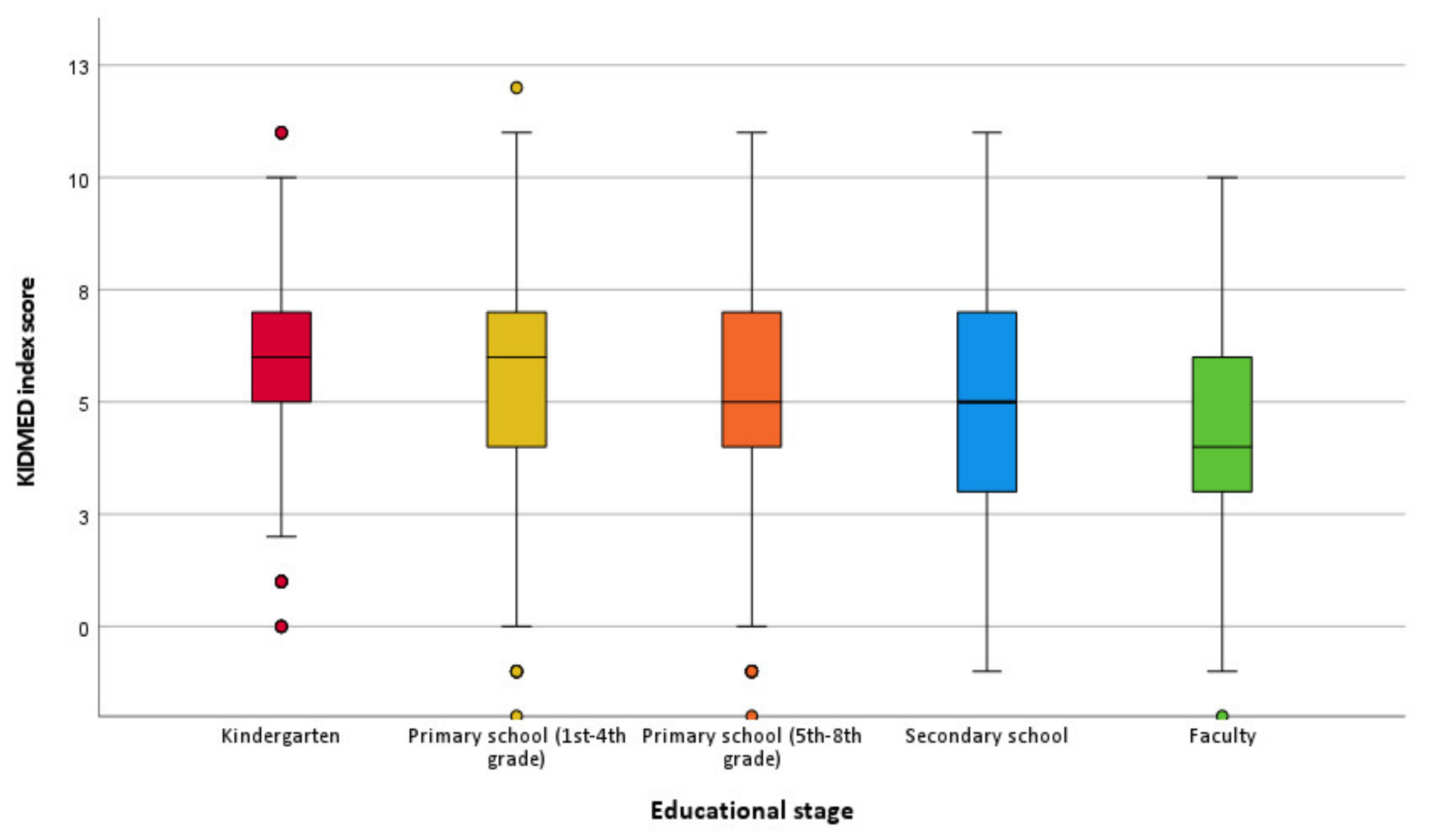
| Poor | 523 (19.2%) | 55 (11.3%) | 158 (16.8%) | 153 (19.6%) | 88 (25.7%) | 69 (39.9%) | <0.001 |
| Average | 1653 (60.7%) | 315 (64.9%) | 599 (63.7%) | 462 (59.2%) | 196 (57.1%) | 81 (46.8%) | |
| Good | 546 (20.1%) | 115 (23.7%) | 184 (19.6%) | 165 (21.2%) | 59 (17.2%) | 23 (13.3%) | |
| KIDMED items, n (%) 2 | |||||||
| Fruit or fruit juice daily | 2321 (85.3%) | 455 (93.8%) | 800 (85%) | 652 (83.6%) | 280 (81.6%) | 129 (74.6%) | <0.001 |
| Second serving of fruit daily | 1271 (46.7%) | 260 (53.6%) | 437 (46.4%) | 369 (47.3%) | 144 (42.0%) | 60 (34.7%) | <0.001 |
| Fresh or cooked vegetables daily | 1942 (71.4%) | 376 (77.5%) | 681 (72.4%) | 538 (69%) | 227 (66.2%) | 117 (67.6%) | 0.003 |
| Fresh or cooked vegetables > 1/day | 585 (21.5%) | 107 (22.1%) | 199 (21.1%) | 172 (22.1%) | 70 (20.4%) | 37 (21.4%) | 0.749 |
| Regular fish consumption (at least 2–3/week) | 658 (24.3%) | 142 (29.3%) | 230 (24.4%) | 177 (22.7%) | 77 (22.4%) | 28 (16.2%) | 0.010 |
| Total Sample | Kindergarten | Primary School (1st–4th Grade) | Primary School (5th–8th Grade) | Secondary School | Faculty | p Value | |
| >1/week fast-food (hamburger) restaurant | 130 (4.8%) | 9 (1.9%) | 17 (1.8%) | 32 (4.1%) | 41 (12%) | 31 (17.9%) | <0.001 |
| Pulses > 1/week | 1556 (57.2%) | 263 (54.2%) | 545 (57.9%) | 461 (59.1%) | 194 (56.6%) | 90 (52%) | 0.429 |
| Pasta or rice almost daily (≥5 days/week) | 427 (15.7%) | 49 (10.1%) | 125 (13.3%) | 113 (14.5%) | 76 (22.2%) | 62 (35.8%) | <0.001 |
| Cereal or cereal product for breakfast | 1555 (57.1%) | 274 (56.5%) | 559 (59.4%) | 459 (58.8%) | 200 (58.3%) | 60 (34.7%) | <0.001 |
| Regular nut consumption (at least 2–3/week) | 1054 (38.7%) | 172 (35.5%) | 346 (36.8%) | 305 (39.1%) | 148 (43.1%) | 81 (46.8%) | 0.041 |
| Use of olive oil at home | 2486 (91.4%) | 463 (95.5%) | 862 (91.6%) | 701 (89.9%) | 306 (89.2%) | 149 (86.1%) | 0.003 |
| No breakfast | 299 (10.99%) | 17 (3.5%) | 45 (4.8%) | 96 (12.3%) | 73 (21.3%) | 67 (38.7%) | <0.001 |
| Dairy product for breakfast | 2413 (88.7%) | 446 (92%) | 856 (91%) | 700 (89.7%) | 291 (84.8%) | 116 (67.1%) | <0.001 |
| Commercially baked goods or pastries for breakfast | 1173 (43.1%) | 167 (34.4%) | 383 (40.7%) | 361 (46.3%) | 176 (51.3%) | 84 (48.6%) | <0.001 |
| Two yoghurts and/or 40 g cheese daily | 1193 (43.84%) | 239 (49.3%) | 387 (41.1%) | 343 (44%) | 155 (45.2%) | 68 (39.3%) | 0.051 |
| Sweets and candy several times a day | 751 (27.6%) | 134 (27.6%) | 244 (25.9%) | 226 (29%) | 89 (25.9%) | 58 (33.5%) | 0.439 |
| Predictors | Average MD Adherence | Good MD Adherence | ||
|---|---|---|---|---|
| OR (95% CI) 1 | p-Value | OR (95% CI) 1 | p-Value | |
| Age | 0.962 (0.933, 0.991) | 0.011 | 0.974 (0.939, 1.011) | 0.165 |
| Number of daily meals on working days | 1.242 (0.913, 1.688) | 0.167 | 1.341 (0.919, 1.957) | 0.128 |
| Number of daily meals on day-offs | 1.264 (0.910, 1.757) | 0.162 | 1.339 (0.903, 1.986) | 0.146 |
| Number of snacks on working days | 1.470 (1.157, 1.867) | 0.002 | 1.978 (1.470, 2.660) | <0.001 |
| Number of snacks on day-offs | 0.773 (0.627, 0.953) | 0.016 | 0.738 (0.567, 0.960) | 0.023 |
| Do you/Does your child participate in organized physical activity? | ||||
| No | 1.016 (0.776, 1.332) | 0.907 | 0.819 (0.589, 1.139) | 0.235 |
| Predictors | Average MD Adherence | Good MD Adherence | ||
| OR (95% CI) 1 | p-Value | OR (95% CI) 1 | p-Value | |
| Yes | - | - | - | - |
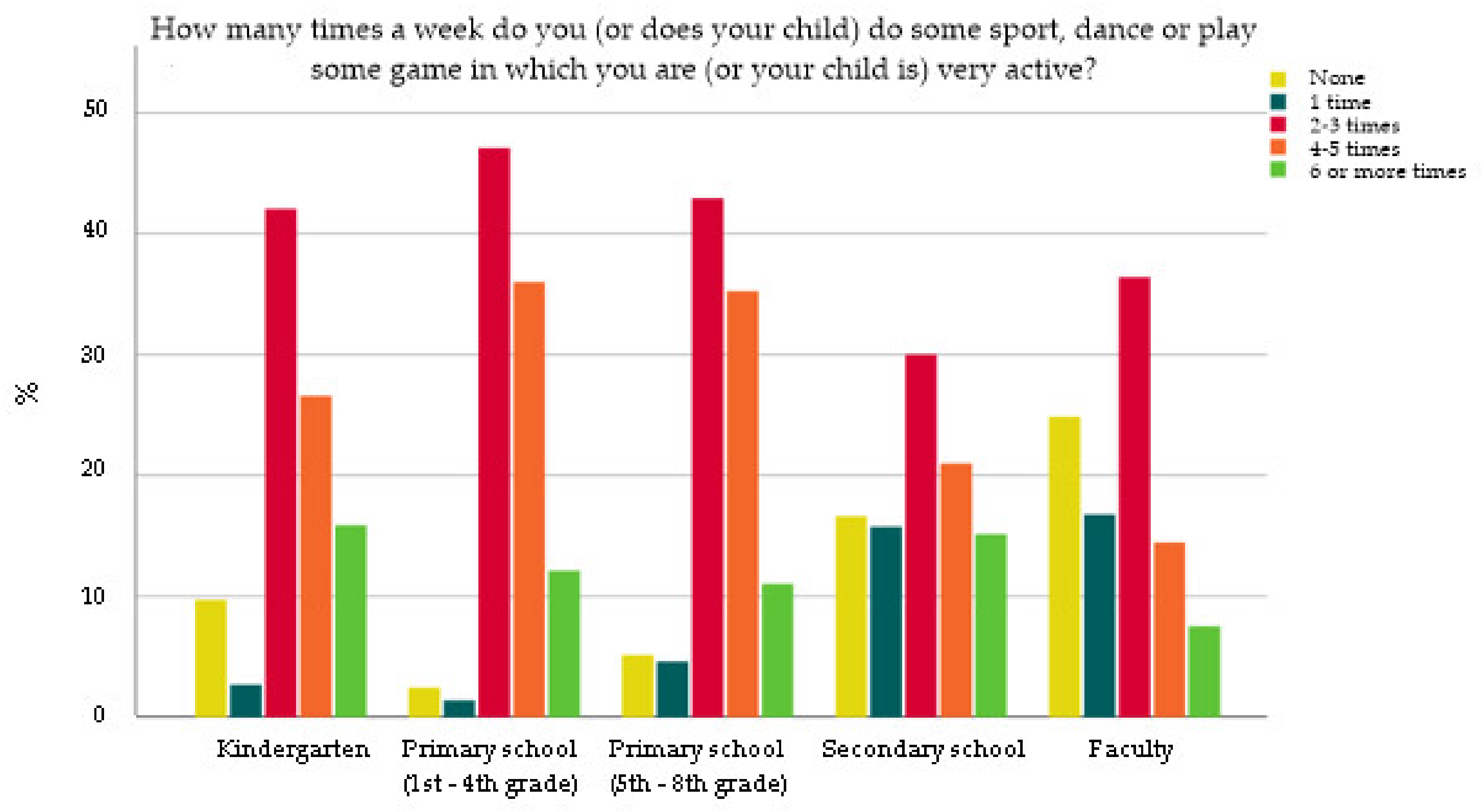
| How many times a week do you (or does your child) do some sport, dance or play some game in which you are (or your child is) very active? | ||||
| None | 0.365 (0.216, 0.615) | <0.001 | 0.283 (0.145, 0.550) | <0.001 |
| 1 time | 0.416 (0.236, 0.734) | 0.002 | 0.374 (0.182, 0.770) | 0.008 |
| 2–3 times | 0.676 (0.463, 0.987) | 0.043 | 0.508 (0.330, 0.782) | 0.002 |
| 4–5 times | 1.222 (0.814, 1.834) | 0.334 | 0.759 (0.478, 1.206) | 0.243 |
| 6 or more times | - | - | - | - |
| Having breakfast together as a family | ||||
| No | 0.644 (0.514, 0.808) | <0.001 | 0.311 (0.233, 0.416) | <0.001 |
| Yes | - | - | - | - |
| Having dinner together as a family | ||||
| No | 0.980 (0.698, 1.375) | 0.906 | 0.789 (0.493, 1.261) | 0.322 |
| Yes | - | - | - | - |
| Predictors | Good | Very Good | ||
|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| How many times a week do you (or does your child) do some sport, dance, or play some game in which you are (or your child is) very active? | ||||
| Predictors | Good | Very Good | ||
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| None | 10.335 (3.140, 34.021) | <0.001 | 7.353 (2.582, 20.940) | <0.001 |
| 1 time | 4.626 (2.565, 8.343) | <0.001 | 4.259 (2.759, 6.573) | <0.001 |
| 2–3 times | 1.626 (0.978, 2.705) | 0.061 | 2.804 (1.990, 3.950) | <0.001 |
| 4–5 times | 0.886 (0.515, 1.525) | 0.662 | 2.196 (1.552, 3.108) | <0.001 |
| 6 or more times | - | - | - | - |
| Mediterranean index score classification | ||||
| Average MD adherence | 0.596 (0.419, 0.848) | 0.004 | 0.812 (0.643, 1.026) | 0.081 |
| Good MD adherence | 0.497 (0.311, 0.794) | 0.003 | 0.646 (0.485, 0.861) | 0.003 |
| Poor MD adherence | - | - | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matana, A.; Franić, I.; Radić Hozo, E.; Burger, A.; Boljat, P. Adherence to the Mediterranean Diet among Children and Youth in the Mediterranean Region in Croatia: A Comparative Study. Nutrients 2022, 14, 302. https://doi.org/10.3390/nu14020302
Matana A, Franić I, Radić Hozo E, Burger A, Boljat P. Adherence to the Mediterranean Diet among Children and Youth in the Mediterranean Region in Croatia: A Comparative Study. Nutrients. 2022; 14(2):302. https://doi.org/10.3390/nu14020302
Chicago/Turabian StyleMatana, Antonela, Ivana Franić, Endica Radić Hozo, Ante Burger, and Petra Boljat. 2022. "Adherence to the Mediterranean Diet among Children and Youth in the Mediterranean Region in Croatia: A Comparative Study" Nutrients 14, no. 2: 302. https://doi.org/10.3390/nu14020302
APA StyleMatana, A., Franić, I., Radić Hozo, E., Burger, A., & Boljat, P. (2022). Adherence to the Mediterranean Diet among Children and Youth in the Mediterranean Region in Croatia: A Comparative Study. Nutrients, 14(2), 302. https://doi.org/10.3390/nu14020302