

Nutritional Status, Body Composition, and Inflammation Profile in Older Patients with Advanced Chronic Kidney Disease Stage 4–5: A Case-Control Study



Abstract
1. Introduction
2. Materials and Methods
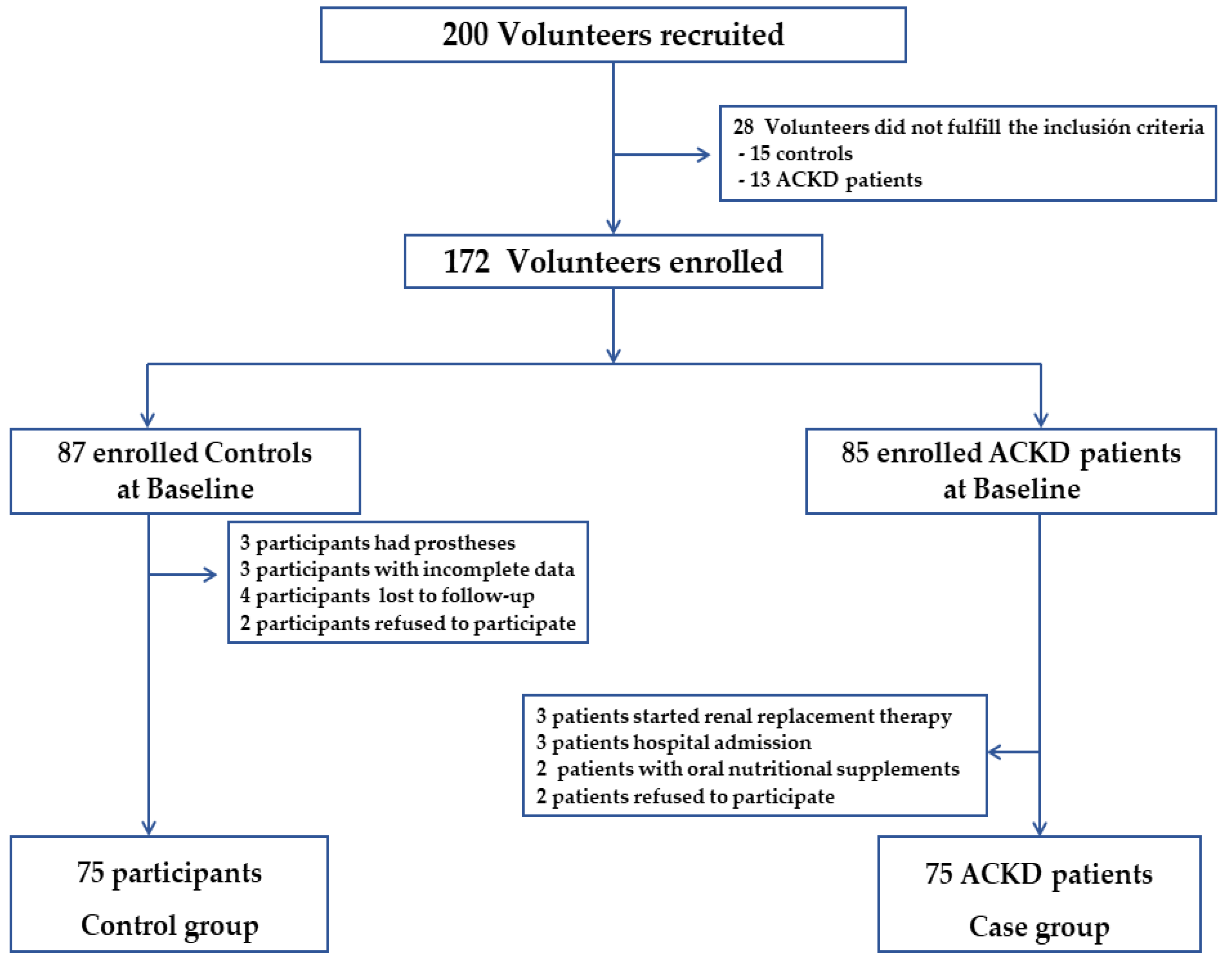
2.1. Patient Population
2.2. Data Collection
2.3. Anthropometric Measurements
2.4. Analysis of Body Composition
2.5. Laboratory Parameters
2.6. Prognosis Nutritional Index
2.7. Statistical Analysis
3. Results
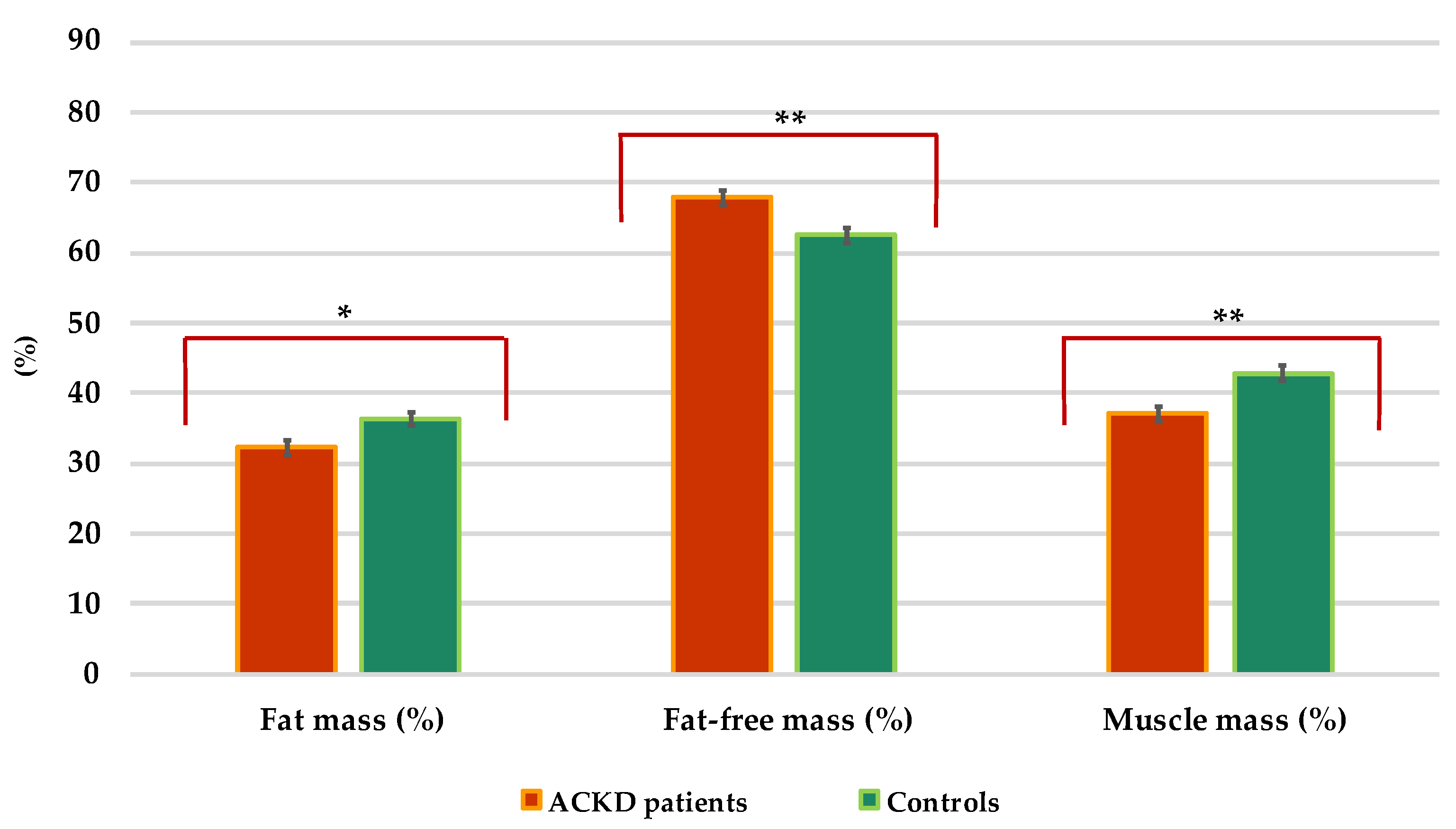
3.1. Global Data and Comparison between Cases and Controls
3.2. Univariate Conditional Regression Analyses
3.3. Multivariate Conditional Regression Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- United Nations. Department of Economic and Social Affairs. Population Division. World Population Prospects. 2022. Available online: https://population.un.org/wpp/ (accessed on 28 July 2022).
- Kovesdy, C.P. Epidemiology of chronic kidney disease: An update 2022. Kidney Int. Suppl. 2022, 12, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Norman, K.; Hass, U.; Pirlich, M. Malnutrition in Older Adults-Recent Advances and Remaining Challenges. Nutrients 2021, 13, 2764. [Google Scholar] [CrossRef] [PubMed]
- Ramon, J.M.; Subira, C. Prevalence of malnutrition in the elderly Spanish population. Med. Clin. 2001, 117, 766–770. [Google Scholar] [CrossRef]
- Carrero, J.J.; Thomas, F.; Nagy, K.; Arogundade, F.; Avesani, C.M.; Chan, M.; Chmielewski, M.; Cordeiro, A.C.; Espinosa-Cuevas, A.; Fiaccadori, E.; et al. Global Prevalence of Protein-Energy Wasting in Kidney Disease: A Meta-analysis of Contemporary Observational Studies from the International Society of Renal Nutrition and Metabolism. J. Ren. Nutr. 2018, 28, 380–392. [Google Scholar] [CrossRef] [PubMed]
- Westland, G.J.; Grootendorst, D.C.; Halbesma, N.; Dekker, F.W.; Verburgh, C.A. The nutritional status of patients starting specialized predialysis care. J. Ren. Nutr. 2015, 25, 265–270. [Google Scholar] [CrossRef]
- Windahl, K.; Faxen Irving, G.; Almquist, T.; Liden, M.K.; van de Luijtgaarden, M.; Chesnaye, N.C.; Voskamp, P.; Stenvinkel, P.; Klinger, M.; Szymczak, M.; et al. Prevalence and Risk of Protein-Energy Wasting Assessed by Subjective Global Assessment in Older Adults with Advanced Chronic Kidney Disease: Results from the Equal Study. J. Ren. Nutr. 2018, 28, 165–174. [Google Scholar] [CrossRef]
- Guligowska, A.; Corsonello, A.; Piglowska, M.; Roller-Wirnsberger, R.; Wirnsberger, G.; Arnlov, J.; Carlsson, A.C.; Tap, L.; Mattace-Raso, F.; Formiga, F.; et al. Association between kidney function, nutritional status and anthropometric measures in older people: The Screening for CKD among Older People across Europe (SCOPE) study. BMC Geriatr. 2020, 20, 366. [Google Scholar] [CrossRef]
- Ahmadi, S.F.; Zahmatkesh, G.; Ahmadi, E.; Streja, E.; Rhee, C.M.; Gillen, D.L.; De Nicola, L.; Minutolo, R.; Ricardo, A.C.; Kovesdy, C.P.; et al. Association of Body Mass Index with Clinical Outcomes in Non-Dialysis-Dependent Chronic Kidney Disease: A Systematic Review and Meta-Analysis. CardioRenal Med. 2015, 6, 37–49. [Google Scholar] [CrossRef]
- Lu, J.L.; Kalantar-Zadeh, K.; Ma, J.Z.; Quarles, L.D.; Kovesdy, C.P. Association of body mass index with outcomes in patients with CKD. J. Am. Soc. Nephrol. 2014, 25, 2088–2096. [Google Scholar] [CrossRef]
- Evans, P.D.; McIntyre, N.J.; Fluck, R.J.; McIntyre, C.W.; Taal, M.W. Anthropomorphic measurements that include central fat distribution are more closely related with key risk factors than BMI in CKD stage 3. PLoS ONE 2012, 7, e34699. [Google Scholar] [CrossRef]
- Cordeiro, A.C.; Qureshi, A.R.; Stenvinkel, P.; Heimburger, O.; Axelsson, J.; Barany, P.; Lindholm, B.; Carrero, J.J. Abdominal fat deposition is associated with increased inflammation, protein-energy wasting and worse outcome in patients undergoing haemodialysis. Nephrol. Dial. Transplant. 2010, 25, 562–568. [Google Scholar] [CrossRef] [PubMed]
- Sezer, S.; Karakan, S.; Acar, N.O. Association of conicity index and renal progression in pre-dialysis chronic kidney disease. Ren. Fail. 2012, 34, 165–170. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Ruperto, M.; Barril, G.; Sanchez-Muniz, F.J. Usefulness of the conicity index together with the conjoint use of adipocytokines and nutritional-inflammatory markers in hemodialysis patients. J. Physiol. Biochem. 2017, 73, 67–75. [Google Scholar] [CrossRef] [PubMed]
- Sanches, F.M.; Avesani, C.M.; Kamimura, M.A.; Lemos, M.M.; Axelsson, J.; Vasselai, P.; Draibe, S.A.; Cuppari, L. Waist circumference and visceral fat in CKD: A cross-sectional study. Am. J. Kidney Dis. 2008, 52, 66–73. [Google Scholar] [CrossRef] [PubMed]
- Norman, K.; Pirlich, M.; Sorensen, J.; Christensen, P.; Kemps, M.; Schutz, T.; Lochs, H.; Kondrup, J. Bioimpedance vector analysis as a measure of muscle function. Clin. Nutr. 2009, 28, 78–82. [Google Scholar] [CrossRef] [PubMed]
- Rosler, A.; Lehmann, F.; Krause, T.; Wirth, R.; von Renteln-Kruse, W. Nutritional and hydration status in elderly subjects: Clinical rating versus bioimpedance analysis. Arch. Gerontol. Geriatr. 2010, 50, e81–e85. [Google Scholar] [CrossRef]
- Hsiung, J.T.; Kleine, C.E.; Naderi, N.; Park, C.; Soohoo, M.; Moradi, H.; Rhee, C.M.; Obi, Y.; Kopple, J.D.; Kovesdy, C.P.; et al. Association of Pre-End-Stage Renal Disease Serum Albumin with Post-End-Stage Renal Disease Outcomes Among Patients Transitioning to Dialysis. J. Ren. Nutr. 2019, 29, 310–321. [Google Scholar] [CrossRef]
- Chen, C.; Zhang, J.; Zhou, Z.; Liu, J.; Li, C.; Liu, C. Impact of serum albumin level and variability on short-term cardiovascular-related and all-cause mortality in patients on maintenance hemodialysis. Medicine 2021, 100, e27666. [Google Scholar] [CrossRef]
- Rymarz, A.; Bartoszewicz, Z.; Szamotulska, K.; Niemczyk, S. The Associations Between Body Cell Mass and Nutritional and Inflammatory Markers in Patients with Chronic Kidney Disease and in Subjects Without Kidney Disease. J. Ren. Nutr. 2016, 26, 87–92. [Google Scholar] [CrossRef]
- Ikizler, T.A.; Burrowes, J.D.; Byham-Gray, L.D.; Campbell, K.L.; Carrero, J.J.; Chan, W.; Fouque, D.; Friedman, A.N.; Ghaddar, S.; Goldstein-Fuchs, D.J.; et al. KDOQI Clinical Practice Guideline for Nutrition in CKD: 2020 Update. Am. J. Kidney Dis. 2020, 76, S1–S107. [Google Scholar] [CrossRef]
- Onodera, T.; Goseki, N.; Kosaki, G. Prognostic nutritional index in gastrointestinal surgery of malnourished cancer patients. Nihon Geka Gakkai Zasshi 1984, 85, 1001–1005. [Google Scholar] [PubMed]
- Hu, X.; Deng, H.; Wang, Y.; Chen, L.; Gu, X.; Wang, X. Predictive value of the prognostic nutritional index for the severity of coronavirus disease 2019. Nutrition 2021, 84, 111123. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y.; Shen, J.; Liu, R.; Feng, Z.; Zhang, C.; Ling, L.; Chen, L. Prognostic value of pretreatment prognostic nutritional index in non-small cell lung cancer: A systematic review and meta-analysis. Int. J. Biol. Markers 2018, 33, 372–378. [Google Scholar] [CrossRef] [PubMed]
- Hua, X.; Long, Z.Q.; Huang, X.; Deng, J.P.; He, Z.Y.; Guo, L.; Zhang, W.W.; Lin, H.X. The Value of Prognostic Nutritional Index (PNI) in Predicting Survival and Guiding Radiotherapy of Patients with T1-2N1 Breast Cancer. Front. Oncol. 2019, 9, 1562. [Google Scholar] [CrossRef]
- Ardehali, S.H.; Eslamian, G.; Malek, S. Associations between systemic inflammation and intestinal permeability with Onodera’s prognostic nutritional index in critically ill patients. Acute Crit. Care 2021, 36, 361–368. [Google Scholar] [CrossRef]
- Ahn, S.S.; Jung, S.M.; Song, J.J.; Park, Y.B.; Lee, S.W. Prognostic nutritional index is associated with disease severity and relapse in ANCA-associated vasculitis. Int. J. Rheum. Dis. 2019, 22, 797–804. [Google Scholar] [CrossRef]
- Barutcu Atas, D.T.M.; Asicioglu, E.; Velioglu, A.; Arikan, H.; Koc, M.; Tuglular, S. Prognostic nutritional index is a predictor of mortality in elderly patients with chronic kidney disease. Int. Urol. Nephrol. 2022, 54, 1155–1162. [Google Scholar] [CrossRef]
- Inker, L.A.; Eneanya, N.D.; Coresh, J.; Tighiouart, H.; Wang, D.; Sang, Y.; Crews, D.C.; Doria, A.; Estrella, M.M.; Froissart, M.; et al. New Creatinine- and Cystatin C-Based Equations to Estimate GFR without Race. N. Engl. J. Med. 2021, 385, 1737–1749. [Google Scholar] [CrossRef]
- Kidney Disease Improving Global Outcomes (KDIGO) 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Int. Suppl. 2013, 3, 150.
- Esquius, M.; Schwartz, S.; Lopez Hellin, J.; Andreu, A.L.; Garcia, E. Anthropometric reference parameters for the aged population. Med. Clin. 1993, 100, 692–698. [Google Scholar]
- WHO. World Health Organization. Body Mass Index-BMI Classification. Available online: https://www.who.int/europe/news-room/fact-sheets/item/a-healthy-lifestyle---who-recommendation (accessed on 28 July 2022).
- World Health Organization WHO. Waist Circumference and Waist-Hip Ratio: Report of a WHO Expert Consultation. 2021. Available online: https://apps.who.int/iris/handle/10665/44583. (accessed on 28 July 2022).
- Valdez, R.; Seidell, J.C.; Ahn, Y.I.; Weiss, K.M. A new index of abdominal adiposity as an indicator of risk for cardiovascular disease. A cross-population study. Int. J. Obes. Relat. Metab. Disord. 1993, 17, 77–82. [Google Scholar] [PubMed]
- Valdez, R. A simple model-based index of abdominal adiposity. J. Clin. Epidemiol. 1991, 44, 955–956. [Google Scholar] [CrossRef]
- Wang, K.; Zelnick, L.R.; Chertow, G.M.; Himmelfarb, J.; Bansal, N. Body Composition Changes Following Dialysis Initiation and Cardiovascular and Mortality Outcomes in CRIC (Chronic Renal Insufficiency Cohort): A Bioimpedance Analysis Substudy. Kidney Med. 2021, 3, 327–334. [Google Scholar] [CrossRef] [PubMed]
- Lukaski, H.C.; Bolonchuk, W.W.; Hall, C.B.; Siders, W.A. Validation of tetrapolar bioelectrical impedance method to assess human body composition. J. Appl. Physiol. 1986, 60, 1327–1332. [Google Scholar] [CrossRef] [PubMed]
- Han, B.G.; Lee, J.Y.; Kim, J.S.; Yang, J.W. Decreased Bioimpedance Phase Angle in Patients with Diabetic Chronic Kidney Disease Stage 5. Nutrients 2019, 11, 2874. [Google Scholar] [CrossRef]
- Kang, S.H.; Cho, K.H.; Park, J.W.; Yoon, K.W.; Do, J.Y. Onodera’s prognostic nutritional index as a risk factor for mortality in peritoneal dialysis patients. J. Korean Med. Sci. 2012, 27, 1354–1358. [Google Scholar] [CrossRef]
- Kato, A.; Tsuji, T.; Sakao, Y.; Ohashi, N.; Yasuda, H.; Fujimoto, T.; Takita, T.; Furuhashi, M.; Kumagai, H. A comparison of systemic inflammation-based prognostic scores in patients on regular hemodialysis. Nephron Extra 2013, 3, 91–100. [Google Scholar] [CrossRef]
- Peng, F.; Chen, W.; Zhou, W.; Li, P.; Niu, H.; Chen, Y.; Zhu, Y.; Long, H. Low prognostic nutritional index associated with cardiovascular disease mortality in incident peritoneal dialysis patients. Int. Urol. Nephrol. 2017, 49, 1095–1101. [Google Scholar] [CrossRef]
- Hu, Y.; Cao, Q.; Wang, H.; Yang, Y.; Xiong, Y.; Li, X.; Zhou, Q. Prognostic nutritional index predicts acute kidney injury and mortality of patients in the coronary care unit. Exp. Ther. Med. 2021, 21, 123. [Google Scholar] [CrossRef]
- Couser, W.G.; Remuzzi, G.; Mendis, S.; Tonelli, M. The contribution of chronic kidney disease to the global burden of major noncommunicable diseases. Kidney Int. 2011, 80, 1258–1270. [Google Scholar] [CrossRef]
- Bikbov, B.; Purcell, C.A.; Levey, A.S.; Smith, M.; Abdoli, A.; Abebe, M.; Adebayo, O.M.; Afarideh, M.; Agarwal, S.K.; Agudelo-Botero, M.; et al. Global, regional, and national burden of chronic kidney disease, 1990-2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2020, 395, 709–733. [Google Scholar] [CrossRef]
- INE. Encuesta Europea de Salud 2020. MSCBS e INE. Available online: https://www.ine.es/jaxi/Datos.htm?path=/t00/ICV/Graficos/dim3/&file=331G2.px (accessed on 20 July 2022).
- Pinto-Sietsma, S.J.; Janssen, W.M.T.; Hillege, H.L.; Navis, G.; Zeeuw, D.; Jong, P.E. Urinary albumin excretion is associated with renal functional abnormalities in a nondiabetic population. J. Am. Soc. Nephrol. 2000, 11, 1882–1888. [Google Scholar] [CrossRef] [PubMed]
- Powell-Wiley, T.M.; Poirier, P.; Burke, L.E.; Despres, J.P.; Gordon-Larsen, P.; Lavie, C.J.; Lear, S.A.; Ndumele, C.E.; Neeland, I.J.; Sanders, P.; et al. Obesity and Cardiovascular Disease: A Scientific Statement from the American Heart Association. Circulation 2021, 143, e984–e1010. [Google Scholar] [CrossRef]
- Davis, E.; Campbell, K.; Gobe, G.; Hawley, C.; Isbel, N.; Johnson, D.W. Association of anthropometric measures with kidney disease progression and mortality: A retrospective cohort study of pre-dialysis chronic kidney disease patients referred to a specialist renal service. BMC Nephrol. 2016, 17, 74. [Google Scholar] [CrossRef]
- Han, B.G.; Lee, J.Y.; Kim, J.S.; Yang, J.W. Clinical Significance of Phase Angle in Non-Dialysis CKD Stage 5 and Peritoneal Dialysis Patients. Nutrients 2018, 10, 1331. [Google Scholar] [CrossRef]
- Vettoretti, S.; Caldiroli, L.; Armelloni, S.; Ferrari, C.; Cesari, M.; Messa, P. Sarcopenia is Associated with Malnutrition but Not with Systemic Inflammation in Older Persons with Advanced CKD. Nutrients 2019, 11, 1378. [Google Scholar] [CrossRef]
- Ruperto, M.; Sanchez-Muniz, F.J.; Barril, G. Predictors of protein-energy wasting in haemodialysis patients: A cross-sectional study. J. Hum. Nutr. Diet. 2014, 29, 38–47. [Google Scholar] [CrossRef]
- Tabinor, M.; Elphick, E.; Dudson, M.; Kwok, C.S.; Lambie, M.; Davies, S.J. Bioimpedance-defined overhydration predicts survival in end-stage kidney failure (ESKF): Systematic review and subgroup meta-analysis. Sci. Rep. 2018, 8, 4441. [Google Scholar] [CrossRef] [PubMed]
- Luo, Q.; Xia, X.; Li, B.; Lin, Z.; Yu, X.; Huang, F. Serum uric acid and cardiovascular mortality in chronic kidney disease: A meta-analysis. BMC Nephrol. 2019, 20, 18. [Google Scholar] [CrossRef]
- Chang, C.C.; Wu, C.H.; Liu, L.K.; Chou, R.H.; Kuo, C.S.; Huang, P.H.; Chen, L.K.; Lin, S.J. Association between serum uric acid and cardiovascular risk in nonhypertensive and nondiabetic individuals: The Taiwan I-Lan Longitudinal Aging Study. Sci. Rep. 2018, 8, 5234. [Google Scholar] [CrossRef]
- Menon, V.; Greene, T.; Wang, X.; Pereira, A.A.; Marcovina, S.M.; Beck, G.J.; Kusek, J.W.; Collins, A.J.; Levey, A.S.; Sarnak, M.J. C-reactive protein and albumin as predictors of all-cause and cardiovascular mortality in chronic kidney disease. Kidney Int. 2005, 68, 766–772. [Google Scholar] [CrossRef] [PubMed]
- Lang, J.; Katz, R.; Ix, J.H.; Gutierrez, O.M.; Peralta, C.A.; Parikh, C.R.; Satterfield, S.; Petrovic, S.; Devarajan, P.; Bennett, M.; et al. Association of serum albumin levels with kidney function decline and incident chronic kidney disease in elders. Nephrol. Dial. Transplant. 2018, 33, 986–992. [Google Scholar] [CrossRef] [PubMed]
- Don, B.R.; Kaysen, G. Serum albumin: Relationship to inflammation and nutrition. Semin. Dial. 2004, 17, 432–437. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | Total (n = 150) | ACKD (n = 75) | Controls (n = 75) | p-Value |
|---|---|---|---|---|
| Male, n (%) | 76 (50.66) | 38 (25.33) | 38 (25.33) | |
| Age (yrs) | 80.07 ± 6.62 | 79.72 ± 6.69 | 80.43 ± 6.57 | 0.450 |
| DM n; (%) | 22 (14.66) | 15 (20.00) | 7 (9.33) | <0.001 |
| BW (%) | 69.46 ± 13.04 | 69.23 ± 12.71 | 69.68 ± 13.43 | 0.830 |
| SBW (%) | 111.38 ± 21.51 | 110.05 ± 18.95 | 112.71 ± 23.84 | 0.560 |
| BMI (kg/m2) | 27.66 ± 5.61 | 26.58 ± 4.64 | 28.73 ± 6.28 | 0.018 |
| WC (cm) | 99.52 ± 12.52 | 97.83 ± 12.41 | 101.26 ± 12.48 | 0.095 |
| Conicity index | 1.38 ± 0.11 | 1.37 ± 0.11 | 1.40 ± 0.12 | 0.130 |
| TSF (%) | 138.68 ± 82.15 | 131.55 ± 71.77 | 145.81 ± 91.29 | 0.290 |
| MAMC (%) | 147.97 ± 29.88 | 148.95 ± 28.65 | 146.99 ± 31.23 | 0.159 |
| TBW (L) | 36.25 ± 6.43 | 37.11 ± 5.90 | 35.37 ± 6.87 | 0.100 |
| ECW (L) | 17.84 ± 4.01 | 20.11 ± 3.68 | 15.54 ± 2.86 | <0.001 |
| ICW (L) | 17.74 ± 3.82 | 17.12 ± 3.75 | 19.22 ± 3.63 | 0.010 |
| Exchangeable Na/K | 1.00 ± 0.25 | 1.10 ± 0.29 | 0.90 ± 0.17 | <0.001 |
| ECM (kg) | 1.12 ± 0.50 | 1.43 ± 0.46 | 0.80 ± 0.29 | <0.001 |
| BCM (kg) | 22.06 ± 5.56 | 19.49 ± 4.36 | 24.63 ± 5.46 | <0.001 |
| FM (kg) | 24.87 ± 9.82 | 22.78 ± 8.35 | 27.01 ± 10.77 | 0.008 |
| FFM (kg) | 44.94 ± 7.53 | 46.02 ± 7.15 | 43.84 ± 7.78 | 0.078 |
| MM (kg) | 29.08 ± 8.83 | 25.69 ± 6.56 | 32.62 ± 9.53 | <0.001 |
| PA (°) | 5.26 ± 1.00 | 4.51 ± 0.86 | 6.09 ± 0.97 | <0.001 |
| Variable | Total (n = 150) | ACKD (n = 75) | Controls (n = 75) | p-Value |
|---|---|---|---|---|
| *e-GFR (mL/min/1.73 m2) | 48.23 ± 35.07 | 14.44 ± 7.11 | 92.03 ± 10.60 | <0.001 |
| s-Creatinine (mg/dL) | 2.38 ± 1.73 | 3.82 ± 1.33 | 0.95 ± 0.28 | <0.001 |
| Uric acid (mg/dL) | 6.15 ± 1.97 | 7.40 ± 1.85 | 4.91 ± 1.14 | <0.001 |
| s-Calcium (mg/dL) | 9.25 ± 1.39 | 9.51 ± 0.81 | 8.11 ± 2.50 | <0.001 |
| s-Phosphorous (mg/dL) | 4.40 ± 0.67 | 4.69 ± 0.77 | 4.12 ± 0.39 | <0.001 |
| s-Potassium (mEq/L) | 4.75 ± 0.57 | 4.85 ± 0.63 | 4.64 ± 0.48 | 0.054 |
| s-Cholesterol (mg/dL) | 170.03 ± 34.21 | 174.03 ± 29.70 | 166.03 ± 37.97 | 0.153 |
| Total proteins (mg/dL) | 6.72 ± 0.67 | 7.02 ± 0.58 | 6.40 ± 0.61 | <0.001 |
| s-Albumin (mg/dL) | 4.04 ± 0.28 | 4.09 ± 0.27 | 3.98 ± 0.28 | 0.030 |
| s-CRP (mg/dL) | 0.71 ± 1.15 | 1.04 ± 1.31 | 0.38 ± 0.84 | <0.001 |
| Hemoglobin (g/dL) | 12.50 ± 1.22 | 12.43 ± 1.10 | 12.58 ± 1.33 | 0.466 |
| Lymphocytes count (×103/mm3) | 1823.72 ± 633.07 | 1730.14 ± 702.54 | 1916.05 ± 545.23 | 0.073 |
| PNI (points) | 49.35 ± 4.4 mediana | 49.27± 4.68 | 49.42 ± 4.13 | 0.828 |
| Variable | OR | St Error | CI95% | p-Value |
|---|---|---|---|---|
| BMI (kg/m2) | 0.933 | 0.028 | 0.285 to 0.088 | 0.027 |
| Conicity index | 0.100 | 0.153 | 0.005 to 2.010 | 0.133 |
| BCM (%) | 0.737 | 0.057 | 0.632 to 0.863 | <0.001 |
| ECM (kg) | 1.392 | 0.109 | 1.193 to 1.625 | <0.001 |
| TBW (%) | 1.078 | 0.030 | 1.020 to 1.138 | <0.001 |
| ECW(%) | 1.437 | 0.123 | 1.213 to 1.701 | <0.001 |
| ICW (%) | 0.686 | 0.062 | 0.573 to 0.822 | <0.001 |
| FM (%) | 0.941 | 0.021 | 0.904 to 0.984 | 0.008 |
| FFM (%) | 1.077 | 0.025 | 1.029 to 1.127 | <0.001 |
| MM (%) | 0.912 | 0.024 | 0.866 to 0.961 | 0.001 |
| PA (°) | 0.036 | 0.037 | 0.004 to 0.278 | <0.001 |
| Total proteins (g/dL) | 7.311 | 3.456 | 2.894 to 18.467 | <0.001 |
| Phosphorous (mg/dL) | 5.338 | 2.098 | 2.470 to 11.536 | <0.001 |
| s-Albumin (g/dL) | 0.289 | 0.411 | 0.072 to 1.149 | 0.072 |
| s-CRP (mg/dL) | 2.167 | 0.556 | 1.310 to 3.584 | 0.003 |
| Lymphocytes count (×103/mm3) | 0.999 | 0.0002 | 0.998 to 1.000 | 0.077 |
| Variable | OR | St Error | CI95% | p-Value |
|---|---|---|---|---|
| Total body water (%) | 1.186 | 0.061 | 1.076 to 1.314 | 0.001 |
| Extracellular mass (kg) | 1.346 | 0.106 | 1.153 to 1.572 | <0.001 |
| Muscle mass (%) | 0.847 | 0.037 | 0.776 to 0.922 | <0.001 |
| Phase angle (°) | 0.058 | 0.059 | 0.008 to 0.4201 | 0.005 |
| s-Albumin (g/dL) | 0.475 | 0.142 | 0.263 to 0.856 | 0.013 |
| s-CRP (mg/dL) | 2.050 | 0.577 | 1.180 to 3.561 | 0.011 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ruperto, M.; Barril, G. Nutritional Status, Body Composition, and Inflammation Profile in Older Patients with Advanced Chronic Kidney Disease Stage 4–5: A Case-Control Study. Nutrients 2022, 14, 3650. https://doi.org/10.3390/nu14173650
Ruperto M, Barril G. Nutritional Status, Body Composition, and Inflammation Profile in Older Patients with Advanced Chronic Kidney Disease Stage 4–5: A Case-Control Study. Nutrients. 2022; 14(17):3650. https://doi.org/10.3390/nu14173650
Chicago/Turabian StyleRuperto, Mar, and Guillermina Barril. 2022. "Nutritional Status, Body Composition, and Inflammation Profile in Older Patients with Advanced Chronic Kidney Disease Stage 4–5: A Case-Control Study" Nutrients 14, no. 17: 3650. https://doi.org/10.3390/nu14173650
APA StyleRuperto, M., & Barril, G. (2022). Nutritional Status, Body Composition, and Inflammation Profile in Older Patients with Advanced Chronic Kidney Disease Stage 4–5: A Case-Control Study. Nutrients, 14(17), 3650. https://doi.org/10.3390/nu14173650