
Biomarkers for Non-Invasive Stratification of Coronary Artery Disease and Prognostic Impact on Long-Term Survival in Patients with Stable Coronary Heart Disease

 , , , ,
, , , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Assessment of Traditional Cardiovascular Risk Factors and Coronary Status
2.3. Laboratory Analysis
2.4. Statistical Analysis
3. Result
3.1. Demographic Data and Clinical Characteristics of the Patient Cohort
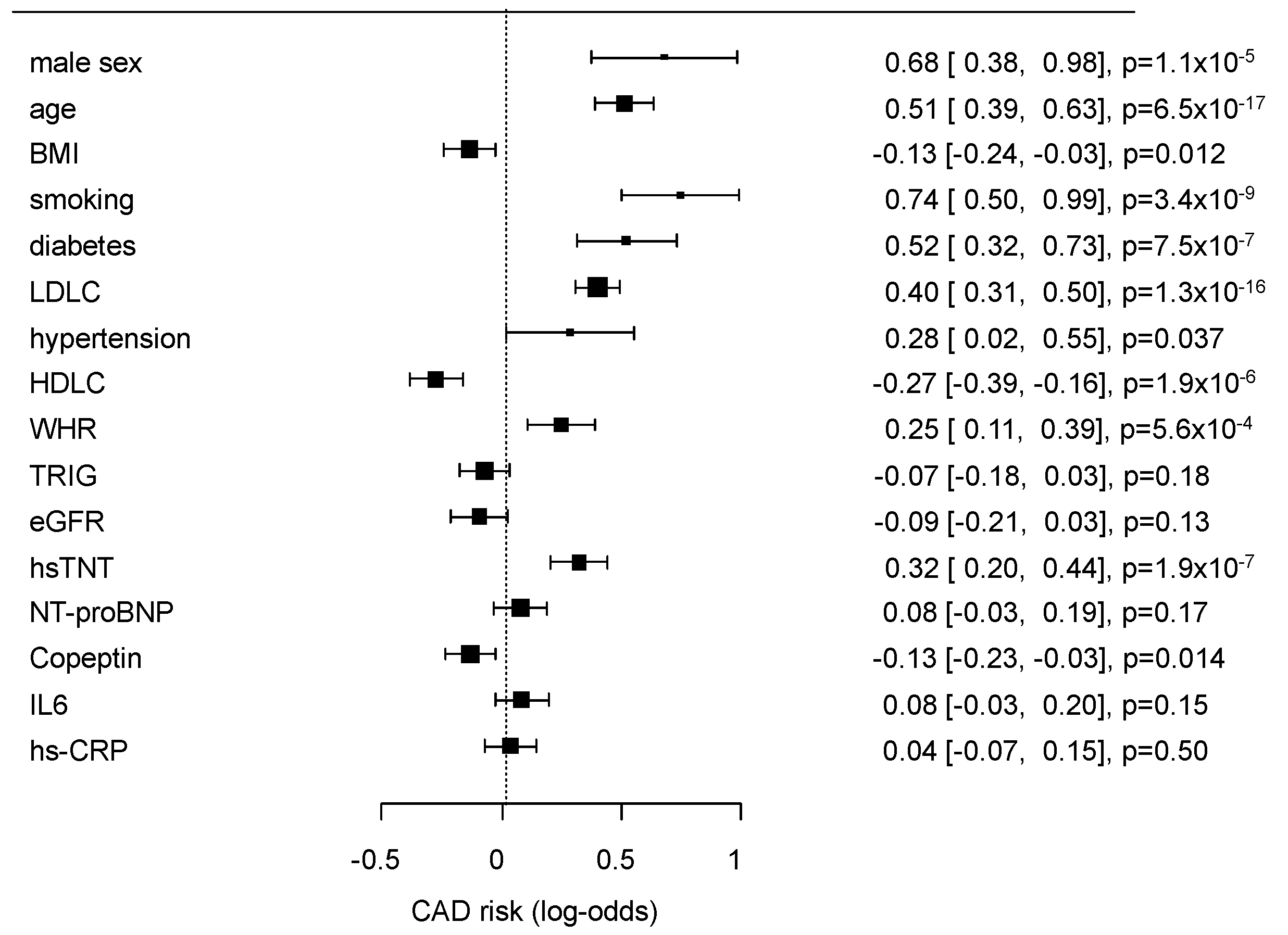
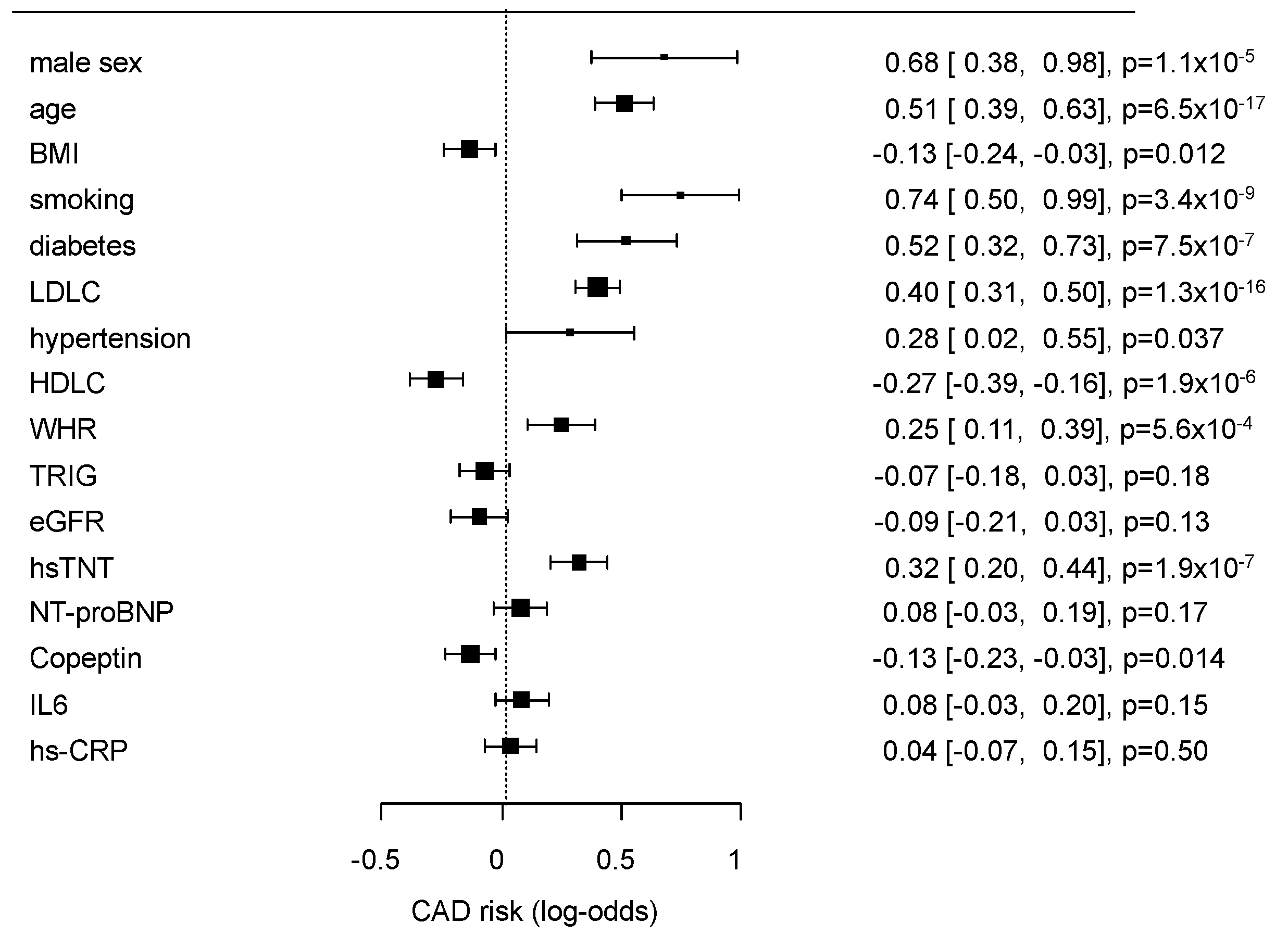
3.2. Biomarkers Indicating the Angiographic Presence of Coronary Artery Disease
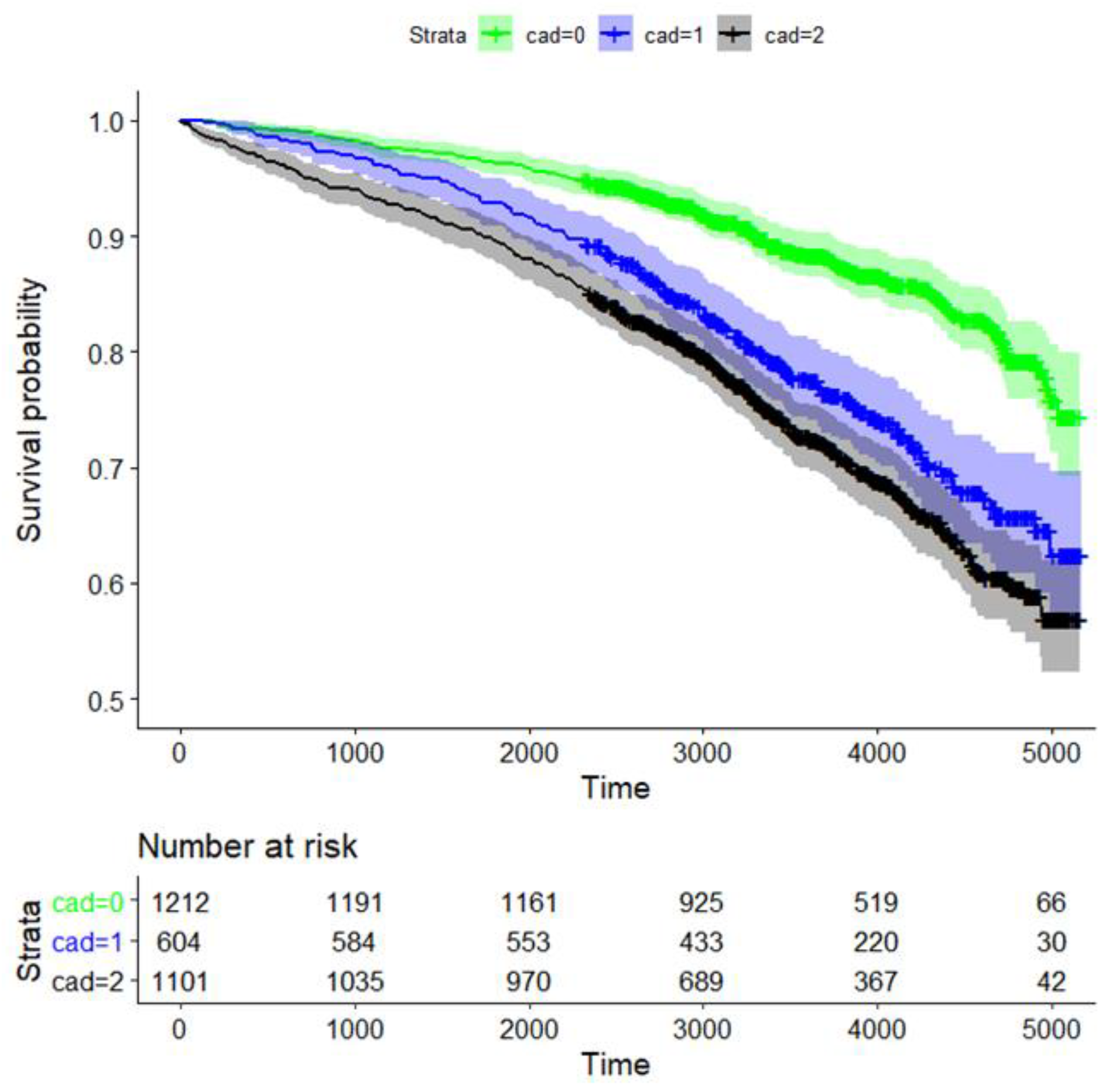
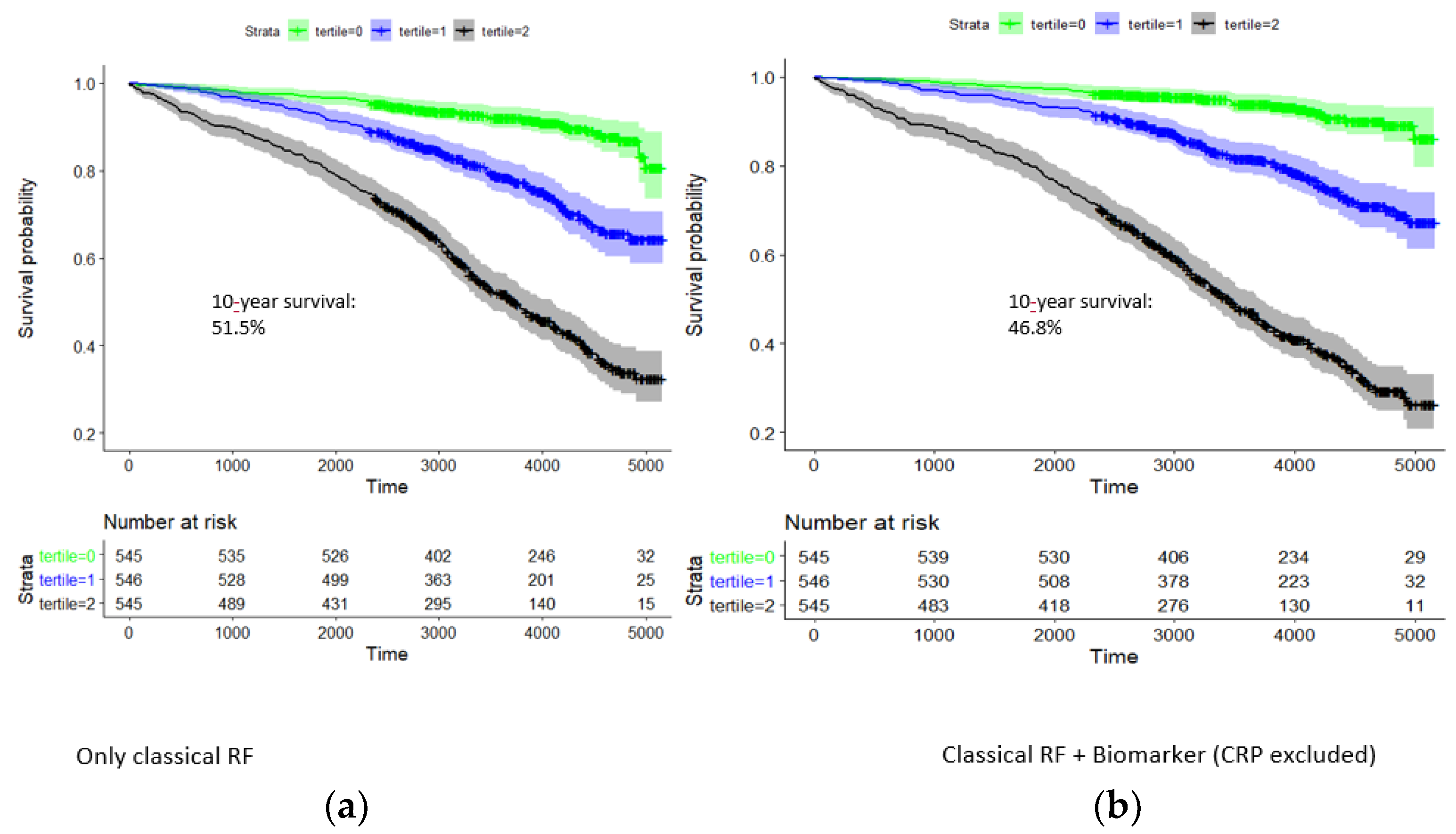
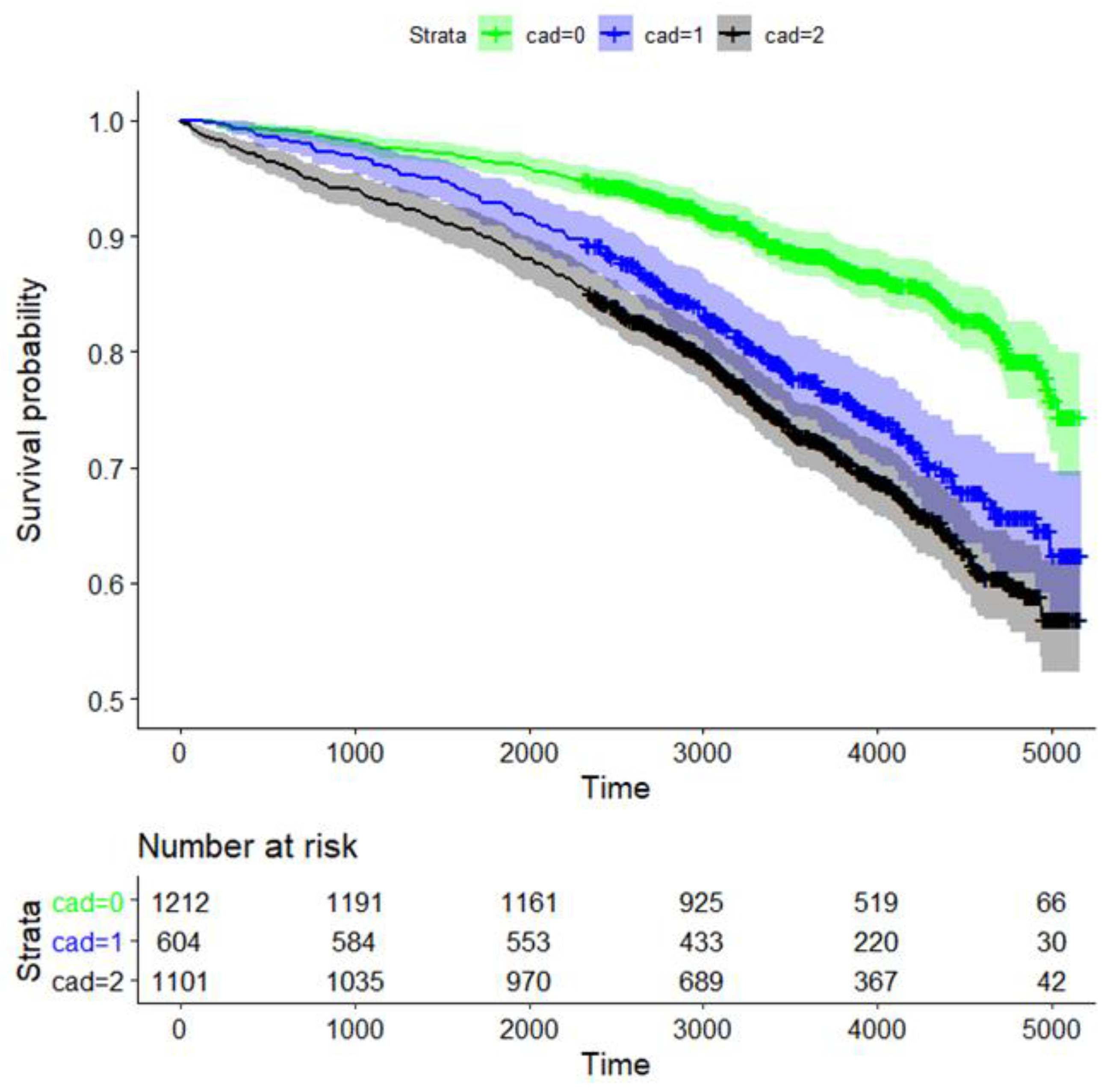
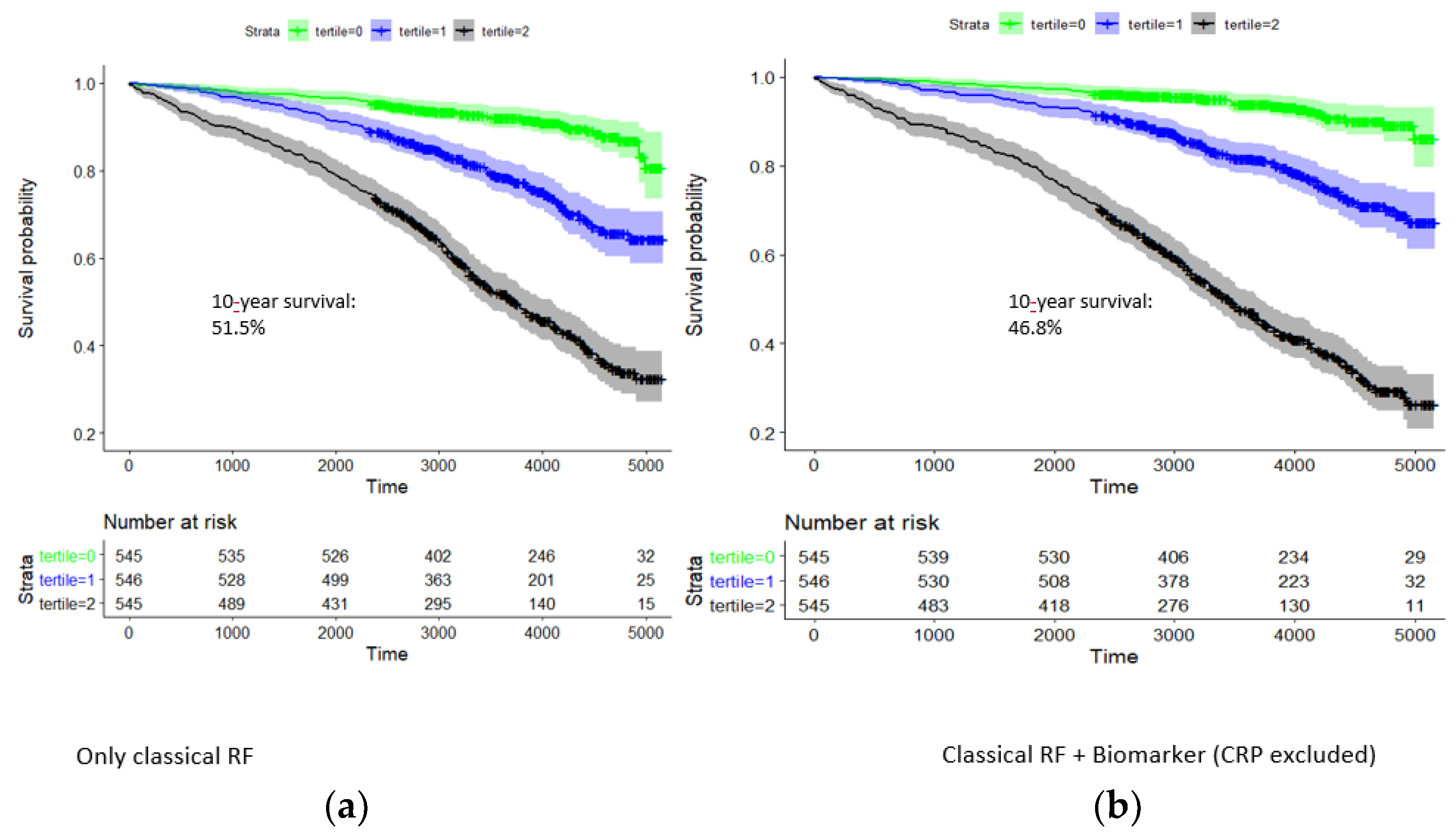
3.3. Selected Biomarkers Associated with Long-Term Mortality in Patients according to Coronary Artery Disease
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Piepoli, M.F.; Hoes, A.W.; Agewall, S.; Albus, C.; Brotons, C.; Catapano, A.L.; Cooney, M.-T.; Corrà, U.; Cosyns, B.; Deaton, C.; et al. 2016 European Guidelines on Cardiovascular Disease Prevention in Clinical Practice. Atherosclerosis 2016, 252, 207–274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collet, J.-P.; Thiele, H.; Barbato, E.; Barthélémy, O.; Bauersachs, J.; Bhatt, D.L.; Dendale, P.; Dorobantu, M.; Edvardsen, T.; Folliguet, T.; et al. 2020 ESC Guidelines for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation. Eur. Heart J. 2021, 42, 1289–1367. [Google Scholar] [CrossRef] [PubMed]
- Lyngbakken, M.N.; Myhre, P.L.; Røsjø, H.; Omland, T. Novel Biomarkers of Cardiovascular Disease: Applications in Clinical Practice. Crit. Rev. Clin. Lab. Sci. 2019, 56, 33–60. [Google Scholar] [CrossRef]
- Ridker, P.M.; Everett, B.M.; Thuren, T.; MacFadyen, J.G.; Chang, W.H.; Ballantyne, C.; Fonseca, F.; Nicolau, J.; Koenig, W.; Anker, S.D.; et al. Antiinflammatory Therapy with Canakinumab for Atherosclerotic Disease. N. Engl. J. Med. 2017, 377, 1119–1131. [Google Scholar] [CrossRef] [PubMed]
- Nidorf, S.M.; Fiolet, A.T.L.; Eikelboom, J.W.; Schut, A.; Opstal, T.S.J.; Bax, W.A.; Budgeon, C.A.; Tijssen, J.G.P.; Mosterd, A.; Cornel, J.H.; et al. The Effect of Low-Dose Colchicine in Patients with Stable Coronary Artery Disease: The LoDoCo2 Trial Rationale, Design, and Baseline Characteristics. Am. Heart J. 2019, 218, 46–56. [Google Scholar] [CrossRef]
- Chapman, A.R.; Lee, K.K.; McAllister, D.A.; Cullen, L.; Greenslade, J.H.; Parsonage, W.; Worster, A.; Kavsak, P.A.; Blankenberg, S.; Neumann, J.; et al. Association of High-Sensitivity Cardiac Troponin I Concentration with Cardiac Outcomes in Patients with Suspected Acute Coronary Syndrome. JAMA 2017, 318, 1913. [Google Scholar] [CrossRef] [PubMed]
- Patterson, C.C.; Blankenberg, S.; Ben-Shlomo, Y.; Heslop, L.; Bayer, A.; Lowe, G.; Zeller, T.; Gallacher, J.; Young, I.; Yarnell, J. Which Biomarkers Are Predictive Specifically for Cardiovascular or for Non-Cardiovascular Mortality in Men? Evidence from the Caerphilly Prospective Study (CaPS). Int. J. Cardiol. 2015, 201, 113–118. [Google Scholar] [CrossRef] [Green Version]
- Scholz, M.; Henger, S.; Beutner, F.; Teren, A.; Baber, R.; Willenberg, A.; Ceglarek, U.; Pott, J.; Burkhardt, R.; Thiery, J. Cohort Profile: The Leipzig Research Center for Civilization Diseases–Heart Study (LIFE-Heart). Int. J. Epidemiol. 2020, 49, 1439–1440. [Google Scholar] [CrossRef]
- Beutner, F.; Teupser, D.; Gielen, S.; Holdt, L.M.; Scholz, M.; Boudriot, E.; Schuler, G.; Thiery, J. Rationale and Design of the Leipzig (LIFE) Heart Study: Phenotyping and Cardiovascular Characteristics of Patients with Coronary Artery Disease. PLoS ONE 2011, 6, e29070. [Google Scholar] [CrossRef]
- Weissgerber, A.; Scholz, M.; Teren, A.; Sandri, M.; Teupser, D.; Gielen, S.; Thiery, J.; Schuler, G.; Beutner, F. The Value of Noncoronary Atherosclerosis for Identifying Coronary Artery Disease: Results of the Leipzig LIFE Heart Study. Clin. Res. Cardiol. 2016, 105, 172–181. [Google Scholar] [CrossRef] [Green Version]
- Loeffler, M.; Engel, C.; Ahnert, P.; Alfermann, D.; Arelin, K.; Baber, R.; Beutner, F.; Binder, H.; Brähler, E.; Burkhardt, R.; et al. The LIFE-Adult-Study: Objectives and Design of a Population-Based Cohort Study with 10,000 Deeply Phenotyped Adults in Germany. BMC Public Health 2015, 15, 691. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beatty, A.L.; Ku, I.A.; Christenson, R.H.; DeFilippi, C.R.; Schiller, N.B.; Whooley, M.A. High-Sensitivity Cardiac Troponin T Levels and Secondary Events in Outpatients with Coronary Heart Disease from the Heart and Soul Study. JAMA Intern. Med. 2013, 173, 763. [Google Scholar] [CrossRef] [PubMed]
- Adamson, P.D.; Hunter, A.; Madsen, D.M.; Shah, A.S.V.; McAllister, D.A.; Pawade, T.A.; Williams, M.C.; Berry, C.; Boon, N.A.; Flather, M.; et al. High-Sensitivity Cardiac Troponin I and the Diagnosis of Coronary Artery Disease in Patients with Suspected Angina Pectoris. Circ. Cardiovasc. Qual. Outcomes 2018, 11, e004227. [Google Scholar] [CrossRef] [PubMed]
- Mohebi, R.; Jackson, L.; McCarthy, C.P.; Murtagh, G.; Murphy, S.P.; Abboud, A.; Miksenas, H.; Gaggin, H.K.; Januzzi, J.L. Relation of High-Sensitivity Cardiac Troponin I and Obstructive Coronary Artery Disease in Patients without Acute Myocardial Infarction. Am. J. Cardiol. 2022, 173, 16–24. [Google Scholar] [CrossRef]
- Bae, Y.J.; Reinelt, J.; Netto, J.; Uhlig, M.; Willenberg, A.; Ceglarek, U.; Villringer, A.; Thiery, J.; Gaebler, M.; Kratzsch, J. Salivary Cortisone, as a Biomarker for Psychosocial Stress, Is Associated with State Anxiety and Heart Rate. Psychoneuroendocrinology 2019, 101, 35–41. [Google Scholar] [CrossRef]
- Nickel, C.H.; Bingisser, R.; Morgenthaler, N.G. The Role of Copeptin as a Diagnostic and Prognostic Biomarker for Risk Stratification in the Emergency Department. BMC Med. 2012, 10, 7. [Google Scholar] [CrossRef] [Green Version]
- Land, H.; Schütz, G.; Schmale, H.; Richter, D. Nucleotide Sequence of Cloned CDNA Encoding Bovine Arginine Vasopressin–Neurophysin II Precursor. Nature 1982, 295, 299–303. [Google Scholar] [CrossRef]
- Schneider, C.; Remmler, J.; Netto, J.; Seehofer, D.; Engelmann, C.; Berg, T.; Thiery, J.; Kaiser, T. Copeptin—A Biomarker of Short-Term Mortality Risk (7 Days) in Patients with End-Stage Liver Disease. Clin. Chem. Lab. Med. 2019, 57, 1897–1905. [Google Scholar] [CrossRef]
- Reichlin, T.; Hochholzer, W.; Stelzig, C.; Laule, K.; Freidank, H.; Morgenthaler, N.G.; Bergmann, A.; Potocki, M.; Noveanu, M.; Breidthardt, T.; et al. Incremental Value of Copeptin for Rapid Rule Out of Acute Myocardial Infarction. J. Am. Coll. Cardiol. 2009, 54, 60–68. [Google Scholar] [CrossRef] [Green Version]
- Leclercq, F.; Iemmi, A.; Kusters, N.; Lattuca, B.; Cayla, G.; Macia, J.-C.; Roubille, F.; Akodad, M.; Cristol, J.-P.; Dupuy, A.-M. Copeptin and High-Sensitivity Cardiac Troponin to Exclude Severe Coronary Stenosis in Patients with Chest Pain and Coronary Artery Disease. Am. J. Emerg. Med. 2016, 34, 493–498. [Google Scholar] [CrossRef]
- Libby, P.; Loscalzo, J.; Ridker, P.M.; Farkouh, M.E.; Hsue, P.Y.; Fuster, V.; Hasan, A.A.; Amar, S. Inflammation, Immunity, and Infection in Atherothrombosis. J. Am. Coll. Cardiol. 2018, 72, 2071–2081. [Google Scholar] [CrossRef]
- Libby, P. Inflammation in Atherosclerosis. Nature 2002, 420, 868–874. [Google Scholar] [CrossRef] [PubMed]
- Elliott, P. Genetic Loci Associated with C-Reactive Protein Levels and Risk of Coronary Heart Disease. JAMA 2009, 302, 37. [Google Scholar] [CrossRef] [Green Version]
- Ridker, P.M.; Rane, M. Interleukin-6 Signaling and Anti-Interleukin-6 Therapeutics in Cardiovascular Disease. Circ. Res. 2021, 128, 1728–1746. [Google Scholar] [CrossRef] [PubMed]
- Winkelmann, B.R.; März, W.; Boehm, B.O.; Zotz, R.; Hager, J.; Hellstern, P.; Senges, J. Rationale and Design of the LURIC Study—A Resource for Functional Genomics, Pharmacogenomics and Long-Term Prognosis of Cardiovascular Disease. Pharmacogenomics 2001, 2, S1–S73. [Google Scholar] [CrossRef] [PubMed]
- Giannitsis, E.; Spanuth, E.; Horsch, A.; Kleber, M.E.; Koch, W.; Grammer, T.B.; Koenig, W.; März, W. High-Sensitivity Cardiac Troponin T and N-Terminal pro-B-Type Natriuretic Peptide Predict Mortality in Stable Coronary Artery Disease: Results from the Ludwigshafen Risk and Cardiovascular Health (LURIC) Study. Clin. Chem. Lab. Med. 2013, 51, 2019–2028. [Google Scholar] [CrossRef]
- Krohn, J.B.; Nguyen, Y.N.; Akhavanpoor, M.; Erbel, C.; Domschke, G.; Linden, F.; Kleber, M.E.; Delgado, G.; März, W.; Katus, H.A.; et al. Identification of Specific Coronary Artery Disease Phenotypes Implicating Differential Pathophysiologies. Front. Cardiovasc. Med. 2022, 9, 778206. [Google Scholar] [CrossRef]
- Nikorowitsch, J.; Ojeda, F.; Lackner, K.J.; Schnabel, R.B.; Blankenberg, S.; Zeller, T.; Karakas, M. Head-to-Head Comparison of the Incremental Predictive Value of The Three Established Risk Markers, Hs-Troponin I, C-Reactive Protein, and NT-ProBNP, in Coronary Artery Disease. Biomolecules 2020, 10, 394. [Google Scholar] [CrossRef] [Green Version]
- Scicchitano, P.; Marzullo, A.; Santoro, A.; Zito, A.; Cortese, F.; Galeandro, C.; Ciccone, A.S.; Angiletta, D.; Manca, F.; Pulli, R.; et al. The Prognostic Role of ST2L and SST2 in Patients Who Underwent Carotid Plaque Endarterectomy: A Five-Year Follow-Up Study. J. Clin. Med. 2022, 11, 3142. [Google Scholar] [CrossRef]
- Marzullo, A.; Ambrosi, F.; Inchingolo, M.; Manca, F.; Devito, F.; Angiletta, D.; Zito, A.; Scicchitano, P.; Ciccone, M.M. ST2L Transmembrane Receptor Expression: An Immunochemical Study on Endarterectomy Samples. PLoS ONE 2016, 11, e0156315. [Google Scholar] [CrossRef]
- Januzzi, J.L.; Zannad, F.; Anker, S.D.; Butler, J.; Filippatos, G.; Pocock, S.J.; Ferreira, J.P.; Sattar, N.; Verma, S.; Vedin, O.; et al. Prognostic Importance of NT-ProBNP and Effect of Empagliflozin in the EMPEROR-Reduced Trial. J. Am. Coll. Cardiol. 2021, 78, 1321–1332. [Google Scholar] [CrossRef] [PubMed]
- Damman, K.; Beusekamp, J.C.; Boorsma, E.M.; Swart, H.P.; Smilde, T.D.J.; Elvan, A.; van Eck, J.W.M.; Heerspink, H.J.L.; Voors, A.A. Randomized, Double-Blind, Placebo-Controlled, Multicentre Pilot Study on the Effects of Empagliflozin on Clinical Outcomes in Patients with Acute Decompensated Heart Failure (EMPA-RESPONSE-AHF). Eur. J. Heart Fail. 2020, 22, 713–722. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanaka, A.; Hisauchi, I.; Taguchi, I.; Sezai, A.; Toyoda, S.; Tomiyama, H.; Sata, M.; Ueda, S.; Oyama, J.-I.; Kitakaze, M.; et al. Effects of Canagliflozin in Patients with Type 2 Diabetes and Chronic Heart Failure: A Randomized Trial (CANDLE). ESC Hear. Fail. 2020, 7, 1585–1594. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Demographic Data, Classical Risk Factors, and Selected Biomarkers of the Studied CAD Cohorts | ||||||||
|---|---|---|---|---|---|---|---|---|
| Characteristics | No CAD a | CAD < 50 | CAD ≥ 50 | CAD0 + CAD1 vs. CAD2 (GC1) k | CAD0 vs. CAD1 + CAD2 (GC2) l | |||
| Median | 25–75 p | Median | 25–75 p | Median | 25–75 p | |||
| N (%) | 1271 | 41.4% | 631 | 20.5% | 1170 | 38.1% | ||
| Sex (N)/Male | 634 | 49.9% | 419 | 66.4% | 913 | 78.0% | <0.001 | <0.001 |
| Female | 637 | 50.1% | 212 | 33.6% | 257 | 22.0% | ||
| Age (years) | 58.8 | 51.2–67.7 | 65.2 | 57.2–71.8 | 65.4 | 57.0–71.7 | <0.001 | <0.001 |
| BMI b (kg/m²) | 28.9 | 25.6–32.6 | 29.7 | 26.9–33.0 | 28.9 | 26.3–32.4 | 0.370 | 0.033 |
| Waist-to-hip ratio | 0.94 | 0.88–1.02 | 0.99 | 0.92–1.04 | 1.01 | 0.95–1.05 | <0.001 | <0.001 |
| Diabetes c (N) | 264 | 20.8% | 221 | 35.0% | 439 | 37.5% | <0.001 | <0.001 |
| Family history with MI d (N) | 304 | 23.9% | 138 | 21.9% | 323 | 27.6% | 0.007 | 0.289 |
| Hypertension (N) | 1040 | 81.8% | 578 | 91.6% | 1044 | 89.2% | 0.002 | <0.001 |
| Antihypertension medication e (N) | 1008 | 79.3% | 562 | 89.1% | 1017 | 86.9% | 0.001 | <0.001 |
| Lipid lowering medication f (N) | 359 | 28.2% | 256 | 40.6% | 504 | 43.1% | <0.001 | <0.001 |
| Current smoker (N) | 212 | 16.7% | 124 | 19.7% | 275 | 23.5% | <0.001 | 0.001 |
| Leukocytes | 6.80 | 5.60–8.10 | 7.00 | 5.90–8.40 | 7.20 | 6.00–8.60 | <0.001 | <0.001 |
| Total cholesterol (mmol/L) | 5.40 | 4.73–6.14 | 5.29 | 4.54–6.17 | 5.47 | 4.62–6.36 | 0.057 | 0.890 |
| LDL-cholesterol i (mmol/L) | 3.24 | 2.60–3.88 | 3.20 | 2.58–3.89 | 3.43 | 2.66–4.23 | <0.001 | 0.004 |
| HDL-cholesterol j (mmol/L) | 1.38 | 1.14–1.70 | 1.26 | 1.04–1.55 | 1.22 | 1.01–1.48 | <0.001 | <0.001 |
| Triglycerides (mmol/L) | 1.57 | 1.07–2.30 | 1.70 | 1.19–2.44 | 1.74 | 1.27–2.48 | <0.001 | <0.001 |
| Creatinine (μmoL) | 74.0 | 64.0–84.0 | 79.0 | 68.0–90.0 | 80.0 | 70.0–92.0 | <0.001 | <0.001 |
| eGFR g (in mL/min/1.73 m²) | 89.34 | 76.57–98.54 | 84.30 | 70.06–95.04 | 83.54 | 70.22–94.73 | <0.001 | <0.001 |
| Selected Biomarkers | ||||||||
| Troponin T (pg/mL) | 5.55 | 3.33–9.28 | 8.02 | 5.14–13.26 | 10.10 | 6.48–17.34 | <0.001 | <0.001 |
| NT-pro BNP h (pg/mL) | 98.6 | 46.0–218.2 | 132.1 | 60.8–353.4 | 173.5 | 75.5–463.8 | <0.001 | <0.001 |
| CRP (mg/L) | 1.83 | 0.97–3.87 | 2.39 | 1.16–4.77 | 2.41 | 1.14–5.16 | <0.001 | <0.001 |
| Interleukin-6 (pg/mL) | 2.01 | 1.50–3.69 | 2.67 | 1.55–4.54 | 3.04 | 1.73–5.91 | <0.001 | <0.001 |
| Copeptin (pmol/L) | 4.44 | 2.90–7.19 | 5.45 | 3.38–8.90 | 5.87 | 3.76–10.12 | <0.001 | <0.001 |
| Univariate (All) | Multivariate (All) | ||||||
|---|---|---|---|---|---|---|---|
| Biomarker | Beta | SE | Pval | Biomarker | Beta | SE | Pval |
| hsTNT | 0.522 | 0.0772 | 1.39 × 10−11 | hsTNT | 0.453 | 0.0871 | 1.91 × 10−7 |
| NT-proBNP | 0.156 | 0.0362 | 1.57 × 10−5 | NT-proBNP | 0.0566 | 0.0416 | 0.173 |
| Copeptin | −0.0933 | 0.069 | 0.176 | Copeptin | −0.182 | 0.0739 | 0.0138 |
| IL6 | 0.229 | 0.0659 | 0.000521 | IL6 | 0.116 | 0.0805 | 0.151 |
| hs-CRP | 0.121 | 0.0432 | 0.00524 | hs-CRP | 0.0344 | 0.0516 | 0.505 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Netto, J.; Teren, A.; Burkhardt, R.; Willenberg, A.; Beutner, F.; Henger, S.; Schuler, G.; Thiele, H.; Isermann, B.; Thiery, J.; et al. Biomarkers for Non-Invasive Stratification of Coronary Artery Disease and Prognostic Impact on Long-Term Survival in Patients with Stable Coronary Heart Disease. Nutrients 2022, 14, 3433. https://doi.org/10.3390/nu14163433
Netto J, Teren A, Burkhardt R, Willenberg A, Beutner F, Henger S, Schuler G, Thiele H, Isermann B, Thiery J, et al. Biomarkers for Non-Invasive Stratification of Coronary Artery Disease and Prognostic Impact on Long-Term Survival in Patients with Stable Coronary Heart Disease. Nutrients. 2022; 14(16):3433. https://doi.org/10.3390/nu14163433
Chicago/Turabian StyleNetto, Jeffrey, Andrej Teren, Ralph Burkhardt, Anja Willenberg, Frank Beutner, Sylvia Henger, Gerhard Schuler, Holger Thiele, Berend Isermann, Joachim Thiery, and et al. 2022. "Biomarkers for Non-Invasive Stratification of Coronary Artery Disease and Prognostic Impact on Long-Term Survival in Patients with Stable Coronary Heart Disease" Nutrients 14, no. 16: 3433. https://doi.org/10.3390/nu14163433
APA StyleNetto, J., Teren, A., Burkhardt, R., Willenberg, A., Beutner, F., Henger, S., Schuler, G., Thiele, H., Isermann, B., Thiery, J., Scholz, M., & Kaiser, T. (2022). Biomarkers for Non-Invasive Stratification of Coronary Artery Disease and Prognostic Impact on Long-Term Survival in Patients with Stable Coronary Heart Disease. Nutrients, 14(16), 3433. https://doi.org/10.3390/nu14163433