
Geographical and Temporal Variability of Ultra-Processed Food Consumption in the Spanish Population: Findings from the DRECE Study

 , and
, and
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Design and Participants
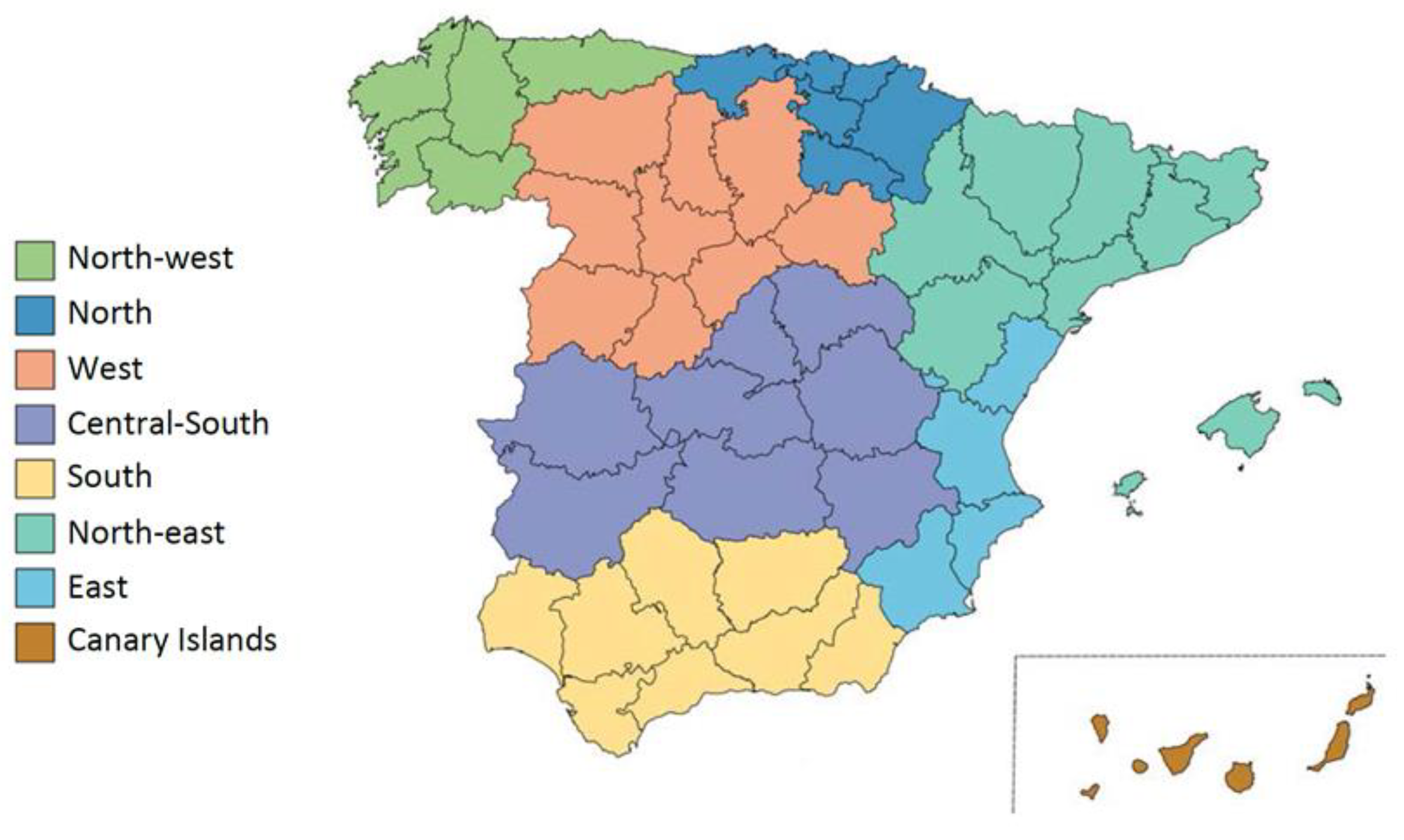
2.2. Geographical Areas
2.3. Dietary Assessment
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mendis, S.; Davis, S.; Norrving, B. Organizational Update: The World Health Organization Global Status Report on Noncommunicable Diseases 2014; One More Landmark Step in the Combat against Stroke and Vascular Disease. Stroke 2015, 46, e121–e122. [Google Scholar] [CrossRef] [PubMed]
- United Nations Political Declaration of the High-Level Meeting of the General Assembly on the Prevention and Control of Non-Communicable Diseases 2011. Available online: https://digitallibrary.un.org/record/710899/ (accessed on 28 May 2022).
- Cena, H.; Calder, P.C. Defining a Healthy Diet: Evidence for the Role of Contemporary Dietary Patterns in Health and Disease. Nutrients 2020, 12, 334. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hawkes, C. Food Policies for Healthy Populations and Healthy Economies. BMJ 2012, 344, e2801. [Google Scholar] [CrossRef]
- Monteiro, C.A. Nutrition and Health. The Issue Is Not Food, nor Nutrients, so Much as Processing. Public Health Nutr. 2009, 12, 729–731. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Diet, Nutrition, and the Prevention of Chronic Diseases: Report of a WHO-FAO Expert Consultation; [Joint WHO-FAO Expert Consultation on Diet, Nutrition, and the Prevention of Chronic Diseases, 2002, Geneva, Switzerland]; WHO Technical Report Series; World Health Organization: Geneva, Switzerland, 2003; ISBN 978-92-4-120916-8. [Google Scholar]
- Wiseman, M.; Cannon, G.; Butrum, R.; Martin, G.; Higginbotham, S.; Jones, C.; Fletcher, M. Policy and Action for Cancer Prevention. Food, Nutrition and Physical Activity: A Global Perspective; World Cancer Research Fund/American Institute for Cancer Research: London, UK, 2009. [Google Scholar]
- Stuckler, D.; McKee, M.; Ebrahim, S.; Basu, S. Manufacturing Epidemics: The Role of Global Producers in Increased Consumption of Unhealthy Commodities Including Processed Foods, Alcohol, and Tobacco. PLoS Med. 2012, 9, e1001235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Monteiro, C.A.; Cannon, G.; Levy, R.; Moubarac, J.-C.; Jaime, P.; Martins, A.P.; Canella, D.; Louzada, M.; Parra, D. NOVA. The Star Shines Bright. World Nutr. 2016, 7, 28–38. [Google Scholar]
- Monteiro, C.A.; Cannon, G.; Levy, R.B.; Moubarac, J.-C.; Louzada, M.L.; Rauber, F.; Khandpur, N.; Cediel, G.; Neri, D.; Martinez-Steele, E.; et al. Ultra-Processed Foods: What They Are and How to Identify Them. Public Health Nutr. 2019, 22, 936–941. [Google Scholar] [CrossRef] [PubMed]
- Moubarac, J.-C.; Batal, M.; Louzada, M.L.; Martinez Steele, E.; Monteiro, C.A. Consumption of Ultra-Processed Foods Predicts Diet Quality in Canada. Appetite 2017, 108, 512–520. [Google Scholar] [CrossRef]
- Martínez Steele, E.; Popkin, B.M.; Swinburn, B.; Monteiro, C.A. The Share of Ultra-Processed Foods and the Overall Nutritional Quality of Diets in the US: Evidence from a Nationally Representative Cross-Sectional Study. Popul. Health Metr. 2017, 15, 6. [Google Scholar] [CrossRef] [Green Version]
- da Costa Louzada, M.L.; Ricardo, C.Z.; Steele, E.M.; Levy, R.B.; Cannon, G.; Monteiro, C.A. The Share of Ultra-Processed Foods Determines the Overall Nutritional Quality of Diets in Brazil. Public Health Nutr. 2018, 21, 94–102. [Google Scholar] [CrossRef] [Green Version]
- Marrón-Ponce, J.A.; Flores, M.; Cediel, G.; Monteiro, C.A.; Batis, C. Associations between Consumption of Ultra-Processed Foods and Intake of Nutrients Related to Chronic Non-Communicable Diseases in Mexico. J. Acad. Nutr. Diet. 2019, 119, 1852–1865. [Google Scholar] [CrossRef] [PubMed]
- Parra, D.C.; da Costa-Louzada, M.L.; Moubarac, J.-C.; Bertazzi-Levy, R.; Khandpur, N.; Cediel, G.; Monteiro, C.A. Association between Ultra-Processed Food Consumption and the Nutrient Profile of the Colombian Diet in 2005. Salud Publica Mex. 2019, 61, 147–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elizabeth, L.; Machado, P.; Zinöcker, M.; Baker, P.; Lawrence, M. Ultra-Processed Foods and Health Outcomes: A Narrative Review. Nutrients 2020, 12, 1955. [Google Scholar] [CrossRef] [PubMed]
- Kelly, B.; Jacoby, E. Public Health Nutrition Special Issue on Ultra-Processed Foods. Public Health Nutr. 2018, 21, 1–4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Casas, R. Moving towards a Healthier Dietary Pattern Free of Ultra-Processed Foods. Nutrients 2022, 14, 118. [Google Scholar] [CrossRef]
- Martínez Steele, E.; Baraldi, L.G.; da Costa Louzada, M.L.; Moubarac, J.-C.; Mozaffarian, D.; Monteiro, C.A. Ultra-Processed Foods and Added Sugars in the US Diet: Evidence from a Nationally Representative Cross-Sectional Study. BMJ Open 2016, 6, e009892. [Google Scholar] [CrossRef] [Green Version]
- Rauber, F.; da Costa Louzada, M.L.; Steele, E.M.; Millett, C.; Monteiro, C.A.; Levy, R.B. Ultra-Processed Food Consumption and Chronic Non-Communicable Diseases-Related Dietary Nutrient Profile in the UK (2008–2014). Nutrients 2018, 10, 587. [Google Scholar] [CrossRef] [Green Version]
- Moodie, R.; Stuckler, D.; Monteiro, C.; Sheron, N.; Neal, B.; Thamarangsi, T.; Lincoln, P.; Casswell, S.; Lancet NCD Action Group. Profits and Pandemics: Prevention of Harmful Effects of Tobacco, Alcohol, and Ultra-Processed Food and Drink Industries. Lancet 2013, 381, 670–679. [Google Scholar] [CrossRef]
- Moubarac, J.-C.; Martins, A.P.B.; Claro, R.M.; Levy, R.B.; Cannon, G.; Monteiro, C.A. Consumption of Ultra-Processed Foods and Likely Impact on Human Health. Evidence from Canada. Public Health Nutr. 2013, 16, 2240–2248. [Google Scholar] [CrossRef] [Green Version]
- Adams, J.; White, M. Characterisation of UK Diets According to Degree of Food Processing and Associations with Socio-Demographics and Obesity: Cross-Sectional Analysis of UK National Diet and Nutrition Survey (2008–12). Int. J. Behav. Nutr. Phys. Act. 2015, 12, 160. [Google Scholar] [CrossRef] [Green Version]
- Batal, M.; Johnson-Down, L.; Moubarac, J.-C.; Ing, A.; Fediuk, K.; Sadik, T.; Tikhonov, C.; Chan, L.; Willows, N. Quantifying Associations of the Dietary Share of Ultra-Processed Foods with Overall Diet Quality in First Nations Peoples in the Canadian Provinces of British Columbia, Alberta, Manitoba and Ontario. Public Health Nutr. 2018, 21, 103–113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bielemann, R.M.; Motta, J.V.S.; Minten, G.C.; Horta, B.L.; Gigante, D.P. Consumption of Ultra-Processed Foods and Their Impact on the Diet of Young Adults. Rev. Saude Publica 2015, 49, 28. [Google Scholar] [CrossRef]
- Cediel, G.; Reyes, M.; da Costa Louzada, M.L.; Martinez Steele, E.; Monteiro, C.A.; Corvalán, C.; Uauy, R. Ultra-Processed Foods and Added Sugars in the Chilean Diet (2010). Public Health Nutr. 2018, 21, 125–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cornwell, B.; Villamor, E.; Mora-Plazas, M.; Marin, C.; Monteiro, C.A.; Baylin, A. Processed and Ultra-Processed Foods Are Associated with Lower-Quality Nutrient Profiles in Children from Colombia. Public Health Nutr. 2018, 21, 142–147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vandevijvere, S.; De Ridder, K.; Fiolet, T.; Bel, S.; Tafforeau, J. Consumption of Ultra-Processed Food Products and Diet Quality among Children, Adolescents and Adults in Belgium. Eur. J. Nutr. 2019, 58, 3267–3278. [Google Scholar] [CrossRef] [PubMed]
- Juul, F.; Martinez-Steele, E.; Parekh, N.; Monteiro, C.A.; Chang, V.W. Ultra-Processed Food Consumption and Excess Weight among US Adults. Br. J. Nutr. 2018, 120, 90–100. [Google Scholar] [CrossRef] [Green Version]
- Nardocci, M.; Leclerc, B.-S.; Louzada, M.-L.; Monteiro, C.A.; Batal, M.; Moubarac, J.-C. Consumption of Ultra-Processed Foods and Obesity in Canada. Can. J. Public Health 2019, 110, 4–14. [Google Scholar] [CrossRef]
- Julia, C.; Martinez, L.; Allès, B.; Touvier, M.; Hercberg, S.; Méjean, C.; Kesse-Guyot, E. Contribution of Ultra-Processed Foods in the Diet of Adults from the French NutriNet-Santé Study. Public Health Nutr. 2018, 21, 27–37. [Google Scholar] [CrossRef] [Green Version]
- da Costa Louzada, M.L.; Baraldi, L.G.; Steele, E.M.; Martins, A.P.B.; Canella, D.S.; Moubarac, J.-C.; Levy, R.B.; Cannon, G.; Afshin, A.; Imamura, F.; et al. Consumption of Ultra-Processed Foods and Obesity in Brazilian Adolescents and Adults. Prev. Med. 2015, 81, 9–15. [Google Scholar] [CrossRef] [Green Version]
- Canella, D.S.; Levy, R.B.; Martins, A.P.B.; Claro, R.M.; Moubarac, J.-C.; Baraldi, L.G.; Cannon, G.; Monteiro, C.A. Ultra-Processed Food Products and Obesity in Brazilian Households (2008–2009). PLoS ONE 2014, 9, e92752. [Google Scholar] [CrossRef] [Green Version]
- Pan American Health Organization. Ultra-Processed Food and Drink Products in Latin America: Trends, Impact on Obesity, Policy Implications. Available online: https://iris.paho.org/handle/10665.2/7699 (accessed on 19 November 2020).
- Neri, D.; Steele, E.M.; Khandpur, N.; Cediel, G.; Zapata, M.E.; Rauber, F.; Marrón-Ponce, J.A.; Machado, P.; da Costa Louzada, M.L.; Andrade, G.C.; et al. Ultraprocessed Food Consumption and Dietary Nutrient Profiles Associated with Obesity: A Multicountry Study of Children and Adolescents. Obes. Rev. 2022, 23 (Suppl. 1), e13387. [Google Scholar] [CrossRef] [PubMed]
- Monteiro, C.A.; Moubarac, J.C.; Levy, R.B.; Canella, D.S.; da Costa Louzada, M.L.; Cannon, G. Household Availability of Ultra-Processed Foods and Obesity in Nineteen European Countries. Public Health Nutr. 2018, 21, 18–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Deus Mendonça, R.; Lopes, A.C.S.; Pimenta, A.M.; Gea, A.; Martinez-Gonzalez, M.A.; Bes-Rastrollo, M. Ultra-Processed Food Consumption and the Incidence of Hypertension in a Mediterranean Cohort: The Seguimiento Universidad de Navarra Project. Am. J. Hypertens. 2017, 30, 358–366. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martinez-Perez, C.; San-Cristobal, R.; Guallar-Castillon, P.; Martínez-González, M.Á.; Salas-Salvadó, J.; Corella, D.; Castañer, O.; Martinez, J.A.; Alonso-Gómez, Á.M.; Wärnberg, J.; et al. Use of Different Food Classification Systems to Assess the Association between Ultra-Processed Food Consumption and Cardiometabolic Health in an Elderly Population with Metabolic Syndrome (PREDIMED-Plus Cohort). Nutrients 2021, 13, 2471. [Google Scholar] [CrossRef] [PubMed]
- Fiolet, T.; Srour, B.; Sellem, L.; Kesse-Guyot, E.; Allès, B.; Méjean, C.; Deschasaux, M.; Fassier, P.; Latino-Martel, P.; Beslay, M.; et al. Consumption of Ultra-Processed Foods and Cancer Risk: Results from NutriNet-Santé Prospective Cohort. BMJ 2018, 360, k322. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.; Hu, E.A.; Rebholz, C.M. Ultra-Processed Food Intake and Mortality in the USA: Results from the Third National Health and Nutrition Examination Survey (NHANES III, 1988–1994). Public Health Nutr. 2019, 22, 1777–1785. [Google Scholar] [CrossRef]
- Bonaccio, M.; Di Castelnuovo, A.; Costanzo, S.; De Curtis, A.; Persichillo, M.; Sofi, F.; Cerletti, C.; Donati, M.B.; de Gaetano, G.; Iacoviello, L. Ultra-Processed Food Consumption Is Associated with Increased Risk of All-Cause and Cardiovascular Mortality in the Moli-Sani Study. Am. J. Clin. Nutr. 2021, 113, 446–455. [Google Scholar] [CrossRef]
- Rico-Campà, A.; Martínez-González, M.A.; Alvarez-Alvarez, I.; de Deus Mendonça, R.; de la Fuente-Arrillaga, C.; Gómez-Donoso, C.; Bes-Rastrollo, M. Association between Consumption of Ultra-Processed Foods and All Cause Mortality: SUN Prospective Cohort Study. BMJ 2019, 365, l1949. [Google Scholar] [CrossRef] [Green Version]
- Blanco-Rojo, R.; Sandoval-Insausti, H.; López-Garcia, E.; Graciani, A.; Ordovás, J.M.; Banegas, J.R.; Rodríguez-Artalejo, F.; Guallar-Castillón, P. Consumption of Ultra-Processed Foods and Mortality: A National Prospective Cohort in Spain. Mayo Clin. Proc. 2019, 94, 2178–2188. [Google Scholar] [CrossRef] [Green Version]
- Romero Ferreiro, C.; Martín-Arriscado Arroba, C.; Cancelas Navia, P.; Lora Pablos, D.; Gómez de la Cámara, A. Ultra-Processed Food Intake and All-Cause Mortality: DRECE Cohort Study. Public Health Nutr. 2021, 25, 1854–1863. [Google Scholar] [CrossRef]
- Imamura, F.; Micha, R.; Khatibzadeh, S.; Fahimi, S.; Shi, P.; Powles, J.; Mozaffarian, D. Dietary Quality among Men and Women in 187 Countries in 1990 and 2010: A Systematic Assessment. Lancet Glob. Health 2015, 3, e132–e142. [Google Scholar] [CrossRef] [Green Version]
- Monteiro, C.A.; Moubarac, J.-C.; Cannon, G.; Ng, S.W.; Popkin, B. Ultra-Processed Products Are Becoming Dominant in the Global Food System. Obes Rev. 2013, 14 (Suppl. 2), 21–28. [Google Scholar] [CrossRef] [PubMed]
- Latasa, P.; da Coasta Louzada, M.L.; Martinez Steele, E.; Monteiro, C.A. Added Sugars and Ultra-Processed Foods in Spanish Households (1990–2010). Eur. J. Clin. Nutr. 2018, 72, 1404–1412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haro, J.M.; Tyrovolas, S.; Garin, N.; Diaz-Torne, C.; Carmona, L.; Sanchez-Riera, L.; Perez-Ruiz, F.; Murray, C.J. The Burden of Disease in Spain: Results from the Global Burden of Disease Study 2010. BMC Med. 2014, 12, 236. [Google Scholar] [CrossRef] [Green Version]
- Shojaei, E.; Rexachs, D.; Wong, A.; Epelde, F.; Luque, E. A Method for Projections of the Emergency Department Behaviour by Non-Communicable Diseases From 2019 to 2039. IEEE J. Biomed. Health Inform. 2020, 24, 2490–2498. [Google Scholar] [CrossRef]
- Trichopoulou, A.; Naska, A.; Costacou, T.; DAFNE III Group. Disparities in Food Habits across Europe. Proc. Nutr. Soc. 2002, 61, 553–558. [Google Scholar] [CrossRef] [Green Version]
- Gómez-Jerique, J.A.; Rubio Herrera, M.A.; Gómez De La Cámara, A.; Gutiérrez Fuentes, J.A. Diet and Cardiovascular Risk in Spain Study (DRECE) Capítulo 2. El proyecto DRECE. Med. Clin. 2011, 12, 3–5. [Google Scholar]
- Martin-Moreno, J.M.; Boyle, P.; Gorgojo, L.; Maisonneuve, P.; Fernandez-Rodriguez, J.C.; Salvini, S.; Willett, W.C. Development and Validation of a Food Frequency Questionnaire in Spain. Int. J. Epidemiol. 1993, 22, 512–519. [Google Scholar] [CrossRef]
- Rodríguez, I.T.; Ballart, J.F.; Pastor, G.C.; Jordà, E.B.; Val, V.A. Validation of a short questionnaire on frequency of dietary intake: Reproducibility and validity. Nutr. Hosp. 2008, 23, 242–252. [Google Scholar]
- Panel de Consumo Alimentario. Available online: https://www.mapa.gob.es/es/alimentacion/temas/consumo-tendencias/panel-de-consumo-alimentario/ (accessed on 17 November 2021).
- Monteiro, C.A.; Cannon, G.; Moubarac, J.-C.; Levy, R.B.; Louzada, M.L.C.; Jaime, P.C. The UN Decade of Nutrition, the NOVA Food Classification and the Trouble with Ultra-Processing. Public Health Nutr. 2018, 21, 5–17. [Google Scholar] [CrossRef] [Green Version]
- Greenacre, M.J. La Práctica del Análisis de Correspondencias; Fundación BBVA: Barcelona, Spain, 2008; ISBN 978-84-96515-71-0. [Google Scholar]
- Romero Ferreiro, C.; Lora Pablos, D.; Gómez de la Cámara, A. Two Dimensions of Nutritional Value: Nutri-Score and NOVA. Nutrients 2021, 13, 2783. [Google Scholar] [CrossRef] [PubMed]
- Hedeker, D.; Gibbons, R.D. Longitudinal Data Analysis; Wiley-Interscience: Hoboken, NJ, USA, 2006; p. 337. ISBN 978-0-471-42027-9. [Google Scholar]
- Willett, W.C.; Sacks, F.; Trichopoulou, A.; Drescher, G.; Ferro-Luzzi, A.; Helsing, E.; Trichopoulos, D. Mediterranean Diet Pyramid: A Cultural Model for Healthy Eating. Am. J. Clin. Nutr. 1995, 61, 1402S–1406S. [Google Scholar] [CrossRef] [PubMed]
- Bonaccio, M.; Costanzo, S.; Di Castelnuovo, A.; Persichillo, M.; Magnacca, S.; De Curtis, A.; Cerletti, C.; Donati, M.B.; de Gaetano, G.; Iacoviello, L.; et al. Ultra-Processed Food Intake and All-Cause and Cause-Specific Mortality in Individuals with Cardiovascular Disease: The Moli-Sani Study. Eur. Heart J. 2022, 43, 213–224. [Google Scholar] [CrossRef] [PubMed]
- Juul, F.; Hemmingsson, E. Trends in Consumption of Ultra-Processed Foods and Obesity in Sweden between 1960 and 2010. Public Health Nutr. 2015, 18, 3096–3107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, L.; Martínez Steele, E.; Du, M.; Pomeranz, J.L.; O’Connor, L.E.; Herrick, K.A.; Luo, H.; Zhang, X.; Mozaffarian, D.; Zhang, F.F. Trends in Consumption of Ultraprocessed Foods Among US Youths Aged 2–19 Years, 1999–2018. JAMA 2021, 326, 519–530. [Google Scholar] [CrossRef]
- de Araújo, T.P.; de Moraes, M.M.; Magalhães, V.; Afonso, C.; Santos, C.; Rodrigues, S.S.P. Ultra-Processed Food Availability and Noncommunicable Diseases: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 7382. [Google Scholar] [CrossRef]
- Boyland, E.J.; Nolan, S.; Kelly, B.; Tudur-Smith, C.; Jones, A.; Halford, J.C.; Robinson, E. Advertising as a Cue to Consume: A Systematic Review and Meta-Analysis of the Effects of Acute Exposure to Unhealthy Food and Nonalcoholic Beverage Advertising on Intake in Children and Adults. Am. J. Clin. Nutr 2016, 103, 519–533. [Google Scholar] [CrossRef]
- Marti, A. Ultra-Processed Foods Are Not “Real Food” but Really Affect Your Health. Nutrients 2019, 11, 1902. [Google Scholar] [CrossRef] [Green Version]
- Oxandabarat, A. OPS/OMS Uruguay—Guía Alimentaria para la Población Uruguaya | OPS/OMS. Available online: https://www3.paho.org/uru/index.php?option=com_content&view=article&id=1375:guia-alimentaria-para-la-poblacion-uruguaya&Itemid=451 (accessed on 30 June 2022).
- Monteiro, C.A.; Cannon, G.; Moubarac, J.-C.; Martins, A.P.B.; Martins, C.A.; Garzillo, J.; Canella, D.S.; Baraldi, L.G.; Barciotte, M.; Louzada, M.L. da C.; et al. Dietary Guidelines to Nourish Humanity and the Planet in the Twenty-First Century. A Blueprint from Brazil. Public Health Nutr. 2015, 18, 2311–2322. [Google Scholar] [CrossRef]
- Mauricio, H.-F.; Batis, C.; Rivera, J.A.; Colchero, M.A. Reduction in Purchases of Energy-Dense Nutrient-Poor Foods in Mexico Associated with the Introduction of a Tax in 2014. Prev. Med. 2019, 118, 16–22. [Google Scholar] [CrossRef]
- Bíró, A. Did the Junk Food Tax Make the Hungarians Eat Healthier? Food Policy 2015, 54, 107–115. [Google Scholar] [CrossRef] [Green Version]
- Baraldi, L.G.; Martinez Steele, E.; Canella, D.S.; Monteiro, C.A. Consumption of Ultra-Processed Foods and Associated Sociodemographic Factors in the USA between 2007 and 2012: Evidence from a Nationally Representative Cross-Sectional Study. BMJ Open 2018, 8, e020574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khandpur, N.; Cediel, G.; Obando, D.A.; Jaime, P.C.; Parra, D.C. Factores sociodemográficos asociados al consumo de alimentos ultraprocesados en Colombia. Rev. Saúde Pública 2020, 54. [Google Scholar] [CrossRef] [Green Version]
- de Deus Mendonça, R.; Pimenta, A.M.; Gea, A.; de la Fuente-Arrillaga, C.; Martinez-Gonzalez, M.A.; Lopes, A.C.S.; Bes-Rastrollo, M. Ultraprocessed Food Consumption and Risk of Overweight and Obesity: The University of Navarra Follow-Up (SUN) Cohort Study. Am. J. Clin. Nutr. 2016, 104, 1433–1440. [Google Scholar] [CrossRef] [PubMed]
- Beslay, M.; Srour, B.; Méjean, C.; Allès, B.; Fiolet, T.; Debras, C.; Chazelas, E.; Deschasaux, M.; Wendeu-Foyet, M.G.; Hercberg, S.; et al. Ultra-Processed Food Intake in Association with BMI Change and Risk of Overweight and Obesity: A Prospective Analysis of the French NutriNet-Santé Cohort. PLoS Med. 2020, 17, e1003256. [Google Scholar] [CrossRef] [PubMed]
- Pestoni, G.; Habib, L.; Reber, E.; Rohrmann, S.; Staub, K.; Stanga, Z.; Faeh, D. Ultraprocessed Food Consumption Is Strongly and Dose-Dependently Associated with Excess Body Weight in Swiss Women. Obesity 2021, 29, 601–609. [Google Scholar] [CrossRef] [PubMed]
- Chandon, P.; Wansink, B. Does Food Marketing Need to Make Us Fat? A Review and Solutions. Nutr. Rev. 2012, 70, 571–593. [Google Scholar] [CrossRef] [Green Version]
- Gómez de la Cámara, A.; De Andrés Esteban, E.; Urrútia Cuchí, G.; Calderón Sandubete, E.; Rubio Herrera, M.Á.; Menéndez Orenga, M.; Lora Pablos, D. Variability of Nutrients Intake, Lipid Profile and Cardiovascular Mortality among Geographical Areas in Spain: The DRECE Study. Geospat. Health 2017, 12, 524. [Google Scholar] [CrossRef]
- Moreiras-Varela, O. The Mediterranean Diet in Spain. Eur. J. Clin. Nutr. 1989, 43 (Suppl. 2), 83–87. [Google Scholar]
- Dinu, M.; Tristan Asensi, M.; Pagliai, G.; Lotti, S.; Martini, D.; Colombini, B.; Sofi, F. Consumption of Ultra-Processed Foods Is Inversely Associated with Adherence to the Mediterranean Diet: A Cross-Sectional Study. Nutrients 2022, 14, 2073. [Google Scholar] [CrossRef]
- Instituto Nacional de Estadística. (National Statistics Institute). Available online: https://www.ine.es/dynt3/inebase/index.htm?padre=1928&capsel=1928 (accessed on 30 June 2022).


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| DRECE I 1991 | DRECE II 1996 | DRECE III 2004 | DRECE IV 2008 | |
|---|---|---|---|---|
| Total energy intake (kcal/day) | 2024.80 (727.09) | 2362.49 (1197) | 2373.91 (1068) | 2441.01 (948.75) |
| NOVA classification (% of energy) | ||||
| NOVA 1 | 45.91 (13.33) | 47.96 (15.58) | 51.47 (14.01) | 55.21 (12.13) |
| NOVA 3+2 | 29.65 (13.24) | 26.43 (15.96) | 21.05 (16.48) | 13.70 (15.37) |
| NOVA 4 | 24.44 (13.95) | 25.61 (16.29) | 27.48 (19.17) | 31.09 (19.24) |
| UPF consumption (NOVA 4) (% of energy) | ||||
| By sex | ||||
| Male | 24.48 (13.89) | 23.71 (16.76) | 26.14 (19.72) | 31.03 (17.57) |
| Female | 24.39 (14.01) | 27.83 (15.16) | 29.01 (15.18) | 31.39 (18.47) |
| By age group | ||||
| 5–24 | 32.79 (12.83) | 31.69 (14.84) | 33.72 (14.04) | 34.12 (11.48) |
| 25–49 | 19.81 (11.62) | 24.70 (16.63) | 26.70 (17.26) | 27.91 (21.01) |
| 50–75 | 16.13 (11.41) | 19.39 (19.01) | 22.01 (12.29) | 25.14 (19.83) |
| By BMI class | ||||
| Normal weight | 16.96 (11.41) | 23.67 (17.30) | 22.76 (18.74) | 27.93 (19.22) |
| Overweight | 19.99 (12.45) | 26.04 (16.15) | 25.88 (19.86) | 31.77 (18.90) |
| Obese | 28.27 (13.85) | 26.11 (15.06) | 28.67 (18.67) | 33.31 (21.15) |
| Estimate | Standard Error | p | |
|---|---|---|---|
| Intercept | 24.49 | 1.21 | <0.001 |
| Time (Cohorts) | |||
| DRECE I 1991 | Ref. | ||
| DRECE II 1996 | 5.31 | 0.62 | <0.001 |
| DRECE III 2004 | 9.63 | 0.66 | <0.001 |
| DRECE IV 2008 | 10.79 | 0.39 | <0.001 |
| Age (years) | −0.15 | 0.01 | <0.001 |
| Sex | |||
| Male | Ref. | ||
| Female | 1.06 | 0.33 | 0.01 |
| BMI (kg/m2) | −0.05 | 0.04 | 0.19 |
| Total energy intake (kcal/day) | 1.86 | 0.19 | <0.001 |
| Geographical Areas | p | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| DRECE I 1991 | North-West | North | North-East | West | Central-South | East | South | Canary Islands | |
| n | 514 | 422 | 683 | 341 | 913 | 553 | 1075 | 178 | |
| Age (years) | 30.04 (15.61) | 30.38 (15.59) | 31.74 (15.59) | 30.22 (15.50) | 30.54 (15.73) | 31.57 (15.58) | 29.89 (15.50) | 29.48 (16.04) | 0.175 |
| Sex (male) | 249 (48.44%) | 206 (48.82%) | 331 (48.46%) | 171 (50.15%) | 440 (48.19%) | 263 (47.56%) | 539 (50.14%) | 89 (50.00%) | 0.977 |
| BMI (kg/m2) | 24.43 (4.61) | 23.53 (4.48) | 24.43 (4.83) | 23.65 (4.47) | 24.05 (5.10) | 24.14 (4.73) | 24.75 (5.68) | 24.09 (5.63) | 0.002 |
| Total energy intake (kcal/day) | 1996.47 (641.84) | 1942.73 (593.48) | 2037.55 (707.23) | 2152.04 (686.01) | 2023.84 (693.92) | 1964.44 (802.26) | 2040.11 (796.11) | 2109.13 (846.20) | <0.001 |
| NOVA classification | |||||||||
| GROUP 4 (% of energy) | 24.47 (14.45) | 25.03 (12.95) | 22.65 (13.75) | 24.60 (12.94) | 24.97 (14.00) | 22.64 (14.02) | 25.15 (14.05) | 28.10 (15.16) | <0.001 |
| DRECE II 1996 | North-West | North | North-East | West | Central-South | East | South | Canary Islands | |
| n | 78 | 124 | 88 | 83 | 162 | 123 | 223 | 47 | |
| Age (years) | 48.29 (13.75) | 46.03 (14.45) | 48.95 (13.64) | 46.05 (15.11) | 47.92 (14.95) | 45.65 (15.35) | 45.53 (14.93) | 44.26 (15.88) | 0.248 |
| Sex (male) | 51 (65.38%) | 73 (58.87%) | 54 (61.36%) | 51 (61.45%) | 97 (59.88%) | 84 (68.29%) | 130 (58.30%) | 26 (55.32%) | 0.415 |
| BMI (kg/m2) | 27.79 (3.76) | 26.69 (4.03) | 28.61 (3.70) | 26.08 (4.06) | 26.86 (4.68) | 27.21 (4.14) | 28.36 (5.49) | 27.75 (6.02) | <0.001 |
| Total energy intake (kcal/day) | 2474.43 (1061) | 2212.04 (751.12) | 2576.62 (2016) | 2359.88 (769.19) | 2178.05 (862.04) | 2625.60 (1149) | 2441.92 (1459) | 1919.39 (770.33) | <0.001 |
| NOVA classification | |||||||||
| GROUP 4 (% of energy) | 25.91 (15.78) | 28.87 (15.90) | 25.53 (16.11) | 25.06 (17.82) | 26.95 (17.41) | 21.85 (15.71) | 23.13 (15.28) | 29.33 (15.12) | 0.010 |
| DRECE III 2004 | North-West | North | North-East | West | Central-South | East | South | Canary Islands | |
| n | 89 | 135 | 192 | 104 | 178 | 45 | 257 | 65 | |
| Age (years) | 44.18 (15.66) | 44.68 (15.13) | 47.80 (16.14) | 44.96 (16.01) | 45.29 (17.18) | 44.93 (14.66) | 44.17 (14.05) | 51.17 (15.40) | 0.061 |
| Sex (male) | 42 (47.19%) | 64 (47.41%) | 86 (44.79%) | 46 (44.23%) | 72 (40.45%) | 21 (46.67%) | 116 (45.14%) | 28 (43.08%) | 0.954 |
| BMI (kg/m2) | 28.52 (5.02) | 26.59 (4.72) | 27.80 (5.36) | 26.70 (4.74) | 26.34 (4.59) | 28.23 (5.11) | 28.38 (5.85) | 28.40 (4.91) | <0.001 |
| Total energy intake (kcal/day) | 2286.15 (1080) | 2580.85 (1353) | 2485.81 (1109) | 2408.26 (969.91) | 2518.23 (1254) | 2368.07 (771.36) | 2114.92 (756.77) | 2311.56 (906.83) | 0.002 |
| NOVA classification | |||||||||
| GROUP 4 (% of energy) | 34.13 (18.02) | 35.34 (15.59) | 32.48 (12.55) | 34.67 (14.78) | 29.99 (19.68) | 25.71 (11.57) | 25.85 (13.51) | 34.42 (12.85) | <0.001 |
| DRECE IV 2008 | North-West | North | North-East | West | Central-South | East | South | Canary Islands | |
| n | 562 | 370 | 833 | 373 | 1037 | 548 | 922 | 190 | |
| Age (years) | 44.06 (14.91) | 45.58 (15.13) | 43.51 (14.32) | 43.28 (14.45) | 43.81 (14.70) | 44.58 (15.32) | 42.88 (14.21) | 42.14 (14.25) | 0.067 |
| Sex (male) | 251 (44.66%) | 176 (47.57%) | 404 (48.50%) | 180 (48.26%) | 469 (45.23%) | 271 (49.45%) | 411 (44.58%) | 95 (50.00%) | 0.372 |
| BMI (kg/m2) | 26.26 (4.13) | 24.67 (3.82) | 25.30 (4.23) | 26.88 (3.91) | 25.17 (4.13) | 24.84 (3.96) | 26.60 (4.46) | 25.87 (4.54) | 0.007 |
| Total energy intake (kcal/day) | 2400.25 (910.08) | 2382.53 (959.17) | 2386.65 (985.88) | 2490.63 (855.33) | 2453.17 (860.99) | 2432.02 (1021) | 2491.67 (1003) | 2530.22 (1001) | 0.005 |
| NOVA classification | |||||||||
| GROUP 4 (% of energy) | 35.47 (16.94) | 36.02 (18.33) | 32.75 (19.76) | 34.01 (17.48) | 30.17 (17.14) | 31.03 (17.60) | 31.28 (18.33) | 34.80 (16.12) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Romero Ferreiro, C.; Cancelas Navia, P.; Lora Pablos, D.; Gómez de la Cámara, A. Geographical and Temporal Variability of Ultra-Processed Food Consumption in the Spanish Population: Findings from the DRECE Study. Nutrients 2022, 14, 3223. https://doi.org/10.3390/nu14153223
Romero Ferreiro C, Cancelas Navia P, Lora Pablos D, Gómez de la Cámara A. Geographical and Temporal Variability of Ultra-Processed Food Consumption in the Spanish Population: Findings from the DRECE Study. Nutrients. 2022; 14(15):3223. https://doi.org/10.3390/nu14153223
Chicago/Turabian StyleRomero Ferreiro, Carmen, Pilar Cancelas Navia, David Lora Pablos, and Agustín Gómez de la Cámara. 2022. "Geographical and Temporal Variability of Ultra-Processed Food Consumption in the Spanish Population: Findings from the DRECE Study" Nutrients 14, no. 15: 3223. https://doi.org/10.3390/nu14153223
APA StyleRomero Ferreiro, C., Cancelas Navia, P., Lora Pablos, D., & Gómez de la Cámara, A. (2022). Geographical and Temporal Variability of Ultra-Processed Food Consumption in the Spanish Population: Findings from the DRECE Study. Nutrients, 14(15), 3223. https://doi.org/10.3390/nu14153223