
Lower Serum Calcium Levels Associated with Disrupted Sleep and Rest–Activity Rhythm in Shift Workers


Abstract
:1. Introduction
2. Materials and Methods
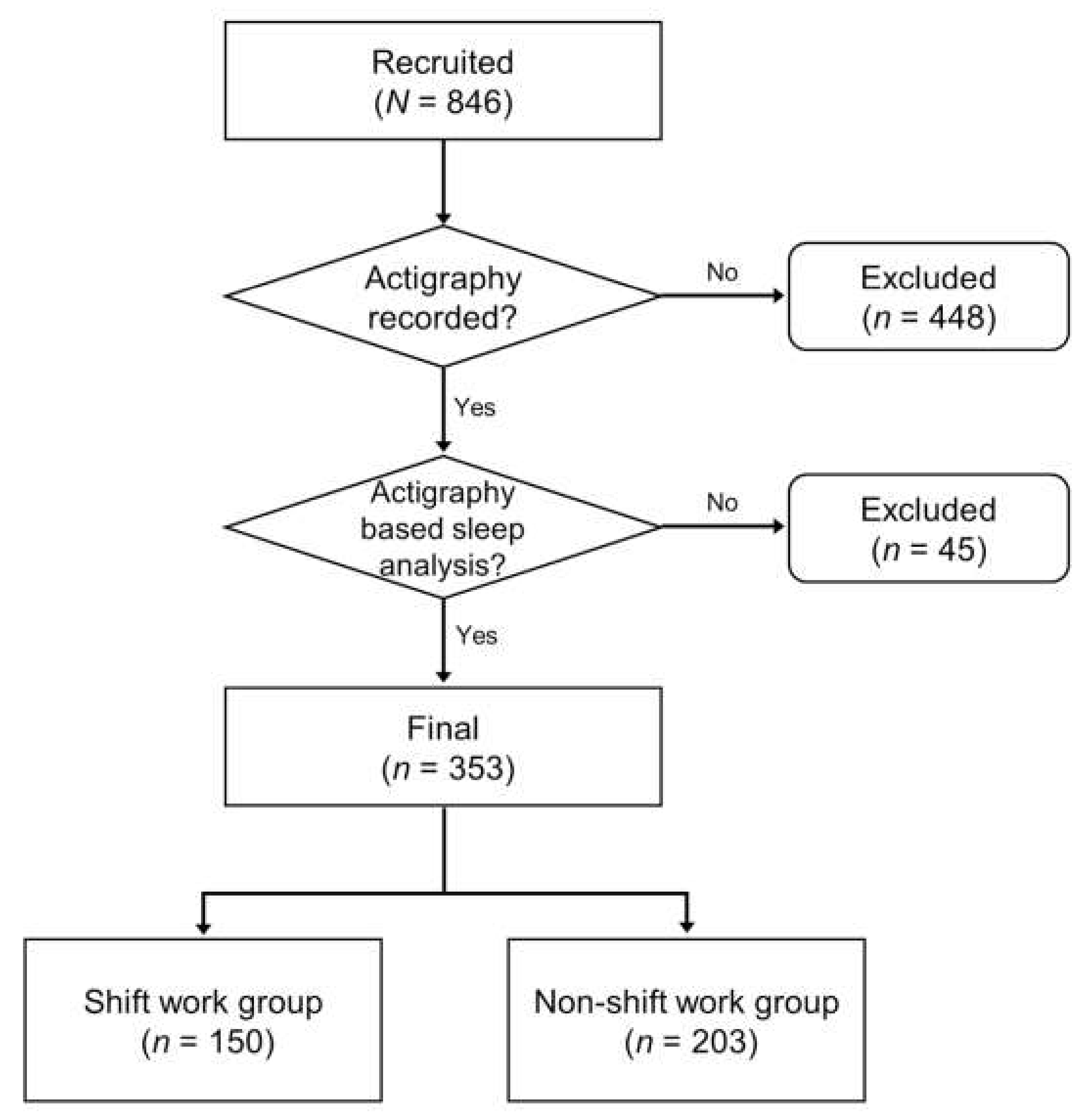
2.1. Subjects
2.2. Demographic and Clinical Characteristics
2.3. Actigraphy-Based Sleep Analysis
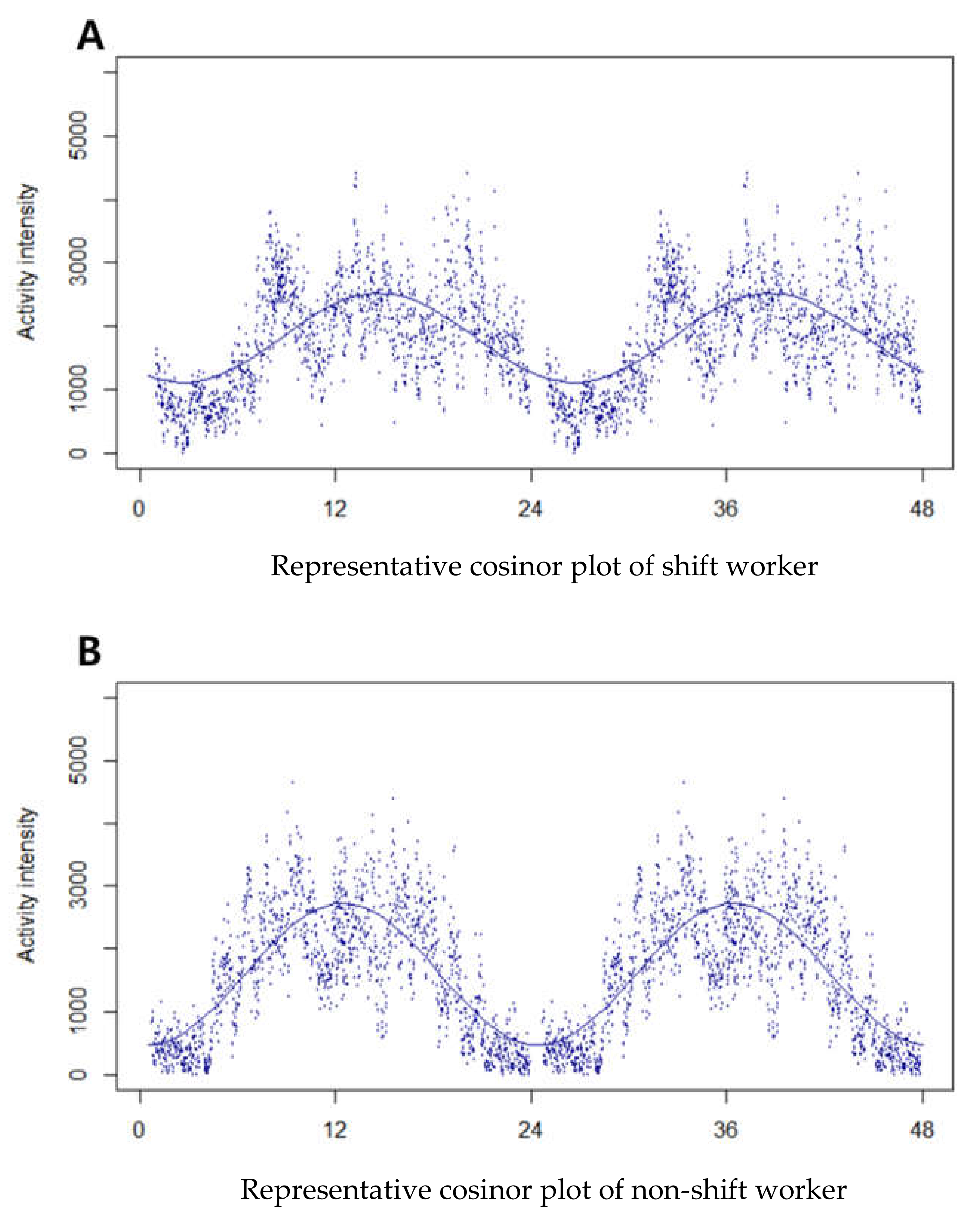
2.4. Cosinor Analysis
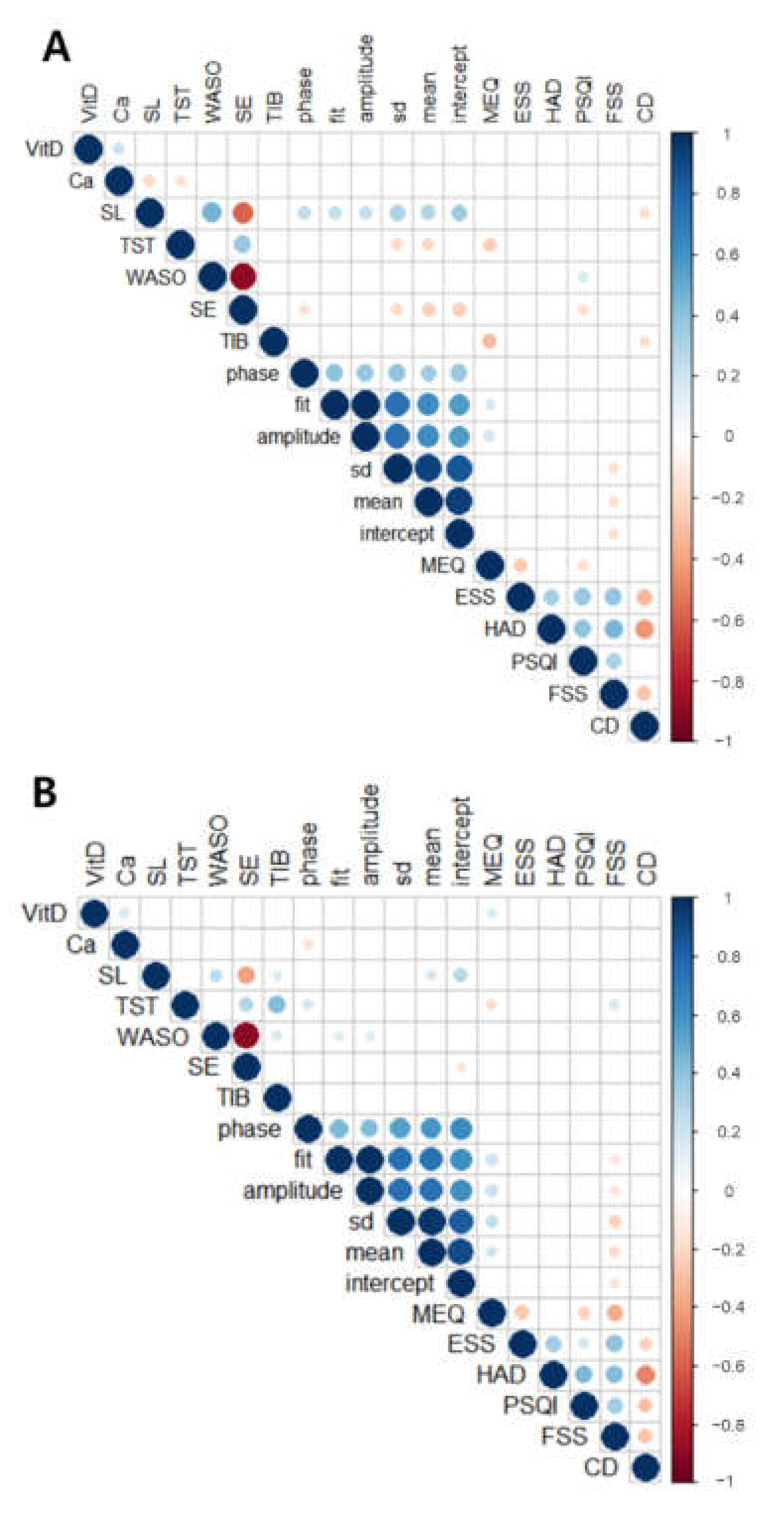
2.5. Statistical Analysis
3. Results
4. Discussion
4.1. Rest–Activity Rhythm Measured by Actigraphy
4.2. No Statistical Difference in Vitamin D Levels between Shift and Non-Shift Workers
4.3. Decreased Serum Calcium Levels in Shift Workers
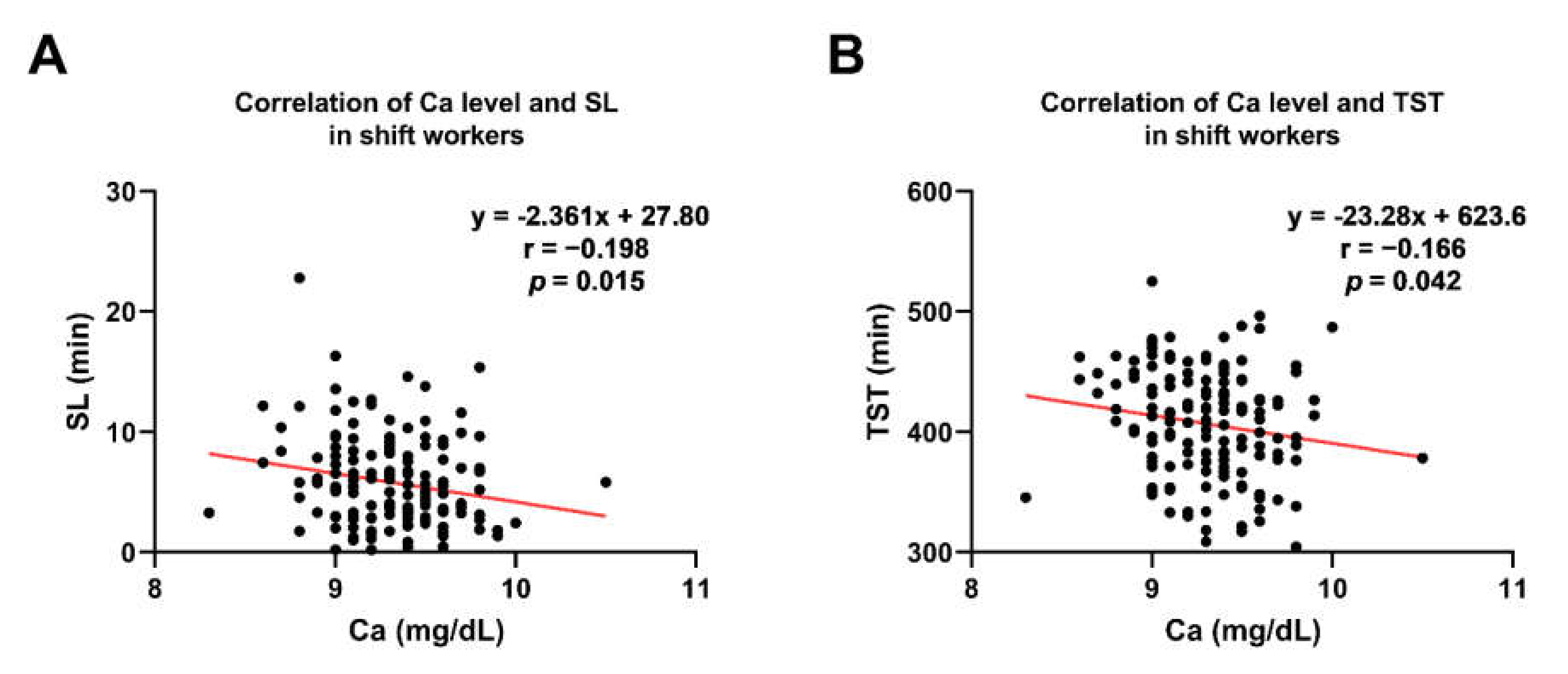
4.4. Lower Calcium Levels Associated with a Longer SL and TST in Shift Workers
4.5. Rest–Activity Rhythm and Calcium Level in the Shift Workers
4.6. Poorer Subjective Sleep Quality in the Shift Workers
4.7. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Boivin, D.B.; Boudreau, P. Impacts of shift work on sleep and circadian rhythms. Pathol. Biol. 2014, 62, 292–301. [Google Scholar] [CrossRef] [PubMed]
- Bajraktarov, S.; Novotni, A.; Manusheva, N.; Nikovska, D.G.; Miceva-Velickovska, E.; Zdraveska, N.; Samardjiska, V.C.; Richter, K.S. Main effects of sleep disorders related to shift work–opportunities for preventive programs. EPMA J. 2011, 2, 365–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ganesan, S.; Magee, M.; Stone, J.E.; Mulhall, M.D.; Collins, A.; Howard, M.E.; Lockley, S.W.; Rajaratnam, S.M.W.; Sletten, T.L. The Impact of Shift Work on Sleep, Alertness and Performance in Healthcare Workers. Sci. Rep. 2019, 9, 4635. [Google Scholar] [CrossRef] [PubMed]
- Nakata, A.; Haratani, T.; Takahashi, M.; Kawakami, N.; Arito, H.; Kobayashi, F.; Fujioka, Y.; Fukui, S.; Araki, S. Association of Sickness Absence with Poor Sleep and Depressive Symptoms in Shift Workers. Chronobiol. Int. 2004, 21, 899–912. [Google Scholar] [CrossRef]
- Kervezee, L.; Kosmadopoulos, A.; Boivin, D.B. Metabolic and cardiovascular consequences of shift work: The role of circadian disruption and sleep disturbances. Eur. J. Neurosci. 2020, 51, 396–412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Megdal, S.P.; Kroenke, C.H.; Laden, F.; Pukkala, E.; Schernhammer, E.S. Night work and breast cancer risk: A systematic review and meta-analysis. Eur. J. Cancer 2005, 41, 2023–2032. [Google Scholar] [CrossRef]
- Holick, M.F.; Chen, T.C. Vitamin D deficiency: A worldwide problem with health consequences. Am. J. Clin. Nutr. 2008, 87, 1080S–1086S. [Google Scholar] [CrossRef] [Green Version]
- Sowah, D.; Fan, X.; Dennett, L.; Hagtvedt, R.; Straube, S. Vitamin D levels and deficiency with different occupations: A systematic review. BMC Public Health 2017, 17, 1–25. [Google Scholar] [CrossRef]
- Divakar, U.; Sathish, T.; Soljak, M.; Bajpai, R.; Dunleavy, G.; Visvalingam, N.; Nazeha, N.; Soh, C.K.; Christopoulos, G.; Car, J. Prevalence of Vitamin D Deficiency and Its Associated Work-Related Factors among Indoor Workers in a Multi-Ethnic Southeast Asian Country. Int. J. Environ. Res. Public Health 2019, 17, 164. [Google Scholar] [CrossRef] [Green Version]
- Kodani, S.; Soya, S.; Sakurai, T. Excitation of GABAergic Neurons in the Bed Nucleus of the Stria Terminalis Triggers Immediate Transition from Non-Rapid Eye Movement Sleep to Wakefulness in Mice. J. Neurosci. 2017, 37, 7164–7176. [Google Scholar] [CrossRef] [Green Version]
- Kim, A.; Latchoumane, C.; Lee, S.; Kim, G.B.; Cheong, E.; Augustine, G.J.; Shin, H.-S. Optogenetically induced sleep spindle rhythms alter sleep architectures in mice. Proc. Natl. Acad. Sci. USA 2012, 109, 20673–20678. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanford, L.D.; Parris, B.; Tang, X. GABAergic regulation of the central nucleus of the amygdala: Implications for sleep control. Brain Res. 2002, 956, 276–284. [Google Scholar] [CrossRef]
- Smith, H.R.; Leibold, N.K.; Rappoport, D.A.; Ginapp, C.M.; Purnell, B.S.; Bode, N.M.; Alberico, S.L.; Kim, Y.C.; Audero, E.; Gross, C.T.; et al. Dorsal Raphe Serotonin Neurons Mediate CO2-Induced Arousal from Sleep. J. Neurosci. 2018, 38, 1915–1925. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gominak, S.C.; Stumpf, W.E. The world epidemic of sleep disorders is linked to vitamin D deficiency. Med. Hypotheses 2012, 79, 132–135. [Google Scholar] [CrossRef]
- Bertisch, S.M.; Sillau, S.; De Boer, I.H.; Szklo, M.; Redline, S. 25-Hydroxyvitamin D Concentration and Sleep Duration and Continuity: Multi-Ethnic Study of Atherosclerosis. Sleep 2015, 38, 1305–1311. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.H.; Chang, J.H.; Kim, D.Y.; Kang, J.W. Association Between Self-Reported Sleep Duration and Serum Vitamin D Level in Elderly Korean Adults. J. Am. Geriatr. Soc. 2014, 62, 2327–2332. [Google Scholar] [CrossRef]
- Majid, M.S.; Ahmad, H.S.; Bizhan, H.; Hosein, H.Z.M.; Mohammad, A. The effect of vitamin D supplement on the score and quality of sleep in 20–50 year-old people with sleep disorders compared with control group. Nutr. Neurosci. 2018, 21, 511–519. [Google Scholar] [CrossRef]
- Huang, W.; Shah, S.; Long, Q.; Crankshaw, A.K.; Tangpricha, V. Improvement of Pain, Sleep, and Quality of Life in Chronic Pain Patients with Vitamin D Supplementation. Clin. J. Pain 2013, 29, 341–347. [Google Scholar] [CrossRef] [Green Version]
- Gutierrez-Monreal, M.A.; Duran, R.C.-D.; Moreno-Cuevas, J.E.; Scott, S.-P. A Role for 1α,25-Dihydroxyvitamin D3 in the Expression of Circadian Genes. J. Biol. Rhythm. 2014, 29, 384–388. [Google Scholar] [CrossRef]
- Jirikowski, G.F.; Kauntzer, U.W.; Dief, A.E.E.; Caldwell, J.D. Distribution of vitamin D binding protein expressing neurons in the rat hypothalamus. Histochem. Cell Biol. 2009, 131, 365–370. [Google Scholar] [CrossRef]
- Pike, J.W.; Zella, L.A.; Meyer, M.B.; Fretz, J.A.; Kim, S. Molecular Actions of 1,25-Dihydroxyvitamin D3 on Genes Involved in Calcium Homeostasis. J. Bone Miner. Res. 2007, 22, V16–V19. [Google Scholar] [CrossRef] [PubMed]
- Fleet, J.C.; Schoch, R.D. Molecular mechanisms for regulation of intestinal calcium absorption by vitamin D and other factors. Crit. Rev. Clin. Lab. Sci. 2010, 47, 181–195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Massimini, M.; Amzica, F. Extracellular calcium fluctuations and intracellular potentials in the cortex during the slow sleep oscillation. J. Neurophysiol. 2001, 85, 1346–1350. [Google Scholar] [CrossRef] [PubMed]
- Tatsuki, F.; Sunagawa, G.A.; Shi, S.; Susaki, E.A.; Yukinaga, H.; Perrin, D.; Sumiyama, K.; Ukai-Tadenuma, M.; Fujishima, H.; Ohno, R.-I.; et al. Involvement of Ca2+-Dependent Hyperpolarization in Sleep Duration in Mammals. Neuron 2016, 90, 70–85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grandner, M.A.; Jackson, N.; Gerstner, J.R.; Knutson, K.L. Sleep symptoms associated with intake of specific dietary nutrients. J. Sleep Res. 2014, 23, 22–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buysse, D.J.; Reynolds, C.F., 3rd; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh sleep quality index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Johns, M.W. A New Method for Measuring Daytime Sleepiness: The Epworth Sleepiness Scale. Sleep 1991, 14, 540–545. [Google Scholar] [CrossRef] [Green Version]
- Horne, J.A.; Ostberg, O. A self-assessment questionnaire to determine morningness-eveningness in human circadian rhythms. Int. J. Chronobiol. 1976, 4, 97–110. [Google Scholar]
- Bjelland, I.; Dahl, A.A.; Haug, T.T.; Neckelmann, D. The validity of the Hospital Anxiety and Depression Scale. An updated literature review. J. Psychosom. Res. 2002, 52, 69–77. [Google Scholar] [CrossRef]
- Krupp, L.B.; LaRocca, N.G.; Muir-Nash, J.; Steinberg, A.D. The Fatigue Severity Scale: Application to Patients with Multiple Sclerosis and Systemic Lupus Erythematosus. Arch. Neurol. 1989, 46, 1121–1123. [Google Scholar] [CrossRef]
- Lee, H.J.; Choi, H.; Yoon, I.-Y. Impacts of serum vitamin D levels on sleep and daytime sleepiness according to working conditions. J. Clin. Sleep Med. 2020, 16, 1045–1054. [Google Scholar] [CrossRef] [PubMed]
- Quante, M.; Kaplan, E.R.; Cailler, M.; Rueschman, M.; Wang, R.; Weng, J.; Taveras, E.M.; Redline, S. Actigraphy-based sleep estimation in adolescents and adults: A comparison with polysomnography using two scoring algorithms. Nat. Sci. Sleep 2018, 10, 13–20. [Google Scholar] [CrossRef] [Green Version]
- Mikulich, S.K.; Zerbe, G.O.; Jones, R.H.; Crowley, T.J. Comparing linear and nonlinear mixed model approaches to cosinor analysis. Stat. Med. 2003, 22, 3195–3211. [Google Scholar] [CrossRef] [PubMed]
- Schoch, S.F.; Kurth, S.; Werner, H. Actigraphy in sleep research with infants and young children: Current practices and future benefits of standardized reporting. J. Sleep Res. 2021, 30, e13134. [Google Scholar] [CrossRef] [PubMed]
- Ancoli-Israel, S.; Martin, J.L.; Blackwell, T.; Buenaver, L.F.; Liu, L.; Meltzer, L.J.; Sadeh, A.; Spira, A.P.; Taylor, D.J. The SBSM Guide to Actigraphy Monitoring: Clinical and Research Applications. Behav. Sleep Med. 2015, 13, S4–S38. [Google Scholar] [CrossRef] [PubMed]
- Itoh, H.; Weng, Z.; Saito, H.; Ogawa, Y.; Nakayama, K.; Hasegawa-Ohira, M.; Morimoto, K.; Maki, S.; Takahashi, M. Association between Night-shift Work and Serum 25-hydroxyvitamin D Levels in Japanese Male Indoor Workers: A Cross-sectional Study. Ind. Health 2011, 49, 658–662. [Google Scholar] [CrossRef] [Green Version]
- Daugaard, S.; Garde, A.H.; Hansen, M.; Vistisen, H.T.; Rejnmark, L.; Kolstad, H.A. Indoor, outdoor, and night work and blood concentrations of vitamin D and parathyroid hormone. Scand. J. Work. Environ. Health 2018, 44, 647–657. [Google Scholar] [CrossRef]
- Jeong, H.; Hong, S.; Heo, Y.; Chun, H.; Kim, D.; Park, J.; Kang, M.-Y. Vitamin D status and associated occupational factors in Korean wage workers: Data from the 5th Korea national health and nutrition examination survey (KNHANES 2010–2012). Ann. Occup. Environ. Med. 2014, 26, 28. [Google Scholar] [CrossRef] [Green Version]
- Holick, M.F. Vitamin D Status: Measurement, Interpretation, and Clinical Application. Ann. Epidemiol. 2009, 19, 73–78. [Google Scholar] [CrossRef] [Green Version]
- Khosla, S. Hypercalcemia and Hypocalcemia. In Harrison’s Principles of Internal Medicine, 19th ed.; Kasper, D., Fauci, A., Hauser, S., Longo, D., Jameson, J.L., Loscalzo, J., Eds.; McGraw-Hill Education: New York, NY, USA, 2014. [Google Scholar]
- Fradkin, L.; Raz, O.; Boaz, M. Nurses who work rotating shifts consume more energy, macronutrients and calcium when they work the night shift versus day shift. Chronobiol. Int. 2019, 36, 288–295. [Google Scholar] [CrossRef]
- Kim, K.-N.; Oh, S.-Y.; Hong, Y.-C. Associations of serum calcium levels and dietary calcium intake with incident type 2 diabetes over 10 years: The Korean Genome and Epidemiology Study (KoGES). Diabetol. Metab. Syndr. 2018, 10, 50. [Google Scholar] [CrossRef] [PubMed]
- Ridefelt, P.; Axelsson, J.; Larsson, A. Diurnal variability of total calcium during normal sleep and after an acute shift of sleep. Clin. Chem. Lab. Med. 2012, 50, 147–151. [Google Scholar] [CrossRef] [PubMed]
- Gillberg, M.; Åkerstedt, T. The Dynamics of the First Sleep Cycle. Sleep 1991, 14, 147–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Åkerstedt, T.; Wright, K.P. Sleep Loss and Fatigue in Shift Work and Shift Work Disorder. Sleep Med. Clin. 2009, 4, 257–271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Booker, L.A.; Magee, M.; Rajaratnam, S.M.; Sletten, T.L.; Howard, M.E. Individual vulnerability to insomnia, excessive sleepiness and shift work disorder amongst healthcare shift workers. A systematic review. Sleep Med. Rev. 2018, 41, 220–233. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Shift Workers (n = 150) | Non-Shift Workers (n = 203) | p-Value |
|---|---|---|---|
| Sex, male, n (%) | 11 (7.3) | 18 (8.9) | 0.604 |
| Age, years | 32.86 ± 0.62 | 40.40 ± 0.88 | <0.001 |
| Body mass index, kg/m2 | 21.12 ± 0.22 | 22.00 ± 0.20 | <0.001 |
| Marital status, married, n (%) | 36 (24.0) | 91 (44.8) | <0.001 |
| Education, college graduates, n (%) | 140 (93.3) | 153 (75.3) | <0.001 |
| Current smoking, n (%) | 9 (6.0) | 23 (11.3) | 0.017 |
| Drinking, n (%) | 94 (62.7) | 112 (55.2) | 0.158 |
| Coffee consumption, cups/day | 1.12 ± 0.07 | 1.23 ± 0.07 | 0.18 |
| Physical activity, n (%) | 90 (60.0) | 113 (55.7) | 0.415 |
| Medication use, n (%) | 29 (16.5) | 57 (23.0) | 0.058 |
| Medical comorbidities, n (%) | 20 (13.3) | 33 (16.3) | 0.447 |
| Shift Workers (n = 150) | Non-Shift Workers (n = 203) | p-Value (p < 0.05 *) | |
|---|---|---|---|
| Laboratory tests | |||
| 25(OH)D (ng/mL) | 13.45 ± 0.46 | 14.58 ± 0.59 | - |
| Calcium (mg/dL) | 9.31 ± 0.03 | 9.38 ± 0.02 | * |
| Actigraphy-based sleep parametersa | |||
| SL, min | 5.83 ± 0.31 | 5.53 ± 0.30 | - |
| TST, min | 406.87 ± 3.61 | 385.73 ± 3.37 | *** |
| WASO, min | 70.94 ± 2.01 | 58.51 ± 1.59 | *** |
| SE, % | 84.08 ± 0.39 | 85.84 ± 0.33 | *** |
| TIB, min | 484.10 ± 7.56 | 441.17 ± 5.11 | - |
| Actigraphy-based activity parametersb | |||
| Phase | 14.72 ± 0.49 | 12.08 ± 0.42 | *** |
| Fit | 0.48 ± 0.02 | 0.59 ± 0.01 | *** |
| Amplitude | 0.48 ± 0.02 | 0.59 ± 0.01 | *** |
| SD | 612.07 ± 24.56 | 759.03 ± 32.77 | - |
| Mean | 1054.62 ± 55.53 | 1042.83 ± 52.67 | - |
| Intercept | 714.62 ± 53.53 | 744.96 ± 33.23 | - |
| Clinical parametersc | |||
| MEQ | 42.58 ± 0.61 | 47.78 ± 0.59 | *** |
| ESS | 9.19 ± 0.27 | 7.80 ± 0.22 | *** |
| HADS | 12.65 ± 0.49 | 11.42 ± 0.38 | * |
| PSQI | 7.91 ± 0.26 | 6.37 ± 0.20 | *** |
| FSS | 45.23 ± 1.18 | 36.05 ± 1.03 | *** |
| CD-RISC | 62.28 ± 1.06 | 63.06 ± 1.07 | - |
| Serum 25-Hydroxyvitamin D Level | ||||
|---|---|---|---|---|
| PSQI Complex | Shift Workers (n = 150) | Non-Shift Workers (n = 203) | ||
| r | p-Value | r | p-Value | |
| Component 1; subjective sleep quality | 0.140 | 0.088 | −0.024 | 0.737 |
| Component 2; sleep latency | −0.029 | 0.725 | 0.080 | 0.254 |
| Component 3; sleep duration | 0.132 | 0.108 | −0.037 | 0.596 |
| Component 4; habitual sleep efficiency | 0.066 | 0.421 | 0.053 | 0.450 |
| Component 5; sleep disturbance | 0.070 | 0.396 | −0.023 | 0.744 |
| Component 6; use of sleep medicine | −0.172 | 0.036 * | 0.081 | 0.248 |
| Component 7; daytime dysfunction | −0.200 | 0.014 * | 0.039 | 0.578 |
| Serum Calcium Level | ||||
|---|---|---|---|---|
| PSQI Complex | Shift Workers (n = 150) | Non-Shift Workers (n = 203) | ||
| r | p-Value | r | p-Value | |
| Component 1; subjective sleep quality | 0.040 | 0.627 | 0.018 | 0.794 |
| Component 2; sleep latency | −0.041 | 0.619 | 0.016 | 0.824 |
| Component 3; sleep duration | 0.004 | 0.959 | −0.049 | 0.491 |
| Component 4; habitual sleep efficiency | −0.019 | 0.817 | 0.020 | 0.775 |
| Component 5; sleep disturbance | −0.017 | 0.834 | 0.020 | 0.780 |
| Component 6; use of sleep medicine | −0.171 | 0.036 * | 0.014 | 0.837 |
| Component 7; daytime dysfunction | −0.201 | 0.014 * | −0.010 | 0.888 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jeon, Y.-S.; Yu, S.; Kim, C.; Lee, H.J.; Yoon, I.-Y.; Kim, T. Lower Serum Calcium Levels Associated with Disrupted Sleep and Rest–Activity Rhythm in Shift Workers. Nutrients 2022, 14, 3021. https://doi.org/10.3390/nu14153021
Jeon Y-S, Yu S, Kim C, Lee HJ, Yoon I-Y, Kim T. Lower Serum Calcium Levels Associated with Disrupted Sleep and Rest–Activity Rhythm in Shift Workers. Nutrients. 2022; 14(15):3021. https://doi.org/10.3390/nu14153021
Chicago/Turabian StyleJeon, Yi-Seon, Seungyeong Yu, Chaeyeon Kim, Hyuk Joo Lee, In-Young Yoon, and Tae Kim. 2022. "Lower Serum Calcium Levels Associated with Disrupted Sleep and Rest–Activity Rhythm in Shift Workers" Nutrients 14, no. 15: 3021. https://doi.org/10.3390/nu14153021
APA StyleJeon, Y.-S., Yu, S., Kim, C., Lee, H. J., Yoon, I.-Y., & Kim, T. (2022). Lower Serum Calcium Levels Associated with Disrupted Sleep and Rest–Activity Rhythm in Shift Workers. Nutrients, 14(15), 3021. https://doi.org/10.3390/nu14153021