
Dietary Supplements in People with Metastatic Cancer Who Are Experiencing Malnutrition, Cachexia, Sarcopenia, and Frailty: A Scoping Review

 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Aims and Methodology
3. Results
3.1. Search Results
3.2. Study Characteristics
3.3. Types of Dietary Supplements
3.4. Forms and Dosages
3.4.1. Vitamins, Minerals, and Other Antioxidants
3.4.2. Proteins and Amino Acids
3.4.3. Fatty Acids
3.4.4. Fiber
3.4.5. Others
3.5. Concomitant Interventions
3.6. Malnutrition-Related Conditions
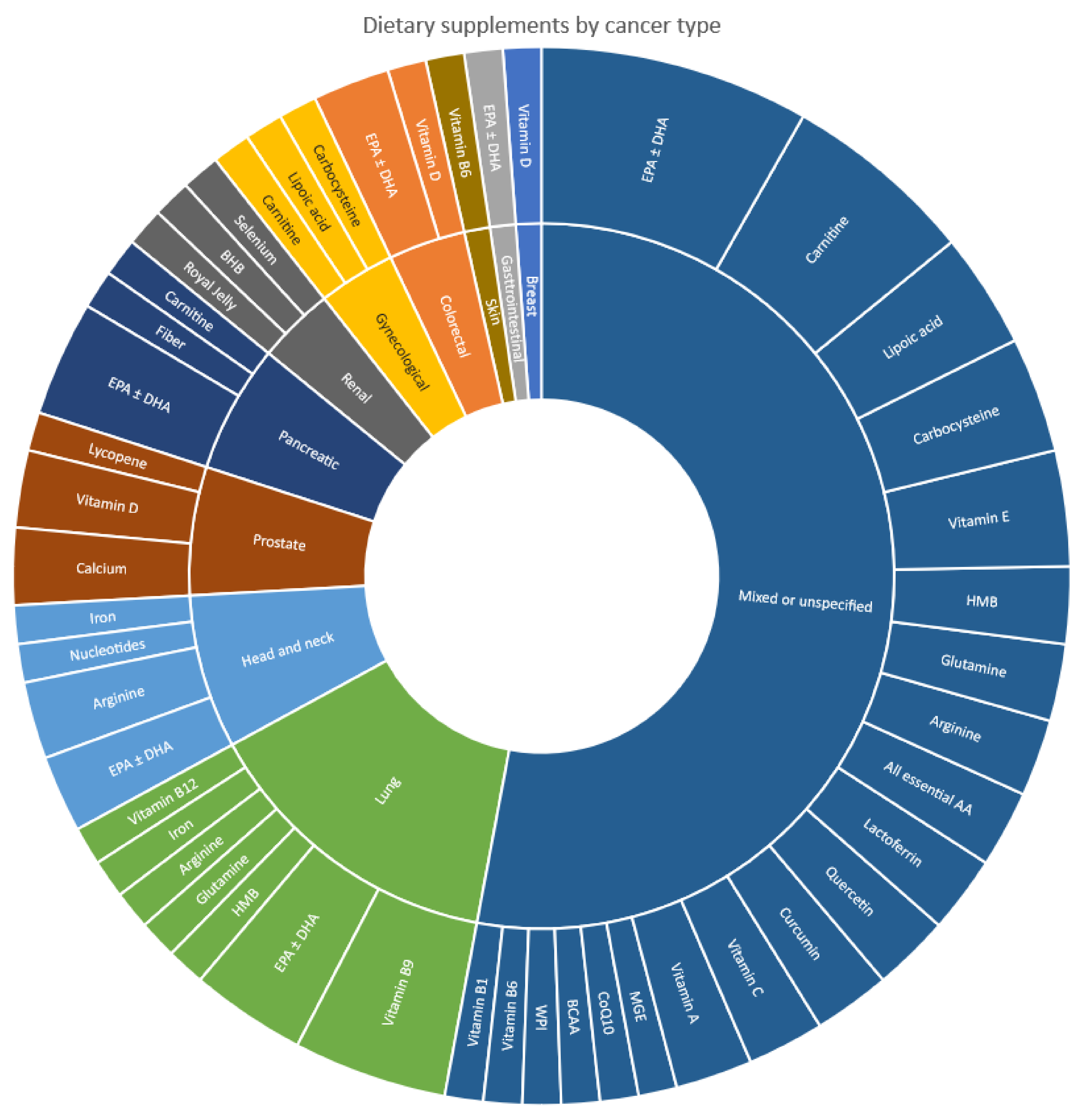
3.7. Cancer Types
3.8. Proposed Effects, Mechanisms/Rationale, and Outcome Measures
3.9. Tools Used in Outcome Measurements
4. Discussion
Implications for Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Miller, K.D.; Nogueira, L.; Mariotto, A.B.; Rowland, J.H.; Yabroff, K.R.; Alfano, C.M.; Jemal, A.; Kramer, J.L.; Siegel, R.L. Cancer treatment and survivorship statistics, 2019. CA Cancer J. Clin. 2019, 69, 363–385. [Google Scholar] [CrossRef] [PubMed]
- Fares, J.; Fares, M.Y.; Khachfe, H.H.; Salhab, H.A.; Fares, Y. Molecular principles of metastasis: A hallmark of cancer revisited. Signal Transduct. Target. Ther. 2020, 5, 28. [Google Scholar] [CrossRef] [PubMed]
- Siemens, W.; Schönsteiner, S.S.; Orellana-Rios, C.L.; Schaekel, U.; Kessler, J.; Eschbach, C.; Viehrig, M.; Mayer-Steinacker, R.; Becker, G.; Gaertner, J. Severe symptoms and very low quality-of-life among outpatients newly diagnosed with advanced cancer: Data from a multicenter cohort study. Support. Care Cancer 2020, 28, 5547. [Google Scholar] [CrossRef]
- Lovelace, D.L.; McDaniel, L.R.; Golden, D. Long-term effects of breast cancer surgery, treatment, and survivor care. J. Midwifery Womens Health 2019, 64, 713–724. [Google Scholar] [CrossRef]
- Moffat, G.T.; Epstein, A.S.; O’Reilly, E.M. Pancreatic cancer—A disease in need: Optimizing and integrating supportive care. Cancer 2019, 125, 3927–3935. [Google Scholar] [CrossRef]
- Brose, M.S.; Bible, K.C.; Chow, L.Q.; Gilbert, J.; Grande, C.; Worden, F.; Haddad, R. Management of treatment-related toxicities in advanced medullary thyroid cancer. Cancer Treat. Rev. 2018, 66, 64–73. [Google Scholar] [CrossRef]
- Chan, K.K.; Bass, A.R. Autoimmune complications of immunotherapy: Pathophysiology and management. BMJ 2020, 369, m376. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.; Molassiotis, A.; Chung, B.P.M.; Tan, J.-Y. Unmet care needs of advanced cancer patients and their informal caregivers: A systematic review. BMC Palliat. Care 2018, 17, 96. [Google Scholar] [CrossRef] [PubMed]
- Segura, A.; Pardo, J.; Jara, C.; Zugazabeitia, L.; Carulla, J.; de Las Peñas, R.; García-Cabrera, E.; Azuara, M.L.; Casadó, J.; Gómez-Candela, C. An epidemiological evaluation of the prevalence of malnutrition in Spanish patients with locally advanced or metastatic cancer. Clin. Nutr. 2005, 24, 801–814. [Google Scholar] [CrossRef] [PubMed]
- Muscaritoli, M.; Lucia, S.; Farcomeni, A.; Lorusso, V.; Saracino, V.; Barone, C.; Plastino, F.; Gori, S.; Magarotto, R.; Carteni, G. Prevalence of malnutrition in patients at first medical oncology visit: The PreMiO study. Oncotarget 2017, 8, 79884. [Google Scholar] [PubMed]
- Omlin, A.; Blum, D.; Wierecky, J.; Haile, S.R.; Ottery, F.D.; Strasser, F. Nutrition impact symptoms in advanced cancer patients: Frequency and specific interventions, a case–control study. J. Cachexia Sarcopenia Muscle 2013, 4, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Miller, J.; Wells, L.; Nwulu, U.; Currow, D.; Johnson, M.J.; Skipworth, R.J. Validated screening tools for the assessment of cachexia, sarcopenia, and malnutrition: A systematic review. Am. J. Clin. Nutr. 2018, 108, 1196–1208. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef]
- Sun, G.; Li, Y.; Peng, Y.; Lu, D.; Zhang, F.; Cui, X.; Zhang, Q.; Li, Z. Can sarcopenia be a predictor of prognosis for patients with non-metastatic colorectal cancer? A systematic review and meta-analysis. Int. J. Colorectal Dis. 2018, 33, 1419–1427. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.S.; Kim, Y.S.; Kim, E.Y.; Jin, W. Prognostic significance of CT-determined sarcopenia in patients with advanced gastric cancer. PLoS ONE 2018, 13, e0202700. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.-M.; Dou, Q.-L.; Zeng, Y.; Yang, Y.; Cheng, A.S.; Zhang, W.-W. Sarcopenia as a predictor of mortality in women with breast cancer: A meta-analysis and systematic review. BMC Cancer 2020, 20, 172. [Google Scholar] [CrossRef]
- Brown, J.C.; Harhay, M.O.; Harhay, M.N. The prognostic importance of frailty in cancer survivors. J. Am. Geriatr. Soc. 2015, 63, 2538–2543. [Google Scholar] [CrossRef]
- Balducci, L.; Stanta, G. Cancer in the frail patient: A coming epidemic. Hematol. Oncol. Clin. N. Am. 2000, 14, 235–250. [Google Scholar] [CrossRef]
- Ethun, C.G.; Bilen, M.A.; Jani, A.B.; Maithel, S.K.; Ogan, K.; Master, V.A. Frailty and cancer: Implications for oncology surgery, medical oncology, and radiation oncology. CA Cancer J. Clin. 2017, 67, 362–377. [Google Scholar] [CrossRef]
- Jeejeebhoy, K.N. Malnutrition, fatigue, frailty, vulnerability, sarcopenia and cachexia: Overlap of clinical features. Curr. Opin. Clin. Nutr. Metab. Care 2012, 15, 213–219. [Google Scholar] [CrossRef]
- Arends, J.; Bachmann, P.; Baracos, V.; Barthelemy, N.; Bertz, H.; Bozzetti, F.; Fearon, K.; Hütterer, E.; Isenring, E.; Kaasa, S. ESPEN guidelines on nutrition in cancer patients. Clin. Nutr. 2017, 36, 11–48. [Google Scholar] [CrossRef]
- Kanarek, N.; Petrova, B.; Sabatini, D.M. Dietary modifications for enhanced cancer therapy. Nature 2020, 579, 507–517. [Google Scholar] [CrossRef] [PubMed]
- European Food Safety Authority. Food Supplements. Available online: https://www.efsa.europa.eu/en/topics/topic/food-supplements (accessed on 7 April 2022).
- U.S. Food & Drug Administration. Dietary Supplement Products & Ingredients. Available online: https://www.fda.gov/food/dietary-supplements/dietary-supplement-products-ingredients (accessed on 7 April 2022).
- Velicer, C.M.; Ulrich, C.M. Vitamin and mineral supplement use among US adults after cancer diagnosis: A systematic review. J. Clin. Oncol. 2008, 26, 665–673. [Google Scholar] [CrossRef] [PubMed]
- Luo, Q.; Asher, G.N. Use of dietary supplements at a comprehensive cancer center. J. Altern. Complement. Med. 2018, 24, 981–987. [Google Scholar] [CrossRef] [PubMed]
- Mochamat; Cuhls, H.; Marinova, M.; Kaasa, S.; Stieber, C.; Conrad, R.; Radbruch, L.; Mücke, M. A systematic review on the role of vitamins, minerals, proteins, and other supplements for the treatment of cachexia in cancer: A European Palliative Care Research Centre cachexia project. J. Cachexia Sarcopenia Muscle 2017, 8, 25–39. [Google Scholar] [CrossRef] [PubMed]
- Peters, M.D.; Marnie, C.; Tricco, A.C.; Pollock, D.; Munn, Z.; Alexander, L.; McInerney, P.; Godfrey, C.M.; Khalil, H.J. Updated methodological guidance for the conduct of scoping reviews. JBI Evid. Synth. 2020, 18, 2119–2126. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.; Horsley, T.; Weeks, L. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Covidence Systematic Review Software, Veritas Health Innovation. Melbourne, Australia. Available online: www.covidence.org (accessed on 17 May 2022).
- National Institutes of Health Office of Dietary Supplements. Background Information: Dietary Supplements. Available online: https://ods.od.nih.gov/factsheets/DietarySupplements-Consumer/ (accessed on 17 May 2022).
- von Haehling, S.; Anker, S.D. Cachexia as a major underestimated and unmet medical need: Facts and numbers. J. Cachexia Sarcopenia Muscle 2010, 1, 1–5. [Google Scholar] [CrossRef]
- Pollock, D.; Davies, E.L.; Peters, M.D.J.; Tricco, A.C.; Alexander, L.; McInerney, P.; Godfrey, C.M.; Khalil, H.; Munn, Z. Undertaking a scoping review: A practical guide for nursing and midwifery students, clinicians, researchers, and academics. J. Adv. Nurs. 2021, 77, 2102–2113. [Google Scholar] [CrossRef]
- Araki, K.; Miyata, Y.; Ohba, K.; Nakamura, Y.; Matsuo, T.; Mochizuki, Y.; Sakai, H. Oral Intake of Royal Jelly Has Protective Effects Against Tyrosine Kinase Inhibitor-Induced Toxicity in Patients with Renal Cell Carcinoma: A Randomized, Double-Blinded, Placebo-Controlled Trial. Medicines 2018, 6, 2. [Google Scholar] [CrossRef]
- Berk, L.; James, J.; Schwartz, A.; Hug, E.; Mahadevan, A.; Samuels, M.; Kachnic, L. A randomized, double-blind, placebo-controlled trial of a beta-hydroxyl beta-methyl butyrate, glutamine, and arginine mixture for the treatment of cancer cachexia (RTOG 0122). Support. Care Cancer 2008, 16, 1179–1188. [Google Scholar] [CrossRef] [PubMed]
- Buijs, N.; van Bokhorst-de van der Schueren, M.A.; Langius, J.A.; Leemans, C.R.; Kuik, D.J.; Vermeulen, M.A.; van Leeuwen, P.A. Perioperative arginine-supplemented nutrition in malnourished patients with head and neck cancer improves long-term survival. Am. J. Clin. Nutr. 2010, 92, 1151–1156. [Google Scholar] [CrossRef] [PubMed]
- Cerchietti, L.C.; Navigante, A.H.; Castro, M.A. Effects of eicosapentaenoic and docosahexaenoic n-3 fatty acids from fish oil and preferential Cox-2 inhibition on systemic syndromes in patients with advanced lung cancer. Nutr. Cancer 2007, 59, 14–20. [Google Scholar] [CrossRef]
- Cereda, E.; Turri, A.; Klersy, C.; Cappello, S.; Ferrari, A.; Filippi, A.R.; Brugnatelli, S.; Caraccia, M.; Chiellino, S.; Borioli, V.; et al. Whey protein isolate supplementation improves body composition, muscle strength, and treatment tolerance in malnourished advanced cancer patients undergoing chemotherapy. Cancer Med. 2019, 8, 6923–6932. [Google Scholar] [CrossRef]
- Gogos, C.A.; Ginopoulos, P.; Salsa, B.; Apostolidou, E.; Zoumbos, N.C.; Kalfarentzos, F. Dietary omega-3 polyunsaturated fatty acids plus vitamin E restore immunodeficiency and prolong survival for severely ill patients with generalized malignancy: A randomized control trial. Cancer 1998, 82, 395–402. [Google Scholar] [CrossRef]
- Antunac Golubić, Z.; Baršić, I.; Librenjak, N.; Pleština, S. Vitamin D Supplementation and Survival in Metastatic Colorectal Cancer. Nutr. Cancer 2018, 70, 413–417. [Google Scholar] [CrossRef] [PubMed]
- Kraft, M.; Kraft, K.; Gärtner, S.; Mayerle, J.; Simon, P.; Weber, E.; Schütte, K.; Stieler, J.; Koula-Jenik, H.; Holzhauer, P.; et al. L-Carnitine-supplementation in advanced pancreatic cancer (CARPAN)--a randomized multicentre trial. Nutr. J. 2012, 11, 52. [Google Scholar] [CrossRef] [PubMed]
- Macciò, A.; Madeddu, C.; Gramignano, G.; Mulas, C.; Floris, C.; Sanna, E.; Cau, M.C.; Panzone, F.; Mantovani, G. A randomized phase III clinical trial of a combined treatment for cachexia in patients with gynecological cancers: Evaluating the impact on metabolic and inflammatory profiles and quality of life. Gynecol. Oncol. 2012, 124, 417–425. [Google Scholar] [CrossRef]
- Macciò, A.; Madeddu, C.; Gramignano, G.; Mulas, C.; Sanna, E.; Mantovani, G. Efficacy and safety of oral lactoferrin supplementation in combination with rHuEPO-beta for the treatment of anemia in advanced cancer patients undergoing chemotherapy: Open-label, randomized controlled study. Oncologist 2010, 15, 894–902. [Google Scholar] [CrossRef]
- Mantovani, G.; Macciò, A.; Madeddu, C.; Serpe, R.; Massa, E.; Dessì, M.; Panzone, F.; Contu, P. Randomized phase III clinical trial of five different arms of treatment in 332 patients with cancer cachexia. Oncologist 2010, 15, 200–211. [Google Scholar] [CrossRef]
- May, P.E.; Barber, A.; D’Olimpio, J.T.; Hourihane, A.; Abumrad, N.N. Reversal of cancer-related wasting using oral supplementation with a combination of beta-hydroxy-beta-methylbutyrate, arginine, and glutamine. Am. J. Surg. 2002, 183, 471–479. [Google Scholar] [CrossRef]
- Ohe, Y.; Ichinose, Y.; Nakagawa, K.; Tamura, T.; Kubota, K.; Yamamoto, N.; Adachi, S.; Nambu, Y.; Fujimoto, T.; Nishiwaki, Y.; et al. Efficacy and safety of two doses of pemetrexed supplemented with folic acid and vitamin B12 in previously treated patients with non-small cell lung cancer. Clin. Cancer Res. 2008, 14, 4206–4212. [Google Scholar] [CrossRef] [PubMed]
- Pratt, V.C.; Watanabe, S.; Bruera, E.; Mackey, J.; Clandinin, M.T.; Baracos, V.E.; Field, C.J. Plasma and neutrophil fatty acid composition in advanced cancer patients and response to fish oil supplementation. Br. J. Cancer 2002, 87, 1370–1378. [Google Scholar] [CrossRef]
- Sánchez-Lara, K.; Turcott, J.G.; Juárez-Hernández, E.; Nuñez-Valencia, C.; Villanueva, G.; Guevara, P.; De la Torre-Vallejo, M.; Mohar, A.; Arrieta, O. Effects of an oral nutritional supplement containing eicosapentaenoic acid on nutritional and clinical outcomes in patients with advanced non-small cell lung cancer: Randomised trial. Clin. Nutr. 2014, 33, 1017–1023. [Google Scholar] [CrossRef] [PubMed]
- Shirai, Y.; Okugawa, Y.; Hishida, A.; Ogawa, A.; Okamoto, K.; Shintani, M.; Morimoto, Y.; Nishikawa, R.; Yokoe, T.; Tanaka, K.; et al. Fish oil-enriched nutrition combined with systemic chemotherapy for gastrointestinal cancer patients with cancer cachexia. Sci. Rep. 2017, 7, 4826. [Google Scholar] [CrossRef]
- Solheim, T.S.; Laird, B.J.A.; Balstad, T.R.; Stene, G.B.; Bye, A.; Johns, N.; Pettersen, C.H.; Fallon, M.; Fayers, P.; Fearon, K.; et al. A randomized phase II feasibility trial of a multimodal intervention for the management of cachexia in lung and pancreatic cancer. J. Cachexia Sarcopenia Muscle 2017, 8, 778–788. [Google Scholar] [CrossRef]
- Ueno, M.; Sugimori, K.; Taguri, M.; Ohkawa, S.; Kobayashi, S.; Miwa, H.; Kaneko, T.; Morimoto, M.; Yamanaka, T. Randomized Phase II Study of Gemcitabine Monotherapy vs. Gemcitabine with an EPA-Enriched Oral Supplement in Advanced Pancreatic Cancer. Nutr. Cancer 2022, 74, 122–130. [Google Scholar] [CrossRef]
- Bitting, R.L.; Tooze, J.A.; Isom, S.; Petty, W.J.; Grant, S.C.; Desnoyers, R.J.; Thomas, A.; Thomas, C.Y.; Alistar, A.T.; Golden, S.L.; et al. Phase I Study of Muscadine Grape Extract for Patients With Advanced Cancer. Am. J. Clin. Oncol. 2021, 44, 239–246. [Google Scholar] [CrossRef]
- Gramignano, G.; Lusso, M.R.; Madeddu, C.; Massa, E.; Serpe, R.; Deiana, L.; Lamonica, G.; Dessì, M.; Spiga, C.; Astara, G.; et al. Efficacy of l-carnitine administration on fatigue, nutritional status, oxidative stress, and related quality of life in 12 advanced cancer patients undergoing anticancer therapy. Nutrition 2006, 22, 136–145. [Google Scholar] [CrossRef]
- Mantovani, G.; Macciò, A.; Madeddu, C.; Gramignano, G.; Lusso, M.R.; Serpe, R.; Massa, E.; Astara, G.; Deiana, L. A phase II study with antioxidants, both in the diet and supplemented, pharmaconutritional support, progestagen, and anti-cyclooxygenase-2 showing efficacy and safety in patients with cancer-related anorexia/cachexia and oxidative stress. Cancer Epidemiol. Biomarkers Prev. 2006, 15, 1030–1034. [Google Scholar] [CrossRef]
- Murphy, R.A.; Mourtzakis, M.; Chu, Q.S.; Baracos, V.E.; Reiman, T.; Mazurak, V.C. Nutritional intervention with fish oil provides a benefit over standard of care for weight and skeletal muscle mass in patients with nonsmall cell lung cancer receiving chemotherapy. Cancer 2011, 117, 1775–1782. [Google Scholar] [CrossRef]
- Naito, T.; Mitsunaga, S.; Miura, S.; Tatematsu, N.; Inano, T.; Mouri, T.; Tsuji, T.; Higashiguchi, T.; Inui, A.; Okayama, T.; et al. Feasibility of early multimodal interventions for elderly patients with advanced pancreatic and non-small-cell lung cancer. J. Cachexia Sarcopenia Muscle 2019, 10, 73–83. [Google Scholar] [CrossRef] [PubMed]
- Pascoe, J.; Jackson, A.; Gaskell, C.; Gaunt, C.; Thompson, J.; Billingham, L.; Steven, N. Beta-hydroxy beta-methylbutyrate/arginine/glutamine (HMB/Arg/Gln) supplementation to improve the management of cachexia in patients with advanced lung cancer: An open-label, multicentre, randomised, controlled phase II trial (NOURISH). BMC Cancer 2021, 21, 800. [Google Scholar] [CrossRef] [PubMed]
- Read, J.A.; Beale, P.J.; Volker, D.H.; Smith, N.; Childs, A.; Clarke, S.J. Nutrition intervention using an eicosapentaenoic acid (EPA)-containing supplement in patients with advanced colorectal cancer. Effects on nutritional and inflammatory status: A phase II trial. Support. Care Cancer 2007, 15, 301–307. [Google Scholar] [CrossRef]
- Maureen Sheean, P.; Robinson, P.; Bartolotta, M.B.; Joyce, C.; Adams, W.; Penckofer, S. Associations Between Cholecalciferol Supplementation and Self-Reported Symptoms Among Women With Metastatic Breast Cancer and Vitamin D Deficiency: A Pilot Study. Oncol. Nurs. Forum 2021, 48, 352–360. [Google Scholar] [CrossRef] [PubMed]
- Takagi, Y.; Hosomi, Y.; Nagamata, M.; Watanabe, K.; Takahashi, S.; Nakahara, Y.; Yomota, M.; Sunami, K.; Okuma, Y.; Shimokawa, T.; et al. Phase II study of oral vitamin B12 supplementation as an alternative to intramuscular injection for patients with non-small cell lung cancer undergoing pemetrexed therapy. Cancer Chemother. Pharmacol. 2016, 77, 559–564. [Google Scholar] [CrossRef]
- Takagi, Y.; Hosomi, Y.; Sunami, K.; Nakahara, Y.; Okuma, Y.; Yomota, M.; Shimokawa, T.; Nagamata, M.; Iguchi, M.; Okamoto, H.; et al. A prospective study of shortened vitamin supplementation prior to cisplatin-pemetrexed therapy for non-small cell lung cancer. Oncologist 2014, 19, 1194–1199. [Google Scholar] [CrossRef][Green Version]
- Tałalaj, M.; Kapitan-Malinowska, B.; Debski, K.; Nowakowski, R.; Marcinowska-Suchowierska, E.; Witeska, A. Administration of 1 alpha-OH vitamin D3 and calcium prevents bone mass loss in patients with advanced prostatic carcinoma after orchidectomy treated with complete androgenic blockade. Endokrynol. Pol. 2005, 56, 225–232. [Google Scholar]
- Taylor, L.A.; Pletschen, L.; Arends, J.; Unger, C.; Massing, U. Marine phospholipids--a promising new dietary approach to tumor-associated weight loss. Support. Care Cancer 2010, 18, 159–170. [Google Scholar] [CrossRef]
- Van Veldhuizen, P.J.; Taylor, S.A.; Williamson, S.; Drees, B.M. Treatment of vitamin D deficiency in patients with metastatic prostate cancer may improve bone pain and muscle strength. J. Urol. 2000, 163, 187–190. [Google Scholar] [CrossRef]
- Wigmore, S.J.; Barber, M.D.; Ross, J.A.; Tisdale, M.J.; Fearon, K.C. Effect of oral eicosapentaenoic acid on weight loss in patients with pancreatic cancer. Nutr. Cancer 2000, 36, 177–184. [Google Scholar] [CrossRef] [PubMed]
- Zhuang, E.; Uchio, E.; Lilly, M.; Zi, X.; Fruehauf, J.P. A phase II study of docetaxel plus lycopene in metastatic castrate resistant prostate cancer. Biomed. Pharmacother. 2021, 143, 112226. [Google Scholar] [CrossRef] [PubMed]
- Barajas-Galindo, D.E.; Vidal-Casariego, A.; Pintor-de la Maza, B.; Fernández-Martínez, P.; Ramos-Martínez, T.; García-Arias, S.; Hernández-Moreno, A.; Urioste-Fondo, A.; Cano-Rodríguez, I.; Ballesteros-Pomar, M.D. Postoperative enteral immunonutrition in head and neck cancer patients: Impact on clinical outcomes. Endocrinol Diabetes Nutr. (Engl. Ed.) 2020, 67, 13–19. [Google Scholar] [PubMed]
- Singh, N.; Aggarwal, A.N.; Kaur, J.; Behera, D. Association of Graded Folic Acid Supplementation and Total Plasma Homocysteine Levels With Hematological Toxicity During First-line Treatment of Nonsquamous NSCLC Patients With Pemetrexed-based Chemotherapy. Am. J. Clin. Oncol. 2017, 40, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Ramalho, R.; Ramalho, P.; Couto, N.; Pereira, P. Omega-3 therapeutic supplementation in a patient with metastatic adenocarcinoma of the pancreas with muscle mass depletion. Eur. J. Clin. Nutr. 2017, 71, 795–797. [Google Scholar] [CrossRef]
- Rauf, M.; Gleason, C.; Nooka, A.K.; Husman, A.; Waller, E.K. Treatment of severe neutropenia with high-dose pyridoxine in a patient with chronic graft versus host disease and squamous cell carcinoma: A case report. J. Med. Case Rep. 2011, 5, 372. [Google Scholar] [CrossRef]
- Yoshii, R.; Yokoyama, J.; Ohba, S.; Fujimaki, M.; Kojima, M.; Ikeda, K. Impact of EPA nutritional approach on cachexic patients with advanced hypopharyngeal cancer treated by induction chemotherapy. Head Neck Oncol. 2014, 6, 18. [Google Scholar]
- Von Haehling, S. Novel treatment approaches to cancer cachexia: Results from two recent randomized controlled trials using essential amino acids and espindolol. J. Cachexia Sarcopenia Muscle 2017, 8, 151. [Google Scholar]
- Madeddu, C.; Gramignano, G.; Tanca, L.; Cherchi, M.C.; Floris, C.A.; Macciò, A. A combined treatment approach for cachexia and cancer-related anemia in advanced cancer patients: A randomized placebo-controlled trial. J. Clin. Oncol. 2014, 32, 189. [Google Scholar] [CrossRef]
- Madeddu, C.; Maccio, A.; Gramignano, G.; Mulas, C.; Floris, C.; Sanna, E.; Cau, M.C.; Panzone, F.; Dessi, M.; Serpe, R.; et al. A randomized phase III clinical trial of a combined treatment with megestrol acetate+carnitine+celecoxib+antioxidants vs. Megestrol acetate alone for patients with cancer cachexia syndrome. Support. Care Cancer 2012, 20, S57–S58. [Google Scholar]
- Garje, R.; Brown, J.A.; Nepple, K.G.; Dahmoush, L.; Bellizzi, A.; Bonner, J.; Mott, S.L.; Zamba, G.; Laux, D.E.; Milhem, M.M.; et al. Preliminary results of phase I clinical trial of high doses of seleno-L-methionine (SLM) in sequential combination with axitinib in previously treated and relapsed clear cell renal cell carcinoma (ccRCC) patients. J. Clin. Oncol. 2019, 37, 660. [Google Scholar] [CrossRef]
- Lugini, A. Phase II clinical trial using aminotrofic in the prevention of anorexia and cachexia in cancer patients receiving chemotherapy: Evaluation of the efficacy and safety. Support. Care Cancer 2013, 21, 46. [Google Scholar]
- Mantovani, G.; Madeddu, C.; Panzone, F.; Cau, M.C.; Antoni, G.; Leo, F.d.; Macciò, A.; Serpe, R. Curcuma Longa extract is effective in improving inflammatory status and redox balance in patients with cancer-related cachexia and oxidative stress. Ann. Oncol. 2012, 23, 463. [Google Scholar] [CrossRef]
- Serpe, R.; Madeddu, C.; Panzone, F.; Antoni, G.; Cau, M.C.; Macciò, A.; Mantovani, G.; Banni, S. Krill oil to improve blood lipids status in advanced cancer patient with cachexia. J. Clin. Oncol. 2012, 30, e19634. [Google Scholar] [CrossRef]
- Ricottone, N. Preventive Surcosomial® iron supplementation in an elder patient undergoing exclusive radiation therapy treatment for nasopharyngeal cancer with laterocervical lymph node metastasis: Clinical case. Expert Rev. Hematol. 2017, 10, 25. [Google Scholar]
- NCT00398333. Study to Assess the Effectiveness of a Omega-3 Enriched Supplement on Chemotherapy Tolerance in Colon Cancer Patients. Available online: https://clinicaltrials.gov/ct2/show/NCT00398333 (accessed on 17 May 2022).
- NCT05119010. A Pilot Study Evaluating a Ketogenic Diet Concomitant to Nivolumab and Ipilimumab in Patients with Metastatic Renal Cell Carcinoma (KETOREIN). Available online: https://clinicaltrials.gov/ct2/show/NCT05119010 (accessed on 17 May 2022).
- Miyata, Y.; Araki, K.; Ohba, K.; Mastuo, T.; Nakamura, Y.; Yuno, T.; Mukai, Y.; Otsubo, A.; Mitsunari, K.; Mochizuki, Y.; et al. Oral intake of royal jelly improves anti-cancer effects and suppresses adverse events of molecular targeted therapy by regulating TNF-α and TGF-β in renal cell carcinoma: A preliminary study based on a randomized double-blind clinical trial. Mol. Clin. Oncol. 2020, 13, 29. [Google Scholar] [CrossRef]
- Martin, L.; Birdsell, L.; MacDonald, N.; Reiman, T.; Clandinin, M.T.; McCargar, L.J.; Murphy, R.; Ghosh, S.; Sawyer, M.B.; Baracos, V.E. Cancer cachexia in the age of obesity: Skeletal muscle depletion is a powerful prognostic factor, independent of body mass index. J. Clin. Oncol. 2013, 31, 1539–1547. [Google Scholar] [CrossRef]
- de Aguiar Pastore Silva, J.; Emilia de Souza Fabre, M.; Waitzberg, D.L. Omega-3 supplements for patients in chemotherapy and/or radiotherapy: A systematic review. Clin. Nutr. 2015, 34, 359–366. [Google Scholar] [CrossRef]
- Colomer, R.; Moreno-Nogueira, J.M.; García-Luna, P.P.; García-Peris, P.; García-de-Lorenzo, A.; Zarazaga, A.; Quecedo, L.; del Llano, J.; Usán, L.; Casimiro, C. n-3 Fatty acids, cancer and cachexia: A systematic review of the literature. Br. J. Nutr. 2007, 97, 823–831. [Google Scholar] [CrossRef]
- Dewey, A.; Baughan, C.; Dean, T.; Higgins, B.; Johnson, I. Eicosapentaenoic acid (EPA, an omega-3 fatty acid from fish oils) for the treatment of cancer cachexia. Cochrane Database Syst. Rev. 2007, 2007, CD004597. [Google Scholar] [CrossRef]
- Dickinson, A. History and overview of DSHEA. Fitoterapia 2011, 82, 5–10. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Inclusion Criteria | Additional Operational Information |
|---|---|
| Human studies | - |
| Primary, quantitative studies, or systematic reviews | Systematic reviews are defined as reviews with a comprehensive search strategy, methods section, and critical appraisal of included studies |
| Studies investigating the effects of dietary supplements (vitamins, minerals, proteins or amino acids, fatty acids, prebiotics or fiber, probiotics, and plant or herbal extracts) whether in isolation or in combination with other dietary supplements or interventions | This includes studies where dietary supplements were not the intervention of interest or all study groups received the same dietary supplements, as intra-group comparisons may have been made, which can provide information on the effects of dietary supplements. |
| Studies conducted among people with metastatic cancer (defined as Stage IV) | This is further defined by the following cut-off values: for primary trials, at least 50% metastatic; for systematic reviews, at least 50% included papers conducted in solely metastatic populations; for studies yet to be completed, only those that set out to recruit solely patients with metastatic cancers. |
| Studies including people with malnutrition cachexia or anorexia, sarcopenia, frailty, or weight loss | Studies that consisted of a subset of patients (any proportion) with these conditions were included. Nutrient deficiencies were also considered a form of malnutrition. If the nutrition status of study participants was not specified, articles were considered to meet the inclusion criteria regarding malnutrition-related conditions as long as they meet the earlier criteria of metastatic cancer, as it has been established in the literature that malnutrition is prevalent in people with advanced cancer [32]. |
| Exclusion Criteria | |
| Animal or laboratory studies | |
| Qualitative studies or narrative/literature reviews | |
| Studies investigating the effects of drugs or traditional medicine (e.g., Chinese herbal therapies) | |
| Supplements administered via intravenous or intramuscular routes (e.g., intravenous ascorbic acid infusion) | |
| Studies investigating the effect of oral nutritional supplements alone, which have not been enhanced with dietary supplement(s) of interest (e.g., unfortified standard formulations of commercial milk-based supplements, such as Ensure®) | |
| Study Type | Number of Studies | Total Participants Range |
|---|---|---|
| Full-text article | ||
| Randomized controlled trial | 18 | 22–472 |
| Quasi-experimental trial | 15 | 12–144 |
| Retrospective cohort observational | 2 | 111–135 |
| Case study | 3 | 1 |
| Conference abstracts | ||
| Randomized controlled trial | 3 | 50–127 |
| Quasi-experimental trial | 4 | 12–36 |
| Case study | 1 | 1 |
| Clinical trial registrations | ||
| Randomized controlled trial | 1 | 13 |
| Cancer Type (Primary) | ||
| Breast | 1 | 11 |
| Colorectal | 3 | 13–72 |
| Gastrointestinal | 1 | 128 |
| Gynecological | 1 | 104 |
| Head and neck | 4 | 1–135 |
| Lung | 8 | 22–225 |
| Pancreatic | 4 | 1–72 |
| Prostate | 3 | 13–51 |
| Renal | 2 | 12–33 |
| Skin | 1 | 1 |
| Mixed or not specified | 19 | 12–472 |
| Country | ||
| Argentina | 1 | 22 |
| Australia | 1 | 23 |
| Canada | 2 | 23–144 |
| Croatia | 1 | 72 |
| Germany | 3 | 31–72 |
| Greece | 1 | 60 |
| India | 1 | 111 |
| Italy | 12 | 1–332 |
| Japan | 8 | 1–225 |
| Mexico | 1 | 92 |
| Netherlands | 1 | 32 |
| Poland | 1 | 1–51 |
| Portugal | 1 | 1 |
| Scotland | 1 | 26 |
| Spain | 2 | 13–135 |
| United States | 8 | 1–472 |
| United Kingdom | 2 | 38–46 |
| Author/ Year Trial No./ Clinical Trial Phase | Cancer | Conditions | Vitamins | Minerals | Antioxidants | Proteins | Amino Acids | FA | Fr | Others | |||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Vitamin A | Vitamin B1 | Vitamin B6 | Vitamin B9 | Vitamin B12 | Vitamin C | Vitamin D | Vitamin E | Calcium | Iron | Selenium | Carbocysteine | Curcumin | Lipoic acid | Lycopene | Quercetin | Lactoferrin | Whey protein isolate | Essential amino acids | Arginine | BCAA | Carnitine | Glutamine | HMB | EPA ± DHA | Fiber | BHB | Coenzyme Q10 | Muscadine Grape Extract | Nucleotides | Royal Jelly | |||
| Full-Text Article | |||||||||||||||||||||||||||||||||
| RCT | |||||||||||||||||||||||||||||||||
| Araki 2019 [34] UMIN000020152 Phase NS | Renal | NS | X | ||||||||||||||||||||||||||||||
| Berk 2008 [35] Trial no. NS Phase III | Mixed | Weight loss | X | X | X | ||||||||||||||||||||||||||||
| Buijs 2010 [36] Trial no. and phase NS | HN | Malnutrition | X | ||||||||||||||||||||||||||||||
| Cerchietti 2007 [37] Trial no. and phase NS | Lung | Cachexia, anorexia | X | ||||||||||||||||||||||||||||||
| Cereda 2019 [38] NCT02065726 Phase NS | Mixed | Malnutrition | X | ||||||||||||||||||||||||||||||
| Gogos 1998 [39] Trial no. and phase NS | Mixed | Malnutrition | X | X | |||||||||||||||||||||||||||||
| Golubić 2018 [40] Trial no. and phase NS | COL | Vitamin D insufficiency | X | ||||||||||||||||||||||||||||||
| Kraft 2012 [41] NCT01330823 Phase NS | PanC | Weight loss | X | ||||||||||||||||||||||||||||||
| Maccio 2012 [42] Trial no. NS Phase III | GYN | Weight loss | X | X | X | ||||||||||||||||||||||||||||
| Maccio 2010 [43] Trial no. and phase NS | Mixed | Anemia | X | ||||||||||||||||||||||||||||||
| Mantovani 2010 [44] Trial no. NS Phase III | Mixed | Cachexia | X | X | X | X | X | X | X | X | |||||||||||||||||||||||
| May 2002 [45] Trial no. and phase NS | Mixed | Weight loss | X | X | X | ||||||||||||||||||||||||||||
| Ohe 2008 [46] Trial no. NS Phase II | Lung | NS | X | ||||||||||||||||||||||||||||||
| Pratt 2002 [47] Trial no. and phase NS | Mixed | Anorexia, weight loss | X | ||||||||||||||||||||||||||||||
| Sanchez-Lara 2014 [48] NCT01048970 Phase NS | Lung | Malnutrition, weight loss | X | ||||||||||||||||||||||||||||||
| Shirai 2017 [49] Trial no. and phase NS | GI | NS | X | ||||||||||||||||||||||||||||||
| Solheim 2017 [50] NCT01419145 Phase II | Mixed | Cachexia | X | ||||||||||||||||||||||||||||||
| Ueno 2022 [51] UMIN000003658 Phase II | PanC | Cachexia | X | ||||||||||||||||||||||||||||||
| Quasi-experimental trial | |||||||||||||||||||||||||||||||||
| Bitting 2021 [52] NCT02583269 Phase I | Mixed | NS | X | ||||||||||||||||||||||||||||||
| Gramignano 2006 [53] Trial no. and phase NS | Mixed | NS | X | ||||||||||||||||||||||||||||||
| Mantovani 2006 [54] Trial no. NS Phase II | Mixed | Weight loss | X | X | X | X | X | X | X | ||||||||||||||||||||||||
| Murphy 2011 [55] Trial no. NS Phase I | Lung | Weight loss | X | ||||||||||||||||||||||||||||||
| Naito 2019 [56] UMIN000023207 Phase NS | Mixed | Cachexia, muscle/weight loss | X | X | X | ||||||||||||||||||||||||||||
| Pascoe 2021 [57] ISRCTN39911673 Phase II | Lung | Cachexia | X | X | X | ||||||||||||||||||||||||||||
| Read 2007 [58] Trial no. NS Phase II | COL | Malnutrition | X | ||||||||||||||||||||||||||||||
| Sheean 2021 [59] NCT02186015 Phase I | Breast | Vitamin D insufficiency | X | ||||||||||||||||||||||||||||||
| Takagi 2016 [60] UMIN000003180 Phase II | Lung | NS | X | X | |||||||||||||||||||||||||||||
| Takagi 2014 [61] UMIN000006546 Phase II | Lung | NS | X | ||||||||||||||||||||||||||||||
| Talalaj 2005 [62] Trial no. and phase NS | ProST | NS | X | X | |||||||||||||||||||||||||||||
| Taylor 2010 [63] Trial no. and phase NS | Mixed | Cachexia | X | ||||||||||||||||||||||||||||||
| Van Veldhuizen 2000 [64] Trial no. NS Phase II | Prostate | Vitamin D insufficiency | X | X | |||||||||||||||||||||||||||||
| Wigmore 2000 [65] Trial no. NS Phase I/II | PanC | Weight loss | X | ||||||||||||||||||||||||||||||
| Zhuang 2021 [66] NCT01882985 Phase II | ProST | NS | X | ||||||||||||||||||||||||||||||
| Retrospective cohort observational | |||||||||||||||||||||||||||||||||
| Barajas-Galindo 2020 [67] Trial no. and phase NS | HN | Malnutrition | X | X | X | ||||||||||||||||||||||||||||
| Singh 2017 [68] Trial no. and phase NS | Lung | NS | X | X | |||||||||||||||||||||||||||||
| Case study | |||||||||||||||||||||||||||||||||
| Ramalho 2017 [69] Trial no. and phase N/A | PanC | NS | X | X | |||||||||||||||||||||||||||||
| Rauf 2011 [70] Trial no. and phase N/A | Skin | Vitamin B6 deficiency, cachexia | X | ||||||||||||||||||||||||||||||
| Yoshii 2014 [71] Trial no. and phase NS | HN | Cachexia | X | ||||||||||||||||||||||||||||||
| Conference Abstract | |||||||||||||||||||||||||||||||||
| RCT | |||||||||||||||||||||||||||||||||
| Haehling 2017 [72] Trial no. and phase NS | Mixed | Cachexia | X | ||||||||||||||||||||||||||||||
| Madeddu 2014 [73] Trial no. and phase NS | NS | Cachexia | X | X | X | ||||||||||||||||||||||||||||
| Madeddu 2012 [74] Trial no. NS Phase III | Mixed | Cachexia | X | X | X | ||||||||||||||||||||||||||||
| Quasi-experimental trial | |||||||||||||||||||||||||||||||||
| Garje 2019 [75] NCT02535533 Phase I | Renal | NS | X | ||||||||||||||||||||||||||||||
| Lugini 2013 [76] Trial no. NS Phase II | NS | NS | X | X | X | ||||||||||||||||||||||||||||
| Mantovani 2012 [77] Trial no. and phase NS | Mixed | Cachexia | X | ||||||||||||||||||||||||||||||
| Serpe 2012 [78] Trial no. and phase NS | Mixed | Cachexia | X | ||||||||||||||||||||||||||||||
| Case Report | |||||||||||||||||||||||||||||||||
| Ricottone 2017 [79] Trial no. and phase N/A | HN | Anemia | X | ||||||||||||||||||||||||||||||
| Clinical Trial Registration | |||||||||||||||||||||||||||||||||
| RCT | |||||||||||||||||||||||||||||||||
| NCT00398333 [80] Phase IV | COL | NS | X | ||||||||||||||||||||||||||||||
| Quasi-experimental trial | |||||||||||||||||||||||||||||||||
| NCT05119010 [81] Phase NS | Renal | NS | X | ||||||||||||||||||||||||||||||
| Dietary Supplement | Hypothesized Effects | Proposed Mechanisms or Rationale | Outcome Measures in Studies Where the Dietary Supplement Was Included |
|---|---|---|---|
| Vitamins, minerals, and other antioxidants | |||
| Vitamin A | Functions as an antioxidant agent to improve CACS as part of an integrated treatment [44,54]. | Reduces proinflammatory cytokines to improve oxidative stress and CACS symptoms, as part of a combination of antioxidants, ONS, and drugs [44,54]. | Weight; LBM; grip strength; REE; leptin, proinflammatory cytokines, antioxidant enzymes, and ROS levels; appetite; fatigue; physical activity level; performance status; QoL; prognostic score. |
| Vitamin B1 | Contributes to prevention of anorexia and cachexia along with Vitamin B6 and amino acids during chemotherapy [76]. | Useful in muscle trophism, along with Vitamin B6 and amino acids [76]. | Nutritional status, clinical status, QoL, adherence to chemotherapy. |
| Vitamin B6 | Oral replacement therapy corrects neutropenia that stems from Vitamin B6 deficiency [70]. Contributes to prevention of anorexia and cachexia along with Vitamin B1 and amino acids during chemotherapy [76]. | Oral replacement therapy corrects Vitamin B6 deficiency and its associated neutropenia [70]. Useful in muscle trophism, along with Vitamin B1 and amino acids [76]. | Nutritional status; vitamin B6 and neutrophil levels; clinical status; QoL, regression of cervical adenopathy; adherence to chemotherapy. |
| Vitamin B9 | Reduces adverse events from pemetrexed therapy [46,60,61,68]. | Reduces toxicity to pemetrexed (an antifolate) when used with Vitamin B12 [46,60,61,68]. Vitamin B9 dosing, however, needs to be optimal to prevent interference with pemetrexed effectiveness [68]. | Total plasma homocysteine levels, QoL, relative dose intensity, tumor response, survival, adverse events (including neutropenia grade and other toxicities). |
| Vitamin B12 | Oral vitamin B12 is an alternative to intramuscular vitamin B12 for purposes of reducing pemetrexed-associated adverse events, when used along with Vitamin B9 [60]. | Oral administration of vitamin B12 is capable of correcting vitamin B12 deficiency and is, thus, an alternative to intramuscular injection [60]. | Total plasma homocysteine levels, tumor response, survival, adverse events (including neutropenia grade and other toxicities). |
| Vitamin C | Functions as an antioxidant agent to improve CACS as part of an integrated treatment [44,54]. | Reduces proinflammatory cytokines to improve oxidative stress and CACS symptoms, as part of a combination of antioxidants, ONS, and drugs [44,54]. | Weight; LBM; grip strength; REE; leptin, proinflammatory cytokines, antioxidant enzymes and ROS levels; appetite; fatigue; performance status; physical activity; QoL; prognostic score. |
| Vitamin D | Improves survival in metastatic colorectal cancer [40]. Replacement therapy improves muscle strength and pain associated with prostate cancer bone metastasis [64]. 1α-OHD3 along with calcium supplementation prevents bone mass loss in men with prostate cancer treated with complete androgenic blockade [62]. Improves symptom burden in women with estrogen receptive–positive metastatic breast cancer [59]. | Exerts anti-cancer effects when converted to calcitriol in the body, by regulating cancer-related genes [40]. Inhibits growth of prostate cancer cells [64]. 1α-OH vitamin D3, along with calcium, prevents bone mass loss [62]. Supplementation improves vitamin D insufficiency to reduce muscle and joint pain that stem from estrogen blockade use and low serum 25-hydroxyvitamin D (25[OH]D) levels [59]. | Anthropometry, bone mineral density, muscle strength, grip strength, 25(OH)D levels, calcium phosphatase and alkaline phosphatase levels, prostate specific antigen levels, CRP levels, proinflammatory cytokines levels, symptom burden, pain, QoL, survival. |
| Vitamin E | Functions as an antioxidant agent to improve CACS as part of an integrated treatment [44,54]. Minimizes side effects of omega-3 supplementation [39]. | Reduces proinflammatory cytokines to improve oxidative stress and CACS symptoms, as part of a combination of antioxidants, ONS, and drugs [44,54]. Compensates for the oxidative effect of omega-3 [39]. | Weight; LBM; grip strength; REE; leptin, albumin, transferrin, proinflammatory cytokines, T-cell subsets, antioxidant enzymes, and ROS levels; appetite; fatigue; performance status; physical activity; QoL; prognostic score; survival. |
| Calcium | Prevents bone mass loss in men treated with complete androgenic blockade, along with 1α-OHD3 [62]. | Calcium, along with 1α-OH vitamin D3, prevents bone mass loss, which people with advanced prostate cancer receiving complete androgenic blockade are more susceptible to [62]. | Bone mineral density; muscle strength; 25(OH)D, calcium phosphatase, alkaline phosphatase, and prostate specific anti-gen levels; pain. |
| Iron | Improves sideropenic anemia when administered in the form of sucrosomial iron, as a supportive therapy alongside radiation therapy [79]. | As radiation therapy can lead to side-effects such as mucositis and dysphagia resulting in malnutrition and subsequent onset of sideropenic anemia, sucrosomial iron improves sideropenic anemia when given concomitantly with radiation therapy [79]. | Weight; hemoglobin, mean corpuscular, mean corpuscular hemoglobin, and total plasma homocysteine levels; mucositis; tumor response; toxicity. |
| Selenium | Improves axitinib therapy response when administered in the form of seleno-L-methionine [75]. | Seleno-L-methionine stabilizes tumor vasculature and reduces risks of angiogenesis, tumor metastasis and treatment resistance when given in combination with chemotherapeutic and vascular endothelial growth factor–targeted agents [75]. | Response, survival, adverse events; toxicity. |
| Carbocysteine | Functions as an antioxidant agent to improve cancer cachexia symptoms as part of an integrated treatment [42,44,54,74]. | Reduces proinflammatory cytokines to improve oxidative stress and CACS symptoms, as part of a combination of antioxidants, ONS, and drugs [44,54]. Important precursor of cell-reduced glutathione and counteracts oxidative stress [42]. | Weight; LBM; grip strength; REE; leptin, CRP, proinflammatory cytokines, ROS, and antioxidant enzyme levels; appetite; fatigue; performance status; physical activity level; QoL; prognostic score; adverse events. |
| Curcumin | Improves nutritional and immunometabolic alterations of cachexia and cancer-related anemia as part of a combined treatment also consisting of L-carnitine, lactoferrin and celecoxib [73]. Exerts antioxidant and anti-inflammatory effects in advanced cancer cachexia [77]. | Possesses anti-inflammatory and antioxidant effects to mitigate inflammation and oxidative stress in cachexia [73,77]. | LBM; serum iron, ferritin, hepcidin, erythropoietin, CRP, proinflammatory cytokines, ROS, antioxidant enzyme, and total blood antioxidant status levels; appetite; fatigue; anemia. |
| Lipoic acid | Functions as an antioxidant agent to improve cancer cachexia symptoms as part of an integrated treatment [42,44,54,74]. | Reduces proinflammatory cytokines to improve oxidative stress and CACS symptoms as part of a combination of antioxidants, ONS, and drugs [44,54]. Important precursor of cell-reduced glutathione and counteracts oxidative stress [42]. | Weight; LBM; grip strength; REE; leptin, CRP, proinflammatory cytokines, ROS, and antioxidant enzyme levels; appetite; fatigue; performance status; physical activity level; QoL; prognostic score; adverse events. |
| Lycopene | Concomitant administration with docetaxel is an effective treatment for prostate cancer [66]. | Possesses antioxidant properties and has chemo preventive effects in prostate cancer; inhibits antiapoptotic protein, and improves antitumor efficacy of docetaxel [66]. | Prostate specific antigen response, survival, adverse events. |
| Quercetin | Functions as an antioxidant agent to improve CACS as part of an integrated treatment [44,54]. | Reduces proinflammatory cytokines to improve oxidative stress and CACS symptoms when used in a combination of antioxidants, ONS, and drugs [44,54]. | Weight; LBM; grip strength, REE; leptin, proinflammatory cytokines, antioxidant enzymes, and ROS levels; appetite; fatigue; performance status; physical activity level; QoL; prognostic score. |
| Proteins and amino acids | |||
| Lactoferrin | Improves nutritional and immunometabolic alterations of cachexia and cancer-related anemia as part of a combined treatment with L-carnitine, curcumin and celecoxib [73]. An alternative to intravenous iron supplementation when combined with recombinant human erythropoietin, in the treatment of anemia in advanced cancer during chemotherapy [43]. | Key in host defense against infection and excessive inflammation [43]. As patients with cancer anemia may have low or normal serum iron levels, yet increased ferritin levels and rich bone marrow iron reserves, it is suggested that cancer anemia is associated with flaws in iron use rather than iron shortage [43]. Lactoferrin, which is involved in iron transport mechanisms, can thus treat this form of iron-related anemia [43,73]. | LBM; hematopoietic response; erythrocyte sedimentation rate; hemoglobin, iron, ferritin, hepcidin, erythropoietin, CRP, proinflammatory cytokine, ROS, and antioxidant enzyme levels; appetite; fatigue; anemia; adverse events. |
| Whey protein isolate | Improves nutritional status of malnourished advanced cancer patients receiving chemotherapy [38]. | Possesses immune-enhancing factors and contains cysteine (a limiting amino acid in the glutathione production), where glutathione protects cells from free radicals and carcinogens. Induces more muscle protein synthesis, being more rapidly digested than other protein sources [38]. | Weight, phase angle, fat-free mass index, grip strength, protein calorie intake, QoL, chemotherapy toxicity. |
| All essential amino acids | Counter wasting processes associated with cancer cachexia [72]. Prevents anorexia and cachexia in cancer during chemotherapy, along with vitamins B1 and B6 [76]. | Useful in muscle trophism, along with vitamins B1 and B6 [76]. | Weight, body composition, nutritional status, clinical status, muscle strength, exercise capacity, QoL, adherence to chemotherapy. |
| Arginine | Prevents cancer recurrence following surgical removal of malignant tumors, especially when administered perioperatively [36]. Improves postoperative recovery as part of an immunonutrition enteral formula in head and neck cancer [67]. Prevents LBM loss and reverses cancer cachexia, as part of a mixture with HMB and glutamine [35,45]. Delays cachexia onset in advanced lung cancer [57]. | Conditionally essential amino acid that acts as a substrate for nitric oxide synthesis (which is potentially toxic to cancer cells), improves immune function [36,45,67], modulates protein turnover [45], fights remnant cancer cells following surgical removal of malignant tumors [36], and improves wound healing [35,67]. Works in synergy with HMB to mitigate muscle loss, and with both HMB and glutamine to reduce muscle damage from ROS and proinflammatory cytokines [57]. | Weight; body composition; LBM; grip strength; energy and protein intake; liver function; renal function; total protein, prealbumin, albumin, globulin, retinol-binding protein, total cholesterol, and triglycerides levels; fatigue; QoL; need for parenteral nutrition during hospital admission; duration of tube feeding; length of hospital stay; fistula incidence after surgery; readmission rates; treatment success; cancer recurrence; metastases or second primary tumors occurrence; survival. |
| Branched chain amino acids (BCAA) | Improves physical function in elderly patients with advanced lung or pancreatic cancer as part of a multimodal intervention with coQ10 and L-carnitine [56]. | Not specified | Weight, BMI, LBM, nutritional status, food intake, physical function/muscle strength, physical activity levels. |
| Carnitine | Improves cancer cachexia in pancreatic cancer [41], and improves fatigue and ROS levels in advanced cancer [53]. As part of a combined treatment, improves cancer cachexia symptoms [42,44,73,74], cancer-related anemia [73], and physical function in elderly patients with advanced lung or pancreatic cancer [56]. | Modulates inflammatory response mechanisms associated with cancer cachexia [41]. Deficiency contributes to cancer cachexia and tumor-associated fatigue [41]. Key in β-oxidation and energy and amino acid metabolism [42,44,53,73]. | Weight; BMI; body composition; LBM; skeletal muscle analysis; grip strength; food intake; nutritional status; nutrition impact symptoms; REE; L-carnitine, iron, ferritin, hepcidin, erythropoietin, hemoglobin; CRP, proinflammatory cytokines, ROS, and antioxidant enzyme levels; appetite; fatigue; performance status; physical function; physical activity level; QoL; global health status; prognostic score; survival; anemia; adverse events/toxicity. |
| Glutamine | As part of a mixture with arginine and HMB, prevents LBM loss and reverses cancer cachexia [35,45] or delays cachexia onset in advanced lung cancer [57]. | Regulates muscle protein synthesis or turnover [35,57] and exerts immune stimulatory effects [45]. Works with both HMB and arginine to reduce muscle damage from ROS and pro-inflammatory cytokines [57]. | Weight; body composition; LBM; grip strength; calorie and protein intake; liver function; renal function; total protein, albumin, globulin, prealbumin, triglyceries and total cholesterol levels; fatigue; QoL; treatment success. |
| HMB | As part of a mixture with arginine and glutamine, prevents LBM loss and reverses cancer cachexia [35,45] or delays cachexia onset in advanced lung cancer [57]. | Modulates protein turnover [45,57] and works in synergy with arginine to mitigate muscle loss [57]. Improves nitrogen balance, inhibits proteolysis-inducing factor [35], and works with arginine and glutamine to reduce muscle damage from ROS and pro-inflammatory cytokines [57]. | Weight; body composition; LBM; grip strength; calorie and protein intake; liver function; renal function; total protein, albumin, globulin and prealbumin levels; triglyceries and total cholesterol levels; fatigue; QoL; treatment success. |
| Fatty Acids | |||
| EPA ± docosahexaenoic acid (DHA) | Modifies membrane composition of neutrophils to reduce inflammation and wasting in advanced cancer [47], improves T-cell subsets and cytokine production when used along with vitamin E [39], and improves SIMS symptoms [37]. Omega-3– or EPA–containing ONS improves nutritional, clinical and inflammatory parameters, and health-related QoL in advanced lung cancer [48]; improves prognosis in advanced gastrointestinal cancer [49] and hypopharyngeal cancer among patients on induction chemotherapy [71]; and improves cachexia during gemcitabine therapy [51]. Improves postoperative recovery in head and neck cancer, as part of an immunonutrition formula [67]. Omega-3–containing ONS as part of a multimodal intervention improves clinical outcomes in cancer [69] and attenuates cachexia in incurable lung or pancreatic cancer [50] or advanced cancer with CACS [44,54]. Marine phospholipids (with >50% phospholipid-bound fatty acids as EPA and DHA) aid in cancer cachexia management [63]. Omega-3 fatty acids (EPA and DHA) in krill oil improve lipid profile disorder and inflammatory processes associated with cachexia [78]. A more purified EPA + DHA supplement is more reliable than fish oil supplements [69]. EPA is a biologically active component of fish oil responsible for anticachectic activity [65]. | Immunomodulatory [49,63,65,71], with EPA in particular having anti-inflammatory, anticachectic, antitumoral, anti-genotoxic, and antioxidant properties [48,49,63,65,71]. EPA partially substitutes arachidonic acid, thereby reducing production of arachidonic acid–derived mediators to exert an anti-inflammatory effect [37,63]. Omega-3 augments defense against tumor cells and tumor cell susceptibility by altering cell membrane composition and directly reducing tumor cell proliferation [39]. By inhibiting proinflammatory cytokines production [48,49,63,65,71], omega-3 improves cancer cachexia [44,51,63,65] and reduces proinflammatory mediators to lower infections [67]. As fatty acids bound to phospholipids-bound are more readily incorporated into plasma phospholipids compared to those bound to triacylglycerols, marine phospholipids can be more effective in a lower dose than fish oil in cancer patients [63]. A purified EPA/DHA supplement offers better outcomes due to possible interactions between platinum-based chemotherapy and fatty acids present in fish oils [69]. | Weight; height; BMI; fat mass; subcutaneous and visceral adipose tissue; LBM; muscle mass; skeletal muscle; phase angle; intracellular water; extracellular water; total body water; grip strength; REE; nutritional status; nutritional, caloric intake and fat intake; complete blood cell count; white blood cell count; leukocytes, thrombocytes, leptin, retinol-binding protein, albumin, pre-albumin, transferrin, total protein, hemoglobin, glucose, sodium, potassium, ionic calcium, creatinine, urea, total and direct bilirubin, aspartate amino transaminase, alanine amino transaminase, lactate dehydrogenase, gamma-glutamyl transferase; gamma glutamil transpeptidase, alkaline phosphatase, creatinine, CRP, ROS, antioxidant enzyme, cytokine, T-cell subsets, carcino-embryonic antigen, carbohydrate antigen 19.9/125, lyso-phosphatidylcholine. total cholesterol, high-density lipoprotein, low-density lipoprotein, very low–density lipoprotein, and triglycerides levels; plasma phospholipid, red blood cell, mononuclear lymphocytes, and neutrophil fatty acid composition; appetite; nausea; vomiting; diarrhea; energy level; physical and overall well-being; fatigue; physical activity level, physical function; performance status; QoL; health-related QoL; disease progression; prognostic score; survival; toxicity; adverse events; safety; therapy response; chemotherapy dose reductions; need for parenteral nutrition during admission; duration of tube feeding; fistula incidence after surgery; mortality; hospital length of stay; hospitalizations; recurrence; readmissions; adherence to intervention. |
| Fiber | |||
| Fiber | Not reported | Not reported | Weight, muscle mass, fat-free mass, fat mass; hemoglobin, glucose, CRP, albumin, AAT, GGT, carcinoembryonic antigen, and carbohydrate antigen 19.9/125 levels. |
| Others | |||
| β-hydroxybutyrate (BHB) | Intake is safe when used while receiving immunotherapy for cancer [81]. | Not reported | Weight; sarcopenia; albuminemia; prealbuminemia; CRP level; QoL; response rate; survival; safety. |
| CoQ10 | Improves physical function in elderly patients with advanced lung or pancreatic cancer as part of a multimodal intervention [56]. | Not reported | Weight, BMI, skeletal muscle analysis, grip strength, food intake, nutritional status, nutrition impact symptoms, physical function, physical activity levels. |
| Muscadine grape extract (MGE) | Improves cancer outcomes by reducing symptom burden and is tolerated and safe for use in patients with metastatic solid tumors who have failed standard therapies [52]. | Muscadine grape contains a high concentration of anthocyanin, ellagic acid, gallic acid, and flavonols and has antioxidant properties. It inhibits tumor cell growth and induces apoptosis, while also reducing systemic inflammation [52]. | CRP, hepatocyte growth factor, IL-6, IL-6 receptor, IL-8, platelet-derived growth factor, TNF-α, vascular endothelial growth factor and phenolic levels; fatigue, QoL, response rate; safety; survival; adherence to intervention. |
| Dietary nucleotides | Improves postoperative recovery in head and neck cancer as part of an immunonutrition enteral formula [67]. | Modulates inflammatory and immune response [67]. | Weight, energy and protein intake, albumin levels, retinol binding protein levels, duration of tube feeding, need for parenteral nutrition during admission, fistula incidence after surgery, length of hospital stay, readmission rates, mortality. |
| Royal jelly | Protects from toxicities induced by tyrosine kinase inhibitors in renal cancer [34]. | Possesses anti-inflammatory and antioxidative effects, influences immune system, and protects from adverse events such as inflammation, oxidative stress and immune system dysfunction induced by anticancer agents [34]. | Tumor necrosis and transforming growth factor levels, adverse events due to tyrosine kinase inhibitors, sustained period of initial tyrosine kinase inhibitors. |
| Outcome Measures | Tools Used |
|---|---|
| Nutritional intake | Two-day or three-day food diary, 24-h diet recall; 10-point verbal scale assessment of nutritional intake [38,50,56,58] |
| Nutritional status | MNA; PG-SGA [50,56] |
| Body composition (including fat-free mass, LBM, muscle mass) | Midarm muscle circumference measurement; skin-fold measurement techniques; body plethysmography; air displacement plethysmograph; BIA; BIVA; CT; DEXA [35,37,38,41,42,44,45,48,49,50,53,54,55,56,57,58,63,65,72] |
| Phase angle | BIVA; BIA [38,48] |
| Grip strength | Handgrip Dynamometer [38,42,44,50,53,54,56,57] |
| Muscle strength/physical performance/exercise capacity | Five times sit-to-stand or chair rise test; 5-m gait speed; 10-m gait speed; stair-climbing power; 6-min walk distance [50,56,64,72] |
| Resting energy expenditure | Indirect calorimetry [42,44,54] |
| Fatigue | MFSI-SF; Brief Fatigue Inventory questionnaire; Schwarz Fatigue Index; numerical rating scale 0–10; Fatigue Severity Scale; PROMIS-fatigue [35,37,41,42,44,50,52,53,54] |
| Appetite | VAS; numerical rating scale 0–10 [37,42,44,54,63] |
| Nausea | Numerical rating scale 0–10 [37] |
| Performance status | ECOG PS scale; Karnofsky performance status/score [37,39,44,51,54] |
| Physical activity level | Electronic wearable device (armband/pedometer/accelerometer/logger) [44,50,56] |
| QoL | EORTC QLQ-C30; EORTC-QLQ-C30 questionnaire with pancreatic cancer–specific module PAN 26; Italian version of EORTC QLQ-C30; QLQ-LC13, EQ-5D; QoL-ACD; FAACT; FACT-L; FACT-G; Functional Assessment Health Survey; Functional Assessment of Cancer Therapy–General as well as –Bone Pain, –Breast and –Endocrine Symptoms subscales; Spitzer Quality of Life Index; Short Form-36 Health Survey; Quality of Life–Oxidative Stress Questionnaire; disease and treatment assessment form [35,38,41,42,44,45,46,48,52,54,57,58,59,63,80,81] |
| Symptom burden | Brief Pain Inventory; Piper Fatigue Scale; Hospital Anxiety and Depression Scale; and Pittsburg Sleep Quality Index [59] |
| Pain | Modified McGill–Dartmouth Pain Questionnaire [64] |
| Prognosis | GPS [44,74] |
| Regression of cervical adenopathy | Clinical examination; positron emission tomography (PET); CT [70] |
| Treatment response | CT, magnetic imaging resonance imaging, or X-ray [52,55] |
| Tumor response | RECIST [46,51,60,61,68,81] |
| Toxicity or adverse events | National Cancer Institute Common Toxicity Criteria for Adverse Events; National Cancer Institute Common Toxicology Criteria; National Cancer Institute Common Terminology Criteria for Adverse Events version 3.0 or 4.0; National Cancer Institute’s Common Toxicity Criteria version 2.0 [38,42,43,46,48,50,51,53,58,60,61,66,68] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Johal, J.; Han, C.Y.; Joseph, R.; Munn, Z.; Agbejule, O.A.; Crawford-Williams, F.; Wallen, M.P.; Chan, R.J.; Hart, N.H. Dietary Supplements in People with Metastatic Cancer Who Are Experiencing Malnutrition, Cachexia, Sarcopenia, and Frailty: A Scoping Review. Nutrients 2022, 14, 2642. https://doi.org/10.3390/nu14132642
Johal J, Han CY, Joseph R, Munn Z, Agbejule OA, Crawford-Williams F, Wallen MP, Chan RJ, Hart NH. Dietary Supplements in People with Metastatic Cancer Who Are Experiencing Malnutrition, Cachexia, Sarcopenia, and Frailty: A Scoping Review. Nutrients. 2022; 14(13):2642. https://doi.org/10.3390/nu14132642
Chicago/Turabian StyleJohal, Jolyn, Chad Yixian Han, Ria Joseph, Zachary Munn, Oluwaseyifunmi Andi Agbejule, Fiona Crawford-Williams, Matthew P. Wallen, Raymond J. Chan, and Nicolas H. Hart. 2022. "Dietary Supplements in People with Metastatic Cancer Who Are Experiencing Malnutrition, Cachexia, Sarcopenia, and Frailty: A Scoping Review" Nutrients 14, no. 13: 2642. https://doi.org/10.3390/nu14132642
APA StyleJohal, J., Han, C. Y., Joseph, R., Munn, Z., Agbejule, O. A., Crawford-Williams, F., Wallen, M. P., Chan, R. J., & Hart, N. H. (2022). Dietary Supplements in People with Metastatic Cancer Who Are Experiencing Malnutrition, Cachexia, Sarcopenia, and Frailty: A Scoping Review. Nutrients, 14(13), 2642. https://doi.org/10.3390/nu14132642