
Role of Diet and Nutrients in SARS-CoV-2 Infection: Incidence on Oxidative Stress, Inflammatory Status and Viral Production

 ,
,  ,
,  ,
,  , , , ,
, , , ,  , ,
, ,  add
Show full author list
add
Show full author list
Abstract
1. Introduction
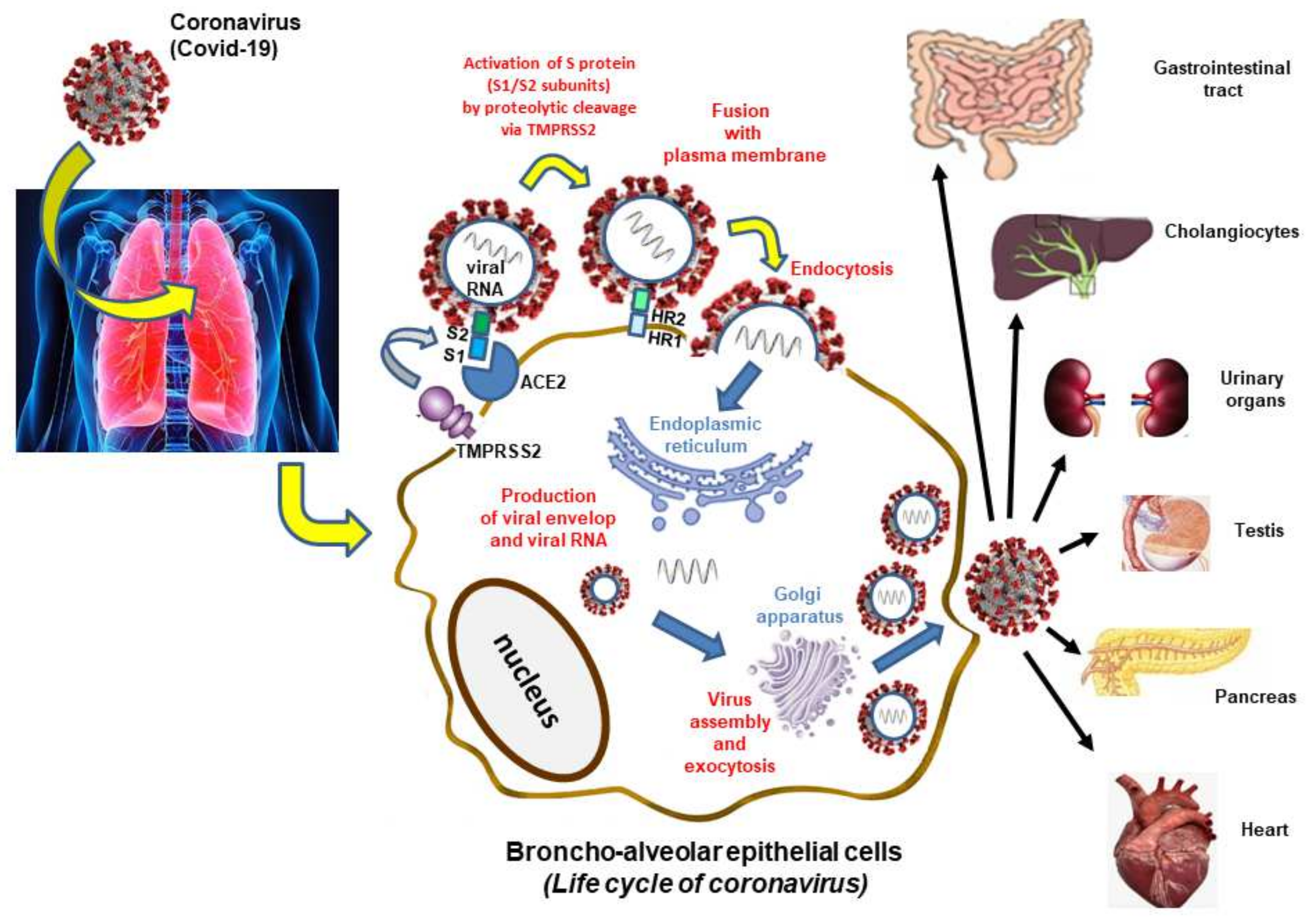
2. Mechanism of SARS-CoV-2 Infection
3. Medicinal Plants and Their Metabolites Used in Case of COVID-19
3.1. Medicinal Plants and Their Extracts
3.2. Major Plant Metabolites
3.2.1. Polyphenols
3.2.2. Terpenoids
Carotenoids
Phytosterols
4. Major Food Groups Efficient in COVID-19 Pathogenesis
4.1. Macronutrients
4.2. Micronutrients (Vitamins and Minerals)
4.2.1. Water-Soluble Vitamins
4.2.2. Fat-Soluble Vitamins: Vitamin D and Vitamin E
4.3. Trace Elements
4.3.1. Magnesium
4.3.2. Iron
4.3.3. Zinc
4.3.4. Selenium
4.4. Polyunsaturated Fatty Acids
5. Perspectives and Emerging Technologies: Plant-Based SARS-CoV-2 Vaccines
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Alam, S.; Bhuiyan, F.R.; Emon, T.H.; Hasan, M. Prospects of nutritional interventions in the care of COVID-19 patients. Heliyon 2021, 7, e06285. [Google Scholar] [CrossRef] [PubMed]
- De Alencar, E.S.; dos Santos Muniz, L.S.; Holanda, J.L.G.; Oliveira, B.D.D.; de Carvalho, M.C.F.; Leitão, A.M.M.; de Alencar Cavalcante, M.I.; de Oliveira, R.C.P.; da Silva, C.A.B.B.; Ferreira Carioca, A.A. Enteral nutritional support for patients hospitalized with COVID-19: Results from the first wave in a public hospital. Nutrition 2022, 94, 111512. [Google Scholar] [CrossRef] [PubMed]
- Thomas, S.; Alexander, C.; Casssady, B.A. Nutrition risk prevalence and nutrition care recommendations for hospitalized and critically-ill patients with COVID-19. Clin. Nutr. ESPEN 2021, 44, 38–49. [Google Scholar] [CrossRef] [PubMed]
- Adhikari, B.; Marasini, B.P.; Rayamajhee, B.; Bhattarai, B.R.; Lamichhane, G.; Khadayat, K.; Adhikari, A.; Khanal, S.; Parajuli, N. Potential roles of medicinal plants for the treatment of viral diseases focusing on COVID-19: A review. Phytother. Res. 2021, 35, 1298–1312. [Google Scholar] [CrossRef] [PubMed]
- Marcello, A.; Civra, A.; Bonotto, R.M.; Alves, L.N.; Rajasekharan, S.; Giacobone, C.; Caccia, C.; Cavalli, R.; Adami, M.; Brambilla, P.; et al. The cholesterol metabolite 27-hydroxycholesterol inhibits SARS-CoV-2 and is markedly decreased in COVID-19 patients. Redox. Biol. 2020, 36, 101682. [Google Scholar] [CrossRef] [PubMed]
- Ghzaiel, I.; Sassi, K.; Zarrouk, A.; Nury, T.; Ksila, M.; Leoni, V.; Bouhaouala-Zahar, B.; Hammami, S.; Hammami, M.; Mackrill, J.J.; et al. 7-Ketocholesterol: Effects on viral infections and hypothetical contribution in COVID-19. J. Steroid Biochem. Mol. Biol. 2021, 212, 105939. [Google Scholar] [CrossRef]
- Gouda, A.S.; Adbelruhman, F.G.; Alenezi, H.S.; Mégarbane, B. Theoretical benefits of yogurt-derived bioactive peptides and probiotics in COVID-19 patients–A narrative review and hypotheses. Saudi J. Biol. Sci. 2021, 28, 5897–5905. [Google Scholar] [CrossRef]
- Schmelter, F.; Föh, B.; Mallagaray, A.; Rahmöller, J.; Ehlers, M.; Lehrian, S.; von Kopylow, V.; Künsting, I.; Lixenfeld, A.S.; Martin, E.; et al. Metabolic and lipidomic markers differentiate COVID-19 from non-hospitalised and other intensive care patients. Front. Mol. Biosci. 2021, 1091, 737039. [Google Scholar] [CrossRef]
- Motti, M.L.; Tafuri, D.; Donini, L.; Masucci, M.T.; De Falco, V.; Mazzeo, F. The Role of Nutrients in Prevention, Treatment and Post-Coronavirus Disease-2019 (COVID-19). Nutrients 2022, 14, 1000. [Google Scholar] [CrossRef]
- Atanasov, A.G.; Zotchev, S.B.; Dirsch, V.M.; Supuran, C.T. Natural products in drug discovery: Advances and opportunities. Nat. Rev. Drug Discov. 2021, 20, 200–216. [Google Scholar] [CrossRef]
- Ahmad, S.; Zahiruddin, S.; Parveen, B.; Basist, P.; Parveen, A.; Parveen, R.; Ahmad, M. Indian medicinal plants and formulations and their potential against COVID-19–preclinical and clinical research. Front. Pharmacol. 2021, 2470, 578970. [Google Scholar] [CrossRef] [PubMed]
- Bhuiyan, F.R.; Howlader, S.; Raihan, T.; Hasan, M. Plants metabolites: Possibility of natural therapeutics against the COVID-19 pandemic. Front. Med. 2020, 7, 444. [Google Scholar] [CrossRef] [PubMed]
- Cock, I.E. An Opinion: Herbal Medicines may Provide a Means of Controlling the COVID-19 Pandemic. Pharmacogn. Commun. 2020, 10, 140–142. [Google Scholar] [CrossRef]
- Brahmi, F.; Vejux, A.; Sghaier, R.; Zarrouk, A.; Nury, T.; Meddeb, W.; Rezig, L.; Namsi, A.; Sassi, K.; Yammine, A.; et al. Prevention of 7-ketocholesterol-induced side effects by natural compounds. Crit. Rev. Food Sci. Nutr. 2019, 59, 3179–3198. [Google Scholar] [CrossRef]
- Debbabi, M.; Nury, T.; Zarrouk, A.; Mekahli, N.; Bezine, M.; Sghaier, R.; Grégoire, S.; Martine, L.; Durand, P.; Camus, E.; et al. Protective effects of α-tocopherol, γ-tocopherol and oleic acid, three compounds of olive oils, and no effect of trolox, on 7-Ketocholesterol-Induced Mitochondrial and Peroxisomal Dysfunction in Microglial BV-2 Cells. Int. J. Mol. Sci. 2016, 17, 1973. [Google Scholar] [CrossRef]
- Yammine, A.; Zarrouk, A.; Nury, T.; Vejux, A.; Latruffe, N.; Vervandier-Fasseur, D.; Samadi, M.; Mackrill, J.J.; Greige-Gerges, H.; Auezova, L.; et al. Prevention by dietary polyphenols (resveratrol, quercetin, apigenin) against 7-Ketocholesterol-Induced oxiapoptophagy in neuronal N2a cells: Potential interest for the treatment of neurodegenerative and age-related diseases. Cells 2020, 9, 2346. [Google Scholar] [CrossRef]
- Kurtz, A.; Grant, K.; Marano, R.; Arrieta, A.; Feaster, W.; Steele, C.; Ehwerhemuepha, L. Long-term effects of malnutrition on severity of COVID-19. Sci. Rep. 2021, 11, 14974. [Google Scholar] [CrossRef]
- Huang, C.; Huang, L.; Wang, Y.; Li, X.; Ren, L.; Gu, X.; Kang, L.; Guo, L.; Liu, M.; Zhou, X.; et al. 6-month consequences of COVID-19 in patients discharged from hospital: A cohort study. Lancet 2021, 397, 220–232. [Google Scholar] [CrossRef]
- Theoharides, T.C. Could SARS-CoV-2 Spike Protein Be Responsible for Long-COVID Syndrome? Mol. Neurobiol. 2022, 59, 1850–1861. [Google Scholar] [CrossRef]
- Scarmeas, N.; Anastasiou, C.A.; Yannakoulia, M. Nutrition and prevention of cognitive impairment. Lancet Neurol. 2018, 17, 1006–1015. [Google Scholar] [CrossRef]
- Sharanya, C.; Sabu, A.; Haridas, M. Potent phytochemicals against COVID-19 infection from phyto-materials used as antivirals in complementary medicines: A review. Future J. Pharm. Sci. 2021, 7, 113. [Google Scholar] [CrossRef] [PubMed]
- Scudellari, M. How the coronavirus infects cells-and why Delta is so dangerous. Nature 2021, 595, 640–644. [Google Scholar] [CrossRef] [PubMed]
- Trougakos, I.P.; Stamatelopoulos, K.; Terpos, E.; Tsitsilonis, O.E.; Aivalioti, E.; Paraskevis, D.; Kastritis, E.; Pavlakis, G.N.; Dimopoulos, M.A. Insights to SARS-CoV-2 life cycle, pathophysiology, and rationalized treatments that target COVID-19 clinical complications. J. Biomed. Sci. 2021, 28, 9. [Google Scholar] [CrossRef] [PubMed]
- Jackson, C.B.; Farzan, M.; Chen, B.; Choe, H. Mechanisms of SARS-CoV-2 entry into cells. Nat. Rev. Mol. Cell Biol. 2022, 23, 3–20. [Google Scholar] [CrossRef]
- Li, S.; Li, S.; Disoma, C.; Zheng, R.; Zhou, M.; Razzaq, A.; Liu, P.; Zhou, Y.; Dong, Z.; Du, A.; et al. SARS-CoV-2: Mechanism of infection and emerging technologies for future prospects. Rev. Med. Virol. 2021, 31, e2168. [Google Scholar] [CrossRef]
- Soldevila, B.; Puig-Domingo, M.; Marazuela, M. Basic mechanisms of SARS-CoV-2 infection. What endocrine systems could be implicated? Rev. Endocr. Metab. Disord. 2021, 23, 137–150. [Google Scholar] [CrossRef]
- Cai, G.; Cui, X.; Zhu, X.; Zhou, J. A hint on the COVID-19 risk: Population disparities in gene expression of three receptors of SARS-CoV. Preprints 2020, 2020020408. [Google Scholar] [CrossRef]
- Zhu, Y.; Xie, D.-Y. Docking characterization and in vitro inhibitory activity of flavan-3-ols and dimeric proanthocyanidins against the main protease activity of SARS-Cov-2. Front. Plant Sci. 2020, 11, 601316. [Google Scholar] [CrossRef]
- De Oliveira, O.V.; Cristina Andreazza Costa, M.; Marques da Costa, R.; Giordano Viegas, R.; Paluch, A.S.; Miguel Castro Ferreira, M. Traditional herbal compounds as candidates to inhibit the SARS-CoV-2 main protease: An in silico study. J. Biomol. Struct. Dyn. 2021, 1–14. [Google Scholar] [CrossRef]
- Acedhars Unilag COVID-19 Response Team; Akindele, A.J.; Agunbiade, F.O.; Sofidiya, M.O.; Awodele, O.; Sowemimo, A.; Ade-Ademilua, O.; Akinleye, M.O.; Ishola, I.O.; Orabueze, I.; et al. COVID-19 Pandemic: A case for phytomedicines. Nat. Prod. Commun. 2020, 15, 5086. [Google Scholar] [CrossRef]
- Belhaj, S.; Zidane, L. Medicinal plants used to boost immunity and decrease the intensity of infection caused by SARS-COV-2 in Morocco. Ethnobot. Res. Appl. 2021, 21, 1–17. Available online: https://ethnobotanyjournal.org/era/index.php/era/article/view/2495 (accessed on 31 January 2022).
- Jamiu, A.T.; Aruwa, C.E.; Abdulakeem, I.A.; Ajao, A.A.; Sabiu, S. Phytotherapeutic Evidence Against Coronaviruses and Prospects for COVID-19. Pharmacogn. J. 2020, 12, 1252–1267. [Google Scholar] [CrossRef]
- Ren, J.-l.; Zhang, A.-H.; Wang, X.-J. Traditional Chinese medicine for COVID-19 treatment. Pharmacol. Res. 2020, 155, 104743. [Google Scholar] [CrossRef] [PubMed]
- Fongnzossie Fedoung, E.; Biwole, A.B.; Nyangono Biyegue, C.F.; Ngansop Tounkam, M.; Akono Ntonga, P.; Nguiamba, V.P.; Essono, D.M.; Forbi Funwi, P.; Tonga, C.; Nguenang, G.M.; et al. A review of Cameroonian medicinal plants with potentials for the management of the COVID-19 pandemic. Adv. Tradit. Med. 2021, 1–26. [Google Scholar] [CrossRef]
- Lin, L.-T.; Hsu, W.-C.; Lin, C.-C. Antiviral natural products and herbal medicines. J. Tradit. Complement. Med. 2014, 4, 24–35. [Google Scholar] [CrossRef] [PubMed]
- Weng, J.-R.; Lin, C.-S.; Lai, H.-C.; Lin, Y.-P.; Wang, C.-Y.; Tsai, Y.-C.; Wu, K.-C.; Huang, S.-H.; Lin, C.-W. Antiviral activity of Sambucus Formosana Nakai ethanol extract and related phenolic acid constituents against human coronavirus NL63. Virus Res. 2019, 273, 197767. [Google Scholar] [CrossRef]
- Tuiskunen Bäck, A.; Lundkvist, Å. Dengue viruses–an overview. Infect. Ecol. Epidemiol. 2013, 3, 19839. [Google Scholar] [CrossRef]
- Pu, W.-L.; Zhang, M.-Y.; Bai, R.-Y.; Sun, L.-K.; Li, W.-H.; Yu, Y.-L.; Zhang, Y.; Song, L.; Wang, Z.-X.; Peng, Y.-F.; et al. Anti-inflammatory effects of Rhodiola rosea L.: A review. Biomed. Pharmacother. 2020, 121, 109552. [Google Scholar] [CrossRef]
- Liu, H.; Lin, S.; Ao, X.; Gong, X.; Liu, C.; Xu, D.; Huang, Y.; Liu, Z.; Zhao, B.; Liu, X.; et al. Meta-analysis of transcriptome datasets: An alternative method to study IL-6 regulation in coronavirus disease 2019. Comput. Struct. Biotechnol. J. 2021, 19, 767–776. [Google Scholar] [CrossRef]
- Jin, Y.-H.; Cai, L.; Cheng, Z.-S.; Cheng, H.; Deng, T.; Fan, Y.-P.; Fang, C.; Huang, D.; Huang, L.-Q.; Huang, Q.; et al. A rapid advice guideline for the diagnosis and treatment of 2019 novel coronavirus (2019-nCoV) infected pneumonia (standard version). Mil. Med. Res. 2020, 7, 4. [Google Scholar] [CrossRef]
- Luo, H.; Tang, Q.; Shang, Y.; Liang, S.; Yang, M.; Robinson, N.; Liu, J.-P. Can Chinese medicine be used for prevention of corona virus disease 2019 (COVID-19)? A review of historical classics, research evidence and current prevention programs. Chin. J. Integr. Med. 2020, 26, 243–250. [Google Scholar] [CrossRef]
- Weng, J.-K. Plant solutions for the COVID-19 pandemic and beyond: Historical reflections and future perspectives. Mol. Plant 2020, 13, 803–807. [Google Scholar] [CrossRef]
- Gangal, N.; Nagle, V.; Pawar, Y.; Dasgupta, S. Reconsidering traditional medicinal plants to combat COVID-19. AIJR Prepr. 2020, 34, 1–6. [Google Scholar]
- Balkrishna, A.; Pokhrel, S.; Singh, J.; Varshney, A. Withanone from Withania somnifera may inhibit novel coronavirus (COVID-19) entry by disrupting interactions between viral S-protein receptor binding domain and host ACE2 receptor. Drug Des. Devel Ther. 2021, 15, 1111–1133. [Google Scholar] [CrossRef] [PubMed]
- Mohan, S.; Elhassan Taha, M.M.; Makeen, H.A.; Alhazmi, H.A.; Al Bratty, M.; Sultana, S.; Ahsan, W.; Najmi, A.; Khalid, A. Bioactive natural antivirals: An updated review of the available plants and isolated molecules. Molecules 2020, 25, 4878. [Google Scholar] [CrossRef] [PubMed]
- Vroh, B.T.A. Diversity of Plants Used in Traditional Medicine against the Main Symptoms of COVID-19 in Sub-Saharan Africa: Review of the Literature. Ethnobot. Res. Appl. 2020, 20, 1–14. Available online: https://ethnobotanyjournal.org/index.php/era/article/view/2161 (accessed on 30 December 2021).
- Mirzaie, A.; Halaji, M.; Dehkordi, F.S.; Ranjbar, R.; Noorbazargan, H. A narrative literature review on traditional medicine options for treatment of corona virus disease 2019 (COVID-19). Complement. Ther. Clin. Pract. 2020, 40, 101214. [Google Scholar] [CrossRef]
- Babich, O.; Sukhikh, S.; Prosekov, A.; Asyakina, L.; Ivanova, S. Medicinal plants to strengthen immunity during a pandemic. Pharmaceuticals 2020, 13, 313. [Google Scholar] [CrossRef]
- Flouchi, R.; Fikeri-Benbrahim, K. Prevention of COVID 19 by aromatic and medicinal plants: A systematic review. Int. J. Pharm. Sci. Res. 2020, 12, 1106–1111. [Google Scholar]
- Bouchentouf, S.; Missoum, N. Identification of Compounds from Nigella Sativa as New Potential Inhibitors of 2019 Novel Coronasvirus (COVID-19): Molecular Docking Study. ChemRxiv 2020. preprint. [Google Scholar] [CrossRef]
- Latruffe, N. Mediterranean Diet and Wine and Health; EUD: Dijon, France, 2017; 204p. (In French) [Google Scholar]
- Ghiringhelli, F.; Rebe, C.; Hichami, A.; Delmas, D. Immunomodulation and anti-inflammatory roles of polyphenols as anticancer agents. Anticancer Agents Med. Chem. 2012, 12, 852–873. [Google Scholar] [CrossRef]
- De Angelis, M.; Della-Morte, D.; Buttinelli, G.; Di Martino, A.; Pacifici, F.; Checconi, P.; Ambrosio, L.; Stefanelli, P.; Palamara, A.T.; Garaci, E.; et al. Protective Role of Combined Polyphenols and Micronutrients against Influenza A Virus and SARS-CoV-2 Infection In Vitro. Biomedicines 2021, 9, 1721. [Google Scholar] [CrossRef]
- Liu, Z.; Xiao, X.; Wei, X.; Li, J.; Yang, J.; Tan, H.; Zhu, J.; Wu, J. Composition and divergence of coronavirus spike proteins and host ACE2 receptors predict potential intermediate hosts of SARS-CoV-2. J. Med. Virol. 2020, 92, 595–601. [Google Scholar] [CrossRef]
- Pincemail, J.; Cavalier, E.; Charlier, C.; Cheramy-Bien, J.-P.; Brevers, E.; Courtois, A.; Fadeur, M.; Meziane, S.; Le Goff, C.; Misset, B.; et al. Oxidative stress status in COVID-19 patients hospitalized in intensive care unit for severe pneumonia. A pilot study. Antioxidants 2021, 10, 257. [Google Scholar] [CrossRef] [PubMed]
- Trujillo-Mayol, I.; Guerra-Valle, M.; Casas-Forero, N.; Sobral, M.M.C.; Viegas, O.; Alarcón-Enos, J.; Mplvo Ferreira, I.; Pinho, O. Western dietary pattern antioxidant intakes and oxidative stress: Importance during the SARS-CoV-2/COVID-19 pandemic. Adv. Nutr. 2021, 12, 670–681. [Google Scholar] [CrossRef] [PubMed]
- Bahun, M.; Jukić, M.; Oblak, D.; Kranjc, L.; Bajc, G.; Butala, M.; Bozovičar, K.; Bratkovič, T.; Podlipnik, Č.; Poklar Ulrih, N. Inhibition of the SARS-CoV-2 3CLpro main protease by plant polyphenols. Food Chem. 2022, 373, 131594. [Google Scholar] [CrossRef]
- Latruffe, N.; Rifler, J.-P. Bioactive polyphenols from grapes and wine emphasized with resveratrol. Curr. Pharm. Des. 2013, 19, 6053–6063. [Google Scholar] [CrossRef] [PubMed]
- Silva, P.; Sureda, A.; Tur, J.A.; Andreoletti, P.; Cherkaoui-Malki, M.; Latruffe, N. How efficient is resveratrol as an antioxidant of the Mediterranean diet, towards alterations during the aging process? Free Radic. Res. 2019, 53 (Suppl. S1), 1101–1112. [Google Scholar] [CrossRef] [PubMed]
- Liao, M.-T.; Wu, C.-C.; Wu, S.-F.V.; Lee, M.-C.; Hu, W.-C.; Tsai, K.-W.; Yang, C.H.; Lu, C.L.; Chiu, S.K.; Lu, K.C. Resveratrol as an adjunctive therapy for excessive oxidative stress in aging covid-19 patients. Antioxidants 2021, 10, 1440. [Google Scholar] [CrossRef]
- Pasquereau, S.; Nehme, Z.; Haidar Ahmad, S.; Daouad, F.; Wallet, J.V.A.C.; Schwartz, C.; Rohr, O.; Morot-Bizot, S.; Herbein, G. Resveratrol inhibits HCoV-229E and SARS-CoV-2 coronavirus replication in vitro. Viruses 2021, 13, 354. [Google Scholar] [CrossRef]
- Tietjen, I.; Cassel, J.; Register, E.T.; Zhou, X.Y.; Messick, T.E.; Keeney, F.; Lu, L.D.; Beattie, K.D.; Rali, T.; Tebas, P.; et al. The Natural Stilbenoid (–)-Hopeaphenol Inhibits Cellular Entry of SARS-CoV-2 USA-WA1/2020, B. 1.1. 7, and B. 1.351 Variants. Antimicrob. Agents Chemother. 2021, 65, e00772-21. [Google Scholar] [CrossRef]
- Xu, H.; Li, J.; Song, S.; Xiao, Z.; Chen, X.; Huang, B.; Sun, M.; Su, G.; Zhou, D.; Wang, G.; et al. Effective inhibition of coronavirus replication by Polygonum cuspidatum. Front. Biosci. 2021, 26, 789–798. [Google Scholar] [CrossRef]
- Ter Ellen, B.M.; Dinesh Kumar, N.; Bouma, E.M.; Troost, B.; van de Pol, D.P.; Van der Ende-Metselaar, H.H.; Apperloo, L.; van Gosliga, D.; van den Berge, M.; Nawijn, M.C.; et al. Resveratrol and pterostilbene inhibit SARS-CoV-2 replication in air–liquid interface cultured human primary bronchial epithelial cells. Viruses 2021, 13, 1335. [Google Scholar] [CrossRef]
- AbdelMassih, A.; Yacoub, E.; Husseiny, R.J.; Kamel, A.; Hozaien, R.; El Shershaby, M.; Rajab, M.; Yacoub, S.; Eid, M.A.; Elahmady, M.; et al. Hypoxia-inducible factor (HIF): The link between obesity and COVID-19. Obes. Med. 2021, 22, 100317. [Google Scholar] [CrossRef] [PubMed]
- McLachlan, C.S. The angiotensin-converting enzyme 2 (ACE2) receptor in the prevention and treatment of COVID-19 are distinctly different paradigms. Clin. Hypertens. 2020, 26, 14. [Google Scholar] [CrossRef] [PubMed]
- Perrella, F.; Coppola, F.; Petrone, A.; Platella, C.; Montesarchio, D.; Stringaro, A.; Ravagnan, G.; Fuggetta, M.P.; Rega, N.; Musumeci, D. Interference of Polydatin/Resveratrol in the ACE2: Spike recognition during COVID-19 infection. A focus on their potential mechanism of action through computational and biochemical assays. Biomolecules 2021, 11, 1048. [Google Scholar] [CrossRef] [PubMed]
- Mittra, I.; de Souza, R.; Bhadade, R.; Madke, T.; Shankpal, P.; Joshi, M.; Qayyumi, B.; Bhattacharjee, A.; Gota, V.; Gupta, S.; et al. Resveratrol and Copper for treatment of severe COVID-19: An observational study (RESCU 002). medRxiv 2020. [Google Scholar] [CrossRef]
- Kelleni, M.T. Resveratrol-zinc nanoparticles or pterostilbene-zinc: Potential COVID-19 mono and adjuvant therapy. Biomed. Pharmacother. 2021, 139, 111626. [Google Scholar] [CrossRef]
- Abboud, R.; Charcosset, C.; Greige-Gerges, H. Interaction of triterpenoids with human serum albumin: A review. Chem. Phys. Lipids 2017, 207, 260–270. [Google Scholar] [CrossRef]
- Vattekkatte, A.; Garms, S.; Brandt, W.; Boland, W. Enhanced structural diversity in terpenoid biosynthesis: Enzymes, substrates and cofactors. Org. Biomol. Chem. 2018, 16, 348–362. [Google Scholar] [CrossRef]
- Ashour, M.; Wink, M.; Gershenzon, J. Biochemistry of terpenoids: Monoterpenes, sesquiterpenes and diterpenes. In Annual Plant Reviews Volume 40: Biochemistry of Plant Secondary Metabolism; Wiley: Hoboken, NJ, USA, 2010; pp. 258–303. ISBN 9781444320503. [Google Scholar] [CrossRef]
- Astani, A.; Schnitzler, P. Antiviral activity of monoterpenes beta-pinene and limonene against herpes simplex virus in vitro. Iran. J. Microbiol. 2014, 6, 149. [Google Scholar]
- Yang, Z.; Wu, N.; Zu, Y.; Fu, Y. Comparative anti-infectious bronchitis virus (IBV) activity of (-)-pinene: Effect on nucleocapsid (N) protein. Molecules 2011, 16, 1044–1054. [Google Scholar] [CrossRef]
- Zamora, A.P.; Edmonds, J.H.; Reynolds, M.J.; Khromykh, A.A.; Ralph, S.J. The in vitro and in vivo antiviral properties of combined monoterpene alcohols against West Nile virus infection. Virology 2016, 495, 18–32. [Google Scholar] [CrossRef]
- Bicchi, C.; Rubiolo, P.; Ballero, M.; Sanna, C.; Matteodo, M.; Esposito, F.; Zinzula, L.; Tramontano, E. HIV-1-inhibiting activity of the essential oil of Ridolfia segetum and Oenanthe crocata. Planta Med. 2009, 75, 1331–1335. [Google Scholar] [CrossRef] [PubMed]
- Cinatl, J.; Morgenstern, B.; Bauer, G.; Chandra, P.; Rabenau, H.; Doerr, H. Glycyrrhizin, an active component of liquorice roots, and replication of SARS-associated coronavirus. Lancet 2003, 361, 2045–2046. [Google Scholar] [CrossRef]
- Haiying, L.; Na, H.; Xiaoyuan, X. The curative effects of glycyrrhizin on patients with SARS. In Annual Meeting of the Society of Infectious and Parasitic Diseases; Chinese Medical Association: Wuhan, China, 2003; pp. 18–22. [Google Scholar]
- Ebrahimi, M.; Farhadian, N.; Amiri, A.R.; Hataminia, F.; Soflaei, S.S.; Karimi, M. Evaluating the efficacy of extracted squalene from seed oil in the form of microemulsion for the treatment of COVID-19: A clinical study. J. Med. Virol. 2022, 94, 119–130. [Google Scholar] [CrossRef] [PubMed]
- Loizzo, M.R.; Saab, A.M.; Tundis, R.; Statti, G.A.; Menichini, F.; Lampronti, I.; Gambari, R.; Cinatl, J.; Doerr, H.W. Phytochemical analysis and in vitro antiviral activities of the essential oils of seven Lebanon species. Chem. Biodivers. 2008, 5, 461–470. [Google Scholar] [CrossRef]
- Chatow, L.; Nudel, A.; Nesher, I.; Hayo Hemo, D.; Rozenberg, P.; Voropaev, H.; Winkler, I.; Levy, R.; Kerem, Z.; Yaniv, Z.; et al. In vitro evaluation of the activity of terpenes and cannabidiol against human coronavirus E229. Life 2021, 11, 290. [Google Scholar] [CrossRef]
- Ibrahim, M.A.; Abdelrahman, A.H.; Mohamed, T.A.; Atia, M.A.; Al-Hammady, M.A.; Abdeljawaad, K.A.; Elkady, E.M.; Moustafa, M.F.; Alrumaihi, F.; Allemailem, K.S.; et al. In silico mining of terpenes from red-sea invertebrates for SARS-CoV-2 main protease (Mpro) inhibitors. Molecules 2021, 26, 2082. [Google Scholar] [CrossRef]
- Meeran, M.N.; Seenipandi, A.; Javed, H.; Sharma, C.; Hashiesh, H.M.; Goyal, S.N.; Jha, N.K.; Ojha, S. Can limonene be a possible candidate for evaluation as an agent or adjuvant against infection, immunity, and inflammation in COVID-19? Heliyon 2021, 7, e05703. [Google Scholar] [CrossRef]
- Maiani, G.; Periago Castón, M.J.; Catasta, G.; Toti, E.; Cambrodón, I.G.; Bysted, A.; Granado-Lorencio, F.; Olmedilla-Alonso, B.; Knuthsen, P.; Valoti, M.; et al. Carotenoids: Actual knowledge on food sources, intakes, stability and bioavailability and their protective role in humans. Mol. Nutr. Food Res. 2009, 53, S194–S218. [Google Scholar] [CrossRef]
- Mueller, L.; Boehm, V. Antioxidant activity of β-carotene compounds in different in vitro assays. Molecules 2011, 16, 1055–1069. [Google Scholar] [CrossRef]
- Kaulmann, A.; Bohn, T. Carotenoids, inflammation, and oxidative stress—Implications of cellular signaling pathways and relation to chronic disease prevention. Nutr. Res. 2014, 34, 907–929. [Google Scholar] [CrossRef]
- Khalil, A.; Tazeddinova, D.; Aljoumaa, K.; Kazhmukhanbetkyzy, Z.A.; Orazov, A.; Toshev, A.D. Carotenoids: Therapeutic Strategy in the Battle against Viral Emerging Diseases, COVID-19: An Overview. Prev. Nutr. Food. Sci. 2021, 26, 241. [Google Scholar] [CrossRef] [PubMed]
- Yim, S.-K.; Kim, I.; Warren, B.; Kim, J.; Jung, K.; Ku, B. Antiviral Activity of Two Marine Carotenoids against SARS-CoV-2 Virus Entry In Silico and In Vitro. Int. J. Mol. Sci. 2021, 22, 6481. [Google Scholar] [CrossRef] [PubMed]
- El Midaoui, A.; Ghzaiel, I.; Vervandier-Fasseur, D.; Ksila, M.; Zarrouk, A.; Nury, T.; Khallouki, F.; El Hessni, A.; Ibrahimi, S.O.; Latruffe, N.; et al. Saffron (Crocus sativus L.): A source of nutrients for health and for the treatment of neuropsychiatric and age-related diseases. Nutrients 2022, 14, 597. [Google Scholar] [CrossRef] [PubMed]
- Lembo, D.; Cagno, V.; Civra, A.; Poli, G. Oxysterols: An emerging class of broad spectrum antiviral effectors. Mol. Aspects Med. 2016, 49, 23–30. [Google Scholar] [CrossRef] [PubMed]
- Foo, C.X.; Bartlett, S.; Ronacher, K. Oxysterols in the Immune Response to Bacterial and Viral Infections. Cells 2022, 11, 201. [Google Scholar] [CrossRef] [PubMed]
- Ohashi, H.; Wang, F.; Stappenbeck, F.; Tsuchimoto, K.; Kobayashi, C.; Saso, W.; Kataoka, M.; Yamasaki, M.; Kuramochi, K.; Muramatsu, M.; et al. Identification of anti-severe acute respiratory syndrome-related coronavirus 2 (SARS-CoV-2) oxysterol derivatives in vitro. Int. J. Mol. Sci. 2021, 22, 3163. [Google Scholar] [CrossRef]
- Straughn, A.R.; Kakar, S.S. Withaferin A: A potential therapeutic agent against COVID-19 infection. J. Ovarian Res. 2020, 13, 79. [Google Scholar] [CrossRef]
- Vandyck, K.; Deval, J. Considerations for the discovery and development of 3-chymotrypsin-like cysteine protease inhibitors targeting SARS-CoV-2 infection. Curr. Opin. Virol. 2021, 49, 36–40. [Google Scholar] [CrossRef]
- Gyebi, G.A.; Ogunyemi, O.M.; Ibrahim, I.M.; Afolabi, S.O.; Adebayo, J.O. Dual targeting of cytokine storm and viral replication in COVID-19 by plant-derived steroidal pregnanes: An in silico perspective. Comput. Biol. Med. 2021, 134, 104406. [Google Scholar] [CrossRef]
- Kritchevsky, D. Phytosterols. Diet. Fiber Health Dis. 2021, 134, 104406. [Google Scholar] [CrossRef]
- Lizard, G. Phytosterols: To be or not to be toxic; that is the question. Br. J. Nutr. 2008, 100, 1150–1151. [Google Scholar] [CrossRef] [PubMed]
- Ping, F.; Wang, Y.; Shen, X.; Tan, C.; Zhu, L.; Xing, W.; Xu, J. Virtual Screening and Molecular Docking to Study the Mechanism of Chinese Medicines in the Treatment of Coronavirus Infection. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2022, 28, e934102. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.; Yang, J. A review of the latest research on M pro targeting SARS-COV inhibitors. RSC Med. Chem. 2021, 12, 1026–1036. [Google Scholar] [CrossRef] [PubMed]
- Roy, A.; Menon, T. Evaluation of bioactive compounds from Boswellia serrata against SARS-CoV-2. Vegetos 2021, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Abdul-Hammed, M.; Adedotun, I.O.; Olajide, M.; Irabor, C.O.; Afolabi, T.I.; Gbadebo, I.O.; Rhyman, L.; Ramasami, P. Virtual screening, ADMET profiling, PASS prediction, and bioactivity studies of potential inhibitory roles of alkaloids, phytosterols, and flavonoids against COVID-19 main protease (Mpro). Nat. Prod. Res. 2021, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Kiani, A.K.; Dhuli, K.; Anpilogov, K.; Bressan, S.; Dautaj, A.; Dundar, M.; Beccari, T.; Ergoren, M.C.; Bertelli, M. Natural compounds as inhibitors of SARS-CoV-2 endocytosis: A promising approach against COVID-19. Acta Bio Med. Atenei Parmensis 2020, 91, e2020008. [Google Scholar] [CrossRef]
- Nivetha, R.; Bhuvaragavan, S.; Muthu Kumar, T.; Ramanathan, K.; Janarthanan, S. Inhibition of multiple SARS-CoV-2 proteins by an antiviral biomolecule, seselin from Aegle marmelos deciphered using molecular docking analysis. J. Biomol. Struct. Dyn. 2021, 1–12. [Google Scholar] [CrossRef]
- Kumar, M.P.; Sundaram, K.M.; Ramasamy, M. Coronavirus spike (S) glycoprotein (2019-ncov) targeted siddha medicines kabasura kudineer and thonthasura kudineer–in silico evidence for corona viral drug. Asian J. Pharm. Res. Health Care 2020, 12, 20–27. [Google Scholar] [CrossRef]
- Jalali, A.; Dabaghian, F.; Akbrialiabad, H.; Foroughinia, F.; Zarshenas, M.M. A pharmacology-based comprehensive review on medicinal plants and phytoactive constituents possibly effective in the management of COVID-19. Phytother. Res. 2021, 35, 1925–1938. [Google Scholar] [CrossRef]
- Khan, M.Y.; Kumar, V. Mechanism & inhibition kinetics of bioassay-guided fractions of Indian medicinal plants and foods as ACE inhibitors. J. Tradit. Complement. Med. 2019, 9, 73–84. [Google Scholar] [CrossRef]
- Liang, S.; Junwei, N.; Chunhua, W.; Baoying, H.; Wenling, W.; Na, Z.; Yao, D.; Huijuan, W.; Fei, Y.; Shan, C.; et al. High-Throughput Screening and Identification of Potent Broad-Spectrum Inhibitors of Coronaviruses. J. Virol. 2022, 93, e00023-19. [Google Scholar] [CrossRef]
- Yang, Y.; Islam, M.S.; Wang, J.; Li, Y.; Chen, X. Traditional Chinese medicine in the treatment of patients infected with 2019-new coronavirus (SARS-CoV-2): A review and perspective. Int. J. Biol. Sci. 2020, 16, 1708. [Google Scholar] [CrossRef] [PubMed]
- Sohail, M.I.; Siddiqui, A.; Erum, N.; Kamran, M. Phytomedicine and the COVID-19 pandemic. In Phytomedicine; Elsevier: Amsterdam, The Netherlands, 2021; pp. 693–708. [Google Scholar] [CrossRef]
- Mazraedoost, S.; Behbudi, G.; Mousavi, S.M.; Hashemi, S.A. COVID-19 treatment by plant compounds. Adv. Nano Res. Technol. 2021, 2, 23–33. [Google Scholar] [CrossRef]
- Jahan, I.; Ahmet, O. Potentials of plant-based substance to inhabit and probable cure for the COVID-19. Turk. J. Biol. 2020, 44, 228–241. [Google Scholar] [CrossRef] [PubMed]
- Shree, P.; Mishra, P.; Selvaraj, C.; Singh, S.K.; Chaube, R.; Garg, N.; Tripathi, Y.B. Targeting COVID-19 (SARS-CoV-2) main protease through active phytochemicals of ayurvedic medicinal plants–Withania somnifera (Ashwagandha), Tinospora cordifolia (Giloy) and Ocimum sanctum (Tulsi)—A molecular docking study. J. Biomol. Struct. Dyn. 2022, 40, 190–203. [Google Scholar] [CrossRef]
- Infusino, F.; Marazzato, M.; Mancone, M.; Fedele, F.; Mastroianni, C.M.; Severino, P.; Ceccarelli, G.; Santinelli, L.; Cavarretta, E.; Marullo, A.G.M.; et al. Diet supplementation, probiotics, and nutraceuticals in SARS-CoV-2 infection: A scoping review. Nutrients 2020, 12, 1718. [Google Scholar] [CrossRef]
- Childs, C.E.; Calder, P.C.; Miles, E.A. Diet and Immune Function. Nutrients 2019, 11, 1933. [Google Scholar] [CrossRef]
- Muscogiuri, G.; Barrea, L.; Savastano, S.; Colao, A. Nutritional recommendations for CoVID-19 quarantine. Eur. J. Clin. Nutr. 2020, 74, 850–851. [Google Scholar] [CrossRef]
- Kiewiet, M.B.; Faas, M.M.; De Vos, P. Immunomodulatory protein hydrolysates and their application. Nutrients 2018, 10, 904. [Google Scholar] [CrossRef]
- Cruzat, V.; Macedo Rogero, M.; Noel Keane, K.; Curi, R.; Newsholme, P. Glutamine: Metabolism and immune function, supplementation and clinical translation. Nutrients 2018, 10, 1564. [Google Scholar] [CrossRef]
- Eguchi, K.; Fujitani, N.; Nakagawa, H.; Miyazaki, T. Prevention of respiratory syncytial virus infection with probiotic lactic acid bacterium Lactobacillus gasseri SBT2055. Sci. Rep. 2019, 9, 4812. [Google Scholar] [CrossRef] [PubMed]
- Xu, K.; Cai, H.; Shen, Y.; Ni, Q.; Chen, Y.; Hu, S.; Li, J.; Wang, H.; Yu, L.; Huang, H.; et al. Management of COVID-19: The Zhejiang experience. Zhejiang Da Xue Xue Bao 2020, 49, 147–157. [Google Scholar] [CrossRef] [PubMed]
- Chourasia, R.; Padhi, S.; Chiring Phukon, L.; Abedin, M.M.; Singh, S.P.; Rai, A.K. A potential peptide from soy cheese produced using Lactobacillus delbrueckii WS4 for effective inhibition of SARS-CoV-2 main protease and S1 glycoprotein. Front. Mol. Biosci. 2020, 7, 601753. [Google Scholar] [CrossRef] [PubMed]
- Çakır, B.; Okuyan, B.; Şener, G.; Tunali-Akbay, T. Investigation of beta-lactoglobulin derived bioactive peptides against SARS-CoV-2 (COVID-19): In silico analysis. Eur. J. Pharmacol. 2021, 891, 173781. [Google Scholar] [CrossRef]
- Rimbach, G.; Minihane, A.M.; Majewicz, J.; Fischer, A.; Pallauf, J.; Virgli, F.; Weinberg, P.D. Regulation of cell signalling by vitamin E. Proc. Nutr. Soc. 2002, 61, 415–425. [Google Scholar] [CrossRef]
- Drewnowski, A. The Nutrient Rich Foods Index helps to identify healthy, affordable foods. Am. J. Clin. Nutr. 2010, 91, 1095S–1101S. [Google Scholar] [CrossRef]
- May, J.M.; Harrison, F.E. Role of vitamin C in the function of the vascular endothelium. Antioxid. Redox Signal. 2013, 19, 2068–2083. [Google Scholar] [CrossRef]
- Carr, A.C.; Maggini, S. Vitamin C and immune function. Nutrients 2017, 9, 1211. [Google Scholar] [CrossRef]
- Horowitz, R.I.; Freeman, P.R.; Bruzzese, J. Efficacy of glutathione therapy in relieving dyspnea associated with COVID-19 pneumonia: A report of 2 cases. Respir. Med. Case Rep. 2020, 30, 101063. [Google Scholar] [CrossRef]
- Yedjou, C.G.; Njiki, S.; Enow, J.; Ikome, O.; Latinwo, L.; Long, R.; Ngnepieba, P.; Alo, R.A.; Tchounwou, P.B. Pharmacological Effects of Selected Medicinal Plants and Vitamins against COVID-19. Jacobs J. Food. Nutr. 2021, 7, 1–16. [Google Scholar] [CrossRef]
- Chiscano-Camón, L.; Ruiz-Rodriguez, J.C.; Ruiz-Sanmartin, A.; Roca, O.; Ferrer, R. Vitamin C levels in patients with SARS-CoV-2-associated acute respiratory distress syndrome. Crit. Care 2020, 24, 522. [Google Scholar] [CrossRef] [PubMed]
- Hemilä, H.; Chalker, E. Vitamin C may reduce the duration of mechanical ventilation in critically ill patients: A meta-regression analysis. J. Intensive Care 2020, 8, 15. [Google Scholar] [CrossRef] [PubMed]
- Hemilä, H.; Chalker, E. Vitamin C can shorten the length of stay in the ICU: A meta-analysis. Nutrients 2019, 11, 708. [Google Scholar] [CrossRef]
- Panagiotou, G.; Tee, S.A.; Ihsan, Y.; Athar, W.; Marchitelli, G.; Kelly, D.; Boot, C.S.; Stock, N.; Macfarlane, J.; Martineau, A.R.; et al. Low serum 25-hydroxyvitamin D (25 [OH] D) levels in patients hospitalised with COVID-19 are associated with greater disease severity: Results of a local audit of practice. medRxiv 2020. [Google Scholar] [CrossRef]
- Suaini, N.H.; Zhang, Y.; Vuillermin, P.J.; Allen, K.J.; Harrison, L.C. Immune modulation by vitamin D and its relevance to food allergy. Nutrients 2015, 7, 6088–6108. [Google Scholar] [CrossRef] [PubMed]
- Sassi, F.; Tamone, C.; D’Amelio, P. Vitamin D: Nutrient, hormone, and immunomodulator. Nutrients 2018, 10, 1656. [Google Scholar] [CrossRef]
- Jain, A.; Chaurasia, R.; Sengar, N.S.; Singh, M.; Mahor, S.; Narain, S. Analysis of vitamin D level among asymptomatic and critically ill COVID-19 patients and its correlation with inflammatory markers. Sci. Rep. 2020, 10, 20191. [Google Scholar] [CrossRef]
- Abdel-Mottaleb, M.S.; Abdel-Mottaleb, Y. In search for effective and safe drugs against SARS-CoV-2: Part III] The electronic factors of Remdesivir and the naturally extracted Aspirochlorine drugs. ChemRxiv 2020. preprint. [Google Scholar] [CrossRef]
- Lee, G.Y.; Han, S.N. The role of vitamin E in immunity. Nutrients 2018, 10, 1614. [Google Scholar] [CrossRef]
- Tavakol, S.; Seifalian, A.M. Vitamin E at a high dose as an anti-ferroptosis drug and not just a supplement for COVID-19 treatment. Appl. Biochem. Biotechnol. 2022, 3, 601–619. [Google Scholar] [CrossRef]
- Calder, P.C.; Carr, A.C.; Gombart, A.F.; Eggersdorfer, M. Optimal nutritional status for a well-functioning immune system is an important factor to protect against viral infections. Nutrients 2020, 12, 1181. [Google Scholar] [CrossRef] [PubMed]
- Berendsen, A.A.; van Lieshout, L.E.; van den Heuvel, E.G.; Matthys, C.; Péter, S.; de Groot, L.C. Conventional foods, followed by dietary supplements and fortified foods, are the key sources of vitamin D, vitamin B6, and selenium intake in Dutch participants of the NU-AGE study. Nutr. Res. 2016, 36, 1171–1181. [Google Scholar] [CrossRef] [PubMed]
- Edeas, M.; Saleh, J.; Peyssonnaux, C. Iron: Innocent bystander or vicious culprit in COVID-19 pathogenesis? J. Infect. Dis. 2020, 97, 303–305. [Google Scholar] [CrossRef] [PubMed]
- Avery, J.C.; Hoffmann, P.R. Selenium, selenoproteins, and immunity. Nutrients 2018, 10, 1203. [Google Scholar] [CrossRef]
- Moghaddam, A.; Heller, R.A.; Sun, Q.; Seelig, J.; Cherkezov, A.; Seibert, L.; Hackler, J.; Seemann, P.; Diegmann, J.; Pilz, M.; et al. Selenium deficiency is associated with mortality risk from COVID-19. Nutrients 2020, 12, 2098. [Google Scholar] [CrossRef]
- Darwesh, A.M.; Bassiouni, W.; Sosnowski, D.K.; Seubert, J.M. Can N-3 polyunsaturated fatty acids be considered a potential adjuvant therapy for COVID-19-associated cardiovascular complications? Pharmacol. Ther. 2021, 219, 107703. [Google Scholar] [CrossRef]
- Pradelli, L.; Mayer, K.; Klek, S.; Omar Alsaleh, A.J.; Clark, R.A.; Rosenthal, M.D.; Axel, R.; Heller, M.D.; Maurizio Muscaritoli, M.D. ω-3 fatty-acid enriched parenteral nutrition in hospitalized patients: Systematic review with meta-analysis and trial sequential analysis. J. Parenter. Enter. Nutr. 2020, 44, 44–57. [Google Scholar] [CrossRef]
- Bistrian, B.R. Parenteral fish-oil emulsions in critically Ill COVID-19 emulsions. J. Parenter. Enter. Nutr. 2020, 44, 1168. [Google Scholar] [CrossRef]
- Baral, P.K.; Amin, M.T.; Rashid, M.; Or, M.; Hossain, M.S. Assessment of Polyunsaturated Fatty Acids on COVID-19-Associated Risk Reduction. Rev. Bras. Farmacogn. 2022, 32, 50–64. [Google Scholar] [CrossRef]
- Shakoor, H.; Feehan, J.; Mikkelsen, K.; Al Dhaheri, A.S.; Ali, H.I.; Platat, C.; Ismail, L.C.; Stojanovska, L.; Apostolopoulos, V. Be well: A potential role for vitamin B in COVID-19. Maturitas 2021, 144, 108–111. [Google Scholar] [CrossRef]
- Tang, C.-F.; Ding, H.; Jiao, R.-Q.; Wu, X.-X.; Kong, L.-D. Possibility of magnesium supplementation for supportive treatment in patients with COVID-19. Eur. J. Pharmacol. 2020, 886, 173546. [Google Scholar] [CrossRef] [PubMed]
- Pal, A.; Squitti, R.; Picozza, M.; Pawar, A.; Rongioletti, M.; Dutta, A.K.; Sahoo, S.; Goswami, K.; Sharma, P.; Prasad, R. Zinc and COVID-19: Basis of current clinical trials. Biol. Trace Elem. Res. 2021, 199, 2882–2892. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Saad, R.; Taylor, E.W.; Rayman, M.P. Selenium and selenoproteins in viral infection with potential relevance to COVID-19. Redox. Biol. 2020, 37, 101715. [Google Scholar] [CrossRef] [PubMed]
- Bhar, A. Is It Possible to Ensure COVID19 Vaccine Supply by Using Plants? Springer: Berlin/Heidelberg, Germany, 2021; pp. 137–141. [Google Scholar] [CrossRef]
- Rosales-Mendoza, S.; Márquez-Escobar, V.A.; González-Ortega, O.; Nieto-Gómez, R.; Arévalo-Villalobos, J.I. What does plant-based vaccine technology offer to the fight against COVID-19? Vaccines 2020, 8, 183. [Google Scholar] [CrossRef]
- Rybicki, E.P. Plant-based vaccines against viruses. Virol. J. 2014, 11, 205. [Google Scholar] [CrossRef]
- Mahmood, N.; Nasir, S.B.; Hefferon, K. Plant-based drugs and vaccines for COVID-19. Vaccines 2021, 9, 15. [Google Scholar] [CrossRef]
- Dhama, K.; Natesan, S.; Iqbal Yatoo, M.; Patel, S.K.; Tiwari, R.; Saxena, S.K.; Harapan, H. Plant-based vaccines and antibodies to combat COVID-19: Current status and prospects. Hum. Vaccines Immunother. 2020, 16, 2913–2920. [Google Scholar] [CrossRef]
- Yonesi, M.; Rezazadeh, A. Plants as a prospective source of natural anti-viral compounds and oral vaccines against COVID-19 coronavirus. Preprints 2020, 2020040321. [Google Scholar] [CrossRef]
- Maharjan, P.M.; Choe, S. Plant-based COVID-19 vaccines: Current status, design, and development strategies of candidate vaccines. Vaccines 2021, 9, 992. [Google Scholar] [CrossRef]
- Shanmugaraj, B.; Siriwattananon, K.; Malla, A.; Phoolcharoen, W. Potential for developing plant-derived candidate vaccines and biologics against emerging coronavirus infections. Pathogens 2021, 10, 1051. [Google Scholar] [CrossRef]
- Mason, H.S.; Lam, D.; Arntzen, C.J. Expression of hepatitis B surface antigen in transgenic plants. Proc. Natl. Acad. Sci. USA 1992, 89, 11745–11749. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.U.; Kadiresen, K.; Gan, W.C.; Ling, A.P.K. Current updates and research on plant-based vaccines for coronavirus disease 2019. Clin. Exp. Vaccine Res. 2021, 10, 13. [Google Scholar] [CrossRef] [PubMed]
- Ward, B.J.; Gobeil, P.; Séguin, A.; Atkins, J.; Boulay, I.; Charbonneau, P.-Y.; Couture, M.; D’Aoust, M.-A.; Dhaliwall, J.; Finkle, C.; et al. Phase 1 randomized trial of a plant-derived virus-like particle vaccine for COVID-19. Nat. Med. 2021, 27, 1071–1078. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Latin/Vernacular Names | Nature of Extracts or Components | Mode of Action | Refs. |
|---|---|---|---|
| Aegle marmelos L./Bael | Purified seselin | Inhibitory potential over multiple SARS-COV-2 targets such as SARS-CoV-2S spike protein, COVID-19 main protease and free enzyme of the SARS-CoV-2 (2019-nCoV) main protease. | [103] |
| Anacyclus pyrethrum L./Akarkara | Pyrethrin | Acts as ligands with viral proteins to prevent the binding of host receptors and the fusion leading to viral replication. | [104] |
| Andrographis paniculata Burm.f./Creat | Andrographolide/Andrographiside | ACE inhibition/SARS-3CLpro inhibition of the NOD-like receptor protein 3 (NLRP3), caspase-1 and interleukin-1β (IL-1β) particules. | [11,39,105] |
| Asparagus racemosus L./Willd | Hydroalcoholic crude extract | ACE inhibition/IC50 = 82.88%. | [106] |
| Camellia sinensis L./Tea plant | Polyphenol (Rutin), theaflavin-3,30-digallate, tannic acid, [−]-epigallocatechin gallate) | ACE inhibition, SARS-3CLpro inhibition. | [105] |
| Carapichea ipecacuanha L./Ipecacuanha | Emetine | Displayed strong anti-CoV activity by blocking MERSCoV entry consistent with pseudovirus entry assays. | [107] |
| Citrus Spp./Citrus | Hesperetin, hesperidin Rhoifolin, Neohesperidin | SARS-3CLpro inhibition in a dose-dependent manner. | [105] |
| Curcuma longa L./Turmeric | Curcumin and its analogue | In a molecular docking study, curcumin and few of its derivatives are suggested as SARS-CoV-2 spike protein inhibitors. | [11] |
| Cynara scolymus L./Globe artichoke | Cynaroside | ACE inhibition/IC50 = 49.7% | [105] |
| Dioscorea batatas L./Chinese yam | - | SARS-3CLpro inhibition/ IC50 = 44 μg/mL. | [105] |
| Erigeron abajoensis L./Cronquist | Flavone (Scutellarin) | ACE inhibition. | [105] |
| Equisetum hyemale L./Rough horsetail | Herbacetin | 3CL inhibitory activity. | [105] |
| Galla chinensis L./Chinese sumac | Tetra-O-galloyl-β-D-glucose | Binding with surface spike protein of SARS-CoV. | [108] |
| Glycyrrhiza glabra L./Black sugar | Glycyrrhizin | Inhibition of COVID-19 replication and entry to its host cells. Glycyrrhizin can inhibit ACE with IC50 > 40%. | [105,108,109] |
| Linum usitatissimum L./Linseed | Herbacetin | SARS-3CLpro inhibition. | [105] |
| Hancornia speciosa L./Gomes | Chlorogenic acid | ACE inhibition. | [105] |
| Houttuynia cordata Thunb./Fish mint | The aqueous extract | Inhibition of RNA-dependent RNA polymerase (RdRp), 3CL-like protease and viral polymerase. | [108,109,110,111] |
| Hypericum perforatum L./St. Johnswort | Hypericin | C-terminal and N-terminal domains of 2019-nCoV NSP 14 can bind Hypericin. | [108] |
| Isatis indigotica L./Woad | Phenol (indigo, sinigrin, aloe emodin, hesperetin, sinigrin), 2,2-Di(3-indolyl)-3-indolone, phaitanthrin D | Inhibit the cleavage activity of SARS-3CLpro enzyme/IC50 = 53.8 ± 4.2 μg/mL. | [105,108,109] |
| Litchi chinensis L./Litchee | Flavonoids such as rhoifolin, pectolinarin, Epigallocatechin gallate, Gallocatechin gallate, quercetin and herbacetin | Inhibition of SARS-3CLpro activity. | [109] |
| Lycoris radiata L./Red spider lily | Glycyrrhizic acid derivatives | Reduction or inhibition of penetration and viral attachment (IC50 = 2.4 ± 0.2 μg/mL). | [110] |
| Nigella sativa L./Black cumin | Nigellidine and α-hederin | High potential to act as COVID-19 treatment in docking studies. | [50] |
| Ocimum sanctum L./Holy basil | Tulsinol and dihydroeugenol | Effective against SARS CoV 2 in molecular docking studies. | [11] |
| Polygonum Multiflorum Thunb./Chinese knotweed | Emodin | Inhibit interaction of SARS-CoV spike protein and ACE2. Inhibit the 3a ion channel of coronavirus SARS-CoV. | [108,111] |
| Psoralea corylifolia L./Purple fleabane | Bavachinin, psoralidin Corylifol | The ethanol extracts of these secondary metabolites show high activity against SARS-CoVPLpro. | [111] |
| Rheum officinale Baill./Chinese rhubarb | Anthraquinone (Emodin) | Positive ACE inhibitor in combination with ACEI/ARB agents. Inhibition of the interaction between SARS-CoV S (IC50 = 1 to 10 μg/mL). In a dose-dependent manner, it drastically blocked the interaction of the ACE2 enzyme of host cell and viral S protein. | [105,110,111] |
| Sambucus Formosana Nakai/Chinese elder | Ethanol extract | Significant reduction in virus yield, plaque formation and virus attachment. | [36] |
| Scutellaria baicalensis L./Georgi | Baicalin, cosmosiin | ACE inhibition and SARS-3CLpro inhibition. | [105,108,109] |
| Toona sinensis Roem./Chinese mahogany | Quercetin and TSL-1 | Inhibition of the cellular entry of SARS-CoV. | [108] |
| Torreya nucifera L./Japanese torreya | Amentoflavone and Apigenin | Showed the most potent 3CLpro inhibitory effect. | [111] |
| Tylophora indica L./Indian ipecac | Tylophorine | Tylophorine-based biomolecules exhibit broad spectrum potential for inhibiting coronaviruses. | [108] |
| Veronicalina riifolia L./Speedwell | Luteolin | Avidly binds with surface spike protein of SARS-CoV. | [108] |
| Withania somnifera (L.) Dunal/Winter cherry | Withanone and withaferin | Effective against SARS CoV-2 in bioinformatic studies. In molecular docking, inhibitors against SARS-CoV-2 Mpro (Main protease). | [11,112] |
| Nutrients Types | Mode of Action against COVID-19 | Refs. |
|---|---|---|
| Macronutrients | ||
| Protein | Oral and IV glutathione, glutathione precursors (N-acetyl-cysteine) block NF-κB. A trial of 2 g of IV improved dyspnea of patients within 1 h of use. Repeated use of both 2000 mg IV glutathione was effective in further relieving respiratory symptoms. | [126] |
| Polyunsaturated fatty acids | Suppress inflammation and augment phagocytosis. Exhibit anti-inflammatory, vasodilatory and platelet anti-aggregatory effects. | [146] |
| Probiotics | Inhibit SARS-CoV-2 main protease, S1 glycoprotein and angiotensin-converting enzyme. | [120,121] |
| Micronutrients | ||
| Vitamin B-complexes |
Vit B1 acts as a carbonic anhydrase isoenzyme inhibitor. Vit B2-UV decreases the infectious titer of SARS-CoV-2 below the limit of detection in human blood and in plasma and platelet products. Vit B9 and its derivatives have strong and stable binding affinities against the SARS-CoV-2, through structure-based molecular docking. | [147] |
| Vitamin C | Inhibits cytokine storm through reducing inflammation rate and respiratory tract infection | [1] |
| Vitamin D | Vitamin D tablets can be taken to reduce mortality rate and suppress cytokine storm in the human body. | [1] |
| Vitamin E | Inactivation of 15-lipoxygenase by the reduction of Fe3+ to Fe2+ leading to ferroptosis prevention. | [137] |
| Magnesium | Reduction in lung inflammation response and oxidative stress, and inhibition of bronchial smooth muscle contraction; favors bronchodilation. | [148] |
| Zinc | Doxycycline, a tetracycline antibiotic, is known to chelate Zn from matrix metalloproteinases, which may help in part to inhibit the COVID-19 infection by limiting its ability to replicate in the host. | [149] |
| Selenium | Enhance adaptive immunity by reinvigorating cytotoxic cells and moderating the release of inflammatory cytokines by the innate immune system. | [150] |
| B12 supplements (500 μg), vitamin D (1000 IU) and magnesium | Reduce COVID-19 symptom severity and the need for oxygen and intensive care support. | [147] |
| Vitamin C and E | Ameliorate cardiac injuries of critically ill COVID-19 patients. | [143] |
| Copper, Iodine, Selenium, Zinc | Immune enhancers towards SARS CoV 2. | [1] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brahmi, F.; Vejux, A.; Ghzaiel, I.; Ksila, M.; Zarrouk, A.; Ghrairi, T.; Essadek, S.; Mandard, S.; Leoni, V.; Poli, G.; et al. Role of Diet and Nutrients in SARS-CoV-2 Infection: Incidence on Oxidative Stress, Inflammatory Status and Viral Production. Nutrients 2022, 14, 2194. https://doi.org/10.3390/nu14112194
Brahmi F, Vejux A, Ghzaiel I, Ksila M, Zarrouk A, Ghrairi T, Essadek S, Mandard S, Leoni V, Poli G, et al. Role of Diet and Nutrients in SARS-CoV-2 Infection: Incidence on Oxidative Stress, Inflammatory Status and Viral Production. Nutrients. 2022; 14(11):2194. https://doi.org/10.3390/nu14112194
Chicago/Turabian StyleBrahmi, Fatiha, Anne Vejux, Imen Ghzaiel, Mohamed Ksila, Amira Zarrouk, Taoufik Ghrairi, Soukena Essadek, Stéphane Mandard, Valerio Leoni, Giuseppe Poli, and et al. 2022. "Role of Diet and Nutrients in SARS-CoV-2 Infection: Incidence on Oxidative Stress, Inflammatory Status and Viral Production" Nutrients 14, no. 11: 2194. https://doi.org/10.3390/nu14112194
APA StyleBrahmi, F., Vejux, A., Ghzaiel, I., Ksila, M., Zarrouk, A., Ghrairi, T., Essadek, S., Mandard, S., Leoni, V., Poli, G., Vervandier-Fasseur, D., Kharoubi, O., El Midaoui, A., Atanasov, A. G., Meziane, S., Latruffe, N., Nasser, B., Bouhaouala-Zahar, B., Masmoudi-Kouki, O., ... Lizard, G. (2022). Role of Diet and Nutrients in SARS-CoV-2 Infection: Incidence on Oxidative Stress, Inflammatory Status and Viral Production. Nutrients, 14(11), 2194. https://doi.org/10.3390/nu14112194