
Synergistic Effects of Korean Red Ginseng Extract and the Conventional Systemic Therapeutics of Atopic Dermatitis in a Murine Model


Abstract
:1. Introduction
2. Materials and Methods
2.1. Animals
2.2. The Induction of AD-Like Skin Lesions
2.3. Animal Groups and Drugs
2.4. The Measurement of the Severity of AD and the Transepidermal Water Loss
2.5. Skin Histology and Immunohistochemical Examination
2.6. Enzyme-Linked Immunosorbent Assay (ELISA)
2.7. Statistical Analysis
3. Results
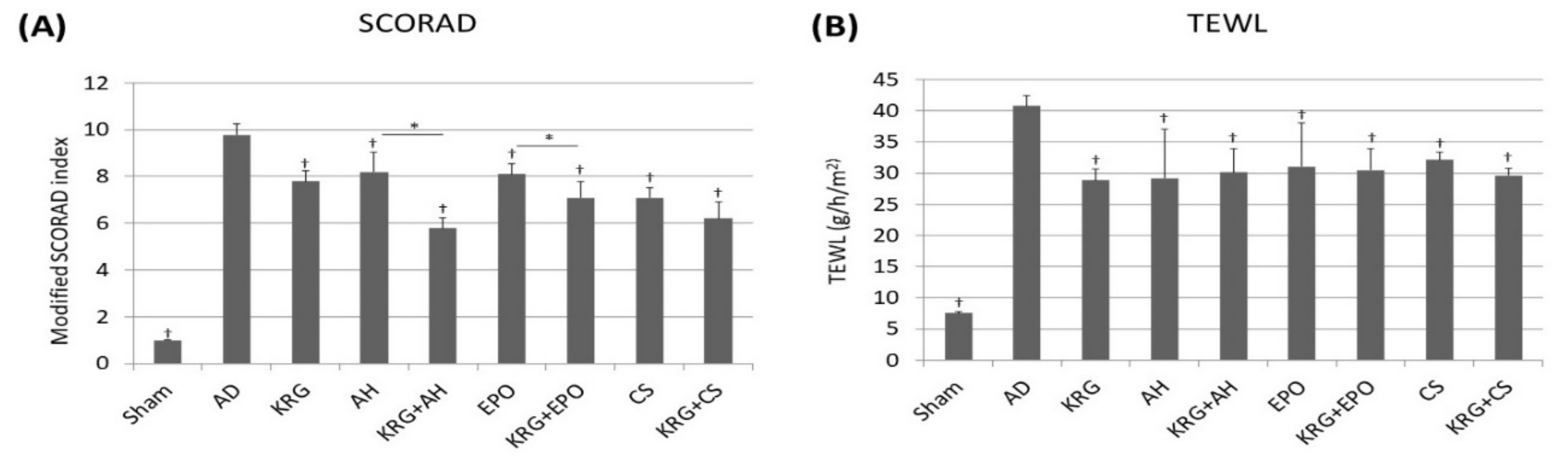
3.1. The Clinical Effects of KRG and the Conventional Systemic Therapeutics of AD on the Skin TNCB-Induced AD Mouse Model
3.2. The Histopathological Changes Caused by the Synergistic Effects of KRG and Conventional Systemic Therapeutics of AD in TNCB-Induced AD Mouse Model
3.3. Serum IgE Levels in TNCB-Induced AD Mouse Model That Was Administered KRG and Conventional Systemic Therapeutics of AD
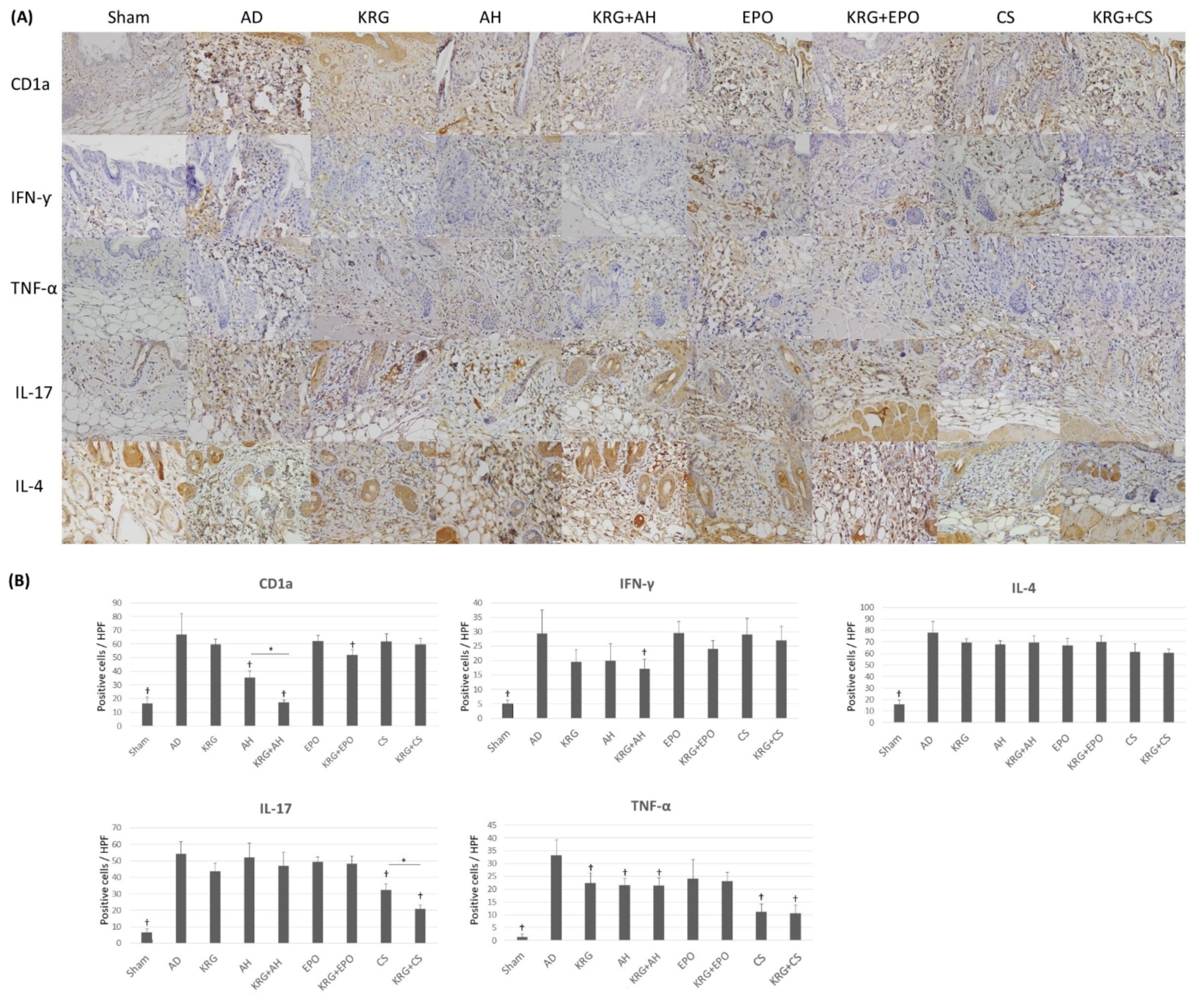
3.4. The Changes in the Expression Profiles of Various Cytokines after the Administration of KRG and Conventional Systemic Treatments of AD in TNCB-Induced AD Mouse Model
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Silverberg, J.I.; Gelfand, J.M.; Margolis, D.J.; Boguniewicz, M.; Fonacier, L.; Grayson, M.H.; Simpson, E.L.; Ong, P.Y.; Fuxench, Z.C.C. Patient burden and quality of life in atopic dermatitis in US adults: A population-based cross-sectional study. Ann. Allergy Asthma Immunol. 2018, 121, 340–347. [Google Scholar] [CrossRef] [Green Version]
- Boguniewicz, M.; Leung, D.Y. Atopic dermatitis: A disease of altered skin barrier and immune dysregulation. Immunol. Rev. 2011, 242, 233–246. [Google Scholar] [CrossRef]
- Yamanaka, K.; Mizutani, H. The role of cytokines/chemokines in the pathogenesis of atopic dermatitis. Pathog. Manag. Atopic Dermat. 2011, 41, 80–92. [Google Scholar]
- Novak, N.; Bieber, T. The role of dendritic cell subtypes in the pathophysiology of atopic dermatitis. J. Am. Acad. Dermatol. 2005, 53, S171–S176. [Google Scholar] [CrossRef]
- Chen, L.; Martinez, O.; Overbergh, L.; Mathieu, C.; Prabhakar, B.; Chan, L. Early up-regulation of Th2 cytokines and late surge of Th1 cytokines in an atopic dermatitis model. Clin. Exp. Immunol. 2004, 138, 375–387. [Google Scholar] [CrossRef]
- Stewart, J.; Morse, P.; Moss, M.; Horrobin Dphil, D.; Burton, J.; Douglas, W.; Gould, D.; Grattan, C.; Hindson, T.; Anderson, J. Treatment of severe and moderately severe atopic dermatitis with evening primrose oil (Epogam): A multi-centre study. J. Nutr. Med. 1991, 2, 9–15. [Google Scholar] [CrossRef]
- He, A.; Feldman, S.R.; Fleischer, A.B., Jr. An assessment of the use of antihistamines in the management of atopic dermatitis. J. Am. Acad. Dermatol. 2018, 79, 92–96. [Google Scholar] [CrossRef]
- Ring, J.; Alomar, A.; Bieber, T.; Deleuran, M.; Fink-Wagner, A.; Gelmetti, C.; Gieler, U.; Lipozencic, J.; Luger, T.; Oranje, A. Guidelines for treatment of atopic eczema (atopic dermatitis) Part II. J. Eur. Acad. Dermatol. Venereol. 2012, 26, 1176–1193. [Google Scholar] [CrossRef]
- Kim, J.E.; Kim, H.J.; Lew, B.-L.; Lee, K.H.; Hong, S.P.; Jang, Y.H.; Park, K.Y.; Seo, S.J.; Bae, J.M.; Choi, E.H. Consensus guidelines for the treatment of atopic dermatitis in Korea (part II): Systemic treatment. Ann. Dermatol. 2015, 27, 578–592. [Google Scholar] [CrossRef] [Green Version]
- Roekevisch, E.; Spuls, P.I.; Kuester, D.; Limpens, J.; Schmitt, J. Efficacy and safety of systemic treatments for moderate-to-severe atopic dermatitis: A systematic review. J. Allergy Clin. Immunol. 2014, 133, 429–438. [Google Scholar] [CrossRef]
- Kang, S.; Amagai, M.; Bruckner, A.L.; Enk, A.H.; Margolis, D.J.; McMichael, A.J.; Orringer, J.S. Fitzpatrick’s Dermatology in General Medicine, 9th ed.; McGrawHill Medical: New York, NY, USA, 2019; pp. 3520–3524. [Google Scholar]
- Sumiyoshi, M.; Sakanaka, M.; Kimura, Y. Effects of Red Ginseng extract on allergic reactions to food in Balb/c mice. J. Ethnopharmacol. 2010, 132, 206–212. [Google Scholar] [CrossRef]
- Kim, H.S.; Kim, D.H.; Kim, B.K.; Yoon, S.K.; Kim, M.H.; Lee, J.Y.; Kim, H.O.; Park, Y.M. Effects of topically applied Korean red ginseng and its genuine constituents on atopic dermatitis-like skin lesions in NC/Nga mice. Int. Immunopharmacol. 2011, 11, 280–285. [Google Scholar] [CrossRef]
- Makky, E.A. Korean Red Ginseng: Benefits Versus Precautions. INNOSC Theranostics Pharmacol. Sci. 2018, 1, 10–13. [Google Scholar] [CrossRef] [Green Version]
- Park, J.D.; Lee, Y.H.; Kim, S.I. Ginsenoside Rf 2, a new dammarane glycoside from Korean red ginseng (Panax ginseng). Arch. Pharmacal Res. 1998, 21, 615–617. [Google Scholar] [CrossRef]
- Lee, H.J.; Cho, S.H. Therapeutic effects of Korean red ginseng extract in a murine model of atopic dermatitis: Anti-pruritic and anti-inflammatory mechanism. J. Korean Med. Sci. 2017, 32, 679–687. [Google Scholar] [CrossRef] [PubMed]
- Cho, E.; Cho, S.H. Effects of Korean red ginseng extract on the prevention of atopic dermatitis and its mechanism on early lesions in a murine model. J. Ethnopharmacol. 2013, 145, 294–302. [Google Scholar] [CrossRef]
- Heo, J.H.; Lee, S.T.; Chu, K.; Oh, M.; Park, H.J.; Shim, J.Y.; Kim, M. An open-label trial of Korean red ginseng as an adjuvant treatment for cognitive impairment in patients with Alzheimer’s disease. Eur. J. Neurol. 2008, 15, 865–868. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Wang, H.; Zhang, M.; Shi, M.; Yang, C.; Ni, Q.; Wang, Q.; Li, J.; Wang, X.; Zhang, C. Safety and antifatigue effect of Korean Red ginseng capsule: A randomized, double-blind and placebo-controlled clinical trial. J. Ginseng Res. 2021, 43, 676–683. [Google Scholar] [CrossRef]
- Schafer, K.A.; Eighmy, J.; Fikes, J.D.; Halpern, W.G.; Hukkanen, R.R.; Long, G.G.; Meseck, E.K.; Patrick, D.J.; Thibodeau, M.S.; Wood, C.E.; et al. Use of severity grades to characterize histopathologic changes. Toxicol. Pathol. 2018, 46, 256–265. [Google Scholar] [CrossRef]
- Khattri, S.; Shemer, A.; Rozenblit, M.; Dhingra, N.; Czarnowicki, T.; Finney, R.; Gilleaudeau, P.; Sullivan-Whalen, M.; Zheng, X.; Xu, H. Cyclosporine in patients with atopic dermatitis modulates activated inflammatory pathways and reverses epidermal pathology. J. Allergy Clin. Immunol. 2014, 133, 1626–1634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Munro, C.; Higgins, E.; Marks, J.; Daly, B.; Friedmann, P.; Shuster, S. Cyclosporin A in atopic dermatitis: Therapeutic response is dissociated from effects on allergic reactions. Br. J. Dermatol. 1991, 124, 43–48. [Google Scholar] [CrossRef] [PubMed]
- Wahlgren, C.; Scheynius, A.; Hägermark, Ö. Antipruritic effect of oral cyclosporin A in atopic dermatitis. Acta Derm.-Venereol. 1990, 70, 323–329. [Google Scholar] [PubMed]
- Koga, C.; Kabashima, K.; Shiraishi, N.; Kobayashi, M.; Tokura, Y. Possible pathogenic role of Th17 cells for atopic dermatitis. J. Investig. Dermatol. 2008, 128, 2625–2630. [Google Scholar] [CrossRef] [Green Version]
- Noda, S.; Suárez-Fariñas, M.; Ungar, B.; Kim, S.J.; de Guzman Strong, C.; Xu, H.; Peng, X.; Estrada, Y.D.; Nakajima, S.; Honda, T.; et al. The Asian atopic dermatitis phenotype combines features of atopic dermatitis and psoriasis with increased TH17 polarization. J. Allergy Clin. Immunol. 2015, 136, 1254–1264. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Cho, S.H. Korean red ginseng extract ameliorates skin lesions in NC/Nga mice: An atopic dermatitis model. J. Ethnopharmacol. 2011, 133, 810–817. [Google Scholar] [CrossRef] [PubMed]
- Hussein, M.R. Evaluation of Langerhans’ cells in normal and eczematous dermatitis skin by CD1a protein immunohistochemistry: Preliminary findings. J. Cutan. Pathol. 2008, 35, 554–558. [Google Scholar] [CrossRef]
- de Jong, A.; Ogg, G. CD1a function in human skin disease. Mol. Immunol. 2021, 130, 14–19. [Google Scholar] [CrossRef]
- Klein, P.A.; Clark, R.A. An evidence-based review of the efficacy of antihistamines in relieving pruritus in atopic dermatitis. Arch. Dermatol. 1999, 135, 1522–1525. [Google Scholar] [CrossRef]
- Bamford, J.T.; Ray, S.; Musekiwa, A.; van Gool, C.; Humphreys, R.; Ernst, E. Oral evening primrose oil and borage oil for eczema. Cochrane Database Syst. Rev. 2013, 4, CD004416. [Google Scholar] [CrossRef]
- Bayles, B.; Usatine, R. Evening primrose oil. Am. Fam. Physician 2009, 80, 1405–1408. [Google Scholar]
- Blunder, S.; Rühl, R.; Moosbrugger-Martinz, V.; Krimmel, C.; Geisler, A.; Zhu, H.; Crumrine, D.; Elias, P.M.; Gruber, R.; Schmuth, M. Alterations in epidermal eicosanoid metabolism contribute to inflammation and impaired late differentiation in FLG-mutated atopic dermatitis. J. Investig. Dermatol. 2017, 137, 706–715. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tamura, Y.; Hirai, A.; Terano, T.; Tahara, K.; Saitoh, J.; Kondo, S.; Samukawa, K.; Yoshida, S. Effect of Korean Red Ginseng on Eicosanoid Biosynthesis in Platelets and Vascular Smooth Muscle Cells. In Proceedings of the Ginseng Society Conference; The Korean Society of Ginseng: Seoul, Korea, 1993; pp. 28–29. [Google Scholar]
- Lee, J.W.; Choi, Y.R.; Mok, H.J.; Seong, H.-A.; Lee, D.Y.; Kim, G.-S.; Yoon, J.H.; Kim, K.P.; Kim, H.D. Characterization of the changes in eicosanoid profiles of activated macrophages treated with 20 (S)-ginsenoside Rg3. J. Chromatogr. B 2017, 1065, 14–19. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Hematoxylin and Eosin | Sham | AD Control | KRG | AH | AH + KRG | EPO | EPO + KRG | CS | CS + KRG |
|---|---|---|---|---|---|---|---|---|---|
| Epidermal change | |||||||||
| Epidermal thickness | 22.61 ± 2.21 | 54.81 ± 4.60 | 42.54 ± 3.16 | 44.36 ± 6.50 | 41.46 ± 5.84 | 56.49 ± 8.66 | 38.31 ± 8.06 | 34.0 ± 7.39 | 27.17 ± 8.93 |
| Hyperkeratosis | 0.20 ± 0.44 | 2.60 ± 0.54 | 1.40 ± 0.54 | 1.40 ± 0.54 | 1.20 ± 0.44 | 2.00 ± 0.70 | 1.40 ± 0.54 | 2.40 ± 0.54 | 2.40 ± 0.54 |
| Spongiosis | 0.00 ± 0.00 | 1.80 ± 0.44 | 1.40 ± 0.54 | 1.40 ± 0.54 | 1.40 ± 0.54 | 1.60 ± 0.54 | 1.40 ± 0.54 | 1.60 ± 0.54 | 1.60 ± 0.54 |
| Dermal change | |||||||||
| Dermal inflammation | 0.61 ± 0.54 | 3.60 ± 0.54 | 2.60 ± 0.54 | 2.60 ± 0.54 | 1.40 ± 0.54 | 3.20 ± 0.44 | 3.00 ± 0.54 | 2.20 ± 0.44 | 1.40 ± 0.54 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Woo, Y.R.; Moon, S.H.; Yu, J.; Cho, S.H. Synergistic Effects of Korean Red Ginseng Extract and the Conventional Systemic Therapeutics of Atopic Dermatitis in a Murine Model. Nutrients 2022, 14, 133. https://doi.org/10.3390/nu14010133
Woo YR, Moon SH, Yu J, Cho SH. Synergistic Effects of Korean Red Ginseng Extract and the Conventional Systemic Therapeutics of Atopic Dermatitis in a Murine Model. Nutrients. 2022; 14(1):133. https://doi.org/10.3390/nu14010133
Chicago/Turabian StyleWoo, Yu Ri, Seok Hoon Moon, Jeesuk Yu, and Sang Hyun Cho. 2022. "Synergistic Effects of Korean Red Ginseng Extract and the Conventional Systemic Therapeutics of Atopic Dermatitis in a Murine Model" Nutrients 14, no. 1: 133. https://doi.org/10.3390/nu14010133
APA StyleWoo, Y. R., Moon, S. H., Yu, J., & Cho, S. H. (2022). Synergistic Effects of Korean Red Ginseng Extract and the Conventional Systemic Therapeutics of Atopic Dermatitis in a Murine Model. Nutrients, 14(1), 133. https://doi.org/10.3390/nu14010133